87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51

of 14
-
Upload
imranjan81 -
Category
Documents
-
view
222 -
download
0
Transcript of 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
1/14
C H A P T E R
3Summary of the Gross
Anatomy of theExtraocular Muscles
D escriptions of the gross anatomy of the extra-ocular muscles can be found readily in stan-dard texts, notably Wolffes Anatomy of the Eye ,now in its 8th edition, 3 Duke-Elder and Wybar, 12
Whitnall,38
and Fink,14
to mention only a few. Thischapter consists of a brief survey of the grossanatomy of these muscles, which is indispensablefor the understanding of how they function innormal and abnormal states.
In humans there are three pairs of extraocularmuscles in each orbit: a pair of horizontal rectusmuscles, a pair of vertical rectus muscles, and apair of oblique muscles. The four rectus musclescome from the depth of the orbit and are attachedto the sclera anterior to the equator near the cor-
nea. The two oblique muscles approach the globefrom in front, at the medial side of the orbit, andcontinue obliquely and laterally to insert on thesclera posterior to the equator on the temporal partof the globe. Contraction of the rectus musclespulls the globe backward and nasalward, and con-traction of the oblique muscles pulls the globeforward and nasalward. The two directions of pullform an angle of 100 to 110 , open toward thenasal side (Fig. 31). On the whole, therefore, apull nasalward is exerted by the tonus of these
muscles that must be balanced by the tension of the temporal part of Tenons capsule and by thesoft tissues nasal to the globe. The backward pullof the rectus muscles is only partly offset by the38
forward pull of the oblique muscles in a ratio of 1:5.5 relative to the axis YY of the globe (seeFig. 31) and only in a ratio of 1:12 relative tothe axis of the orbit (or the direction of pull of
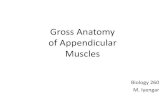
FIGURE 31. Relation of the eyes to the pull of the
horizontal rectus and oblique muscles, right eye. (Modi-ed from Zoth O: Augenbewegungen und Gesichtswahr-nehmungen. In Nagel W, ed: Handbuch der Physiologiedes Menschen, vol 3. Braunschweig, Friedr Vieweg &Sohn, 1905, p 296.)
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
2/14
Summary of the Gross Anatomy of the Extraocular Muscles 39
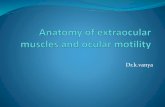
FIGURE 3 2. Posterior aspect of orbit showing topographic relationship of muscle origins in theannulus of Zinn. N, cranial nerve.
the rectus muscles). Here again, Tenon s capsule,fastened to the orbital rim and the retrobulbartissue, must provide the necessary balance. 39
Rectus Muscles
The rectus muscles are more or less at narrowbands that attach themselves with broad, thin ten-dons to the globe. There are four of these muscles:the medial (internal), the lateral (external), thesuperior , and the inferior .
The extraocular muscles have delightful syn-onyms in the old anatomical texts, some of whichwe cannot refrain from quoting: medial rectus(bibitorius, the drinking, because the eyes arecrossed while looking at the bottom of the cup);lateral rectus (indignatorius, the angry); superior
rectus (superbus, the proud; pius, the pious, be-cause the upward turning of the eyes expressesdevotion); inferior rectus (humilis, the humble).The superior oblique is also known as patheticus(the pathetic). 26 Powell 31 called the oblique mus-cles amatorii, quod sint velut in amore duces et furtivum oculorum jactus promoveant (for they areas leaders in love and promote furtive glances of the eyes).
The origins of the rectus muscles, the superioroblique muscle, and the levator muscle of the
upper lid are at the tip of the orbital pyramid.There the origins of the muscles are arranged in amore or less circular fashion (the annulus of Zinn ),surrounding the optic canal and in part the supe-
rior orbital ssure (Fig. 32). Through this ovalopening created by the origins of the muscles, theoptic nerve, the ophthalmic artery, and parts of cranial nerves III and VI enter the muscle coneformed by the body of the rectus muscles.
The interlocking of muscle and tendon bersat the site of origin creates an extremely strong
anchoring of the extraocular muscles. Avulsion of a muscle at the origin is rare even in cases wheretraction or trauma is sufciently severe to causeavulsion of the optic nerve. 33 Attachments existbetween the origins of the medial and superiorrecti and the dura of the optic nerve. This explainsthe pain occurring on eye movements in patientswith optic neuritis. 33
The medial and lateral rectus muscles followthe corresponding walls of the orbit for a goodpart of their course, and the inferior rectus muscle
remains in contact with the orbital oor for onlyabout half its length. The superior rectus muscleis separated from the roof of the orbit by thelevator muscle of the upper lid.
If the rectus muscles were to continue theircourse in their original direction, they would nottouch the globe; but about 10 mm posterior to theequator, the muscle paths curve toward the globerather abruptly and eventually insert on the scleraat varying distances from the corneal limbus. Thereason for this change in course is musculo-orbital
tissue connections (the muscle pulleys; see be-low). Charpy, 5 quoting Motais, 28 describes howrecurrent bers may detach themselves from thebulbar side of the rectus muscles near their inser-
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
3/14
40 Physiology of the Sensorimotor Cooperation of the Eyes
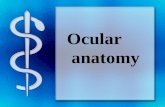
FIGURE 3 3. Insertions of rectus
muscles. Average measurements arein millimeters. (Data from Apt L: Ananatomical evaluation of rectus mus-cle insertions. Trans Am OphthalmolSoc 78:365, 1980.)
tion, attaching themselves to the sclera 1 to 5mm behind the insertions. Scobee 32 called theseattachments footplates and attributed considerableimportance to them in the etiology of esotropia(see Chapter 9).
Because the insertions of the rectus musclesare not equidistant from the corneal limbus, theydo not lie on a circle that is concentric with it butrather on a spiral (the spiral of Tillaux ). The inser-tion of the medial rectus muscle is closest to thecorneal limbus, followed by the inferior, lateral,and superior rectus insertions, with the superiorrectus insertion being the most distant (Fig. 3 3).
The lines of insertion are generally not straight,but are more or less curved and sometimes evenwavy. The straightest ones are the insertions of
the medial and lateral rectus muscles, but thesetoo are often slightly convex toward the corneallimbus. Fuchs 15 found in 50 cadaver eyes thatin half the cases the horizontal meridian cut theinsertions symmetrically. For the rest of the cases,up to two thirds of the width of the tendon of themedial rectus muscle was above the horizontalmeridian and that of the lateral rectus muscle wasbelow it. Fuchs found also that the insertion line of these muscles was perpendicular to the horizontalmeridian in less than half the eyes. In the others
the insertion lines ran obliquely up and in, in thecase of the medial rectus, and up and out, in thecase of the lateral rectus.
The lines of insertion of the superior and infe-
rior rectus muscles are markedly convex towardthe corneal limbus and run obliquely upward andlaterally. The rounded, temporal ends of their in-sertions therefore are more distant from the cor-neal limbus than their nasal ends. The amount of
obliquity varies in different eyes but is usuallymarked and, according to Fuchs, 15 is usually of the same degree for the two muscles of the sameeye. The lines of insertion are cut asymmetricallyby the vertical meridian. The greater part of thetendon (two thirds of its width according to Fuchs)of the superior rectus lies temporal to the merid-ian. In one third of the eyes, Fuchs found thatthe meridian bisected the inferior rectus tendon;otherwise, the larger segment of the insertion linewas found to lie lateral to it.
The normal distance between muscle insertionand limbus is of importance during operationsand reoperations on the extraocular muscles. Databased on measurements taken by Apt 1 from ca-daver eyes of adult subjects (mean age, 60.3 years)are shown in Figure 3 3 and Table 3 1. Theanterior limbus was de ned by Apt as the transi-tion from clear cornea to gray and the posterior limbus as the transition from gray cornea to whitesclera. While the means are similar to those of another recent study, 23 the range of variations be-
tween data reported elsewhere in the literature isremarkable. 15, 16, 22, 24, 35 The experienced surgeon isaware how often differences of several millimetersfrom the norms shown in Figure 3 3 can be found.
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
4/14
Summary of the Gross Anatomy of the Extraocular Muscles 41
TABLE 3 1. Distance from Limbus to Rectus Muscle Insertions
Mean SD (mm) Range (mm)
Medial rectus insertionAnterior limbus to midpoint of insertion 5.3 0.7 3.6 7.0Posterior limbus to midpoint of insertion 4.7 0.6 3.0 6.4
Inferior rectus insertionAnterior limbus to midpoint of insertion 6.8 0.8 4.8 8.5Posterior limbus to midpoint of insertion 5.9 0.8 3.9 7.6
Lateral rectus insertionAnterior limbus to midpoint of insertion 6.9 0.7 5.4 8.5Posterior limbus to midpoint of insertion 6.3 0.6 4.8 7.9
Superior rectus insertionAnterior limbus to midpoint of insertion 7.9 0.6 6.2 9.2Posterior limbus to midpoint of insertion 6.7 0.6 5.0 8.0
From Apt L: An anatomical evaluation of rectus muscle insertions. Trans Am Ophthalmol Soc 78:365, 1980.
Since a topographic correlation exists between
the location of the tendon insertion and the oraserrata and since the distance of the ora from thelimbus depends on the anteroposterior diameter of the globe, 36, 37 the distance of the tendon from thelimbus may be in uenced by age and axial refrac-tive errors of the eye. 15 If these variations in thelocation of the insertion are not taken into account(see Table 3 1), the value of geometric calcula-tions in predicting the results of surgery on theaction of the extraocular muscles is limited. Forinstance, the effect of a 4-mm muscle recessionwill vary signi cantly with the distance of theanatomical insertion from the limbus. These con-siderations apply especially when considering theeffect of muscle surgery in infants. Table 3 2shows a substantial difference in mean anatomicaldata obtained from adult and newborn eyes. Ac-cording to Souza-Dias and coworkers, 35 age differ-
TABLE 3 2. Comparative Measurements ofMedial and Lateral Rectus Muscles in Adults*
and Newborns Medial LateralRectus RectusMuscle Muscle
Length 37.7 (28) 36.3 (31.6)Width 10.4 (7.9) 9.6 (6.9)Distance from limbus 5.7 (3.9) 7.5 (4.8)
(middle of insertion)
*Data from Lang J, Horn T, Eichen U von den: U ber die ausserenAugenmuskeln und ihre Ansatzzonen. Gegenbaurs MorpholJahrb 126:817, 1980.
Data Weiss L: U ber das Wachstum des menschlichen Auges
und u ber die Vera nderungen der Muskelinsertionen am wach-senden Auge. Anat Hefte 25 (pt 1):191, 1897; Schneller F:Anatomisch-physiologische Untersuchungen u ber die Augen-muskeln Neugeborener. Graefes Arch Clin Exp Ophthalmol47:178, 1899.
Measurements from newborn in parentheses.
ences in the distance between limbus and insertion
can be neglected in strabismus operations in chil-dren older than 6 months. In view of the fact thatthe longitudinal growth of the eye is not com-pleted by that age, we take a more conservativeview and would put the age at which adult dosagesof strabismus surgery may be applied at 2 yearsand older.
The length of the rectus muscles exclusive of tendon is fairly constant, but there are variationsbetween the width of the insertion and the lengthof tendon of the different muscles (Table 3 3).Other anatomical data of importance to the kine-matics of the eye are discussed in Chapter 4.
Muscle Pulleys
Modern imaging techniques such as computed to-mography (CT) scanning 34 and magnetic reso-nance imaging (MRI) 6, 10, 27 have revealed that thepaths of the rectus muscles remain xed relativeto the orbital wall during excursions of the globe
and even after large surgical transpositions.7, 8
Only the anterior aspect of the muscle moves withthe globe relative to the orbit, as it must on ac-count of its scleral attachment. In other words,there is no sideslip of the rectus muscles in rela-tion to the orbital walls when the eye moves fromprimary into secondary gaze positions (Fig. 3 4).Demer and coworkers 10 suspected from thesendings that there must be musculo-orbital cou-pling through tissue connections that constrain themuscle paths during rotations of the globe. Subse-
quent studies with high-resolution MRI con rmedthis notion by demonstrating retroequatorial in-ections of the rectus muscle paths 6, 10 (Fig. 3 5).Gross dissection of orbits and histologic and histo-
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
5/14
42 Physiology of the Sensorimotor Cooperation of the Eyes
TABLE 3 3. Means and Range (in parentheses) of Measurements of Rectus Muscles (mm)*
Medial SuperiorRectus Inferior Rectus Lateral Rectus RectusMuscle Muscle Muscle Muscle
Length 37.7 (32.0 44.5) 37.0 (33.0 42.5) 36.3 (27.0 42.0) 37.3 (31.0 45.0)
Length of tendon 3.0 (1.0 7.0) 4.7 (3.0 7.0) 7.2 (4.0 11.0) 4.3 (2.0 6.0)Width of tendon 10.4 (8.0 13.0) 8.6 (7.0 12.0) 9.6 (8.0 13.0) 10.4 (7.0 12.0)
From Lang J, Horn T, Eichen U von den: U ber die ausseren Augenmuskeln und ihre Ansatzzonen. Gegenbaurs Morphol Jahrb126:817, 1980.
*Data from right eye.Exclusive of tendon.
chemical studies 10, 30 showed that these in ectionsare caused by musculo-orbital tissue connectionsin the form of broelastic sleeves that consistof smooth muscle, collagen, and elastin. During
contraction the muscles travel through thesesleeves which act as pulleys by restraining themuscle paths. The orbital layer of the rectus mus-cle inserts directly on the pulley, whereas theglobal layer continues anteriorly to insert intothe sclera.
These pulleys are located in a coronal planeanterior to the muscle bellies and about 5 to 6 mmposterior to the equator. They are compliant ratherthan rigid, receive rich innervation involving nu-merous neurotransmitters in humans and mon-keys, 9, 11 and change their positions as a functionof gaze direction. For instance, the pulleys of thehorizontal rectus muscle move posteriorly duringmuscle contraction. 8 This adjustability of pulleypositions and the different insertion sites of theglobal and orbital layers of extraocular musclesmay play a major but still unde ned role in ocularkinematics. 8, 9, 30
The demonstration of muscle pulleys is incom-
FIGURE 3 4. Two-mm-thick,320- m resolution axial MRI scanof a normal left orbit showing theinection of the horizontal rectusmuscles as they pass throughtheir respective pulleys during ab-duction and adduction. MR, me-dial rectus; LR; lateral rectus.(From Demer JL: Orbital connec-tive tissue in binocular alignmentand strabismus. In LennerstrandG, Ygge J, eds: Advances in Stra-
bismus, Proceedings of Interna-tional Symposium at the Wenner-Gren Center, Stockholm, June1999. London, Portland Press,2000, p 17.)
patible with the classic view according to whichthe direction of pull of a rectus muscle is deter-mined by its functional insertion at the point of tangency with the globe and its origin at the
annulus of Zinn. 10 Actually, the functional originof a rectus muscle is located at its pulley. Itfollows that atypical location of a pulley (seeChapter 19) or pathologic conditions that mayinuence pulley function may cause certain formsof strabismus. Moreover, the nding of stabilityof the muscle paths during excursions of the globethrough muscle pulleys may change our conceptsabout the function of the rectus muscles in tertiarygaze. Further reference to the muscle pulleys ismade in the appropriate sections of this book.
Oblique Muscles
From its origin above and medial to the opticforamen, the superior oblique muscle courses an-teriorly in a line parallel with the upper part of the medial wall of the orbit, reaching the trochleaat the angle between the superior and medial wall.
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
6/14
Summary of the Gross Anatomy of the Extraocular Muscles 43
FIGURE 3 5. Two-mm-thick, 320- m resolution axial MRI scan of normal left orbit in primary andsecondary gaze positions, showing near constancy of the positions of the rectus muscles posteriorto the pulleys. IR, inferior rectus; SR, superior rectus; MR, medial rectus; LR, lateral rectus; ON,optic nerve. Note stability of the coronal sections of the rectus muscles but movement of the sectionof the optic nerve in secondary gaze postions. (Courtesy of Dr. J.L. Demer, Los Angeles.)
The trochlea is a tube 4 to 6 mm long formed inits medial aspect by bone (the trochlear fossa of the frontal bone). The rest of the circumference iscomposed of connective tissue that may containcartilaginous or bony elements. After passing thetrochlea, the superior oblique muscle turns in lat-erodorsally, forming an angle of about 54 withthe pretrochlear or direct portion of the muscle.
A brillar, vascular sheath surrounds the intra-trochlear superior oblique tendon. This portion of the tendon consists of discrete bers with few
inter brillar connections, as reported by Helvestonand coworkers. 21 Each ber of the tendon movesthrough the trochlea in a sliding, telescoping fash-ion with the central bers undergoing maximal
and the peripheral bers the least excursion. Thetotal travel of the central bers appears to be 8mm in either direction. 20
Helveston and coworkers 21 also described abursa-like structure lying between the trochlearsaddle and the vascular sheath of the superioroblique tendon and postulated that pathologic al-terations of the bursa may be a factor in theetiology of Brown syndrome (see Chapter 21).
At about the distal third of the direct portion(10 mm behind the trochlea), the muscle becomes
tendinous and remains tendinous in its entire post-trochlear or reected part. The tendon passes un-der the superior rectus muscle, fans out, andmerges laterally with the sclera to the vertical
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
7/14
44 Physiology of the Sensorimotor Cooperation of the Eyes
FIGURE 3 6. Relationships of tendons of superioroblique muscle. Measurements are in millimeters. (Modi-ed from Fink WH: Surgery of the Vertical Muscles of
the Eyes, ed 2. Spring eld, IL, Charles C Thomas, 1962.)
meridian, forming a concave curved line towardthe trochlea (Fig. 3 6). The anterior end of theinsertion lies 3.0 to 4.5 mm behind the lateral endof the insertion of the superior rectus muscle and13.8 mm behind the corneal limbus. The posteriorend of the insertion lies 13.6 mm behind themedial end of the insertion of the superior rectusmuscle and 18.8 mm behind the corneal limbus.
The width of the insertion of the superior obliquemuscle varies greatly (from 7 to 18 mm, Fink 14 )but is 11 mm on average. The medial end of theinsertion lies about 8 mm from the posterior poleof the globe. Near its insertion the posterior borderof the muscle is related to the superior vortex vein.
The length of the direct part of the superioroblique muscle is about 40 mm and that of thereected tendon is about 19.5 mm. From a physio-logic and kinematic standpoint, the trochlea is theorigin of the muscle.
The inferior oblique muscle is the shortest of all the eye muscles, being only 37 mm long. Itarises in the anteroinferior angle of the bony orbitin a shallow depression in the orbital plate of themaxilla near the lateral edge of the entrance intothe nasolacrimal canal. The origin is readily lo-cated by drawing a perpendicular line from thesupraorbital notch to the lower orbital margin.
The muscle continues from its origin backward,upward, and laterally, passing between the oorof the orbit and the inferior rectus muscle. It
inserts by a short tendon (1 to 2 mm) in theposterior and external aspect of the sclera. Thewidth of the insertion varies widely (5 to 14 mm,Fink 14 ) and may be around 9 mm on average. The
insertion forms a curved concave line toward theorigin of the muscle. Its anterior margin is about10 mm behind the lower edge of the insertion of the lateral rectus muscle; its posterior end is 1 mmbelow and 1 to 2 mm in front of the macula (Fig.37). Near its insertion the posterior border of themuscle is related to the inferior vortex vein.
Unlike the other extraocular muscles, espe-cially the superior obliques, which have both mus-cular and tendinous components, the inferioroblique is almost wholly muscular. It forms anangle of about 51 with the vertical plane of theglobe.
Fascial System
Tenons Capsule
The eyeball is suspended within the orbit by asystem of fasciae. The way in which this isachieved represents an ideal solution to the prob-lem of suspending a spheroid body in a cone-shaped cavity. The bulk of the system is made upof Tenon s capsule, which is a condensation of brous tissue that covers the eyeball from theentrance of the optic nerve to near the corneallimbus, where it is rmly fused with the conjunc-tiva. Except for this area of fusion, the two struc-tures are separated by the subconjunctival space .Tenon s capsule is also separated from the sclera.Between the two is the episcleral space (Tenonsspace) , which can be readily injected (Fig. 3 8).On its outer aspect the capsule is intimately relatedto the orbital reticular tissue. Its posterior edge is
FIGURE 3 7. Course of inferior oblique muscle and therelationships of its tendon. Measurements are in millime-ters. (Modi ed from Fink WH: Surgery of the VerticalMuscles of the Eyes, ed 2. Spring eld, IL, Charles CThomas, 1962.)
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
8/14
Summary of the Gross Anatomy of the Extraocular Muscles 45
FIGURE 3 8. Tenon s space shown by injection with In-dia ink. (Modi ed from Charpy A: Muscles et capsulede Tenon. In Poirier P, Charpy A, eds: Traite danatomiehumaine, new ed, vol 5/2. Paris, Masson, 1912, p 539.)
not clearly delineated; it is thin and more or lesscontinuous with the meshwork of the orbital fat.
If the globe is enucleated, one can see theanterior orice of Tenon s capsule, the borders of which were attached to the sclera before enucle-ation; the posterior orice , which is fused withthe sheaths of the optic nerve; and the smoothinner surface with the slits of entry for the extraoc-ular muscles. The openings for the vortex veinsare small and not readily visualized (Fig. 3 9).
Muscle Sheaths and Their Extensions The extrinsic ocular muscles pierce Tenon s cap-sule, enter the subcapsular space, and insert into
FIGURE 3 9. Anterior and posteriorori ce of Tenon s capsule shownafter enucleation of the globe. (Modi-
ed from Charpy A: Muscles et cap-sule de Tenon. In Poirier P, Charpy A,eds: Traite danatomie humaine, newed, vol 5/2. Paris, Masson, 1912, p539.)
the sclera. Therefore, one can distinguish an extra-capsular and an intracapsular portion of eachmuscle.
In their extracapsular portions, the extrinsic eyemuscles are enveloped by a muscle sheath . Thissheath is a re ection of Tenon s capsule and runsbackward from the entrance of the muscles intothe subcapsular space for a distance of 10 to 12mm. At the lower aspect of the entrance, Tenon scapsule is reduplicated. At the upper aspect, itcontinues forward as a single membrane (Fig.310). The muscle sheaths of the four rectus mus-cles are connected by a formation known as theintermuscular membrane , which closely relatesthese muscles to each other (Fig. 3 11). In addi-tion, there are numerous extensions from all the
sheaths of the extraocular muscles, which form anintricate system of brous attachments intercon-necting the muscles, attaching them to the orbit,supporting the globe, and checking the ocularmovements. These will now be described in theiressential features.
The fascial sheath of the superior rectus muscleclosely adheres in its anterior external surface tothe undersurface of the sheath of the levator mus-cle of the upper lid. In front of the equator thesheath of the superior rectus muscle also sends a
separate extension obliquely forward that widensand ends on the lower surface of the levator mus-cle. The fusion of the two muscles accounts forthe cooperation of upper lid and globe in elevationof the eye, a fact that must be kept in mind whensurgical procedures on the superior rectus muscleare being considered.
The fascial sheath of the inferior rectus muscledivides anteriorly into two layers: an upper one,which becomes part of Tenon s capsule, and a
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
9/14
46 Physiology of the Sensorimotor Cooperation of the Eyes
FIGURE 3 10. Check ligaments of medial
and lateral rectus muscles. Reduplication ofTenon s capsule, forming the muscle sheathof the rectus muscles.
lower one, which is about 12 mm long and endsin the brous tissue between the tarsus of thelower lid and the orbicularis muscle (Figs. 3 11and 3 12). This lower portion forms part of Lock-wood s ligament.
The fascial sheath of the re ected tendon of
the superior oblique muscle consists of two layersof strong connective tissue (Fig. 3 13). The twolayers are 2 to 3 mm thick, so the tendon and itssheath have a diameter of about 5 to 6 mm. Thepotential space between the sheath and the tendonis continuous with the episcleral space. Materialinjected into Tenon s space therefore may pene-trate into the space between tendon and sheath. 2
Many attachments extend from the sheath of the
FIGURE 3 11. Intermuscular membranes and fas-cial extensions of the superior, lateral, and inferiorrectus muscles (right eye).
superior oblique muscle to other areas: to thesheath of the levator muscle, to the sheath of thesuperior rectus muscle, to the conjoined sheath of these two muscles, and to Tenon s capsule, behind,above, and laterally. The numerous ne brils thatconnect the inner surface of the sheath to the
tendon are an important feature (see Fig. 3 13).Some authors 19, 29 have rejected the idea of thesuperior oblique tendon having a separate sheathand favor the view that what appears to be sheathare actually re ections of anterior and posteriorTenon s capsule. This concept is of interest inconnection with the etiology of Brown syndrome.
The fascial sheath of the inferior oblique mus-cle covers the entire muscle. It is rather thin at the
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
10/14
Summary of the Gross Anatomy of the Extraocular Muscles 47
FIGURE 3 12. Fascial sheath of the inferior rectus mus-cle and Lockwood s ligament.
origin but thickens as the muscle continues later-ally and develops into a rather dense membranewhere it passes under the inferior rectus muscle.At this point, the sheath of the inferior obliquemuscle fuses with the sheath of the inferior rectusmuscle (see Fig. 3 12). This fusion may be quiterm and complete or so loose that the two musclesmay be relatively independent of each other. Nearthe insertion of the muscle the sheath of the infe-rior oblique muscle also sends extensions to thesheath of the lateral rectus muscle and to thesheath of the optic nerve.
FIGURE 3 13. Fascial sheath of the re ected tendon ofthe superior oblique muscle. (Modi ed from Berke RN:Tenotomy of the superior oblique for hypertropia [prelimi-nary report]. Trans Am Ophthalmol Soc 44:304, 1946.)
Ligament of Lockwood
The blending of the sheaths of the inferior obliqueand inferior rectus muscles and the extensions thatgo from there upward on each side to the sheathsof the medial and lateral rectus muscles form a
suspending hammock, which supports the eyeball.This part of the fascial system has been termedthe suspensory ligament of Lockwood . Extensionsof brous bands to the tarsal plate of the lowerlid, the orbital septum, and the periosteum of theoor of the orbit also form part of Lockwood sligament (see Fig. 3 12).
Check Ligaments
The medial and lateral rectus muscles possess
well-developed brous membranes that extendfrom the outer aspect of the muscles to the corres-ponding orbital wall.
The check ligament of the lateral rectus muscleappears in horizontal sections as a triangle, theapex of which is at the point where the sheath of the muscle pierces Tenon s capsule. From there itgoes forward and slightly laterally, fanning out toattach to the zygomatic tubercle, the posterioraspect of the lateral palpebral ligament, and thelateral conjunctival fornix (see Fig. 3 10).
The check ligament of the medial rectus muscleextends from the sheath of the muscle, attachingto the lacrimal bone behind the posterior lacrimalcrest and to the orbital septum behind. It is trian-gular and unites at its superior border with astrong extension from the sheath of the levatormuscle and a weaker extension from the sheath of the superior rectus muscle. The inferior border isfused to extensions from the inferior oblique andinferior rectus muscle sheaths.
The other extraocular muscles do not haveclearly distinct check ligaments such as those of the medial and lateral rectus muscles. However,the various extensions of the muscle sheaths tothe sheaths of other muscles, the orbital wall, andTenon s capsule undoubtedly ful ll the task of checking the action of these muscles. Actually, ithas been said (with considerable truth) by Duke-Elder, 12, p. 451 who quotes Dwight, 13 that the com-plexities of Tenon s capsule are limited only bythe perverted ingenuity of those who describe it.
Intracapsular Portion of the Muscle
The muscles move freely through the openings inTenon s capsule. In the intracapsular portion,
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
11/14
48 Physiology of the Sensorimotor Cooperation of the Eyes
FIGURE 3 14.The falciform folds of Gue rin, one on eachside of the rectus muscles. (Modi ed from Gue rin G:
Me moire sur la myotomie oculaire par la me thode sous-conjonctivale. Gazette Med Paris, 1842.)
which for the rectus muscles is 7 to 10 mm inlength, they have no sheath but are covered byepiscleral tissue fused with the perimysium. Thistissue expands laterally, going along the muscleon each side, from the entry of the muscle intothe subcapsular space to the insertion. Posteriorly,
this tissue attaches to the capsule and laterally tothe sclera. At the tendon this tissue becomes ratherdense and appears to serve to xate the tendon,forming the falciform folds of Gue rin 17 or admini-cula of Merkel 25, 26 (Fig. 3 14). Merkel and Kal-lius remarked that these structures make it dif cultto determine accurately the width of the insertions.
Functional Role of the Fascial System
Aside from its role in connecting the globe withthe orbit and of supporting and protecting it, themain task of Tenon s capsule is to serve as a cavitywithin which the eyeball may move. Helmholtz 18
compared the movements of the eyeball in Tenon scapsule to the movements of the head of the femurin the cotyloid fossa. However, Tenon s capsuledoes not have the anatomical characteristics of synovial tissue, nor is it a serous membrane.
The complicated system of fasciae and liga-ments is of considerable importance in the control
of the eye movements. It prevents or reduces re-tractions of the globe, as well as movements inthe direction of action of the muscle pull. Thus,the position of the center of rotation of the eyeball
remains fairly constant in relation to the orbitalpyramid (see Chapter 4). Also, owing particularlyto the action of the check ligaments, the eye move-ments become smooth and dampened. As the mus-cles contract, their action is graduated by the elas-ticity of their check systems, which limits theaction of the contracting muscle and reduces theeffect of relaxation of the opposing muscles (seeSherrington s law, Chapter 4, p. 63). This ensuressmooth rotations and lessens the shaking up of thecontents of the globe when the eyes suddenly stopor change the direction of their movement.
Developmental Anomalies ofExtraocular Muscles and theFascial System
Gross developmental anomalies of the extraocularmuscles are infrequent. The cases recorded in theliterature are grouped together and reported withgreat completeness by Duke-Elder 12, p. 979 Many of these reports are fascinating, but it would serveno useful purpose to discuss them in this book.Unless the anomaly is extreme, such as the totalabsence of a muscle, it is not likely to have a
major effect on the coordination of the eye move-ments or on the relative position of the eyes, sinceeven the experimental transposition of various ex-traocular muscles does not permanently destroythis coordination.
Patients with congenital absence of a musclepresent with the clinical picture of complete paral-ysis (see Chapter 20). There may be no preopera-tive clues to alert the surgeon that the apparentlyparalyzed muscle is absent. Consequently, the sur-geon must be prepared to use alternative surgical
approaches if a muscle cannot be located at thetime of the operation.
Anomalies of the fascial system are more com-mon than those of the muscles, and it is probablethat they have functionally, and therefore clini-cally, a more profound effect on the ocular motil-ity. These anomalies act as a check to activeand passive movements of the globe in certaindirections, although the muscles that should pro-duce the active movement may be quite normalanatomically and functionally. To this group be-
long a number of clinical entities, such as thevarious forms of strabismus xus and the superioroblique tendon sheath syndrome of Brown, 4 whichare discussed in Chapter 21.
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
12/14
Summary of the Gross Anatomy of the Extraocular Muscles 49
Innervation of ExtraocularMuscles
The medial, superior, and inferior rectus musclesand the inferior oblique muscle are all innervated
by cranial nerve III, the oculomotor nerve. Thebranches enter their respective muscles from thebulbar side. The branches intended for the medialrectus muscle enter its belly 15 mm from theorigin of the muscle; those for the inferior rectusmuscle enter at the junction of the posterior andmiddle third of the belly; and those for the inferioroblique muscle enter just after the muscle passeslateral to the inferior rectus muscle. All thesebranches are innervated by the inferior division of cranial nerve III.
The branches for the superior rectus muscleoriginate from the upper division of the oculomo-tor nerve and enter the muscle at the junction of the posterior and middle thirds (Fig. 3 15). Thelateral rectus muscle is innervated by cranial nerveVI, the abducens nerve, which enters the muscle15 mm from its origin on the bulbar side (seeFig. 3 15).
The superior oblique muscle differs from theother ve extraocular muscles in that cranial nerveIV, the trochlear nerve, which innervates it, enters
FIGURE 3 15. Innervation of the extraocular muscles. N, cranial nerve.
the muscle from the outer (orbital) surface nearthe lateral border after crossing over from themedial side. The nerve divides into three or fourbranches. The most anterior branch enters thebelly at the juncture of the posterior and middlethird of the muscle and the most posterior at about8 mm from its origin (see Fig. 3 15).
Sensory organs have been described in the ex-traocular muscles. They presumably provide amore or less de ned stretch effect. Although theinnervation of these organs has not been followedin humans, it is likely to take the route of theophthalmic division of the trigeminal nerve.
Blood Supply of Extraocular
Muscles
All extraocular muscles are supplied by the lateraland medial muscular branches of the ophthalmicartery. The lateral branch supplies the lateral andsuperior rectus muscles, the levator muscle of theupper lid, and the superior oblique muscle. Themedial branch, the larger of the two, supplies theinferior and medial rectus muscles and the inferioroblique muscle. The inferior rectus muscle andthe inferior oblique muscle also receive a branch
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
13/14
50 Physiology of the Sensorimotor Cooperation of the Eyes
FIGURE 3 16. The anterior ciliary arteries. (From LastRJ: Wolff s Anatomy of the Eye and Orbit, ed 6. Philadel-phia, HK Lewis, 1968.)
from the infraorbital artery, and the medial rectusmuscle receives a branch from the lacrimal artery.
The arteries to the four rectus muscles give riseto the anterior ciliary arteries. Two arteries emergefrom each tendon, except for the lateral rectusmuscle, which has only one. There are exceptionsto this rule, however, as any muscle surgeon canreadily con rm. Variations in the number of ante-rior ciliary arteries supplied by each muscle be-come clinically relevant with regard to the anteriorsegment blood supply when disinserting more thantwo rectus muscle tendons during muscle surgery(see Chapter 26).
The anterior ciliary arteries pass to the epi-sclera, give branches to the sclera, limbus, andconjunctiva, and pierce the sclera not far from thecorneoscleral limbus (Fig. 3 16). These perforat-ing branches cross the suprachoroidal space toterminate in the anterior part of the ciliary body.Here they anastomose with the lateral and mediallong ciliary arteries to form the major arterialcircle of the iris.
The veins from the extraocular muscles corre-spond to the arteries and empty into the superiorand inferior orbital veins, respectively.
REFERENCES
1. Apt L: An anatomical evaluation of rectus muscle inser-tions. Trans Am Ophthalmol Soc 78:365, 1980.
2. Berke RN: Tenotomy of the superior oblique for hyper-tropia (preliminary report). Trans Am Ophthalmol Soc44:304, 1946.
3. Bron AJ, Tripathi RC: Wolffe s Anatomy of the Eye and
Orbit, ed 8. London, Chapman & Hall, 1997.4. Brown HW: Congenital structural muscle anomalies. In
Allen, JH, ed: Strabismus Ophthalmic Symposium I. StLouis, Mosby Year Book, 1950, p 205.
5. Charpy A: Muscles et capsule de Tenon. In Poirier P,
Charpy A, eds: Traite danatomie humaine, new ed vol5/2. Paris, Masson, 1912, p 539.
6. Clark RA, Miller JM, Demer JL.: Location and stabilityof rectus muscle pulleys. Muscle paths as function of gaze.Invest Ophthalmol Vis Sci 38:227, 1997.
7. Clark RA, Rosenbaum AL, Demer JL: Magnetic resonanceimaging after surgical transposition de nes the anteropost-erior location of the rectus muscle pulleys. J AAPOS3:9, 1999.
8. Demer JL, Miller JM, Poukens V: Surgical implications of the rectus extraocular muscle pulleys. Pediatr OphthalmolStrabismus 33:208, 1996.
9. Demer JL, Oh SY, Poukens V: Evidence for active controlof rectus extraocular muscle pulleys. Invest Ophthal VisSci 41:1280, 2000.
10. Demer JL, Miller JM, Poukens V, et al: Evidence forbromusclar pulleys of the recti extraocular muscles. In-vest Ophthalmol Vis Sci 36:1125, 1995.
11. Demer JL, Pukens V, Miller JM, Mircevych P: Innervationof extraocular pulley smooth muscle in monkeys and hu-mans. Invest Ophthalmol Vis Sci 38:1774, 1997.
12. Duke-Elder S, Wybar KC: The Anatomy of the VisualSystem. System of Ophthalmology, vol 2. St Louis,Mosby Year Book, 1961.
13. Dwight T: The anatomy of the orbit and the appendagesof the eye. In Norris WF, Oliver CA, eds: System of Diseases of the Eye, vol 1. Philadelphia, JB Lippincott,1897, p 99.
14. Fink WH: Surgery of the Vertical Muscles of the Eyes, ed2. Spring eld, IL, Charles C Thomas, 1962.
15. Fuchs E: Beitrage zur normalen Anatomie des Augapfels.Graefes Arch Ophthalmol 30(4):1, 1894.
16. Gat L: Einige Beitra ge zur Topographie des Ansatzes dervier geraden Augenmuskeln. Ophthalmologica 14:43,1947.
17. Gue rin G: Me moire sur la myotomie oculaire par la me th-
ode sous-conjonctivale. Gazette Med Paris, 1842.18. Helmholtz H von: In Southall PC, ed: Helmholtz s Treatiseon Physiological Optics. English translation from the 3rdGerman edition, Ithaca, NY, Optical Society of America,1924. Quoted from reprint, New York, Dover Publications,vol 3, 1962, p 38.
19. Helveston EM: Brown syndrome: Anatomic considerationsand pathophysiology. Am Orthoptics J 43:31, 1993.
20. Helveston EM: The in uence of superior oblique anatomyon function and treatment. Binocular Vision StrabismusQ:14:16, 1999.
21. Helveston EM, Merriam WW, Ellis FD, et al: The trochlea:A study of the anatomy and physiology. Ophthalmology89:124, 1982.
22. Howe L: Insertion of the ocular muscles. Trans Am Oph-thalmol Soc 9:668, 1902.
23. Lang J, Horn T, Eichen U von den: U ber die a usserenAugenmuskeln und ihre Ansatzzonen. Gegenbaurs Mor-phol Jahrb 126:817, 1980.
24. Last RJ: Wolff s Anatomy of the Eye and Orbit, ed 6.Philadelphia, HK Lewis & Co, 1968.
25. Merkel F: Makroscopische Anatomie. In Graefe A, Sae-misch Th, eds: Handbuch der gesammten Augenheilkunde,ed 1, vol 1. Leipzig, Wilhelm Engelmann, 1874, p 56.[See also Merkel and Kallius. 27, p 73 ]
26. Merkel F, Kallius E: Makroscopische Anatomie desAuges. In Graefe A, Saemisch Th, eds: Handbuch dergesammten Augenheilkunde, ed 2, vol 1. Leipzig, WilhelmEngelmann, 1910, p 65 n.
27. Miller JM: Functional anatomy of human rectus muscles.Vision Res 29:223, 1989.
28. Motais E: L appareil moteur de l oeuil de l homme etdes verte bre s. Deductions physiologiques et chirurgicales(strabisme). Paris, A. Delahaye & E. Lecrosnier, 1887.
-
8/6/2019 87_Ch 3 - Summary of the Gross Anatomy of the Extra Ocular Muscles, p. 38-51
14/14
Summary of the Gross Anatomy of the Extraocular Muscles 51
29. Parks MM: The superior oblique tendon 33rd DoyneMemorial Lecture. Trans Ophthalmol Soc UK 97:288,1977.
30. Porter JD, Pukens V, Baker RS, et al: Structure functioncorrelations in the human medial rectus extraocular musclepulleys. Invest Ophthalmol Vis Sci 37:468, 1996.
31. Powell T: Elementa opticae. London, F. Griswold, 1651 p18. [About this exceedingly rare book and its author, seeBurian HM: A text for the times of Cromwell. DartmouthColl Libr Bull 4:19, 1943.]
32. Scobee RC: Anatomic factors in the etiology of strabis-mus. Am J Ophthalmol 31:781, 1948.
33. Sevel P: The origins and insertions of the extraocularmuscles: Development, histologic features, and clinicalsigni cance. Trans Am Ophthalmol Soc 84:488, 1986.
34. Simonsz HJ, Harting F, de Waal BJ, et al: Sidewaysdisplacement and curved path of recti eye muscles. ArchOphthalmol 103:124, 1985.
35. Souza-Dias C, Prieto-Diaz J, Uesugui CF: Topographicalaspects of the insertions of the extraocular muscles. JPediatr Ophthalmol Strabismus 23:183, 1986.
36. Stangl R, Muhlendyck H, Kraus-Mackiw E: Muskelansatz-Limbusdistanz und Sehnenla nge der Musculi recti in Ab-hangigheit von der Bulbusgro sse bzw. vom Altern. InKommerell G, ed: Augenbewegungssto rungen: Neuro-physiologie und Klinik. JF Bergmann, Munich, 1978, p 33.
37. Thiel HL: Zur topographischen und histologischen Situa-tion der Ora serrata. Graefes Arch Clin Exp Ophthalmol156:590, 1955.
38. Whitnall SE: The Anatomy of the Human Orbit and Ac-cessory Organs of Vision, ed 2. New York, HumphreyMilford, 1932.
39. Zoth O: Augenbewegungen und Gesichtswahrnehmungen.In Nagel W, ed: Handbuch der Physiologie des Menschen,vol 3. Braunschweig, Friedrich Vieweg & Sohn, 1905,p 296.