30 SCHIZOPHRENIA BULLETIN Treatment of Schizoaffective Disorders · 2017-06-02 · 30 SCHIZOPHRENIA...
19
30 SCHIZOPHRENIA BULLETIN Treatment of Schizoaffective Disorders by Paul J. Goodnick and Herbert Y. Meltzer Abstract Studies that compare the treatment response of patients diagnosed as primary affective disorder or schizo- affective disorder are reviewed. Although relatively few controlled or uncontrolled studies of the chemotherapy of schizoaffective disorders have been conducted, available evidence suggests that: (1) lithium carbonate is effective in the initial treatment of both schizo- affective mania and mania; (2) antidepressants alone, neuroleptics alone, or their combination can be effective in the initial treatment of both schizoaffective depression and primary depression; and (3) prophy- lactic administration of lithium carbonate may reduce the frequency and duration of relapse in both schizoaffective manic and schizo- affective depressed patients. Thus, treatment studies indicate that the schizoaffective disorders are very similar to the primary affective disorders with regard to response to pharmacologlc treatment. Evidence from this laboratory that schizo- affective manic patients respond more slowly than manic patients to lithium or neuroleptic treatment is presented. The controversy as to whether schizoaffective disorder is a subtype of schizophrenia (American Psychiatric Association 1968; Detre and Jarecki 1971), a form of primary affective illness (Pope and Lipinski 1978), or a unique syndrome with a unique etiology, biological concom- itants, genetic predispositions, and treatment outcome (American Psychiatric Association 1980; Klein et al. 1981) has been reviewed in other articles in this issue from the vantage point of epidemiology, family history, genetics, and biological studies. Clinical response to somatic treatment may also be of value in clarifying the relationship between the major psychoses. For example, it has been suggested that a good thera- peutic response to lithium or antide- pressant drug treatment may be a criterion for differentiation of primary affective illness from other types of psychiatric illness (Forssman and Walinder 1970; Sicignano and Lichtenstein 1978). Other investi- gators have discussed and usually rejected this possibility (Noack and Trautner 1951; Kingstone 1960; Wharton and Fieve 1966; Goodwin, Murphy, and Bunney 1969; Shopsin, Johnson, and Gershon 1971; Dunner and Fieve 1978; Schou 1979; Braden et al. 1982). Should established therapies of affective disorders fail to be of clinical value in the treatment of schizoaffective depression, schizo- affective mania, or both, this would provide some indication that the latter are either not related to affective disorders or that they are -very distinct subtypes of affective disorders with an important discon- tinuity in the area of treatment response. However, prophylactic effects of somatic treatment on affective and schizoaffective disorders might be more informative because of the greater likelihood that a common etiological factor might have to be present for a prophylactic effect to be manifest. We will review studies which compare various effects of somatic treatment in schizoaffective and major affective disorders: (1) the effectiveness of various drug treatments in the initial treatment of schizoaffective mania and depression; (2) prophylactic treatment of schizo- affective and primary affective disorders; (3) differences in drug Reprint requests should be sent to Dr. P.J. Goodnick, Illinois State Psychiatric Institute, 1601 W. Taylor St., Chicago. 1L 60612.
Transcript of 30 SCHIZOPHRENIA BULLETIN Treatment of Schizoaffective Disorders · 2017-06-02 · 30 SCHIZOPHRENIA...

30 SCHIZOPHRENIA BULLETIN
Treatment ofSchizoaffective Disorders
by Paul J. Goodnickand Herbert Y. Meltzer
Abstract
Studies that compare the treatmentresponse of patients diagnosed asprimary affective disorder or schizo-affective disorder are reviewed.Although relatively few controlled oruncontrolled studies of thechemotherapy of schizoaffectivedisorders have been conducted,available evidence suggests that: (1)lithium carbonate is effective in theinitial treatment of both schizo-affective mania and mania; (2)antidepressants alone, neurolepticsalone, or their combination can beeffective in the initial treatment ofboth schizoaffective depression andprimary depression; and (3) prophy-lactic administration of lithiumcarbonate may reduce the frequencyand duration of relapse in bothschizoaffective manic and schizo-affective depressed patients. Thus,treatment studies indicate that theschizoaffective disorders are verysimilar to the primary affectivedisorders with regard to response topharmacologlc treatment. Evidencefrom this laboratory that schizo-affective manic patients respondmore slowly than manic patients tolithium or neuroleptic treatment ispresented.
The controversy as to whetherschizoaffective disorder is a subtypeof schizophrenia (AmericanPsychiatric Association 1968; Detreand Jarecki 1971), a form of primaryaffective illness (Pope and Lipinski1978), or a unique syndrome with aunique etiology, biological concom-itants, genetic predispositions, andtreatment outcome (AmericanPsychiatric Association 1980; Klein etal. 1981) has been reviewed in otherarticles in this issue from the vantagepoint of epidemiology, familyhistory, genetics, and biologicalstudies. Clinical response to somatic
treatment may also be of value inclarifying the relationship betweenthe major psychoses. For example, ithas been suggested that a good thera-peutic response to lithium or antide-pressant drug treatment may be acriterion for differentiation ofprimary affective illness from othertypes of psychiatric illness (Forssmanand Walinder 1970; Sicignano andLichtenstein 1978). Other investi-gators have discussed and usuallyrejected this possibility (Noack andTrautner 1951; Kingstone 1960;Wharton and Fieve 1966; Goodwin,Murphy, and Bunney 1969; Shopsin,Johnson, and Gershon 1971; Dunnerand Fieve 1978; Schou 1979; Bradenet al. 1982). Should establishedtherapies of affective disorders fail tobe of clinical value in the treatmentof schizoaffective depression, schizo-affective mania, or both, this wouldprovide some indication that thelatter are either not related toaffective disorders or that they are-very distinct subtypes of affectivedisorders with an important discon-tinuity in the area of treatmentresponse. However, prophylacticeffects of somatic treatment onaffective and schizoaffective disordersmight be more informative becauseof the greater likelihood that acommon etiological factor mighthave to be present for a prophylacticeffect to be manifest.
We will review studies whichcompare various effects of somatictreatment in schizoaffective andmajor affective disorders: (1) theeffectiveness of various drugtreatments in the initial treatment ofschizoaffective mania and depression;(2) prophylactic treatment of schizo-affective and primary affectivedisorders; (3) differences in drug
Reprint requests should be sent to Dr.P.J. Goodnick, Illinois State PsychiatricInstitute, 1601 W. Taylor St., Chicago. 1L60612.
VOL. 10, NO. 1, 1984 31
response between schizoaffective andprimary affective disorders; and (4)the relationship of various diagnosticcriteria for schizoaffective disorder todrug response. The treatment ofschizoaffective disorders with lithiumwas recently reviewed by Delva andLetemendia (1982) and Fieve andGoodnick (1983).
Initial Treatment ofSchizoaffective Mania
The initial treatment of schizo-affective mania and mania withlithium, neuroleptics, or the combi-nation has been intensivelyinvestigated. There are 14 publishedstudies other than case reports, sixdouble-blind and eight open, of theeffect of these drug treatments inschizoaffective mania. Table 1 listseach of these studies, along with adescription of the subjects, diagnosticcriteria, response measures, drugsand dosages, duration of treatment,and an overall summary of theclinical outcome.
Several problems complicate theinterpretation of these studies.Firstly, before the development of theresearch diagnostic criteria (RDC) bySpitzer, Endicott, and Robins (1978),there was even greater ambiguity andvariation in the diagnostic criteria forall three diagnostic categories thancurrently exists. Some studiesinitially included schizoaffectivepatients with schizophrenic patientsand only later considered bothgroups separately. This raises thepossibility that the schizoaffectivepatients included were those whosesymptomatology was closer toschizophrenia than to affectiveillness. Studies designed to contrastthe response of schizoaffective witheither primary affective disorder orschizophrenia are more likely toproduce reliable comparisons.Secondly, many studies (Rice 1956;
Wharton and Fieve 1966; Gottfries1968; Aronoff and Epstein 1970;Megrabyan et al. 1979; Pope et al.1980) did not apply rating scales to ^measure clinical change. However,we have opted to include their resultsin this review when we consider theglobal assessments of all studies.Finally, in all but two studies,treatment periods were 1 month orless which may be inadequate toassess clinical efficacy (see below).
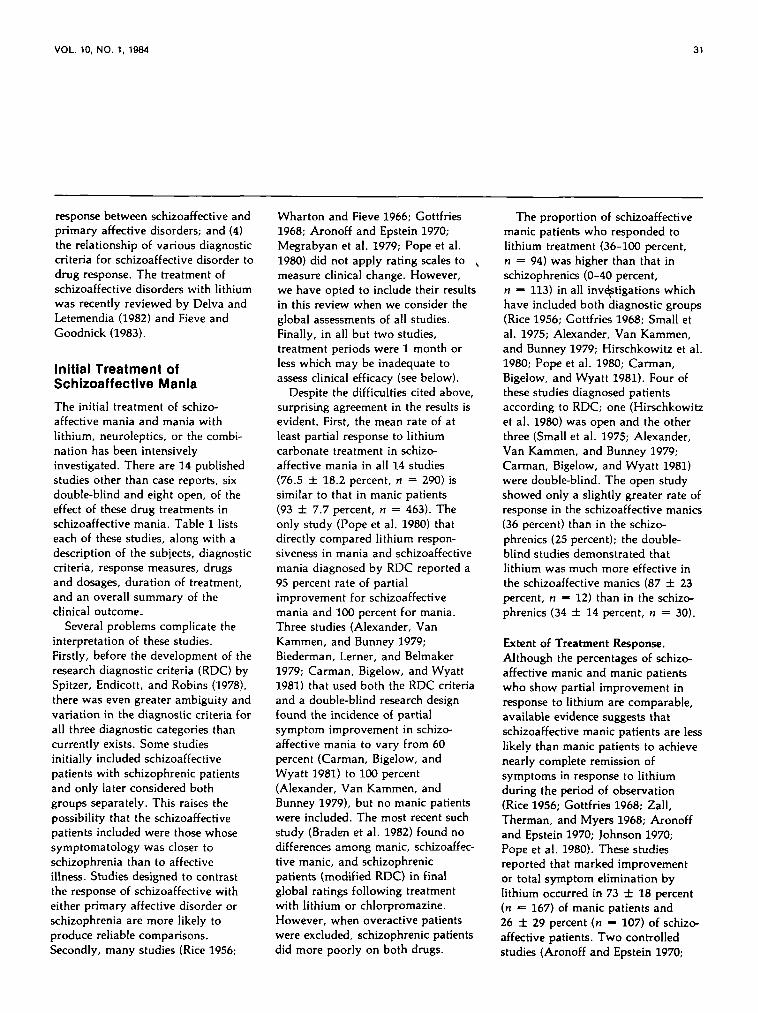
Despite the difficulties cited above,surprising agreement in the results isevident. First, the mean rate of atleast partial response to lithiumcarbonate treatment in schizo-affective mania in all 14 studies(76.5 ± 18.2 percent, n = 290) issimilar to that in manic patients(93 ±7.7 percent, n = 463). Theonly study (Pope et al. 1980) thatdirectly compared lithium respon-siveness in mania and schizoaffectivemania diagnosed by RDC reported a95 percent rate of partialimprovement for schizoaffectivemania and 100 percent for mania.Three studies (Alexander, VanKammen, and Bunney 1979;Biederman, Lerner, and Belmaker1979; Carman, Bigelow, and Wyatt
1981) that used both the RDC criteriaand a double-blind research designfound the incidence of partialsymptom improvement in schizo-affective mania to vary from 60percent (Carman, Bigelow, andWyatt 1981) to 100 percent(Alexander, Van Kammen, andBunney 1979), but no manic patientswere included. The most recent suchstudy (Braden et al. 1982) found nodifferences among manic, schizoaffec-tive manic, and schizophrenicpatients (modified RDC) in finalglobal ratings following treatmentwith lithium or chlorpromazine.However, when overactive patientswere excluded, schizophrenic patientsdid more poorly on both drugs.
The proportion of schizoaffectivemanic patients who responded tolithium treatment (36-100 percent,n = 94) was higher than that inschizophrenics (0-40 percent,n — 113) in all investigations whichhave included both diagnostic groups(Rice 1956; Gottfries 1968; Small etal. 1975; Alexander, Van Kammen,and Bunney 1979; Hirschkowitz et al.1980; Pope et al. 1980; Carman,Bigelow, and Wyatt 1981). Four ofthese studies diagnosed patientsaccording to RDC; one (Hirschkowitzet al. 1980) was open and the otherthree (Small et al. 1975; Alexander,Van Kammen, and Bunney 1979;Carman, Bigelow, and Wyatt 1981)were double-blind. The open studyshowed only a slightly greater rate ofresponse in the schizoaffective manics(36 percent) than in the schizo-phrenics (25 percent); the double-blind studies demonstrated thatlithium was much more effective inthe schizoaffective manics (87 ± 23percent, n ~ 12) than in the schizo-phrenics (34 ± 14 percent, n = 30).
Extent of Treatment Response.Although the percentages of schizo-affective manic and manic patientswho show partial improvement inresponse to lithium are comparable,available evidence suggests thatschizoaffective manic patients are lesslikely than manic patients to achievenearly complete remission ofsymptoms in response to lithiumduring the period of observation(Rice 1956; Gottfries 1968; Zall,Therman, and Myers 1968; Aronoffand Epstein 1970; Johnson 1970;Pope et al. 1980). These studiesreported that marked improvementor total symptom elimination bylithium occurred in 73 ± 18 percent(n «= 167) of manic patients and26 ± 29 percent (n - 107) of schizo-affective patients. Two controlledstudies (Aronoff and Epstein 1970;

Ta
ble
1.
Ac
ute
tre
atm
en
t o
f s
ch
izo
aff
ec
tlv
e m
an
ia a
nd
man
ia
Stu
dy
Ric
e (1
956)
Gp
ttfr
les
(196
8)
Zal
l, T
her
man
,*
Mye
rs(1
968)
Aro
noff
&E
pst
ein
(19
70)
Joh
nso
n(1
970)
Prt
en,
Caf
fey,
&K
lett
(19
72a,
1972
6)
Sm
all
et a
l.(1
975)
Bro
ckln
gto
net
al.
(197
8)
Meg
rab
yan
et a
l. (1
979)
Ale
xan
der
,V
an K
amm
en,
& B
un
ney
(197
9)
Su
bje
cts
37 M
D9
SA
12 S
32 M
D19
SA
10 S
33 M
D10
SA
12 M
D6
SA
19 M
D11
SA
255
MD
83 S
A
4 S
AM
4 S
AD
14 S
19 S
AM
23 S
A
3 S
AM
5 S
AD
5S
Dia
gn
ost
iccr
iter
ia
Au
tho
r's
Un
stat
ed
Au
tho
rs'
Au
tho
rs'
Au
tho
r's
DS
M-I
IM
ayer
-Gro
ss
Fel
gh
ner
Au
tho
rs'
PS
EA
uth
ors
'
Au
tho
rs'
RD
CD
SM
-II
Res
po
nse
mea
sure
s
Au
tho
r's
Un
stat
ed
Au
tho
rs'
Au
tho
rs'
BP
RS
CG
I
BP
RS
IMP
SP
IP BP
RS
CG
IN
OS
IE
BP
RS
Au
tho
rs'
Bun
ney-
Ham
bu
rg
Med
icat
ion
Lit
hiu
m
Lit
hiu
mP
lace
bo
Lit
hiu
mP
lace
bo
Lit
hiu
m
Lit
hiu
mP
lace
bo
Lit
hiu
m
CP
Z
Co
nti
nu
edn
euro
lep
tlc
Lit
hiu
mP
lace
bo
Lit
hiu
m
CP
Z
Lit
hiu
mP
lace
bo
Lit
hiu
mP
lace
bo
Do
se
0.4-
2.4
Blo
od
lev
el1.
0 m
Eq
/l
Max
imu
mb
loo
d l
evel
1.5
mE
q/l
Min
imu
mb
loo
d l
evel
0.9
mE
q/l
Blo
od
lev
el1.
0-2.
5 m
Eq
/l
Blo
od
lev
el0.
6-2.
0 m
Eq
/l10
00 m
g
Blo
od
lev
el0.
6-1.
0 m
Eq
/l
Th
erap
euti
cb
loo
d l
evel
sM
inim
um
400
mg
Blo
od
lev
els
1.5-
2.0
mE
q/l
Blo
od
lev
els
0.7-
1.2
mE
q/l
Du
rati
on
1 m
on
th
6 w
eeks
2 w
eeks
10-1
4 d
ays
21 d
ays
3 w
eeks
4 w
eeks
1 m
on
th
Un
kno
wn
3 w
eeks
Co
nd
itio
n
Op
en
Op
en
Op
en
Var
iou
s
Do
ub
le-b
lind
Do
ub
le-b
lind
Do
ub
le-b
lind
Do
ub
le-b
lind
Un
kno
wn
Do
ub
le-b
lind
Res
ult
s
(% I
mp
rove
d+
re
cove
red
)M
D9
2S
A7
8S
25
(% I
mp
rove
d)
MD
94
SA
84
SO
(% I
mp
rove
d)
MD
79
SA
90
(lit
tle
effe
cton
S t
ype
sym
pto
ms)
(% I
mp
rove
d)
MD
100
SA
67
(% I
mp
rove
d)
MD
95
SA
45
(Im
pro
vem
ent
aver
-ag
ed o
ver
enti
reg
rou
p)
Lit
hiu
m =
CP
Z"H
igh
ly a
ctiv
e,"
CP
Zb
ette
r
(% I
mp
rove
d)
SA
M 1
00S
AD
25
S4
3
(% I
mp
rove
d)
Lit
hiu
m 8
3C
PZ
80
(% I
mp
rove
d)
Lit
hiu
m 8
3
(% I
mp
rove
d)
SA
M 1
00S
AD
40
S4
0
N O -o 3D m I-

Ble
der
man
,Le
rner
, &
Bel
mak
er(1
979)
Po
pe
et a
l.(1
980)
36 S
A
34 M
O52
SA
41 S
RO
C
RD
C
BP
RS
CG
IB
elg
el-M
urp
hy
Ph
ysic
ian
no
tes
Co
nti
nu
edn
euro
lep
tlc
Lit
hiu
mP
lace
bo
Lit
hiu
mN
euro
lep
tlcs
Min
imu
m12
00 m
g
Un
kno
wn
4 w
eeks
Var
iab
le
Do
ub
le-b
lind
Op
en
Car
man
,B
lgel
ow
,&
Wya
tt (
1981
)
Hlr
ech
kow
ltz
et a
l. (1
980)
Qo
od
nlc
k &
Mel
tzer
(198
3)
11 S 5 S
AM
2 S
AD
20
S11
SA
41 M
D30
SA
RD
C
RD
C
RD
C
IBR
S
NH
SI
AD
RS
SA
DS
-CB
PR
S
Co
nti
nu
ed
Blo
od
lev
el
4 w
eeks
neu
role
ptl
c 0.
75-1
.3 m
Eq
/lL
ith
ium
Pla
ceb
o
Lit
hiu
m
Lit
hiu
m
Neu
role
ptl
c
Blo
od l
evel
2
wee
ks1.
1-1.
4 m
Eq
/l
Blo
od
lev
els
0.8-
1.5
mE
q/l
Eq
uiv
alen
tC
PZ
BOO
mg
Var
iab
le
Do
ub
le-b
lind
Op
en
Op
en
Lit
hiu
m b
ette
r th
anp
lace
bo
In
5 s
ub-
scal
es o
f B
PR
S
(%
Mo
der
atel
yIm
prov
ed)
Man
ia:
Lit
hiu
m 1
00[n
=
13)
Lit
hiu
m+
neu
role
ptl
c 10
0(n
=
17)
Neu
role
ptl
c 67
(n =
3)
Sch
lzo
man
lc:
Lit
hiu
m 9
5(n
=
20)
Lit
hiu
m +
ne
uro-
lep
tlc
86 (
n =
14
)N
euro
lep
tlc
83(n
=
12)
Sch
izo
ph
ren
ia:
Neu
role
ptl
c 55
(n =
40
)
(%
Imp
rove
d)
Psy
cho
sis:
SA
M 6
0S
18
Aro
usa
l: S
AM
80
S3
6
% I
mp
rove
d:
S2
5.0
SA
36
.0
(%
Imp
rove
d)
MD
100
SA
100
Dif
fere
nce
s o
nly
In
deg
ree
and
rate
of
resp
on
se
O O
MD
i
man
ic-d
epre
ssiv
e; S
A =
sc
hlz
oaf
fect
lve;
S =
» sc
hiz
op
hre
nic
; S
AM
=
sch
lzo
affe
ctlv
e m
anic
(u
sed
wh
en s
chlz
oaf
fect
lve
dep
ress
ed a
lso
pre
sen
t);
SA
D =
sc
hlz
oaf
fect
lve
dep
ress
ed;
RD
=
recu
rren
t d
epre
ssiv
e; N
-DD
=
no
nd
elu
slo
nal
dep
ress
ion
; D
D =
d
elu
sio
nal
dep
ress
ion
; U
P =
u
nip
ola
r;B
P =
b
ipo
lar;
BP
RS
=
Bri
ef P
sych
iatr
ic R
atin
g S
cale
; IM
PS
=
Inp
atle
nt
Mu
ltid
imen
sio
nal
Psy
chia
tric
Sca
le;
CG
I =
Clin
ical
glo
bal
Im
pre
ssio
n;
HA
M =
H
amilt
on
; P
IP =
P
sych
oti
c In
pat
len
t P
rofi
le;
NO
SIE
=
Nu
rses
Ob
serv
atio
n S
cale
for
In
pat
len
t E
valu
atio
n;
RD
C =
R
esea
rch
Dia
gn
ost
ic C
rite
ria;
WH
O o
W
orl
d H
ealt
h O
rgan
izat
ion
; D
SM
=
Dia
gn
ost
ic a
nd
Sta
tist
ical
Man
ual
; P
SE
=
Pre
sen
t S
tate
Exa
min
atio
n;
SC
L-9
0 =
Sym
pto
m C
hec
klls
t-90
;N
HS
I a
New
Hav
en S
chiz
op
hre
nia
In
dex
; IB
RS
=
Inp
atle
nt
Beh
avio
ral
Rat
ing
Sca
le;
SA
DS
=
Sch
edu
le f
or
Aff
ecti
ve D
iso
rder
s an
d S
chiz
op
hre
nia
;C
PZ
=
chlo
rpro
maz
lne;
EC
T =
el
ectr
oco
nvu
lslv
e th
erap
y; "
S"D
=
"Sch
izo
ph
ren
ic m
ixtu
re"
dep
ress
ion
; S
AS
II
= S
oci
al A
dju
stm
ent
Sca
le;
AD
RS
=
Aff
ecti
ve D
iso
rder
Rat
ing
Sca
le.

34 SCHIZOPHRENIA BULLETIN
Johnson 1970) reported manicpatients to have a significantly better
. response to lithium than schizo-affective patients: manic patients(n = 31), 71-79 percent remission;schizoaffective manic patients(n = 17), 9-33 percent remission.However, neither of these studiesused the RDC. All five studies thatdid not use the RDC reported thatonly a small proportion of schizo-affective manics had a nearly fullremission after lithium: mean15 ± 13 percent, range 9-33 percent(n •= 55). Only one (Pope et al.1980) of the six reports, an open oneusing retrospective analysis,employed the RDC. These investi-gators reported marked improvementafter lithium treatment in both manicpatients (92 percent) and schizo-affective patients (80 percent). Thus,a smaller proportion of schizo-affective manic patients diagnosed bycriteria other than the RDC show acomplete response to lithiumcompared to patients who meet theRDC for schizoaffective mania.
Response of Thought Disorder toLithium. An important considerationis the differential response ofparticular symptoms to lithiumtreatment in the schizoaffectivemanic patients. There have beenthree (Small et al. 1975; Biederman,Lerner, and Belmaker 1979; Carman,Bigelow, and Wyatt 1981) double-blind, placebo-controlledinvestigations of lithium carbonate inthe treatment of schizoaffectivemanic patients maintained on neuro-leprics, and one such study(Alexander, Van Kammen, andBunney 1979) in which lithium alonewas used. Three of these studies(Alexander, Van Kammen, andBunney 1979; Biederman, Lerner,and Belmaker 1979; Carman,Bigelow, and Wyatt 1981) used theRDC whereas the other (Small et al.
1975) used criteria devised by itsinvestigators. Biederman, Lerner, andBelmaker (1979) reported lithiummore effective than placebo inreducing ratings of conceptualdisorganization in RDC schizo-affective manic patients; Small et al.(1975) did not find this in schizo-affective manic patients. Alexander,Van Kammen, and Bunney (1979)and Carman, Bigelow, and Wyatt(1981) did not rate change in thoughtdisorder. Several open studies,including Rice (1956) and Zall,Therman, and Myers (1968), foundlithium was effective only in treatingaffective symptoms, in a highproportion of schizoaffective manicpatients. Lithium had a beneficialeffect on thought disorder in only0-10 percent of schizoaffective manicpatients.
Response of Hallucinations toLithium. Auditory hallucinationshave been reported to respond tolithium (Forssman and Walinder1970; Freedman and Schwab 1978;Braden and Quails 1979;Wagemaker, Lippmann, and Bryant1979). Two controlled studies haveused the Brief Psychiatric RatingScale (BPRS; Overall and Gorham1962) to evaluate changes in halluci-nations in schizoaffective manicpatients. The study that used RDCcriteria found lithium to have a slightadvantage over placebo (Biederman,Lerner, and Belmaker 1979); theother showed no difference (Small etal. 1975).
Response of Paranoia and Delusionsto Lithium. There are some data onthe effectiveness of lithium treatmentof paranoid delusions and unspecifiedpsychotic symptoms in schizo-affective manic patients. As withhallucinations, case reports showalmost total remission of these symp-toms in schizoaffective patients
treated with lithium alone (Forssmanand Walinder 1970; Freedman andSchwab 1978; Braden and Quails1979; Wagemaker, Lippmann, andBryant 1979). Alexander, VanKammen, and Bunney (1979) andCarman, Bigelow, and Wyatt (1981)reported results of double-blind,placebo-controlled studies whichfound significant improvement in"psychosis" in schizoaffective manics(RDC) after lithium therapy. Twofurther studies (Small et al. 1975;Biederman, Lerner, and Belmaker1979) that presented change in BPRSratings during lithium treatmentfound no significant change inunusual thinking but significantimprovement in suspiciousness.Biederman, Lerner, and Belmaker(1979) used the RDC, whereas Smallet al. (1975) used Feighner criteria fordefining mania but used their owncriteria to define schizoaffectivemania. In a study of schizoaffectivemanics diagnosed by the RDC(Biederman, Lerner, and Belmaker1979), lithium was significantly betterthan placebo on BPRS subscales.Thus, the three studies that appliedthe RDC for schizoaffective maniadescribed significant lithium-inducedimprovement in psychotic symptoms,whereas the one study that did notfound no response.
Comparison of Lithium andNeuroleptic Response. The relativeefficacy of lithium carbonate andneuroleptics, or their combination, inthe treatment of mania and schizo-affective mania has been examined inonly five studies (Shopsin, Kim, andGershon 1971; Johnson et al. 1971;Prien, Caffey, and Klett 1972a,1972k; Braden et al. 1982). Shopsin,Kim, and Gershon (1971) reportedthat chlorpromazine (CPZ) treatmentproduced greater improvement in 15BPRS items in a group of schizo-affective (n = 4) and schizophrenic

VOL. 10, NO. 1, 1984 35
(n = 17) patients than did lithium.These differences reached statisticalsignificance for the BPRS itemssomatic concern, grandiosity, andsuspiciousness. Johnson et al. (1971)reported the results of a single-blindtrial of CPZ or lithium in 21 manicand 13 schizoaffective manicpatients. Manic patients had anoverall favorable response to bothCPZ and lithium; CPZ was superioronly for the mannerisms scale.However, schizoaffective patientssignificantly responded to CPZ butnot to lithium. The two medicationsproduced equal improvement inpsychotic symptoms, i.e., conceptualdisorganization, suspiciousness,hallucinations, and unusual thoughts.Prien, Caffey, and Klett (1972a,1972b) reported results of theVeterans Administration-NationalInstitute of Mental Health collab-orative study of acute treatment ofmanic (n — 255) and schizoaffectivemanic illness (n = 83). Lithium andCPZ were equally effective in bothgroups overall, but CPZ producedmore rapid sedation in those patientsin both diagnostic groups who were"highly active." Furthermore, in the"highly active" schizoaffectivesubgroup, CPZ produced greaterbenefit than lithium in BPRSconceptual disorganization, suspi-ciousness, and hallucinatorybehavior. Pope et al. (1980), in theonly study using RDC, reportedmoderate improvement or better inmanic patients following eitherlithium alone or lithium plus neuro-leptic in all 30 patients studied. Sucha response was found in two of threemanic patients receiving neurolepticalone. The comparative effectivenessof drug treatments in schizoaffectivepatients was as follows: lithiumalone (95 percent, n = 20), lithiumplus neuroleptic (86 percent,n " 14), and neuroleptic alone (83percent, n = 12). Here, as before.
when schizoaffective patients werediagnosed by specific criteria, theirresponse was similar to that foundfor manic patients, i.e., there is littledifference in therapeutic effectbetween lithium alone, neurolepticalone, or lithium plus neuroleptic.Braden et al. (1982) also found thataside from an initial advantage forchlorpromazine over lithium inoveractive patients, lithium andchlorpromazine produced similarclinical improvement.
Latency to Response inSchizoaffectives and Manic-Depressives. There is some evidenceto suggest that manic patientsrespond more rapidly to lithium thando schizoaffective manic patients.The two studies showing the greatestdiscrepancy in response rates tolithium between manic andschizoaffective manic patients hadthe shortest treatment periods.Aronoff and Epstein (1970), withonly 2 weeks of treatment, reported100 percent of 12 manic patients butonly 67 percent of 6 schizoaffectivemanic patients responded; Johnson(1970), with a 3-week duration oftherapy, found improvement in 95percent of 19 manic but only 45percent of 11 schizoaffective manicpatients. Of the more recent studies,the one with the lowest rate ofresponse to lithium in schizoaffectivemanic patients (36 percent) used onlya 2-week period of drug adminis-tration (Hirschkowitz et al. 1980). Ofthe 10 studies indicating duration oftreatment (table 1), the meanproportion of schizoaffective manicpatients showing improvement in thefive studies with a treatment durationof > 4 weeks was 85 ± 9 percent(n = 56). The five studies with atreatment period of < 3 weeksreported a lower percentage ofresponse, 52 ± 34 percent (n = 41).These rates were nearly significantly
different (t •=• 2.13, df - 8, p < .10).The correlation between treatmentweeks and percentage of schizo-affective patients responding(r - 0.62, df = 8, p < .10) was alsonearly significant.
A Study of Rate and Extent ofSymptom Response In Manics andSchizoaffectives. Some of thequestions concerning symptomimprovement and rate of response inmania and schizoaffective maniahave been considered in a recentlycompleted study from this laboratory(Goodnkk and Meltzer 1983).Preliminary results will be reportedhere. Seventy-one patients,subdivided into both major (mania,n — 41, and schizoaffective mania,n — 30) and minor (mania:psychotic, n = 23, and nonpsy-chotic, n = 18; schizoaffectivemania: mostly affective, n = 17, andmostly schizophrenic, n = 13)categories, were diagnosed accordingto the RDC, and by the presence orabsence of delusions, hallucinations,or both. The dose of lithium was1,500-1,800 mg/day in both diag-nostic groups, regardless of whetherneuroleptic drugs were also admin-istered. The peak daily dose ofneuroleptic in chlorpromazineequivalents was 1,200-1,400 mg/dayin both diagnostic groups, regardlessof whether lithium was also given.Of the 41 manic patients, 25 receivedlithium alone, 3 received neurolepticalone, and 13 received lithium plusneuroleptic. Of the 30 schizoaffectivepatients, 9 received lithium alone, 11neuroleptic alone, and 10 receivedlithium plus neuroleptic. This distri-bution was significantly different(chi-square •= 11.08, p - 0.004).The patients were evaluated by atrained clinical psychologist with twoinstruments: the BPRS completed atadmission and discharge/ and theSchedule for Affective Disorders and

36 SCHIZOPHRENIA BULLETIN
Schizophrenia-Change (SADS-C;Endicott and Spitzer 1978) completedweekly. Furthermore, the GlobalAdjustment Scale (GAS) from theSADS-C was evaluated to identifythe week in which each patientreached 80 percent of maximalimprovement. Comparisons werethen made between diagnostic groupswith regard to: (1) change inSADS-C and BPRS subscale andtotal scores; (2) mean number ofweeks until 80 percent of maximalimprovement was reached; and (3)response to particular treatmentregimens.
Symptom Response. Evaluation ofclinical response by diagnosis andtreatment showed no majordifferences between schizoaffectivemanic and manic patients withregard to changes in GAS or totalBPRS for all treatment (see table 2)or for the three types of treatments.An analysis of the response of
specific SADS-C and BPRS items isof interest with regard to the issue oflithium specificity for affectivesymptoms. First, as shown in table 2,both schizoaffective and manicpatients showed a good response,'with significant improvementobserved in both affective symptoms(SADS-C manic syndrome, delusionsof grandeur; BPRS grandiosity,excitement) and nonaffectivesymptoms (SADS-C delusions ofreference and persecution, thoughtdisorder; BPRS conceptual disorgan-ization, suspiciousness, halluci-nations). The only exception is theSADS-C rating for auditory halluci-nations for which the manic patientgroup did not show significantimprovement. This is most likely dueto the low baseline rating of thissymptom in those patients, sinceimprovement was clearly evident,from an initial mean score of 0.82 toa final of 0.08. The combination oflithium plus neuroleptic was superior
to lithium alone only in reducing thesuspiciousness score on the BPRS(F - 5.35, df - 2, p = .04). Therewas no drug X diagnosis interactionfor the suspiciousness item. Nodifferences among treatmentcategories were found for thoughtdisorder, hallucinations, or delusions.This indicates that lithium is effectivefor nonaffective symptoms, and thatthe three treatments are equally effec-tive in decreasing nonaffective symp-toms. The finding that psychoticsymptoms in the schizoaffectivemanic patients respond to lithiumagrees with those of Biederman,Lerner, and Belmaker (1979);Alexander, Van Kammen, andBunney (1979); and Carman,Bigelow, and Wyatt (1981). They arealso in accord with those of Pope etal. (1980), in that all RDC schizo-affective manic patients showedmarked improvement duringtreatment; GAS scores increased amean of 40.3 points (141 percent
Table 2. Changes in symptom ratings after treatment
SADS-CGASManic syndromeAuditory hallucinationsDelusions of reference & persecutionDelusions of grandeurThought disorderBPRS (scales 0-6)Total BPRSConceptual disorganizationGrandiositySuspiciousnessHallucinationsExcitement
Baseline
Schizoaffec-tive mania
(n = 30)
28.6 ±14.117.0 ± 12.92.57 ± 2.873.03 ± 2.123.37 ± 2.703.22 ± 3.32
29.3 ±11.43.03 ± 1.942.71 ± 2.072.34 ± 1.942.31 ± 2.012.31 ± 1.86
Bipolarmania
(n = 41)
32.8 ± 13.021.2 ± 8.80.82 ± 1.451.71 ± 2.041.97 ± 2.200.95 ± 1.63
21.3 ± 10.92.10 ± 1.553.10 ± 1.661.48 ± 1.681.10 ± 1.562.18 ± 1.68
After treatment
Schizoaffec-tive mania(n = 30)
68.9 ± 16.9 1
1.81 ± 3.95 '0.38 ± 1.18'0.28 ± 0.77 1
0.53 ± 1.19'0.47 ± 1.44'
7.6 ± 9.0 '0.35 ± 1.05'0.64 ± 1.23 '0.42 ± 0.96 1
0.13 ± 0.57 '0.42 ± 0.92 '
Bipolarmania
(n = 41)
72.1 ± 17.3'3.08 ± 6.13 '0.08 ± 0.350.32 ± 0.83 1
0.52 ± 1.47 '0.02 ± 0.16 '
5.4 ± 5.7 '0.10 ± 0.38 1
0.69 ± 1 . 3 6 '0.31 ± 0.69 1
0.13 ± 0.57 '0.44 ± 0.94 1
1 p < .005.

VOL. 10, NO. 1, 1984 37
greater than baseline), and totalBPRS scores decreased 21.7 points(74 percent less than baseline).
Rate of Response. A significantdifference in the duration oftreatment needed to reach 80 percentof maximal improvement was foundfor the two diagnostic groups.Overall, schizoaffective patientsrequired 61.6 ± 31.5 days to achievethis degree of improvement, whereasbipolar manic patients required only26.6 ± 18.9 days (p < .001). Thus,it took about twice as long for eachtreatment to achieve the same degreeof effectiveness in the schizoaffectivemanic patients compared to themanic patients.
Neurotoxidty. Johnson (1970) andShopsin, Johnson, and Gershon(1971) concluded that lithium wasmore likely to produce neurotoxicityin schizophrenic and schizoaffectivepatients than in manic patients. Westand Meltzer (1979) also concludedthat acute manic, schizophrenic, andschizoaffective patients were atgreater risk for lithium-inducedneurotoxicity than chronically illpatients. West (1982) suggested thatthe relevant issue for vulnerability toneurotoxicity was not the diagnosisof schizophrenia or schizoaffectivedisorder, but rather duration ofillness; acutely ill patients are morelikely to become neurotoxic duringlithium treatment than chronically illpatients.
Conclusion. In conclusion, lithiumappears to be equally effective in theacute treatment of schizoaffectivemanic and manic patients diagnosedaccording to the RDC. Lithium aloneand neuroleptics alone producecomparable overall improvement andare effective in the treatment ofnonaffective and affective symptomsin both schizoaffective manic and
manic patients. Those studies whichhave reported that neuroleptics aremore effective than lithium in thetreatment of schizoaffective patientshave used criteria other than theRDC. Schizoaffective patients werefound to require a significantlylonger period of drug administrationthan manic patients to achievecomparable remission. Both disordersresponded to treatment with lithium,neuroleptics, and combinedtreatment. Thus, consideration ofdata on treatment of schizoaffectivemania and mania suggests there is noreason to reject the hypothesis thatschizoaffective disorder, as definedby RDC, is a variant of bipolardisorder. However, the much longerperiod which schizoaffective patientsrequire to respond to medicationcompared to manic patients may berelated to important differences inseverity of illness or possiblyunderlying biology.
Initial Treatment ofSchizoaffective Depression
There are 12 published controlledstudies (eight double-blind and fouropen) concerning the efficacy ofpharmacotherapy in the treatment ofschizoaffective depression. Table 3provides a description of thesubjects, diagnostic criteria, responsemeasures, drugs and dosages,duration of treatment, and an overallsummary of the clinical outcome.
Interpretation of these results iscomplicated by the same factorsdiscussed above with reference to thedrug treatment studies of schizo-affective manic patients: problems indiagnosis, lack of application ofstandard measures of clinical change,and variability in treatment periods.
Antidepressant Response. Fourstudies (Angst 1961; Greenblatt,Grosser, and Wechsler 1962; Hordernet al. 1963; Avery and Winokur
1977) have compared the response ofmajor and schizoaffective depressionto antidepressants. The proportion ofpatients who showed improvementwere: bipolar depressives (54 ± 18percent, n = 64), unipolardepressives (59 ± 18 percent,n " 237), and schizoaffectivedepressives (54 ± 18 percent,n «« 49). Three studies that used theRDC—one retrospective (Avery andWinokur 1977), one double-blind(Brockington et al. 1978), and oneopen (Brockington, Kendell, andWainwright 1980)—report a low rateof response of schizoaffective patientsto antidepressant drugs (37 ± 8percent, n = 150). These results aregenerally supported by anotherdouble-blind study (Prusoff et al.1979) which evaluated the effect ofadding amitriptyline to neurolepticsin 40 depressed schizophrenics whowere diagnosed according toDSM-III, but who would probablymeet the RDC for schizoaffectivedepression. Little significantimprovement was found. Twoarticles (Greenblatt, Grosser, andWechsler 1962; Hordern et al. 1963)published data comparing psychoticdepression and schizoaffectivedepression. The rate of response ofschizoaffective depressed patients(23-50 percent, n = 35) was slightlylower than that of psychoticdepressed patients (30-67 percent,n — 33). These results for delusionaldepression are comparable to othermore recent reports (Glassman,Kantor, and Shostak 1975; Nelsonand Bowers 1978; Avery andLubriano 1979).
Neuroleptic Response. Brockingtonet al. (1978) and Brockington,Kendell, and Wainwright (1980)examined the effect of neurolepticsalone, or in combination with antide-pressants, in the acute treatment ofschizoaffective depression. The 1978

Tab
le 3
. A
cute
tre
atm
ent
of
sch
lzo
affe
ctlv
e d
epre
ssio
n a
nd
maj
or
dep
ress
ion
Dia
gn
ost
ic
Res
po
nse
Stu
dy
Su
bje
cts
crit
eria
m
easu
res
Med
icat
ion
D
ura
tio
n
Co
nd
itio
n
Res
ult
s
An
gst
(19
61)
Qre
en
bla
tt,
Gro
sser,
& W
ech
sler
(196
2)
Hord
ern
et
al.
(196
3)
41 M
D
Au
tho
r's
17 R
D7
SA
25 M
D
Au
tho
rs'
24"P
sych
o-
ne
uro
tic"
10P
sych
otic
31 S
A
11
0N
-DD
A
uth
ors
'23
DD
4"S
"D
Au
tho
r's
Glo
ba
l(a
uth
ors
')M
en
tal
sta
tus
score
Depre
ssio
nra
ting
HA
MD
Imlp
ram
lne
200
mg
EC
T(>
9 tr
eat-
ments
)Is
ocar
boxa
zld
40-5
0 m
gP
henelz
lne
60
-75
mg
Imlp
ram
lne
150-
187
mg
Am
itrl
pty
llne
200
mg
Imlp
ram
lne
200
mg
Nonre
sponders
rece
ive
EC
T(a
ll S
A o
na
mitr
lpty
llne
)
2 w
eeks
8 w
eeks
Open
DB
4-6
wee
ksD
B
%
Impro
ved
MD
63
.4R
D5
8.8
SA
D 5
7.1
% M
ark
ed
Im
pro
vem
ent
AD
E
CT
T
ota
lM
D
40.0
80
.0
48.0
Psy
cho-
ne
uro
tic
87.0
71
.0
84.0
Psy
cho
tic
30.0
50
.0
33.0
SA
D
23.0
60
.0
29.0
% Im
pro
vem
ent
to a
mitrl
pty
llne
No
nd
elu
-si
on
al
88.0
De
lusi
on
al
67.0
SA
D
50.0
Sm
all
et a
l.(1
975)
Ave
ry &
Wln
oku
r(1
977)
14 S 4 S
AD
444
UP
47 B
P54
SA
Fe
lgh
ne
r+
a
uth
ors
'
Felg
hner
dia
gn
osi
sR
DC
(S
A)
BP
RS
CG
IN
OS
IE
Clin
ica
lg
lob
al
(MD
note
s)
Co
ntin
ue
dn
eu
role
ptlc
Lith
ium
0.6
-1.0
mE
q/l
Pla
cebo
Am
itrl
pty
llne
150
mg
Imlp
ram
ine
150
mg
Desl
pra
mln
e15
0 m
gN
ort
rlp
tylln
e15
0 m
gP
rotr
lpty
llne
45 m
gP
henelz
lne
45 m
gT
ran
ylcy
pra
mln
e30
mg
Isoca
rboxa
zld
30 m
gE
CT 5 t
rea
tme
nts
4 w
eeks
4 w
eeks
(min
imu
m 2
weeks
at
Indic
ate
ddru
g d
ose
)
DB
Re
tro
spe
ctiv
e
UP
BP
SA
D
% P
osi
tive
resp
onse
S
43.0
SA
D
25.0
%
Impro
ved
aft
er
tre
atm
en
tE
CT
A
D52
26
43
3341
33
co O I N o TJ I ;o m z C m 2

Bro
ckln
gto
net
al.
(197
8)41
SA
(36 s
tud
ied
)P
SE
+a
uth
ors
'B
PR
SP
SE
Am
ltrl
pty
llne
150-2
50 m
g (1
3)C
PZ 450-7
50 m
g (
11)
Co
mb
ine
d (
12)
1 m
on
thD
B%
Im
pro
ved a
fte
r tr
ea
tme
nt
(all
SA
D)
Am
itrlp
ty-
line
45C
PZ
54
Am
ltryp
ty-
line +
CP
Z
75
O z o
Ale
xan
de
r, V
anK
am
me
n,
& B
unney
(197
9)
Van
Ka
mm
en
,A
lexa
nd
er,
&B
unney
(198
0)
Pru
80ff e
t a
l.(1
979)
5S
5 S
AD
1S 10 S
AD
40 D
ep S
RD
CD
SM
-II
RD
C
DS
M-I
IN
HS
I+
aut
hors
'
Bun
ney-
Ha
mb
urg
Bunney-
Ham
burg
NH
SI
BP
RS
HA
M de
pre
ssio
nR
ask
inS
CL
-90
SA
S I
I
Lith
ium
mea
n16
00 m
g0.7
-1.2
mE
q/l
pla
sma
Pla
cebo
Lith
ium
900-2
100 m
g0.7
-1.3
mE
q/l
pla
sma
Co
ntin
ue
dperp
henazl
ne
Am
ltrl
pty
llne
100-2
00 m
gP
lace
bo
Hlr
ach
kow
ltzet
al.
(198
0)
Bro
ckln
gto
n,
Ke
nd
ell,
&W
aln
wrl
gh
t(1
980)
20
S9 S
AD
2 S
AM
4S
8M
D60
SA
D4 O
the
r
Ca
rma
n,
11 S
Blg
elo
w,
2 S
AD
& W
yatt
(19
81)
RD
C
RD
C
RD
C
3 w
eeks
D
B
3 w
eeks
D
B
1-6 m
on
ths
DB
NH
SI
AD
RS
Au
tho
rs'
IBR
S
Lith
ium
1.1
-1.4
mE
q/l
Trl
cycl
lc a
nti-
de
pre
ssa
nts
,va
rio
us
ne
uro
lep
tlcs
EC
T
Co
ntin
ue
dn
eu
role
ptlc
Lit
hiu
m0.7
5-1
.3 m
Eq/l
Pla
cebo
2 w
eeks
Var
iabl
e
4 w
eeks
Ope
n
Open
DB
Imp
rove
d:
S 4
0%
SA
40
%
Impro
vem
ent
In d
ep
ress
ion
ratin
g (
more
th
an 1
.5)
60
% o
f S
AD
Sym
pto
m I
mpro
vem
ent
of.0
5 s
ign
ific
an
ceB
PR
S t
ho
ug
ht
dis
ord
er
(6H
AM
D s
om
atlz
a-
tlo
n
(2H
AM
D a
nxi
ety
-d
ep
ress
ion
(4R
ask
in
mo
nth
s)
mo
nth
s)
mo
nth
s)
de
pre
ssio
n
(4 m
on
ths)
%
Imp
rove
d:
S 2
5.0
SA
36
.0
% I
mp
rove
d o
f S
AD
Trl
cycl
lc 3
3N
eu
role
ptlc
55
EC
T 6
2
%
Impro
ved
Psy
cho-
sis
S
18S
AD
0
Dep
res
slo
n36 50
See
no
te t
o t
ab
le 1
fo
r d
efi
nit
ion
s of
ab
bre
via
tion
s.

40 SCHIZOPHRENIA BULLETIN
report was based on a double-blindstudy including amitriptyline alone(150-200 mg), chlorpromazine alone(450-750 mg), and combinedtreatment. The proportion of patientswho recovered in response tochlorpromazine alone was greaterthan the proportion who respondedto amitriptyline. The combination ofdrugs produced partial improvementin a higher proportion of patientsthan either individual treatment (75percent combined, 54 percent chlor-promazine alone, and 46 percentamitriptyline alone). In an openstudy, Brockington, Kendell, andWainwright (1980) also reported thatneuroleptic alone was superior totricyclic antidepressant alone: 55percent of neuroleptic-treated patientsimproved compared to 33 percent oftricyclic antidepressant-treatedpatients.
Lithium Response. Five studies(Small et al. 1975; Alexander, VanKammen, and Bunney 1979; VanKammen, Alexander, and Bunney1980; Hirschkowitz et al. 1980;Carman, Bigelow, and Wyatt 1981)have examined the response ofschizoaffective depressed patients tolithium carbonate. Lithium appearsto have comparable modest efficacyfor both schizoaffective depressionand some forms of schizophrenia. Allbut one of these studies (Small et al.1975) applied RDC. All but one(Hirschkowitz et al. 1980) weredouble-blind. It should be noted thatHirschkowitz et al. (1980) did notseparately describe the clinicalresponse of schizoaffective manic andschizoaffective depressed patients tolithium; therefore, it is not possibleto evaluate fully the results of thisstudy. The proportion of schizo-phrenic and schizoaffective patientswho responded to lithium in theother four reports was 36 ± 8percent (n — 5) and 38 ± 10 percent
(n = 30), respectively. VanKammen, Alexander, and Bunney(1980) reported that 6/10 (60 percent)of schizoaffective depressed patientsreceiving lithium had a reduction ofat least 1.5 on the depression ratingon the Bunney-Hamburg scale.
Electroshock Response. Seven reports(Greenblatt, Grosser, and Wechsler1962; Hordern et al. 1963; Folstein,Folstein, and McHugh 1973; Wells1973; Avery and Winokur 1977;Brockington, Kendell, andWainwright 1980; Ries et al. 1981)present data on the efficacy ofelectroconvulsive therapy (ECT) inthe treatment of schizoaffectivedepression. Two of these (Greenblatt,Grosser, and Wechsler 1962; Averyand Winokur 1977) compared theefficacy of ECT in schizoaffectivedepression and major depression.Both studies demonstrated similarrates of response in bipolardepression (43-80 percent, n = 19),unipolar depression (52-89 percent,n °= 132), and schizoaffectivedepression (41-80 percent, n = 27).Two studies that did not use theRDC (Greenblatt, Grosser, andWechsler 1962; Hordern et al. 1963)report a higher rate of response toECT in schizoaffective depression(80-100 percent) than do studies thatused the RDC (Avery and Winokur1977; Brockington, Kendell, andWainwright 1980) (41-62 percent).These four studies report that ECT ismore effective than pharmacotherapyin the treatment of schizoaffectivedepression. A similar conclusion hasbeen reached with regard topsychotic depression. Overall,54 ± 12 percent (n =• 56) markedlyimproved following ECT, but only30 ±6 percent (n - 75) after antide-pressants. Three studies (Folstein,Folstein, and McHugh 1973; Wells1973; Ries et al. 1981) noted thatschizoaffective patients responded
better to ECT than did schizo-phrenics, and that the response ratein the schizoaffectives was compara-ble to that usually reported in affec-tive patients.
Thus, the response to drugtreatment and ECT of schizoaffectivedepressed patients is not significantlydifferent from that of majordepression, very close to that foundin delusional depression, butsignificantly better than that ofschizophrenics. ECT is superior toantidepressant drugs but, even then,the maximal percentage of RDCschizoaffective depressed patientsresponding is approximately 50percent. Few schizoaffectivedepressed patients respond to eitherantidepressant alone or lithiumalone.
A Study of Symptom Response inSchizoaffective Depression. Thecomparative effectiveness of drugtreatment of schizoaffectivedepression and major depression onspecific symptoms was considered ina retrospective analysis from thiscenter. Fifty-six patients with majordepressive disorder and 44 patientswith schizoaffective depression,diagnosed according to the RDC,were included in an analysis ofsymptom change during the course oftreatment with neuroleptics orantidepressants. A criterion forinclusion in this analysis was apretreatment GAS rating from theSADS of 60 or below. A furtherrequirement was a 3-week treatmentperiod with a neuroleptic at a dose ofat least 600 mg equivalent of chlor-promazine or 150 mg imipramine,desipramine, amitriptyline, ormaprotiline, of 75 mg of nortrip-tyline, and of 300 mg of trazodone.The patients were evaluated weeklyby a trained psychologist with theSADS-C. Symptom response wasmeasured by change in the GAS,
VOL. 10, NO. 1, 1984 41
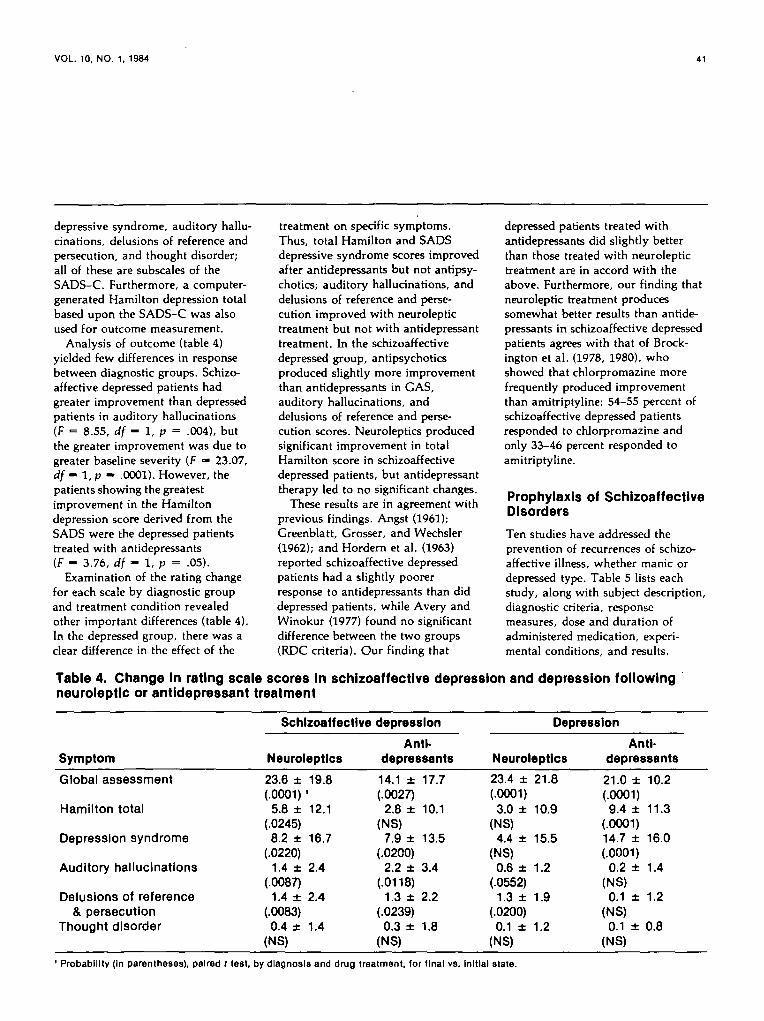
depressive syndrome, auditory hallu-cinations, delusions of reference andpersecution, and thought disorder;all of these are subscales of theSADS-C. Furthermore, a computer-generated Hamilton depression totalbased upon the SADS-C was alsoused for outcome measurement.
Analysis of outcome (table 4)yielded few differences in responsebetween diagnostic groups. Schizo-affective depressed patients hadgreater improvement than depressedpatients in auditory hallucinations(F = 8.55, df - 1, p = .004), butthe greater improvement was due togreater baseline severity (F — 23.07,df - 1, p - .0001). However, thepatients showing the greatestimprovement in the Hamiltondepression score derived from theSADS were the depressed patientstreated with antidepressants(F - 3.76, df - 1, p = .05).
Examination of the rating changefor each scale by diagnostic groupand treatment condition revealedother important differences (table 4).In the depressed group, there was aclear difference in the effect of the
treatment on specific symptoms.Thus, total Hamilton and SADSdepressive syndrome scores improvedafter antidepressants but not antipsy-chotics; auditory hallucinations, anddelusions of reference and perse-cution improved with neuroleptictreatment but not with antidepressanttreatment. In the schizoaffectivedepressed group, antipsychoticsproduced slightly more improvementthan antidepressants in GAS,auditory hallucinations, anddelusions of reference and perse-cution scores. Neuroleptics producedsignificant improvement in totalHamilton score in schizoaffectivedepressed patients, but antidepressanttherapy led to no significant changes.
These results are in agreement withprevious findings. Angst (1961);Greenblatt, Grosser, and Wechsler(1962); and Hordern et al. (1963)reported schizoaffective depressedpatients had a slightly poorerresponse to antidepressants than diddepressed patients, while Avery andWinokur (1977) found no significantdifference between the two groups(RDC criteria). Our finding that
depressed patients treated withantidepressants did slightly betterthan those treated with neuroleptictreatment are in accord with theabove. Furthermore, our finding thatneuroleptic treatment producessomewhat better results than antide-pressants in schizoaffective depressedpatients agrees with that of Brock-ington et al. (1978, 1980), whoshowed that chlorpromazine morefrequently produced improvementthan amitriptyline; 54-55 percent ofschizoaffective depressed patientsresponded to chlorpromazine andonly 33-46 percent responded toamitriptyline.
Prophylaxis of SchizoaffectiveDisorders
Ten studies have addressed theprevention of recurrences of schizo-affective illness, whether manic ordepressed type. Table 5 lists eachstudy, along with subject description,diagnostic criteria, responsemeasures, dose and duration ofadministered medication, experi-mental conditions, and results.
Table 4. Change in rating scale scores in schizoaffective depression and depression followingneuroleptic or antidepressant treatment
Schizoaffective depression Depression
Symptom
Global assessment
Hamilton total
Depression syndrome
Auditory hallucinations
Delusions of reference& persecution
Thought disorder
Neuroleptics
23.6 ± 19.8(.0001)'
5.8 ± 12.1(.0245)8.2 ± 16.7
(.0220)1.4 ± 2.4
(.0087)1.4 ± 2.4
(.0083)0.4 ± 1.4
(NS)
Anti-depressants
14.1 ± 17.7(.0027)
2.8 ± 10.1(NS)
7.9 ± 13.5(.0200)
2.2 ± 3.4(.0118)
1.3 ± 2.2(.0239)
0.3 ± 1.8(NS)
Neuroleptics
23.4 ±(.0001)3.0 ±
(NS)4.4 ±
(NS)0.6 ±
(.0552)1.3 ±
(.0200)0.1 ±
(NS)
21.8
10.9
15.5
1.2
1.9
1.2
Anti-depressants
21.0 ±(.0001)9.4 ±
(.0001)14.7 ±(.0001)
0.2 ±(NS)0.1 ±
(NS)0.1 ±
(NS)
10.2
11.3
16.0
1.4
1.2
0.8
1 Probability (In parentheses), paired t test, by diagnosis and drug treatment, for final vs. Initial state.

Tab
le 5
. P
rop
hyl
acti
c tr
eatm
ent
of s
chiz
oaf
fect
lve
dis
ord
ers
Dia
gnos
tic
Res
pons
eS
tudy
S
ubje
cts
crite
ria
mea
sure
s M
edic
atio
nD
ose
Dur
atio
n
Con
ditio
nR
esul
ts
Hof
man
net
al.
(197
0)
Aro
noff
&E
pste
in (1
970)
Ang
stet
al.
(197
0)
Prle
n, C
afle
y,&
Kle
tt(1
973,
197
4)
46 M
D54
RD
19 S
A
12 M
D6S
A
114
MD
58 R
D72
SA
192
MD
6SA
DS
M-I
IA
utho
rs'
Aut
hors
'
WH
OA
utho
rs'
DS
M-I
IM
ayer
-Gro
ss
Aut
hors
Aut
hors
'
Hos
pita
lad
mis
sion
Cha
nge
Intre
atm
ent
IMP
SG
loba
l af
fect
ive
KA
S
Lith
ium
Lith
ium
Lith
ium
Lith
ium
Pla
cebo
Unk
now
n
Min
imum
bloo
d le
vel
0.6
mE
q/l
0.8-
1.2
mE(
bloo
d le
v
0.5-
1.4
mE
q/l
bloo
d le
vel
Unk
now
n
3 ye
ars
1-4
year
s
Ope
n
Ope
n
Ope
n
2 ye
ars
Dou
ble-
blin
d
% A
t le
ast
mod
erat
epr
even
tion
MD
72S
A53
% M
oder
ate
prev
entio
nM
D58
SA
83
% W
ith d
ecre
ased
freq
uenc
y of
epis
odes
MD
67R
D57
SA
49
% S
ever
e re
laps
eaf
ter d
isco
n-tin
uing
lithi
umM
D31
SA
60
Sm
ulev
ltch
et a
l. (1
974)
Hul
lln,
McD
onal
d,&
Alls
opp
(197
5)
50 M
D49
SA
9 M
47 M
D36
RD
3SA
WH
OD
SM
-II
Aut
hors
'
Aut
hors
'
Hos
pita
lad
mis
sion
sTi
me
Inho
spita
l
Lith
ium
Pla
cebo
Lith
ium
Pla
cebo
0.6-
0.8
mE
q/l
bloo
d le
vel
0.6-
1.4
mE
q/l
bloo
d le
vel
1-3
year
s
18-7
5 m
onth
s
Ope
n
Ope
n
Effe
ctiv
e %
MD
88S
A83
% R
eadm
issi
ondu
ring
treat
men
tM
0M
D45
RD
19
SA
33
Per
rls (197
8)
Tre
ss &
Haa
g (1
979)
18"C
yclo
idps
y-ch
osis
"
21 M
D22
SA
Aut
hor's
(sim
ilar
to D
SM
-II
"sch
lzo-
affe
ctlv
e")
Leon
hard
Aut
hors
'
Epi
sode
sM
onth
s of
hosp
italiz
e-tlo
n
Epi
sode
s
Lith
ium
Pla
cebo
Lith
ium
0 6-
0.8
m E
q/I
bloo
d le
vel
Unk
now
n
1-8.
5 ye
ars
Ope
n
MD
: 2.
8 ±
1.8y
ear3
SA
: 2.
4 ±
1.4
year
s
Ope
n
% R
educ
tion
afte
rtre
atm
ent
Epi
sode
s 76
Mon
ths
hosp
ltall-
zatlo
n 90
% R
educ
tion
Inre
laps
e/pa
tient
/ye
arM
D51
SA
69
CO O I Isl o -0 I 3J m zCD 3 z

VOL. 10, NO. 1, 1984 43
co co 2 CO
- £ ° -o§O +5o
o
E
JC
o gco o
Ooa:
2<2 co
OQa:
lig •IT
a CO
SI15
1 CO
3 5 1> m
E a:
S c5 oii 3
S o
co 3E nII o
ii
The 10 studies compare results on220 schizoaffective patients,diagnosed according to variousdiagnostic criteria, with that of 574manic-depressive and 148 patientswith recurrent depression. Only 1 ofthe 10 studies was double-blind; itincluded only six schizoaffectivesubjects. All 10 studies used lithiumcarbonate for prophylaxis.
Some of the earlier studies report abetter response in bipolar patients(67-72 percent, n = 365) than inschizoaffective manic patients (40-53percent, n = 97) (Angst et al. 1970;Hofmann et al. 1970; Prien, Caffey,and Klett 1973, 1974). The finding ofAngst et al. (1970) that lithiumsignificantly reduced the frequency ofepisodes in schizoaffective patientsand the report of Prien, Caffey, andKlett (1973, 1974) that the relapserate of schizoaffective patientsincreased to 60 percent after the dis-continuation of lithium stronglyindicate that lithium was exerting aprophylactic action, even in theabsence of a placebo control. Recentstudies, which have had equalnumbers of subjects in eachdiagnostic group and clearly definedcriteria for diagnosis, have reportedmore equivalent efficacy in bothdiagnostic groups than the earlierones. Thus, the studies of Rosenthalet al. (1980) and Sarantidis andWaters (1981), which used the RDC,found that schizoaffective patients re-mained as well on lithium as didmanic patients. Rosenthal et al.(1980) compared the probability ofnonrelapse in manic and schizo-affective manic patients at weeks 16,52, and 104 of lithium treatment.After 1 year of treatment, schizo-affective patients were 13 percentmore likely to be in remission thanmanic patients; after 2 years, schizo-affective patients were 6 percent lesslikely than manic patients to still bein remission. Sarantidis and Waters
(1981) used length of hospitalizationas the criterion for lithium response.The proportion of patients having atleast a fair lithium response wasslightly greater in schizoaffectivemanic patients (89 percent) than inmanic patients (78 percent). Thedecrease in days spent in the hospitalcompared to the year beforebeginning prophylaxis with lithiumwas 62 percent for the manic patientsand 76 percent for the schizoaffectivepatients.
Thus, lithium carbonate,administered at the usual dosesneeded to achieve a plasmaconcentration of 0.6-1.0 mEq/1,appears to be effective in preventingrecurrences of schizoaffectivedisorder in up to 90 percent ofpatients.
Somatic Treatments ofSchizoaffective DisordersOther than Lithium,Neuroleptlcs, andConventional Antidepressants
Apomorphine and Bromocriptine.Dopamine agonists in low doses havebeen administered to psychoticpatients on the premise that stimu-lation of dopamine autoreceptors caninhibit the synthesis and release ofdopamine (Meltzer 1982). Recentstudies (Corsini et al. 1981; Meltzeret al. 1983) have suggested that lowdose dopamine agonist treatmentmay be more effective in the treat-ment of schizoaffective patients thanschizophrenics. Corsini et al. (1981)administered 1 mg of apomorphineintramuscularly to 36 patients orig-inally diagnosed as schizophrenic.Eighteen of these patients showedeither improvement of at least 75percent in baseline Brief PsychiatricRating Scale (BPRS) scores(responders) or no improvement(nonresponders). Diagnosis of thesepatients according to the RDC

44 SCHIZOPHRENIA BULLETIN
indicated that seven of the nineresponders fulfilled criteria forschizoaffective disorder, manic type.Only one of the nine nonresponderswas schizoaffective (depressed type).
. Meltzeretal. (1983) administeredbromocriptine (0.5-6.0 mg/day) toseven schizophrenic and two schizo-affective patients after a 2-4 weekplacebo period. One of the schizo-affective patients showed markedimprovement and the othermoderate, as contrasted to mildimprovement in three of the sevenschizophrenic patients. The otherfour worsened following initialmodest improvement. The schizo-affective depressed patient whoresponded best demonstrated markedimprovement in both affective andpsychotic symptoms on 0.25-0.50mg/day for 3 weeks; a drug responsewas suggested by the relapse andrestoration of improvement when themedication was first withdrawn andthen reinstated.
Des-Tyr-y-Endorphln. The effect ofdes-tyrosine-y-endorphin (DTyE) hasbeen extensively investigated inschizophrenic and schizoaffectivepatients (Verhoeven et al. 1981;Meltzer et al. 1982; Van Praag et al.1982). Verhoeven et al. (1981) andVan Praag et al. (1982) administeredDTyE in doses of 1 mg intramus-cularly for 8-10 days. Nine of 23patients had a slight to moderateresponse; a marked response wasobserved in seven. All patients werealso being treated with neurolepticswhich had not been effective bythemselves. The schizoaffectivepatients (n •» 4) responded consid-erably less well than the chronicschizophrenic patients. Meltzer et al.(1982) conducted an open study ofDTyE in which the drug was admin-istered for 12 days in doses rangingfrom 1 to 10 mg/day. The studygroup included seven schizophrenicpatients and one schizoaffective
manic—mostly schizophrenic patientaccording to RDC. As in theprevious study, the schizoaffectivepatient did much less well than theschizophrenic patients. Threeinstances of moderate or markedimprovement and three of minimalimprovement were found in the sevenschizophrenic patients. There are nodata available on the effect of DTyEin patients with RDC diagnoses ofmajor affective disorder. The datafor the effectiveness of DTyE inschizophrenia and its ineffectivenessin schizoaffective disorders are farfrom conclusive.
L-Tryptophan. The "permissive"hypothesis of affective disorders isbased upon a serotonin deficiencyleading to vulnerability to developeither mania or depression (Prange etal. 1973). For this reason, theserotonin precursor, L-tryptophan,has been used for both the treatmentand prevention of manic-depressivedisorder (Van Praag 1982). A recentstudy compared the clinical responseto L-tryptophan plus lithium versusplacebo plus lithium in manic andschizoaffective manic patients(Brewerton and Reus 1983). Adouble-blind placebo-controlled studywith a 21-day drug treatment periodwas conducted. The patient sampleincluded nine patients with adiagnosis of bipolar disorder andseven with a diagnosis of schizo-affective disorder, according toDSM-III. All patients had ManicState Rating Scale (Beigel, Murphy,and Bunney 1971) scores above 24 atbaseline. L-Tryptophan was adminis-tered in increasing doses over 6 daysto a maximum dose of 3 grams, threetimes per day, between meals.Overall, the patients of bothdiagnostic types who received L-tryptophan showed greaterimprovement on both the ManicState Rating Scale and the Brief
Psychiatric Rating Scale as comparedto those who received only lithium,but this was considered to be moreevident in the schizoaffectivepatients. However, the relativelyliberal use of as needed neurolepticmedication makes it difficult tointerpret this finding.
Bupropion. There is extensiveevidence that bupropion is aneffective antidepressant for unipolarand bipolar depression (Maxwell etal. 1981). It produces few sideeffects, and, of particular impor-tance, has not been noted to producean exacerbation of psychoticsymptoms. This possibility had beenanticipated because bupropion is aneffective inhibitor of dopamineuptake and has few other knownactions (Cooper, Hester, andMaxwell 1980). A recent investi-gation of the antidepressant action ofbupropion suggests a significantdifference between schizoaffectivepatients and those with major affec-tive disorder. Goode and Manning(1983) treated nine schizoaffectivedepressed patients (RDC) withbupropion alone at a dose of 750mg/day. Three of the patients expe-rienced severe exacerbations ofschizophrenic-type symptoms thatrequired their discontinuation fromthe study. The other six patients didnot do particularly well. Eleven otherpatients received bupropion plushaloperidol; five were judged veryimproved and four moderatelyimproved. If it can be confirmed thatbupropion alone may produce antide-pressant effects in major depressionwith psychotic symptoms, but isineffective in schizoaffectivedepression except for producing anexacerbation of schizophrenic-typesymptoms, this drug could become auseful tool for identifying biologicaldifferences between these types ofpatients.

VOL. 10, NO. 1, 1984 45
Summary
Based on our review of the literature,the following major conclusionsconcerning the chemotherapy ofschizoaffective disorders and affectivedisorders can be drawn:
• Lithium carbonate and neuro-leptics, alone or in combination,are effective treatments for maniaand schizoaffective mania andproduce improvement in mood aswell as psychotic symptoms.
• Schizoaffective manic patientsrequire a significantly longer timethan manics to respond to thesemedications. This may be anindication of a qualitative or aquantitative difference between thetwo types of disorders.
• Schizoaffective depressed patientsmay respond to either neurolepticsor antidepressants, or the combin-ation, but their course is much lesspredictable than that of patientswith major depressive disorder.
• Lithium 'carbonate is an effectiveprophylactic treatment of schizo-affective disorder, with results atleast as good as in bipolar affectiveillness. This result suggests thatthere is overlap in the etiology ofschizoaffective and affectivedisorders.
Despite the abundance of studieswe have reviewed, there is stillconsiderable need for further studieswhich include a large series ofsubjects diagnosed by RDC or othercriteria which provide for the differ-entiation of subtypes of schizo-affective disorder. Ideally, thesestudies should include manic, majordepression, and schizophrenicpatients as comparison groups anduse random assignment to treatmentif more than one treatment is to becompared. Carbamazepine or L-tryptophan, with or without lithium,which have been reported to have
some efficacy in the major affectivedisorders, could be useful agents toinclude in some such studies.Prophylactic studies with lithium,carbamazepine, L-tryptophan, 5-hydroxyrryptophan, or placebo witha large cohort of schizoaffectivedepressed and manic patients, studiedover a long period of time andcompared with pure bipolar patients,should identify patients who arenonresponders. The nonresponderswould represent a potential group ofsubjects for further study of thepossibility that some schizoaffectivepatients are more like schizophrenicsor are a unique psychosis.
References
Alexander, P.E.; Van Kammen,D.P.; and Bunney, W.E., Jr. Anti-psychotic effects of lithium in schizo-phrenia. American Journal ofPsychiatry, 136:283-287, 1979.American Psychiatric Association.DSM-II: Diagnostic and StatisticalManual of Mental Disorders. 2nd ed.Washington, DC: The Association,1968.
American Psychiatric Association.DSM-III: Diagnostic and StatisticalManual of Mental Disorders. 3rd ed.Washington, DC: The Association,1980.
Angst, J. A clinical analysis of theeffects of tofranil in depression.Psychopharmacologia, 2:381-407,1961.
Angst, J.; Weis, P.; Grof, P.;Baastrup, P.C.; and Schou, M.Lithium prophylaxis in recurrentaffective disorders. British Journal ofPsychiatry, 116:604-613, 1970.
Aronoff, M.S., and Epstein, R.S.Factors associated with poor responseto lithium carbonate: A clinicalstudy. American Journal ofPsychiatry, 127:472-480, 1970.
Avery, D., and Lubriano, A.
Depression treated with imipramineand ECT: The DeCarolis studyreconsidered. American Journal ofPsychiatry, 136:559-562, 1979.
Avery, D., and Winokur, G. Theefficacy of electroconvulsive therapyand antidepressants in depression.Biological Psychiatry, 12:507-523,1977.Beigel, A.B.; Murphy, D.L.; andBunney, W.E., Jr. The Manic StateRating Scale. Archives of GeneralPsychiatry, 25:256-262, 1971.
Biederman, ].; Lerner, Y.; andBelmaker, R.H. Combination oflithium carbonate and haloperidol inschizoaffective disorder. Archives ofGeneral Psychiatry, 36:327-333,1979.Braden, W.; Fink, E.B.; Quails,C.B.; Ho, C.K.; and Samuels, W.O.Lithium and chlorpromazine inpsychotic patients. PsychiatryResearch, 7:69-81, 1982.
Braden, W., and Quails, C.B. Racingthoughts in depressed patients.Journal of Clinical Psychiatry,40:336-339, 1979.
Brewerton, T.D., and Reus, V.I.Lithium carbonate and L-tryptophanin the treatment of bipolar andschizoaffective disorders. AmericanJournal of Psychiatry, 140:757-760,1983.
Brockington, I.F.; Kendell, R.E.;Kellett, J.M.; Curry, S.H.; andWainwright, S. Trials of lithium,chlorpromazine, and amitriptyline inschizoaffective patients. BritishJournal of Psychiatry, 133:162-168,1978.Brockington, I.F.; Kendell, R.E.; andWainwright, S. Depressed patientswith schizophrenic or paranoidsymptoms. Psychological Medicine,10:665-675, 1980.
Carman, J.S.; Bigelow, L.B.; andWyatt, R.J. Lithium combined withneuroleptics in chronic schizophrenic

46 SCHIZOPHRENIA BULLETIN
and schizoaffective patients. Journalof Clinical Psychiatry, 42:124-128,1981.
Cooper, B.A.; Hester, T.J.; andMaxwell, R.A. Behavioral andbiochemical effects of the antide-pressant bupropion (Wellbatrin):Evidence for selective blockade ofdopamine uptake in vivo. Journal ofPharmacology and ExperimentalTherapeutics, 215:127-134, 1980.
Corsini, G.U.; Pitzalis, G.F.;Bernardi, F.; Bocchetta, A.; and DelZompo, M. The use of dopamineagonists in the treatment of schizo-phrenia. Neuropharmacology,20:1309-1313, 1981.
Delva, N.J., and Letemendia, F.J.J.Lithium treatment in schizophreniaand schizoaffective disorders. BritishJournal of Psychiatry, 141:387-400,1982.
Detre, T.P., and Jarecki, H.B.Modern Psychiatric Treatment.Philadelphia: J.B. Lippincott Co.,1971.Dunner, D.L., and Fieve, R.R. Thelithium ion: Its impact on diagnosticpractice. In: Akiskal, H.S., andWebb, W.L., eds. PsychiatricDiagnosis: Exploration of BiologicalPredictors. New York: SP Medicaland Scientific Books, 1978. pp.233-246.
Endicott, J., and Spitzer, R.L. Adiagnostic interview: The Schedulefor Affective Disorders and Schizo-phrenia. Archives of GeneralPsychiatry, 35:837-844, 1978.
Fieve, R.R., and Goodnick, P.J.Lithium: Toward a resolution ofclinical and basic science issues.In: Cavenar, J.O., Jr., and Brodie,H.K.H., eds. Critical Issues inPsychiatry. Philadelphia: J.B.Lippincott Co., 1983. pp. 49-77.
Folstein, M.; Folstein, S.; andMcHugh, P.R. Clinical predictors ofimprovement after electroconvulsive
therapy of patients with schizo-phrenia, neurotic reactions andaffective disorders. BiologicalPsychiatry, 7:146-152. 1973.
Forssman, H., and Walinder, J.Lithium as an aid in psychiatricdiagnostics. Ada Psychiatrica Scan-dinavica, Suppl. 219:59-66, 1970.
Freedman, R., and Schwab, P.J.Paranoid symptoms in patients on ageneral hospital psychiatric unit.Archives of General Psychiatry,35:387-390, 1978.
Glassman, A.H.; Kantor, S.J.; andShostak, M. Depression, delusions,and drug response. American Journalof Psychiatry, 132:716-719, 1975.
Goode, D.J., and Manning, A.A.Comparison of bupropion alone andwith haloperidol in schizoaffectivedisorder, depressed type. Journal ofClinical Psychiatry, 44:253-255, 1983.
Goodnick, P.J., and Meltzer, H.Y."Lithium Treatment of Schizomaniaand Mania." Presented at the AnnualMeeting of the American PsychiatricAssociation, New York, May 1-6,1983.
Goodwin, F.K.; Murphy, D.L.; andBunney, W.E., Jr. Lithium carbonatetreatment in depression andmania: A longitudinal double-blindstudy. Archives of GeneralPsychiatry, 21:486-492, 1969.
Gottfries, C.S. Effect of lithium saltson various kinds of psychiatricdisorders. Ada Psychiatrica Scan-dinavica, Suppl. 203:157-167, 1968.
Greenblatt, M.; Grosser, G.H.; andWechsler, H. A comparative study ofselected antidepressant medicationsand ECT. American Journal ofPsychiatry, 119:144-153, 1962.
Hirschkowitz, J.; Casper, R.; Garver,D.L.; and Chang, S. Lithiumresponse in good prognosis schizo-phrenia. American Journal ofPsychiatry, 137:916-920, 1980.
Hofmann, G.; Kremser, M.;Katschnig, H.; and Scheiber, V.Prophylaktische Lithiutherapie beimanisch-depressivem Krankheits-geschenen und bei Legierungs-psychosen. International Pharma-copsychiatry, 4:187-193, 1970.
Hordern, A.; Holt, N.F.; Burt, C.G.;and Gordon, W.F. Amitriptyline indepressive states. British Journal ofPsychiatry, 109:815-825, 1963. •
Hullin, R.P.; McDonald, R.; andAIlsopp, M.N.E. Further report onprophylactic lithium in recurrentaffective disorders. British Journal ofPsychiatry, 126:281-284, 1975.
Johnson, G. Differential response tolithium carbonate in manicdepressive and schizoaffectivedisorders. Diseases of the NervousSystem, 31:613-615, 1970.
Johnson, G.; Gershon, S.; Burdock,E.I.; Floyd, A.; and Hekimian, L.Comparative effects of lithium andchlorpromazine in the treatment ofacute manic states. British Journal ofPsychiatry, 119:267-276, 1971.
Kingstone, E. The lithium treatmentof hypomanic and manic states.Comprehensive Psychiatry,11:317-320, 1960.
Klein, D.F.; Gittelman, R.; Quitkin,F.; and Rifkin, A. Diagnosis andDrug Treatment of PsychiatricDisorders. Baltimore and London:Williams & Wilkins Company, 1981.
Maxwell, R.A.; Mehta, N.B.;Tucker, W.E., Jr.; Schroeder, D.H.;and Stern, W.E. Bupropion. Pharma-cologic and Biochemical Properties ofDrug Substances, 3:1-55, 1981.
Megrabyan, A.A.; Khachaturyan,A.M.; Amadyan, M.G.; andBurnazyan, G.A. The treatment ofschizoaffective psychoses withlithium carbonate. Zhumal Eksperi-mental'nov i Klinicheskoy Meditsiny,19(4):54-58, 1979.

VOL. 10, NO. 1, 1984 47
Meltzer, H.Y. Dopamineautoreceptor stimulation: Clinicalsignificance. Pharmacology,Biochemistry, and Behavior,17(Suppl. l):l-10, 1982.
Meltzer, H.Y.; Busch, D.A.; Tricou,B.J.; and Robertson, A. Effect of(des-tyr)-gamma-endorphin in schizo-phrenia. Psychiatry Research,6:313-326, 1982.
Meltzer, H.Y.; Kolakowska, R.;Robertson, A.; and Tricou, B.J.Effect of low dose bromocriptine inthe treatment of psychosis: Thedopamine autoreceptor stimulationstrategy. Psychopharmacology,81:37-41, 1983.
Nelson, J.C., and Bowers, M.B., Jr.Delusional unipolar depression:Description and drug response.Archives of General Psychiatry,35:1321-1328, 1978.
Noack, C.H., and Trautner, E.M.The lithium treatment of mania andpsychosis. Medical Journal ofAustralia, 38:219-222, 1951.
Overall, J.E., and Gorham, D.R. TheBrief Psychiatric Rating Scale.Psychological Reports, 10:799-812,1962.
Perris, C. Morbidity suppressiveeffect of lithium carbonate in cycloidpsychosis. Archives of GeneralPsychiatry, 35:328-331, 1978.Pope, H.G., and Lipinski, J.F.Diagnosis in schizophrenia andmanic-depressive illness. Archives ofGeneral Psychiatry, 35:811-828,1978.
Pope, H.G.; Lipinski, J.F.; Cohen,B.M.; and Axelrod, D.T. "Schizo-affective disorder": An invaliddiagnosis? A comparison of schizo-affective disorder, schizophrenia, andaffective disorder. American Journalof Psychiatry, 137:921-927, 1980.
Prange, A.J., Jr.; Sisk, J.L.; Wilson,I.C.; Morris, C.E.; Hall, CD.; and
Carman, J.S. Balance, permission,and discrimination among amines: Atheoretical consideration of theactions of L-tryptophan in disordersof movements and affect.In: Barchas, J. and Usdin, E., eds.Serotonin and Behavior. NewYork: Academic Press, Inc., 1973.pp. 539-548.Prien, R.F.; Caffey, E.M.; and Klett,C.J. A comparison of lithiumcarbonate and chlorpromazine in thetreatment of excited schizoaffectives.Archives of General Psychiatry,27:182-189, 1972a.Prien, R.F.; Caffey, E.M.; and Klett,C.J. Comparison of lithiumcarbonate and chlorpromazine in thetreatment of mania. Archives ofGeneral Psychiatry, 26:146-153,1972b.
Prien, R.F.; Caffey, E.M.; and Klett,C.J. Prophylactic efficacy of lithiumcarbonate in manic-depressive illness.Archives of General Psychiatry,28:337-341, 1973.
Prien, R.F.; Caffey, E.M.; and Klett,C.J. Factors associated with treat-ment success in lithium carbonateprophylaxis. Archives of GeneralPsychiatry, 31:189-192, 1974.
Prusoff, B.A.; Williams, D.H.;Weissman, M.M.; and Astrachan,B.M. Treatment of secondarydepression in schizophrenia. Archivesof General Psychiatry, 36:569-575,1979.
Rice, D. The use of lithium salts inthe treatment of manic states.Journal of Mental Sciences,102:604-611, 1956.
Ries, R.K.: Wilson, L; Bokar, J.A.;and Chiles, J.A. ECT in medicationresistant schizoaffective disorders.Comprehensive Psychiatry,33:167-173, 1981.
Rosenthal, N.E.; Rosenthal, L.N.;Stallone, F.; Dunner, D.L.; andFieve, R.R. Toward the validation of
RDC schizoaffective disorder.Archives of General Psychiatry,37:804-810, 1980.Sarantidis, D., and Waters, B.Predictors of lithium prophylaxiseffectiveness. Progress in Neuro-psychopharmacology, 5:507-510,1981.
Schou, M. Lithium in the treatmentof other psychiatric and non-psychiatric disorders. Archives ofGeneral Psychiatry, 36:856-859,1979.
Shopsin, B.; Johnson, G.; andGershon, S. Neurotoxicity withlithium: Differential drugresponsiveness. InternationalPharmacopsychiatry, 5:170-182,1971.
Shopsin, B.; Kim, S.S.; and Gershon,S. A controlled study of lithium vs.chlorpromazine in acute schizo-phrenics. British Journal ofPsychiatry, 119:435-440, 1971.
Sicignano, J.R., and Lichtenstein, J.Rediagnosis of schizophrenia asbipolar affective illness. Hospital andCommunity Psychiatry, 29:112-114,1978.
Small, J.G.; Kellams, J.J.; Milstein,V.; and Moore, J. A placebo-controlled study of lithium combinedwith neuroleptics in chronic schizo-phrenic patients. American Journal ofPsychiatry, 132:1315-1317, 1975.
Smulevitch, A.B.; Zavidovskaya,G.I.; Igonin, A.L.; and Mikhailova,N.M. The effectiveness of lithium inaffective and schizoaffectivepsychoses. British Journal ofPsychiatry, 125:65-72, 1974.
Spitzer, R.L.; Endicott, J.; andRobins, E. Research DiagnosticCriteria for a Selected Group ofFunctional Disorders. NewYork: New York State PsychiatricInstitute, 1978.Tress, W., and Haag, H. Verglei-

48 SCHIZOPHRENIA BULLETIN
chende Erfahrungen mit der rezidiv-prophylaktischen lithium-langzeit-medikation bei schizoaffektivenPsychosen. Nervenarzt, 50:524-526,1979.
Van Kammen, D.P.; Alexander,P.E.; and Bunney, W.E., Jr. Lithiumtreatment in post-psychoticdepression. British Journal ofPsychiatry, 136:479-485, 1980.
Van Praag, H.M. Serotoninprecursors in the treatment ofdepression. In: Ho, B.T.; Schooler,J.C.; and Usdin, E., eds. Serotonin inBiological Psychiatry. NewYork: Raven Press, 1982. pp.259-286.Van Praag, H.M.; Verhoeven,W.M.A.; Van Ree, J.M.; and deWied, D. The treatment of schizo-phrenic psychoses with gamma-typeendorphins. Biological Psychiatry,17:83-98, 1982.
Verhoeven, W.M.A.; Westenberg,
H.G.M.; Gerritsen, T.W.; VanPraag, H.M.; Thijssen, J.H.H.;Schwarz, F.; Van Ree, J.M.; and deWied, D. (Des-tyrosine)-gamma-endorphin in schizophrenia: Clinical,biochemical, and hormonal aspects.Psychiatry Research, 5:293-309,1981.
Wagemaker, H., Jr.; Lippmann, S.;and Bryant, D.R. Lithium responseof a patient diagnosed as paranoidschizophrenic. Psychiatric Opinion,16:45-47, 1979.Wells, D.A. Electroconvulsivetreatment for schizophrenia: A ten-year survey in a university hospitalpsychiatric department. Compre-hensive Psychiatry, 14:291-298, 1973.
West, A.P. Lithium neurotoxicity inschizophrenic and schizoaffectivepatients. International Psycho-pharmacology, 17:91-103, 1982.
West, A.P., and Meltzer, H.Y.Paradoxical lithium neurotox-
icity: Five case reports and ahypothesis about risk for neuro-toxicity. American Journal ofPsychiatry, 136:963-966, 1979.
Wharton, R.W., and Fieve, R.R. Theuse of lithium in the affectivedisorders. American Journal ofPsychiatry, 123:706-712, 1966.
Zall, H.; Therman, P.G.; and Myers,J.M. Lithium carbonate: A clinicalstudy. American Journal ofPsychiatry, 125:549-555, 1968.
The Authors
Paul J. Goodnick, M.D., is AssistantProfessor of Psychiatry, and HerbertY. Meltzer, M.D., is Professor ofPsychiatry, Pritzker School ofMedicine, University of Chicago,Chicago, IL. Drs. Goodnick andMeltzer are also at the Illinois StatePsychiatric Institute.
Announcement The annual meeting of the AmericanPsychopathological Association willbe held March 1-3, 1984, at the St.Regis-Sheraton Hotel, New York,NY.
The theme of the meeting is"Controversies in Schizophrenia."
Articles from invited guests will bepresented in plenary sessions.
For further information, writeto: Nancy C. Andreasen, M.D.,Secretary, Department of Psychiatry,The University of Iowa, 500 NewtonRd., Iowa City, IA 52242.