31^ Al 8/d A/0. /?7| LECITHIN TREATMENT FOR TARDIVE .../67531/metadc330807/m2/1/high_re… ·...
144
31^ Al 8 / d A/0. /?7| LECITHIN TREATMENT FOR TARDIVE DYSKINESIA: A CLINICAL EVALUATION DISSERTATION Presented to the Graduate Council of the North Texas State University in Partial Fulfillment of the Requirements For the Degree of DOCTOR OF PHILOSOPHY By Lynn Aikin Price, M,S, Denton, Texas December, 1982
Transcript of 31^ Al 8/d A/0. /?7| LECITHIN TREATMENT FOR TARDIVE .../67531/metadc330807/m2/1/high_re… ·...

3 1 ^
Al 8 / d
A/0. / ? 7 |
LECITHIN TREATMENT FOR TARDIVE DYSKINESIA:
A CLINICAL EVALUATION
DISSERTATION
Presented to the Graduate Council of the
North Texas State University in Partial
Fulfillment of the Requirements
For the Degree of
DOCTOR OF PHILOSOPHY
By
Lynn Aikin Price, M,S,
Denton, Texas
December, 1982

Price., Lynn Aikin, Lecithin Treatment for Tardive
Dyskinesia; A Clinical Evaluation. Doctor of Philosophy
(Ecological and Behavioral Medicine), December, 1982,
136 pp., 23 tables, 8 figures, references, 78 titles.
Tardive dyskinesia is an insidious and debilitating
extrapyramidal side effect of neuroleptic drug treatment.
Recent research has suggested that lecithin has been
effective in treating tardive dyskinesia.
Lecithin's effects were evaluated under double-blind
placebo controlled conditions in 45 male inpatients.
Treatment conditions included a placebo control group, a
lecithin treatment group, and a no-treatment control group.
Fifteen subjects were randomly assigned to each group.
Subjects in the lecithin group received 60 gms/day of
lecithin (33 gins of phosphatidylcholine) . Subjects in the
placebo group received a similar mixture which contained
no lecithin. Subjects received mixtures for 9-11 days.
Treatment effectiveness was determined by subjective,
objective, and global evaluations. All subjects were
evaluated 3 to 4 days prior to treatment and following
9 to 11 days of treatment.
Data were analyzed using a factorial analysis of
covariance. Treatment conditions, age, and length of
neuroleptic treatment were the classification variables.

For each treatment measure, pretest score was the covariant
and posttest score was the variant.
Results indicated that few measures demonstrated
treatment effects. Symptom severity measures showed no
significant differences for any of the classification
variables.
Of the measures assessing motor performance ability,
only dominant hand finger oscillation measures showed a
significant reduction due to lecithin's effects. The inter-
action of treatment conditions and age suggested that only
younger subjects responded to lecithin's effects by
reducing dominant hand finger oscillation. The interaction
of treatment conditions and length of neuroleptic treatment
indicated that shorter-term treated subjects were more
responsive to lecithin's effects.
No significant effects of lecithin were reflected in
measures assessing sensory-motor integration or speech
sounds articulation. Subjective global evaluations of
treatment were determined by researcher and subjects.
Results indicated that global evaluations were not signif-
icantly related to treatment conditions.
Overall, results did not demonstrate lecithin's
effectiveness in reducing symptom severity or improving
motor performance. These findings did not support
lecithin's claim as an effective treatment for tardive
dyskinesia.


TABLE OF CONTENTS
Page
LIST OF TABLES vii
LIST OF ILLUSTRATIONS ix
LECITHIN TREATMENT FOR TARDIVE DYSKINESIA: A CLINICAL TREATMENT
Introduction 1
Cholinomimetic Treatment Effects on TD Physostigmine treatment Choline treatment Lecithin treatment
Method 52
Subjects Measures Procedures
Results 57
Discussion 66
Appendices 90
References 127
V I

LIST OP TABLES
Table Page
1. Antipsychotic Agents . . . . . . . . . . . . . 89
2. Differential Diagnostic Categories for Tardive Dyskinesia go
3. Relative Sequence of Onset of Extrapyramidal Side Effects 16
4. Studies Using Physostigmine in tne Treatment of Tardive Dyskinesia 92
5. Studies Using Choline Chloride in the Treatment of Tardive Dyskinesia , . ? , . , . 94
6. Studies Using Lecithin in the Treatment of Tardive Dyskinesia . . . . . . . . . . . . . . 96
7. Summary of Analysis of Covariance for Total Score on Simpson Tardive Dyskinesia Rating Scale H I
8. Summary of Analysis of Covariance for Total Number of Scored Items on Simpson Tardive Dyskinesia Rating Scale . 112
9. Summary of Analysis of Covariance for Bucco-Lingual-Masticatory Symptoms on Simpson Tardive Dyskinesia Rating Scale . . 1 1 3
10. Summary of Analysis of Covariance for Total Score on Selt-Report Tardive Dyskinesia Rating Scale . , » . . . . . 114
11. Summary of Analysis of Covariance for Dominant Hand Finger Oscillation Rate , . . t 115
12. Summary of Analysis of Covariance for Non-Dominant Hand Finger Oscillation Rate , , 1 1 6
13. Summary of Analysis of Covariance for Purdue Pegboard Test 117
vii

Table Page
14. Summary of Analysis of Covariance for Minnesota Rate of Manipulation Test . . . . . . 118
15. summary of Analysis of Covariance for Line Tracing Task . . . . . . . , , . , . . . 119
16. Summary of Analysis of Covariance for Bender-Gestalt Total Score 120
17. Summary of Analysis of Covariance for Bender-Gestalt Category Score . . . . . . . . . 121
18. Summary of Analysis of Covariance for Digit Symbol Test 122
19. Summary of Analysis of Covariance for Trails A Test . . . . . . . . . . . . . . . . 123
20. Summary of Analysis of Covariance for Speech Sounds Test . . . . . . . . . . . . . . 124
21. Subjects Assigned to Treatment Response Categories by Self-Evaluation . . . . . . . . . 64
22. Subjects Assigned to Treatment Response Categories by Researcher's Evaluation . . . . . 65
23. ANCOVA Distribution of Subjects to Cells . . . 125
viii

LIST OF ILLUSTRATIONS
Figure Page
1. Striatal DA/ACh Activity in Acute EPS Disorders 14
2. Striatal DA/ACh Activity in Tardive Dyskinesia 15
3. Presumed Functioning of Pre- and Post-Synaptic Dopaminergic Neurons in the Nigrostriatal System 21
4. Direct Inhibitory Action of DA Neurons of the Nigrostriatal Pathway on ACh Neurons of the Striatum 29
5. Reciprocal Interaction Between Dopamine and Cholinergic Neurons in the Striatum 31
6. Pathophysiology and Cholinergic Treatment Effects on Striatal Neurons 37
7. Interaction of Treatment Conditions and Age for Dominant Hand Finger Oscillation 60
8. Interaction of Treatment Conditions and Length of Neuroleptic Treatment for Dominant Hand Finger Oscillation 62
IX

LECITHIN TREATMENT FOR TARDIVE DYSKINESIA:
A CLINICAL EVALUATION
Tardive dyskinesia, an insidious and debilitating
extrapyramidal side effect of drug treatment in major
psychiatric disorders, has been the cause of considerable
concern in the long-term use of neuroleptics (Ayd, 1977;
Crane, 1968). The concern has centered around the issue of
whether the benefits derived from long-term maintenance
doses of neuroleptics outweigh the risk of developing tardive
dyskinesia (TD). Because the demographics of this disorder
have been illusive, risk factors associated with TD were
only marginal predictors of who would develop TD. Hence,
medical judgment usually favored continued neuroleptic
treatment at the expense of increasing the likelihood of TD.
To date, research efforts aimed at disclosing salient
and highly predictable risk factors which herald the onset
of the disorder have been disappointing. The risk factors
revealed by these research efforts have proved to be signif-
icant only for population demographics and essentially poor
predictors of TD for any given individual. Hence, for the
individual on neuroleptic therapy, risk factors have been
largely ignored in favor of continued pharmacotherapy for
the major psychiatric disorder. In view of these consider-
ations, it seems both plausible and practical to pursue

research efforts aimed at a treatment for tardive dyskinesia.
In the late 1950s, the syndrome of oral-lingual-
masticatory movements in patients treated with phenothiazines
was first described (Hall, Jackson, & Swain, 1956;
Schonecker, 1957; Sigwald, Bouttier, Raymondeau, & Piot,
1959). A striking predilection for involuntary and
repetitive movements that typically affect orofacial
structures has been noted in tardive dyskinesia (TD).
Because facial movements were the most obvious and frequently
encountered disorder of TD (Crane, 1968), additional terms
such as "orofacial dyskinesia" and "bucco-linguo-masticatory
syndrome" (BLM) were used interchangeably with tardive
dyskinesia (Kobayashi, 1977).
Movement disorders in other areas of the body were also
frequently noted. Druckman, Seelinger, and Thulin (1962)
noted continuous jerky movements of the extremities
(particularly of the fingers, toes, wrists, and ankles), and
tonic contraction of neck and back muscles.
Symptoms characteristic of tardive dyskinesia have been
graphically described by numerous writers (Ananth, 1980;
Carpenter & Rudo, 1979; Casey, 1978; Crane, 1968, 1973;
Jeste & Wyatt, 1979; Klawans, 1973; Kobayashi, 1977; Quitkin,
Rifkin, Feld, & Klein, 1977; Schiele, Gallant, Simpson,
Gardner, & Pole, 1973; Sovner, 1978). Symptom characteristics
presented by the American College of Neuropsychopharmacology

Food and Drug Administration Task Force (Schiele et al.,
1973) have become the established standard for the syndrome.
In older chronic patients, TD has been characterized by
stereotyped, repetitive, involuntary movements of the mouth,
lips, and tongue. Sometimes these movements were accompanied
by choreiform movements of the limbs and trunks. The most
commonly described symptoms which made up the "bucco-linguo-
masticatory" triad consisted of sucking and smacking
movements of the lips, lateral jaw movements, puffing of
cheeks, and tongue thrusting, rolling, or fly-catching
movements. Occasionally, the BLM triad was heralded by
tick-like, grimacing movements of the lips and eyes.
Additionally, the extremities have shown choreiform movements
that were variable, purposeless, involuntary, and quick.
Frequently, athetoid movements which were continuous,
arrhythmic, worm-like, slow movements in the distal parts
of the limbs have been associated with choreiform movements.
Together, these movements comprised the choreoathetoid
postural movements characteristic of TD. Trunkal movements
either in an anterior-posterior direction, or from side to
side have been observed in some patients.
The symptom severity and the configuration of symptoms
displayed at any given time have been reported to be quite
variable (Ananth, 1980; Carpenter & Rudo, 1979,* Crane, 1968;
Jeste & Wyatt, 1979; Schiele et al., 1973). In general,

severity of movements correlated with the general level of
arousal. Movements tended to worsen under emotional tension
and increased activity, to abate in state of relaxation and
quiesence, and to disappear altogether during sleep
(Crane, 1968; Schiele et al., 1973). Additionally, voluntary
activity of affected areas, often (but not always) has been
associated with reduce abnormal movements (Crane, 1968).
Likewise, fewer abnormal movements have been associated with
volitional control (Crane, 1968).
The configuration of abnormal movements in various body
parts has been shown to vary in intensity (mild to severe)
from one body part to another as well as from one time to
another within the same body part (Crane, 1968). For
example, tongue protrusion has been observed to be severe
at one time and mild to absent at another time, while
choreoathetoid movements of fingers may be mild in the first
instance and severe in the second. Knowledge of the patho-
physiology of dyskinetic movements has thus far been
inadequate to account for the variability in symptom
characteristics.
Tardive dyskinesia has been intimately associated with
the use of neuroleptic drugs (Crane, 1968), Though the
cause of TD has not been completely understood, epidemiologic
evidence has implicated neuroleptic drugs as a major, (but
neither necessary nor sufficient) cause of the syndrome

(Carpenter & Rudo, 1979). The role of neuroleptic drugs has
been considered insufficient to show causality because not
all patients chronically administered neuroleptics display
the syndrome. Moreover, neuroleptics have been considered
unnecessary to the development of the BLM dyskinetic
syndrome because it occasionally occurs spontaneously in
aging (Faurbye, Rasch, Petersen, Brandberg, & Rakkenberg,
1964). However, since TD has been operationally defined as
late or tardive onset of dyskinetic movements due to long-
term neuroleptic treatment (Crane, 1968? Faurbye, 1970),
neuroleptics have been considered necessary but not
sufficient to account for the syndrome.
Faurbye et al. (1964) first observed dyskinetic
manifestations in patients treated with phenothiazines and
related compounds. Drugs of this type have become known as
antipsychotics, major tranquilizers, or neuroleptics (see
Table 1, Appendix A).
It has been well established that the onset of symptoms
was insidious. In early stages, symptoms have appeared as
vermicular ripples of the tongue, inability to protrude the
tongue without retraction, or inability to sustain protrusion
(Carpenter & Rudo, 1979; Schiele et al,, 1973). Because of
the insidious onset, most often tardive dyskinesia has been
noticed only after the syndrome was fully established
(Crane, 1968).

A primary consideration in the diagnosis of tardive
dyskinesia has involved the duration of neuroleptic treatment
and changes in neuroleptics associated with the appearance
of the dyskinetic manifestations. For patients maintained
on neuroleptics, the emergence of tardive dyskinesia has
been reported to occur as early as 90 days from the onset
of neuroleptic therapy. If dystonic movements were noted to
occur earlier in drug treatment, most likely they were due
to other extrapyramidal disorders (Carpenter & Rudo, 1979).
Often TD manifestations appeared or became intensified
following termination or reduction of neuroleptic dosage
(Crane, 1968, 1973; Faurbye et al., 1964). Conclusively,
the role of neuroleptic involvement in the etiology of TD
has been well established.
The course of TD has not been completely understood.
Present evidence has indicated that in some instances TD
was reversible, while in other instances it appeared to be
irreversible or persistent. Most researchers have
acknowledged that it was quite probable that both subtypes
existed (Carpenter & Rudo, 1979; Casey, 1976, 1978? Crane,
1968, 1972, 1973, 1977; Jeste & Wyatt, 1979; Kobayashi, 1977;
Marsden, Tarsy, & Baldessarini, 1975; Quitkin et al., 1977; &
Simpson, 1980b). Although persistence of TD, even after the
discontinuation of neuroleptics, has been a characteristic
feature (Crane, 1968, 1972, 1973, 1977; Kobayashi, 1977),

spontaneous remission following drug withdrawal has been
reported. Estimates of spontaneous remission have varied
greatly and ranged from 2-40% by Kobayashi (1977), approx-
imately 30% by Marsden et al. (1975), and from 0-90% by
Simpson (1980b).
Most researchers have agreed that symptomatology
decreases over a period of several months following discon-
tinuation of the neuroleptic and have advocated drug
withdrawal at first signs of tardive dyskinesia (Carpenter &
Rudo, 1979; Crane, 1968, 1972, 1973, 1977; Jeste & Wyatt,
1979; Quitkin et al., 1977). Several researchers have
concluded that the major variable in the reversibility of
TD may be the length of time that symptoms have persisted
prior to drug withdrawal and not the age at onset of the
symptoms (Carpenter & Rudo, 1979; Casey, 1978; Quitkin
et al., 1977). Jeste and Wyatt (1979) maintained that
withdrawal of neuroleptics resulted in spontaneous remission
in younger and non-BD patients. For cases of persistent
dyskinesia, evidence has indicated that following drug
withdrawal the condition does not usually progress in
severity (Schiele et al., 1973).
There has been some belief that persistent dyskinesia
reflected Irreversible brain damage (Jeste & Wyatt, 1979).
Consistent with this view were the findings of Christiansen,
Moller, and Faurbye (1970). The investigation of 28 brains

8
from patients who at the time of death had persistent oral
dyskinesia in comparison to brains from a control group
matched for age and sex, revealed lesions of the substantia
nigra in combination with midbrain and brain stem lesions
were characteristic of the tardive dyskinesia group.
Whether persistent tardive dyskinesia reflects a permanent
change in brain function and structure is an issue requiring
further validation.
As noted in the preceding discussion, the course of TD
has been believed to be either persistent or reversible.
Casey (1978) has proposed that a more parsimonious explana-
tion of the course of TD is that it occurs along a continuum
of persistence. Symptoms that resolve may reflect a
temporary alteration in CNS function, while those that
persist may reflect a permanent change in CNS function.
Factors predisposing to tardive dyskinesia have been
widely studied, but the results are conflicting. Probably
the most convincing risk factors have involved age, duration
of neuroleptic use, and quantity of neuroleptics. A more
comprehensive overview of risk factors has recently been
published in a task force report on tardive dyskinesia
(Baldessarini, Cole, Davis, Simpson, Tarsy, Gardos, &
Preskorn, 1980). Age was probably the single most important
risk factor (Ezrin-Waters, Seeman, & Seeman, 1981).
Patients above 50 were at greater risk for TD than were

younger patients (Carpenter & Rudo, 1979; Crane, 1968, 1973).
Some studies have also demonstrated a correlation between
age at the time of diagnosis or age at the onset of neuro-
leptic treatment and tardive dyskinesia (Crane, 1973; Jus,
Pineau, Lachance, Plechat, Jus, Pires, & Villeneure, 1976).
Another group of factors which correlated with
increased incidence of TD has included the duration, quantity,
and type of drugs used by the patient. Several researchers
have concluded that the number of years of neuroleptic
treatment are correlated with the occurrence of TD
(Carpenter & Rudo, 1979; Crane, 1968, 1973; Ezrin-Waters
et al., 1981). It also has been reported that large doses
of neuroleptics were more likely to produce TD (Carpenter
& Rudo, 1979; Crane, 1977) especially among older patients
(Crane, 1977). Types of drugs associated with increased
incidence of TD were Haldol, Depot drug (Ezrin-Waters et al.,
1981) and antiparkinson medications (Carpenter & Rudo, 1979).
Other factors, including organic brain damage, sex,
and earlier acute extrapyramidal disorders, have been less
widely accepted as risk factors. Several researchers have
maintained that organic brain damage is predictive of TD
(Carpenter & Rudo, 1979; Crane, 1968; Klawans, 1973).
Others (Ananth, 1980; Carpenter & Rudo, 1979) have discussed
sex as a risk factor. Females have been reported to be at
greater risk of developing TD than males. The emergence of

10
acute extrapyramidal disorders early in neuroleptic treatment
also has been reported to correlate with TD. Conclusively,
these factors are believed to reflect an inconsistent
relationship with TD.
Overall, the risk factors presented in this section
have been reflected in the demographics of the population of
patients studied. Nevertheless, they have not been shown
to be reliable predictors of TD for individual patients.
Surprisingly little is actually known about the
prevalence of tardive dyskinesia among patients who have
undergone neuroleptic therapy. In chronic care hospitals,
reports on prevalence have ranged from 0.5% to 56% (Jus et
al., 1976). In an outpatient clinic a recent report has
found about 40% of patients on long-term neuroleptic
treatment show some degree of TD (Ezrin-Waters et al., 1981).
In a review on the prevalence of TD, Kazamatsuri et al.
(1972) concluded that the following factors are responsible
for the variability in prevalence estimates: (1) lack of
common criteria in recording the presence or absence of TD,
(2) the possibility that neuroleptics suppress TD, (3) the
highly variable definition of TD. Other considerations
accounting for the variability in prevalence estimates have
included: (1) different criteria for diagnosis of TD,
(2) difference in the severity of TD for diagnosis, (3) the
population in which the survey took place, (4) inclusion of

li
other extrapyramidal disorders, and (5) the age of the
population. Judging from the number of variables encountered
when attempting to assess the prevalence of TD, one is not
surprised to find such a wide range of variability.
The diagnosis of tardive dyskinesia has been suspected
when the classical BLM movements and also choreiform
movements of the extremities and trunk were observed following
months or years of neuroleptic use, or following discontinua-
tion or reduction of neuroleptic drugs. However, before a
definite diagnosis of TD could be made, it was necessary to
differentially rule out other diagnostic categories. Major
differential categories have included (1) spontaneous
dyskinesias, (2) dyskinesias related to neurological
disorders, (3) psychoneurological dyskinesias, (4) dyskinesias
due to metabolic disorders, (5) dyskinesias of other extra-
pyramidal side effects, (6) dyskinesias produced by drugs
other than neuroleptics, (7) dyskinesias produced by
electroconvulsive therapy, (8) prostetically induced
dyskinesias. In addition to giving due consideration to an
accurate differential diagnosis, it has been advisable to
consider the possibility of mixed syndromes of dyskinesias.
In these syndromes some of the dystonic movements could have
been due to tardive dyskinesia while other dystonic
mannerisms could have been due to differential syndromes.
A detailed outline of differential diagnostic categories for
TD is presented in Table 2 (see Appendix B).

12
Probably the most difficult differential category
noted has been that of spontaneous dyskinesias. Because
all patients within the population studied have had a
history of neuroleptic treatment, it has been most difficult
to differentiate between BLM tardive dyskinesias and
spontaneous dyskinesias. Moreover, differential diagnosis
has become increasingly difficult with the elderly
psychiatric patient, since the BLM syndrome may be related
to senile chorea (Klawans, 1973) rather than to TD. In
younger patients treated with neuroleptics, spontaneous
cases of dyskinesias have been infrequent as compared to
drug related ones. Berger (1980) reported estimates that
from 1-20% of TD patients actually suffer from spontaneous
dyskinesia. Kobayashi (1977) reported that among a mixed
population of psychiatric patients, 3 - 6% were estimated
to suffer from spontaneous rather than drug induced TD.
Contrastingly, estimates of spontaneous dyskinesia among
elderly, chronically institutionalized patients were reported
to be as high as 40%. Conclusively, differential diagnosis
ruling out the possibility of spontaneous dyskinesias in the
elderly psychiatric patient has been, at best, tenuous.
Differential diagnosis of dyskinesias related to
neurological disorders have not posed such a perplexing
diagnostic problem. Both medical history and diagnostic
criteria associated with the neurological disorder have

13
facilitated a differential diagnosis from tardive dyskinesia.
Psychoneurological dyskinesias have been rather
difficult to distinguish from TD. Chronic schizophrenic
mannerisms and stereotypes have been reported to resemble TD.
Though the stereotyped movements of schizophrenia include
many of the BLM dyskinetic movements, choreoathetoid
movements present in TD rarely have been observed in
schizophrenia. Additionally, in schizophrenia, abnormal
movements have been associated with disjointed speech,
sounds, or utterances and symbolically charged movements.
Also, schizophrenic mannerisms have been associated with
akinetic and bizarre posturing of body parts, rather than
choreoathetoid postures (Carpenter & Rudo, 1979).
Dyskinesias due to metabolic disorders have been
easily ruled out by appropriate laboratory tests.
Dyskinesias of this type have been infrequently encountered
and pose few problems in differential diagnosis.
Other extrapyramidal disorders which also result from
neuroleptic treatment have posed a major differential
diagnostic problem. These have included (1) pseudo-
Parkinsonism, (2) akathisia, (3) acute dystonic reaction,
(4) Pisa syndrome, (5) rabbit syndrome. Despite the super-
ficial similarity of the abnormal movements, these disorders
have been considered the neurochemical obverse of TD.
Theoretically, these disorders represented a reduction in

1.4
striatal dopaminergic (DA) activity and a concomitant
enhancement of cholinergic (ACh) activity. Hypothetically,
they were early manifestations of dopamine receptor
blockade caused by the administration of the neuroleptic.
These disorders responded to treatment with anticholinergic
drugs by reestablishing the DA/ACh balance (Carpenter &
Rudo, 1979; Kobayashi, 1977; Schiele et al., 1973). The
relationship between dopaminergic and cholinergic activity
DA
treatment with DA ACh anticholinergic*' |
agents .ACh
acute reaction restored to DA receptor homeostasis blockade
Figure 1. Striatal DA/ACh in Acute EPS Disorders
in the striatum for these types of disorders is depicted
graphically in Figure 1.
In contrast to these syndromes which were viewed as
manifestations of DA receptor blockade, tardive dyskinesia
was believed to represent a hypersensitivity of post-synaptic
dopamine receptors (Klawans, 1973); wherein an increase in
striatal dopaminergic activity and a concomitant decrease in
cholinergic activity has occurred. These disorders responded
to treatment with cholinergic drugs by reestablishing the
DA/ACh balance (Carpenter & Rudo, 1979; Kobayashi, 1977;
Schiele et al., 1973). The neurotransmitter imbalance

15
believed to be responsible for TD is shown in Figure 2.
Tardive dyskinesia has been shown to respond to treatment
with cholinergic drugs (Davis, Berger, & Hollister, 1975;
Davis, Hollister, Barchas, & Berger, 1976; Growdon, Hirsch,
Wurtman, & Weiner, 1977; Tamminga, Smith, Ericksen, Chang,
& Davis, 1977). The relationship between dopaminergic and
cholinergic activity in the striatum is presented in Figure 2
ACh treatment with DA ACh cholinergic I
DA y S | agents
tardive (late) restored reactions to homeostasis hypersensitivity of DA receptors
Figure 2. Striatal DA/ACh Activity in Tardive Dyskinesia
Another primary difference between initial and tardive
manifestations of abnormal movements in the course of neuro-
leptic therapy has been the time between the initiation of
neuroleptic treatment and the appearance of symptoms
(Carpenter & Rudo, 1979). As indicated in Table 3, acute
dystonic reactions have been noted during the first few days
of neuroleptic therapy. Akathisias have been observed several
days after the initiation of treatment. Pseudo-Parkinsonism
has been reported to develop from approximately one week to
three months following the beginning of neuroleptic treatment.

16
M-l O W
•P 4J U 0 O CO H4 C MH O W
m Q) O >0
CO •H 0 w
0 a rH G rH £> <D «
P TJ E-» CT-H
0 2 co re
JH CD N > ft
•H <0 -P M cd -P
rH X 0 W OJ
10 0 •H 4J •H e , 0 X ^ g -P P X u
0 -P
MH 0 O 03 W -P -P G C 0 0
> > o o e e
0 p
o> _ _ C w oi S E O X -P 0 0 -P 0 G
0 0 4-1 rC £ 0 U 0
• • > 1 > 1 u In
; fd (d -P -P
03 CP 0 1 G G P G G 3 p J-t »H "H rH rH -P MH £ 0 0 o *w 0 > > U P & c c ftfoOHH
<—I CN 00 ^ Lf)
G hh c o
G O tfi
rH •H 0) «—1 4J -H = «p •H -p RJ O D> -H •P 3 T5 <0 G fd 03 O }-( 14-! •H C& *0 fO rH G 0> fd -P 0 rH O Dl G 0 A: O >i-H G •H 0 (h »H iH -P -P -H 4-> > rH »H 1 *H fO rH •P 0 u 1 0 rH *0 > UH •H E 0 X E rH *H -H *4-1 03 •P 03 0 *H D»rH P
O 0 d In di -H (d rG G -P 2 s EH = OS W CO
03 •H 03 o • • • • • • •
0 >i 0» rH <N CO 4 5 6 7
G •p u 03 rH p 03 p CD U D> H •H G -P u-i o W M-i M CD •H .p 0! Q W
0» W G 4J
•H G O 0 fd 0 E
w E >•» >1 0 •H -H 0 > rH U W fij O rH Cn iH •P 4-» E 0 fd C G 0 rH E 0 P 0
•h id u E *H rH +> -H O 0 0 O M U G > > 03 0 fd xi O G P EH fe < E H E
rH O CO •H
T3 G •H O E «P rd 03 03 u u >1 G >i 0 P O OiTJ •H d M 0 +j M 0 -p 0 4-> to P rd X -H 0 0 W Q < u
w •H rC •P fd
Ai <
03 •H G o
I K O G
•O -H P X 0 M 01 ft & A
rd •H 03
0) 0 > G
•H -H
M 03 03 }H Eh Q

17
Tardive dyskinesia has not been shown to develop prior to
three months of neuroleptic treatment.
Other characteristic differences between tardive
dyskinesia and other extrapyramidal syndromes have been
related to the discontinuation or change in dosage.
Researchers have found that tardive dyskinesia has either
appeared for the first time or has become worse following
discontinuation or reduction of neuroleptics (Crane, 1968).
In contrast, they have noted that other extrapyramidal
disorders have improved or abated altogether shortly
following dose reducation or discontinuation (Carpenter
& Rudo, 1979). Accordingly, researchers have evidenced
that an increase in the dosage of neuroleptics has alternated
or masked symptoms of TD and augmented symptoms of other EPS
disorders (Crane, 1968; Schiele et al., 1973).
Dyskinesias produced by drugs other than neuroleptics
have included 1-dopa and antihistamine decongestants. The
mode of action of these drugs has indicated that they produce
a pseudo-tardive dyskinesia effect. Accordingly, it is
believed that the underlying neurochemical mechanism of these
drugs may be identical to that of tardive dyskinesia. In
support of this contention, it has been demonstrated that
antihistamines have an anticholinergic effect
(Schiele et al., 1973) which shifts the balance of striatal
dopamine and acetycholine in the same directions as does TD.

18
L-dopa, a precursor of dopamine, enhances dopaminergic
activity and attenuates cholinergic activity.
ECT induced dyskinesias have presented little problems
in differential diagnosis because this information is readily
available in the medical records.
The oromandibular chewing syndromes also has presented
little problems for differential diagnosis of TD. When the
patient has obtained dentures which fit well, this syndrome
has disappeared.
The mixed syndromes of tardive dyskinesia have posed a
considerable problem for both accurate diagnosis and assess-
ment of treatment results in TD. Research efforts have been
well advised to eliminate the mixed syndromes altogether
or risk invalid results. Conclusively, a detailed and
extensive consideration of differential diagnosis of tardive
dyskinesia has been deemed imperative in both clinical and
research efforts.
The search for the underlying pathophysiological
mechanisms of TD has been fervently pursued during the past
decade. Despite these efforts, the state of empirical
findings has left many inferences open to conjecture and
speculation. In the following discussion, several hypothe-
tical models of the pathophysiology of TD will be presented
as they evolve chronologically in the literature.

19
The search for the underlying pathophysiological
mechanisms of tardive dyskinesia began with the observation
that TD was intimately associated with the long-term use of
neuroleptics (Crane, 1968? Faurbe et al., 1964). Initially,
the mode of action of the neuroleptic on central nervous
system's neurons and neurotransmitters was investigated as
a mechanism for the pathophysiology of TD.
Neuroleptics, known to block the action of dopamine in
the limbic system, were also believed to interfere with
dopamine transmission in the nigro-striatal pathway and the
striatum (Carlsson, 1970). Neuroleptics, by instituting
a blockade of dopamine (DA) striatal receptors, have been
shown to produce a "chemical denervation" of these receptors
in the striatum (Carlsson, 1970). Research efforts have
revealed that homeostatic mechanisms in the DA neurons and
post-synaptic dopaminergic receptor sites were engaged in an
effort to overcome the neuroleptic blockage imposed on the
DA receptors by increasing DA synthesis and turnover
(Prange, Sisk, & Wilson, 1972) and by increasing the
sensitivity or number of post-synaptic DA receptor sites
(Klawans & Rubovits, 1972). The compensatory increase in
the sensitivity of the receptors has been termed "denervation
hypersensitivity" and has been proposed by Klawans (.1973) as
a hypothesis accounting for the hyperkinetic manifestations
of tardive dyskinesia. Herein, Klawans (1973) has proposed

2Q
that a reduction in dopaminergic neurotransmission caused by
antidopaminergic treatment, resulted in a compensatory
increased sensitivity of the receptors. It has seemed quite
\*ArAr/\/~ Normal
Neuroleptic Action
Tardive Dyskinesia
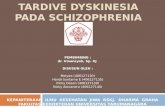
mum Figure 3. Presumed functioning of pre- and post-synaptic
dopaminergic neurons in the nigrostriatal system. (1) Under normal conditions, (2) during neuroleptic blockade ot DA receptors, (3) during hypersensitivity of DA receptors with TD.
likely that TD may be an overt manifestation of the abnormal
responses of such neurons. Figure 3 illustrates this
hypothesis.
Although both increased synthesis and turnover of
dopamine and denervation hypersensitivity have been shown to
be likely compensatory mechanisms for overcoming neuroleptic
blockade of DA receptors, probably the former mechanism has

21
functioned more in earlier stages of neuroleptic treatment
(Davis, Berger, & Hollister, 1979), and has not seemed to be
an important mechanism of abnormal neuronal responses in TD
(Carlsson, 1975; Davis, Berger, & Hollister, 1979; Klawans,
1973; Marsden & Jenner, 1980). However, dopamine receptor
hypersensitivity was present along with a disappearance of
DA receptor antagonism between six months and a year
following the initiation of neuroleptic drug treatment.
In this period, dopamine produced excessive stimulation of
adenylcyclase and the number of DA receptors increased above
control levels. Six months following drug withdrawal,
adenylcyclase activity remained enhanced but DA receptor
numbers tended to return toward baseline. Hence, it has
appeared that hypersensitivity of dopamine receptors in
the striatum was an important factor in the pathophysiology
of tardive dyskinesia.
Pharmacological effects of drugs on tardive dyskinesia
has contributed support to the denervation hypersensitivity
hypothesis. In general, drugs which have decreased dopa-
minergic activity in the striatum have reduced the dyskinetic
manifestations, and drugs which have enhanced activity have
augmented these symptoms. Since it is beyond the scope of
the present work to detail research in this area, the reader
is referred to several comprehensive literature reviews
(Jeste & Wyatt, 1970; Kazamatsuri et al., 1972; Kobayashi, 1977)

22
Drugs which reduce dopamine transmission in the CNS
have been divided into two principal classes: (1) dopamine
depleting drugs and (2) dopamine blocking drugs. Researchers
have demonstrated that dopamine depleting drugs acted by-
preventing intraneuronal storage in presynaptic vesicles.
Because these drugs do not block postsynaptic receptors,
they have not led to the denervation hypersensitivity
produced by dopamine blocking drugs. Among the dopamine
depleting drugs, reserpine and tetrabenzine have been widely
used in the treatment of TD. It has been demonstrated in
numerous studies that they were useful in the treatment of
TD due to their ability to reduce striatal dopaminergic
activity. However, these drugs have produced deleterious
side effects and therefore, they have not been recommended.
It has been demonstrated that dopamine blocking drugs
antagonize dopamine receptors by interfering with cell
membrane function and the respiratory enzymes of cyclic AMP
(Faurbye, 1970; Marsden & Jenner, 1980). Among dopamine
blocking drugs, the neuroleptics pimozide, phenothiazine,
thioxanthene, and butyrophenone, have been widely used in
the treatment of major psychiatric disorders. Their clinical
effectiveness in the treatment of both psychiatric disorders
and tardive dyskinesia has been reported to be due to
reduction in dopaminergic activity. Paradoxically, neuroleptic
drugs which caused TD have attenuated symptoms by

23
reestablishing the dopamine blockade which has been overcome
by compensatory mechanisms of the neurons. Such a treatment
strategy has been shown to perpetuate a vicious cycle between
ever increasing hypersensitivity and higher doses of neuro-
leptics required to reduce symptoms. Thus, it has been viewed
contrary to common sense to treat a syndrome with the drug
that caused it (Casey, 1978).
Other drugs which have been shown to reduce dopaminergic
activity have also been shown to be effective in reducing
symptoms of tardive dyskinesia (Kazamatsuri et al., 1972;
Kobayashi, 1977). These drugs have included lithium carbonate,
alphamethylparatyrosine, papaverine, and alphamethyldopa.
Essentially, drugs which have reduce dopaminergic
activity via depleting stores of DA, blocking DA receptors,
or some other mode of action, all have tended to reduce the
availability of DA to hypersensitive receptors and thereby
have attenuated dyskinetic manifestations of TD. This
evidence has supported the denervation hypersensitivity
hypothesis of tardive dyskinesia.
Other evidence in support of the present hypothesis has
concerned drugs which increase dopaminergic activity in the
striatum. Drugs such as 1-dopa (a dopamine precursor)
(Gerlach, Reisby, & Randrup, 1974) and amphetamine (a drug
which increases DA activity) (Growdon, Hirsh, Wurtman, &
Weiner, 1977), have exacerbated tardive dyskinesia movements.

24
This has been considered further evidence that TD reflected
dopaminergic hypersensitivity (Crane, 1973; Klawans, 1973).
A hypothesis for denervation hypersensitivity of
dopaminergic receptors of the striatum has been presented and
evidenced by pharmacological manipulation of drugs which
have affected these receptors. Despite the expected correla-
tion of drug effects on the dystonic manifestation of tardive
dyskinesia, this model has been unable to account for the
drug effects which have affected cholinergic neurotransmitter
systems and TD. Conclusively, a simple model of hyper-
sensitivity in DA striatal neurons has been inadequate to
fully account for the pathophysiological mechanisms of TD
(Klawans, 1973; Klawans & Rubovits, 1974).
Strategies for cholinergic manipulation of tardive
dyskinesia came about as a result of the observation that
Parkinsonism and TD seemed to be at opposite ends of an
extrapyramidal spectrum of excessive or insufficient dopa-
minergic activity. Based on observations that Parkinson's
Patients benefitted from treatment with 1—dopa and anti-
cholinergic drugs (i.e., increasing the DA/ACh ratio) and
that these strategies worsened or precipitated TD,
researchers reasoned that treatment strategies aimed at
increasing cholinergic activity would be beneficial for TD
(Gerlach et al., 1974; Klawans, 1973; Klawans & Rubovits,
1974) . Hence, Parkinsonism and TD seemed also to be at
opposite ends of the cholinergic spectrum.

25
In initial attempts to demonstrate a cholinergic
involvement, Klawans and Rubovits (1974), Gerlach, Reisby,
and Randrup (1974), and Fann, Lake, Gerber, and McKenzie
(1974), demonstrated that i.v. physostigmine (an anticholine-
sterase inhibitor) improved abnormal movements in patients
with tardive dyskinesia. By augmenting cholinergic
functioning, these studies presented evidence for hypo-
cholinergic functioning in the pathophysiology of TD.
Pharmacological evidence has supported the hypothetical
role of cholinergic activity in tardive dyskinesia.
Numerous studies employing cholinergic agents such as
physostigmine, deanol, choline chloride, and lecithin have
demonstrated effectiveness in the treatment of TD (reviewed
by Casey and Tepper (1979) and Jeste and Wyatt (1979).
Accordingly, anticholinergic drugs such as scopolamine or
benaotropin have worsened TD symptoms in the majority of
patients treated (Gerlach et al., 1974; Klawans & Rubovits,
1974).
The hypothesis for hypocholinergic functioning in the
striatum has been supported by pharmacological studies.
Hence, the inadequacy of a single neurotransmitter model of
TD has been established. Further, research has indicated
that there is a reciprocal balance between cholinergic and
dopaminergic activity (see Figure 1 and 2). From these
conclusions, it has been deduced that there were two

26
pharmacological alternatives for the treatment of TD:
(1) strategies which decrease DA activity and (2) strategies
which increase ACh activity. As previously noted, it has
been deemed unwise to choose the former tactic, since this
could worsen the condition in the long run. Obviously,
strategies aimed at increasing cholinergic activity has been
the treatment of choice.
Hypocholinergic/hyperdopaminergic pathophysiological
mechanisms of tardive dyskinesia have been proposed and
evidenced by pharmacological manipulations. Additionally,
the apparent reciprocal relationship between DA and ACh
activity has been established. However, a neuroanatomical
model whereby these transmitter systems can interact in
order to establish this self-regulatory modulating effect
will further illuminate and support the role of these
biochemical mechanisms in the pathophysiology of TD.
Tardive dyskinesia has been shown to be an extrapyramidal
disorder of the basal ganglia. The striatum comprised of the
caudate nucleus and the putamen has been found to be
principally involved in this disorder. Afferent connections
to this region have been shown to arise principally from
dopamine synthesizing cells in the substantia nigra via the
nigrostriatal pathway and to project to dopamine sensitive
cells in the striatum. Many cells in the striatum have been
shown to be sensitive to cholinergic stimulation. Their

27
afferents are also believed to arise from dopamine synthe-
sizing cells in the substantia nigra. It has been demonstrated
that efferent pathways from the striatum enter the globus
pallidus, the chief motor outflow of the corpus striatum,
and project via the various multi-synaptic pathways of the
extrapyramidal motor system to motor neurons by way of the
rubrospinal, reticulospinal, or vestibulospinal tracts
(Gardner, 1975).
The simplest neuronal model to explain the reciprocal
relationship between dopamine and acetylcholine in the
striatum has been one where the DA neurons of the substantia
nigra send their inhibitory axonal processes rostrally to
terminate on dendrites of small cholinergic interneurons
of the striatum. The only biochemical afferents thus far
identified for this population of cholinergic interneurons
have been the dopaminergic nigrostriatal tract (McGeer,
Grewaal, & McGeer, 1974). The work of McGeer and associates
(1974) suggested that some DA receptors are located on
cholinergic neurons. Moreover, this work suggested that DA
neurons exert a direct inhibitory action on cholinergic
neurons. Hence, the post-synaptic receptors on cholinergic
neurons have been found to be inhibitory. Consequently,
increased activity of dopaminergic activity in the substantia
nigra, due to denervation hypersensitivity, has been shown
to result in inhibition of cholinergic neurons in the striatum.

2:8
This mechanism is illustrated in Figure 4. However, this
mechanism has also been found to be inadequate to fully
account for the reciprocal relationship between DA and ACh
activity. In order to fully account for this reciprocal
Substantia Nigra
via Nigrostriatal Pathway
DA neurons
•\ h Striatum
ACh neurons
iMAMA/ls Figure 4. Direct inhibitory action of DA neurons of the
Nigrostriatal Pathway on ACh neurons of the striatum. (1) Excitatory DA receptors promote depolarization in substantia nigra neurons. (2) Inhibitory DA receptors promote hyper-polarization in striatal cholinergic neurons.
interaction, the model must also provide a means for
cholinergic neurons to influence dopaminergic activity.
In order for cholinergic treatment to modify the
activity of DA neurons, it was reasoned that cholinergic
systems must have input onto DA neurons (Kobayashi, 1977).
Tarsy (1977) has demonstrated that cholinergic agents affect
synthesis, turnover, and release of DA in the basal ganglia.
The mechanism mediating this effect has been shown to be via
a GABA feedback mechanism (Groves, Wilson, Young, & Rebec, 1975)

29
These researchers have demonstrated that striatal cholinergic
interneurons synapse with gabanergic cell bodies on which
they have an excitatory effect. Other researchers have
confirmed that the post-synaptic effects of ACh in the
striatum are mediated by excitatory muscarinic cholinergic
receptors (Kobayashi, 1977; Macintosh, 1979; Tune & Coyle,
1980).
The overall effect of cholinergic suppression of DA
neurons in the substantia nigra have prompted researchers to
formulate a more complete neuronal model of regulatory
mechanisms of DA/ACh modulation (Davis, Berger, & Hollister,
1979; Groves et al., 1977; Tune & Coyle, 1980). This model
is shown in Figure 5. It can be seen from this model that
dopaminergic and cholinergic activity are reciprocally
related through GABA regulatory feedback mechanism.
The pharmacological rationale for cholinergic treatment
of tardive dyskinesia has been established with the validation
of the hypocholinergic hypothesis. Several therapeutic
strategies aimed at increasing the activity of acetylcholine
in the striatum have been presented. These strategies have
been divided into acute versus chronic cholinomimetic action
due to differences in their mode of action on acetylcholine
augmentation (Casey & Tepper, 1979) . The mode of action has
been expressed in view of the mechanisms of synthesis and
degradation of the acetylcholine molecule.

30
(3)
GABA
B
W - / a
Figure 5. Reciprocal interaction between dopamine and cholinergic neurons in the striatum. (A) illustrates that increases in DA activity produce decreases in ACh activity. (1) Depolarization of DA neurons results in hyperpolarization of ACh neurons due to inhibi-tory properties of post-synaptic DA receptors of synapse. (2) Consequently, excitatory ACh transmitter activity is reduced at synapse and (3) inhibitory GABA transmitter activity is reduced at synapse. Hence, DA neurons are free from gabanergic inhibition. (B) shows that increases in ACh activity produce decreases in DA activity. (2) Depolarization of GABA neuron due to the excitatory properties of the post-synaptic ACh receptors at synapse. (3) Inhibitory properties of GABA post-synaptic receptors at synapse promote hyperpolarization of the DA neuron. Hence, ACh neurons are free from dopaminergic inhibition.

31
The following equation represents these reactions:
cholineacetylas^
acetyl Coenzyme A + choline ACh + Coenzyme A
acetylcholinesterase
It has been demonstrated that physostigmine acts in an acute
manner by preventing the degratory enzyme, acetylcholine-
sterase, from breaking up the ACh molecule (Casey & Tepper,
1979). Since these reactions occur only within the neuron
and its adjacent synapse, physostigmine is believed to act
rapidly and directly upon CNS mechanisms. Cholinomimetic
drugs such as deanol, choline chloride, and lecithin have
been considered to act chronically due to increased delay of
therapeutic effects and enhanced central cholinergic tone
(Casey & Tepper, 1979).
Metabolic effects of cholinomimetic treatment has
suggested that their clinical effectiveness was due to
increased cholinergic activity in the striatum. Since it
has been demonstrated that de novo synthesis of choline does
not take place in the brain, brain choline must be derived
from plasma-free choline and lysophosphatidyl choline
(Aquilonious & Eckernas, 1975). Numerous studies have
demonstrated that elevations in plasma-free choline, brain
choline, central ACh levels, and cerebrospinal fluid (CSF)
choline correlate with therapeutic effects of cholinomimetics.
Elevations in plasma-free choline have been demonstrated
following choline chloride administration using both

intraperitoneum injections in rats (Cohen & Wurtman, 1975),
oral administration in rats (Cohen & Wurtman, 1976), and in
humans (Aquilonius & Eckernas, 1975). Further, increased
concentration of brain choline (Cohen & Wurtman, 1976) and
brain acetylcholine levels has been reported in rat studies
(Cohen & Wurtman, 1976; Hirsch, Growdon, & Wurtman, 1977)
and inferred in human studies by a perfect correlation
between physostigmine and choline chloride effects on
tardive dyskinesia (Davis, Hollister, Barchas, & Berger, 1976)
Finally, evidence indicating increase in CSF choline
content (Growdon, Cohen & Wurtman, 1977) has suggested an
increased breakdown of central ACh activity due to an
increase in cholinergic tone, because the net effect of
choline transport has been found to be from the brain to
the CSF.
Just as orally administered, choline chloride has
increased plasma-free choline, so has lecithin. Moreover,
evidence indicated that orally administered choline equiv-
alents of lecithin have produced greater increases in plasma-
free choline (265% over baseline compared to 86%) and longer
lasting effects (24 hours compared to 12 hours) than has
equivalent oral doses of choline chloride (Wurtman, Hirsch,
& Growdon, 1977) .
In conclusion, chronically administered cholinomimetics,
deanol, choline chloride, and lecithin have been assumed to

33
reflect increased central cholinergic activity due to their
correlation with physostigmine treatment (Davis et al.,
1976) and the correlation between the metabolic effects and
treatment effects. Nevertheless, there has been some dispute
whether increased cholinergic tone reflects precursor or
agonist properties of these drug effects.
There has been little dispute concerning the mode of
action of physostigmine effects in tardive dyskinesia.
Contrastingly, the mode of action of the chronic cholinomi-
metics has been controversial. One view maintained that
these drugs act as precursors of ACh (Cohen & Wurtman, 1976;
Hirsch, Growdon, & Wurtman, 1977), while the other held that
they act as agonists which directly stimulate the muscarinic
post-synaptic receptors (Jenden, 1979; Macintosh, 1979).
Increases in free choline and plasma-free choline in
whole brain and caudate regions in rats were taken as evidence
that choline intake into the CNS affects ACh concentration by
accelerating synthesis of ACh (Cohen & Wurtman, 1976).
A later study demonstrated increased ACh activity at the
site of cholinergic terminals following administration of
choline chloride (Hirsch et al., 1977). These results were
interpreted as evidence of enhanced release of the transmitter,
thereby inferring increased synthesis and release of ACh.
Conclusions contrary to these were evidenced by the
transport kinetics of choline into the neuron (Jenden, 1979;
Macintosh, 1979). Choline for ACh synthesis enters the

34
neuron via a choline transport system which was unsaturated
at normal plasma levels of choline. Jenden (1979) and
Macintosh (1979) agreed that 10-fold increases in plasma
choline would have very little (less than 10 percent)
effect on the rate of choline transport. Additionally, they
agreed that only during extreme synaptic activity, which is
certainly not the case in TD, could choline become the
rate limiting factor for ACh turnover (Macintosh, 1979).
Both researchers have concurred that most likely choline
acts as an agonist rather than a precursor.
That choline acts as an agonist is a more tenable
position for several reasons. First, evidence offered in
support of the precursor mode of action has not been
incompatible with agonist effects. An increase in brain
or plasma choline and increased post-synaptic activity would
also occur if the cholinomimetic acted as an agonist.
Second, stores of ACh in synaptosomes of striatal neurons
have been shown to be increased significantly in TD due to
inhibition of the neurons (McGeer et al., 1974). Consequently,
there is no need for increased synthesis to further increase
these stores. Third, transport affinity constants have
suggested that choline is not likely to be taken into the
cell. Fourth, agonist effects have offered a more parsimon-
ious explanation of treatment effect.

35
In Figure 6, a mode of treatment effects in TD which is
consistent with the known pathophysiology of TD as well as
with agonist effects of cholinomimetics is proposed. It is
readily observable that agonist effects on cholinergic post-
synaptic receptors offer a plausible and parsimonious
mechanism for drug action (Figure 6c). It is interesting
to note from this model that treatment does not affect
cholinergic neurons but rather indirectly attenuates the
hyperactive DA neuron via a GABA feedback loop.
Cholinomimetic Treatment Effects on TD
Treatment studies employing physostigmine, choline
chloride, and lecithin are summarized in Tables 4, 5, and
6 respectively. Treatment effects of these drugs will be
reviewed in the following discussion.
Physostigmine treatment. Physostigmine, an anticholiner-
terase agent, was the first drug used to test whether increases
in acetylcholine activity would be effective in reducing
tardive dyskinesia symptoms. Although Fann, Lake, Gerber,
and McKenzie (1974) were actually first to report positive
effects, their initial reports were for the most part
confirmed by their colleagues (Davis et al., 1975, 1976;
Gerlach et al., 1974; Klawans & Rubovits, 1974; Moore &
Bowers, 1980; Tamminga, Smith, Ericksen, Chang, & Davis, 1977).
In contrast, to reports demonstrating effectiveness, Tarsey,
Leopold, and Sax (1974) found no improvement in any of seven

36
s//.|DA
GABA
Figure 6. Pathophysiology and cholinergic treatment effects on striatal neurons. (A) Initial effects of neuroleptic treatment. (1) DA receptor blockade at synapse and (2) facilitates firing of ACh neurons and (3) a consequent inhibition of DA neurons via GABA feedback at synapse. Acute dystonic reactions may result. (B) Late effects of neuroleptic treatment. (1) Hypersensitivity of DA receptors at synapse and (2) inhibits firing of ACh neurons and (3) facilitates firing of DA neurons due to inhibition of GABA feedback at synapse. Tardive dyskinesia may result. (C) Treatment effects in tardive dyskinesia. (2) Cholinomimetics may directly stimulate cholinergic post-synaptic receptors on GABA neurons and consequently inhibit firing of DA neurons via GABA inhibitory post-synaptic receptors at synapse. (3) In turn, reduced firing of DA neurons facilitates firing of ACh neurons. Improvement in dyskinetic symptoms may result.

37
patients treated with physostigmine. A summary of the
results obtained in these studies is presented in Table 4
(see Appendix C).
Of the 55 patients treated with intravenous injection
of physostigmine, 36 patients showed improvement (i.e., 65%)
within about 60 minutes. Improvements were maintained for
up to 24 hours. One of these studies (Fann et al., 1974),
demonstrated a statistical difference between baseline and
treatment measures for severity of symptoms. Conversely,
two other studies (Gerlach et al., 1974; Moore & Bowers,
1980), using a statistical analysis of the data, found no
significant overall treatment effects, but, nevertheless,
reported treatment effectiveness in some of the patients
treated. Several studies (Gerlach et al., 1974; Klawans &
Rubovits, 1974; Tamminga et al., 1977) employed some type
of placebo control strategy. Together, these studies
indicated that 77% of these patients have benefitted from
treatment. The only double blind placebo controlled study
{Tamminga et al., 1977) showed an 83% improvement ratio.
Contrary to expectations, the percentage of patients improved
in open trials (55%) has been considerably less than that
obtained for combined placebo controlled studies (77%).
Although apparent inconsistencies in the expected
effects of control measures on the percentage of patients
improved by physostigmine treatment have been noted, overall,

38
there has been sufficient improvement in patients (65%) to
evidence the beneficial effects of cholinergic enhancement
in the treatment of tardive dyskinesia. However, as a
practical means of long-term treatment, physostigmine has
been inadequate because of the marked peripheral side effects,
the short duration of effectiveness, and the inconvenient
mode of administration. In search of a more practical means
of cholinergic treatment, research efforts have explored
the effectiveness of choline chloride treatment.
Choline treatment. Choline, a precursor of acetyl-
choline, was first used in the treatment of tardive dyskinesia
by Davis, Berger, and Hollister (1975). Following initial
reports of effectiveness, choline treatment has been
investigated in several other studies (Davis et al., 1976;
Gelenberg, 1979; Gelenberg, Doller-Wojcik, & Growdon, 1979a,b?
Growdon, Hirsch, Wurtman, & Weiner, 1977; Tamminga et al.,
1977). These studies are summarized in Table 5 (see
Appendix D).
The total number of patients treated with choline
chloride in these studies is 34. Overall, 59% of the
patients have benefitted from this treatment. Four of the
five studies presented do not employ placebo control measures.
One study (Growdon et al., 1977) employed a double blind
crossover design and reported that 45% of the patients were
improved. This figure is in marked contrast to the 59%

39
improvement ratio reported when all studies were considered
together, and in even greater contrast to the reports of the
combined open studies, which reported a 79% improvement ratio.
Notably, in this instance the design of the study has had
considerable effects on the results.
The daily dose of choline chloride varied from a maximum
of 13.5 grams per day to 20 grams. The study which showed
the lowest percentage of improvement also had the lowest
maximum daily dose of choline (13.6 grams) (Growdon et al.,
1977). Maximum daily doses of choline chloride in the other
studies ranged from 16 to 20 grams per day. In comparing
the treatment results of these studies, variability in
dosage may be one factor which could have accounted for
differences in the percentage of patients improved. However,
it is likely that the single most significant factor
accounting for the difference in percentage of improvement
obtained by Growdon and associates (1977) and the other
researchers has been due to the design employed in the study.
In comparing these studies, another interesting issue
has concerned the use of concurrent medications. In five
of the six studies cited in Table 5, the neuroleptic status
of the patient was unchanged. In contrast, in one study
(Tamminga et al., 1977) all neuroleptic medication was
discontinued two weeks prior to the study. This strategy
has been controversial. Advocates of this method have

40.
maintained that concurrent medications could interact with
treatment effects and thereby obscure results (Jeste &
Wyatt, 1979). However, as evidenced by the number of
studies in which concurrent neuroleptics were unchanged,
most researchers have maintained that discontinuing
neuroleptics worsened the TD symptoms displayed and overall
affected the stability of the baseline measure.
Another point which merits consideration has been that
of discontinuing concurrent anticholinergic medication
(Growdon et al., 1977). This strategy has seemed justifiable
because anticholinergics counter the increases in cholinergic
effects produced by the cholinergic treatment.
A final issue has concerned the treatment duration.
Although the duration of treatment has varied greatly
(from 8 - 6 0 days), beneficial treatment effects were obtained
after eight days of treatment by Davis (1975). Other
researchers have confirmed that this duration is adequate to
obtained treatment effects (Tamminga et al., 1977). The fact
that therapeutic benefits were obtained for up to eight weeks
has suggested that long-term treatment effects are possible.
Overall, choline chloride has seemed to be an effective
and possibly long-term treatment of tardive dyskinesia for
a considerable percentage of patients. However, several
studies have reported adverse side effects due to this
treatment (Davis et al., 1976; Growdon et al., 1977;
Tamminga et al., 1977). Side effects noted were: dizziness.

41
depression, nausea, stomach cramps, diarrhea, increased
salivation, lacrimination, blurred vision, anorexia, and a
fishy body odor. These adverse effects have imposed limits
upon the feasibility of choline chloride treatment of
tardive dyskinesia.
Lecithin treatment. Lecithin or phosphatidylcholine,
is a phospholipid which has been found to occur naturally
in all tissues of the body (Fox, Betzing, & Lekim, 1979).
Moreover, it has been determined that it is the normal
dietary source of choline. As such, this phospholipid-bound
choline has been shown to be a major source of brain choline,
and therefore, has therapeutic potential for tardive
dyskinesia. As previously noted, lecithin has been shown
to produce greater and longer lasting effects on plasma
choline elevations than does choline chloride (Wurtman et al.,
1977) and to increase brain acetylcholine levels (Hirsch &
Wurtman, 1978).
The effects of lecithin on tardive dyskinesia were
first tested by Growdon and associates (Growdon, Gelenberg,
Doller, Hirsch, & Wurtman, 1978). Of the three patients
treated, all showed improvement. Validation of these
results were obtained in later studies (Barbeau, 1978, 1979?
Gelenberg, 1979; Gelenberg, Doller-Wojcik, & Growdon, 1979a, b;
Jackson, Davis, Cohen, & Nuttall, 1981; Jackson, Nuttall,
Ibe, & Berez-Cruet, 1979). A summary of these studies is
presented in Table 6 (see Appendix E).

42
The total number of cases of tardive dyskinesia treated
with lecithin has been 20. These studies have concurred
that all patients treated with lecithin have shown improve-
ment. Conclusions drawn from a cursory overview of these
reports have indicated that lecithin has been an effective
treatment for tardive dyskinesia in all patients. However,
a more critical evaluation should be undertaken before these
reports are accepted.
Overall, the demographic features of the patients
studied represented a heterogeneous group. Sex was
relatively equally represented (7 males and 8 females
reported). Age ranged from relatively young patients (27-32)
(Gelenberg et al., 1979) to middle-aged (mean of 57) (Jackson
et al., 1979, 1981) to relatively elderly (Mean of 64)
(Barbeau, 1979). Collectively, age factors tended to be more
representative of the middle-aged to moderately elderly age
groups (i.e., 67% of patients studied were in this group).
However, the age distribution in this sample, was, overall,
representative of that occurring in the population of patients
with TD, since older patients are at greater risk of
developing TD (Baldessarini et al., 1980; Jeste & Wyatt, 1981),
Essentially, the demographic variables represented in this
sample did not differ from those of the population. Hence, it
is unlikely that treatment effectiveness has been biased by
demographic sampling errors.

4 3
In contrast, several methodological issues may have
biased reported results of treatment effectiveness. The
first issue has concerned the small number of patients in
the sample. The second issue has involved the criteria
used to determine whether the treatment was effective. The
third issue has considered the use of placebo controls.
The fourth issue has regarded methods of assessing treatment
effects.
Statistical sampling is based on the assumption that
the sample is not characteristically different from the
population. When the number in the sample is small, the
statistical probability of sampling error increases. Due
to the small sample reported, lecithin treatment may have
been more effective when applied to this particular sample
than when applied to all patients with TD. Judging from
the percentage of patients improved by other cholingergic
strategies, it appears that lecithin treatment effectiveness
may have been overstated in part due to the small number of
patients thus far treated.
The criteria used to determine whether a treatment is
effective could have significantly biased the results.
In only one study, researchers have performed a statistical
analysis of the data (Jackson et al., 1979). Using a
double-blind crossover design, this study has demonstrated
by use of a one-tailed paired student's t-test, that

44
severity ratings showed a significant difference between
treatment and placebo following eight days of lecithin
treatment (£<.05). This difference was maintained for a
10-day period following discontinuation of treatment.
Although, Jackson and associates (.1981) utilized the same
study as Jackson and coworkers (1979), different schedules
for assessing changes in severity of TD produced consistent
results. Although the latter researchers did not perform
a statistical analysis of their data, an analysis of
variance with repeated measures on one variable (undertaken
by the present author) demonstrated that between day 7 and
day 14 of lecithin treatment a significant (JD < .05) reduction
in symptoms occurred between treatment and placebo groups.
The criteria used to determine effectiveness in all
other studies (see Table 6, Appendix E) was based upon the
percentage of change from baseline scores or upon unstated
criteria. Although such means of assessing changes seemed
to reflect basic overall trends for individuals, it has not
accurately reflected whether treatment effects among the
group treated were of a significant magnitude to demonstrate
that these trends were not a chance occurrence. For example,
Gelenberg and coworkers (1979), using percent of change
from baseline measures, reported improvement in severity
of symptoms for all five patients treated. However, an
analysis of variance with repeated measures on one variable

45
(performed by the present author) disclosed that treatment
effects for these patients were insignificant (jd = 2.5) .
In defense of nonstatistical assessment methods, group
data employed in statistical analysis could have obscured
treatment effects when some patients respond differently to
treatment than others. Some researchers have maintained
that subtypes involving different pathophysiological
mechanisms may exist in TD (Carroll, Curtis, & Kokmen, 1977;
Casey, 1978; Casey & Tepper, 1979; Crane, 1968; Fann et al.,
1977; Gelenberg et al., 1979b; Gerlach et al., 1974; Moore &
Bowers, 1980). If this is shown to be the case, then
statistical measures could have obscured valuable treatment
effects for that subset of patients who responded favorably
to treatment. Nevertheless, it is likely that nonstatistical
analysis of treatment effects in 70% of the patients treated
has contributed greatly to an overstatement of lecithin's
effectiveness.
A third issue has regarded the use of appropriate
placebo controls. Only one study has employed placebo
controls (Jackson et al., 1979, 1981). Although this study
used a double-blind crossover design, these results did not
differ from those obtained in open trials. Despite the
fact that this design has ruled out placebo effects (i.e.,
a positive response to random treatments), it was unable to
evaluate spontaneous fluctuations in symptoms as they occur

4 6
when no treatment is offered, or to detect a general trend
of improvement over time. The importance of assessing change
over time is a viable consideration because there have been
reports of spontaneous rates of remission between 19 - 40%
even when patients continued on neuroleptics (Ananth, 1980).
Moreover, it has been reported that TD could subside spon-
taneously after only a period of a few weeks (Kazamatsuri
et al., 1972), although this was uncommon. Without adequate
control measures, variability in the symptom array and spon-
taneous remission rates could confound drug response results
(Berger, 1980; Casey & Tepper, 1979; Quitkin et al., 1977;
Tamminga et al., 1977). For the reasons stated, it is
beneficial to employ a no treatment control group as well as
a placebo control group. This additional control would
further distinguish placebo and treatment effects from
spontaneous variability or remission.
A fourth issue has regarded the methods of assessing
treatment effects. In the studies reviewed, only two methods
of assessment have been used. One method has been to
assess changes in the frequency of dyskinetic movements.
The other has been to assess severity on tardive dyskinesia
rating scales.
Although the rating scale methods are qualitative rather
than quantitative measures of symptoms, these seemed
preferable for several reasons. First, because frequency

47
measures required videotaping, patients were made very aware
that their symptoms were being obtrusively observed.
Because patients usually have voluntary control over their
symptoms for brief periods of time, they may have self-
consciously limited their movements (Fann et al., 1974;
Kuzamatsuri et al., 1972). In contrast, rating scales could
be completed when the patient was entirely unaware that his
symptoms were being assessed. Second, frequency measures
required the selection of one or two prominent symptoms,
which were reassessed upon each assessment period. Due to
the marked variability in symptoms from time to time, the
researcher could be recording spurious data which did not
reflect the ubiquitous displays of the symptoms. Conversely,
the use of rating scales has permitted evaluation of movements
in all parts of the body. Hence, spurious inconsistencies
reflected in the variability of movements in different body
parts from one assessment period to another has little effect
on the overall rating score. A third problem with counting
movements per minute was the short duration of time sampled.
This method was judged to be far from accurate since rates
of movements oyer a short period of time could vary greatly
from one time to another (Kazamatsuri et al., 1972). A
further problem with this method has been the technical
problem encountered with videotaping. Often shadows obscured
the movements and the three-dimensional characteristics of

48
the movement were lost to the two-dimensional display
(Kazamatsuri et al., 1973). Overall, methods of assessing
treatment effects could have contributed to biased reports
of lecithin's effectiveness.
In addition to the possibility that reports of
lecithin's effectiveness have been biased by various question-
able methodologies, these studies also have failed to
consider a number of other important means of evaluating
treatment effects. Among these were the following:
1. A global assessment of treatment effects as
measured by both researcher's and subject's overall
evaluation;
2. A detailed self-report assessment of symptom
array and severity as measured by the subjects' responses
to the Self-Report Tardive Dyskinesia Rating Scale;
3. An evaluation of subjects' fine and gross motor
performance abilities as measured by several motor tasks;
4. An assessment of speech articulation as measured
by subjects' ability to articulate speech sounds.
In summary, although the present literature has shown
lecithin to be an effective treatment for tardive dyskinesia,
questions have been raised which challenge the validity of
lecithin's reported effectiveness. Overall, the demographic
distribution of the sample of patients studied has not
differed from that of the population. However, other

49
considerations offered have challenged the reports of
lecithin's effectiveness. The small number of patients
sampled could have biased treatment effects by reporting on
a subset of patients with TD. The appropriateness of the
data analysis has been questioned. Overall, a more
conservative statistical analysis of the data seems necessary
in order to substantiate reports of lecithin1s effectiveness
which were obtained largely from nonstatistical data analysis.
The use of inadequate placebo control measures has also been
considered. It has been suggested that an additional
control measure which could reflect spontaneous fluctuation
and/or remission of symptoms would be beneficial. Assessment
measures which assess treatment effects both subjectively
and objectively have been offered as a means of demonstrating
lecithin's effectiveness. Finally, it has been suggested
that additional research is much needed in this area in
order to clarify lecithin's proposed effectiveness in treating
tardive dyskinesia.
The purpose of the present study was to more extensively
examine the effects of lecithin treatment on tardive
dyskinesia with due regard given to the objectionable
methodologies employed in previous studies. The objective
of this study was to evaluate the effects of lecithin
administered under double—blind, placebo controlled conditions
and to compare statistically these treatment effects with

5Q
no-treatment control measures. Further, a more extensive
clinical assessment of treatment effects which employs
subjective, objective, and global evaluations as dependent
measures has been suggested and was believed to be significant
in more thoroughly evaluating the effects of lecithin on
tardive dyskinesia. In accordance with the stated objective,
the following hypotheses were adopted in order to test
lecithin's effectiveness.
1. Symptom severity measures as determined by the
Simpson Tardive Dyskinesia Rating Scale will demonstrate that
lecithin treated subjects, as compared to subjects in the
placebo or no treatment control groups, will show signif-
icantly reduced symptoms subsequent to treatment.
2. Symptom severity measures as assessed by the Self-
Report Tardive Dyskinesia Rating Scale will show a signif-
icant reduction for subjects treated with lecithin as
compared to those in the placebo and no-treatment control
groups.
3. Motor performance as measured by (a) the Finger
Oscillation subtest from the Halstead-Reitan Battery,
(b) the Purdue Pegboard Test, (c) the Minnesota Rate of
Manipulation Test, and (d) a line tracing task will reveal
that subjects in the lecithin group, as compared to those in
the two control groups, will show a significant improvement
subsequent to treatment.

51
4. Integrative sensory motor performance as evaluated
by (a) the Bender-Gestalt Visual Motor Test, (b) the Digit
Symbol subtest from the Wechsler Adult Intelligence Scale,
and (c) the Trails A subtest from the Halstead-Reitan Battery
will show a significant improvement for subjects in the
lecithin group as compared to subjects in the two control
groups.
5. Speech articulation as measured by a modification
of the Speech Sounds Perception subtest of the Halstead-
Reitan Battery will demonstrate that subjects treated with
lecithin show significantly improved speech articulation
while those in the two control groups will show no signif-
icant change.
6. An overall global evaluation of treatment effects
as determined by both researcher and subjects will indicate
that lecithin treated subjects will show significant overall
improvement while subjects in the two control groups will
show no change.
Method
Subjects
Subjects were 45 volunteer male inpatients from the
Veterans Administration Medical Center in Waco, Texas, who
displayed symptoms of tardive dyskinesia. The population
was comprised of the following major psychiatric diagnoses:
schizophrenia (68.9%), organic brain syndrome (28.9%), and

52
bipolar affective disorder (2.2%). Subjects ranged in ages
from 26 to 77. The mean age of the subjects was 56.15
(standard deviation = 9.7). Years of neuroleptic treatment
ranged from 2 to 26 years. The mean length of treatment was
17.29 (standard deviation = 8.5) years.
Criteria for including subjects into the study were
the following:
1. Visible dyskinetic movements of the choreoathetotic
variety, occurring in the orofacial regions and/or in the
extremities following a prolonged exposure to neuroleptics;
2. A duration of tardive dyskinesia lasting at least
3 months, i.e., stable and chronic;
3. No family history of hedepodegenerative disease
that involves dyskinetic movements;
4. No exposure to medicines, other than neuroleptics,
or other treatments that could account for the dyskinetic
movements;
5. A thorough discriminating evaluation of the disorder
to rule out other extrapyramidal disorders and other
differential diagnostic categories.
Criteria for excluding subjects from the study were
the following:
1. Physical disorders in which there is a contraindi-
cation of increased lipid content in the diet, e.g., coronary
heart disease or arteriolsclerosis;

53
2. Physical disorders affecting the gastrointestinal
tract which could be worsened by constituents of the
treatment, e.g., gastric, duodenal ulcers, or chronic
gastritis;
3. Other acute or chronic illness which would prevent
patients from participating in the study.
Details of the experimental study were explained to
subjects randomly selected to be in lecithin or the placebo
treatment group. Following this explanation, each subject
was asked if he would be willing to participate in the study.
Those who chose to participate gave their informed consent
(see Appendix E) and were included in the study according
to the provision of a protocol on tardive dyskinesia
previously approved for the Beckham (1981) lecithin treatment
study by the North Texas State University Use of Human
Subjects Review Board and the Veterans Administration
Medical Center (VAMC) Human Studies Subcommittee. For the
subjects in the no-treatment group, a similar induction
procedure approved by the VAMC Human Studies Subcommittee
was followed (see Appendix G). These subjects were neither
informed of nor offered any treatment.
Subjects evaluated in the present study overlap with
those included in the Beckham (1981) study. Approximately
60% of the subjects participating in the present study had
been included in the Beckham study.

54
Measures
Twelve assessment devices were used to evaluate all
subjects from 3 to 4 days prior to the initiation of treatment
and after 9 to 11 days of treatment. The following measures
were used:
1. Measures assessing symptoms severity include the
Simpson Tardive Dyskinesia Scale (Appendix H) and the Self-
Report Tardive Dyskinesia Rating Scale (Appendix I);
2. Measures evaluating motor performance ability
include: (a) the Finger Oscillation subtest from the
Halstead-Reitan Battery, .(b) Purdue Pegboard Test,
(c) Minnesota Rate of Manipulation Test, and (d) a line
tracing task;
3. Assessment of performance on integrative sensory-
motor tasks include: (a) the Bender-Gestalt Visual Motor
Test, (b) Digit Symbol subtest from the Wechsler Adult
Intelligence Scale (WAIS), and (c) Trails A subtest from
the Halstead-Reitan Battery;
4. Assessment of speech articulation was measured by
using a modification of the Speech Sounds Perception Test
of the Halstead-Reitan Battery (Appendix J);
5. A global overall measure of treatment effects was
obtained by both researcher's and subject's evaluation of
whether or not the treatment had been effective in reducing
dyskinetic symptoms.

55
Procedure
Subjects were randomly assigned to the three conditions
(15 in each group) in an effort to avoid systematic bias due
to subject age, duration of exposure to neuroleptics,
symptom severity, or diagnostic factors. Although the
subjects assigned to one of the treatment groups were
informed that they would receive either the lecithin treat-
ment or a placebo control treatment, neither the patients
nor the researcher knew to which group any individual had
been assigned.
Neuroleptic medication was unchanged in all subjects
participating in the study (N - 41). Those subjects taking
no neuroleptics (N = 4) were maintained on this status.
Anticholinergics were discontinued approximately 3 days
prior to baseline measures for 7 of the subjects. It was
clinically unfeasible to discontinue anticholinergics in
7 other patients. However, only one of these patients was
assigned to lecithin treatment group.
All subjects received their usual diet. No attempts
were made to increase the calorie intake of the patients
in the no-treatment control group.
Lecithin granuals (Lethicon, American Lecithin
Corporation) containing approximately 55% phosphatidylcholine
(see Appendix K) were mixed with 8 oz. of milk. The placebo
substance consisted of a mixture of corn oil and crushed

56
graham crackers. The placebo substance resembled the
lecithin mixture in taste, appearance, and thickness.
These mixtures were dispensed by the hosptial pharmacy and
administered to the subjects in the two treatment groups
twice daily. Subjects in the lecithin treatment group
received a daily dose of 60 grams of the lecithin compound
(33 grams of phosphatidylcholine). Doses were administered
to the subjects by the ward nurse who observed that they
consumed all of the mixture. At the final session, each
subject was informed that the research project was concluded
and thanked for his participation in the research.
Results
A one-way analysis of avariance was performed on
subject variables to determine if there were initial
differences among the groups. These analyses show no
significant differences for age (JD>.2), duration of
neuroleptic treatment (JD >.2), or initial symptom severity
(p- >.2). A chi square analysis of diagnostic categories
demonstrates no significant difference among the groups
(X = 4.8, df = 4, £ >.5). Therefore, random assignment
of subjects to treatment conditions is an effective means of
eliminating systematic bias due to initial differences in
the distribution of subjects among the groups.
Treatment effects are analyzed using a factorial
analysis of covariance. Treatment conditions, age, and

57
length of neurolpetic treatment are the classification
variables. The treatment conditions include a placebo
control group, a lecithin treatment group, and a no-treatment
control group. Age factors are determined by dividing the
subjects according to a median split (median = 56 years)
into younger or older halves. Duration of neuroleptic
treatment factors are determined by dividing the subjects
according to a median split (median = 19 years) into shorter
or longer halves. For each treatment measure, the pretest
score is the covariant and the posttest score is the variant.
Effects of the independent variable, lecithin treatment,
are assessed in terms of a number of dependent measures.
Measures assessing symptom severity include the Simpson
Tardive Dyskinesia Rating Scale (STDRS) and the Self-Report
Tardive Dyskinesia Rating Scale (SRTDRS). Examiner ratings
which employ the Simpson scale show no significant effects
of treatment conditions for the total score (see Table 7,
Appendix L), the total number of scored items (see Table 8,
Appendix M), or the bucco-linguo-masticatory triad (see
Table 9, Appendix N). Subjects' evaluations are measured
by the Self-Report Tardive Dyskinesia Rating Scale. This
measure also demonstrates no significant effect of treatment
conditions. Statistical values determined for this measure
are listed in Table 10 (Appendix 0). Neither examiner nor
subject rating scale measures show any significant change
in symptom severity due to lecithin treatment.

58
Only one measure evaluating motor performance ability
shows significant treatment effects. Measures recorded for
the finger oscillation task are the average score on three
triads of ten second duration. The finger oscillation test
with the dominant hand shows significant effects of lecithin
treatment. The ANCOVA indicates that there is a significant
overall effect of lecithin treatment (p. < .05). Regardless
of the affects of age or duration of neuroleptic treatment,
there is an overall significant reduction in dominant hand
tapping speed. The Newman-Kuels post hoc analysis indicates
that the lecithin group is significantly different from
the placebo control and the no-treatment control groups
(JQ < .05). Statistical values obtained for dominant hand
finger oscillation measures are listed in Table 11
(Appendix P).
Further, the ANCOVA shows that age has a significant
overall effect on dominant hand tapping speed (p.< .0001).
Older subjects are slower regardless of treatment conditions
or duration of neuroleptic treatment.
A significant interaction of treatment conditions and
age is evidenced by the ANCOVA (p <.05). This interaction
is graphically illustrated in Figure 7. Adjusted means for
dominant hand tapping speed for younger and older subjects
are plotted across treatment conditions. The Tukey A post
hoc analysis reveals that the significant difference is

59
CD 4-> rd Ph
o •p (d r-t i—I •H 0 to a
a> 01 a •H
c to <D S t> CD •P 05 S3 T T3 <
50
48
46
44
42
40 -
38 -
36
34
32
30
Figure 7.
A *
X Placebo Lecithin No-Treatment
Control
Interaction of treatment conditions and age for dominant hand finger oscillation rate.
found between younger and older subjects of the placebo group
and younger and older subjects of the no-treatment control
group (£< .05). Younger and older subjects in the lecithin
group do not differ significantly on dominant hand tapping
speed.

6Q
The ANCOVA reveals another significant interaction
between treatment conditions and duration of neuroleptic
treatment. Adjusted group means of short- and long-term
neuroleptic treatment plotted across the three treatment
conditions are shown in Figure 8. The Tukey A post hoc
analysis shows a significant difference between short- and
long-term treated subjects in the placebo group (p< .04).
In summary, the analysis indicates four significant
findings. First, there is an overall significant effect of
treatment conditions on dominant hand tapping speed.
Specifically, tapping speed is reduced in the lecithin group.
Second, there is an overall age effect. Older subjects
perform this task slower than do younger subjects. Third,
treatment conditions and age show a significant interaction.
Lecithin effectively reduces dominant hand tapping speed in
younger subjects. Fourth, duration of neuroleptic treatment
and treatment conditions also interact significantly. The
complexities of this interaction are more difficult to
interpret definitely because the no-treatment control group
measure does not confirm that response differences are due
to duration of neuroleptic treatment factors.
The only factor significantly affecting nondominant hand
finger oscillation is age. Regardless of treatment conditions
or length of neuroleptic treatment, older subjects have a
slower tapping speed (p < .01). Statistical values obtained
for this measure are shown in Table 12 (Appendix Q).

61
CD -P fd Pd
£ o +> d t—i i—i •H O CO O u a> O* d •H Pm £ rd <D s-n3 (L) •P CO 3 *r~l <c
48
46 ~
44 -
42
40
38
36
34
32 -
30
Figure 8.
• • shorter
• longer
JL Placebo Lecithin No-Treatment
Control
Interaction of treatment conditions and length of neuroleptic treatment for dominant hand finger oscillation rate.
The Purdue Pegboard Test measures consist of the total
number of pegs placed in holes for three consecutive trials
of thirty seconds duration. The three trials include
dominant hand performance, nondominant hand performance,
and performance of both hands working together in a

6 o
coordinated fashion. No significant effects are found among
the experimental conditions, nor are age or duration of
neuroleptic treatment effects evident. Table 13 (Appendix R)
lists statistical values obtained for this measure.
The Minnesota Rate of Manipulation Test measures
recorded are the fastest of two dominant hand trials in
which the subject is able to fill all the holes with pegs.
The analysis indicates that there is an overall effect for
duration of neuroleptic treatment (jd < .05) . Regardless of
the treatment conditions, subjects with shorter duration of
neuroleptic treatment perform this task faster. The ANCOVA
indicates no difference among the adjusted means for the
three treatment conditions. Statistical values for these
measures are listed in Table 14 (Appendix S).
The line tracing task measures the total number of
deviations from a straight line of ten inches. The subject's
ability to perform this task is not influenced by treatment
conditions. In Table 15 (Appendix T), statistical values
are listed for this measure.
None of the integrative sensory-motor performance task
reflect differences among the treatment conditions. The
Bender-Gestalt measures recorded are the scores obtained
by use of the Hain's scoring method. Both total score and
categore scores are used in the analysis. Results indicate
no significant effect of treatment. In Tables 16 and 17

63
(Appendixes U and V), statistical values obtained for this
measure are listed. The Digit Symbol subtest and the Trails
A subtest do not show any differences due to treatment
conditions. In Tables 18 and 19 respectively (Appendices
W and X), statistical values obtained for these measures
are listed.
The subject's ability to articulate speech sounds does
not reflect any differences due to treatment conditions.
Statistical values obtained for this measure are shown in
Table 20 (Appendix Y) .
Subjective global measures of treatment effects assessed
by both examiner and subject indicate no globally recognized
difference among the three experimental conditions. A chi
square analysis of the subject's estimate of whether he has
benefitted, not changed, or has become worse indicates that
these evaluations are not significantly related to treatment
conditions (x2 = 1-31, df. = 2, £ < .75, (j>_ = .21) . In the
placebo group 12 of 15 subjects report no change in their
dyskinetic movements, and 3 subjects believe that they are
improved. In the lecithin group, 1 subject reports being
worse, 10 report no change, and 4 report improvement.
Table 21 lists the number of subjects assigned to various
treatment response categories as determined by subjects'
global evaluation of treatment effects. Overall, 67% of the
subjects in the lecithin treatment group report no change

64
in their symptoms. In the placebo group, 80% report no
change.
Table 21
Subjects Assigned to Treatment Response Categories by Self-Evaluation
Treatment Response Categories
Group Worse No Chanae Improved
Placebo 0 12 3
Lecithin 1 10 4
A chi square analysis of the researcher's estimate of
change due to treatment indicates no significant relation
between treatment groups and global assessment (X-2 = 1.05,
df = 4, £ < .95, = .11). The research reports that
13 of 15 subjects in the placebo group show no change and 3
subjects appear improved. In the lecithin group, 12 subjects
show no change, 2 appear improved, and 1 appears worse. In
the no-treatment control group, 12 subjects are unchanged,
2 show improvement, and 1 subject is worse. In Table 22,
the number of subjects assigned to various treatment response
categories by the researcher's global evaluation are shown.
Overall, the researcher assesses that 87% of the subjects
in the placebo control group show no change and 80% of the
subjects in the lecithin group and the no-treatment control
group show no change.

65
Table 22
Subjects Assigned to Treatment Response Categories by Researcher's Evaluation
Treatment Response Categories
Group Worse No Change Improved
Placebo
Lecithin
No-Treatment Control
0
1
13
12
12
2
2
A chi square analysis undertaken to determine whether
the subject and the researcher concur on their global
evaluation of treatment effects indicates that their
evaluations are not significantly related (x2 = -007, df =1,
p = .93, <j>_ = .01). Nevertheless, they are in agreement on
67% of the evaluations.
Discussion
Overall, results of the study do not support the
prediction that lecithin treated subjects will show signif-
icant reduction in dystonic movements and increased control
over voluntary movements and speech articulation. The only
significant finding suggests that lecithin modulates response
rate for rapid dominant hand finger osciallation. The finding
that lecithin treated subjects show attenuated dominant hand
volitional response rates may suggest that lecithin reduces

66
the extrapyramidal motor activity which in turn influences
peripheral motor neuron activity.
Although lecithin treatment is shown to have significant
overall effect in reducing dominant hand finger oscillation,
interesting differential effects of lecithin treatment are
shown by the interaction of age and the duration of
neuroleptic treatment.
The interaction of lecithin treatment and age (see
Figure 7) suggests that younger subjects respond to lecithin
treatment with reduced dominant hand finger oscillation rate,
but older subjects do not. Further, regardless of treatment
conditions, younger subjects perform faster on this task
than do older subjects. Despite this overall effect of age,
the performance of younger and older lecithin treated
subjects does not differ significantly as does the performance
of younger and older subjects in both the placebo and
no-treatment control groups. Hence, due to lecithin effects,
younger subjects' performance becomes nonsignificantly
different from that of older subjects.
The interaction of lecithin treatment and duration of
neuroleptic treatment (see Figure 8) shows that dominant
hand finger oscillation rate differs for short- and long-term
treated subjects in the placebo group. Because there is no
difference in performance between short- and long-term
treated subjects in the no-treatment control group, the

67
significance of this interaction becomes more speculative.
Nevertheless, some trends reflected in this interaction may
be important.
For example, short-term treated subjects of the
lecithin treatment group show a marked reduction in tapping
speed which is notably less, but not significantly different
from the responses of longer-term treated subjects. For those
subjects who were offered no treatment, shorter- and longer-
term treated subjects perform essentially the same on this
measure.
Duration of neuroleptic treatment is not a significant
factor on performance of this task as evidenced by the
performance of the no-treatment control group. However,
shorter-term treated subjects tend to respond with reduced
tapping speed in response to lecithin treatment. In
comparison to responses of shorter-term treated subjects in
the placebo control group, shorter-term treated subjects in
the lecithin group show a markedly diminished tapping rate.
Overall, Figure 8 shows a marked variability in
response to treatment effects in shorter-term treated
subjects. There is virtually no difference in treatment
response for longer-term treated subjects. Hence, it is
possible that duration of neuroleptic treatment affects
subjects' responsiveness to lecithin treatment. That is,
shorter-term treated subjects respond to lecithin by a

68
suppression of dominant hand finger* oscillation while
longer—term treated subjects do not show this response.
Persistence or reversibility of tardive dyskinesia
symptoms represents a conceptual framework in which these
results can be examined. Researchers maintain that TD
occurs along a continuum of reversibility (Casey, 1978,*
Jeste & Wyatt, 1979; Quitkin et al., 1977). When neuro-
leptics are withdrawn, symptoms that resolve are believed
to reflect a temporary alteration in CNS function. Those
which persist are viewed as an indication of permanent
change in the CNS function (Casey, 1978). The reversibility
of TD symptoms by drug withdrawal has been demonstrated in
patients who have taken drugs for a relatively short period
of time (Quitkin et al., 1977) as well as in younger,
nonbrain damaged patients (Jeste & Wyatt, 1979). On the
other hand, persistent TD is believed to reflect irreversible
brain damage (Christensen et al., 1970? Jeste & Wyatt, 1979).
Although the effects of the present study do not
produce remission of TD symptoms, treatment response to
lecithin is specific for a certain subset of subjects who
are younger and have had a shorter duration of neuroleptic
treatment. These results may suggest that for those subjects
who demonstrate a response to treatment, the underlying
pathophysiology represents a temporary alteration in CNS
function. For those who show no treatment response, it is

59
likely that pathophysiology represents a permanent change
in CNS function.
The biochemical mechanism for cholinergic intervention
is believed to be acetylcholine receptors located on post
synaptic gabinergic neuron which feedback onto dopamine
(DA) neurons of the substantia nigra. The effect of this
mechanism is to attentuate the hyperactivity of these DA
neurons. In younger and shorter-term treated subjects,
lecithin treatment effects imply that this CNS regulatory
mechanism is intact, while lack of treatment effects obtained
among older and longer-term treated subjects suggests that
this feedback mechanism is not functional. This model seems
consistent with present findings because, in younger and
shorter-term treated subjects, extrapyramidal outflow
(evidenced by reduced dominant hand finger oscillation) is
attenuated most likely due to suppression of DA neurons.
In older and longer-term treated subjects, DA neurons
apparently are not suppressed and consequently, extra-
pyramidal outflow remains unchanged.
Age and duration of neuroleptic treatment influence
results obtained from three dependent measures. First, age
is an overall significant factor in dominant hand finger
oscillation. Regardless of treatment conditions, younger
subjects perform faster than do older subjects. Overall,
this finding seems to be an indication of a more intact

70
extrapyramidal system. Even when younger subjects show-
response to treatment by reduced finger oscillation rate,
these measures are greater than those of older subjects
under any treatment condition (see Figure 7). Hence, age
effects are displayed ubiquitously and likely reflect the
integrity of the extrapyramidal motor outflow of the CNS.
Second, age is also a significant factor in nondominant
hand finger oscillation. Similarly, younger subjects
perform this task at a faster rate than do older subjects.
Third, duration of neuroleptic treatment is shown to
affect subjects' performance on the Minnesota Rate of
Manipulation Test. Regardless of treatment conditions or
age, subjects who have received shorter-term neuroleptic
treatment perform this task faster. In accordance with
these findings, longer-term neuroleptic treatment may produce
disintegration of this motor system and be reflected in
overall diminished response rates.
Overall, lack of treatment effectiveness seems to be
accurately reflected in the dependent measures. Nevertheless,
possible short-comings of the study should be acknowledged.
Although subjects were randomly assigned to treatment condi-
tions, subjects were not matched for equal distribution of
age and length of neuroleptic treatment factors because this
was unfeasible due to limited number of available subjects.
There is an unequal distribution of these factors. The distri-
bution of subjects to cells in the ANCOVA is shown in Appendix Z,

71
The unequal distribution of subjects could be
problematic for accurate interpretation of interaction
effects. Interpreting 3-way interactions would be
particularly problematic because they represent the greatest
disproportion in cell frequencies. Since no significant
3—way interactions are obtained, this does not affect
present findings. Although less problematic, 2-way inter-
actions may reflect bias due to unequal distribution among
cell frequencies. The ANCOVA indicates a significant
difference in response to lecithin for younger and older
subjects. The particular distribution of subjects to cells
in this interaction (see Appendix Z) does not, however,
suggest the likelihood of strong bias due to disproportional
cell frequencies. The ANCOVA further indicates a signif-
icant difference between the response of short-term and
long-term treated subjects. Herein, the particular
distribution of subjects to cell is more disporportionate
(see Appendix Z). This may have biased results somewhat.
The finding that lecithin attenuates dominant hand
finger oscillation among younger and shorter-term treated
subjects may be regarded only as exploratory data. Because
no other dependent measure showed significant treatment
effects, it is possible that these findings represent a
violation of statistical probability (i.e., finding
significance where none actually exists). Further research

7 2
is necessary before a definitive assertion regarding
lecithin effects on dominant hand finger oscillation rate
can be accepted.
Findings of the present study are in marked contrast
to those of previous studies that found lecithin effective
in reducing dyskinetic movements. A number of experimental
factors may account for these discrepant findings.
Differences in subject population may contribute to
these differences. Subjects' age, duration of neuroleptic
treatment, symptom severity, chronicity, differential
diagnosis, and psychiatric diagnosis may effect treatment
effectiveness.
To determine whether age factors contribute discrepant
findings reported here, mean age and age range reported in
previous studies are examined and compared with those of
this study. The mean age for subjects in this study is 56
(standard deviation = 9.7) years. Ages range from 26 to 77.
In only one study, are age factors notably different from
those reported here (see Table 6, Appendix E) (Gelenberg
et al., 1979a, b). In this study, subjects' ages range from
27 to 32. It is likely that younger subjects are represen-
tative of those patients who exhibit reversible TD. Therefore,
they likely would be more responsive to treatment. Other
studies report beneficial effects of lecithin among
subject populations with age ranges comparable to those

73
of this study. Four subjects with a mean age of 63.7
(standard deviation = 5.8) years (Barbeau, 1979) and six
subjects with a mean age of 57 years and a range from 49
to 60 (Jackson et al., 1979, l98l) all show beneficial
effects of lecithin treatment. Thus it is difficult to
conclude that age is a significant factor which accounts
for the reported differences.
The length of neuroleptic treatment is another factor
which may be significant for treatment effectiveness.
Because patients treated for longer periods do not show
reversibility of dyskinetic symptoms when neuroleptics are
discontinued (Quitkin et al., 1977), it is reasonable to
infer that these patients would De less responsive to
lecithin treatment. Present findings suggest that long-term
treated subjects do not show response to lecithin treatment.
Jackson et al.. (i979, 1^81; reported that the 6 subjects
treated had received neuroleptics virtually continuously for
at least 4 years, although the range was from 4 to 23 years.
Their results indicate that all patients showed a significant
reduction in dyskinetic movements. In the present study,
the average length of neuroleptic treatment is 17,3
(standard deviation = 8.5) years. The range is from 2 to 26
years. Based on similar length of of treatment between
previous reports and the present, it is unlikely that the
duration of neuroleptic treatment can account for the
reported differences.

74
Severity of the tardive dyskinesia may also be a
factor accounting for discrepant reports. In the present
study, average initial severity of TD (measured by the
Simpson scale) is moderate. The range is from mild to
severe. A comparison to previous reports (Table 6,
Appendix E) reveals that the initial severity of TD reported
in other studies does not differ from those reported here.
Hence, initial severity measures do not seem to be a
significant factor which accounts for the reported
differences.
Duration of the tardive dyskinesia measures are largely
speculative because symptom onset is insidious. Because the
course of TD is progressive, severity measures are often
more reliable estimates of symptom chronicity than are
speculations as to its onset. In the present study and in
several others (Barbeau, 1978? Growdon et al., 1978; Jackson
et al./ 1979, 1981), researchers have disregarded the
importance of tne duration of the TD as a crucial factor
affecting the results. Hence, duration of TD is an
unreliable measure and cannot be used as a factor which
accounts for treatment effects.
Criteria for establishing a differential diagnosis of
TD from other extrapyramidal disorders could account for
discrepant findings. However, the criteria for establishing
a diagnosis of TD are believed to have judiciously excluded

75
subjects with other extrapyramidal syndromes in both this
and previous studies.
Psychiatric diagnosis within the subject population may
also influence results. Tardive dyskinesia is more
prevalent in patients with diagnosed organic brain syndromes
(OBS). Reports suggest that these patients are unlikely to
demonstrate reversibility of TD when neuroleptics are
withdrawn (Jeste & Wyatt, 1979). In previous reports,
(Gelenberg et al., 1979a, b; Jackson et al., ±979, 1981) no
subjects had a diagnosis of OBS. In the present study,
within the lecithin treatment group, three subjects (20%)
have this diagnosis. Although it is unlikely that such a
smail number of subjects have significantly affected
results, it is possiDle that including subjects with OBS
may have influenced the present results. Nevertheless, it
seems unlikely that marked discrepancies reported in this
study are fully accounted for by the inclusion of these
subjects.
Other likely considerations which may account for these
differences involve experimental procedures such as, dosage,
length of lecithin treatment, and concurrent medications
are considered.
Dosage is an important consideration when evaluating
response to treatment. Previous research suggests that
lower doses of cholinomimetics, presumed to act as agonists

76
on Gabanergic post synaptic receptors, may be more effective
than higher doses. According to Macintosh (1979),
muscarinic receptors are activated by lower concentrations
of cholinomimetics than are nicotinic receptors. At higher
doses nicotinic receptors are also activated; thereby
promoting both activating and blocking effects. Consequently,
smaller doese may be more effective than larger doses. In
partial support of this contention, Gelenberg et al. (1979b)
reported that larger doses (21 gms per day) of lecithin
for shorter periods (2 weeks) do not produce the positive
effects seen after smaller doses over longer duration
(6 - 8 weeks). However, the interaction of dose and duration
does not necessarily indicate that large doses have blocking
effects. It is more likely that the duration of lecitnin
treatment xs more significant tnan dose size.
Reports of lecithin effectiveness have evidenced a wide
range of dose effectiveness. It can be seen from Table 6
(see Appendix E) that dosages ranging from 2.4 gms per day
to 35 gms per day of lecithin close equivalents have been
reported effective in reducing dyskinetic manifestations.
The present study uses a dose of 33 gms per day which is
within the range of those previously found effective.
Hence, dosage does not appear to be a significant factor
which accounts for the lack of treatment effectiveness.

77
The length of lecithin treatment may affect the
results. Jackson et al. (1979) have demonstrated that
after 8 days of lecithin treatment, lecithin effects were
shown to significantly reduce aystonic movements* However, .
these researchers noted continued improvement through the
i4th and final day of their study. Geienberg et al.
(1979a, b) have noted continued improvement throughout eight
weeks of treatment. Both research teams have, therefore,
advocated continued long-term lecithin treatment intervention,
In previously reported studies, the duration of
lecithin treatment ranged from 2 weeks to 20 weeks (see
Table 6, Appendix E). Statistically significant differences
in severity of TD were noted after 8 days of treatment. In
the present study, treatment lasts from 9 to li days.
According to the findings reported by Jackson et al. (1979)
the length of treatment employed in the present study should
be adequate to obtain significant reduction in dyskinetic
movements. However, since beneficial effects are not
obtained, it is worthwhile to consider that lack of treatment
effectiveness is in part due to the relatively short duration
of lecithin treatment.
Concurrent medications may also be considered a factor
influencing the results of this study. In studies
previously undertaken ana the present, the neuroleptic
medication status remained essentially unchanged.

7:8
However, changes in anticholinergic drugs are called for in
order to assure that these drugs do not counter the effects
of cholinergic treatment. Discontinuation of anticholiner-
gics was notea by Jackson et al. (1979, 1981) and also
employed in the present study. Overall, continued neuro-
leptic medication assures stability of baseline measures as
well as contributes to the efficacy of lecithin effectiveness,
In the present study, the procedures regarding the use of
concurrent neuroleptic medications seem appropriate.
Anticholinergics were discontinued in all but one subject
in the lecithin group. However, it is doubtful that this
has significantly affected the results. Overall, results
are not likely due to variable effects of other medications.
Adequate design is crucial to obtaining clear and
unbiased data. When appropriate control measures are
instituted, experimental error due to experimenter bias and
to placebo effects is reduced considerably. Although
design has been shown to signficantly affect choline
treatment results by reducing the percentage of subjects
improved in open trials from 79% to 45% in a double blind
study (Growdon et al., 1977), design thus far has not been
demonstrated to affect results of lecithin treated subjects.
Studies employing double-blind crossover design to test the
effects of lecithin report improvement in all six patients
treated (Jackson et al., 1979, 1981). Present results,

79
however, offer a challenge to reports of lecithin's
effectiveness obtained in controlled sutdies.
Jackson et al. (1979, 1981) have demonstrated an
impressive differential response to lecithin treatment in
a double-blind crossover, placebo controlled study. The
present study, using a double-blind placebo controlled
design reports no such differences.
Design of the present study, using both a placebo
control measure and a no-treatment control measure, necessi-
tates that treatment effects must differ from both control
measures. Use of a second control measure further reduces
experimental error and increases validity of the results
more than does a design which utilizes a single control
measure.
Other considerations which may account for reported
differences include dependent measures such as subjective
severity ratings and global evaluations.
Means of subjectively assessing treatment effects include
the Simpson Tardive Dyskinesia Rating Scale, the Self-Report
Tardive Dyskinesia Rating Scale, and overall global
assessments of subjects and researcher. None of these
measures evidence beneficial effects of lecithin.
Severity rating scales are commonly used to evaluate
treatment effects. Previous studies (Gelenberg et al.,
1979a, b; Jackson et al., 1979, 1981) have reported reduced

80
severity of dyskinetic movements reflected in these measures.
Present results do not confirm these reports. However, it
is possible that differences in the scales used account for
some of these discrepancies.
Previous studies (Gelenberg et al., 1979a, b? Jackson
et al., 1979, 1981) have used the Abnormal Involuntary
Movement Scale (AIMS). The present study uses the Simpson
Tardive Dyskinesia Rating Scale (STDRS). Differences in
reports of lecithin's effectiveness may be attributable in
part to differences in what the scales measure. First, the
AIMS distinguishes between the severity of the movement on
a 5 point scale. The STDRS uses a 6 point scale. Second,
only 7 grossly localized areas are distinguished by AIMS
and only one rating is made for each affected area. The
STDRS lists 34 discrete localized movement disorders and
allows rating on each individual type of dystonic movement.
Third, the AIMS uses overall global evaluation. Three of
the 12 items on the scale are used to evaluate these global
measures. No global measures are reported by the STDRS.
Essentially, the main difference in the scales is that
the AIMS yields a very global and nondiscrete estimate of
the severity of dystonic movements, while the STDRS permits
a very discriminating evaluation of the symptom array.
Further, it is likely that the specificity which the STDRS
permits encourages the rater to carefully evaluate in a

81
methodological manner, the presence or absence and severity
of each dystonic movement displayed. In contrast, the rater
using the AIMS is forced to make gross generalizations about
the severity of movements in fairly large body areas.
Overall, a more precise evaluation is possible with the STDRS.
It is contrary to common judgment that an instrument
which permits largely global evaluations would be more
revealing of treatment effects than would one which allows
discrete evaluation of subtle movement characteristics.
Thus, the lack of treatment effectiveness found in the
present study cannot be accounted for by weakness of the
STDRS to reflect changes in movements. Overall, the ability
of the STDRS to precisely and distinctly assess the array of
diskinetic movements is judged superior to that of the AIMS
scale. This must be taken into account when comparing the
results obtained from the STDRS with those obtained form
the AIMS.
Differences in the way the severity rating scales are
used may also account for the discrepant findings. The
length of the rating period may contribute to differences.
Longer rating periods would naturally increase the total
number of symptoms displayed as well as the overall reliability
of symptoms noted. Because the interval of the symptom
occurrence may exceed the length of the rating period, a
problem associated with using shorter rating periods is the

82
considerable variability of symptoms displayed. Accordingly,
Jackson et al. (1979, 1981) noted that AIMS subscores do not
demonstrate consistent differential change. This is likely
since the short duration of assessment would likely not
reveal a ubiquitous display of the total symptom array.
The longer rating period is superior because ample time is
allowed for assessing symptoms and establishing a reliable
baseline of symptom array. The present study demonstrates
reliability of differential components which is evidenced
not only in the no-treatment control group, but in both the
lecithin treatment group and the placebo control group.
Increased level of extrapyramidal outflow may also
contribute to reported differences. Severity of dystonic
movements increases with increased levels of arousal. Since
in the present study symptom severity ratings are assessed
during states of motor activity on timed performance tasks,
it is possible that lecithin treatment effects which might
be demonstrated at lower levels of motor activity are masked
at higher levels of EPS activity.
In support of this supposition, some researchers
(Tamminga et al., 1977) have suggested that cholinomimetics
may act as a generalized sedative. If lecithin acts through
a generalized reduction in EPS outflow, possibly at increased
levels of motor activity, sedative effects are counteracted.
Thus, the discrepant reports of lecithin's effectiveness may

83
be attributable to differential effects of lecithin which are
due to the level of activity of the extrapyramidal motor
system.
Subjects' awareness can also affect severity ratings.
As previously noted, subjects can volitionally control
dystonic movements for short periods of time. Accordingly,
subjects' awareness of rating procedures in noncontrolled
studies (Gelenberg et al., 1979a, b) is likely to affect
results. However, in highly controlled studies (Jackson
et al., 1979, 1981), it is unlikely that results are
attributable to subject awareness. Therefore, subject
awareness is not a likely factor which accounts for discrepant
reports of lecithin's effectiveness.
The preceding discussion has addressed issues concerned
with reported differences of lecithin's effectiveness as
assessed by symptom severity measures. Studies assessing
lecithin's effectiveness in terms of frequency measures have
not been considered because changes in symptom severity are
not necessarily related to change in frequency. Therefore,
results of this study neither address nor preclude the
validity of findings that lecithin reduces the frequency of
dyskinetic movements. To the contrary, it is quite possible
that lecithin's effects produce changes in the frequency of
movements without affecting the severity (i.e., amplitude)
of the movement.

84
Self-report measures are another means of evaluating
treatment effectiveness. The Self-Report Tardive Dyskinesia
Rating Scale and a global evaluation indicates that subjects
in the present study are not aware of improvement in their
dyskinetic movements. In contrast, Barbeau (1979) in a
noncontrolled study notes that subjects report a marked
improvement in muscle tension felt in the face and neck.
It is likely that these reports are confounded by the
positive expectancies of subjects, since no controls were
instituted.
Studies which employ self-report measures (Barbeau,
1979; and the present study) find that these measures concur
with the overall reported effectiveness of lecithin.
Essentially, subjects* reports appear to be a valuable means
of assessing treatment effects provided that adequate control
measures are used. However, subjects' reports of treatment
effectiveness in noncontrolled studies may reflect subject
expectancy and thus account in part for discrepant reports.
Data analysis is one of the most important factors
affecting treatment results. Of the lecithin treatment
studies only the study undertaken by Jackson et al. (1979,
1981) demonstrated a statistically significant difference
between lecithin and placebo control groups. All other
studies have interpreted their results from a non-statistical
percentage of change from baseline.

85
According to Davis et al. (1976), results of any study
evaluating treatment effects on tardive dyskinesia must be
interpreted with great caution because TD is characterized
by extreme variability from day to day. They reported that
day-to-day fluctuation in symptomatology can vary by 25% in
either direction which makes reports based on percentage of
change from baseline subject to a great deal of experimental
error. Of the total number of patients thus far treated
with lecithin, 70% of the reported findings are based on
this type of analysis. Further confounding these results,
it should be noted that all of these studies employ no
control measures to rule out positive expectancy. Hence,
results reported for most patients are subject to viable
criticism regarding experimental error due to spontaneous
fluctuations in symptoms.
Using a one-tailed paired student's t-test, the Jackson
study demonstrates a significant difference (JD <. .05) in
mean total AIMS scores following eight days of treatment.
The greatest difference is demonstrated on the 14th and
final day of treatment (p < .01). The double-blind corss-
over design lends further credibility to this report
because placebo effects and researcher bias are effectively
eliminated. Differences in subjects' responses to treatments
are impressively demonstrated in this repeated measures
design. The present study reports finding to the contrary,
despite the fact that statistical methods are appropriate.

86
The difference in reported treatment effects obtained from
these two studies does not seem to be due to statistical
error. Nevertheless, the lack of statistical analysis in
70% of the cases reported may account for some of the
reported differences.
Summary and Conclusions
Present findings do not indicate that lecithin is an
effective treatment for tardive dyskinesia. Findings
suggest that lecithin has an attenuating effect on dominant
hand finger oscillation for some subjects with tardive
dyskinesia. This suggests that lecithin may have an overall
effect of diminishing the rate at which extrapyramidal
motor outflow influences peripheral motor neurons.
A number of factors which may explain the lack of
treatment effectiveness have been explored. Although most
of the factors discussed are ruled out as plausible consider-
ations accounting for lack of treatment effectiveness,
several variables may be significant. If, indeed, lecithin
is an effective treatment for tardive dyskinesia, it is
possible that the inclusion of subjects with organic brain
syndromes and the short duration of lecithin treatment have
obscured treatment effectiveness. Since subjects with
known central nervous system lesions may manifest irreversible
tardive dyskinesia, lack of responsiveness in these subjects
could have concealed overall treatment effectiveness, but

87
this is doubtful. Because all of these subjects fell into
the older age grouping, statistical analysis would have
partitioned out this subtest of subjects and distinguished
them from younger subjects who were more likely to respond
to treatment. It is unlikely that the inclusion of QBS
subjects contributes significantly to lack of treatment
effectiveness. The short duration of lecithin treatment
may contribute to the lack of treatment effectiveness.
Although previous studies report beneficial effects after
8 days of treatment, continued improvement is reported for
up to 2 months. Longer treatment would likely promote
large, more discernible changes. This issue seems to be
a valid point of criticism of this study.
If, on the other hand, lecithin is actually not an
effective treatment for tardive dyskinesia, several factors
may be responsible for reducing experimental error, and
thereby, demonstrating that lecithin is ineffective in
treating tardive dyskinesia. The double-blind design which
employs both placebo control and no-treatment control groups
considerably reduces experimental error due to subject
expectancies, researcher bias, and baseline variability of
the syndrome. The Simpson Tardive Dyskinesia Rating Scale
reflects precise characteristics of the disorder and
demonstrates reliability of baseline measures. Longer rating
periods are effective in reducing experimental error due to

88
variability of symptom displayed over shorter rating sessions,
By use of appropriate statistical measures, the probability
of drawing erroneous conclusions is greatly reduced.
Another possibility is that lecithin effectiveness is
contingent upon the level of extrapyramidal arousal.
Perhaps, lecithin effects are notable during quiescence, but
not during states of increased extrapyramidal arousal.
These results suggest that during states of increased
extrapyramidal activation, dystonic movements remain
essentially unchanged from baseline measures.
In conclusion, results do not support previous findings
that lecithin is an effective agent in reducing tardive
dyskinesia. Due to the many variables involved in comparing
the results of this study with those reported previously,
a definitive conclusion regarding the efficacy of lecithin
treatment becomes an issue of conjecture which must be
addressed in future research efforts. The findings of this
study raise valid questions regarding the beneficial
effectiveness of this treatment. Hopefully, these findings
will contribute to more realistic evaluations of lecithin
treatment effectiveness and stimulate further investigation
of more effective means of treating tardive dyskinesia.

89
Appendix A
Table 1 Antipsychotic Agents
Commercial Name Generic Name
Phenothiazines: Compazine Etrafon (Triavil) Largon Levoprome* Mellaril Phenergan Proketazine Prolixin (Permitil) Quide Repoise Serentil Sparme Stealzine Thorazine Tindril Torecan Trilafon Vesprin
Butyrophenones: Haldol Innovar*
Thioxanthenes: Navane Teractan
Prochlorperazine Perphenazine and amitriptyline Propiomazine Methotrimeprazxne Thioridazine Promethazine Carpenazine Fluphenazine Piperacetazine Butaperazine Mesoridazine Promazine Trifluoperazine Chlorpromazine Acetophenazine Thiethylperazine Perphenazine Tr i f1uproma z ine
Haloperidol Droperidol
Thiothixene Chlorprothixene
*Not marketed as an antipsychotic (Schiele et al., 19/3)

9 . Q
A p p e n d i x B
£> tO
w 0 c *H
w >1 o
13 J-f (C
J-i 0 M-i
10 0 •H
o o> 0 -p fd o
V •H 4J to o c & =13
0 u H 3 c CO
r-r-cr>
•»• i—i CO r- •. o -H v H £ 4J
0} i-> - >* fd » (0 >( c XI s: fd 0 > ^ *
!d r-{ 0 ^ vC 4J
r- to »»c\ o 00 H b vO
H C O r-
*> rJi CTN d) ifl H G •—i a M -SH fd tO D O G
rc • » ^
in to v o r - H O
on ^ oo H H a>
-8 RH
H H N fd (d -P 0
0 .Q +J 4J O U 0 0 0 0
cc a; c ->1 0 k •* JQ TJ O X) ^ « c o> 3 U G p-fd fd fd ON ^ S E ^ h
o 00 ON rH
u 0 cn
0 03
o in 00 r-cr> o> r—f rH
JH , 0 v£» vo rH vO CT> t— r- (0 r-i-( <Ti a 0 1—1 rH -J -H a 0
•> -H -H G *H C\ ON ON G C 0 c— r— r— -f-t -H 13 •H
<r» ^ M W Jh h h h cd rd fd
co to fd to * - •> ifi w 2 to . . . 0 0 0
H H H T J H3 »% u rd <d n) h co oo oo n 00 rH
fd £> vo (d VD 03 4-> 4-J -P CD 0> Ox* ft} ON ffi 0 0 0 H H H rH
>-£ *-ii U U U - v . «. 0 0 a > i 0 0 0 j x , 0 >i G G G W G G G t O G to C G G U f C f C t O U rd M ( d a J r t f f d ^ ^ M r d <d E - ' h h ^ O U U h O H
03 0 •H
0 CT 0 •P fC O
U •H •P W 0
S (0 •H a
fd •H 4J G a>
0 *h
Q
to <d *H CO <D G •H r* W >i a
w 3 O o a (0 •P c
a w
c 0 w
O
0 I—I •H c 0) CO 0
pu
w fd •H 10 0 G •ri
GO
Q
1? 0 -P fd rH 0 OS
>i 0' C «—f o rC •P fd CM
W 0 U (0 0 fd TJ 0 *H (0 O -H
G O -H -P <d i-j O •H U
0) 0 £ 4i O 0 iH *0 U G O
Q] (1) K M W O (3fC (fltJ O •H "O t) (I) M C r C TJ W - H 0 O -H O
- > to w co m o H C (0 - "H «H V-t rH (0 O U E ^ ' O X I (d U -P 0> (0 •H Di rC U} U O U D C IC C - -H -H *H C - H 0 0 G - P G G h + » o » id o O C O C B1 U P A >^-H 03 ^ a u w s d i O u <Li 5Z
SO M 0 73 SH 0 (0 •H T3 +J
G O £ 0 >
O £
a •H iH <G ,c ft 0 CJ C 0 +J
W o a
to £ to •H U
to 0 fd G •H G to <d 0 £ G •H u * •rH % G
0 to V U fd
rG •H rH a to to £ fd O 0 0 to u N ft G 'H *H •H >, *H T3 D r C r* -H O 0 0 to o rH to 0 !>« U 0 u U u U 0 p •H u oJ 0 G to •rH G O rH 0 O ti U O ft
X & G XI >H U U fd (d ffi
4J CO 0 & S

Appendix B—Continued 91
<0 V u p o w
GJ P G
• H -p G 0 u 1
XI r0
O 00 ON
u QJ
QJ CQ
O O O 0 0 0 0 CO O N 0 > ON
oj D o H H H t* >< >1 0 0 0 O O V
QJ QJ C C P P P
cn H H H v r- r- r-• r- r- r-
H O N O N ON H) r| H H O O 00 00
- P •> •» «• O N O N (D -H *H t) H H 43 43 43 c to to to * QJ d d d M M T3 >i>i>i(D (D to d d d 0> cn M 43 43 .Q u U d O 0 O QJ <D S ca tn
(0 d •H (0 to <D 0) •H c CO •H O d o» •H (0 0) to >1 +> QJ •0 (0 C u * H to X a
O (0 GJ c • H >1 W 0 Q d u • H « •H 0) 4-> 0 u WOE O c fl> 0) P CO d D» o C TJ 'H 0) d p •HOC U • H T» ^ U 0 0 o G to ft to o E w >i C • H <U o r—1 T J W - H c E $-i d >i O 4 0 O *0 •H i—l •o -H 4 U c -p r—1 Q> +J d d to H3 N c d O QiCu • H C « 0 o p <1) 1 50 TJ >i k * H TD H O •H to +» QJ c C CD£ <U • H 4-4 0> •H 3 +i d 4-1 u> D (U d 3 (0 X5 • H 0 oi a> w 0 * H d Q u P S C U C < & I OS
d Q M
o H 00 r-ON ON rH
M in >1 0) r-- -P o*<y« 4-> U iH d 0 <D CQ <• CD d ,v E w8 ON to <0 r- <D ON <.
ON CQ rH Tf fH O we O • £ • ^ rH U <H (!) d QJ d to TD d -P G «p X (I) D Q) U
«
U * >i U 0 JS 43 QJ C O U 43 G d P O d 43 d P EH 0-I fa w
to d •H W4J to d g Q) -H d G 10 -P •HOW X c o K-H D >*x c T3 W O O •CO (D d) TD •P T3 d OJ 0) "HOC QJ P -H U 13 E G (0 0>-H -p 3 tQ i-l d *H Q ft43 O -H M T 3 4-> 0 I G
I C H < 1 -P o
to d •H Q> C •H X 10 >i T3 13 QJ O 3 *0 G •H
a ra o 43
- P
(D > •H CO •H > c O O o u ±> o QJ
d rH JQ •H TJ C d I u o
d
TS <D 43 (0
o r- XJ oo r- p O N O N ft ri H C
P u o •> QJ "0 £ G 3 d c o; .c O O QJ 00 CD b U ON O* (D
H H tfl U CQ 0) -U U <D C QJ <D TD Q> (1) CJ1DW ftu J-4 M in i-i -H QJ OJ (0 d M CQflSUC
•H P (0 Q P 0) to 6H Q G d v« £H •H •H w8 CO QJ ws to a) C ft G O >i QJ u •H •H •P E JJ O O to 0 QJ M QJ o to
>i d M T3 QJ o to Q Q o QJ G P 0 EH k4 •P >i •O E 4-i to W C O O w» CJ Q •H M •H EH O G T3 to E G •H *H t*. C Q) W O c d rH >i E •H -P QJ 4 rH t0 O G to d M XJ d U O >i-H 43 o o> TJ to T3 to ft O • H c c G •H O -H +J -H >i •H <D 43 N G Q) > CO -P • H d rC QJ H 3 d 43 tJ» +J 43 H 3 to UA: o u W o 0 ft < < w o 0 X M • H CU 2

92
Appendix C
Table 4 Studies Using Physostigmine
in the Treatment of Tardive Dyskinesia
Study Subjects TD Characteristics
Number
Duration of
Age Sex TD
Severity Maximum of Daily TP Dose
Fann, Lake, Gerber 7 & McKenzie (1974)
55-70 1M chronic mild 40 mg/kg i.v. to with meth-
severe scopolamine
Gerlach, Reisby, & Randrup (1974)
44.7 5M 25 N.S. 1 mg i.v. (20-69) months with meth-
(2-96) scopolamine
Klawans & Rubovits 12 55.8 5M (1974) (39-71)IF
N.S. N.S. 1 mg i.v. with meth-scopolamine
Tarsy, Leopold, & Sax (1974)
47-67 6M IF
chronic 1-1.5 mg i.v. with meth-scopolamine
Davis, Berger, & Hollister (1975)
39 1M N.S. N.S. 3 mg i.v.over. 30 min. with
methscopolamine
Davis, Hollister, Barchos, & Berger (1976)
N.S. 4M 3 chronic N.S. (1-2 years) 1 recent (3 months)
3 mg i.v. with meth-scopolamine
Tamminga, Smith, Ericksen, Chang, & Davis (1977)
25-73 3M N.S. moderate 0.5-2 mg to with meth-
severe scopolamine
Moore & Bowers (1980)
10 N.S. 2M at least N.S. 8F 6 months
2 mg i.v. with meth-scopolamine

93
Table 4--Continued
Procedures Data Results
Duration of
Treatment
Design Concurrent of Medications Study
Assessment Measures Analysis
acute reaction (24 hrs.)
all continued open severity
t-test 6 a l b
(signif-icant)
acute reaction
all continued
single blind scopolamine
frequency Wilcoxon & severity test (non-5 a
combined signif-formula icant)
3 b
acute reaction (60 min.)
8 continued 4 off medi-cations
single blind scopolamine performance non- 10a
edrophonium task statis-controls tical
2 b
acute reaction
5 continued 2 off medi-cations
open 0 a 7 b
acute reaction
N.S. open frequency non- 10a
statis-tical
2 b
acute reaction
1 continued 3 off medi-cations
open frequency non-statis-tical
4 a 0 b
acute discontinued reaction 2 weeks
pretrial
double blind neostigmine & methexital controls
severity non-(Smith statis-Scale) tical
5 a 1 b
acute all continued reaction medications
open frequency per 1 min.
5 a 5 b paired t-test (not significant)
Improved
'unimproved

94
Appendix D
Table 5 Studies Using Choline Chloride
in the Treatment of Tardive Dyskinesia
Study Subjects TD Characteristics
Number Acre
Duration of
Sex TD
Severity Maximum of Daily TD Dose
Davis, Berger, & Hollister (1975)
1 39 1M N.S. N.S. 16 gms
Davis, Hollister, Barchas, & Berger (1976)
4 N.S. 4M 3chronic N.S. (1-2 yrs.) 1 recent (3 months)
16-20 gms
Tamminga, Smith, Ericksen, Chang & Davis (1977)
4 45 2M N.S. moderate to
severe
18 gms
Growdon, Hirsch, Wurtman, & Weiner (1977)
20 N.S. 5M stable, N.S. about chronic 13.6 gms
(200 mg/kg)
Gelenberg, 5 27-32 5M chronic mild Dollerwojcik, (1-5 yrs) to Growdon (1979a, b) severe
12-17 gms

Appendix D—Continued 95
Table 5—Continued
Procedures Data Results
Duration of Concurrent
Treatment Medications
Design of
Study Assessment Measures Analysis
8 days N.S. open frequency non- la
statistical 0b
15-21 days 1 continued 3 off medi-cations
open frequency Mann-per 45 Whitney
2 failed test
3a lb
15-21 days discontinued 2 weeks pretrial
open severity non- 2a
(Smith statistical Scale)
2b
14 days 13 continued double with 7 off medica- blind 10-day tions, discon- cross washout tinued anti- over
ACh medication
cL 3D frequency non- 9 11 per 30 statistical
6-8 weeks (42-56 days)
4 continued 1 off medi-cation
open severity (AIMS SCALE)
non-statistical {% change fm baseline)
5a 0 b
Improved
^Unimproved

96
Appendix E
Table 6 Studies Using Lecithin in the Treatment of Tardive Dyskinesia
Study Subj ects TD Characteristics
Duration Severity Maximum of of Daily
Number Acre Sex TD TD Dose
Growdon, Gelenberg, 3 N.S. N.S.N.S. N.S. 40 gms @ 16% Dollerwojcik, 8 0 gms @ 4% Hirsch, & Wurtman 60 gms @ 4% (1978)
Barbeau (1978) 2 N.S. N.S.N.S. N.S. 49 gms @ 20%
Gelenberg, 5 27-32 5M chronic mild 105 gms @ 20% Dollerwojcik, to & Growdon severe (1979a, b)
Barbeau (1979) 4 63.7 1M chronic N.S. 49 gms @ 20% (±5.8) 3F (7.2+2. 1 (±5.8)
years)
Jackson, Nuttall, 6 57 1M N.S. moderate 50 gms @ 70% Ibe, & Perez- to Cruet (1979) severe
Jackson, Davis, 6 57 1M N.S. moderate 50 gms @ 70% Cohen, & Nuttall (49-60) to (1981) (reported on severe same study as Jackson et al., 1979a)

Appendix E—Continued 97
Table 6—Continued
Procedures Data Results
Duration Design of Concurrent of Assessment
Treatment Medications Study Measures Analysis
2 weeks to 2 continued open frequency non- 3a ok 2 months 1 off per 30 sec. statistical (14-60 medication (% change fm days) baseline)
N.S. N.S. open frequency non- 2a 0b
per 5 min. statistical
6-8 weeks 4 continued open severity non- 5a 0b
(42-56 days) 1 off (AIMS statistical medication Scale)
average of N.S. open frequency non- 4a 0b
20 weeks per 5 min. statistical (140 days) avg. max.
final improvement
14 days 5 continued double severity paired 6a ob
with 10 day 1 discontinued blind (AIMS students washout medications cross- Scale) t-test period 2 weeks prior, over signif-
discontinue anti- icant ACh medications
14 days (same as double severity non- 6a ob
with 10 day previous blind (AIMS statistical washout study) cross- Scale) period over
Improved
^Unimproved

98
Appendix F
Information about Lecithin Therapy for Tardive Dyskinesia
Tardive dyskinesia is a well recognized side-effect of a large number of medications used in psychiatric treatment. Tne disorder usually involves involuntary movements in the mouth, face, tongue, or hands. Movements often persist for months to years after the medication which causes the diosrder nas been discontinued.
There is no known treatment for the disorder. However, recent research has suggested that lecithin, a nutrient found in eggs and soybeans, may be a treatment for tardive dyskinesia. This study is being undertaken to investigate the effectiveness of lecithin as a treatment for tardive dyskinesia.
If you participate in this study, you would take an addi-tional medication in the morning tor two weeks. The medication, which will be mixed in a glass of milk, would either be lecithin or another substance which has no effect on tardive dyskinesia symptoms. Neither you, your doctor, nor the experimenter would know which substance you had taken until the experiment is over.
You would also be videotaped four times—once before and once after the study, as well as twice while you were taking the study medication, uach tape will last about 5 minutes. You would be taped here at the hospital and the tapes will toe rated by people assisting in this research. Your identity as a participant would not be revealed in any puDlished or oral presentation of the results of this study. The tapes will be destroyed after they are rated.
The experimental medication may make your tardive dyskinesia symptoms worse, better, or may have no effect at all. The effects of the experimental medication probably will not last after you are no longer taking it. No side effects are expected, but if any occur, you would notify your ward nurse or doctor immediately. All your other medications and therapies would continue as usual. You would be free to withdraw from the study at any time.
The experimenter is available to answer any questions you have about this study and you may also wish to consult your doctor. After the study is over, the experimenter will be

Appendix F—Continued 99
available to tell you wnicn substance you took and to explain the outcome of the study.
In the unlikely event you are injured as a result of participation in this study, the Waco VAMC will furnish medical care as provided oy Federal statute. Compensation for such injury may be available to you under the provis-ions of Title 38, United States Code, Section 351, and/or the Federal Tort Claims Act. For further information, contact the VA District Legal Counsel at 756-6511, ext. 626,
I' certify that the above written summary was discussed and explained fully to me by Lynn A. Price on this date.
Date Subj ect
Witness
Witness

100.
Appendix G
Information about Variability in the Short-Term Re-Evaluation of Symptom Severity
in Tardive Dyskinesia
Tardive dyskinesia is a well recognized side effect of a large number of medications used in psychiatric treatment. The disorder usually involves involuntary movements in the mouth, face, tongue, or hands. Movements often last for months to years after the medications which cause the disorder have been discontinued. Perhaps you have noticed some of these movements in your body.
Because we do not know how you are affected by the extra movements, we are going to be testing some patients in the hospital so that we can find out more about tardive dyskinesia. If you participate in this study, you will be asked some questions about how you have been feeling and whether you have noticed or are bothered by the extra movements that you may have noticed. Also, you will be asked to do a few simple things with your hands to listen and repeat some sounds. If at any time you wish to with-draw from the study, you may do so. If you participate in this study, your identity as a participant will not be revealed in any published or oral presentation of the results of this study. The results will be incorporated in a doctoral dissertation to be deposited in the library of North Texas State University.
If you have any further questions, the experimenter or the staff psychologist will be available to answer your questions,
In the unlikely event you are injured as a result of parti-cipation in this study, the Waco VAMC will furnish medical care as provided by Federal statute. By participating in this program you will not waive any legal rights or remedies available to you, nor will you waive any VA benefits to which you may be entitled.
I, , certify that the above written summary was discussed and explained fully to me by Ms. Lynn Price on this date.
Date Subject
Witness Experimenter

Appendix H
The Simpson Tardive Dyskinesia Rating Scale (Full Scale)
101
Patient
Date
Setting
FACE
1. Blinking of eyes 1 2 3 4 5 6
2. Tremor of eyelids 1 2 3 4 5 6
3. Tremor of upper lip 1 2 3 4 5 6 (Rabbit syndrome)
4. Pouting of lower lip 1 2 3 4 5 6
5. Puckering of lips 1 2 3 4 5 6
6. Sucking movements 1 2 3 4 5 6
7. Chewing movements 1 2 3 4 5 6
8. Smacking of lips 1 2 3 4 5 6
9. Bon bon sign 1 2 3 4 5 6
10. Tongue protrusion 1 2 3 4 5 6
11. Tongue tremor 1 2 3 4 5 6
12. Choreoathetoid movements of the tongue 1 2 3 4 5 6
13. Facial tics 1 2 3 4 5 6 14. Grimacing 1 2 3 4 5 6 15. Other (describe)
1 2 3 4 5 6 16. Other (describe)
1 2 3 4 5 6 NECK AND TRUNK
17. Head nodding 1 2 3 4 . 5 6 18. Retrocollis 1 2 3 4 5 6 19. Spasmodic torticollis 1 2 3 4 5 6

Appendix H—Continued 102
20.
21. 22. 23.
Torsion movements (trunk)
Axial hyperkinesia (copulat
Rocking movement
Other (describe)
24. Other (describe)
CD U <u > CD W (U >i S-i rH <D
(D (1) > -P -P (D -p fd (0 (Q
G CD •0 0) 0) >i to 1—1 S-l •Q •H 0 O (D
a a 2 >
1 2 3 4 5 6
:i 2 3 4 5 6
i 2 3 4 5 6
i 2 3 4 5 b
i 2 3 4 5 6
EXTREMITIES (upper)
25. Ballistic movements
Choreoathetoid movements-fingers
Choreoathetoid movements-wrists
2 6 .
27.
28.
1
1
1
Pill-rolling movements or finger counting
29. Caressing or rubbing face and hair
30. Rubbing of thighs
31. Other (describe)
32. Other (describe)
(lower)
l
1
2
2
2
2
2
2
2
3 4
3 4
3 4
3 4
3 4
3 4
3 4
3 4
5
5
5
5
5
5
5
6
6
6
6
6
6
6
33. Rotation and/or flexion of ankles 1 2 3 4 5 6
34. Toe movements 1 2 3 4 5 6
35. Stamping movements-standing 1 2 3 4 5 6
36. Stamping movements-sitting 1 2 3 4 5 6
37. Restless legs 1 2 3 4 5 6
38. Crossing/uncrossing legs-sitting 1 2 3 4 S 6
39. Other (describe) 1 2 3 4 5 6

Appendix H—Continued 103
40. other (describe)
ENTIRE BODY
41. Holokinetic movements
42. Akathisia
43. Other (describe)
1 2
X 2
3 4
3 4
5 b
5 6
5 6
COMMENTS

104
Appendix I
Self-Report Tardive Dyskinesia Rating Scale
Name
I.D. #_
Date
Pre ( ) Post ( )
Below are listed some feelings which you may or may not have. Read each one carefully then answer by placing a circle around one of the numbers on the right. The meaning of each number is described below.
1.
2,
3.
4.
0 =
1 =
2 =
3 =
4 =
Absent. This feeling or symptom is one which you do not have. Mild or. slightly present. This feeling or symptom may be present but it is so mild that it is difficult to determine whether you really have it or not. Moderate. This feeling or symptom is one that you definitely have. Moderately severe. This feeling is present much of the time. It may prevent you from doing things you would like to do. Very severe. This feeling or symptom is present almost all of the time. It causes you great difficulty in doing the things you would like to do.
My hands and feet feel cold.
I have trouble sleeping.
I have had difficulty eating.
I am aware of lip movements such as smacking or sucking.
+•> G d) w Q (0
0
0
0
a> u
4-> £ a) > D* •H
CD W CD H >i U W H CD CD CD > U 4-> •P CD 0 fd fd W
u u nd CD CD >s i—[ <3 d u
0 0 0 £ e B >
1 2 3 4
1 2 3 4 1 £ 3 4
1 2 3 4

Appendix I—Continued 105
0) <D
5.
6. 7.
b.
9.
•P > rC <D tn U1
*H CD rH >i U W rH (D
CD CD > U -P •P <D
•p o m rd CO £ u u CD CD CD > i CQ HI nS U
sx •H 0 O CD rd S e 6 >
I wake up feeling tired in the mornings.
I have a poor appetite.
I feel that I can't control some of my movements.
Movements in parts of my body annoy me.
0
0
0 My speech is affected by uncontrollable movements of my mouth.0
10. I am troubled by constipation. 0
11. I have had attacks of nausea and vomiting lately. u
12. I am troubled by uncontrollable movements which interfere with what I am trying to ao. 0
13. I am troubled by hand movements when writing. 0
14. I become distracted by uncontrollable movements when I am watching T.V. or reading so that I lose track of what 0 is going on for a moment.
±5. I am bothered by stomach acid. 0
±6. Swallowing is difficult for me. 0
17. My physical health is a s good as tnat of most of my friends. o
18. i am bothered by pains over the heart and in my chest. 0
1
1
1
1
1
1
2
2
2
2
A
2
2
2
3
3
3
3
3
3
4
4
4
4
4
4
1 2 3 4
1 2 3 4
1 2 3 4
1 2 3 4

Appendix I—Continued 106
CD u 0)
4-> > & CD t n CO
*H 0) r—{ u CO rH Q)
CD <D U - p • P 0)
4-> 0 (0 rd CO a u u 0) CD Q) > 1 CO i H * 0 u
XX - H O 0 0) (0 £ £ S >
19. My chewing is affected by the uncontrollable mouth movements. 0 i 2 3 4
20. My breathing is affected by sudden movements in my body. 0 1 2 3 4
21. Parts of my body often have feelings like burning, tingling, or crawling, or like going to 0 1 2 3 4 sleep.
22. I have had difficulty in starting
or holding my bowel movements. 0 1 2 3 4
23. I have trouble walking. 0 1 2 3 4
24. Movements which I cannot control
make me self-conscious. 0 1 2 ^ 4
25. I feel pain in the back of my neck. 0 i 2 3 4
26. I am troubled by discomfort in the pit of my stomach. 0 1 2 3 4
27. I have trouble with my muscles twitching or jumping. U 1 2 3 4
28. There seems to be a fullness in my head or nose. 0 1 Z 3 4
29. I have noticed a change in my walking rhythm or gait. 0 1 2 3 4
30. X feel that other people act differently towards me because of my uncontrollable movements. 0 1 2 3 4
.51. I have difficulty in keeping my balance. 0 1 2 3 4
3.2. I have noticed uncontrolled move-ments in one or both my arms. 0 1 2 3 4

Appendix I—Continued 10?
33. I stroke or rub my face or hair
CD &-I 0)
- P > rG a>
w -H <D H > i to r~i <D
<D 0) > Ul •P • p 0)
- p 0 fd rtf 01 £ k a> TJ cu 0) > i (0 1—i Tf "O & H o O <u fd E E g >
without meaning to do it. 0 1 3 4
34. ± feel as if there were a tight band about my head. u 1 2 3 4
35. I have stomach trouble. 0 1 2 3 4
36. I have vomited blood or coughed up blood. 0 1 2 3 4
37. During the past few years I have not been well. 0 ± 2 3 4
38. I am troubled by movements of my eyelids or eyebrows. u 1 2 3 4
39. My fingers seem to move about more now than they used to. 0 1 2 3 4
40. I seem to be gaining or losing weight. 0 1 2 3 4
41. The top of my head sometimes feels tender. 0 1 2 3 4
42. I seem to tire quicKly. 0 1 2 3 4
43. I have dizzy spells. 0 1 2 3 4
44. I have noticed unnecessary movements in my jaw. 0 1 2 3 4
45. It is difficult for me to sit or stand still. 0 1 2 3 4
4b. When I read my eyes seem to tire easily. 0 1 2 3 4
47. I feel weak all over. 0 1 2 3 4 48. I have headaches. 0 1 2 3 4
49. My hands seem to fidget when I'm not doing anything with them. 0 1 2 3 4

Appendix I—Continued 108
0 M 0)
4-> > r C CU Cn CQ *ri 0 ) t—I >i u w i—f CD
CD Q> P> u • P - P CD 0 rd rd W
u M 0) Q) >i
- i *0 u - H o O CD £ e £ >
-p c <D w A nJ
50. I am troubled by the uncontrolled
movements in parts of my body. 0 1 2 3 4
51. At times X feel like swearing. 0 1 2 3 4
52. I notice my heart pounding and shortness of breath, 0 1 2 3 4
53. I get angry sometimes. U 1 2 3 4
54. I have noticed that I cross and uncross my legs while sitting more than most people do. 0 1 2 3 4
55. I dislike some people. 0 1 2 3 4
b6. If I don't feel well, I sometimes
become cross. 0 l 2 3 4
57. My body hurts all over. . 0 1 2 3 4
58. I have movements in my body wnich are difficult for me to control. 0 1 2 3 4
59. I have numbness in one or more
regions of my skin. 0 1 2 3 4
60. Sometimes I feel hate for someone, 0 i 2 3 4
61. I am annoyed by the unnecessary movements in my body, 0 i 2 3 4
62. I notice my ears ringing or buzzing. U i 2 3 4
63. I am annoyed by unnecessary movements in my face. 0 1 2 3 4

10.9
Appendix J
Speech Sounds Perception and Articulation
Name
I.D.#
Date
Pre ( ) Post ( )
Score
1.
2. 3.
4.
5.
6.
7.
8. 9.
10. 11. 12.
13.
14.
15.
16. 17.
18.
19.
20,
Theeks
Weej
leeg
teest
freeb
preeb
sheecti
neek
wheesh
preet
preem
f eez
sheez
veeth
theela
preet
teep
steeks
preet
zeend
21. 22. 23.
24.
25.
2 b.
27.
28.
29,
3u.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
deeld
weef
theer
meeld
seet
heek
meem
theer
heez
theep
wheep
keem
neek
sheem
theep
wee Id
teed
theez
weev
leeng
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
b4.
b5.
56,
57,
58,
59,
60,
sheen
geerd
geen
weeng
teed
teets
zeet
beet
teer
deeb
heem
theer
feeth
reek
yeed
deet
deez
teeld
meer
wheem

110.
Appendix K
Compositional Data on Lethicon
Phosphatidyl Choline 51 - 55 Phosphatidyl Ethanolamine 19 - 22 Monophsphatidyl Inositol 1 - 3 Lysosphosphatidyl Choline-Lysophosphatidyl Ethanolamine 2 .5 . 3
Phosphatidic Acid 2 .5 - 4 N-Acetyl-Phosphatidyl Ethanolamine 3 — 4 Glyceryl Phosphoryl Choline 0 .5 -
Free Fatty Acid 1 - 2
Sterolglycoside esters b — 7 Sterolglycoside 0 .5 - 1 Free Sterols 1 — 2 Monodiglyceride 0 .5 — 1 Triglyceride 2 - 3 Moisture 1 — 1.! Ethanol 0 .3 — 0.' D-Alpha-Tocopherol 0 .1 — o.;
% % %
% %
°/ /o
°/ 7o
°/ so
%
%

Ill
Appendix L
c; J-i 0 o CO 0
rr f-H CO d U 4-» W 0 H cn
C ^ -H 0 -P U4 fD
0; 0)
V ti C H d w H d>
r- #H C flj -H
0 > X r-4 o w ,Q O >1 rd a £h UH
0 0 >
M -H H 13 W U N fD H ^ (0 c c < 0
w a
0 g •H
t-j 03 £ g O
P to
0\
M
wj s i
SI
coi w |
CD U i-i P O W
O
w c o
•rH P •H
c o u
•P C CD £
d CD to Eh
G Cn <
r-m
o vo
CM m
-P c o E •P d o
Eh
O *H -P a> Ok
rH o M
<d
c o •H -P A3 p
Q
o CM
00 VO
• r fN rH vr CO 00 rH rH r- CO KT ro ID ON
ro fO CM rH o if) 00 cr o r—« rH CN VO ro
H
CN m
t^ CM i-H 00 VO vO Lf> CM l> 00 00 r- rH to * • • • • • *
v£> no CM CM o rH m X o t-H CN ro rH rH iH CN
rH
0 -p c
c a> 0 E •H -p •p X f0 to 0
CD u CD M p
< a < o
X X X *H •P to
DQ w £ w a rH c C CD C <D rH 0 0 E 0 rH CD
•rH -H -p •H 0 U -P -P d •P i-<
U
•HI •H CD •H P c ^ u TJ a> •H
C C EH C 2 c 0 0 -P a o a a u-i •H
•H o •P +> -p •p G G ft c c rH 0) Q) CD CD O d E E *H E *H P -p •P 0 JJ 4J TD d m tc (T3 •rH a) G) 3 0 ^ « J-i s-f CD u p CD £H EH £ CH Q as.

112
Appendix M
to e 0 P M *0 O u o u CQ 0 U-l H 0 (0 u u w
0 £ D> £ G P *H 2 «P fO rH Ctf ro -P nj 0 *H t-i W a
00 u c O *H 0 «M X H K & 0) >n to U Q E G fO 0 •H > U -H fO T3 > Ui 0 (0 U H M-i G 0 0 w w a
£ Ui -H >iCO rH r0 G C 0 <
l*-l 0 >1 rtJ
V '
ft
M
coj X\
M Ol
ooi
o o in
cr. r-* cr,
<S) rH 00 <N CN rH r* in (N rH in CO m • • • * • • •
r—! oo rH rH rH H
CM ro
0> rH oo CN sD O t— CM CN O VD rH • • • • • • •
CO ro O CN CO 00 50
-P •P g G 0) a 0 e 0 6 •p •H «P rfl +> X (0 0) <0 0 SH a u 0 u EH o> < p O. -P
DEH < 0 g o •H X X 0 X -H •P £ •P W 03 ft tc M +» W ft rH
G 0 c G (0 G 0 rH 0 rH 0 0 0 O rH 0 •H 0 H •H M •H 0 U P u -P -P £H -P M -H p •H •H •H p G H3 0 0 13 O TJ 0 •H G z c G -H G 2 0 0 O -P 0 -p O m 0 u O ft 0
U M-» 0 -H
-P -P •P rH \ g c G G O G G rH
<D 0 0 0 0 U 0 0 (0 <D e •H e £ 3 E -H P
U •p •P -p •P 0 +> -P n3 M fd rd 2 fO to H a 0 0) 0 0 0 U W 0 u Di P J-i m M P 0 C-4 < Q E-t EH 0 LH 3 en

Appendix N
113
« § «P A E
TO
>1 M 0 •p (0 0
•H O -M rH W f0 «J U
S CO rH D» (0 G P -H 0>«P G <0 H OS J
1 fO O -H 0 w O 0
ON P G
ffi -H 0
rH P (0 X I O >1 rd TW D E-F
(D 0 O > G H
10 »0 -H p P M M EH > O G U 0
W
U-I ft O G
•H to w H W G > I O
«H to G
<
O >1 p ro P TO
v
Qi ro
PM!
81 P P
R-
W G O
•H •P •HI
G O U
-P C 0 S Xi a} 0 u
r-o
00 r-
CN O
CN ro
00 VO ro rH o vO C\' 00 CN l> rH H VO r-
00
LH
CM
O
O R-
R^ OO
CN <H
00 TT
CM RO
r- vO ro O O rr r-rH VO r- rvj • • • • • • «
ro "5J* CM Ch uo rH ro rH VO i f ) rH CNJ in -P 4-> G G 0) G 0 E O E •P -H •P ro 4J X r0 0 ro 0 u A> M 0 P E-< D> < P
P +J < 0 G a *H X X CD X -H •P B P (0
ft CO to -P W ft rH 0 G G fO G 0 -H rH O O <D O H 0
0 •H •H P •H O a u •P 4J E-» - P P p •H H •H p G
<D *0 *0 V T3 0 -H Z G G -H G S
O O -P O p U U ft O •H O 0i 0 & G -P •P rH 4-> \ G £ G O G G rH O CP CD H 0 o fO -H E S P £ -H p 4-> -P -P 0 -P -P H3 ro <0 re S d d *H CD P Q 0 0 P W CT> P P P M-L P P 0 < Q tH B O ^ Q BZ
ft *
(0 •P U 0 -r-i •Q P (0
P <D O* C P 0 >1
C 10 p 0 V rH O
c 0 0 £ •P CD JD
W 0 H 0 U c 0 p 0)
M •H U
0 W
T0 U 0) JQ
> I T> P
- P W
o •P
© U G (0 ft U P •H o I P "P •H 01 G
W 0) O
<W FO O H ft
•P O G G -H *
O

114
Appendix 0
G S-t 0 G 0 rH W 10 0 rH WD cn
0 G EH -H •P U it o os 4-i c0 G -H o w
G G HJ G •H *H o u A; rH <0 « > J>I G O Q rH u JQ G fO 4-1 > H 0 *H "0 IQ U *h rd to e-i >1 rH P rd G Q < ft
G •H & O I <4-1 >iH U G to 00 p: £= G 3 O CO
OJ
M
"I Si
Ql
LO NO
03 G O •H -P -H G O o -p G G G £
U -P (0 3 G G O k CP W EH <
CN m
-P c 0 £ -P ifl G E-» U -H •P ft G
<U 25
G o •H 4-' fO tl 2 P
0 01 <
10 G O •H •P •H <V G O U -P G G a -P (0 G
in CN
,*N
C G\ vO r r VD r -r r \> r - r—1 rH m UD r - CM vD o CO ro r\j ro rH rH un
o> vO 00 CN r - r - 00 ro ro
• • • » • •
vO Lf) r» in CN O ro (N CN} Ch VO
CN •—i rH H rH
00
c o *H -P nJ P Q -P G X G £ co .p G fO O G H U +> E-< •H •o U G »H O -P D ft G -M rH G O G M £ P •P <D RJ S G ti m 0
•P G © £ •P X fU G G i-j CJ> E-» < U X *H -P W ft G G O rH •H 0 •P M •H D rcj G G 2 O U tP O •P G G G O £ -H -P -P d fC G i-i
U P EH Q

115
Appendix P
-P r* <d c -H E O 3 <D JH -P o to
4H 0 G) C U 0 C -H (0 P -w nJ rH U rH rH (0 r-i
> -H (D 0 o rH O w Q c M-4 tH O SH 0) W O* •H C to -H >1
rH (0 TS c c < rtJ a: U-t 0
m
V
m
Cul
Wf sl
* * * * ro o o a. PO rr © "sr «3< o o ro o o rH
o O r-• r vO CT» vO o
ro C* O ro ro CM rH
O rH o r- VO ro in ro <0 rH ro CN in TT ao vO
vD VO ON rH O 00 00 TM CO CO in <N Ch <N
w c 0 •H
•P •H
'O c 0 o •p c a) (D g
U •p (C
d CD G>
0 ^ cn CO H <
<1> s •p fO o u B*
U •H •P ft G) i—i o u p
<1) <4-4
o G O -H -P rd i-t Q
0) Cn <
to c o •H -P •H c o o -p c 0) s •P rfl o
c o •H -p f0 J-t Q +> c X 0)
e W 4J c rd O <D •H M •P ^ H TJ U C -H O -P U ft <u -P rH c o <D U B P 4J Q> (0 S3 d) 1H H4 E-< O
co
O rH o ro r- o r j rH ro m rH X ro o • • » • • • •
ro r- ro CN o> CM O 00 CN r- r- O r-
rH TT rH rH H r- 00 ro
-P C <t> £ •P X to G) 0) M D1 tH X -H •P W ft C Q> O «H •H O •P M •H 3 U <D C Z O U <u o -p c c (D O E *H P .p flj (0 O Jh h 3
rH in rH O ro O O O P
fO r-i •H (0
> >
>
W 4-» 0) o el oi QJ £* £-» * * *

116
Appendix Q
•P c to c •Hi £ 0 Q
G O 2 0)
-P ^ (0 o & iw
c 0 0
a -h c -p fO A3
CN *H rH r—! rH
d *H 0 > U <-H o w & U O fO &H M-) M
0 O D*
ra c •H *H to Pn
rH *0 nj a a ro < X
VP 0
u m
i w
V
01
M
SI
W| w!
O o
sO cn
00 r-r-
iH O r-CM
o
ON
r- XT cr» O 00 VD ro O LO a CM o CM LD sO CN ro CN ro rH <N CN CN
CO Cr. <** rH MD rH CTt r- ro rH 00 rH :> » > • • • t •
in c* <N o CN LO CN ro rH H rH CN r-
•P -P G G 0 G 0 6 0 B -P -rH -P (3 •P X (0 0 A3 0 M 0 0 E-« 91 3 tF c-1 *s Q -P < 0 G V *H X X 0) X -H 4-i E •P to CO ft SO to -P W ft rH G 0 c G rd G 0 rH 0 rH 0 0 0 O H 0 •H 0 •H H Jh -H 0 o •p u •P +J EH •P M
o •H 3 ••H •H •H 3 G »0 0 a T> 0 T3 0 -rH c 2S c G *«H G 2 JC 0 0 0 -P 0 4-» o 4-J u O ft U 14-1 *H 0 <1) o •p -p -P rH •p \ G g G G 0 G G rH
0 0 a 0 0 0 d s H £ e 3 S -H •p •p -P -p o -P -P ro fO ft? rO fO z as d -rH 0 0 0 0 0 M to 3 fi M <P M P 0 < Q C-f EH O EH Q X
irt »h o o
PJ 01 * * *

117
Appendix R
a fij Eh
O V c fa •H 4-i td w > a) o EH u T> iw M O (C TO S •H D> TO 0 >iCu r-H m o c s < o
u m 3 o a.
u (0 B
01 oo o o CM CO Oj
o m
CO & vD vO r- CM r-
o o
a Cn <
in
+> g <» I rd (I)
•P a. G) j—i o 3 <D 2
G O -H -P fO Q
m r-v£> r-O o CM rH
G 0 •H -P fd 0 M O1 3 < Q -P C X X <D c; TO w 5 G G fO 0 0 CD •H *H !L| -P -P Eh •H TJ *d o G G -H 0 0 -P O O Oi <D jj -P rH G G 0 CD <D k E £ 3 •P -P 0 to fO 23 0) <D Jh S-i 4-1 Eh Sh 0
ro x
00 O rH rH 00 «r no CO CN O CM in O in vO CM HI rH vO
ou
-P G CD g -P X to <D d) CP Eh < U X -H •P w a G <D O H •H 0 •P U •H Tf <D G 23 O o P o •P G G <D O
B -H •P -P rtJ (0 (D M Ih 3 Eh Q

118
Appendix S
U O -P W 0 0 Eh U G G r0 O •H -H U -P its ro > '—! O P O 04 -H M-i G 1—1 O ro S 0) w
rH -H 4-1 XX M O (0 >1 rH 0 ro -P G rO < C£ 4-f <0 O -P O >1 w M 0 (0 G i c g -H P 2 W
V
M
to! SI
H Ql
vc CM
in m
0 0> <
* !>
O VD
oo ro rO ro
•P G O E •P d 0 U £-« U
*H •P a 0) -H o u p 0 &
O G O 4-> (0 U P P
LTl vO
-5f
r- O cn cr* if) rH 00 ro 0 r- O 00 * • • • • # •
ro !/> vO •H 00 Ok m o> 0 rH vO rH
cn ro
O r- rH CN vO o> no O m rH 00 rH • • • • • • •
LD ro CN <D vO 0 Cv ON & ON rH ro •*o in ro •p G G 0 0 £
-H •P •P X rd (0 0 0 M 0 i-t P D>&H < Q +> G < 0 X X 0 X -H 6 4-J 0] CO W -p w a rH C G ro G 0 rH O O <D O H 0 -H f-l •H O O -P -P EH -P M O •H •H -H P G 'O 0 0 TJ 0 -H c G H G S3 ,C 0 O -P O •P 0 O ft OM-4 -H 0 O »: •p -P rH -P \ c G O G G rH 0 0 u 0 O ro £ £ P S -H p
-P -P 0 -P -P T3 (0 ro S ro ro H 0 0 0 M W U J-i 4-1 U P 0 cH O E-< Q Qi OJ *

119
Appendix T
0 —-f
(0 E-l
01
w | SI
ol
w|
0) u J-l 3 o CO
r—i
vC
m ro
LO LC
o 00
vc r>j r*
ro CM CM
0 )
S1 <
LO in
r - r o r o r - CO i n «x> O 0 0 r o VD vO v£>
cm r s j <N CN r H r -
r-<N
r o r o "*3* VO o r o o 0 0 r o r o 0 0
t n CM CN ro
20
6
-P +> G G G O 0 <D £ •rl E -P -P •P
m X fO 0 <D u 0) G) t-i 1H CT> E-f
< •P < 0 X G O
X <D X -H -P CO E -P CO ft w G -P W ft H 0 g 0 fO G <D rH
H 0 -H <D O H <u O •H -P 5H •H O o
•P -H EH -P M P • H T J • H p G 0) *0 G U T3 CD -H 55 g 0 * H G 25 A:
0 O +> 0 • p 4-1 u ft U <w • H O -P <D 0 £
+> <D H •P \ g g G 0 G G f H 0 <D 0) U G 0 fO
* H e E P E * H P -P -P + j Q) •P -P T3 fO f0 ( 0 2 ; fO <tf • H U <U 0) CD M W P M 4-1 0
Q E-t E O En Ci X

120
Appendix U
JH 0 4-1 O U G Q fd M *H O m a (0 w > O r-l o to •P
>O *P O
rH O EH
0) W 4J H -HI rH X> w to (V >.+> H rH U1 to O
G O < 1
u 4-1 D 0 a G >s (D U CQ
f0 3 W
01
W
CO!
S I
CO CO ON VO
O
ro CM
ON ON
v£> 0>
•P G
O
E -P
F0 (1)
UI 0)
EH < O
X -P
W D4 w G O G
O rH O
-r-l 0 •H •P u -P
H p •H <v
G 25 G
O O o 4-1 0
U
.p •P G G G
CD o CL) E *H E P> -p -P F0 m a; Q) k a> u TJ- D M
EH < Q EH
rH LO
00 vO
G 0 •H •P 10
3 Q -P
C X <D
£ W -p G F*J O 0) -H S-» -P EH •H *0 U G -H O -P O A
<U -P «H G O O M s s +> ty M 2 0)
EH O
rH •H o r-\ in CM o O O ON ro rH VD r-• • • « • • •
CM CM 25
12
00 12
ON CM
CM rH o CM o in m O O ON VO ro CM ro • • • • t •
( r* O 00 to (N rH VO ro -P G <D 6 -P
X FT Q)
V U CNEN <
V X -H
+J
W CU G G)
O rH •H O
TL 0) G 25 O O M-L
O -P G G <L> O
IS D FD CD M U 2 T-T Q
RH <D C
G
•H rG •P
FO
TJ *H 10 <D G5

121
Appendix V
0 vw <1) 0 U U C 0 fO O •H CO Li fO >i > Li 0 0 U CP 0 r- 4-1 4-> rH 0 fO O a a:
rH -H -P CO rH ra fO •H -P rs w c a; < o i <P M 0 0) >1 c ^ a) d GG
m
M
£i
Qi
col wl
o p u 2 O CO
L D CD
0 vD
vO vD "53* ro
FO O o CM
VO O r-ro *0 o
CO H
o L O
ro ro
( N
in RH vO ro CM 0 0
© O r- RH RH i—T • • • • • * •
H O R H
•P •P C C <u G (D E 0 e •P * H +>
rO •P X fO 0 (0 d) a E-i <1> D tH C7> a +> < 0 < c 0 -H x <u X • H
•P X E •P CO to ft CO +J w ft RH c Q) CO c ro c CI) R H
0 R H c 0 <D 0 RH a • H 0 0 • H I - I - H 0 o •P U -p •p B -p u • H 3 • H • H - H 3 c <D T3 V u T3 0) • H
C Z c C -H c z rC 0 0 0 -P 0 •P O 4 H u U ft o 4-1 - H
0 o 0 3= -P -p -P - H .p \ C G c C 0 c c RH
a> O 0 QJ U a) 0 m e £ E P E • H P •p -P 43 -P (I) -p •P H3 fO (0 ro (0 S A3 CO • H
Q) <D in <D QJ Q) u CO SH o> 3 SH I H 3 <D TH < Q JH H 0 E-» Q 0$

122
Appendix W
u c <4H 0) 0 G rC •H rd -P > W O (1) O B
00 UH H rH °E <D rU
W £ r-i •H >i rQ W [0 fO &H H 4-' t0 -H G D> H o
0
>i u {g s
V
0\
w Sf
H Qi
Si
o M 0 O OQ
CO o r-i CM
ro CO •H CN lO r-r- •-i v£> rH o vD ro CN CM rH
-o <N in 00 vO VO o r - vO —1 CO rH in
CO ln r - o CN CN rH vO vD LO ro
rH
CN <H H CN CN CN CN
r* CM tn 00 m CN OJ 00 r- vD ro r- no in • • t • • • •
in r- 00 ro 00 rH r-H ro ro o 00 -i r—1 r—i H -P -p G G <D G 0) E O e -P -P m •P x td Q> 03 0) U <D U 0 M D> J3 D>EH < Q -P < O G a •H X X O X H -P E •P w w ft Ui W -P w ft rH c Q G G fO G 0) rH 0 r-f O O 0) O "H Q) -H O •H •H •H O CJ -P -P -P tH -P U *H 3 •H •H •H 3 G V O TJ X3 O <3 0 •H c 25 G G H G 2 -G o O O -P O 4J u UH U O ft V 4-t •H O O 0 3= •P «P •P r—1 -p \
G G G G O G G iH 0) O a a) u Q O r0 E •H E 6 5 E -H p •P 4-> •P •P <L> 5 -P it ro KJ f0 z rd n3 *H 0 Q) di Q 0 M W U Di 3 JH JH M-i Q) EH < 3 JH £H O EH Q cr;

123
Appendix X
(C t-
u 0
0 o c fO •H >
O -P o to
CL5 4-1 ^ O <
W •H to W iH
rH fO ro u < ^
'm-J o
>i u rd
p 1/2
v
0\
M
col Si
N Qi
co tfij
o o u p o Uj
CO IT)
<0 in
CO m
CO *5* oo
o CO
m rr rH 00 !> r - CN (N CO in CM vO CTt r -• • • • * • •
*3" CN CT> O o 0> 0 o in in o r - CO rH CM CO 00 r0 rH rH in rH O CN
o 00
H rH VD ON m ro in in ro ON vO • « • • • • •
00 «3< CN 00 rH H rH 00 CTi in rH o ON CO <N 00 r*> VO ro H CN '.n ro vD
vO
-P -P c C 0 c: 0 E 0 e •P •H -P to +> X A3 0 rO 0 i-» 0 M 0 U H 0> P D>£H
< Q -P < U c U "H X X 0 X *H -P E P W w ft w W -p W ft rH
c 0 £ C ro C 0 rH 0 rH c 0 0 0 H 0 -H 0 -H M -H 0 o -P M -P •P EH -P U
o
-H P *H -H •H P c TJ 0 TJ HD U T3 0 •H C 52 G C -H G 53 0 0 0 4-> 0 u U U ft a m •H
0 0 0 4-' -P -P rH p \ c c C C 0 c a -H 0 0 0 0 ^ 0 0 rO % •H £ 6 3 E *H P •P -P -P -P 0 -P -P a rO m rO f0 S rd ro •H 0 0 0 0 0 M CO H P U M +J ^ P 0 EH < Q EH Eh 0 !H Q VC

124
Appendix Y
U 0
*4-!
OJ 0 c d •H u d +J > w 0 0 O H
o MH W CM 0
c <D to 3
-H 0 XJ W LO d H ,c
d u G <D < 0
ft M-l CO 0
>i U d g
CO
Qj
Wl si
J11 w|
n oo
X CM
tc G 0 -H -P •H T5 G 0 O
•P G 0)
GJ £ U 4->
(TJ 3 <D <D 0 U D> CO EH «<
i n \o IT)
ro vO
00 i n
o oo
CN CM
£T> O v£J O 00 rH in vO CM o • • • • • • t
<r CM CN i n ro C* rH •-H UT) CM "M
<N 00
c- «?P o ro ro o Ch 00 to 00 00 CO
» • * • t • •
X CJ (N j-4 r- 00 CM CM in in rr H rH
00
-P •P G c 0> G (U £ 0 £ .p •H 4-* ro -P X d <D d 0 M <D iH 0) in EH O 3 EH
< Q -P < U G U -H X X 0) X -rH -P 6 -p in
ft w w -P w ft rH QJ G g d £ (D rH
rH 0 0 0 0 rH <D 0 •H H u H 0 O U -P -P E-» -P JH 2 •H •iH •H 3 G Q) V •o U T3 CJ •H S G G -H G SZ rG
o O 4-> 0 -P i+-i u O ft O 4H •H 0 a) 0
-P •P rH •p c G G 0 C G rH 0 <u <U QJ O d -H £ £ £ -H 4-> 4-> 4-> <D -P -P *0 d d IS d d •H in Q) <L CJ 5H W 3 U M lM JH P OJ Q £H 0 cH O OS

125
Appendix Z
ro CN CD •H rQ
rd Eh
CO
CD O O •P CO •p o CD •r-1
•Q 2 CO UH o c o •H 4-> ,Q Sh 4J CO •H Q g
O O 13 C
10 a o *H +> •H
c o u -p £ <D E -P 03 0 M Eh
•P G (D e -P CO CD En I O 23
CO D* 1—1 £ ro ro 0 0 u rH ±> l> 00 on vo c 0 -P o U
0 ^ LO rC CO
a 0> •H £ LO <£> rC 0 -P «—1 •H r- CO rH O rH CD -p J CO M
CO c 0 <N CM C 0 rC 0 •H £0 •H •P -P O u rd rd u CD <D -P rQ
-P £ tn 0 C H £ ro XI H O CD r—1 O >i oo r- co i> J2 •
rd rd & -p rH S
1 i £ *P a.
S 1 CD rd CD £ 0 CD -P E 0) £ i-l •P E EH rC O LO ro rd -P
&H rC 0 rd CO M CD
-P U
-P U •h a -P -h ft -P cd a rH 0 O rH M O 3 U
•P CD 3 fi £ CD CD £ E MH •P O MH rd O
CO CD £ M o a 0 Eh •h o -P -P -H o mh rd -P rd 0 M rd Ph 3 Sh c ro S3 -P CP 0 -P 0 £ -H £-i Or> £ -p a) 3 TJ -P 0 C 3 TJ SH tn *r~> 0 rH fd rC 0 O rH O £ X5 CD >H O «L| w »J CD >H o rC O 2 tn 3 O* cn j co <C Q c a
b

126
References
Ananth, J. Tardive dyskinesia: myths and realities.
Psvchosomatics, 1980, 21, 389-396.
Aquilonius, S. M., & Eckernas, S. A. Plasma concentration
of free choline in patients with high doses of choline
chloride. New England Journal of Medicine, 1975, 293,
1105-1106.
Ayd, F. J., Jr. Ethical and legal dilemmas posed by
tardive dyskinesia. International Drug Therapy
Newsletter, 1977, 12 , 29-36.
Baldessarini, R. J., Cole, J. C., Davis, J. M., Simpson, G.,
Tarsy, D., Gardos, G., & Preskorn, S. H. Tardive
dyskinesia summary of a task force report of the American
Psychiatric Association. American Journal of Psychiatry,
1980, 137, 1163-1172.
Barbeau, A. Drugs affecting movement disorders. Annual
Review of Pharmacology, 1974, 14, 91-113.
Barbeau, A. Lecithin in neurological disorders. New
England Journal of Medicine, 1978, 298, 299-300.
Barbeau, A. Lecithin in movement disorders. In Barbeau, A.,
Growdon, J. H., & Wurtman, R. J. (Eds.), Nutrition and
the Brain Series (Vol. 5). New York: Raven Press, 1979,
263-272.
Beckham, B. J. Lecithin Therapy for Tardive Dyskinesia.
Doctoral Dissertation, North Texas State University, 1981.

127
Berger, P. Tardive dyskinesia: recent developments.
•International Drug Therapy Newsletter, 1980, 15, 17-20.
Carisson, A. Biochemical implications of dopa-induced action
on the central nervous system with particular reference
to abnormal movements. In Barbeau, A., & McDowell, F. H.
fKds.), L-dopa and Parkinsonism. Philadelphia: F. A.
Davis Co., 1970, 205-212.
Carisson, A. Some aspects of dopamine in the basal ganglia.
In Yahr, M. P. (Ed.). The Basal Ganglia. Washington,
D. C.: Raven Press, 1976, 181-189.
Carpenter, W. T., Jr., & Rudo, A. B. Prevention and early
detection of tardive dyskinesia. Behavioral Medicine,
1979, 6, 33-37.
Carroll, B. J., Curtis, G. C., & Kokmen, E. Paradoxical
response to dopamine agonists in tardive dyskinesia.
American Journal of Psychiatry, 1977, 134, 785-7«9.
Casey, D. E. Tardive dyskinesia: are there subtypes?
The New England Journal of Medicine, 1976, 295, 1078.
Casey, D. E. Managing tardive dyskinesia. Journal of
Clinical Psychiatry, 1978, 39., 748-753.
Casey, D. E., & Tepper, S. Cholinergic aspects of tardive
dyskinesia. In Obeols, J. (Ed.).' Biological Psychiatry
Today (Vol. 2A). New York: Biomedical Press, 1979.

128
Christensen, E., Moller, J. E., & Faurbye, A.
Neuropathological investigation of 28 brains from
patients with dyskinesia. Acta Psvchiatrica Scandinavia.
ly70, 46, 14-23.
Clow, A., Jenner, P., & Marsden, C. D. Changes in dopamine
mediated behavior during one year's neuroleptic adminis-
tration. European Journal of Pharmacology, 1979, 57,
365-375.
Cohen, E. L., & Wurtman, R. J. Brain acetylcholine:
increases after systemic choline administration.
Life Science, 1975, 16., 1095-1102.
Cohen, E. I & Wurtman, r. J. Brain acetylcholine: control
by dietary choline. Science, 1976, 191, 561-562.
Crane, G. E. Tardive dyskinesia in patients treated with
major neuroleptics: a review of the literature.
American Journal of Psychiatry, 1968, 124, 40-48.
Crane, G. E. Prevention and management of tardive dyskinesia.
American Journal of Psychiatry, 1972, 129, 126-127.
Crane, G. E. Persistent dyskinesia. British Journal of
Psychiatry, 1973, 122, 395-405.
Crane, G. E, The prevention of tardive dyskinesia.
American Journal of Psychiatry. 1977, 134, 756-758.
Davis, ,K. L., Berger, P. A., & Hollister, L. E. Choline for
tardive dyskinesia. New England Journal of Medic-ine,
19/5, 293. 152.

129
Davis, K. L., Berger, P. A., Hollister, L. E. Clinical
and perclinical experience with choline chloride in
Huntington's disease and tardive dyskinesia: unanswered
questions. In Barbeau, A., Growdon, J. H., & Wurtman,
R. J. (Eds.), Nutrition and the Brain Series (Vol. 5).
New York; Raven Press, 1979, 305-316.
Davis, K. L., Hollister, L. E., Barchas, J. D., & Berger,
P. A. Choline in tardive dyskinesia and Huntington's
disease. Life Science, i97b, X9, 1507-1516.
Druckman, R., Seelinger, D., & Thulin, B. Chronic
involuntary movements induced by phenothiazines.
Journal of Nervous and Mental Disorders, 1962, 135, 69-76.
Eichberg, D. Personal communication, March 19, 1981.
Ezrin-Waters, C., Seeman, M. V., & Seeman, P. Tardive
dyskinesia in schizophrenic outpatients: prevalence
and significant variables. Journal of Clinical
Psychiatry, 1981 42, 16-22.
Fann, W. E., Lake, C. R., Gerber, C. J., & McKenzie, G. M.
Cholinergic suppression of tardive dyskinesia.
Psvchopharmacolog ia, 1974, 37, 101-107.
Fann, W. E., Stafford, J. R., Malone, R. L., Frost, J. D.,
& Richman, B. W. Clinica.1 research techniques in
tardive dyskinesia. American Journal of Psychiatry, 1977,
134-,- 759-762.

13Q
Faurbye, A., Rasch, P. J., Peterson, P. B., Brandberg, G.,
& Pekkenberg, ,H. Neurological symptoms in pharmaco-
therapy of psychosis. Acta Psvchiatrica Scandinavica,
1974, 40, 10-27.
Faurbye, A. The structure and biochemical basis of movement
disorders in treatment with neuroleptic drugs and in
extrapyramidal diseases. Comprehensive Psychiatry, 1970,
il, 205-225.
Fox, J. M., Betzing, H., & Lekim, D. Pharmacokinetics of
orally ingested phosphatidylcholine. In Barbeau, A.,
Growdon, J. H., & Wurtman, R. J. (Eds.), Nutrition and
the Brain Series (Vol. 5). New York: Raven Press,
1979, 95-108.
Garnder, E. Fundamentals of Neurology, Philadelphia: W. B.
Saunders Co., 1975.
Gelenberg, A. J. Choline and lecithin for the treatment of
tardive dyskinesia. Psychopharmacolocrv Bulletin, 1979,
15, 74-75.
Gelenberg, A. J., Doller-Wojcik, J. C., & Growdon, J. H.
Choline and lecithin in the treatment of tardive
dyskinesia: preliminary results from a pilot study.
American Journal of Psychiatry, 1979, 136, 772-776.

131
Gelenberg, A. J., Doller-Wojcik, J. C., & Growdon, J. H.
Lecithin for the treatment of tardive dyskinesia.
In Barbeau, A., Growdon, J. H., & Wurtman, R. J. (Eds.),
Nutrition and the Brain Series (Vol. 5), New York:
Raven Press, 1979, 285-304.
Gerlach, J., Keisby, N., & Randrup, A. Dopaminergic hyper-
sensitivity and cholinergic hypofunction in the patho-
physiology of tardive dyskinesia. Psvchopharmacolog ia.
1974, 34/ 21-35.
Groves, P. M., Wilson, C. J., Young, S. J., & Rebec, G. V.
Self-innibition by dopaminergic neurons: an alternative
to tne "normal feedback loop" hypothesis for the mode of
action of certain psychotropic drugs. Science, 1975,
190, 522-529.
Growdon, J. H., Cohen, E. L., & Wurtman, R. J. Effects of
oral choline administration on serum and CSF levels in
patients with Huntington's disease. Journal of
Neurochemistrv, 1977, 28, 229-231.
Growdon, J. H., Gelenberg, A. H., Doller, J., Hirsch, ,M. J.,
& Wurtman, R. J. Lecithin can suppress tardive dyskinesia,
New England Journal of Medicine. 1978, 298, 1029-1030.
Growdon, J. H., Hirsch, JYL. J., Wurtman, R. J., & Wiener, W.
Oral choline administration to patients with tardive
dyskinesia. New England Journal of Medicine, 1977, 297.
524-527.

132
Hall, K., Jackson, R. B., & Swan, J. M. Neurotoxic reaction
resulting from choloropromazine administration. Journal
of the American Medical Association, 1956, 161, 214.
Hirsch, ,M. J., Growdon, J. H., & Wurtman, R. J. Increases
in hippocampal acetylcholine after choline administration.
Brain Research, 1977, 125, 383-385.
Hirsch, M. J., & Wurtman, R. J. Lecithin consumption
increases in acetylcholine concentration in rat brain
and aarenal gland. 'Science, 1978, 202, 223-225.
Jackson, I. V., Nuttall, E. A., Ibe, I. 0., & Perez-Cruet, J.
Treatment of tardive dyskinesia with lecithin. American
Journal of Psychiatry, 1979, 136, 1458-146U.
Jackson, I. V., Davis, L. G., Conen, R. K., & Nuttall, E. A.
Lechithin administration in tardive dyskinesia: clinical
and biochemical correlates. Biological Psychiatry, 1981,
16, 85-90.
Jenden, D. J. An overview of choline and acetylcholine
metabolism in relation to the therapeutic use of choline.
In Barbeau, A-, Growdon, J. H., & Wurtman, R. J. (Eds.),
Nutrition and the Brain Series (Vol. 5). New York:
Raven Press, 1979, 13-24.
Jeste, D. V., & Wyatt, ,R. J. In search of treatment for
tardive dyskinesia: review of the literature.
Schizophrenia Bulletin, 1979, 5_, 251-293.

133
Jeste, p. V., & Wyatt, R. J. Changing epidemiology of
tardive dyskinesia: an overview. American Journal of
Psychiatry, 1981, 138, 297—3U9.
Jus, A., Pineau, R., Lachance, R., Plechat, ;G., Jus, K.,
Pires, P., & Villeneure, R. Epidemiology of tardive
dyskinesia, Part I. Diseases of the Nervous System,
ly76, 37, 210-214.
Kazamatsuri, H., Chien, C., & Cole, J. C. Therapeutic
approaches to tardive dyskinesia: a review of the
literature. Archives of General Psychiatry, 1972, 27,
491-499.
Klawans, H. L., Jr., & Rubovits, R. An experimental model
of tardive dyskinesia. Journal of Neural Transmission,
1972, 33, 235-246.
Klawans, H. L., Jr., & Rubovits, R. Etfects of cholinergic
and anticholingergic agents on tardive dyskinesia.
Journal of Neurology, Neurosuraerv, and Psychiatry,
1974, 27, 941-947.
Kobayashi, R. M. Drug therapy of tardive dyskinesia.
New England Journal of Medicine, 1977, 296, '257-260.
Marsden, C. D,, & Jenner, P. The pathophysiology of extra-
pyramidal side-effects of neuroleptic drugs.
Psychologica 1 Medicine, 1980, JLO, 55—72.

134
Marsden, C. D., Tarsy, D., & Baldessarini, R. J.
Spontaneous and drug induced movement disorders in
psychotic patients. In Benson, D. F., & Blumer, P.
(Eds.)/ Psychiatric Aspects of Neurological Disease.
New York: Grune & Stratton, 1975, 219-226.
Moore, D. C., & Bowers, M. B. Identification of a subgroup
of tardive dyskinesia patients by pharmacologic probes.
American Journal of Psychiatry. 1980, 137, 1202-1205.
Macintosh, F. C. Are acetylcholine levels related to
acetylcholine release? In Barbeau, A., Growdon, J. H.,
& Wurtman, R. J. (Eds.), Nutrition and the Brain Series
(Vol. 5). New York: Raven Press, 1979, 201-218.
McGeer, P. L., Grewaal, D. S., & McGeer, E. G. Influences
of noncholinergic drugs on rat striatal acetylcholine.
Brain Research, 19/4, 80., 2H-217.
Prange, A. J., Sick, J. L., & Wilson, A. C. Balance,
permission, and discrimination among amines: a
theoretical consideration of the action of 1-tryptophan
in disorders of movement and effect. In Proceedings of
the National Institute of Mental Health Serotonin
Conference. Palo Alto, California. Government Printing
Office, 1972, 966-1489,
Quitkin, F., Rifkin, A., Gochfield, L., & Klein, D. F.
Taraive dyskinesia: are first signs reversible?
American Journal of Psychiatry. 19/7, 134, 84-87.

135
Schiele, B. c., Gallant, D., Simpson, G-, Gardner, E. A.,
& Cole, J. 0. Neurologic syndromes associated with
antipsychotic drug use. New England Journal of Medicine,
1973, 289. 20-23.
Schoenecker, M. Ein eigentumlicher syndrome in orgalen
Bereich bei megaphen applikation. Nervemarzt, 1957, 28,
35.
Sigwald, J., Bouttier, D., Raymondeau, C., & Piot, C.
Wuatre cas de dyskinesie facio-bucco-linguo-masticatrice
a evolution prolongee seconaaire a un traitement par les
neuroleptiques. Revue Neuroloaiaue, 1959, luO, 751-755.
Simpson, G. M. Simpson tardive dyskinesia rating scale.
In Fann, W. E., Smith, R. C., Davis, J. M., & Domino,
E. F. (Eas.), Tardive Dvskinesia. New York: SP Medical
& Scientific Books, 1980.
Sover, R. Tardive Dyskinesia: Diagnosis and Treatment.
East Hnover, New Jersey. Sandoz Pharmaceuticals Medical
Education Service, 1978.
Sutcher, ,H. D., Underwood, R. B., & Beatty, R. A. Orofacial
dyskinesia: a dental dimension. Journal of the
American Medical Association. 1971, 216, 14b9-i463.
Tamminga, C. A., Smith, R. C., Ericksen, S. E., Chang, S.,
& Davis, J. M. Cholinergic influences in tardive
dyskinesia. American Journal of Psychiatry. 1977, 134,
769-774.

136
Tanner, C. M., Goetz, C. G., & Klawans, H. L. Cholinergic
mechanisms in movement disorders: results of physos-
tigmine and scopolamine administration. In Barbeau, A.,
Growdon, J. H., & Wurtman, R. J. (Eds.)/ Nutrition and
the Brain Series (Vol. 5). New York: Raven Press,
1979, 273-284.
Tarsy D. Dopamine-acetylcholine interaction in the basal
ganglia. In Field, W. S. (Ed.), Neurotransmitter
Function, Basic and Clinical Aspects. New York:
Symposia Specialists Medical Books, 1977, 213-246.
Tarsy, D., & Baldessarini, R. J. The tardive dyskinesia
syndrome. In Klawans, H. L. (Ed), Clinical Neuropharma-
cology (Vol. 1). New York: Raven Press, 1976, 29-61.
Tarsy, D., Leopold, N., & Sax, D. S. Physostigmine in
choreiform movement disorders. Neurology, 1974, 24, 28-33,
Thach, B. T., Chase, T. N., & Bosma, J. F. Oral facial
dyskinesia associated with prolonged use of antihistaminic
decongestants. New England Journal of Medicine, 1975,
293, 486-487.
Tune, L., & Coyle, J. T. Serum levels of anticholinergic
drugs in treatment of acute extrapyramidal side effects.
Archives of General Psychiatry. 1980, 31_, 293-291.
Wurtman, R. J., Hirsch, M. M., & Growdon, J. H. Lecithin
consumption raises serum-free choline levels. Lancet,
2, 68-69.