82085243 case-study-on-pregnancy-induced-hypertension-eclampsia
53
Homework Help https://www.homeworkping.com/ Research Paper help https://www.homeworkping.com/ Online Tutoring https://www.homeworkping.com/ click here for freelancing tutoring sites Our Lady of Fatima University College of Nursing Regalado, Quezon City A Case Study on Pregnancy-Induced Hypertension
-
Upload
homeworkping3 -
Category
Education
-
view
2.486 -
download
4
Transcript of 82085243 case-study-on-pregnancy-induced-hypertension-eclampsia

Homework Help
https://www.homeworkping.com/
Research Paper help
https://www.homeworkping.com/
Online Tutoring
https://www.homeworkping.com/
click here for freelancing tutoring sites
Our Lady of Fatima University
College of NursingRegalado, Quezon City
A Case Study onPregnancy-Induced Hypertension
In Partial Fulfillment of the Requirements in
Nursing Care ManagementRelated Learning Experience

Presented by:BSN 2A1-2Group 10
Espellogo, Leizel Y.Falle, Mery Ann M.Gianchand, Olivia E.
Hinanay, Ely JohnMaglaoy, Manuel David B.
Manuel, Janine M.Mateo, Donna Marie
First SemesterS.Y 2011-2012
I. Introduction
Hypertensive disorders of pregnancy also known as Pregnancy Induced Hypertension are
high blood pressure disorders of pregnancy which is one of the major problem for mother in
pregnancy.PIH is common in pregnant teens and in women over age 40 but it also develops
during the second half of the pregnancy and usually after the 20th week of gestation.PIH is
usually present to those person with a previous history of PIH, chronic hypertension, lupus,
alcohol, drug or tobacco abuse, presence of diabetes, underweight or overweight, kidney disease
and expected twins or triplets. The warning signs of PIH those people are rapid weight gain, 4-5
lbs in a single week, a rise in blood pressure, protein in urine, severe headaches, blurry visions,
severe pain over the stomach under the ribs of the mother who have PIH and decrease in amount
of urine. PIH can prevent prematurity and death of the baby through the following closely by the
medical professional and attending pre-natal checkup. PIH can cause low birth weight of the
baby.

Therefore, it is necessary to all health worker engaged on themselves all about clinical
knowledge and skills and to develop their values to be able to become an efficient and effective
competent individual when it comes health assessment in performing their duties and
responsibilities when it comes to health assessments.
II. Objectives
General:
This study aims to improve our skills, knowledge and attitude in performing our duties
and responsibilities to give an efficient and effective outcome especially to the health of the
patients.
Specific:
1. To identify factors if having pregnancy induced hypertension.

2. To develop a teaching program that will educate patients specially those who are susceptible
of pregnancy induced hypertension.
3. To understand the disease process, its etiology, signs and symptoms, pathophysiology and
diagnostic procedure.
4. To promote awareness to individual by imparting knowledge so they could learn and
understand more about pregnancy induced hypertension.
5. To discuss and describe interventions for health promotion, prevention and treatment of
patient pregnancy induced hypertension.
III. Patient’s Profile
A. Biographical Data
1. Name: Mrs. R.E.R.
2. Address: Sto. Nino 1 Sapang Palay, SJDM
3. Age: 30
4. Birthdate: June 19,1981
5. Sex: Female
6. Race: Filipino
7. Marital status: Married
8. Occupation: Housewife
9. Religion: Catholic
10. Health Care financing and usual source of Medical Care:
Supported by the patient’s parents since the patient and his husband doesn’t have
source of income

A. Working Diagnosis
Postpartum Hypertension (pre-eclampsia)
B. Chief Complaint and Reason for Visit:
Hypertension
C. History of Present Illness:
Our patient had 3 pregnancies; all children were born at right gestational age. She had no
history of abortion and multiple births. All children are living. According to the patient she has
been experiencing intrapartal and PIH every time she gets pregnant. She got complete pre-natal
check-ups from the health center. Her blood pressure started to get elevated on the 3rd trimesters
of each pregnancy and continues even after she gave birth. After she gave birth to her youngest
son at home, the attending midwife decided to bring her to the hospital for referral since her
blood pressure went up to 200/140 mmHg. This was her first time to be admitted to the hospital
due to postpartum hypertension.
D. Past History:
Mrs. R.E.R. already gave birth to 3 boys. Her first child was born April 23, 2003 and the
next child was born March 14, 2008 and just on September 25, 2011 she gave birth to another
baby boy. All children were born full term. She gave birth to her children at home by normal
delivery and was attended by a midwife.
E. Family History of Illness:
The patient has a family history of hypertension. According to her, both of her parents
have hypertension.
IV. Physical Assessment

Assessment Normal Findings Actual Findings InterpretationBody Build,
Height & WeightProportionate Varies With
Lifestyle
Proportionate Varies With Lifestyle
Proportionate body there is no evidence of physical
problemsPosture And Gait Stands normally Stands normally Relaxed, erect posture;
coordinated movementBody And Breath
OdorNo Body Or Breath
OdorNo Body Or Breath
OdorProper hygiene
maintenanceSigns Of Distress No Distress Noted distress noted Because of lack of sleep,
distress notedAttitude Cooperative Cooperative Thinks normally, proper to
the situationAffect Or Mood Appropriate To The
SituationAppropriate To The
SituationShe acts and think
normally appropriate to the situation
Quantity, Quality And Organization
Of Speech
Understandable, Moderate Pace,
Thought Association
Understandable, Moderate Pace,
Thought Association
Can speak normally, with normal voice tone
Relevance And Association
Thought Exhibits
Logical Sequence Make Sense, Has Sense Of Reality
Logical Sequence Make Sense, Has Sense
Of Reality
Talking with sense means she thinking normally
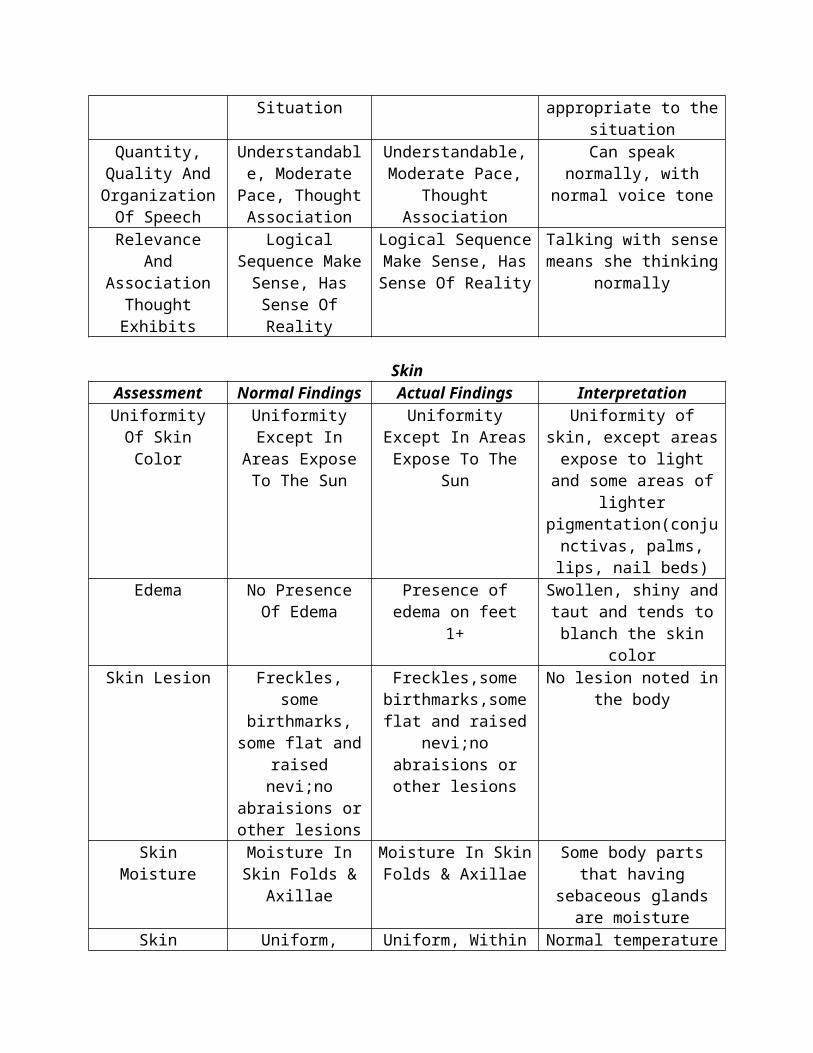
SkinAssessment Normal Findings Actual Findings Interpretation
Uniformity Of Skin Color
Uniformity Except In Areas Expose To
The Sun
Uniformity Except In Areas Expose To The
Sun
Uniformity of skin, except areas expose to light and
some areas of lighter pigmentation(conjunctivas
, palms, lips, nail beds)Edema No Presence Of
EdemaPresence of edema on
feet 1+Swollen, shiny and taut and tends to blanch the
skin colorSkin Lesion Freckles, some
birthmarks, some flat and raised
nevi;no abraisions or other lesions
Freckles,some birthmarks,some flat and raised nevi;no abraisions or other
lesions
No lesion noted in the body
Skin Moisture Moisture In Skin Folds & Axillae
Moisture In Skin Folds & Axillae
Some body parts that having sebaceous glands
are moistureSkin Temperature Uniform, Within
Normal RangeUniform, Within Normal Range
Normal temperature uniformity
Skin Turgor Skin Springs Back To Previous State
When Pinched
Skin Springs Back To Previous State When Pinched, except the
Skin stays pinched or tented or moves back
slowly

part with edema
Skull and FaceAssessment Normal Findings Actual findings Interpretation
Head Rounded And Symmetrical, Smooth Skull Contour, No
Nodules
Rounded And Symmetrical, Smooth
Skull Contour, No Nodules
Normal, no signs of any deformities and signs of
skull contour and nodules
Eyes and VisionEyebrows Evenly Distributed,
Symmetrical, Skin Intact
Evenly Distributed, Symmetrical, Skin
Intact
Properly distributed, equal
Eyelids Skin Intact, No Discharges, No Discoloration, Symmetrical
Skin Intact, No Discharges, No Discoloration, Symmetrical
Can blink normally
Eyelashes Equally Distributed,
Slightly Curved Outward
Equally Distributed, Slightly Curved
Outward
Turned outward, equally distributed, muscle normally contract
Conjunctiva Shiny, Smooth ,Sometimes
Appear Red Or Pink
Pale conjunctiva Pale, possible anemia
Lacrimal Gland No Edema Or Tearing
No Edema Or Tearing Normal no evidence of any swelling or tenderness
Cornea Transparent, Shiny, Smooth, Blinks When Cornea Is
Touched
Transparent, Shiny, Smooth, Blinks When
Cornea Is Touched
Corneal sensitivity test active,trigeminal nerve is intact,cornea clarity and
texture normal.Pupils Black Color,smooth
border,PERRLABlack Color, smooth
border,PERRLAPupils are equal,constrict to light dilate in the dark
Eyes(Visual Acuity)
Can see without using eyeglasses
Can’t see without eyeglasses
Nearsightedness, can see only when objects are near
Ears and HearingAuricles Color Is Uniform,
Symmetric, Mobile, Firm pinna Recoils
When Folded
Color Is Uniform, Symmetric, Mobile, Firm pinna Recoils
When Folded
Color same as facial skin,auricle aligned with outer canthus of the eye.
Response To Normal Voice
Tone
Normal Voice Tone Audible
Cannot hear Normal Voice Tone
Abnormal cannot hear Normal voice, normal
voice tones
Nose and SinusesNares Symmetric,
Straight, No Discharges, Non
Swelling, Uniform Color, Not Tender
Symmetric, Straight, No Discharges, Non Swelling, Uniform Color, Not Tender
No presence of lesions,air moves freely as the client
breaths
Lining Of Nose Nasal Septum In Midline
Nasal Septum In Midline
Normal and in midline
MouthLips And Buccal
MucosaPink, Soft,
SymmetricalPale lips and buccal
mucosaAbnormal, possible
anemiaTeeth And Gums Complete Complete No tooth decay,smooth
shiny tooth enamel,no dentures
Tongue In Midline, Freely Movable, Pink
In Midline, Freely Movable, Pink
In Central position,moist,slightly
rough ;thin whitish coating,normal,can move
freelyPalates And Uvula,
TonsilsLight Pink, No
Discharges, Present Gag Reflex
Light Pink, No Discharges, Present
Gag Reflex
No discoloration, palates are lighter pink hard
palate
Neck and Musculoskeletal SystemShape And Symmetry
Symmetrical Symmetrical Positioned in midline
Spinal Deformities Vertically Aligned Vertically Aligned Normal, no deformities
Inspect Neck Muscles
Symmetrical With Head Centered
Symmetrical With Head Centered
No swelling or masses,coordinated,smoot
h movements with no discomfort
Observe Head Movement
Coordinated, Smooth, Movement
With No Discomfort, Equal
Strength
Coordinated, Smooth, Movement With No Discomfort, Equal
Strength
No discomfort, can hyper extends, laterally flexes
and rotates
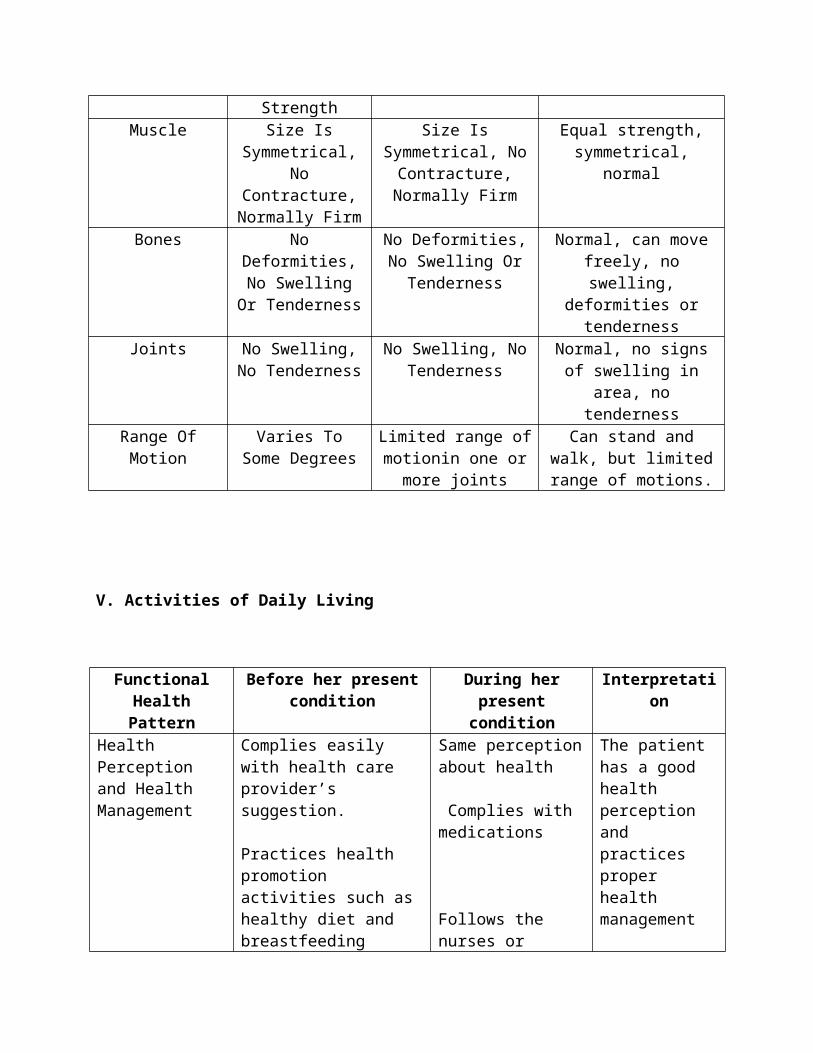
Muscle Size Is Symmetrical, No
Contracture, Normally Firm
Size Is Symmetrical, No Contracture, Normally Firm
Equal strength, symmetrical, normal
Bones No Deformities,No Swelling Or
Tenderness
No Deformities,No Swelling Or
Tenderness
Normal, can move freely, no swelling, deformities
or tendernessJoints No Swelling, No No Swelling, No Normal, no signs of

Tenderness Tenderness swelling in area, no tenderness
Range Of Motion Varies To Some Degrees
Limited range of motionin one or more
joints
Can stand and walk, but limited range of motions.
V. Activities of Daily Living
Functional Health Pattern
Before her present condition
During her present condition
Interpretation
Health Perception and Health Management
Complies easily with health care provider’s suggestion.
Practices health promotion activities such as healthy diet and breastfeeding
Visits the health center for check-up when sick.
Does not have traditional health beliefs and
Same perception about health
Complies with medications
Follows the nurses or doctor’s suggestion
The patient has a good health perception and practices proper health management
Nutritional and Metabolic
Eats 3 times daily. The usual food intake would be composed of fish and vegetables, seldom eats meat Drinks 5 glasses of water and 2 cups of coffee a day
Takes vitamins as a supplement
Skin color was fair, height proportional to body weight
Same amount and quality of food is taken
Coffee was eliminated
Discontinued taking vitamins
Pale color of skin, height still proportional to body weight
Patient’s diet had no change so it can’t be directly inferred that skin pallor was due to diet.
Elimination Moves bowel once a day without difficulty
Same bowel movement frequency
Bowel movement was affected because patient

Soft firm stoolVoids fair amount of urine without difficulty in normal frequency
Clear, yellow urine
Difficulty moving bowels although stool quality is soft and firm
More frequency in voiding urine in the lesser amount and same quality
can’t exert enough effort to expel stool.
Activity – Exercise Considers doing household chores as an exercise
Leisure time spent by chatting with friends and playing with kids
No exercise done due to confinement
Leisure time spent by chatting with husband
Exercise was eliminated since she cannot do household chores while in the hospital and she didn’t replace it by another form of exercise.
Sleep-Rest Has 6 - 8 hours of sleep everyday
Deep, uninterrupted sleep
Gets enough energy from sleepDoesn’t need any sleep aids
Has maximum of 3 hours of interrupted sleep
Takes nap in the afternoon to compensate lost sleeping hours
Inadequate sleep due to noisy environment,
Cognitive-Perceptual
Normal hearing acuity and does not use hearing aid
Uses eyeglasses
Able to comprehend easily
Asks to repeat the questions during the interview
Eyeglasses left at home
Comprehension has changed because patient can’t hear clearly.
Self-Perception and Self-Concept Pattern
Feels good about herselfHas ability to do normal activities without helpDoesn’t have anything that causes anger, anxiety and depression
Had worried about her child’s nutrition since the newborn was left at home but now feels better because the newborn is already with her
Anxiety is no longer an issue since her baby is already with her.

VI. Development Tasks
Generativity vs. Stagnation
At the age of 30, the significant task of the patient is to perpetuate culture and transmit values of culture through the family and working to establish a stable environment. In her age, success is achieved by contributing to the world by being active in their home and community or society. Mrs. R.E.R. is a full time housewife since she got married so she only had continued to build her life focusing on her family. Although she shows self fulfillment in terms of being a mother and wife, she manifested the feeling of lack of accomplishment because she mentioned that she also wants to play a different role in the society by having a career or job someday.
VII. Laboratory/Diagnostic Findings
Date Procedure Norms Result
Analysis Interpretation
September 25, 2011
Hemoglobin 115-155 95 Due to blood loss which causes decreased RBC
resulting to low Hgb
Decreased
Hematocrit 0.40-0.48
0.30 Due to blood loss which causes decreased RBC
resulting to low Hgb
Decreased
WBC Count 5.0-10.0 12.9 Urinary tract infection IncreasedLymphocyte
s0.2-0.4 0.25 No viral or chronic bacterial
infectionNormal
Gabriel J. Cruz , MD, DPSPPATHOLOGIST
ROUTINE URINALYSIS September 25, 2011
Urine Result Analysis InterpretationColor Amber Normal urine concentration Normal
Transparency Turbid Bacterial Infection AbnormalReaction Acidic Due to the amount of sodium
and excess acid retained by the body
Abnormal
Specific Gravity 1.02 Normal urine concentration NormalProtein + + + + Hypertension affects filtration
that can cause excessive protein in urine
Abnormal
Sugar Negative No diabetes NormalRBC 3-5/HPF No bleeding in urinary system Normal
Pus Cells 8-10/HPF Bacterial infection in urinary tract
Abnormal
Epithelial Cells + Inflammation within urinary tract
Abnormal
Bacteria + Infection on urinary tract AbnormalMucus Threads + Inflammation within urinary
tractAbnormal
Amorphous Urates + Uric acid crystals Abnormal
Gabriel J. Cruz , MD, DPSPPATHOLOGIST
VIII. Anatomy and Physiology (Affected Organ)
HEART
The heart is responsible for maintaining adequate circulation of oxygenated blood around
the vascular network of the body. It is a four-chamber pump, with right side receiving
deoxygenated blood from the body at low pressure and pumping it to the lungs. And at the left
side receiving oxygenated blood form the lungs and pumping I at the high pressure around the
body. The myocardium is a specialized form of muscle, consisting of individual cells joined by
electrical connections. The contraction of each cell is produced by a rise in intracellular leading
to spontaneous depolarization, and as each cell electrically connected to its neighbor, contraction
of one cell leads to wave of depolarization and contraction across the myocardium. This
depolarization and contraction of the heart is controlled by a specialized group of cells localized
in the sino-atrial node in the right atrium pacemaker cells.
KIDNEY

The kidney is the responsible for the volume and concentration of fluids in the body by
producing urine. Urine is produce in a process called glomerular filtration, which remove as the
waste products, minerals and water from the blood. The kidney maintains the volume of the fluid
in the body and also the concentration of urine by filtering the waste product and reabsorbing
useful substances and water from the blood. The kidney also performs detoxification of harmful
substances increase absorption of calcium by producing calcitrol (form of vitamin D) and also
secretes rennin (hormone that regulates blood pressure and electrolyte.)
IX. Pathophysiology (Flowchart)
(Predisposing) (Precipitating)
Age: 30 Lifestyle: drinks occasionally
Stress (Financial needs of the family)
Gender: F
Eating habits
Race: Filipino
Family History: both parents have hypertension.

VASOSPASM
VASCULAR EFFECT KIDNEY INTERSTITIAL EFFECT
VASOCONSTRICTION KIDNEY EFFECT EDEMA
DECREASE URINE
INCREASE OF BP OUTPUT AND PROTENURIA (160/120) (150ml)
Who is at risk for Pregnancy induced hypertension?
-PIH is more common during a woman’s first pregnancy and in women whose mothers or sisters
had PIH. The risk of PIH is higher in women carrying multiple babies, in teenage mothers and in
women older than 40 years of age. Other women at risk include those who had high blood
pressure or kidney disease before they became pregnant.
How does vasospasm affects the Heart?
Vasospasm happens by increased cardiac output that injures the endothelial cells of the arteries.
The blood vessels during pregnancy are resistant to the effects of pressors substances such as
angiotensin and norepinephrine, so blood pressure remain normal during pregnancy.
How does vasospasm affects the Kidney?
Vasospasm in the kidney increases blood flow resistance. Degenerative changes develop in the
kidney glomeruli because of back-pressure. This leads to increased permeability of the
glomerular membrane, allowing the serum proteins albumin and globulin to escape into the urine

the degenerative changes also results in decreased glomerular filtration, so there is a decrease
urine output and clearance of creatinine.
X. Course in the Ward
Mrs. R.E.R. a 30 year old postpartum who gave birth to her baby at home attended by a midwife was suspected to have a postpartum hypertension was admitted to the Ospital ng Lungsod ng San Jose Del Monte.
DAY 1 (Sept. 25 2011, 7pm-7am)
As the client admitted by Dr. Roberto Enriquez to the OB ward, she was given a liter of intravenous fluid of D5LR solution at 20 gtts/min. She was inserted a Foley catheter connected to the urine bag and Vital signs were taken. She was instructed for NPO. And as of 4pm she was given an initial dose of MgSO4, 4grams infused 250ml 5% of dextrose solution, her blood pressure was monitored 200/100. At 5pm she had given MgSO4 5grams diluted in 10ml of sodium chloride in each buttock deep intramuscular and she was asked by the nurse if she didn’t experience abdominal pain, nausea or vomiting before the medication was administered. After that her Blood pressure was 170/100, and after 30 minutes she had given Hydralizine 5ml every 6 hours intravenous, it was administered slowly. And as of 2am she was given Amlodipine 5mg twice a day as ordered by the physician.
DAY 2 (Sept. 26 2011, 7am-7pm)

Her Blood pressure was 140/100 and had continued MgSO4. As ordered by the physician the dose of Amlodipine increased to 10mg twice a day. And once she completed the MgSO4 , the nurse may remove the inserted Foley catheter. Her hemoglobin count was 95, and urinalysis result was +4 as seen and examined by Dra. Garza who ordered to discontinue antibiotics and to start Cephalexine 500mg/cap every 6 hours in 7 days and FeSO4 twice a day . and the patient was told she may go home if she completed MgSO4 and was controlled her Blood pressure with Amlodipine . She was also instructed to take Diazepam 5g twice a day in 1 week continuously even she’s at home.
DAY 3 (Sept. 27 2011, 7pm-7am)
Her blood pressure was150/100 and was referred to Dra. Comia, then her oral medications were given and then were referred to OB.
DAY 4 (Sept. 28 2011, 7am-7pm)
She walked slowly with an intravenous fluid and was referred to MS-OB and vital signs were taken. Her medications were given; her Blood pressure was monitored and was referred to Dr. Nieto.
DAY 5(Sept. 29 2011, 7pm-7am)
She was taken a low sodium low fat diet and still taking her medication, vital signs were taken. Her Blood was monitored. Clonidine 5g was given sublingual as instructed by the physician. Then her blood pressure became 150/90 after an hour. She was referred to Dr. Gonzales with orders in and carried out.
DAY 6 (Sept. 30 2011, 7am-7pm)
Oral medications were given, uterus was firm and contracted, her vital signs were taken and blood pressure was monitored 150/100. She was advised to breastfeed.

.

XI. Nursing Care Plans
ASSESSMENT DIAGNOSIS PLANNING INTERVENTION RATIONALE EVALUATIONSubjective:None
Objective:PittingEdema:3secondsLowerextremities:BipedalEdema
UO:150 cc per hour
VS:BP: 160/120BT: 36.4PR: 104RR: 18
Excessive fluid volume related to increasedfluid retention as manifested by the presence of edema in the feet.
Short Term Goal:After 8 hours of nursing intervention the patient’s edema will be decreased as evidenced by pitting edema (1-2 seconds)
Long Term Goal:After 2 days of nursing intervention, the patient will have stabilized fluid volume as evidenced by balanced input/output, vital signs within client’s normal limits and free of signs of edema
Independent>Monitor urine output
>Monitor BP
>Encourage the patient to eat fruits and vegetables that has high diuretic property
>Elevate edematous extremities, change in position frequently
>Discuss the importance of fluid restrictions
Dependent:>Insert indwelling urinary catheter as per doctors order
>Restrict sodium and fluid intake as indicated
>Kidney function is directly correlated to circulatory fluid volume, so that if fluid is trapped in third spaces, output decreases and specific gravity increases.
>Changed parameters may indicate altered fluid or electrolyte status.
>Helps to increase urine output thus decreases fluid retention
>Helps to reduce tissue pressure and risk of skin breakdown. to increase venous blood return
>Helps the client to understand the relationship of food restriction to her condition
>Provides accurate hourly totals of urine output, and monitors client for developing renal problems or oliguria.
>Restricting the sodium in the diet will favor the renal excretion of excess fluid. Fluid restriction may decrease intravascular volume and myocardial workload
Short Term Goal:After 8 hours of nursing intervention the patient’s edema was decreased as evidenced by pitting edema (1-2 seconds
Long Term Goal:After 2 days of nursing intervention, the patient had stabilized fluid volume as evidenced by balanced input/output, vital signs within client’s normal limits and free of signs of edema

ASSESSMENT DIAGNOSIS PLANNING INTERVENTION RATIONALE EVALUATIONSubjective:
“Di ko alam kung bakit nakaconfine pa ako, mataas nga ang bp ko pero feeling ko okay naman ako dahil wala naman akong masakit na nararamdaman” as verbalized by the client.
Objective:
>Observed confusion when patient was asked about her condition
>Lack of information source ( no television and radio at home)
Knowledge regarding condition, prognosis Related to lack of exposure/unfamiliarity with information as manifested by statement of misconceptions
Short Term Goal:After 4 hours of nursing intervention, client will identify signs/symptoms requiring medical evaluation.
Long Term Goal:After 1 day of nursing intervention, the client will verbalize understanding of disease and appropriate treatment plan.
Independent: >Assess client’s knowledge of the disease process.
>Provide information about the disease and the complications that it can cause.
>Provide information about signs/symptoms, and instruct client when to notify healthcare provider.
>Keep client informed of health status, results of tests.
>Establishes data base and provides information about areas in which learning is needed.
>Makes the client know the importance of treatment and management of her condition.
>Helps ensure that client seeks timely treatment indicating worsening of condition or additional complications.
>Fears and anxieties can be compounded when client does not have adequate information about the state of the disease process.
Short Term Goal:After 4 hours of nursing intervention, client was able to identify signs/symptoms requiring medical evaluation.
Long Term Goal:After 1 day of nursing intervention, the verbalized understanding of disease process and appropriate treatment plan.

ASSESSMENT DIAGNOSIS PLANNING INTERVENTION RATIONALE EVALUATIONSubjective:
> "Hindi ako makatulog ng maayos, halos tatlong oras lang na deretsong tulog sa isang araw tapos putol-putol na". As verbalized by the client.
Objective:
>Pale conjunctiva, lips, palm and skin
>Frequent yawning
>Dark circles under the eyes
VS:BP: 160/120BT: 36.4PR: 104RR: 18
>Disturbed sleep pattern related to uncomfortable environment as manifested by pale conjunctiva, lips, palm and skin frequent yawning and dark circles under the eyes.
Short Term Goal:>After 4 hours of nursing intervention the client will demonstrate relaxation skills and other methods to promote sleep.
Long Term Goal:>After 1 day of nursing intervention the client will be able to sleep at least 8 hours a day.
Independent:>advise to establish regular bedtime and wakeup time and a short daytime nap.
>Advise to take warm bath before bedtime.
>Advise to wear loose-fitting shirts.
>Advise to drink 1 glass of warm milk before sleeping.
>encourage voiding before going to sleep.
Collaborate:>Advise the roommates to lower their voices and prevent noise at bedtime.
>To promote good sleeping pattern
>To promote feeling of freshness before sleeping.
>To promote comfort while sleeping.
>Milk contains tryptophan, a precursor of serotonin, which is thought to induce and maintain sleep.
>To avoid interruption in the middle of sleep.
>To reduce noise destruction for the comfortable sleep of the patients.
Short Term Goal:>After 4 hours of nursing intervention the client was able to demonstrate relaxation skills and other methods to promote sleep.
Long Term Goal:>After 1 day of nursing intervention the client was able to sleep at least 8 hours a day.

XII. Drug Study
Name of Drug
Classification Mechanism of Actions Indication Contraindication Adverse Effect Drug to Drug Interaction
Nursing Consideration
Amlodipine Antianginal
Antihypertensive
Calcium Channel Blocker
Inhibits the movement of calcium ions across the membranes of cardiac and arterial muscle cells; inhibits transmembrane calcium flow, which result in the depression of impulse formation in specialized cardiac pacemaker cells, slowing of the velocity of conduction of the cardiac impulse, depression of myocardial contractility , and dilation of coronary arteries and arterioles and peripheral arterioles; these effects lead to decreased cardiac work, decreased cardiac oxygen consumption, and in patients with vasospastic (Prinzmetal’s) angina,increased delivery of oxygen to cardiac cells.
Angina pectoris due to coronary artery spasm (Prinzmetal’s variant angina)
Chronic stable angina, alone or in combination with other drugs
To reduce the risk of hospitalization due to angina and to reduce the need for coronary revascularization procedures in patients with angiographically documented CAD without heart failure or ejection fraction less than 40%
Essential hypertension, alone or in combination with other antihypertensives
Contraindicated with allergy to amlodipine, impaired hepatic or renal function, sick sinus syndrome, heart block (second or third degree), and lactation.
Use cautiously with heart failure, pregnancy.
CNS: Dizziness,light-headedness, headache, asthenia, fatigue,lethargy
CV: Peripheral edema, arrhythmias
Dermatologic: Flushing, rash
GI: Nausea, abdominal discomfort
Monitor BP very carefully if patient is also on nitrates.
Monitor cardiac rhythm regularly during stabilization of dosage and periodically during long-term therapy.
Administer drug without regard to meals.

Name of Drug
Classification Mechanism of Actions
Indication Contraindication Adverse Effect Drug to Drug Interaction
Nursing Consideration
Cephalexin Antibiotic
Cephalosporin (first generation)
Bactericidal: Inhibits synthesis of bacterial cell wall, causing cell death.
Respiratory tract infections caused by Streptococcus pneumonia, group A beta hemolytic streptococci.
Skin and skin structure infections caused by staphylococcus, streptococcus
Otitis media caused by S. pneumonia, Haemophilusinfluenzae, streptococcus, staphylococcus, Moraxella catarrhalis
Bone infections caused by staphylococcus, Proteus mirabilis
GU infections caused by Escherichia coli, P. mirabilis, Klebsiella
Contraindicated with allergy to cephalosporins or penicillins.
Use cautiously with renal failure, lactation, pregnancy.
CNS: Headache, dizziness, lethargy, paresthesia
GI: Nausea, vomiting, diarrhea, anorexia, abdominal pain, flatulence, pseudomembranous colitis, hepatotoxicity
GI: Nephrotoxicity
Hematologic: Bone marrow depression
Hypersensitivity: Ranging from rash to fever to anaphylaxis; serum sickness reaction
Other: Super infections
Increased nephrotoxicity with amino glycosides
Increased bleeding effects with oral anticoagulants
Disulfiramlike reaction may occur if alcohol is taken within 72 hr after cephalexin administration
Arrange for culture and sensitivity tests of infection before and during therapy if infection does not resolve.
Give drug with meals; arrange for small, frequent meals if GI complications occur.
Refrigerate suspension, discard after 14 days.
Name of Drug
Classification Mechanism of Actions
Indication Contra indication
Adverse Effect Drug to Drug Interaction
Nursing Consideration
Cefuroxime Antibiotic
Cephalosporin
Bactericidal: Inhibits synthesis of bacterial cell wall, causing cell death.
Pharyngitis, tonsillitis, caused by Streptococcus pyogenes
Otitis media caused by Stretococcus pneumonia, S.pyogenes, Haemophilus influenza, Moraxella catarrhalis
Acute bacterial maxillary sinusitis caused by S. pneumonia, H. influenza
Lower respiratory infections caused by S. pneumonia, Haemophilus parainfluenza, H. influenza
UTIs caused by Escherichia coli, Klebsiella pneumonia
Uncomplicated gonorrhea (urethral and endocervical)
Skin and skin structure infections, including impetigo caused by Streptococcus aureus, S. pyogenes
Treatment of early Lyme disease
Contraindicated with allergy to cephalosporins or penicillins.
Use cautiously with renal failure, lactation, pregnancy
CNS: Headache, dizziness, lethargy, paresthesias
GI: Nausea, vomiting, diarrhea, anorexia, abdominal pain, flatulence, pseudomembranous colitis, hepatotoxicity
GU: Nephrotoxicity Hematologic: Bone
marrow depression Hypersensitivity:
Ranging from rash to fever to anaphylaxis; serum sickness reaction
Local: Pain, abscess at injection site, phlebitis, inflammation at IV site
Other: Super infections, disulfiram-like reaction with alcohol
Increased nephrotoxicity with amino glycosides
Increased bleeding effects with oral anticoagulant
Risk of disulfiram-like reaction with alcohol; avoid this combination during and for 3 days after completion of therapy
Culture infection site, and arrange for sensitivity test before and during therapy if expected response is not seen.
Give oral drug with food to decreased GI upset and enhance absorption.
Give oral tablets to children who can swallow tablets; crushing the drug results in a bitter, unpleasant taste. Use solution for children who cannot swallow tablets.
Have vitamin K available in case hypoprothrombinemia occurs.
Discontinue if hypersensitivity reaction occurs.

Name of Drug Classification Mechanism of Actions
Indication Contraindication Adverse Effect
Drug to Drug Interaction
Nursing Consideration
Ferrous sulfate Iron preparation
Elevates the serum iron concentration, and is then converted to Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron.
Prevention and treatment of iron deficiency anemia
Dietary supplement for iron
Unlabeled use: Supplemental use during epoetin therapy to ensure proper hematologic response to epoetin
Contraindicated with allergy to any ingredient; sulfite allergy; hemochromatosis, hemosiderosis, hemolytic anemia.
Use cautiously with normal iron balance; peptic ulcer, regional enteritis, ulcerative colitis.
CNS: CNS toxicity, acidosis, coma and death with overdose
GI: GI upset, anorexia, nausea, vomiting, constipation, diarrhea, dark stools, temporary staining of the teeth(liquid preparations)
Decreased anti-infective response to ciprofloxacin, norfloxacin, ofloxacin; separate doses by at least 2 hr
Decreased absorption with antacids, cimetidine
Decreased effects of levodopa if taken with iron
Increased serum iron levels with chloramphenicol
Decreased absorption of levothyroxine; separate doses by at least 2 hr
Confirm that patient does have iron deficiency anemia before treatment.
Give drug with meals (avoiding milk, eggs, coffee, and tea) if GI discomfort is severe; slowly increase to build up tolerance.
Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth; have the patient drink solution with a straw.
Warm patient that stool may be dark or green.
Arrange for periodic monitoring of Hct and Hgb levels.

Name of Drug
Classification Mechanism of Actions
Indication Contraindication Adverse Effect Drug to Drug Interaction
Nursing Consideration
Hydralazine Antihypertensive
Vasodilator
Acts directly on vascular smooth muscle to cause Vasodilation, primarily arteriolar, decreasing peripheral resistance; maintains or increases renal and cerebral blood flow.
Oral: Essential hypertension alone or in combination with other drugs
Parenteral: Severe essential hypertension when drug cannot be given orally or when need to lower BP is urgent
Unlabeled uses: Reducing afterload in the treatment of heart failure, severe
Contraindicated with hypersensitive ty to hydralazine, tartrazine (in 100-mg tablets marketed as Apresoline); CAD, mitral valvular rheumatic heart disease (implicated in MI).
Use cautiously with CVAs; increased in tracranial pressure (drug-induced BP decrease increases risk of cerebral ischemia); severe hypertensionwith uremia; advanced renal damage; slow acetylators
CNS: Headache, peripheral neuritis, dizziness, tremors, psychotic reactions characterized by depression, disorientation, or anxiety
CV: Palpitation, tachycardia, angina pectoris, hypotension, paradoxical pressor response, orthostatic hypotension
GI: Anorexia, nausea, vomiting,diarrhea, constipation, paralytic ileus
GU: Difficult micturition, impotence
Hematologic: Blood dyscrasias
Hypersensitivity: Rash, urticaria, pruritis; fever, chills, arthralgia,
Increased pharmacologic effects of beta-adrenergic blockers and hydralazine when given concomitantly; dosage of beta blocker may need adjustment
Give oral drug with food to increase bioavailability (drug should be given in a consistent relationship to ingestion of food for consistent response to therapy).
Drug may cause a syndrome resembling SLE. Arrange for CBC, lupus erythematosus (LE) cell preparations, and ANA titers before and periodically during prolonged therapy, even in the asymptomatic patient. Discontinue if blood dyscrasias occur. Reevaluate therapy if ANA or LE tests are positive.
Arrange for pyridoxine therapy if patient develops symptoms of peripheral neuritis.
Monitor patient for orthostatic

aortic insufficiency, and after valve replacement (doses up to 800 mg tid)
(higher plasma levels may be achieved; lower dosage may be adequate); lactation, pregnancy,pulmonary hypertension.
eosinophilia; rarely, hepatitis, obstructive jaundice
Other: Nasal congestion, flushing, edema, muscle cramps, lymphadenopathy, splenomegaly, dyspnea, lupus-like syndrome, possible carcinogenesis, lacrimation, conjunctivitis
hypotension, which is most marked in the morning and in hot weather, and with alcohol or exercise

Name of Drug
Classification Mechanism of Actions
Indication Contraindication Adverse Effect Drug to Drug Interaction
Nursing Consideration
Magnesium Sulfate
Antiepileptic
Electrolyte
Laxative
Cofactor of many enzyme systems involved in neurochemical transmission and muscular excitability; prevents or controls seizures by blocking neuromuscular transmission; attracts and retains water in the intestinal lumen and distends the bowel to promote mass movement and relieve constipation.
Acute nephritis (children), to control hypertension
IV: Hypomagnesemia, replacement therapy
IV or IM: Preeclampsia or eclampsia
PO: Short-term treatment of constipation
PO: Evacuation of the colon for rectal and bowel examinations
To correct or prevent hypomagnesemia in patients on parenteral nutrition
Contraindicated with allergy to magnesium products; heart block, myocardial damage; abdominal pain, nausea, vomiting, or other symptoms of appendicitis; acute surgical abdomen, fecal impaction, intestinal and biliary tract obstruction, hepatitis. Do not give during 2 hr preceding delivery because of risk of magnesium toxicity in the
CNS: Weakness, dizziness, fainting, sweating (PO)
CV: Palpitations
GI: Excessive bowel activity, perianal irritation (PO)
Metabolic: Magnesium intoxication(flushing, sweating, hypotension, depressed reflexes, flaccid paralysis, hypothermia, circulatory collapse, cardiac and CNS depression-parenteral); hypocalcemia
Potentiation of neuromuscular blockade produced by non-depolarizing neuromuscular relaxants
Reserve IV use in eclampsia for immediate life-threatening situations
Give IM route by deep IM injection of the undiluted (50%) solution for adults; dilute to a 20% solution for children.
Give oral magnesium sulfate as a laxative only as a temporary measure. Arrange for dietary measures (fiber, fluids), exercise, and environmental control to return to normal bowel activity.
Do not give oral magnesium sulfate with abdominal pain, nausea, or vomiting.
Monitor bowel function; if diarrhea and cramping occur, discontinue oral drug.
Maintain uterine

Unlabeled uses: Inhibition of premature labor (parenteral), adjust treatment of exacerbations of acute asthma; treatment torsades de pointes, atypical ventricular arrhythmias
neonate. Use
cautiously with renal insufficiency.
with tetany (secondary to treatment of eclampsia-parenteral)
output at a level of 100 ml every 4 hr during parenteral administration.
Name of Drug
Classification Mechanism of Actions
Indication Contraindication Adverse Effect Drug to Drug Interaction
Nursing Consideration

Methyldopa Antihypertensive
Sympatholytic
Mechanism of action not conclusively demonstrated; probably due to drugs metabolism, which lower arterial BP by stimulating CNS alpha2-adrenergic receptors, which in turn decreases sympathetic outflow from the CNS,
Hypertension IV
methyldopate: Acute hypertensive crisis; not drug of choice because of slow onset of action
Unlabeled uses: Hypertension of pregnancy
Contraindicated with hypersensitivity to methyldopa, active hepatic disease, previous methyldopa therapy associated with liver disorders.
Use cautiously with previous liver disease, renal failure, dialysis, bilateral cerebrovascular disease, pregnancy, RR lactation.
CNS: Sedation, headache ,asthenia, weakness (usually early and transient), dizziness, light-headed symptoms of cerebrovascular insufficiency, paresthesias, parkinsonism, Bells palsy,decreased mental acuity, involuntary choreoathetotic movements, psychic disturbances
CV: Bradycardia, prlonged carotid anus hypersensitivity, aggravation of angina pectoris,paradoxical pressor response, pericarditis, myocarditis, orthostatic hypotension, edema
Dermatologic: Rash seen as eczema or lichenoid eruption, toxic epidermal necrolysis fever, lupus like syndrome
Endocrine: Breast enlargement, gynecomastia, lactation, hyperprolactinemia, amenorrhea, galactorrhea,
Potentiation of the pressor effect of sympathomimetic amines
Increased hypotension with levodopa
Risk of hypotension during surgery with central anesthetic; monitor patient carefully
Administer IV slowly over 30-60 min; monitor injection site
Add athiazide to drug regimen or increase dosage if methyldopa tolerance occurs

impotence, failure to ejaculate, decreased libido
GI: Nausea, vomiting, distention, constipation, flatus, diarrhea, colitis, dry mouth, sore or black tongue, pancreatitis, sialadenitis, abnormal liver function tests, jaundice, hepatitis, hepatic necrosis.
Hematologic: Positive Coombs test, hemolytic anemia, bone marrow depression leucopenia, granulocytopenia, thrombocytopenia, positive tests for antinuclear antibody, lupus like syndrome, and rheumatoid factor

XIII. Discharge Planning
MEDICATION Advise patient not to skip the medication that the doctor ordered
EXERCISE/ENVIRONMENT Enough rest Elevate feet several times a day during the day
TREATMENT Use of drugs Catheterization Obtaining labs(CBC,PLATELETS COUNT,LIVER
FUNCTION)
HEALTH TEACHING
Encourage patient for sodium restriction Encourage to avoid foods rich in oils and fats Encourage patient to limit her daily activities and
exercise Encourage to avoid Salty, high fat diet, instead eat
healthy foods. Advise to continue medicine as prescribed Separate utensils for the mother and other things that
will be used for the whole family Encourage eat high protein foods, calcium,
magnesium, zinc, vitamin c and e Health teachings for symptoms mild and severe pre-
eclampsia
OPD FOLLOW UP Observe carefully for symptoms Give instruction about what symptoms to watch for so
she can alert clinician if additional symptoms occur between visits
Provide information about how to control the disease
DIET
Low fats and sodium diet, restriction if possible High in protein, calcium and iron Adequate fluid intake Eat fresh green healthy leafy vegetables and fresh
fruits
SPIRITUAL/SEX Limit sexual activity Provide spiritual and emotional support
Homework Help
https://www.homeworkping.com/

Math homework help
https://www.homeworkping.com/
Research Paper help
https://www.homeworkping.com/
Algebra Help
https://www.homeworkping.com/
Calculus Help
https://www.homeworkping.com/
Accounting help
https://www.homeworkping.com/
Paper Help
https://www.homeworkping.com/
Writing Help
https://www.homeworkping.com/
Online Tutor
https://www.homeworkping.com/
Online Tutoring
https://www.homeworkping.com/
Homework Help
https://www.homeworkping.com/

Math homework help
https://www.homeworkping.com/
Research Paper help
https://www.homeworkping.com/
Algebra Help
https://www.homeworkping.com/
Calculus Help
https://www.homeworkping.com/
Accounting help
https://www.homeworkping.com/
Paper Help
https://www.homeworkping.com/
Writing Help
https://www.homeworkping.com/
Online Tutor
https://www.homeworkping.com/
Online Tutoring
https://www.homeworkping.com/