32. Grief and Mourning
7
3 2 GRIEF AND MOURNING Stephen R . Shuchter M.D., and Sidney Zisook, M.D All psychiatrists encounter patients who have experienced the death of a loved one. Such losses often are quite traumatic and painful and can precipitate both psychological and medical sequelae which may require intervention. Appreciating the effects o death on survivors can be a crucial ele- ment in assessing t he putient. 1. What is grief? Grief comprises the myriad psychological, physiologic, and behavioral responses which accom- pany the human awareness of an irrevocable loss such as a pending or actual loss of a close friend or relative. It is an extraordinarily powerful emotion. Manifestations o Normal Grief Psychological Physiologic Numbness or dissociation Sense of loss Anguish Insomnia Yearning Agitation Autonomic discharge: gastrointestinal, cardiovascu lar, respiratory, neuromuscular Anger Guilt Apathy Anxiety and fear Intrusive images Cognitive disorganization Distractibility Hallucinatory experiences Regression Anorexia 2 Wha t are the psychological aftereffects? The psychological sequelae may include experiences of intense anguish and emotional pain ac- companied by crying, feelings of loss, and yearning for the one who has died; feelings of anger or guilt; transient periods of numbness, shock, or disbelief, when the loss does not register emotionally; a sense of apathy or lack of direction; anxiety and fearfulness; intrusion of painful images and mem- ories, especially if the nature or course of death was traumatic to the survivor; and cognitive disorga- nization. Behaviorally, survivors frequently search for evidence that their loved one is still alive. They may experience multiple sensory hallucinations of the deceased, most often i n the form of sensing their presence but also including auditory, visual, haptic, and olfactory hallucinations. Many grieving persons attempt to isolate themselves from social contacts, which are too painful because of the memories they evoke. They may avoid discussing their loss or even confronting mun- dane experiences of life or possessions of the deceased which can trigger their anguish. The aggre- gation of these powerful emotional and cognitive forces often leads to a regression: an emotional state in which the grieving person feels overwhelmed, out of control, helpless, and child-like in heightened dependency. 3. What forms of physiol ogic respons es are common? Physiologic responses occur frequently, often in reaction to reminders of the loss. They take the form of sudden autonomic discharge with acute symptoms reflecting the pangs of grief: chest pain 160
Transcript of 32. Grief and Mourning
8/12/2019 32. Grief and Mourning
http://slidepdf.com/reader/full/32-grief-and-mourning 1/6
32 GRIEF A N D MOURNINGStephen R. S h u c h t e r M.D., and Sidney Zisook, M.D
All psychiatrists encounter patients who have experienced the death of a loved one. Such lossesoften are quite traumatic and painful and can precipitate both psychological and medical sequelaewhich may require intervention. Appreciating the effects o death on survivors can be a crucial ele-ment in assessing the putient.
1. What is grief?Grief comprises the myriad psychological, physiologic, and behavioral responses which accom-
pany the human awareness of an irrevocableloss such as a pending or actualloss of a close friend or
relative. It is an extraordinarily powerful emotion.Manifestations o Normal Grief
Psychological PhysiologicNum bness or dissociationSense of loss
Anguish InsomniaYearning Agitation
Autonomic discharge: gastrointestinal,cardiovascu lar, respiratory, neuromuscular
AngerGuiltApathy
Anxiety and fearIntrusive imagesCognitive disorganizationDistractibilityHallucinatory experiencesRegression
Anorexia
2 What are the psychological aftereffects?The psychological se quelae may include experiences of intense anguish and em otional pain ac-
companied by crying, feelings ofloss, and yearning for the one who has died; feelings of anger or
guilt; transient periods of numbness, shock, or disbelief, when theloss does not register emotionally;a sense of apathy or lack of direction; anxiety and fearfulnes s; intrusion of painful im ages and m em-ories, especially if the nature o r courseof death was traumaticto the survivor; and cognitive disorga-nization. Behaviorally, survivors frequently search for evidence that their loved oneis still alive.They may exp erience multiple sensory hallucinations of the d eceased,most often in the for m ofsensing their presence but also including auditory, visual, haptic, and olfactory hallucinations.
Many grieving persons attempt to isolate themselves from social contacts, which are too painfulbecause of the mem ories they evoke. They may avoid discussing theirloss or even confronting m un-dane experiences of life or possessions of the deceased which can trigger their anguish. The agg re-gation of these powerful emotional and cognitive forces often leads to aregression: an emotionalstate in which the grieving person feels overwhelm ed, out of control, helpless, and child-like inheightened dependency.
3. What forms of physiologic responses are common?Physiologic responses occur frequently, often in reaction to reminders of theloss. They take the
form of sudden autonomic discharge with acute symptoms reflecting the pangs of grief: chest pain
160
8/12/2019 32. Grief and Mourning
http://slidepdf.com/reader/full/32-grief-and-mourning 2/6
Grief and Mourning 161
“heartache”), gastrointestinal distress “a knife in the belly”), dyspn ea, paresthesias, pa lpitations,dizziness, nausea, tremulousness, and others. Acutely grieving survivors may dem onstrate hypercor-tisolism, sleep and appetite disturbances, and continuously heightened autonomic arousal.
4 Are all losses the same?No. Althoug h the word “grief” generally is reserved for the feelings and behavior associated with
death e.g., bereavem ent), the same sort of reaction is seen after anyloss considered important by theindividual. Exam ples are stillbirth and miscam age, loss of a job, failing health, disability, amputation,loss of home, or divorce. Indeed, divorce, especially when dependent children are involved, can leadto som e of the most tumultuous and persistent grief reactions. Som etimesa loss that seems trivial tothe outside observer, such as the death ofa pet or a favorite celebrity, or losing an ob ject of sentimen-tal value, is followed by a severe grief reaction because the loss hasa disproportionate significance.The grief also can occur when the lossis intangible, suchas after a stroke or cataract, when the loss isafunction of a part of the body. In each of these examples, the individual loses someone or somethingthat is emotionally or physically “partof themselves.” Th e m eaning of such losses, the intensity of thegrief, and the way people u ltimately cope with the changes in their lives vary from person to person.
5. What is mourning?Mourning isan important aspect of the total grief reaction. It refers toa prescribed set of experi-
ences-which may includea time-frame anda series of behaviors, rituals, and observances-that re-flect a given culture’s or religion’s v iews abou t the meaning s of life and death an d the role of theindividual survivor within this context. Mo urning customs m ay be strictly defined: the w idow shouldwear black and avoid pleasantries for a year; the funeral and m emorial services should contain cer-tain elements; prayers for the dead are said on particular occasions. S om e grief experiences, suchashallucinations, may be more acceptable or even desirable in certain cultures.
In the United States, no standard traditions dictate the decisions and behavior of survivors.There are few tight-knit commu nities where widowed men and and w omen are scrutinized o r moni-tored. Individuals’ religious beliefs may dictate some traditions, but for the most part, mourning hasevolved toward a more individualized and relatively unstructured experience.
6. What is pathologic grief?Patholog ic grief isa commonly used term w ith an elusive definition. It originally referred to those
patients whose grief was absen t or excessive ly intense or prolonged . It also referred to situations wheregrieving patients developed medical or psychiatric illnesses. Although clinicians will likely continue toencoun ter references to pathologic grief, it is not a useful concept. First, the spectrum of n ormative re-sponses to loss is enorm ous. Som e people’s grief is brief and limited in terms o f their emotional re-sponses and sequelae; others grieve profoundly for a long time. Furthermore, particularly following thedeath of a spouse ora child, survivors are likely to continue to m anifest elements of grief intermittentlythroughout their lives. Responses at both ends of this continuum are norm al and no t pathologic.
Second, som e individuals are vulnerable to the development of medical and psychiatric illnessesin the context of grief. These illnessesalso d o not con stitute pathologic grief,but idiosyncratic vul-nerability genetic and developm ental),as expressed at a point of an enormou s stressor.
7 How long does grief last?There is great variability in the course of grief. The most important determinant of the length
and intensity of grief is the closeness of the relationship between the deceased and survivor: howcentra l that person was to the survivor’s emo tional life.In the closest of relationships, an acuteperiod of grief may last froma few weeks to several months, and protracted grief m ay last for years.If you encounter such extended grief,or a persistent, intense grief a year or more after the death,consider the possibility of major depression.
8. Does grief end?The most comm on and clinically norm al forms of protracted grief occur on an intermittent basis
for several years, or forever.A person w ho has lost a child may exp erience elements of acute grief
8/12/2019 32. Grief and Mourning
http://slidepdf.com/reader/full/32-grief-and-mourning 3/6
I62 Grief and Mourn ing
every time he or she hears the name of the child, on special occasions birthdays, holidays, anniver-saries), or when seeing the child’s picture. Such grief, often referred to as anniversary reactionsusually is short-lived and dissipates in minutes. Similarly, when a clinician makes an inquiry into theemotions of any patient’s loss, it should be recognized that in such a regressively oriented explo-
ration, elements of grief are likely to appear and are normal. It is a mistake to think that grief “re-solves” in the sense that it disappears or goes away. In most people, grief is circumscribed andsuppressed, only to re-emerge in response to familiar triggers.
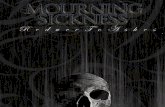
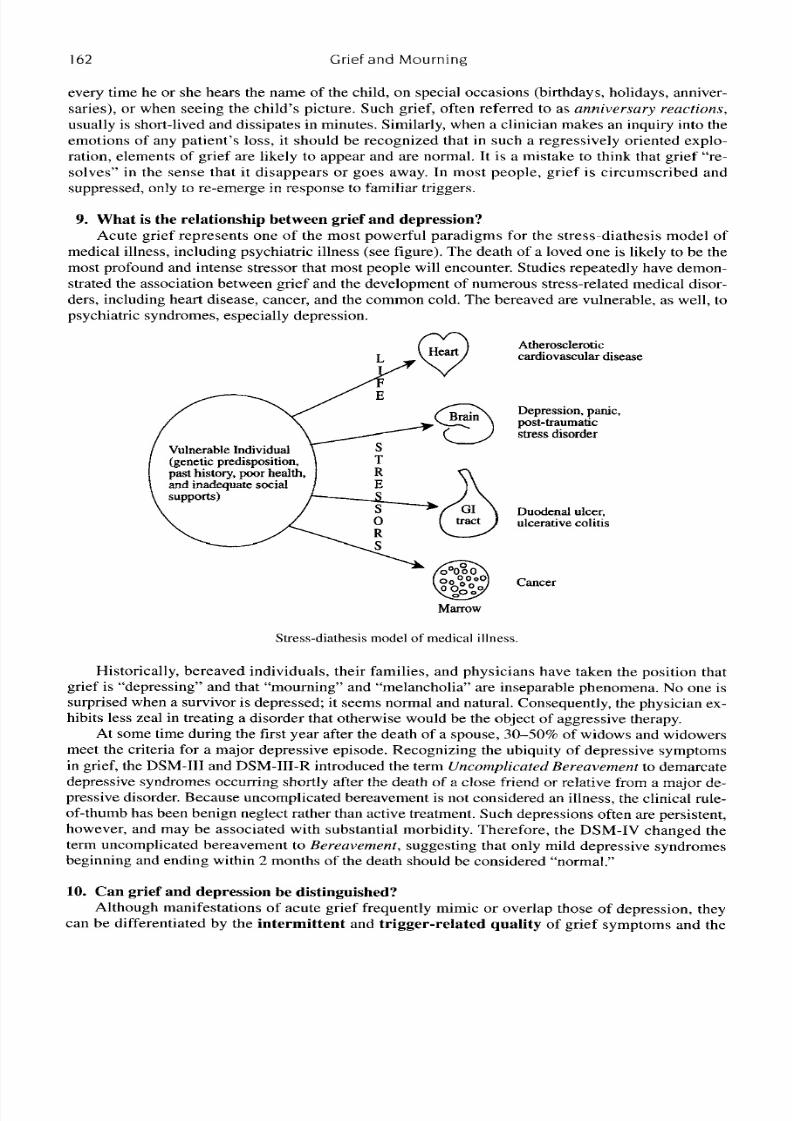
9 What is the relationship between grief and depression?Acute grief represents one of the most powerful paradigms for the stress-diathesis model of
medical illness, including psychiatric illness see figure). The death of a loved one is likely to be themost profound and intense stressor that most people will encounter. Studies repeatedly have demon-strated the association between grief and the development of numerous stress-related medical disor-ders, including heart disease, cancer, and the common cold. The bereaved are vulnerable, as well, topsychiatric syndromes, especially depression.
25 theroscleroticcardiovascular disease
Vulnerable Individual(genetic predisposition,past history, poor health,
nd inadequate social
Depression, panic,post-traumatics t r ss disorder
Duodenal ulcer,ulcerative colitis
Cancer
Marrow
Stress-diathesis model of medical illness
Historically, bereaved individuals, their families, and physicians have taken the position thatgrief is “depressing” and that “mourning” and “melancholia” are inseparable phenomena. No one issurprised when a survivor is depressed; it seems normal and natural. Consequently, the physician ex-hibits less zeal in treating a disorder that otherwise would be the object of aggressive therapy.
At some time during the first year after the death of a spouse, 30-50 of widows and widowersmeet the criteria for a major depressive episode. Recognizing the ubiquity of depressive symptomsin grief, the DSM-111 and DSM-111-R introduced the term Uncomplicated Bereavement to demarcatedepressive syndromes occurring shortly after the death of a close friend or relative from a major de-pressive disorder. Because uncomplicated bereavement is not considered an illness, the ciinical rule-
of-thumb has been benign neglect rather than active treatment. Such depressions often are persistent,however, and may be associated with substantial morbidity. Therefore, the DSM-IV changed theterm uncomplicated bereavement to Bereuvemenf suggesting that only mild depressive syndromesbeginning and ending within 2 months of the death should be considered “normal.”
10. Can grief and depression be distinguished?Although manifestations of acute grief frequently mimic or overlap those of depression, they
can be differentiated by the intermittent and trigger-related quality of grief symptoms and the
8/12/2019 32. Grief and Mourning
http://slidepdf.com/reader/full/32-grief-and-mourning 4/6
Grief and Mourning I63
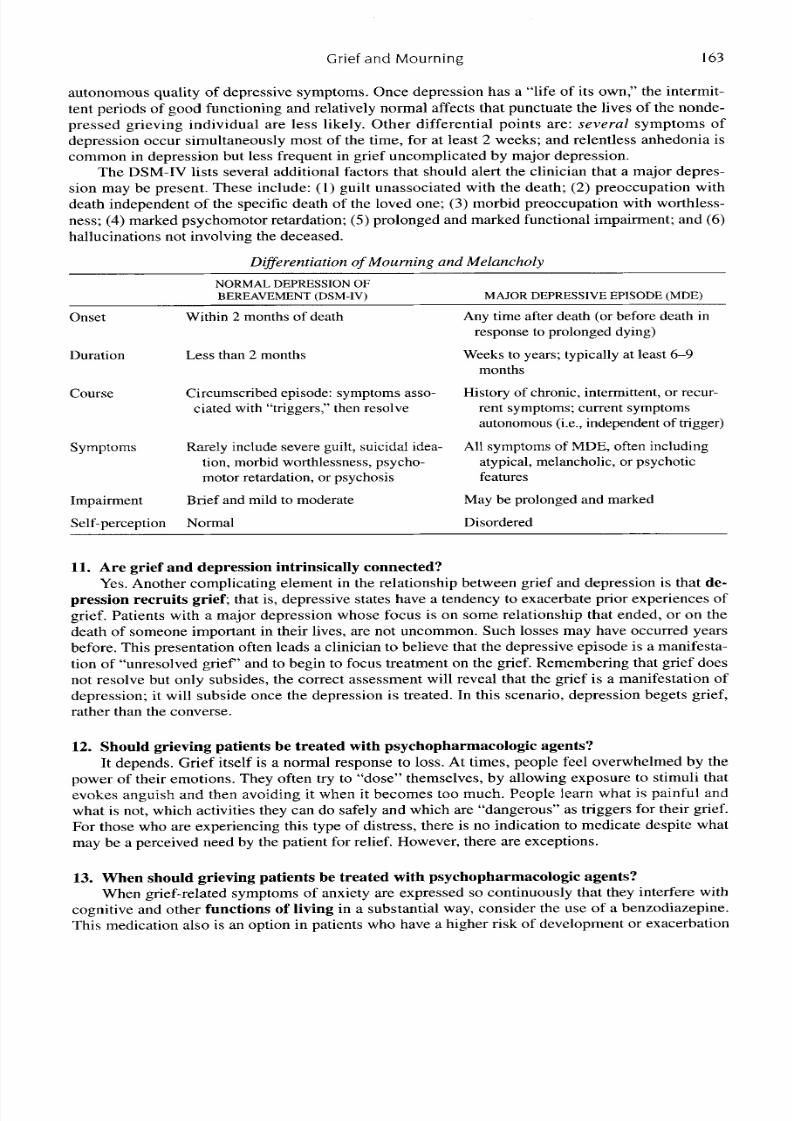
autonomous quality of depressive symptoms. Once depression has a “life of its own,” the intermit-tent periods of good functioning and relatively normal affects that punctuate the lives of the nonde-pressed grieving individual are less likely. Other differential points are: several symptoms ofdepression occur simultaneously most of the time, for at least 2 weeks; and relentless anhedonia is
common in depression but less frequent in grief uncomplicated by major depression.The DSM-IV lists several additional factors that should alert the clinician that a major depres-sion may be present. These include: 1 ) guilt unassociated with the death; (2) preoccupation withdeath independent of the specific death of the loved one; 3) morbid preoccupation with worthless-ness; (4) marked psychomotor retardation; 5 )prolonged and marked functional impairment; and (6)hallucinations not involving the deceased.
Differentiation o Mourning and M elancholy
NORMAL DEPRESSIONOFBEREAVEMENT DSM-IV) MAJOR DEPRESSIVE EPISODE MD E)
Onset Within 2 months of death
Duration Less than 2 months
Course Circumscribed episode: symptoms asso-ciated with “triggers,” then resolve
Symptoms Rarely include severe guilt, suicidal idea-tion, morbid worthlessness, psycho-motor retardation, or psychosis
Impairment
Self-DerceDtion Normal
Brief and mild to moderate
Any time after death or before death inresponse to prolonged dying)
monthsWeeks to years; typically at least 6-9
History of chronic, intermittent, or recur-rent symptoms; current symptomsautonomous i.e., independent of trigger)
All symptoms of MDE, often includingatypical, melancholic, or psychoticfeatures
May be prolonged and marked
Disordered
11. Are grief and depression intrinsically connected?Yes. Another complicating element in the relationship between grief and depression is that de-
pression recruits grief that is, depressive states have a tendency to exacerbate prior experiences ofgrief. Patients with a major depression whose focus is on some relationship that ended, or on thedeath of someone important in their lives, are not uncommon. Such losses may have occurred years
before. This presentation often leads a clinician to believe that the depressive episode is a manifesta-tion of “unresolved grief’ and to begin to focus treatment on the grief. Remembering that grief doesnot resolve but only subsides, the correct assessment will reveal that the grief is a manifestation ofdepression; it will subside once the depression is treated. In this scenario, depression begets grief,rather than the converse.
12. Should grieving patients be treated with psychopharmacologic agents?It depends. Grief itself is a normal response to loss. At times, people feel overwhelmed by the
power of their emotions. They often try to “dose” themselves, by allowing exposure to stimuli thatevokes anguish and then avoiding it when it becomes too much. People learn what is painful and
what is not, which activities they can do safely and which are “dangerous” as triggers for their grief.For those who are experiencing this type of distress, there is no indication to medicate despite whatmay be a perceived need by the patient for relief. However, there are exceptions.
13. When should grieving patients be treated with psychopharmacologic agents?When grief-related symptoms of anxiety are expressed so continuously that they interfere with
cognitive and other functions of living in a substantial way, consider the use of a benzodiazepine.This medication also is an option in patients who have a higher risk of development or exacerbation
8/12/2019 32. Grief and Mourning
http://slidepdf.com/reader/full/32-grief-and-mourning 5/6
164 Grief and Mourning
of a major depression o r anxiety disorder. Usually, benzodiazepines are used as needed for relativelybrief periods.
When substantialsleep disorders develop, short-term intervention with pharmacology can beboth hum ane and helpful. Agents include:1 ) hypno tics, 2) short-acting anxiolytics, or( 3 ) ow
doses of sedating antidepressants e.g., trazodone,50 mg). A persistent and continu ous sleep disor-der with features of early, middle, or late insomnia m ay indicate the onset of m ajor depression, re-quiring closer monitoring and possible use of antidepressants in standard doses.
Depression is under-diagnosed and often under-treated even when diagnosed. Historically,physicians have been reluctantto treat the depression of bereavement aggressively, feeling that treat-ing such depression interferes with normal grief and nature’s restorative properties. However, de-pression is depression, regardless of the context in w hich it appea rs or the existential reasonablenessof its presentation. Depression carries with it substantial morbidity, both medical and psychological.Treat major depression a ggressively, even i t appears n the context o bereavement
14. How can I counsel the bereaved to get past their loss or to put it behind them?You cannot, and you ought not try. The death of one’s spouse o r child or sibling is forever, andelements of the survivor’s griefalso will last forever. Healthy p eople find many ways to cope withtheir losses and grief. Oneof the most “human” ways to deal with suchloss is to mitigate against itby keeping the loved on e alive.It is normal and healthy f or survivors to maintaina relationship withthe deceased.
Survivors frequently have a sense that their loved one is with them, watching over them, pro-tecting them. It is not uncom mon for a widow to carry on conversations w ith her dead husband o r toask for his advice. These and sim ilar phenomena occur in healthy people w ith intact reality-testingwhose sensory perceptions are highly directed toward keeping their loved ones alive.As time goesby, the actual sense of their loved one’s presence evolves into an emotiona l feeling of the person’splace in their heart. Qualities of the deceased m ay becom e incorporated into the identity of the sur-vivor. Cherished p ossessions and me mories keep the deceased alive for those who have physicallylost them. lmportant emotional ties do not d isappear when our loved one s die, and clinicians mustlearn to appreciate these conne ctions, respect them, an d even foster communication about them. Forsurvivors, life will go on, and more comfortably once they have established an emotionally viableway of sustaining their relationship with the deceased.
Therefore, it isnot helpful to convince a bereaved individual to “let go” or get on with life in away that disregards the loved one. Instead, let such patients know you care. Listen when they feellike talking. Offer the perspective of som eone wh o identifies with the painful and often protractedcourse of grief. Be ready to step in when, and if, a major depressionor other m edical or psychiatriccomplications develop.
15. What are the other common problems of the bereaved?Frequently, problems develop because of thereactions of others to grief. Friends and family
may be unable to tolerate grief and m ay avoid the bereaved or, when with them, discourage themfrom expressing what they feel. Grieving persons m ay feel isolated,at times because of their reluc-tance to inflict their ow n suffering on others. In time, they will find closeness and comfort withothers who have felt such pain and with whom they feela common bond. For this reason, involve-ment in a bereavement suppo rt group usually is helpful.
Of particular concern is the difficulty physicians and therapists can have in dealing with the be-
reaved, particularly those in the most acute throes of grief. Empathetic clinicians may find them-selves experiencing much anguish and helplessness in the faceof their patients’ suffering. At timesthis may feel intolerable, and clinicians m ay become inclined t o push their patients away or to divertthem from their grief. Oth er therapists may fe ar being “sw allowed up” by the intense need of thegrieving person. Th e intense regressionof grief is, however, a time-limited phenomenon, and theclinician’s em otion al availabilityis central to his or her ability to help the bereaved. The healthyclinician em erges from the suffering, often stronger fo r the experience.
8/12/2019 32. Grief and Mourning
http://slidepdf.com/reader/full/32-grief-and-mourning 6/6
Grief and Mourning 165
BIBLIOGRAPHY1 Burnell GM, Burnell AL eds): Clinical M anagement of Bereavement: A Handbook for Healthcare
2. Jacobs S ed): Pathologic Grief: Maladaptationto Loss. Washington, DC, American Psychiatric Press, 1993.3 . Osterweis M, SolomonF, Green M eds): Bereavement: Reactions, Conseq uences, and Care. W ashington,
4. Prigerson HG Reynolds CF, Jacobs SC,e t al: Results of a consensus conference torefine diagnostic criteria
5. Raphael B (ed): The Anatomy of B ereavement. New York, Basic Books, 1983.6. Reynolds CF, Miller M D, Pastem akRE, et al: Treatmentof bereavement-related m ajor depressive episodes
in later life: A co ntrolled study of acute and continuation treatment with nortriptyline and interpersonalpsychotherapy. Am Psychiatry 156:202-208, 1999.
Professionals. New York, Human Sciences Press, 1989.
DC, National Academy Press, 1984.
for traumatic grief. Br J Psychiatry,In Press.
7. Rynearson EK ed): Bereavement. Psychiatric Annals SpecialIssue) 16:268-318, 1986.8. Rynearson EK ed): Pathologic Bereavement. Psychiatric Annals Special Issue) 20:294-348, 1990.9. Shuchter SR ed): Dimensionsof Grief: Adjusting to the Death ofa Spouse. San Francisco, Jossey-Bass,
10Stroebe MS, Stroe be W, Hansson RO eds): Handbook of Bereavement: Theory, Research and Intervention.
11. Worden JW ed): Grief Counseling and Grief Therapy: A Handbook fo r the Mental Health Practitioner. 2nd
12. Wortman CB, Silver RC: Th e mythsof coping with loss. Co nsult Clin Psycho1 57:349-357, 198 9.13 Zisook S Shu chter SR: Major depression associated with widow hood. Am Assoc Geriatr Psychiatry: 316-
14. Zisook S ed): Grief and Bereavement. Psychiatr Clin North Am 10:329-510, 1987.15. Zisook S, Chentsova-Dutton Y Shuchter S R : PSTD following bereavement. Ann Clin Psychiatry
16. Zisook S, Shu cbter SR: Psychotherapy of the depressions in spousal bereaveme nt. Psycho ther Pract
17. Zisook S, Schuchter S R, PederelliP et al: Bupropion: Treatment of bereavem ent. Am Psychiatry, In Press.
1986.
Cambridge, Cambridge University Press, 1993.
ed. New York, Springer, 1991
326, 1993.
lO 4): 157-163, 1999.
2 :3 14 5 , 1996.