
3.the cost effectiveness & real world impact of quadrivalent
37
The Cost Effectiveness & The Cost Effectiveness & Real World Impact of Real World Impact of Quadrivalent HPV vaccine Quadrivalent HPV vaccine Endy M. Moegni KOGI XV Bali Nusa Dua Convention Center 29 Juni- 5 Juli 2012
-
Upload
tofik-apik -
Category
Health & Medicine
-
view
370 -
download
2
Transcript of 3.the cost effectiveness & real world impact of quadrivalent

The Cost Effectiveness & The Cost Effectiveness & Real World Impact of Real World Impact of
Quadrivalent HPV vaccineQuadrivalent HPV vaccine
Endy M. Moegni
KOGI XV
Bali Nusa Dua Convention Center
29 Juni- 5 Juli 2012

Quadrivalent HPV VaccineQuadrivalent HPV Vaccine((4 in 14 in 1 HPV vaccine) HPV vaccine)
Diphtheria antitoxin discovered
1895
Pneumococcal (14-valent polysaccharide)*
1977
Measles, mumps, rubella (MMR)*
1971
Measles (live attenuated virus)*
1968
Mumps*
1967
Measles (live)*
1963
Rotavirus*
2006
Zoster (live)*
2006
Human Papillomavirus*
2006
Measles, mumps, rubella virus vaccine live (new rubella strain: RA 27/3)*
1978
Hepatitis A (inactivated)*
1996
Haemophilus influenzae type b (conjugated)*
1989
Measles, mumps, rubella, varicella*
2005
Haemophilus influenzae type b / Hepatitis B*
1996
Haemophilus influenzae type b (liquid)*
1996
Varicella (chicken pox) virus*
1995
Hepatitis B (recombinant)*
1986
Pneumococcal (23-valent polysaccharide)*
1983
Hepatitis B (plasma derived)*
1981
The First Cancer Vaccineof the World
Tam Kar Fai

Cervical Cancer Is Essentially Caused Cervical Cancer Is Essentially Caused by Oncogenic HPVby Oncogenic HPV
HPV is a main cause of cervical cancer
Analysis of 932 specimens from women in 22 countries indicated prevalence of HPV DNA in cervical cancers worldwide = 99.7%.
1. Muñoz N, Bosch FX, de Sanjosé, et al. N Engl J Med. 2003;348:518–527. 2. Walboomers JM, Jacobs MV, Manos MM, et al. J Pathol. 1999;189:12–19.
HPV and Anogenital WartsHPV and Anogenital Warts
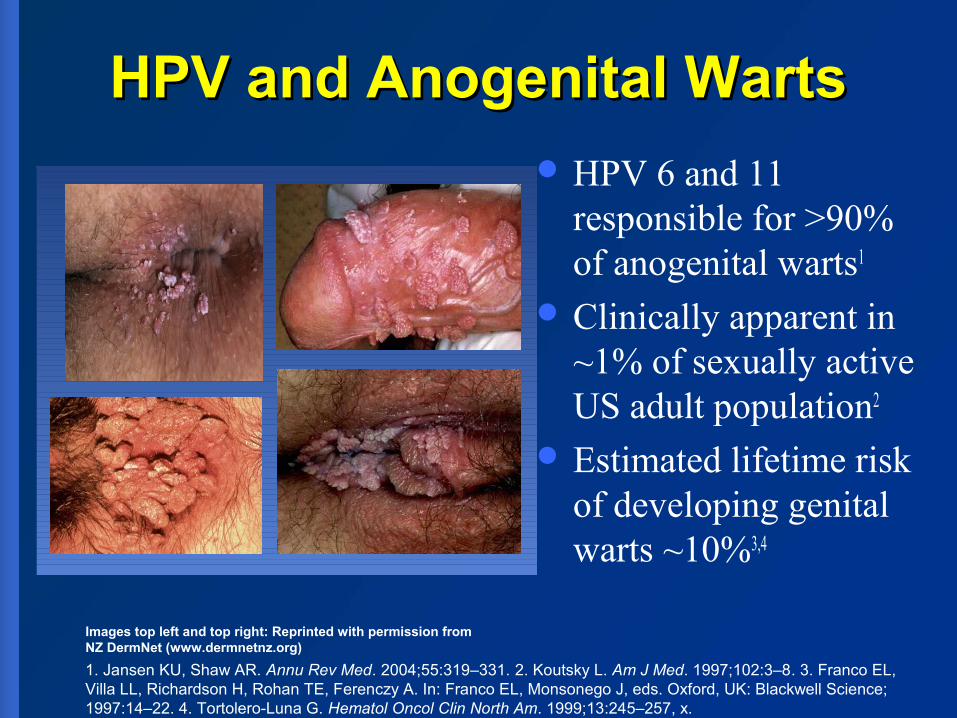
HPV 6 and 11 responsible for >90% of anogenital warts1
Clinically apparent in ~1% of sexually active US adult population2
Estimated lifetime risk of developing genital warts ~10%3,4
1. Jansen KU, Shaw AR. Annu Rev Med. 2004;55:319–331. 2. Koutsky L. Am J Med. 1997;102:3–8. 3. Franco EL, Villa LL, Richardson H, Rohan TE, Ferenczy A. In: Franco EL, Monsonego J, eds. Oxford, UK: Blackwell Science; 1997:14–22. 4. Tortolero-Luna G. Hematol Oncol Clin North Am. 1999;13:245–257, x.
Images top left and top right: Reprinted with permission fromNZ DermNet (www.dermnetnz.org)
Vaginal Intraepithelial Neoplasia Vaginal Intraepithelial Neoplasia (VaIN(VaIN))
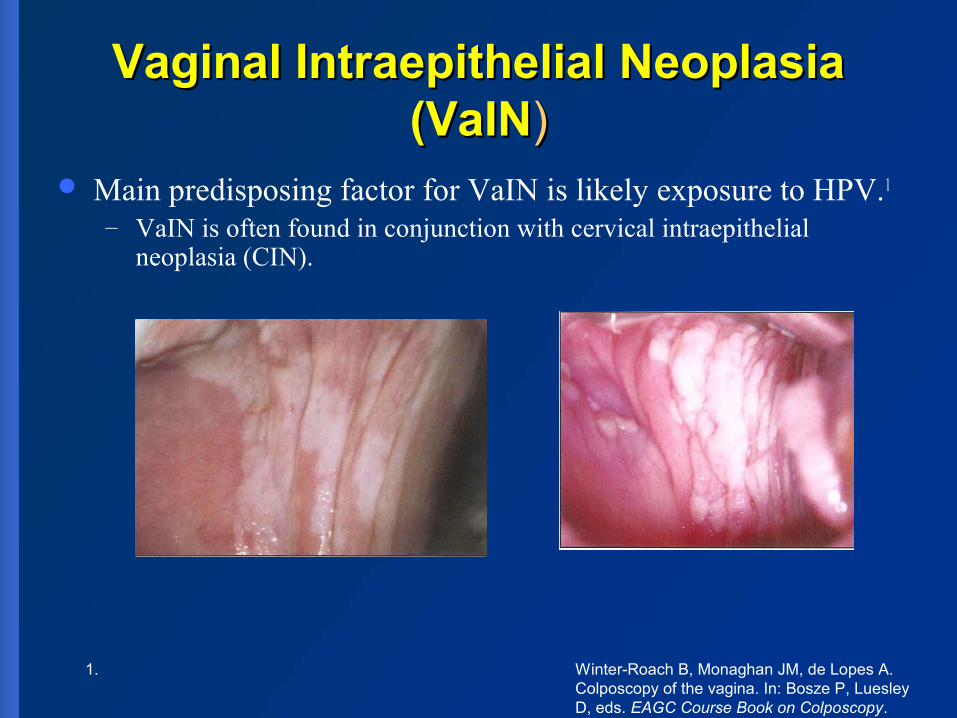
Main predisposing factor for VaIN is likely exposure to HPV.1
– VaIN is often found in conjunction with cervical intraepithelial neoplasia (CIN).
1. Winter-Roach B, Monaghan JM, de Lopes A. Colposcopy of the vagina. In: Bosze P, Luesley D, eds. EAGC Course Book on Colposcopy. Budapest: Primed-X Press; 2004:120–123.

Vulval Intraepithelial Neoplasia Vulval Intraepithelial Neoplasia (VIN)(VIN)
HPV 16 appears to be the dominant HPV type associated with high-grade VIN (up to 81% in VIN 3)3
– Majority of VIN 1 cases are associated with HPV types 6 and 113
– HPV 6, 11, 16, or 18 can be found in VIN 2 or 34
Photo courtesy of Dr. J. Monsonego
Photos courtesy of Dr. E.J. Mayeaux
. 3. Buscema J, Naghashfar Z, Sawada E, et al. Obstet Gynecol. 1988;71:601–606. 4. Koutsky L. Am J Med. 1997;102:3–8..

VaIN and VIN are of concern because they are considered as precancerous lesions with about 40 - 50% associated with HPV infection
In UK, vulval cancer is 6 times and vaginal cancer 20 times less common than cervical cancer1
No screening programme exists
1. 1. Gonzalez Inchaurraga MA et al. HPV and carcinogenesis. Acta Dermatovenerol. 2002;1:1-8.Gonzalez Inchaurraga MA et al. HPV and carcinogenesis. Acta Dermatovenerol. 2002;1:1-8.2. Parkins DM et al. International Agency for Research on Cancer, 2002;8.2. Parkins DM et al. International Agency for Research on Cancer, 2002;8.

Phylogenetic Tree of HPV FamilyPhylogenetic Tree of HPV Family
HPV 16 Related
HPV18 Related

Infection From Time of First Sexual Intercourse
0.0
0.2
0.4
0.6
0.8
1.0
04
81
21
62
02
42
83
23
64
04
44
85
25
6
Mo
nth
s S
ince
Fir
st In
terc
ou
rse
Cumulative Incidence of HPV Infection
From Winer RL, Lee S-K, Hughes JP, Adam DE, Kiviat NB, Koutsky LA. Genital human papillomavirus infection: Incidence and risk factors in a cohort of female university students. Am J Epidemiol. 2003;157:218–226, by permission of Oxford University Press.
Study of female college students (N=603)

Treatment of HPV Infection

GARDASIL is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA.*VLP = Virus-like particle. 1. Villa LL, Costa RL, Petta CA, et al. Lancet Oncol. 2005;6:271–278.
Quadrivalent HPV L1 VLP VaccineQuadrivalent HPV L1 VLP Vaccine11
Quadrivalent HPV L1 VLP vaccine– (Types 6, 11, 16, 18)
VLPs manufactured in:– Yeast– Recombinant VLPs (empty shell protein L1)– Do not contain Virus DNA (not infectious)
Amorphous Aluminum Hydroxyphosphate Sulfate Adjuvant (225 μg per dose)
No Mercury preservative (thimerosal) Storage: 2 to 8 OC

Dosage & AdministrationDosage & Administration
3 doses within 6 months– (0, 2, 6 months)
0.5 mL volume IM injection Package:
– Prefilled syringe– Shake well before use
Injection Site:– Upper arm (Deltoid region)– Thigh (higher anterolateral area)

3
North America:
USACanada Mexico
9
South America:Brazil BoliviaArgentina UruguayPeru EcuadorColombia ChileParaguay
35
Middle East & Africa:
Gabon NamibiaIsrael C.A.R.Morocco MauritiusKenya KuwaitMauritania UAE Guinea Eq. EthiopiaUganda TogoMalawi Congo BrazzavilleJordan EgyptCote d’Ivoire Burkina FasoChad Bahrain Botswana Lebanon Tanzania ZambiaSouth Africa Cameroon NigeriaPakistan Tunisia MaliGuinea Conakry Saudi Arabia Rwanda
22
Asia Pacific & Japan:KyrgyzstanUzbekistanKazakhstanAustraliaIndonesia KoreaTaiwanHong KongSingaporeNew ZealandMacauMalaysiaPhilippinesThailandIndiaVietnamFijiBhutanGeorgiaJAPANSri LankaBrunei
42
Europe:
Germany Cyprus Ireland France Czech Republic LatviaUK Denmark LithuaniaSpain Estonia LuxembourgItaly Finland MaltaAustria Greece NetherlandsBelgium Hungary NorwayBulgaria Iceland PolandPortugal Romania SlovakiaSlovenia Sweden SerbiaMontenegro Switzerland LiechtensteinBosnia Russia BelarusCroatia Turkey UkraineHerzogovina Macedonia Albania
Caribbean & Central America:
Costa Rica Trinidad/TobagoPuerto Rico El SalvadorGuatemala HondurasCuraçao NicaraguaBermuda PanamaBahamas Cayman IslandsBarbados ArubaJamaica Dominican Republic
16
Gardasil / Silgard ApprovalsGARDASIL approved in 127 countries (includes 24 GAVI-eligible)
GAVI – Eligible Registration Approvals (24): Burkina Faso, Cameroon, Central African Republic, Chad, Congo (DR), Cote d’Ivoire, Ethiopia, Guinea (Conakry), India, Kenya, Kyrgyzstan, Malawi, Mali, Mauritania, Nicaragua, Nigeria, Pakistan, Rwanda, Tanzania, Togo, Uganda, Uzbekistan, Vietnam, Zambia
as of 8 June 2012

HPV Recommendations by National Expert Advisory Bodies on Immunization: 40 Countries
National Funding by 38 Countries
Update: June 8, 2012
Cayman Is.
3North America
USA Canada Mexico
3South AmericaArgentina PeruGuyana
3Middle East & Africa
KuwaitUAELesotho
6Asia PacificAustraliaNew ZealandMalaysiaIndiaSingaporeJapan
23EuropeAustriaBelgiumBulgariaCzech RepublicDenmarkFranceGermanyGreeceIcelandIrelandItalyLatviaLuxemburgMacedoniaNetherlandsNorwayPortugalRomaniaSloveniaSpainSwedenSwitzerlandUnited Kingdom
Caribbean & Central America
Puerto Rico Panama
2
FUNDING
GARDASIL only
Bivalent Only
Both vaccines
No funding

HPV Vaccine: National Immunization Program
Eleven European countries (Germany, France, Italy, Belgium, Austria, Norway, Sweden, Greece, Denmark, Luxemburg and Switzerland), as well as the United States, Canada, Australia and UK have already reviewed the positive public health impact and recommended the quadrivalent HPV vaccine for universal human papillomavirus vaccination with accelerated reviews.
15 countries15 countries

Sustained clinical efficacy Sustained clinical efficacy and antibody titer and antibody titer for for at leastat least 5 years 5 years
10 000
1 000
100
10
GMT (mMU/mL)
GARDASIL
Natural infection
0 7 12 18 24 30 36 54 60months
GARDASIL 100%
1st 2nd 3rd
Dose
Clinical efficacy
* N
eutr
alis
i ng
antib
o die
s(H
PV ty
pe 1
6)
185 years
* against infection, CIN (Cervical intraepithelial neoplasia) and genital warts due toHPV types 6,11,18; 5 yrs follow up (after dose 1) of a subset (241 women, vaccine& placebo) from a phase II efficacy study
Villa L High Sust Eff Proph Quad HPV Vacc 5 Year Followup Br J Can 2006 95 1459
1. C. Fraser et al. / Vaccine 25 (2007) 4324–4333
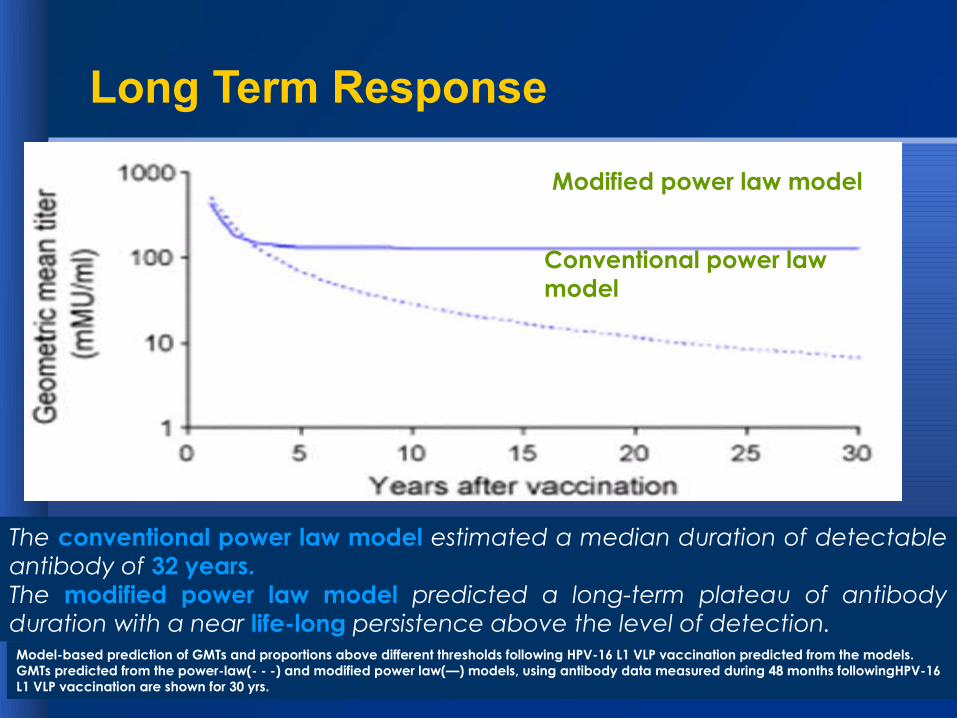
Model-based prediction of GMTs and proportions above different thresholds following HPV-16 L1 VLP vaccination predicted from the models. GMTs predicted from the power-law(- - -) and modified power law(—) models, using antibody data measured during 48 months followingHPV-16 L1 VLP vaccination are shown for 30 yrs.
Modified power law model
Conventional power law model
The conventional power law model estimated a median duration of detectable antibody of 32 years.The modified power law model predicted a long-term plateau of antibody duration with a near life-long persistence above the level of detection.
Long Term Response

CDC 2010 Mar – Gardasil Q&A for public
Accessed 10 Jul 2010http://www.cdc.gov/vaccines/pubs/vis/downloads/vis-hpv-gardasil.pdf

Australia Free National Australia Free National HPV vaccination ProgramHPV vaccination Program
Malaysia Free National Malaysia Free National HPV vaccination ProgramHPV vaccination Program
The near disappearance of genital warts in young women 4 years after
commencing a national human papillomavirus (HPV) vaccination
programme
Tim R H Read,1 Jane S Hocking,2 Marcus Y Chen,1 Basil Donovan,3Catriona S Bradshaw,4 Christopher K Fairley1

• From July 2004 to June 2011,• 52 454 new patients were seen at Melbourne
Sexual Health Centre and 5021 (9.6%, 95% CI 9.3% to 9.8%) were diagnosed with GW.
• From July 2004 to June 2007, the proportions with GW either increased or did not change in all groups.
Tim R H Read,1 Jane S Hocking,2 Marcus Y Chen,1 Basil Donovan,3Catriona S Bradshaw,4 Christopher K Fairley1

Results

• The two 12-month periods of 2007/2008 and 2010/2011, GW declined in women under 21 years from 18.6% to 1.9% and in heterosexual men under 21 years from 22.9% to 2.9%.
• There was no significant change in GW in women $30 years (OR 0.97, 95% CI 0.84 to 1.12), heterosexual men $30 years (OR 0.97, 95% CI 0.89 to 1.06) or in homosexual men (OR 0.95, 95% CI 0.85 to 1.07).
Tim R H Read,1 Jane S Hocking,2 Marcus Y Chen,1 Basil Donovan,3Catriona S Bradshaw,4 Christopher K Fairley1

Conclusions
• The dramatic decline and near disappearance of GW in women and men under 21 years of age, 4 years after commencing this programme, suggest that the basic reproductive rate has fallen below one.

Comparative Cost-Effectiveness of Comparative Cost-Effectiveness of HPV Vaccines in the Prevention of HPV Vaccines in the Prevention of Cervical Cancer in MalaysiaCervical Cancer in Malaysia
• Cost effectivenes options were compared for three programs i.e. screening via Pap smear; modeling of HPV vaccination (QV and BV) and combined strategy (screening plus vaccination).
Sharifa WP Ezat1*, Syed Aljunid2

MethodsMethods
For this cross sectional study in 2006-2009 respondents were interviewed from six public Gynecology-Oncology hospitals. (502 cervical cancer patients participated).
Methods included expert panel discussions to estimate treatment costs by severity and direct interviews with respondents using costing and quality of life questionnaires.
Sharifa WP Ezat 1*, Syed Aljunid2

Results A total of 502 cervical cancer patients participated with a mean age at 53.3±11.2
years and a mean marriage length of 27.7±12.1 years, Malays accounting for 44.2%.
Cost/quality adjusted life year (QALY) for Pap smear
Cost/quality adjusted life year (QALY) for strategy with HPV vaccination only
Cost/quality adjusted life year (QALY) for strategy with combined strategy (screening + HPV vaccination)
1 Malaysian Ringgit = Rp 2,950 Ezat et al. 2011. Asian Pacific J Cancer Prev, 11, 1-6

ResultsResults((Incremental Cost Effectiveness Ratio (ICER)Incremental Cost Effectiveness Ratio (ICER)))

ConclusionsConclusions
QV is more cost effective than BV. The QV combined strategy was more
cost effective than any method except Pap smear screening with high population coverage.
Sharifa WP Ezat 1*, Syed Aljunid2

Comparing Bivalent and Quadrivalent Human Papillomavirus Comparing Bivalent and Quadrivalent Human Papillomavirus Vaccines: Economic Evaluation Based on Transmission Vaccines: Economic Evaluation Based on Transmission
ModelModelAuthor: Jit et alAuthor: Jit et al

ResultsResults Effect on disease:
– Use of either vaccine is expected to substantially decrease the incidence of HPV related cancers regardless of which scenario is assumed
– By 2109, HPV vaccine may prevent:
– Use of the qHPV is expected to decrease the incidence of vaccine type warts and recurrent respiratory papillomatoses by up to 95% if duration of protection is lifelong.
Cervical cancer cases reduction
vulval, vaginal,and anal cancers cases reduction
QHPV 700 (630–800) to1000 (940–1100)
430 (380–490) to630 (950–670)
BHPV 730 (650–830) to1100 (990–1200)
Jit et al. 2011. BMJ 2011;343:d5775

Conclusions
• The quadrivalent vaccine may have an advantage over the bivalent vaccine in reducing healthcare costs and QALYs lost.

UK switched to QV from Sept 2012
United Kingdom (UK) Department of Health announced that from next September 2012, UK will use QV for HPV vaccination program in UK
QV protects against the two types of HPV virus that cause more than 70 percent of cervical cancer in England and two types of HPV virus that cause 90 percent of genital warts.

Eradication of Cervical Cancer and Eradication of Cervical Cancer and HPV Related DiseasesHPV Related DiseasesNot a Dream AnymoreNot a Dream Anymore……


References
• Donovan et al. 2010. Quadrivalent human papillomavirus vaccination and trends in genital warts in Australia: analysis of national sentinel surveillance data. DOI:10.1016/S1473-3099(10)70225-5
• Read et al. The near disappearance of genital warts in young women 4 years after commencing a national human papillomavirus (HPV) vaccination programme. Sex Transm Infect. doi:10.1136/sextrans-2011-050234
• Ezat et al. 2011. Comparative Cost-Effectiveness of HPV Vaccines in the Prevention of Cervical Cancer in Malaysia. Asian Pacific J Cancer Prev, 11, 1-6.
• Jit et al, Comparing bivalent and quadrivalent human papillomavirus vaccines: economic evaluation based on transmission model BMJ 2011;343:d5775


















