3 questions to ask on SINCE1845 end-of-life care choices 3 … · 2019-11-07 · BINNY BANSAL and...
1
SINCE 1845 This is a personalised copy. Not for circulation. Source: The Straits Times © Singapore Press Holdings Limited. Permission required for reproduction. | TUESDAY, MARCH 6, 2018 | THE STRAITS TIMES | Sneeze or cough MIND & BODY B11 SPECIAL | SPH CONTENT LAB Ask e Experts What is bladeless laser cataract surgery? Brought to you by Dr David Goh Medical director and senior consultant ophthalmologist, Novena Bladeless Cataract Surgery Centre TREATMENT FOR PRESBYOPIA AND CATARACT ■ 100% bladeless cataract surgery ■ Computer-guided lens implantation Q My 62-year-old uncle has cataracts and has been advised to go for bladeless laser cataract surgery. Can you tell me more about this procedure? A As a person ages, a cataract can occur when the natural lens inside the eye becomes cloudy, causing symptoms such as blurred vision, glare or halos around bright lights, loss of colour or depth perception, and difficulty with vision in dim light. Cataracts cannot be treated by medication or wearing spectacles, so surgery is the best option. What is cataract surgery? Modern cataract surgery is a safe and effective 20-minute outpatient procedure that involves making a 2mm incision on the cornea, cutting the cataract into small pieces, re- moving the pieces and implanting a lens implant. The surgery is also an opportuni- ty for patients to correct or reduce pre-existing myopia (short-sighted- ness), astigmatism and presbyopia (“lao hua”). Traditional cataract surgery For the last 50 years, surgeons have been performing cataract surgery with a manual technique — using blades to make corneal incisions, and phacoemulsification (ultrasound) to cut up cataracts — which has limited precision and possible human error. Modern cataract surgery In bladeless laser cataract surgery, a femtosecond laser machine is used to complete many of the steps pre- viously performed manually by the surgeon, thus reducing the chance of human errors. This allows cataract surgery to become more precise and, ultimate- ly, improve on safety and visual out- comes. The femtosecond laser system uses a technology that is based on: ■ 3D Optical Coherence To- mography (OCT) imaging: Like a fingerprint, every eye has a unique size and shape. Before the treatment, the femtosecond laser system scans the patient’s eye and makes precise 3D maps of eye structures using real-time, high-definition OCT im- aging (below) to plan a customised treatment map of each eye. ■ Laser precision: Without man- ual cuts, the femtosecond laser (gas bubbles) creates a precise opening on the lens capsule for the removal of the cataract. ■ Gentler cataract surgery: The femtosecond laser then softens and divides the cataract into multi- ple pieces, blade-free. The surgeon can remove the cataract more gen- tly, which also enables faster post-op visual recovery for pa- tients. Computer–guided lens implantation After the removal of the cataract, the surgeon uses a computer-guided lens implantation sys- tem (left) that enables him to see alignment images during the actu- al insertion of the lens implant. This helps the implant at- tain near-perfect overlap and accu- rate centration. Overall advantages The advantages of using femtosec- ond laser and computer-guided lens implantation systems include: ■ Improved safety and precision, ■ Can be performed using topical anaesthetic eye-drops, ■ No sharp blades involved, ■ No stitches required, ■ More precise alignment of artifi- cial lens implant, and ■ Quicker return of vision after sur- gery.
Transcript of 3 questions to ask on SINCE1845 end-of-life care choices 3 … · 2019-11-07 · BINNY BANSAL and...

SINCE 1845
78PAGES INFIVEPARTS$1.10Tosubscribe: 6388-3838sphsubscription.com.sg
ASingaporePressHoldingspublication
MCI (P)041/02/2016��
Ravi Velloor
Seven people operating at the fron-tiers of technology’s interface withbusiness, collectively called “TheDisruptors”, are this year’s StraitsTimes Asians of the Year.
Mr Nadiem Makarim of Go-Jek,Mr Anthony Tan and Ms Tan HooiLing of Grab, Mr Tan Min-Liang ofRazer, Mr Pony Ma of Tencent and
Mr Sachin Bansal and Mr BinnyBansal of Flipkart were chosen froma crowded field by the editors of TheStraits Times for the annual award.
Breaking from tradition, editorsof the 171-year-old newspaper thisyear chose to name a cluster of indi-viduals, recognising that credit forthe changes sweeping the conti-nent are too widespread to bepinned to a single individual’sbreast. Accordingly, the names in-
clude business leaders from Asia’sbig-population nations – China, In-dia and Indonesia – as well as fromMalaysia and Singapore.
The award citation noted thateach, in his or her own way, had“made the inevitable march of tech-nology easier to understand and ac-cept by millions of people con-cerned about their old ways of lifeyielding to an unfamiliar new one”.
Selection committee chairman
Warren Fernandez, who is the edi-tor-in-chief of the English, Malayand Tamil Media Group of SingaporePress Holdings as well as ST editor,noted that 2016 hadbeen an especial-ly surprising year politically. “Thesesurprises are driven by underlyingforces of major technological andeconomic change brought about bythe disruption that is sweepingacross just about every sector of oureconomies and societies. Exactly
how people, governments and busi-nesses respond to these changeswill have major political and elector-al implications in the years ahead.”
The Asian of the Year award rec-ognises a person or people whohave contributed significantly toimproving lives at home or in thewider region. The inaugural Asianof the Year, in 2012, was then Myan-mar President Thein Sein. The fol-lowing year, the award was shared
by Prime Minister Shinzo Abe ofJapan and President Xi Jinping ofChina. In 2014, the award went toIndia’s Prime Minister NarendraModi and, last year, it was awardedposthumously to Mr Lee KuanYew, Singapore’s founding father.
SEE TOP OF THE NEWS A4,EDITORIAL A19
Charissa Yong
The growing mood of anxiety anddiscontent and the ground gainedby extreme political parties inmany developed countries will im-pact not just the world economy,but global security and stability,Prime Minister Lee Hsien Loongsaid yesterday.
There will be major consequenc-es for small, open countries such
as Singapore that have relied onopen trade and making friends,and sought opportunities to coop-erate, he said.
It will also be harder to prosper to-gether in this new climate, wherecountries are turning inward and be-coming more protectionist, seeingothers’ gains as their loss, he added.
Mr Lee gave this reading of recenttrends in a speech to 2,500 People’sAction Party (PAP) members attheir biennial party conference.
He called on members to under-stand what the trend means for Sin-gapore and to help ensure the PAPremains a party with strong sup-port from all segments of society.
“The external world is changing...in a very fundamental way not ad-vantageous to us. We have to watchthis, we have to know how this is go-ing to impact us over the next fewyears,” he said.
Mr Lee, who is PAP secretary-gen-eral, noted that voters around theworld are unhappy that the benefitsof growth are not reaching them,and feel threatened that immigrantsare competing for their jobs.
He cited the recent United States
election, the Brexit vote and therise of extreme parties in Europe asexamples of voters’ weariness oftrade and wariness of immigrants.
“This looks like the trend now. Ido not know how far it will go, but Ido not like the direction the trend isgoing,” he said. “If more countriesturn this way, the world is going tochange, and change for the worse.”
Singapore prospered in the past50 years by working hard, but itwas fortunate to have a favourableexternal environment: A peacefulAsia and an international orderwhere countries big and small coop-erate and compete under rules thatare fair to all, giving small countries
“a right to their place in the sun”.Today, countries are flexing
their muscles and becoming in-creasingly assertive.
“Nobody can tell how relations be-tween the big powers will develop,”said Mr Lee. “If US-China relationsgrow tense, Singapore is going to bein a very difficult spot, because weregard both the US and China as ourfriends and do not want to have tochoose between them.”
Meanwhile, obstacles to trade areincreasing and Singapore’s exports– a key pillar of its economy – arenot growing by very much either.
But Singapore has to accept theworld as it is, not as it wishes it tobe, said Mr Lee.
“We ourselves must remain open,because if we close up like othercountries, our people will be fin-ished,” he said.
Besides understanding the globalclimate, Mr Lee spelt out two otherways for the ruling party to preparefor the next general election, whichmust be held by April 2021.
First, the party must strive to im-prove the lives of Singaporeans.
He cited two ways of doing so: By
equipping Singaporeans with theskills to take care of themselvesthrough schools and training pro-grammes, and by strengthening so-cial safety nets.
Second, the PAP must remain astrong, national party that reachesout to all segments of society andrepresents them. It must also stayfocused on serving the people, andprovide strong leadership, he said.
“Politics is the same everywhere.It is people, it is trust, it is knowingyou care for me,” he added.
“Unless we have this deep in ourDNA, we will not be able to hold ourposition in Singapore.”
SEE TOP OF THE NEWS A8
PM: Rising global discontentwill affect stability, securityIt will be harder to prosper together, andS’pore must keep watch over impact of trend
THE DISRUPTORSS T R A I T S T I M E S A S I A N S O F T H E Y E A R
PONY MA, founder, CEOand executive director
of Tencent HoldingsNADIEM MAKARIM, founder and CEO of Go-Jek
BINNY BANSAL and SACHIN BANSAL, co-founders of Flipkart
ANTHONY TAN and TAN HOOI LING, co-founders of Grab
TAN MIN-LIANG, co-founder and CEO of Razer Inc
EXCELLENCE IN REDESIGN: SOCIETY OF NEWS DESIGN BEST IN NEWSPAPER DESIGN, BEST NEWS WEBSITE: WAN-IFRA
World Tempest over Trump’s Taiwan phone call A10 • Education Is PSLE a necessary checkpoint? B10&11
HomeDelivered food? Prepare to pay more B1
Serving up friendship with meals
Connecting home cooks to customers
ST CAUSES WEEK Top of the News A6 SportRunner dies during marathon raceC12
dies during marathon
This is a personalised copy. Not for circulation.Source: The Straits Times © Singapore Press Holdings Limited. Permission required for reproduction.
While many prefer to spend their last days in the comfort of their own homes, this is not always possible.
Some ailing elderly may need round-the-clock care and a hospice or nursing home would be a better option. For those who prefer their own homes, special caregiving ar-rangements need to be made.
Either way, family members should first start a dialogue with the elderly person to manage his expec-tations, said Ms Sherlyn Lee, a regis-tered nurse and nursing manager at Active Global Caregivers.
“The outlook towards end-of-life care and the choices made in ad-vance-care planning vary widely be-tween patients and caregivers.”
According to official estimates, more than 10,000 Singaporeans are expected to require end-of-life care by 2020.
In deciding end-of-life options for a loved one, Ms Lee said three is-sues should be addressed:
1. WHERE DO THEY WISH TO SPEND THEIR FINAL DAYS?If the answer is “at home”, the fam-ily can consider engaging a home hospice service where doctors, nurses and social workers visit the patient’s home to manage his medi-cal condition, said Ms Lee.
“The frequency of home visits range from monthly to fortnightly, depending on the patient’s needs.”
Home hospice care is provided by registered charities and is free to all patients, regardless of age, religion, ethnicity, nationality and financial status.
Alternatively, the patient can be enrolled in a hospice daycare cen-tre. This is suitable if the patient does not need 24-hour nursing assis-tance, said Ms Lee. Such hospices in-clude HCA Hospice Care and Assisi Hospice. They are usually open from 8am to 5.30pm on weekdays.
There is a nominal fee of $15 per day for two-way transport of the pa-tient. The fee also covers meals and therapy activities. Subsidies are available based on means-testing.
Another option is to hire a live-in caregiver. This is ideal for highly de-pendent patients who do not want to stay in an institution, said Ms Lee.
The live-in caregiver could be an overseas-trained nurse or nursing aide, and the monthly cost of hiring one is between $700 and $1,000.
But if the patient does not mind staying in an institution, the family can opt for a nursing home, in-pa-tient hospice or hospital.
A nursing home will be able to pro-vide skilled care and assist the pa-tient with daily activities such as taking a shower. “Some nursing homes are also equipped to care for the elderly with special needs, in-cluding dementia and psychiatric conditions,” said Ms Lee.
A hospice may offer similar care but is typically catered to patients with less than three months to live. The staff will help the patient cope with the advanced stages of his ill-ness and provide comfort.
A hospital can provide palliative care for serious conditions such as advanced cancer, for example, to help patients manage pain.
2. WHAT ARE THE MEDICAL CHOICES TO WEIGH? When the disease is in its final throes, the medical team will usu-ally discuss with the patient and his family whether to pursue aggres-sive treatment or focus on provid-ing comfort, said Ms Lee.
Pain management is another con-sideration. While painkillers pro-vide relief, they may make the pa-tient groggy. Hence, some may wish to reduce the dosage “to keep a clear head and enable them to carry on meaningful social engagement with their loved ones”, she added.
For tube-fed patients, they may wish to decide to do away with the tube and eat normally, even though it means they may not get sufficient nutrition.
And finally, there is the choice to place a “do not resuscitate” order.
“Some patients opt not to be resus-citated in the event that they col-lapse,” said Ms Lee. “It is important to have a discussion in advance to avoid highly stressed and emotional situations during critical moments.”
3. WHAT ARE THE SOCIAL AND SPIRITUAL CHOICES THAT CAN BOOST THE QUALITY OF ONE’S END-OF-LIFE CARE?Some of these factors include pre-paring a will in advance, asking the patient who he wants to be sur-rounded by during his last days, and making arrangements for spiritual and psychological support where necessary, suggested Ms Lee.
“Coping with impending death can be emotionally draining and dra-matic for the patient and his family members, but having a good plan for social and spiritual support can help people be at peace,” she said.
Poon Chian Hui
Daniel Victor
When you feel a sneeze or a cough coming on, covering your mouth prevents the spread of infectious germs. You probably knew that.
But the way you cover up also matters, and there are plenty of people who have not yet heard the consensus guidance of health offi-cials: If no tissue is available, you should aim into your elbow, not your hand. Even if that means breaking a long-held habit.
“If somebody sneezes into their hands, that creates an opportu-nity for those germs to be passed on to other people, or contami-nate other objects that people touch,” said Dr Vincent Hill, chief of the waterborne disease preven-tion branch of the Centres for Dis-ease Control and Prevention (CDC) in the United States.
Germs are most commonly spread by the respiratory droplets emitted from sneezing and cough-ing. When they land on your hands, they are transmitted to things like doorknobs, elevator buttons and other surfaces people around you are likely to also touch.
Sneezing and coughing into your arm has become the standard sug-gestion of not just the CDC, but also organisations like the American Academy of Paediatrics and the American Public Health Associa-tion.
Even the New York City subway system occasionally runs an an-nouncement asking riders to “cough or sneeze into the bend of your arm or use a tissue”.
The suggestion is relatively new. The CDC guidance has become of-ficial only in the last 10 to 15 years,
Dr Hill said.Dr Georges Benjamin, executive
director of the American Public Health Association, said he began seeing the suggestion more promi-nently about 10 years ago.
Children are frequently taught in school the proper way to cough or sneeze – sometimes referred to as the Dracula cough, since it makes you look like the count cov-ering up with his cape.
University of Missouri-Kansas City School of Medicine professor of paediatrics Mary Anne Jackson said the term “cough etiquette” first turned up in 2000, and she traced the suggestion to sneeze into your arm to 2003, when Sars fears were widespread.
It gained further prominence in 2009, when the H1N1 swine flu pandemic struck the US.
That year, Ms Kathleen Sebe-lius, then the Health and Human Services Secretary, shamed NBC journalist Chuck Todd for his sneezing etiquette at a White House press briefing. (Rush Lim-baugh, the conservative radio host, later dismissed her advice as coming from “elitist snobs”.)
To be clear, the manoeuvre does not eliminate all risk, even if it is the best tactic available.
Studies have shown that even masks cannot prevent all droplets from becoming airborne, Prof Jack-son said.
But anything to reduce the amount of flying particles helps. And health officials keep coming back to a drum that can never be beaten enough: Make sure you consistently wash your hands.
“Hand washing is one of the most important things people can do to keep healthy,” Dr Hill said. NYTIMES
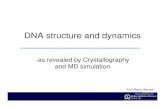
If the patient does not mind staying in an institution, the family can opt for a nursing home. A nursing home will be able to provide skilled care and assist the patient with daily activities. Some are also equipped to care for the elderly with special needs, such as dementia. ST PHOTO: KUA CHEE SIONG
CONTACT USEditorial inquiries: 6319-5397 Ad sales: Aileen Chua 6319-2292, [email protected]; Joseph Lee 6319-2078, [email protected]; Wendy Wong 6319-2232, [email protected]
Tips on picking a caregiving plan and preparing for the inevitable
Sneeze or cough into your elbow, not your hand
AskTheExperts
What is bladeless lasercataract surgery?Brought to you by
SPECIAL | SPH CONTENT LAB
Q My 62-year-old uncle hascataracts and has been advisedto go for bladeless laser cataractsurgery. Can you tell me moreabout this procedure?
A As a person ages, a cataractcan occur when the naturallens inside the eye becomescloudy, causing symptoms suchas blurred vision, glare or halosaround bright lights, loss of col-our or depth perception, anddifficulty with vision in dim light.
Cataracts cannot be treated bymedication or wearing specta-cles, so surgery is the best option.
What is cataract surgery?Modern cataract surgery is asafe and effective 20-minuteoutpatient procedure that in-volves making a 2mm incisionon the cornea, cutting the cata-ract into small pieces, removingthe pieces and implanting a lensimplant.
The surgery is also an oppor-tunity for patients to corrector reduce pre-existing myopia(short-sightedness), astigmatismand presbyopia (“lao hua”).
Traditional cataract surgeryFor the last 50 years, surgeonshave been performing cataractsurgery with a manual tech-nique — using blades to makecorneal incisions, and phaco-emulsification (ultrasound) tocut up cataracts — which haslimited precision and possiblehuman error.
Modern cataract surgeryIn bladeless laser cataract sur-gery, a femtosecond laser ma-chine is used to complete manyof the steps previously per-formed manually by the sur-
geon, thus reducing the chanceof human errors.
This allows cataract surgeryto become more precise and,ultimately, improve on safetyand visual outcomes.
The femtosecond laser sys-tem uses a technology that isbased on:
■ 3D Optical Coherence To-mography (OCT) imaging: Likea fingerprint, every eye has aunique size and shape. Beforethe treatment, the femtosecondlaser system scans the patient’seye and makes precise 3D mapsof eye structures using real-time,high-definition OCT imaging(below) to plan a customisedtreatment map of each eye.
■ Laserprecision: Without man-ual cuts, the femtosecond laser(gas bubbles) creates a preciseopening on the lens capsule forthe removal of the cataract.
■ Gentler cataract surgery: Thefemtosecond laser then softensand divides the cataract intomultiple pieces, blade-free.The surgeon can remove thecataract more gently, which alsoenables faster post-op visualrecovery for patients.
Medical director andsenior consultant ophthalmologist,Novena Bladeless CataractSurgery Centre
Dr David Goh
Computer–guided lensimplantationAfter the remov-al of the cataract,the surgeon uses acomputer-guidedlens implantationsystem (left) thatenables him to seealignment imagesduring the actualinsertion of the
lens implant. This helps the im-plant attain near-perfect over-lap and accurate centration.
Overall advantagesThe advantages of using fem-tosecond laser and computer-guided lens implantation sys-tems include:■ Improved safety and precision,■ Can be performed using
topical anaesthetic eye-drops,■ No sharp blades involved,■ No stitches required,■ More precise alignment of
artificial lens implant, and■ Quicker return of vision
after surgery.
TREATMENT FORPRESBYOPIAAND CATARACT■ 100% bladeless cataract surgery■ Computer-guided lens
implantation
EYE SEMINARMarch 14 (6.30pm to 7.30pm) orMarch 17 (12.30pm to 1.30pm)
Venue: Seminar Room #19-03,Royal Square Medical Suites,101 Irrawaddy Road, Singapore.
Admission is free.Call 6560-2220 to register.
PLAN AHEAD
Some patients opt not to be resuscitated in the event that they collapse. It is important to have a discussion in advance to avoid highly stressed and emotional situations during critical moments.
’’MS SHERLYN LEE, nursing manager at Active Global Caregivers.
HelpAtYourFingertips
3 questions to ask on end-of-life care choices
| TUESDAY, MARCH 6, 2018 | THE STRAITS TIMES | MIND&BODY B11
While many prefer to spend their last days in the comfort of their own homes, this is not always possible.
Some ailing elderly may need round-the-clock care and a hospice or nursing home would be a better option. For those who prefer their own homes, special caregiving ar-rangements need to be made.
Either way, family members should first start a dialogue with the elderly person to manage his expec-tations, said Ms Sherlyn Lee, a regis-tered nurse and nursing manager at Active Global Caregivers.
“The outlook towards end-of-life care and the choices made in ad-vance-care planning vary widely be-tween patients and caregivers.”
According to official estimates, more than 10,000 Singaporeans are expected to require end-of-life care by 2020.
In deciding end-of-life options for a loved one, Ms Lee said three is-sues should be addressed:
1. WHERE DO THEY WISH TO SPEND THEIR FINAL DAYS?If the answer is “at home”, the fam-ily can consider engaging a home hospice service where doctors, nurses and social workers visit the patient’s home to manage his medi-cal condition, said Ms Lee.
“The frequency of home visits range from monthly to fortnightly, depending on the patient’s needs.”
Home hospice care is provided by registered charities and is free to all patients, regardless of age, religion, ethnicity, nationality and financial status.
Alternatively, the patient can be enrolled in a hospice daycare cen-tre. This is suitable if the patient does not need 24-hour nursing assis-tance, said Ms Lee. Such hospices in-clude HCA Hospice Care and Assisi Hospice. They are usually open from 8am to 5.30pm on weekdays.
There is a nominal fee of $15 per day for two-way transport of the pa-tient. The fee also covers meals and therapy activities. Subsidies are available based on means-testing.
Another option is to hire a live-in caregiver. This is ideal for highly de-pendent patients who do not want to stay in an institution, said Ms Lee.
The live-in caregiver could be an overseas-trained nurse or nursing aide, and the monthly cost of hiring one is between $700 and $1,000.
But if the patient does not mind staying in an institution, the family can opt for a nursing home, in-pa-tient hospice or hospital.
A nursing home will be able to pro-vide skilled care and assist the pa-tient with daily activities such as taking a shower. “Some nursing homes are also equipped to care for the elderly with special needs, in-cluding dementia and psychiatric conditions,” said Ms Lee.
A hospice may offer similar care but is typically catered to patients with less than three months to live. The staff will help the patient cope with the advanced stages of his ill-ness and provide comfort.
A hospital can provide palliative care for serious conditions such as advanced cancer, for example, to help patients manage pain.
2. WHAT ARE THE MEDICAL CHOICES TO WEIGH? When the disease is in its final throes, the medical team will usu-ally discuss with the patient and his family whether to pursue aggres-sive treatment or focus on provid-ing comfort, said Ms Lee.
Pain management is another con-sideration. While painkillers pro-vide relief, they may make the pa-tient groggy. Hence, some may wish to reduce the dosage “to keep a clear head and enable them to carry on meaningful social engagement with their loved ones”, she added.
For tube-fed patients, they may wish to decide to do away with the tube and eat normally, even though it means they may not get sufficient nutrition.
And finally, there is the choice to place a “do not resuscitate” order.
“Some patients opt not to be resus-citated in the event that they col-lapse,” said Ms Lee. “It is important to have a discussion in advance to avoid highly stressed and emotional situations during critical moments.”
3. WHAT ARE THE SOCIAL AND SPIRITUAL CHOICES THAT CAN BOOST THE QUALITY OF ONE’S END-OF-LIFE CARE?Some of these factors include pre-paring a will in advance, asking the patient who he wants to be sur-rounded by during his last days, and making arrangements for spiritual and psychological support where necessary, suggested Ms Lee.
“Coping with impending death can be emotionally draining and dra-matic for the patient and his family members, but having a good plan for social and spiritual support can help people be at peace,” she said.
Poon Chian Hui
Daniel Victor
When you feel a sneeze or a cough coming on, covering your mouth prevents the spread of infectious germs. You probably knew that.
But the way you cover up also matters, and there are plenty of people who have not yet heard the consensus guidance of health offi-cials: If no tissue is available, you should aim into your elbow, not your hand. Even if that means breaking a long-held habit.
“If somebody sneezes into their hands, that creates an opportu-nity for those germs to be passed on to other people, or contami-nate other objects that people touch,” said Dr Vincent Hill, chief of the waterborne disease preven-tion branch of the Centres for Dis-ease Control and Prevention (CDC) in the United States.
Germs are most commonly spread by the respiratory droplets emitted from sneezing and cough-ing. When they land on your hands, they are transmitted to things like doorknobs, elevator buttons and other surfaces people around you are likely to also touch.
Sneezing and coughing into your arm has become the standard sug-gestion of not just the CDC, but also organisations like the American Academy of Paediatrics and the American Public Health Associa-tion.
Even the New York City subway system occasionally runs an an-nouncement asking riders to “cough or sneeze into the bend of your arm or use a tissue”.
The suggestion is relatively new. The CDC guidance has become of-ficial only in the last 10 to 15 years,
Dr Hill said.Dr Georges Benjamin, executive
director of the American Public Health Association, said he began seeing the suggestion more promi-nently about 10 years ago.
Children are frequently taught in school the proper way to cough or sneeze – sometimes referred to as the Dracula cough, since it makes you look like the count cov-ering up with his cape.
University of Missouri-Kansas City School of Medicine professor of paediatrics Mary Anne Jackson said the term “cough etiquette” first turned up in 2000, and she traced the suggestion to sneeze into your arm to 2003, when Sars fears were widespread.
It gained further prominence in 2009, when the H1N1 swine flu pandemic struck the US.
That year, Ms Kathleen Sebe-lius, then the Health and Human Services Secretary, shamed NBC journalist Chuck Todd for his sneezing etiquette at a White House press briefing. (Rush Lim-baugh, the conservative radio host, later dismissed her advice as coming from “elitist snobs”.)
To be clear, the manoeuvre does not eliminate all risk, even if it is the best tactic available.
Studies have shown that even masks cannot prevent all droplets from becoming airborne, Prof Jack-son said.
But anything to reduce the amount of flying particles helps. And health officials keep coming back to a drum that can never be beaten enough: Make sure you consistently wash your hands.
“Hand washing is one of the most important things people can do to keep healthy,” Dr Hill said. NYTIMES
If the patient does not mind staying in an institution, the family can opt for a nursing home. A nursing home will be able to provide skilled care and assist the patient with daily activities. Some are also equipped to care for the elderly with special needs, such as dementia. ST PHOTO: KUA CHEE SIONG
CONTACT USEditorial inquiries: 6319-5397 Ad sales: Aileen Chua 6319-2292, [email protected]; Joseph Lee 6319-2078, [email protected]; Wendy Wong 6319-2232, [email protected]
Tips on picking a caregiving plan and preparing for the inevitable
Sneeze or cough into your elbow, not your hand
AskTheExperts
What is bladeless lasercataract surgery?Brought to you by
SPECIAL | SPH CONTENT LAB
Q My 62-year-old uncle hascataracts and has been advisedto go for bladeless laser cataractsurgery. Can you tell me moreabout this procedure?
A As a person ages, a cataractcan occur when the naturallens inside the eye becomescloudy, causing symptoms suchas blurred vision, glare or halosaround bright lights, loss of col-our or depth perception, anddifficulty with vision in dim light.
Cataracts cannot be treated bymedication or wearing specta-cles, so surgery is the best option.
What is cataract surgery?Modern cataract surgery is asafe and effective 20-minuteoutpatient procedure that in-volves making a 2mm incisionon the cornea, cutting the cata-ract into small pieces, removingthe pieces and implanting a lensimplant.
The surgery is also an oppor-tunity for patients to corrector reduce pre-existing myopia(short-sightedness), astigmatismand presbyopia (“lao hua”).
Traditional cataract surgeryFor the last 50 years, surgeonshave been performing cataractsurgery with a manual tech-nique — using blades to makecorneal incisions, and phaco-emulsification (ultrasound) tocut up cataracts — which haslimited precision and possiblehuman error.
Modern cataract surgeryIn bladeless laser cataract sur-gery, a femtosecond laser ma-chine is used to complete manyof the steps previously per-formed manually by the sur-
geon, thus reducing the chanceof human errors.
This allows cataract surgeryto become more precise and,ultimately, improve on safetyand visual outcomes.
The femtosecond laser sys-tem uses a technology that isbased on:
■ 3D Optical Coherence To-mography (OCT) imaging: Likea fingerprint, every eye has aunique size and shape. Beforethe treatment, the femtosecondlaser system scans the patient’seye and makes precise 3D mapsof eye structures using real-time,high-definition OCT imaging(below) to plan a customisedtreatment map of each eye.
■ Laserprecision: Without man-ual cuts, the femtosecond laser(gas bubbles) creates a preciseopening on the lens capsule forthe removal of the cataract.
■ Gentler cataract surgery: Thefemtosecond laser then softensand divides the cataract intomultiple pieces, blade-free.The surgeon can remove thecataract more gently, which alsoenables faster post-op visualrecovery for patients.
Medical director andsenior consultant ophthalmologist,Novena Bladeless CataractSurgery Centre
Dr David Goh
Computer–guided lensimplantationAfter the remov-al of the cataract,the surgeon uses acomputer-guidedlens implantationsystem (left) thatenables him to seealignment imagesduring the actualinsertion of the
lens implant. This helps the im-plant attain near-perfect over-lap and accurate centration.
Overall advantagesThe advantages of using fem-tosecond laser and computer-guided lens implantation sys-tems include:■ Improved safety and precision,■ Can be performed using
topical anaesthetic eye-drops,■ No sharp blades involved,■ No stitches required,■ More precise alignment of
artificial lens implant, and■ Quicker return of vision
after surgery.
TREATMENT FORPRESBYOPIAAND CATARACT■ 100% bladeless cataract surgery■ Computer-guided lens
implantation
EYE SEMINARMarch 14 (6.30pm to 7.30pm) orMarch 17 (12.30pm to 1.30pm)
Venue: Seminar Room #19-03,Royal Square Medical Suites,101 Irrawaddy Road, Singapore.
Admission is free.Call 6560-2220 to register.
PLAN AHEAD
Some patients opt not to be resuscitated in the event that they collapse. It is important to have a discussion in advance to avoid highly stressed and emotional situations during critical moments.
’’MS SHERLYN LEE, nursing manager at Active Global Caregivers.
HelpAtYourFingertips
3 questions to ask on end-of-life care choices
| TUESDAY, MARCH 6, 2018 | THE STRAITS TIMES | MIND&BODY B11
While many prefer to spend their last days in the comfort of their own homes, this is not always possible.
Some ailing elderly may need round-the-clock care and a hospice or nursing home would be a better option. For those who prefer their own homes, special caregiving ar-rangements need to be made.
Either way, family members should first start a dialogue with the elderly person to manage his expec-tations, said Ms Sherlyn Lee, a regis-tered nurse and nursing manager at Active Global Caregivers.
“The outlook towards end-of-life care and the choices made in ad-vance-care planning vary widely be-tween patients and caregivers.”
According to official estimates, more than 10,000 Singaporeans are expected to require end-of-life care by 2020.
In deciding end-of-life options for a loved one, Ms Lee said three is-sues should be addressed:
1. WHERE DO THEY WISH TO SPEND THEIR FINAL DAYS?If the answer is “at home”, the fam-ily can consider engaging a home hospice service where doctors, nurses and social workers visit the patient’s home to manage his medi-cal condition, said Ms Lee.
“The frequency of home visits range from monthly to fortnightly, depending on the patient’s needs.”
Home hospice care is provided by registered charities and is free to all patients, regardless of age, religion, ethnicity, nationality and financial status.
Alternatively, the patient can be enrolled in a hospice daycare cen-tre. This is suitable if the patient does not need 24-hour nursing assis-tance, said Ms Lee. Such hospices in-clude HCA Hospice Care and Assisi Hospice. They are usually open from 8am to 5.30pm on weekdays.
There is a nominal fee of $15 per day for two-way transport of the pa-tient. The fee also covers meals and therapy activities. Subsidies are available based on means-testing.
Another option is to hire a live-in caregiver. This is ideal for highly de-pendent patients who do not want to stay in an institution, said Ms Lee.
The live-in caregiver could be an overseas-trained nurse or nursing aide, and the monthly cost of hiring one is between $700 and $1,000.
But if the patient does not mind staying in an institution, the family can opt for a nursing home, in-pa-tient hospice or hospital.
A nursing home will be able to pro-vide skilled care and assist the pa-tient with daily activities such as taking a shower. “Some nursing homes are also equipped to care for the elderly with special needs, in-cluding dementia and psychiatric conditions,” said Ms Lee.
A hospice may offer similar care but is typically catered to patients with less than three months to live. The staff will help the patient cope with the advanced stages of his ill-ness and provide comfort.
A hospital can provide palliative care for serious conditions such as advanced cancer, for example, to help patients manage pain.
2. WHAT ARE THE MEDICAL CHOICES TO WEIGH? When the disease is in its final throes, the medical team will usu-ally discuss with the patient and his family whether to pursue aggres-sive treatment or focus on provid-ing comfort, said Ms Lee.
Pain management is another con-sideration. While painkillers pro-vide relief, they may make the pa-tient groggy. Hence, some may wish to reduce the dosage “to keep a clear head and enable them to carry on meaningful social engagement with their loved ones”, she added.
For tube-fed patients, they may wish to decide to do away with the tube and eat normally, even though it means they may not get sufficient nutrition.
And finally, there is the choice to place a “do not resuscitate” order.
“Some patients opt not to be resus-citated in the event that they col-lapse,” said Ms Lee. “It is important to have a discussion in advance to avoid highly stressed and emotional situations during critical moments.”
3. WHAT ARE THE SOCIAL AND SPIRITUAL CHOICES THAT CAN BOOST THE QUALITY OF ONE’S END-OF-LIFE CARE?Some of these factors include pre-paring a will in advance, asking the patient who he wants to be sur-rounded by during his last days, and making arrangements for spiritual and psychological support where necessary, suggested Ms Lee.
“Coping with impending death can be emotionally draining and dra-matic for the patient and his family members, but having a good plan for social and spiritual support can help people be at peace,” she said.
Poon Chian Hui
Daniel Victor
When you feel a sneeze or a cough coming on, covering your mouth prevents the spread of infectious germs. You probably knew that.
But the way you cover up also matters, and there are plenty of people who have not yet heard the consensus guidance of health offi-cials: If no tissue is available, you should aim into your elbow, not your hand. Even if that means breaking a long-held habit.
“If somebody sneezes into their hands, that creates an opportu-nity for those germs to be passed on to other people, or contami-nate other objects that people touch,” said Dr Vincent Hill, chief of the waterborne disease preven-tion branch of the Centres for Dis-ease Control and Prevention (CDC) in the United States.
Germs are most commonly spread by the respiratory droplets emitted from sneezing and cough-ing. When they land on your hands, they are transmitted to things like doorknobs, elevator buttons and other surfaces people around you are likely to also touch.
Sneezing and coughing into your arm has become the standard sug-gestion of not just the CDC, but also organisations like the American Academy of Paediatrics and the American Public Health Associa-tion.
Even the New York City subway system occasionally runs an an-nouncement asking riders to “cough or sneeze into the bend of your arm or use a tissue”.
The suggestion is relatively new. The CDC guidance has become of-ficial only in the last 10 to 15 years,
Dr Hill said.Dr Georges Benjamin, executive
director of the American Public Health Association, said he began seeing the suggestion more promi-nently about 10 years ago.
Children are frequently taught in school the proper way to cough or sneeze – sometimes referred to as the Dracula cough, since it makes you look like the count cov-ering up with his cape.
University of Missouri-Kansas City School of Medicine professor of paediatrics Mary Anne Jackson said the term “cough etiquette” first turned up in 2000, and she traced the suggestion to sneeze into your arm to 2003, when Sars fears were widespread.
It gained further prominence in 2009, when the H1N1 swine flu pandemic struck the US.
That year, Ms Kathleen Sebe-lius, then the Health and Human Services Secretary, shamed NBC journalist Chuck Todd for his sneezing etiquette at a White House press briefing. (Rush Lim-baugh, the conservative radio host, later dismissed her advice as coming from “elitist snobs”.)
To be clear, the manoeuvre does not eliminate all risk, even if it is the best tactic available.
Studies have shown that even masks cannot prevent all droplets from becoming airborne, Prof Jack-son said.
But anything to reduce the amount of flying particles helps. And health officials keep coming back to a drum that can never be beaten enough: Make sure you consistently wash your hands.
“Hand washing is one of the most important things people can do to keep healthy,” Dr Hill said. NYTIMES
If the patient does not mind staying in an institution, the family can opt for a nursing home. A nursing home will be able to provide skilled care and assist the patient with daily activities. Some are also equipped to care for the elderly with special needs, such as dementia. ST PHOTO: KUA CHEE SIONG
CONTACT USEditorial inquiries: 6319-5397 Ad sales: Aileen Chua 6319-2292, [email protected]; Joseph Lee 6319-2078, [email protected]; Wendy Wong 6319-2232, [email protected]
Tips on picking a caregiving plan and preparing for the inevitable
Sneeze or cough into your elbow, not your hand
AskTheExperts
What is bladeless lasercataract surgery?Brought to you by
SPECIAL | SPH CONTENT LAB
Q My 62-year-old uncle hascataracts and has been advisedto go for bladeless laser cataractsurgery. Can you tell me moreabout this procedure?
A As a person ages, a cataractcan occur when the naturallens inside the eye becomescloudy, causing symptoms suchas blurred vision, glare or halosaround bright lights, loss of col-our or depth perception, anddifficulty with vision in dim light.
Cataracts cannot be treated bymedication or wearing specta-cles, so surgery is the best option.
What is cataract surgery?Modern cataract surgery is asafe and effective 20-minuteoutpatient procedure that in-volves making a 2mm incisionon the cornea, cutting the cata-ract into small pieces, removingthe pieces and implanting a lensimplant.
The surgery is also an oppor-tunity for patients to corrector reduce pre-existing myopia(short-sightedness), astigmatismand presbyopia (“lao hua”).
Traditional cataract surgeryFor the last 50 years, surgeonshave been performing cataractsurgery with a manual tech-nique — using blades to makecorneal incisions, and phaco-emulsification (ultrasound) tocut up cataracts — which haslimited precision and possiblehuman error.
Modern cataract surgeryIn bladeless laser cataract sur-gery, a femtosecond laser ma-chine is used to complete manyof the steps previously per-formed manually by the sur-
geon, thus reducing the chanceof human errors.
This allows cataract surgeryto become more precise and,ultimately, improve on safetyand visual outcomes.
The femtosecond laser sys-tem uses a technology that isbased on:
■ 3D Optical Coherence To-mography (OCT) imaging: Likea fingerprint, every eye has aunique size and shape. Beforethe treatment, the femtosecondlaser system scans the patient’seye and makes precise 3D mapsof eye structures using real-time,high-definition OCT imaging(below) to plan a customisedtreatment map of each eye.
■ Laserprecision: Without man-ual cuts, the femtosecond laser(gas bubbles) creates a preciseopening on the lens capsule forthe removal of the cataract.
■ Gentler cataract surgery: Thefemtosecond laser then softensand divides the cataract intomultiple pieces, blade-free.The surgeon can remove thecataract more gently, which alsoenables faster post-op visualrecovery for patients.
Medical director andsenior consultant ophthalmologist,Novena Bladeless CataractSurgery Centre
Dr David Goh
Computer–guided lensimplantationAfter the remov-al of the cataract,the surgeon uses acomputer-guidedlens implantationsystem (left) thatenables him to seealignment imagesduring the actualinsertion of the
lens implant. This helps the im-plant attain near-perfect over-lap and accurate centration.
Overall advantagesThe advantages of using fem-tosecond laser and computer-guided lens implantation sys-tems include:■ Improved safety and precision,■ Can be performed using
topical anaesthetic eye-drops,■ No sharp blades involved,■ No stitches required,■ More precise alignment of
artificial lens implant, and■ Quicker return of vision
after surgery.
TREATMENT FORPRESBYOPIAAND CATARACT■ 100% bladeless cataract surgery■ Computer-guided lens
implantation
EYE SEMINARMarch 14 (6.30pm to 7.30pm) orMarch 17 (12.30pm to 1.30pm)
Venue: Seminar Room #19-03,Royal Square Medical Suites,101 Irrawaddy Road, Singapore.
Admission is free.Call 6560-2220 to register.
PLAN AHEAD
Some patients opt not to be resuscitated in the event that they collapse. It is important to have a discussion in advance to avoid highly stressed and emotional situations during critical moments.
’’MS SHERLYN LEE, nursing manager at Active Global Caregivers.
HelpAtYourFingertips
3 questions to ask on end-of-life care choices
| TUESDAY, MARCH 6, 2018 | THE STRAITS TIMES | MIND&BODY B11
Ask The Experts
What is bladeless laser cataract surgery?
While many prefer to spend their last days in the comfort of their own homes, this is not always possible.
Some ailing elderly may need round-the-clock care and a hospice or nursing home would be a better option. For those who prefer their own homes, special caregiving ar-rangements need to be made.
Either way, family members should first start a dialogue with the elderly person to manage his expec-tations, said Ms Sherlyn Lee, a regis-tered nurse and nursing manager at Active Global Caregivers.
“The outlook towards end-of-life care and the choices made in ad-vance-care planning vary widely be-tween patients and caregivers.”
According to official estimates, more than 10,000 Singaporeans are expected to require end-of-life care by 2020.
In deciding end-of-life options for a loved one, Ms Lee said three is-sues should be addressed:
1. WHERE DO THEY WISH TO SPEND THEIR FINAL DAYS?If the answer is “at home”, the fam-ily can consider engaging a home hospice service where doctors, nurses and social workers visit the patient’s home to manage his medi-cal condition, said Ms Lee.
“The frequency of home visits range from monthly to fortnightly, depending on the patient’s needs.”
Home hospice care is provided by registered charities and is free to all patients, regardless of age, religion, ethnicity, nationality and financial status.
Alternatively, the patient can be enrolled in a hospice daycare cen-tre. This is suitable if the patient does not need 24-hour nursing assis-tance, said Ms Lee. Such hospices in-clude HCA Hospice Care and Assisi Hospice. They are usually open from 8am to 5.30pm on weekdays.
There is a nominal fee of $15 per day for two-way transport of the pa-tient. The fee also covers meals and therapy activities. Subsidies are available based on means-testing.
Another option is to hire a live-in caregiver. This is ideal for highly de-pendent patients who do not want to stay in an institution, said Ms Lee.
The live-in caregiver could be an overseas-trained nurse or nursing aide, and the monthly cost of hiring one is between $700 and $1,000.
But if the patient does not mind staying in an institution, the family can opt for a nursing home, in-pa-tient hospice or hospital.
A nursing home will be able to pro-vide skilled care and assist the pa-tient with daily activities such as taking a shower. “Some nursing homes are also equipped to care for the elderly with special needs, in-cluding dementia and psychiatric conditions,” said Ms Lee.
A hospice may offer similar care but is typically catered to patients with less than three months to live. The staff will help the patient cope with the advanced stages of his ill-ness and provide comfort.
A hospital can provide palliative care for serious conditions such as advanced cancer, for example, to help patients manage pain.
2. WHAT ARE THE MEDICAL CHOICES TO WEIGH? When the disease is in its final throes, the medical team will usu-ally discuss with the patient and his family whether to pursue aggres-sive treatment or focus on provid-ing comfort, said Ms Lee.
Pain management is another con-sideration. While painkillers pro-vide relief, they may make the pa-tient groggy. Hence, some may wish to reduce the dosage “to keep a clear head and enable them to carry on meaningful social engagement with their loved ones”, she added.
For tube-fed patients, they may wish to decide to do away with the tube and eat normally, even though it means they may not get sufficient nutrition.
And finally, there is the choice to place a “do not resuscitate” order.
“Some patients opt not to be resus-citated in the event that they col-lapse,” said Ms Lee. “It is important to have a discussion in advance to avoid highly stressed and emotional situations during critical moments.”
3. WHAT ARE THE SOCIAL AND SPIRITUAL CHOICES THAT CAN BOOST THE QUALITY OF ONE’S END-OF-LIFE CARE?Some of these factors include pre-paring a will in advance, asking the patient who he wants to be sur-rounded by during his last days, and making arrangements for spiritual and psychological support where necessary, suggested Ms Lee.
“Coping with impending death can be emotionally draining and dra-matic for the patient and his family members, but having a good plan for social and spiritual support can help people be at peace,” she said.
Poon Chian Hui
Daniel Victor
When you feel a sneeze or a cough coming on, covering your mouth prevents the spread of infectious germs. You probably knew that.
But the way you cover up also matters, and there are plenty of people who have not yet heard the consensus guidance of health offi-cials: If no tissue is available, you should aim into your elbow, not your hand. Even if that means breaking a long-held habit.
“If somebody sneezes into their hands, that creates an opportu-nity for those germs to be passed on to other people, or contami-nate other objects that people touch,” said Dr Vincent Hill, chief of the waterborne disease preven-tion branch of the Centres for Dis-ease Control and Prevention (CDC) in the United States.
Germs are most commonly spread by the respiratory droplets emitted from sneezing and cough-ing. When they land on your hands, they are transmitted to things like doorknobs, elevator buttons and other surfaces people around you are likely to also touch.
Sneezing and coughing into your arm has become the standard sug-gestion of not just the CDC, but also organisations like the American Academy of Paediatrics and the American Public Health Associa-tion.
Even the New York City subway system occasionally runs an an-nouncement asking riders to “cough or sneeze into the bend of your arm or use a tissue”.
The suggestion is relatively new. The CDC guidance has become of-ficial only in the last 10 to 15 years,
Dr Hill said.Dr Georges Benjamin, executive
director of the American Public Health Association, said he began seeing the suggestion more promi-nently about 10 years ago.
Children are frequently taught in school the proper way to cough or sneeze – sometimes referred to as the Dracula cough, since it makes you look like the count cov-ering up with his cape.
University of Missouri-Kansas City School of Medicine professor of paediatrics Mary Anne Jackson said the term “cough etiquette” first turned up in 2000, and she traced the suggestion to sneeze into your arm to 2003, when Sars fears were widespread.
It gained further prominence in 2009, when the H1N1 swine flu pandemic struck the US.
That year, Ms Kathleen Sebe-lius, then the Health and Human Services Secretary, shamed NBC journalist Chuck Todd for his sneezing etiquette at a White House press briefing. (Rush Lim-baugh, the conservative radio host, later dismissed her advice as coming from “elitist snobs”.)
To be clear, the manoeuvre does not eliminate all risk, even if it is the best tactic available.
Studies have shown that even masks cannot prevent all droplets from becoming airborne, Prof Jack-son said.
But anything to reduce the amount of flying particles helps. And health officials keep coming back to a drum that can never be beaten enough: Make sure you consistently wash your hands.
“Hand washing is one of the most important things people can do to keep healthy,” Dr Hill said. NYTIMES
If the patient does not mind staying in an institution, the family can opt for a nursing home. A nursing home will be able to provide skilled care and assist the patient with daily activities. Some are also equipped to care for the elderly with special needs, such as dementia. ST PHOTO: KUA CHEE SIONG
CONTACT USEditorial inquiries: 6319-5397 Ad sales: Aileen Chua 6319-2292, [email protected]; Joseph Lee 6319-2078, [email protected]; Wendy Wong 6319-2232, [email protected]
Tips on picking a caregiving plan and preparing for the inevitable
Sneeze or cough into your elbow, not your hand
AskTheExperts
What is bladeless lasercataract surgery?Brought to you by
SPECIAL | SPH CONTENT LAB
Q My 62-year-old uncle hascataracts and has been advisedto go for bladeless laser cataractsurgery. Can you tell me moreabout this procedure?
A As a person ages, a cataractcan occur when the naturallens inside the eye becomescloudy, causing symptoms suchas blurred vision, glare or halosaround bright lights, loss of col-our or depth perception, anddifficulty with vision in dim light.
Cataracts cannot be treated bymedication or wearing specta-cles, so surgery is the best option.
What is cataract surgery?Modern cataract surgery is asafe and effective 20-minuteoutpatient procedure that in-volves making a 2mm incisionon the cornea, cutting the cata-ract into small pieces, removingthe pieces and implanting a lensimplant.
The surgery is also an oppor-tunity for patients to corrector reduce pre-existing myopia(short-sightedness), astigmatismand presbyopia (“lao hua”).
Traditional cataract surgeryFor the last 50 years, surgeonshave been performing cataractsurgery with a manual tech-nique — using blades to makecorneal incisions, and phaco-emulsification (ultrasound) tocut up cataracts — which haslimited precision and possiblehuman error.
Modern cataract surgeryIn bladeless laser cataract sur-gery, a femtosecond laser ma-chine is used to complete manyof the steps previously per-formed manually by the sur-
geon, thus reducing the chanceof human errors.
This allows cataract surgeryto become more precise and,ultimately, improve on safetyand visual outcomes.
The femtosecond laser sys-tem uses a technology that isbased on:
■ 3D Optical Coherence To-mography (OCT) imaging: Likea fingerprint, every eye has aunique size and shape. Beforethe treatment, the femtosecondlaser system scans the patient’seye and makes precise 3D mapsof eye structures using real-time,high-definition OCT imaging(below) to plan a customisedtreatment map of each eye.
■ Laserprecision: Without man-ual cuts, the femtosecond laser(gas bubbles) creates a preciseopening on the lens capsule forthe removal of the cataract.
■ Gentler cataract surgery: Thefemtosecond laser then softensand divides the cataract intomultiple pieces, blade-free.The surgeon can remove thecataract more gently, which alsoenables faster post-op visualrecovery for patients.
Medical director andsenior consultant ophthalmologist,Novena Bladeless CataractSurgery Centre
Dr David Goh
Computer–guided lensimplantationAfter the remov-al of the cataract,the surgeon uses acomputer-guidedlens implantationsystem (left) thatenables him to seealignment imagesduring the actualinsertion of the
lens implant. This helps the im-plant attain near-perfect over-lap and accurate centration.
Overall advantagesThe advantages of using fem-tosecond laser and computer-guided lens implantation sys-tems include:■ Improved safety and precision,■ Can be performed using
topical anaesthetic eye-drops,■ No sharp blades involved,■ No stitches required,■ More precise alignment of
artificial lens implant, and■ Quicker return of vision
after surgery.
TREATMENT FORPRESBYOPIAAND CATARACT■ 100% bladeless cataract surgery■ Computer-guided lens
implantation
EYE SEMINARMarch 14 (6.30pm to 7.30pm) orMarch 17 (12.30pm to 1.30pm)
Venue: Seminar Room #19-03,Royal Square Medical Suites,101 Irrawaddy Road, Singapore.
Admission is free.Call 6560-2220 to register.
PLAN AHEAD
Some patients opt not to be resuscitated in the event that they collapse. It is important to have a discussion in advance to avoid highly stressed and emotional situations during critical moments.
’’MS SHERLYN LEE, nursing manager at Active Global Caregivers.
HelpAtYourFingertips
3 questions to ask on end-of-life care choices
| TUESDAY, MARCH 6, 2018 | THE STRAITS TIMES | MIND&BODY B11
Brought to you by
While many prefer to spend their last days in the comfort of their own homes, this is not always possible.
Some ailing elderly may need round-the-clock care and a hospice or nursing home would be a better option. For those who prefer their own homes, special caregiving ar-rangements need to be made.
Either way, family members should first start a dialogue with the elderly person to manage his expec-tations, said Ms Sherlyn Lee, a regis-tered nurse and nursing manager at Active Global Caregivers.
“The outlook towards end-of-life care and the choices made in ad-vance-care planning vary widely be-tween patients and caregivers.”
According to official estimates, more than 10,000 Singaporeans are expected to require end-of-life care by 2020.
In deciding end-of-life options for a loved one, Ms Lee said three is-sues should be addressed:
1. WHERE DO THEY WISH TO SPEND THEIR FINAL DAYS?If the answer is “at home”, the fam-ily can consider engaging a home hospice service where doctors, nurses and social workers visit the patient’s home to manage his medi-cal condition, said Ms Lee.
“The frequency of home visits range from monthly to fortnightly, depending on the patient’s needs.”
Home hospice care is provided by registered charities and is free to all patients, regardless of age, religion, ethnicity, nationality and financial status.
Alternatively, the patient can be enrolled in a hospice daycare cen-tre. This is suitable if the patient does not need 24-hour nursing assis-tance, said Ms Lee. Such hospices in-clude HCA Hospice Care and Assisi Hospice. They are usually open from 8am to 5.30pm on weekdays.
There is a nominal fee of $15 per day for two-way transport of the pa-tient. The fee also covers meals and therapy activities. Subsidies are available based on means-testing.
Another option is to hire a live-in caregiver. This is ideal for highly de-pendent patients who do not want to stay in an institution, said Ms Lee.
The live-in caregiver could be an overseas-trained nurse or nursing aide, and the monthly cost of hiring one is between $700 and $1,000.
But if the patient does not mind staying in an institution, the family can opt for a nursing home, in-pa-tient hospice or hospital.
A nursing home will be able to pro-vide skilled care and assist the pa-tient with daily activities such as taking a shower. “Some nursing homes are also equipped to care for the elderly with special needs, in-cluding dementia and psychiatric conditions,” said Ms Lee.
A hospice may offer similar care but is typically catered to patients with less than three months to live. The staff will help the patient cope with the advanced stages of his ill-ness and provide comfort.
A hospital can provide palliative care for serious conditions such as advanced cancer, for example, to help patients manage pain.
2. WHAT ARE THE MEDICAL CHOICES TO WEIGH? When the disease is in its final throes, the medical team will usu-ally discuss with the patient and his family whether to pursue aggres-sive treatment or focus on provid-ing comfort, said Ms Lee.
Pain management is another con-sideration. While painkillers pro-vide relief, they may make the pa-tient groggy. Hence, some may wish to reduce the dosage “to keep a clear head and enable them to carry on meaningful social engagement with their loved ones”, she added.
For tube-fed patients, they may wish to decide to do away with the tube and eat normally, even though it means they may not get sufficient nutrition.
And finally, there is the choice to place a “do not resuscitate” order.
“Some patients opt not to be resus-citated in the event that they col-lapse,” said Ms Lee. “It is important to have a discussion in advance to avoid highly stressed and emotional situations during critical moments.”
3. WHAT ARE THE SOCIAL AND SPIRITUAL CHOICES THAT CAN BOOST THE QUALITY OF ONE’S END-OF-LIFE CARE?Some of these factors include pre-paring a will in advance, asking the patient who he wants to be sur-rounded by during his last days, and making arrangements for spiritual and psychological support where necessary, suggested Ms Lee.
“Coping with impending death can be emotionally draining and dra-matic for the patient and his family members, but having a good plan for social and spiritual support can help people be at peace,” she said.
Poon Chian Hui
Daniel Victor
When you feel a sneeze or a cough coming on, covering your mouth prevents the spread of infectious germs. You probably knew that.
But the way you cover up also matters, and there are plenty of people who have not yet heard the consensus guidance of health offi-cials: If no tissue is available, you should aim into your elbow, not your hand. Even if that means breaking a long-held habit.
“If somebody sneezes into their hands, that creates an opportu-nity for those germs to be passed on to other people, or contami-nate other objects that people touch,” said Dr Vincent Hill, chief of the waterborne disease preven-tion branch of the Centres for Dis-ease Control and Prevention (CDC) in the United States.
Germs are most commonly spread by the respiratory droplets emitted from sneezing and cough-ing. When they land on your hands, they are transmitted to things like doorknobs, elevator buttons and other surfaces people around you are likely to also touch.
Sneezing and coughing into your arm has become the standard sug-gestion of not just the CDC, but also organisations like the American Academy of Paediatrics and the American Public Health Associa-tion.
Even the New York City subway system occasionally runs an an-nouncement asking riders to “cough or sneeze into the bend of your arm or use a tissue”.
The suggestion is relatively new. The CDC guidance has become of-ficial only in the last 10 to 15 years,
Dr Hill said.Dr Georges Benjamin, executive
director of the American Public Health Association, said he began seeing the suggestion more promi-nently about 10 years ago.
Children are frequently taught in school the proper way to cough or sneeze – sometimes referred to as the Dracula cough, since it makes you look like the count cov-ering up with his cape.
University of Missouri-Kansas City School of Medicine professor of paediatrics Mary Anne Jackson said the term “cough etiquette” first turned up in 2000, and she traced the suggestion to sneeze into your arm to 2003, when Sars fears were widespread.
It gained further prominence in 2009, when the H1N1 swine flu pandemic struck the US.
That year, Ms Kathleen Sebe-lius, then the Health and Human Services Secretary, shamed NBC journalist Chuck Todd for his sneezing etiquette at a White House press briefing. (Rush Lim-baugh, the conservative radio host, later dismissed her advice as coming from “elitist snobs”.)
To be clear, the manoeuvre does not eliminate all risk, even if it is the best tactic available.
Studies have shown that even masks cannot prevent all droplets from becoming airborne, Prof Jack-son said.
But anything to reduce the amount of flying particles helps. And health officials keep coming back to a drum that can never be beaten enough: Make sure you consistently wash your hands.
“Hand washing is one of the most important things people can do to keep healthy,” Dr Hill said. NYTIMES
If the patient does not mind staying in an institution, the family can opt for a nursing home. A nursing home will be able to provide skilled care and assist the patient with daily activities. Some are also equipped to care for the elderly with special needs, such as dementia. ST PHOTO: KUA CHEE SIONG
CONTACT USEditorial inquiries: 6319-5397 Ad sales: Aileen Chua 6319-2292, [email protected]; Joseph Lee 6319-2078, [email protected]; Wendy Wong 6319-2232, [email protected]
Tips on picking a caregiving plan and preparing for the inevitable
Sneeze or cough into your elbow, not your hand
AskTheExperts
What is bladeless lasercataract surgery?Brought to you by
SPECIAL | SPH CONTENT LAB
Q My 62-year-old uncle hascataracts and has been advisedto go for bladeless laser cataractsurgery. Can you tell me moreabout this procedure?
A As a person ages, a cataractcan occur when the naturallens inside the eye becomescloudy, causing symptoms suchas blurred vision, glare or halosaround bright lights, loss of col-our or depth perception, anddifficulty with vision in dim light.
Cataracts cannot be treated bymedication or wearing specta-cles, so surgery is the best option.
What is cataract surgery?Modern cataract surgery is asafe and effective 20-minuteoutpatient procedure that in-volves making a 2mm incisionon the cornea, cutting the cata-ract into small pieces, removingthe pieces and implanting a lensimplant.
The surgery is also an oppor-tunity for patients to corrector reduce pre-existing myopia(short-sightedness), astigmatismand presbyopia (“lao hua”).
Traditional cataract surgeryFor the last 50 years, surgeonshave been performing cataractsurgery with a manual tech-nique — using blades to makecorneal incisions, and phaco-emulsification (ultrasound) tocut up cataracts — which haslimited precision and possiblehuman error.
Modern cataract surgeryIn bladeless laser cataract sur-gery, a femtosecond laser ma-chine is used to complete manyof the steps previously per-formed manually by the sur-
geon, thus reducing the chanceof human errors.
This allows cataract surgeryto become more precise and,ultimately, improve on safetyand visual outcomes.
The femtosecond laser sys-tem uses a technology that isbased on:
■ 3D Optical Coherence To-mography (OCT) imaging: Likea fingerprint, every eye has aunique size and shape. Beforethe treatment, the femtosecondlaser system scans the patient’seye and makes precise 3D mapsof eye structures using real-time,high-definition OCT imaging(below) to plan a customisedtreatment map of each eye.
■ Laserprecision: Without man-ual cuts, the femtosecond laser(gas bubbles) creates a preciseopening on the lens capsule forthe removal of the cataract.
■ Gentler cataract surgery: Thefemtosecond laser then softensand divides the cataract intomultiple pieces, blade-free.The surgeon can remove thecataract more gently, which alsoenables faster post-op visualrecovery for patients.
Medical director andsenior consultant ophthalmologist,Novena Bladeless CataractSurgery Centre
Dr David Goh
Computer–guided lensimplantationAfter the remov-al of the cataract,the surgeon uses acomputer-guidedlens implantationsystem (left) thatenables him to seealignment imagesduring the actualinsertion of the
lens implant. This helps the im-plant attain near-perfect over-lap and accurate centration.
Overall advantagesThe advantages of using fem-tosecond laser and computer-guided lens implantation sys-tems include:■ Improved safety and precision,■ Can be performed using
topical anaesthetic eye-drops,■ No sharp blades involved,■ No stitches required,■ More precise alignment of
artificial lens implant, and■ Quicker return of vision
after surgery.
TREATMENT FORPRESBYOPIAAND CATARACT■ 100% bladeless cataract surgery■ Computer-guided lens
implantation
EYE SEMINARMarch 14 (6.30pm to 7.30pm) orMarch 17 (12.30pm to 1.30pm)
Venue: Seminar Room #19-03,Royal Square Medical Suites,101 Irrawaddy Road, Singapore.
Admission is free.Call 6560-2220 to register.
PLAN AHEAD
Some patients opt not to be resuscitated in the event that they collapse. It is important to have a discussion in advance to avoid highly stressed and emotional situations during critical moments.
’’MS SHERLYN LEE, nursing manager at Active Global Caregivers.
HelpAtYourFingertips
3 questions to ask on end-of-life care choices
| TUESDAY, MARCH 6, 2018 | THE STRAITS TIMES | MIND&BODY B11
While many prefer to spend their last days in the comfort of their own homes, this is not always possible.
Some ailing elderly may need round-the-clock care and a hospice or nursing home would be a better option. For those who prefer their own homes, special caregiving ar-rangements need to be made.
Either way, family members should first start a dialogue with the elderly person to manage his expec-tations, said Ms Sherlyn Lee, a regis-tered nurse and nursing manager at Active Global Caregivers.
“The outlook towards end-of-life care and the choices made in ad-vance-care planning vary widely be-tween patients and caregivers.”
According to official estimates, more than 10,000 Singaporeans are expected to require end-of-life care by 2020.
In deciding end-of-life options for a loved one, Ms Lee said three is-sues should be addressed:
1. WHERE DO THEY WISH TO SPEND THEIR FINAL DAYS?If the answer is “at home”, the fam-ily can consider engaging a home hospice service where doctors, nurses and social workers visit the patient’s home to manage his medi-cal condition, said Ms Lee.
“The frequency of home visits range from monthly to fortnightly, depending on the patient’s needs.”
Home hospice care is provided by registered charities and is free to all patients, regardless of age, religion, ethnicity, nationality and financial status.
Alternatively, the patient can be enrolled in a hospice daycare cen-tre. This is suitable if the patient does not need 24-hour nursing assis-tance, said Ms Lee. Such hospices in-clude HCA Hospice Care and Assisi Hospice. They are usually open from 8am to 5.30pm on weekdays.
There is a nominal fee of $15 per day for two-way transport of the pa-tient. The fee also covers meals and therapy activities. Subsidies are available based on means-testing.
Another option is to hire a live-in caregiver. This is ideal for highly de-pendent patients who do not want to stay in an institution, said Ms Lee.
The live-in caregiver could be an overseas-trained nurse or nursing aide, and the monthly cost of hiring one is between $700 and $1,000.
But if the patient does not mind staying in an institution, the family can opt for a nursing home, in-pa-tient hospice or hospital.
A nursing home will be able to pro-vide skilled care and assist the pa-tient with daily activities such as taking a shower. “Some nursing homes are also equipped to care for the elderly with special needs, in-cluding dementia and psychiatric conditions,” said Ms Lee.
A hospice may offer similar care but is typically catered to patients with less than three months to live. The staff will help the patient cope with the advanced stages of his ill-ness and provide comfort.
A hospital can provide palliative care for serious conditions such as advanced cancer, for example, to help patients manage pain.
2. WHAT ARE THE MEDICAL CHOICES TO WEIGH? When the disease is in its final throes, the medical team will usu-ally discuss with the patient and his family whether to pursue aggres-sive treatment or focus on provid-ing comfort, said Ms Lee.
Pain management is another con-sideration. While painkillers pro-vide relief, they may make the pa-tient groggy. Hence, some may wish to reduce the dosage “to keep a clear head and enable them to carry on meaningful social engagement with their loved ones”, she added.
For tube-fed patients, they may wish to decide to do away with the tube and eat normally, even though it means they may not get sufficient nutrition.
And finally, there is the choice to place a “do not resuscitate” order.
“Some patients opt not to be resus-citated in the event that they col-lapse,” said Ms Lee. “It is important to have a discussion in advance to avoid highly stressed and emotional situations during critical moments.”
3. WHAT ARE THE SOCIAL AND SPIRITUAL CHOICES THAT CAN BOOST THE QUALITY OF ONE’S END-OF-LIFE CARE?Some of these factors include pre-paring a will in advance, asking the patient who he wants to be sur-rounded by during his last days, and making arrangements for spiritual and psychological support where necessary, suggested Ms Lee.
“Coping with impending death can be emotionally draining and dra-matic for the patient and his family members, but having a good plan for social and spiritual support can help people be at peace,” she said.
Poon Chian Hui
Daniel Victor
When you feel a sneeze or a cough coming on, covering your mouth prevents the spread of infectious germs. You probably knew that.
But the way you cover up also matters, and there are plenty of people who have not yet heard the consensus guidance of health offi-cials: If no tissue is available, you should aim into your elbow, not your hand. Even if that means breaking a long-held habit.
“If somebody sneezes into their hands, that creates an opportu-nity for those germs to be passed on to other people, or contami-nate other objects that people touch,” said Dr Vincent Hill, chief of the waterborne disease preven-tion branch of the Centres for Dis-ease Control and Prevention (CDC) in the United States.
Germs are most commonly spread by the respiratory droplets emitted from sneezing and cough-ing. When they land on your hands, they are transmitted to things like doorknobs, elevator buttons and other surfaces people around you are likely to also touch.
Sneezing and coughing into your arm has become the standard sug-gestion of not just the CDC, but also organisations like the American Academy of Paediatrics and the American Public Health Associa-tion.
Even the New York City subway system occasionally runs an an-nouncement asking riders to “cough or sneeze into the bend of your arm or use a tissue”.
The suggestion is relatively new. The CDC guidance has become of-ficial only in the last 10 to 15 years,
Dr Hill said.Dr Georges Benjamin, executive
director of the American Public Health Association, said he began seeing the suggestion more promi-nently about 10 years ago.
Children are frequently taught in school the proper way to cough or sneeze – sometimes referred to as the Dracula cough, since it makes you look like the count cov-ering up with his cape.
University of Missouri-Kansas City School of Medicine professor of paediatrics Mary Anne Jackson said the term “cough etiquette” first turned up in 2000, and she traced the suggestion to sneeze into your arm to 2003, when Sars fears were widespread.
It gained further prominence in 2009, when the H1N1 swine flu pandemic struck the US.
That year, Ms Kathleen Sebe-lius, then the Health and Human Services Secretary, shamed NBC journalist Chuck Todd for his sneezing etiquette at a White House press briefing. (Rush Lim-baugh, the conservative radio host, later dismissed her advice as coming from “elitist snobs”.)
To be clear, the manoeuvre does not eliminate all risk, even if it is the best tactic available.
Studies have shown that even masks cannot prevent all droplets from becoming airborne, Prof Jack-son said.
But anything to reduce the amount of flying particles helps. And health officials keep coming back to a drum that can never be beaten enough: Make sure you consistently wash your hands.
“Hand washing is one of the most important things people can do to keep healthy,” Dr Hill said. NYTIMES
If the patient does not mind staying in an institution, the family can opt for a nursing home. A nursing home will be able to provide skilled care and assist the patient with daily activities. Some are also equipped to care for the elderly with special needs, such as dementia. ST PHOTO: KUA CHEE SIONG
CONTACT USEditorial inquiries: 6319-5397 Ad sales: Aileen Chua 6319-2292, [email protected]; Joseph Lee 6319-2078, [email protected]; Wendy Wong 6319-2232, [email protected]
Tips on picking a caregiving plan and preparing for the inevitable
Sneeze or cough into your elbow, not your hand
AskTheExperts
What is bladeless lasercataract surgery?Brought to you by
SPECIAL | SPH CONTENT LAB
Q My 62-year-old uncle hascataracts and has been advisedto go for bladeless laser cataractsurgery. Can you tell me moreabout this procedure?
A As a person ages, a cataractcan occur when the naturallens inside the eye becomescloudy, causing symptoms suchas blurred vision, glare or halosaround bright lights, loss of col-our or depth perception, anddifficulty with vision in dim light.
Cataracts cannot be treated bymedication or wearing specta-cles, so surgery is the best option.
What is cataract surgery?Modern cataract surgery is asafe and effective 20-minuteoutpatient procedure that in-volves making a 2mm incisionon the cornea, cutting the cata-ract into small pieces, removingthe pieces and implanting a lensimplant.
The surgery is also an oppor-tunity for patients to corrector reduce pre-existing myopia(short-sightedness), astigmatismand presbyopia (“lao hua”).
Traditional cataract surgeryFor the last 50 years, surgeonshave been performing cataractsurgery with a manual tech-nique — using blades to makecorneal incisions, and phaco-emulsification (ultrasound) tocut up cataracts — which haslimited precision and possiblehuman error.
Modern cataract surgeryIn bladeless laser cataract sur-gery, a femtosecond laser ma-chine is used to complete manyof the steps previously per-formed manually by the sur-
geon, thus reducing the chanceof human errors.
This allows cataract surgeryto become more precise and,ultimately, improve on safetyand visual outcomes.
The femtosecond laser sys-tem uses a technology that isbased on:
■ 3D Optical Coherence To-mography (OCT) imaging: Likea fingerprint, every eye has aunique size and shape. Beforethe treatment, the femtosecondlaser system scans the patient’seye and makes precise 3D mapsof eye structures using real-time,high-definition OCT imaging(below) to plan a customisedtreatment map of each eye.
■ Laserprecision: Without man-ual cuts, the femtosecond laser(gas bubbles) creates a preciseopening on the lens capsule forthe removal of the cataract.
■ Gentler cataract surgery: Thefemtosecond laser then softensand divides the cataract intomultiple pieces, blade-free.The surgeon can remove thecataract more gently, which alsoenables faster post-op visualrecovery for patients.
Medical director andsenior consultant ophthalmologist,Novena Bladeless CataractSurgery Centre
Dr David Goh
Computer–guided lensimplantationAfter the remov-al of the cataract,the surgeon uses acomputer-guidedlens implantationsystem (left) thatenables him to seealignment imagesduring the actualinsertion of the
lens implant. This helps the im-plant attain near-perfect over-lap and accurate centration.
Overall advantagesThe advantages of using fem-tosecond laser and computer-guided lens implantation sys-tems include:■ Improved safety and precision,■ Can be performed using
topical anaesthetic eye-drops,■ No sharp blades involved,■ No stitches required,■ More precise alignment of
artificial lens implant, and■ Quicker return of vision
after surgery.
TREATMENT FORPRESBYOPIAAND CATARACT■ 100% bladeless cataract surgery■ Computer-guided lens
implantation
EYE SEMINARMarch 14 (6.30pm to 7.30pm) orMarch 17 (12.30pm to 1.30pm)
Venue: Seminar Room #19-03,Royal Square Medical Suites,101 Irrawaddy Road, Singapore.
Admission is free.Call 6560-2220 to register.
PLAN AHEAD
Some patients opt not to be resuscitated in the event that they collapse. It is important to have a discussion in advance to avoid highly stressed and emotional situations during critical moments.
’’MS SHERLYN LEE, nursing manager at Active Global Caregivers.
HelpAtYourFingertips
3 questions to ask on end-of-life care choices
| TUESDAY, MARCH 6, 2018 | THE STRAITS TIMES | MIND&BODY B11
Dr David Goh
Medical director and senior consultant ophthalmologist, Novena Bladeless Cataract Surgery Centre
TREATMENT FOR PRESBYOPIA AND CATARACT■ 100% bladeless cataract surgery■ Computer-guided lens implantation
Q My 62-year-old uncle has cataracts and has been advised to go for bladeless laser cataract surgery. Can you tell me more about this procedure?
A As a person ages, a cataract can occur when the natural lens inside the eye becomes cloudy, causing symptoms such as blurred vision, glare or halos around bright lights, loss of colour or depth perception, and difficulty with vision in dim light.
Cataracts cannot be treated by medication or wearing spectacles, so surgery is the best option.
What is cataract surgery?Modern cataract surgery is a safe and effective 20-minute outpatient procedure that involves making a 2mm incision on the cornea, cutting the cataract into small pieces, re-moving the pieces and implanting a lens implant.
The surgery is also an opportuni-ty for patients to correct or reduce pre-existing myopia (short-sighted-ness), astigmatism and presbyopia (“lao hua”).
Traditional cataract surgeryFor the last 50 years, surgeons have been performing cataract surgery with a manual technique — using blades to make corneal incisions, and phacoemulsification (ultrasound) to cut up cataracts — which has limited precision and possible human error.
Modern cataract surgeryIn bladeless laser cataract surgery, a femtosecond laser machine is used to complete many of the steps pre-viously performed manually by the
surgeon, thus reducing the chance of human errors.
This allows cataract surgery to become more precise and, ultimate-ly, improve on safety and visual out-comes.
The femtosecond laser system uses a technology that is based on:
■ 3D Optical Coherence To-mography (OCT) imaging: Like a fingerprint, every eye has a unique size and shape. Before the treatment, the femtosecond laser system scans the patient’s eye and makes precise 3D maps of eye structures using real-time, high-definition OCT im-aging (below) to plan a customised treatment map of each eye.
■ Laser precision: Without man-ual cuts, the femtosecond laser (gas bubbles) creates a precise opening on the lens capsule for the removal of the cataract.
■ Gentler cataract surgery: The femtosecond laser then softens and divides the cataract into multi-ple pieces, blade-free. The surgeon can remove the cataract more gen-tly, which also enables faster post-op
visual recovery for pa-tients.
Computer–guided lens implantationAfter the removal of the cataract, the surgeon uses a computer-guided lens implantation sys-tem (left) that enables him to see alignment images during the actu-al insertion of the lens
implant. This helps the implant at-tain near-perfect overlap and accu-rate centration.
Overall advantagesThe advantages of using femtosec-ond laser and computer-guided lens implantation systems include:■ Improved safety and precision,■ Can be performed using topical anaesthetic eye-drops,■ No sharp blades involved,■ No stitches required,■ More precise alignment of artifi-cial lens implant, and■ Quicker return of vision after sur-gery.