![arXiv:2009.14544v1 [physics.acc-ph] 30 Sep 2020 transform, tune … · 2020. 10. 1. · Fig. 3. ”Soldier of Fortune” of ”Deep Purple” in time-domain representation Time Duration](https://static.fdocuments.net/doc/165x107/610dc491fbb11c7c792bcc3a/arxiv200914544v1-30-sep-2020-transform-tune-2020-10-1-fig-3-asoldier.jpg)
7th Group Soldier awarded Purple Heart
8
Friday, January 17, 2014 THE RED 7 .NET Service members hold memorial for fallen Soldier PAGE 3 ALSO INSIDE Briefs .............................. 7 Philpott............................6 Former Special Forces medic works to reduce battlefield deaths PAGE 2 7th Group Soldier awarded Purple Heart PAGE 4
Transcript of 7th Group Soldier awarded Purple Heart

F r i d a y , J a n u a r y 1 7 , 2 0 1 4 T H E R E D 7 . n E T
Service members hold memorial for
fallen SoldierPage 3
aLSO INSIDe
Briefs...............................7
Philpott............................6
Former Special Forces medic works to reduce
battlefield deathsPage 2
7th Group Soldier awarded
Purple HeartPaGE 4

Page 2 | THE RED 7 | Friday, January 17, 2014
By.DaviD.vergun
Army News Service
WaSHingTOn – A physician who was an Army Special Forces combat medic has designed a fel-lowship program that he hopes will improve the survival chances of battlefield casualties.
The aim of the Military Emer-gency Medical Services and Disas-ter Medicine Fellowship Program is to train physicians for the chal-lenges of pre-hospital care on the battlefield, in defense of the home-land or wherever else troops may be, said Army Lt. Col. (Dr.) Robert Mabry, the fellowship’s program director, at San Antonio Military Medical Center in Texas.
“Pre-hospital care” is that criti-cal time between a traumatic event and when care is received at a mili-tary treatment facility.
Mabry and his colleagues con-ducted a study of service members injured on the battlefield in Iraq and Afghanistan from 2001 to 2011. The study found that of the 4,596 battlefield fatalities analyzed, 87.3 percent died of their injuries before ever reaching a medical facility.
Of those deaths, 75.7 percent were classified as nonsurvivable, meaning they would have died even had they reached the facil-ity earlier, and 24.3 percent were deemed potentially survivable.
That study, the first of its kind, was published in the Journal of Trauma and Acute Care Surgery in 2012.
Although battlefield medicine has vastly improved during every war since World War II, Mabry said, that 24.3 percent statistic cited in his study – those who died who might have lived – kept nagging him. “That’s where we can make the biggest difference in improving patient outcomes,” he said.
Mabry found that no one “owns” responsibility for battlefield care
delivery. “No single senior military medical leader, directorate, divi-sion or command is uniquely fo-cused on battlefield care,” he said.
Commanders on the ground do own the assets of battlefield care – medics, battalion physicians, physician assistants, flight med-ics and all the equipment – but they are “neither experts in, nor do they have the resources to train their medical providers for forward medical care,” he said. Commanders rely on the medical departments to provide the right personnel, training, equipment and doctrine, he continued, but the medical departments “defer responsibility to line command-ers,” he added.
“While this division of respon-sibility may at first glance seem reasonable,” Mabry said, “the net negative effect of line command-ers lacking expertise and medical leaders lacking operational control is analogous to the axiom, ‘When everyone is responsible, no one is responsible.’”
One of the main difficulties in addressing pre-hospital care, he said, is that “we know very little about what care is provided be-fore casualties reach the combat hospital.”
Only one military unit – the Army’s 75th Ranger Regiment – tracks what happens to every casualty during all phases of care, Mabry said.
“Ranger commanders routine-ly use this data to improve their casualty response systems,” he
said, adding that the Rangers “are the only U.S. military unit that can demonstrate no potentially pre-ventable deaths in the pre-hospital setting after more than a decade of combat.”
While only the 75th Rangers did pre-hospital tracking, once the wounded arrived at a combat sup-port hospital, they were met with “robust surgical support and had less than a 2 percent chance of dy-ing,” he said.
Those who did die at the combat support hospital generally had a severe head injury or were in pro-found shock due to the loss of blood when they arrived, but some had conditions that were “potentially salvageable had they had some ag-gressive resuscitation in the field,” he added.
But the culture of military medi-cine is “hospital-based,” the doc-tor reiterated, and “no one owns battlefield medicine.”
The hospital-based mentality has its roots in the Cold War. Dur-ing the Vietnam War and later, the idea was to “put as many patients as possible in a helicopter and fly them as fast as you can to get them off the battlefield to the field hos-pital,” Mabry said. After Vietnam, those doctors, nurses and med-ics returned to the United States, took off their uniforms and “built our civilian trauma systems,” he said. Before Vietnam, he added, emergency medical services, trauma surgery and emergency medicine didn’t exist as we know them today.
As a result of the war experi-ence, sick or injured civilians in the United States today are transport-ed to a trauma center by helicop-ter, accompanied by a critical-care flight paramedic and a critical-care flight nurse – both highly trained and very experienced.
In Afghanistan, speed became a problem, he said. “When I was deployed in 2005,” he explained, “I would have to wait three hours for medevacs sometimes, and if it were a host-nation casualty, some-times even longer.”
And the level of care in-flight was less than premium, the doctor added.
“The medics, through no fault of their own, were still trained at the basic medic level,” he said. “At that time, flight medics had no requirement to provide any hands-on care to an actual patient during their training. For many, their first encounter with a seriously injured casualty was during the first flight of their first deployment.”
Mabry concluded from his stud-ies and field experience that the solution to the care gap cannot be addressed with a single-ban-dage approach. A solution, he said, would require “evidence-based improvements in tactical combat casualty care guidelines, data-driv-en research, remediation of gaps in care and updated training and equipment.”
And to supervise those med-ics, their training and the mede-vac equipment and procedures, there would need to be a specially trained and qualified physician in charge of that pre-hospital phase, he said.
Mabry’s own experience in-cludes 11 years as an enlisted Soldier, starting out in the infan-try and then becoming a Special Forces medic with a tour in Moga-dishu, Somalia, in 1993 during the
Former Special Forces combat medic designs medical fellowship program to reduce battlefield deaths
Year No. 4 edition No. 3
The Red 7 is published by the Northwest Florida Daily News, a pri-vate firm in no way connected with the 7th Special Forces Group (Airborne) or the U.S. Army.
This publication’s content is not necessarily the official view of, or endorsed by, the U.S. govern-ment, the Department of Defense, the Depart-ment of the Army or 7th Special Forc-es Group (Airborne). The official news source for 7th Special Forces Group (Airborne) is http://www.soc.mil/.
The appearance of advertising in this publication does not constitute endorsement by the U.S. govern-ment, the Department of Defense, the Department of the Army, 7th Special Forces Group (Airborne) or the Northwest Florida Daily News for products or services advertised. Ev-erything advertised in this publication shall be made available for purchase, use or patronage without regard to race, color, religion, sex, national ori-gin, age, marital status, physical handi-cap, political affiliation or any other nonmerit factor of the purchaser, user or patron. Editorial content is edited, prepared and provided by the North-west Florida Daily News.
Mail2 Eglin Parkway nE,
Fort Walton Beach, FL 32548
News(850) 315-4450
Fax: (850) 863-7834e-mail:
advertising863-1111 Ext. 1322
ConTaCTUsTracey Steele
Editor315-4472
Susan Fabozzinews assistant
Improving battlefield care
as a result of the war experience, sick or injured civilians in the United States today are transported to a trauma center by helicopter, accompanied by a critical-care flight paramedic
and a critical-care flight nurse – both highly trained and very experienced.
See baTTLeFIeLD Page 5

By.arMY.LT..J.g...BrYan.e..MiTCHeLL
Special to The Red 7
CaMP.MarMaL,.afghan-istan.— Hundreds of troops gathered Sunday, Jan. 12, in a dingy airplane hangar that had been diligently transformed into a place of mourning and solemn remembrance.
Service members from at least a dozen countries came together to pay their respects to Army 1st Class William “Kelly” Lacey, a 38-year-old Northwest Florida native, who was killed in an attack the week before.
“He died a warrior’s death, defending his Sol-diers,” Capt. David Darling said during the ceremony.
On Jan. 4, less than two weeks before he was set to return home, Lacey sprung from his bed shortly after sunrise. Insurgents had struck his outpost on the Nangarhar Province compound.
“He was the first on the scene,” Chaplain David How-ell said. “Vulnerable and ex-posed but suppressing fire.”
A car bomb had slashed through a section of the pe-rimeter wall. At least six en-emy fighters, some clad in suicide vests, were storming the base.
Lacey assumed a high position in a guard tower and is credited with killing three assailants — two wear-ing suicide vests — before a rocket-propelled grenade took his life. No other Ameri-cans were killed.
“The lives he saved are countless as he defended the camp and the Soldiers he cared about so greatly,” said 1st Sgt. Louis Steinke, who organized Sunday’s me-morial ceremony.
Lacey was born in the hos-pital at Eglin Air Force Base and raised in Niceville before he moved to Laurel Hill after
high school graduation. He joined the Army in
2003. He first distinguished himself as a paratrooper with the 82nd Airborne Division and had served three tours in Iraq and one previous tour to Afghanistan.
He was bred to wave away exhaustion like a pesky mosquito.
“In his mind, it was al-ways too early to quit. You always persevere, you find a way,” Howell said. “Danger was a familiar companion to Lacey, but he was often found smiling and ready to help anyone.”
His decorations include the Purple Heart, Bronze Star with Valor and Army Commendation Medal.
“Without question or pause, he was willing to march into hell for a heav-enly cause,” Howell said.
Lacey left behind a wife, Ashley; their 4-year-old daughter, Lily; and three old-er stepchildren in Fort Knox, Ky. He kept a small stuffed turtle in the cargo pocket of his fatigues; Lily had an iden-tical one back home.
During the ceremony, a Soldier read aloud a letter from Ashley. In it, she de-scribed Lacey as a Soldier brimming with positivity and recalled their rendezvous with fate.
Before the two were mar-ried, they were deployed together in Iraq. Ashley’s vehicle was struck by a road-side bomb and Lacey pulled her from the wreckage.
“We then developed a bond that no one can com-pare,” she wrote in the letter. “He saved my life.”
Exactly one year later, they were wed.
“I spent every day of the past five years owing my life to him and feeling so lucky to have him,” she wrote. She said the last time they spoke was a video chat a few hours before the attack. He was smiling and laughing.
During the ceremony, an American Soldier played taps and a German officer played Amazing Grace on the bagpipes. Not a lot of eyes were dry.
After the official party made their final salute, the hangar remained silent for almost an hour as troops took turns paying their respects in front of Lacey’s Fallen Sol-dier Battle Cross: at the base were his boots; his rifle stood upright, strung with his dog tags; and his helmet sat on top. Nearby was the small stuffed turtle.
As the procession wound down and with only a few mourners left in the han-gar, Steinke began carefully
packing the items away to ship them home.
Last, he held the turtle for a moment, pausing and
closing his eyes, and then placed it in the box. It would go alone to be reunited with its twin across the ocean.
Daily. news. Staff. Writer.Lauren. Sage. reinlie. contrib-uted.to.this.report..
Friday, January 17, 2014 | THE RED 7 | Page 3
6518102
10
90 1087
87
89
191
Mulat
Rd.
Avalon
Blvd
.
Woo
dbineRo
ad
NorthropBerryhill Rd.
Mun
sonHw
y.
Willard Norris Rd.
Hamilton Bridge Rd.
WhitingField
SpencerField
2
3
1
4
5
67
8
9
Pace/Milton
10
10
9090
4
85
188
85
85
OldBethe
l Rd.
Airport Rd.
Skyline Dr.
Redstone Ave.
Adams HomesMain Office
John King Rd.
P.J. Adams
Villa
crest
N. Antioch
Rd.
2
3
4
5
1
Crestview1. Thousand Oaks(850) 994-3571
2. Tiburon East(850) 995-7795
3. Berry Place(850) 995-4111
4. Ventura Estates(850) 983-3867
5. Ashley Place(850) 994-2314
6. North Hills(850) 623-0907
7. Whisper Creek(850) 623-3966
8. Twelve OaksPlantation(850) 995-7038
9. Autumn Pines(850) 995-7155
1. Alicia Place(850) 682-5132
2. Old Bethel Estates(850) 626-1961
3. Silver Creek(850) 423-0600
4. Nanterre(850) 423-0600
Pace/Milton Crestview
BuildingHomes andRelationships for 20 Years!S TA NDARD F E AT UR E S I N C L UD EQuality Construction, All Brick,Garden Tub, Finished Garage/Garage DoorOpener, 1 year BuilderWarranty,10 Year StructuralWarranty, Moen Faucetsand 50 GallonWater Heater
C LO S I N G CO S T S PA I D *Milton/Pace homes starting in the $130’sCrestview homes starting in the $160’sModel Homes OpenDaily until 6:00 pm* $1 VAMove In
*SEE SITE AGENT FOR DETAILS
BL#CBC0435186 1 4 8 O L D B A G D A D H I G H W A Y , M I L T O N , F L O R I D A • ( 8 5 0 ) 6 2 6 - 1 9 6 1
of Northwest Florida
Service members hold memorial for fallen Soldier
u.S..arMY
Soldiers pay their respects Jan. 12 at a memorial for Sgt. 1st Class William K. Lacey, who died in Afghanistan last week.

Page 4 | THE RED 7 | Friday, January 17, 2014
STaff.SgT..PeTer.J..BerarDi..| U.S. Army Reserve
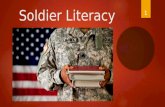
Sgt. 1st Class Thomas C. Pollard is awarded the Purple Heart by Vice Chief of Staff of the Army Gen. John F. Campbell at San Antonio Military Medical Center on Fort Sam Houston in San Antonio Jan. 3. Pollard was assigned to 3rd Battalion, 7th Spe-cial Forces Group as an engineer in Afghanistan and was injured by direct fire while performing his duties Dec. 10, 2013. Our Army appreciates the service and sacrifice he and his family continue to make in selfless service to our nation, said Campbell.
7th Group Soldier awarded Purple Heart

Friday, January 17, 2014 | THE RED 7 | Page 5
3034
260
3034071
Now Enrolling forSpring Classes
Massage Therapy & Skin CareAccepting Post 911,
Montgomery GI Bill & MyCAA
Soothing Arts HealingTherapies School of Massage
& Skincare
Visit SoothingArts.com formore information.
850-736-9931email: [email protected]
2103
664
battle made famous in the movie “Black Hawk Down.” He said those experiences had a profound impact on him and shaped his desire to become an Army doctor – which he did.
He later returned to Spe-cial Forces as a battalion surgeon and served tours in Afghanistan in 2005 and 2010.
Mabry illustrated the power of patient outcome data and how it can drive changes in military medicine – something he hopes to do with his fellowship program. His team tracked down a National Guard medevac unit from California whose members were mostly all critical-care-trained para-medics in their civilian jobs – working for the California Highway Patrol and other stateside EMS agencies. They deployed to Afghani-stan about four years ago, taking their civilian EMS model with them, he said.
“I compared their patient outcomes to the standard medevac outcomes and found a 66 percent reduc-tion in mortality using the civilian medic system,” he said. As a result of that out-come, the Army revamped its training of flight medics.
Airway treatment is another example of how patient outcome data can drive procedural changes, Mabry said.
“If you get an airway in-jury in the field, you’re usu-ally shot in the neck or in the face and have a trau-matic disruption of the air-way,” he explained. A study revealed that when medics perform a cricothyrotomy — cutting an incision in the neck so patients can breathe –they failed at that procedure about 30 percent of the time, Mabry said, not-ing that it’s a very high-risk, high-stress, yet ultimately life-saving procedure. “So armed with that data,” he said, “we went back and fig-ured out a way to make the procedure smoother and
simpler.”The result is that med-
ics now have a tool that will make them more proficient at cricothyrotomies.
“So that’s what I’m try-ing to get at — training phy-sician leaders who can look at problems or opportuni-ties for improvements in the field, who have the ability to articulate how to improve systems, give medics better training, better tools, and so to improve patient out-comes,” Mabry said. “We want doctors who can look at the data and training and protocols, and use research to solve those battlefield pre-hospital problems.”
The sort of system Mabry said he’s describing is simi-lar to what civilian EMS di-rectors do stateside.
This summer, the first fellow will graduate from the program’s two-year curriculum. “We’re one of the first EMS programs in the U.S. to be accredited, so we’re excited about that,” Mabry said. The program was accredited in October 2012.
The first year is the ci-vilian EMS fellowship, ac-credited by the American Council on Graduate Medi-cal Education and the Amer-ican Board of Emergency Medicine. During that first year, the doctors work at a big-city EMS agency, learn-ing the “system of systems” of EMS, Mabry said, using a term that refers to the over-all EMS system.
This enables them to be able to direct a military
EMS system, he explained.The second year is the
military portion, which is non-accredited. Each ser-vice has its own unique re-quirements, Mabry said. In the Army, for example, the doctor would work with the battalion medical officers at the Tactical Combat Medi-cal Care course, participate in medic training at the combat medic schoolhouse, and see how this all works at the strategic level at the In-stitute of Surgical Research and Joint Trauma System in San Antonio.
Additionally, the fellows will learn about homeland security medical proce-
dures and integrate with local, regional and national disaster planners, Mabry said. They also learn about international disaster sup-port — things such as earth-quakes and tsunamis — that the services might be called upon to support.
During the entire two-year period, the fellows are studying in the evenings for a master’s degree in public health.
Mabry described the curriculum of the program’s first fellow, who will gradu-ate in the summer. His first year was with the San Anto-nio Fire Department EMS. For his second year, he at-
tended the National Park Service Search and Rescue Course and did his public health practicum with the Joint Trauma System.
He’s now at Johns Hop-kins University attending the Health Emergencies in Large Populations Course, designed primarily for in-ternational disaster relief work. He’s working with some of the world’s leading experts in the field, Mabry added.
Then he goes to the flight surgeon course. Upon completion of his fellowship June 30, he’s projected to go to Afghanistan for six months to work in the Joint Trauma System as the pre-hospital director. His follow-on assignment will be in the Army’s Critical Care Flight Paramedic Training Pro-gram in San Antonio.
Three other fellows are going through their first year: one Air Force and two Army doctors. For next year, Mabry said, he hopes to get a Navy doctor in the fellow-ship, though the Navy cur-rently is not providing the funding. The idea is to get
three fellows a year, repre-senting each of the services, he said.
Once the physicians complete their fellowships, Mabry said, the goal is to get them in positions where their training will make a difference: division sur-geons, brigade surgeons, Special Forces group sur-geons, directors of trauma systems, training programs and so on.
While military doctors already are highly trained and motivated, Mabry said, he’s looking for those who think outside the box, see problems from unique per-spectives and perform at all levels: leadership, research, training, problem solving.
Eventually, Mabry said, he hopes to build a cadre who collaborate across the services to “shed light on that battlefield blind spot” of pre-hospital care and change the mindset from hospital-centric care to one that provides state-of-the-art care across the entire chain of survival, starting in the pre-hospital setting at the point of injury.
baTTLeFIeLD FrOM Page 2
Mabry’s own experience includes 11 years as an enlisted Soldier, starting out in the infantry and
then becoming a Special Forces medic with a tour in Mogadishu, Somalia, in 1993 during the battle made famous in the movie “Black Hawk Down.”
He said those experiences had a profound impact on him and shaped his desire to become an army
doctor – which he did.
3034
232

Page 6 | THE RED 7 | Friday, January 17, 2014
Magnolia Grillmagnoliagrillfwb.com
Tom & Peggy Rice • Proprietors850-302-0266
157 Brooks St. SE, Fort Walton Beach, FLSteaks - Seafood - Italian
2103571
3030951
IN STOCKColt AR’s, Daniels Defense AR’s
Sig Sauer 516 & 716’s,Beretta CX4 Storm
Target
DestinBridge Destin
Commons
Gulf
Shor
eDr
ive
Winn Dixie Big Kahuna’sX
Over 1,000 new and used guns in stock.Lowest Prices in the Panhandle.Military and law enforcement discounts.
WE BUY, SELL & TRADE
850-269-0450981 Hwy 98 Ste. 2 Destin, FL
In the Winn-Dixie Shopping Center
Northwest Florida’s Premier Sig Sauer Dealerwith Special Military & Police Pricing
Open Mon. - Sat. 10am - 6pm • Closed Sunday & Tuesday
LAYAWAYS AVAILABLE
• 1,000 New & Used Guns in Stock• Lowest Prices Guaranteed• Largest Selection on the Panhandle• DPMS Sportical AR-15's - $649• Daniel Defense AR-15's starting at - $1499• Ammo Back in Stock• Silencers, Suppressors& Short Barrel Rifles
WE BUYGUNS FORCASH!!!
Open Tuesday through Saturday 10am-6pm
NOW A CLASS III DEALER
3034
264
2096
211
Car, Truck & SUV Accessories
Since 1988
www.AccentTops.comAccent Tops & Trailers657 BEAL PARKWAY850-862-2400
Hard & Soft Bed CoversBed Liners & MatsToolboxes-HitchesToppers & LidsWindow VisorsStep Bars-Running Boards-Seat Covers
2102
027
TRICARE beneficia-ries soon will have to pay out of pocket for certain diagnostic genetic tests that their civilian physi-cians order, but that the Defense Health Agency doesn’t view as ap-propriate or medically necessary.
In January 2013, with-out notice to beneficiaries or to health care provid-ers, TRICARE stopped reimbursing clinical labo-ratories for more than 100 different genetic or “mo-lecular pathology” tests.
Beneficiaries haven’t complained yet because the laboratories impacted are still providing the tests that physicians order at no charge, said Julie Khani, vice presi-dent of American Clinical Laboratory Association (ACLA), which lobbies on behalf of the affected laboratories.
To date, labs have provided about $10 mil-lion worth of free tests to TRICARE users. “That’s
obviously unsus-tainable,” Khani said.
Most of these tests cost about $60 but a few carry charges of several thousand
dollars.Medical science has
seen an explosion of clini-cal tests designed to diag-nosis and treat ailments based on a patient’s DNA. With thousands of new tests added annu-ally, driven by demand for personalized medicine, the Food and Drug Ad-ministration is weighing the need to regulate the industry.
One of the more rou-tine genetic tests that TRICARE no longer cov-ers is used to determine if a woman who is pregnant carries a marker for cys-tic fibrosis, which would increase chances of the
baby having the disease.If the woman has the
marker, the father usu-ally also is tested because both parents must have the CF gene for the fetus to be at risk. If both par-ents are found to have it, the likelihood of their baby having CF is one in four, according to the Cys-tic Fibrosis Foundation
With this test no longer covered, “TRICARE ben-eficiaries will not receive the standard of care or benefits equal to other insured patients,” Khani said. The American Con-gress of Obstetricians and Gynecologists has recom-mended prenatal testing for CF for more than a decade, she said.
“It’s covered by Medic-aid and other commercial health plans. It is also the standard of care under VA-DOD clinical practice guidelines for manage-ment of pregnancy,” Khani said. “Clearly, an important test.”
The Defense Health
Agency disagrees. Al-though no official was made available to be interviewed, DHA gave written responses to our questions. In one, it dis-missed the significance of the prenatal CF testing.
“Awareness that a fe-tus is at increased risk of having CF, in and of itself, does not usually change the management of labor, delivery and the neona-tal period,” wrote DHA officials.
Also, they noted, in-fants at birth are tested for a host of health condi-tions, including CF, and those tests continue to be covered by TRICARE.
In July, DHA did re-move the CF test from its “no government pay” list, but DHA has continued to refuse to reimburse labo-ratories such tests.
Reps. Tom Marino and James P. McGovern, co-chairs of the Congres-sional Cystic Fibrosis Caucus, urged Lt. Gen. Douglas J. Robb, director
of DHA, in a letter signed Monday to reconsider the decision not to cover prenatal CF testing, argu-ing that “patient care will suffer.”
What drove the deci-sion by TRICARE last January to stop reimburs-ing for many genetic or laboratory-developed tests (Lets) was the American Medical Asso-ciation’s publication of new Current Procedural Terminology (CPT) codes for laboratory tests. The codes gave greater trans-parency to how TRICARE was being billed, DHA said. It could “identify specific laboratory devel-oped tests that 1) have not been approved or cleared by the Food and Drug Administration and/or 2) failed to meet TRICARE criteria for coverage.”
For example, DHA said, “demand genetic testing that is not medi-cally necessary or does not assist in medical man-agement of the patient” is not reimbursable. Also, DHA emphasized that TRICARE cannot cover any laboratory developed test that has not been ap-proved by the FDA.
The ACLA criticizes
DHA on this point, argu-ing that TRICARE does cover many other labora-tory-developed tests not FDA approved, including pap smears, a routine test for cervical cancer.
The DHA “has a flawed interpretation of its own policy” which “places TRICARE out of step with other government and commercial payers, and it impacts the patient,” said Khani. “We are deeply concerned that TRICARE beneficiaries will be de-nied vital services that are critical to the diagno-sis and treatment of dis-ease. And these are tests TRICARE has covered historically.”
If TRICARE doesn’t be-gin soon to pay for these tests, doctors won’t stop ordering them but labora-tories will have no choice but to charge patients for their cost, Khani said.
The Military Coalition, an umbrella group of mili-tary associations and vet-erans groups, recognizes that laboratory profits and some very complex medical questions are en-twined in this debate be-tween DHA and industry.
Some lab fees soon will be billed to TRICaRE patients
See TrIcare Page 7
Tom Philpott

Friday, January 17, 2014 | THE RED 7 | Page 7
111550
6Stop by or call
502 “W” D Avenue, Ste 100, Eglin AFB850-882-1321 • military.umuc.edu/eglinsupport
Recognized as a 2014 Military Friendly School™
by G.I. Jobs and Military Advanced Education
AT YOUR SERVICE SINCE 1947
THE EDUCATION YOU WANT.THE SUPPORT YOU DESERVE.
You’ll find University of Maryland University College (UMUC)online and on-site right here at Eglin AFB, along with ourNational Testing Center. We stand ready to help you pursueyour degree and advance your career in cybersecurity,business and management, public safety and otherin-demand fields.
In person or online, UMUC representatives can help you
•Make the most of your military benefits.
• Determine whether your military experience equalsacademic credit.
•Map out your path to degree completion.
• Apply for admission and register.
But one clear concern for beneficiary advocates, said Kathy Beasley, co-chair of the coalition’s health subcommittee, is that DHA has created two standards of care regard-ing molecular pathology tests. Patients who use civilian providers will have to pay for these tests, while patients at military clinics and hos-pitals won’t. Providers in the direct care system can continue to order such tests knowing the military will pay for them.
“TRICARE benefi-ciaries without access to military treatment
facilities are relegated to second-class health care. This is troubling,” Beas-ley said.
DHA acknowledges this disparity in access to laboratory services between purchased care and direct care. Officials explained that a single contract is in effect that allows Army, Navy and Air Force providers to request lab services if military facilities can-not perform the tests in house.
“As this is not a DHA contract, we are in the process of gathering data regarding the tests being
ordered by MTF provid-ers and will examine any changes that need to be made to the contract,” DHA said. “Lab testing, whether ordered in the private sector or by MTF providers, needs to be safe and effective.”
But DHA said differ-ences in lab test cover-age might survive any such review because purchased care has more restrictive laws and regulations.
.Send.comments.to.Military.update,.P.O..Box.231111,.Centreville,.va,.20120,[email protected].
TrIcare FrOM Page 6
from.staff.reports
Settlement of estate
Anyone having any claims on or obligations to the estate of SSG Vazquez, Richard L. of B Company, 3rd Battalion, 7th Special Forces Group (Airborne), should contact the summa-ry-court officer CW2 De Je-sus, Carlos at 850-885-2855.
DeerS/ID office closed for training
The Eglin DEERS/ID of-fice will be closed for train-ing on Jan. 22. They will be back to normal business hours on Jan. 23.
Hurlburt Field is avail-able for expired ID cards and urgent DEERS up-dates. Their MPS customer service number is 884-2657. To avoid long wait times, ID card appointments can be made at https://rapids-ap-pointments.dmdc.osd.mil.
Scholarships for Military children Applications for the 2014
Scholarships for Military
Children Program became available Dec. 3 at com-missaries worldwide or on the Internet at http://www.militaryscholar.org. Applica-tions must be turned in to a commissary by close of business Feb. 28. Packages must be hand-delivered or mailed. The packages may not be emailed or faxed. This year’s award amount has risen to $2,000, and the program awards at least one scholarship at each commissary with quali-fied applicants. Applicants should ensure that they and their sponsor are enrolled in the Defense Enrollment Eligibility Reporting Sys-tem database and have a military ID card. For more information, students or sponsors should call schol-arship managers at 856-616-9311 or email them at [email protected].
New bible StudyThe Eglin Protestant
Women of the Chapel will begin a new Bible study at 6 p.m. every Tuesday, be-ginning Jan. 14 at the Eglin Chapel Center. For infor-mation, call Toni Scott at 240-4626.
Parent/ Teen DinnerA parent teen dinner on
internet safety will be held at 5 p.m. Feb. 10 at the Eglin Youth Center. The event is free and open to any parent of a child in fifth grade and older. The Okaloosa County Sheriff ’s Office will be lead-ing separate discussions for parents and teens on top-ics such as online predators and cyber bullying. Come see how to keep your teen safe online and enjoy a free dinner provided by the Youth Program. Reserve your spot now by calling Family Advo-cacy at 883-8149.
antique Show tickets for Fisher House Tickets are currently
available for the 52nd an-nual Antique Show and Sale to be held at the NW Florida Fairgrounds on Jan. 24-26. Purchase your tickets for $4 each through Fisher House of the Emerald Coast and save a $1 off the regular ad-mission. For information, including purchasing tick-ets, contact Kim Henderson at [email protected] or call (850) 259-4956.
RED 7 BRiEfs

Page 8 | THE RED 7 | Friday, January 17, 2014
2101912
212 Hollywood Blvd SW • Fort Walton Beach, FL 32548850-664-7000
www.PrestonHood.com*Sale price plus tax, title, license and dealer fee. Sale prices includes all factory incentives/ rebates and dealer savings, Silverado sale price includes trade-in and V-6 bonus cash (Must purchase a vehicle with V6 engine and trade in a1999 or newer vehicle to qualify.) Subject to prior sale.**Lease payment based 36 month lease, 12,000 miles per year, $2,869 total due at signing includes $2,670 cash down $199 first months payment and $0 security deposit, withapproved credit thru Ally Bank, plus tax, license and dealer fee. Residual Value $14,888.65 ^ Financing on select vehicles for limited terms with approved credit. Not available with leases and some other offers. Some customers may
not qualify. Tax, title, license, dealer fees and optional equipment extra. Expires 2/1/2014. See dealer for complete details. #13-153321
PRESTON HOOD CHEVROLET
0% For 60 monthFinancing available^
get our lowest livemarket Price on Your
new chevY todaY!
all-new 2014 chevY silverado double cablive market Price
$25,993*STARTING AT
all new 14 20 chevY chevY chev adoversil
0% APR foR 36 months on All Gm CeRtified Used VehiCles
GM Certified Pre Owned and Quality used Cars fOr all BudGets!YEAR MAKE MODEL STOCK PRICE YEAR MAKE MODEL STOCK PRICEYEAR/MAKE/MODEL.............................StK # .......... PRicE2000 chEvROLEt vEntuRE .......... P13187A .........$2,9951998 chEvROLEt cAMARO .............. 13715c .........$3,2252001 POntiAc SunfiRE SE .............. 14201B ........ $3,9951999 niSSAn QuESt SE ................. P13202A ........ $3,9952001 chEvY SiLvERADO 1500......... 14285A .........$4,9952000 chEvROLEt iMPALA................. 14177A ........ $5,9952006 niSSAn ALtiMA SE-R ...............14234E ........ $5,9952002 SAtuRn LS.................................14342A ........ $5,9952002 chEvY SiLvERADO 1500 ........ 13472A ........ $5,9982000 GMc YuKOn SLE ....................t14418c ........ $6,995
1998 chEvROLEt c/K 1500 .............14201c ........ $6,9952008 POntiAc GRAnD PRix ............13680B .........$7,9952007 POntiAc G6...............................14424B ........ $8,9952009 chEvROLEt hhR Lt ............... 14309A .......$10,9952007 tOYOtA AvALOn.....................t14431B .......$10,9952004 DODGE RAM 1500...................t14210A .......$10,9952004 niSSAn 350Z tOuRinG...........13482A ....... $11,9952009 POntiAc G6 ............................P13156A .......$12,9952008 niSSAn titAn SE...................142595D .......$12,9952007 tOYOtA cAMRY.........................14319n .......$12,9952013 chEvROLEt SPARK .................. P13176 .......$13,995
new 2014 chevrolet sonic ltThe #1 Selling Small Car On The gulf COaST!
live market Price
$15,987*STARTING AT
new 2014 chevY eQuinoX
all new 14 20 chevY chevY chev
new 14 20 chevlive market Price
$23,489*STARTING AT
$199/mo.**
WaSHingTOn. (Army News Service) — The En-listed Voluntary Early Sepa-ration Program and Enlisted Involuntary Early Separa-tion Program have some im-portant changes that took effect Jan. 1.
vOLunTarY.SeParaTiOnThe Enlisted Voluntary
Early Separation Program is designed for Soldiers who have employment offers and want to separate prior to the expiration of their term of service, or ETS. They can now request getting out up to 180 days prior to their ETS.
Soldiers can request the separation through their local commanders, if they can show adequate salary or compensation from their potential civilian employers, and that the separation won’t hurt their ability to support their families, said James R. Bragg, branch chief for Retention and Reclassifica-tion - Involuntary/Voluntary Separation program, Hu-man Resources Command, at Fort Knox, Ky.
Bragg added that of that 180-day maximum period, the Soldier would need a minimum of 90 days for nor-mal transition/separation processing.
The previous voluntary separation policy was for Soldiers planning to attend college. That policy allows them to separate up to 90 days early, so they can begin their semester work, Bragg said. That policy remains in effect. Nothing has changed with that policy.
The new policy allowing for early separation for a job opportunity can be “good for the Soldiers and their families” as they transition, Bragg said.
Further details of the changes can be found in All Army Activity message 340/2013.
invOLunTarY.SeParaTiOn
The Enlisted Involuntary Early Separation Program has been in effect for some time for Soldiers whose units are deploying and their ETS date is during that deployment.
In those cases, Soldiers would be offered the chance to re-enlist, extend or choose a different unit or military occupational specialty, said Bragg. If they didn’t, they would be involuntarily sepa-rated up to one year before their ETS. That remains in effect.
The big change is that besides deploying units, the policy now also covers units that are going to be deacti-vated, he said.
For Soldiers in units that will be deactivating, they’ll be given 45 days to extend or re-enlist from the time they’re notified, Bragg continued. If the Soldier chooses not to ex-tend or re-enlist, the Soldier’s ETS would be reduced up to a year’s time — depending on the date his or her unit is deactivating — but not less than 90 days for the transi-tion/separation processing.
The policy would not apply to units that are deactivating but are then reactivating as a different unit, at the same location. In that case, the Sol-diers would remain with their unit until their ETS dates, he added.
Although no Soldier has yet been affected by the change, Bragg said he ex-pects there will be involun-tary separations for those in units deactivating as the drawdown continues.
“We always give the Sol-dier the opportunity to stay with the team first,” he added.
The policy for involun-tary early separations can be found in All Army Activity message 339/2013 and Mili-tary Personnel 13-375.
Whether nor not Soldiers choose the voluntary separa-tion route or the involuntary, they are afforded, as always, the opportunity to speak with a reserve-component career counselor for possible offer-ings in the National Guard or Army Reserve, said Col. Charles A Slaney, program manager for reserve com-ponent career counselors, HRC.
u.S..arMY.PHOTO.iLLuSTraTiOn
The Enlisted Voluntary Early Separation Program and Enlisted Involuntary Early Separation Program have some important changes that took effect Jan. 1.
Changes to enlisted separation policy aim to provide Soldiers options