3 mm Volume 11 - Stony Brook Medicine
4
Volume 11 Issue 4 • October-December 2019 •
Transcript of 3 mm Volume 11 - Stony Brook Medicine

Journ
al o
f Glo
bal In
fectio
us D
iseases • V
olu
me 1
1 • Issu
e 3
• Ju
ly-S
ep
tem
ber 2
019 • P
ages ***-***
spine3 mm
Volume 11 Issue 4 • October-December 2019 •

Letters to Editor
locally. We believe that with continued collaborative efforts, we will hopefully reduce the threat of AR in the coming years.[18]
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
Vikas Yellapu1,2, Nicholas Roma3, Victoria Ngo3, Parampreet Kaur1, Richard Snyder4
Departments of 1Research and Innovation, 2Orthopaedics and 4Internal Medicine, St. Luke’s University Health Network, Bethlehem, 3Lewis Katz School
of Medicine, Temple University, Philadelphia, Pennsylvania, USA
Address for correspondence: Dr. Vikas Yellapu, 801 Ostrum Street, Bethlehem, Pennsylvania 18015, USA.
E‑mail: [email protected]
RefeRences1. Cooper MA, Shlaes D. Fix the antibiotics pipeline. Nature 2011;472:32.2. Hampton T. Report reveals scope of US antibiotic resistance threat.
JAMA 2013;310:1661-3.3. The Center for Disease, Dynamics Economics and Policy.
ResistanceMap: Antibiotic resistance 2019. Available from: https://resistancemap.cddep.org/. [Last accessed on 2019 Jul 30].
4. Ventola CL. The antibiotic resistance crisis: Part 1: Causes and threats. P T 2015;40:277-83.
5. Nurse-Findlay S, Taylor MM, Savage M, Mello MB, Saliyou S, Lavayen M, et al. Shortages of benzathine penicillin for prevention of mother-to-child transmission of syphilis: An evaluation from multi-country surveys and stakeholder interviews. PLoS Med 2017;14:e1002473.
6. Wyber R, Taubert K, Marko S, Kaplan EL. Benzathine penicillin G for the management of RHD: Concerns about quality and access, and opportunities for intervention and improvement. Glob Heart 2013;8:227-34.
7. Langreth R. Antibiotics Aren’t Profitable Enough for Big Pharma to Make More. Bloomberg Businessweek; 2019.
8. Talkington, Kathy. “Antibiotics Currently in Global Clinical Development.” The Pew Charitable Trusts, Feb. 2014, https://www.pewtrusts.org/en/research-and-analysis/data-visualizations/2014/antibiotics-currently-in-clinical-development.
9. O’Neill J. Antimicrobials in agriculture and the environment: Reducing unnecessary use and waste. Rev Antimicrob Resist 2015; 1:1-44.
10. Van Boeckel TP, Brower C, Gilbert M, Grenfell BT, Levin SA, Robinson TP, et al. Global trends in antimicrobial use in food animals. Proc Natl Acad Sci U S A 2015;112:5649-54.
11. Cuong NV, Padungtod P, Thwaites G, Carrique-Mas JJ. Antimicrobial
usage in animal production: A review of the literature with a focus on low- and middle-income countries. Antibiotics (Basel) 2018;7. pii: E75.
12. Dall C. FDA Reports Major Drop in Antibiotics for Food Animals. Center for Infectious Disease Research and Policy; 2018.
13. Lhermie G, Gröhn YT, Raboisson D. Addressing antimicrobial resistance: An overview of priority actions to prevent suboptimal antimicrobial use in food-animal production. Front Microbiol 2016;7:2114.
14. Charani E, Cooke J, Holmes A. Antibiotic stewardship programmes – What’s missing? J Antimicrob Chemother 2010;65:2275-7.
15. Goff DA, Kullar R, Goldstein EJ, Gilchrist M, Nathwani D, Cheng AC, et al. A global call from five countries to collaborate in antibiotic stewardship: United we succeed, divided we might fail. Lancet Infect Dis 2017;17:e56-63.
16. Gilchrist M, Wade P, Ashiru-Oredope D, Howard P, Sneddon J, Whitney L, et al. Antimicrobial stewardship from policy to practice: Experiences from UK antimicrobial pharmacists. Infect Dis Ther 2015;4:51-64.
17. Center of Disease Control and Prevention. Antibiotic Resistance Data.2018. Available from: https://gis.cdc.gov/grasp/PSA/MapView.html. [Last accessed on 2019 Jul 30].
18. Hwang TJ, Carpenter D, Kesselheim AS. Paying for innovation: Reimbursement incentives for antibiotics. Sci Transl Med 2015;7:276fs9.
19. The Center for Disease, D.E.P., ResistanceMap: Animal Use. 2019.https://resistancemap.cddep.org/AnimalUse.php.
20. The Center for Disease, D.E.P.,ResistanceMap: Antibiotic Use.2019.https://resistancemap.cddep.org/AntibioticUse.php
21. Tracking global trends in the effectiveness of antibiotic therapy using the Drug Resistance Index. BMJ Global Health, 2019. 4(2): p. e001315.
Access this article online
Quick Response Code:Website: www.jgid.org
DOI: 10.4103/jgid.jgid_115_19
How to cite this article: Yellapu V, Roma N, Ngo V, Kaur P, Snyder R. Key factors in antibiotic resistance. J Global Infect Dis 2019;11:163-5.Received: 29 August 2019 Accepted: 04 September 19 Published: 26 November 2019© 2019 Journal of Global Infectious Diseases | Published by Wolters Kluwer - Medknow
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Adjuvant Maggot Debridement Therapy for Deep Wound Infection due to Methicillin‑resistant Staphylococcus aureus
Sir,
Community-acquired methicillin-resistant Staphylococcus aureus (MRSA) is the leading cause of skin and soft-tissue infections in the United States.[1] The management of chronic wounds poses a challenge for clinicians despite
technological advances of modern medicine. The use of maggots to heal wounds existed from antiquity.[2] There is growing evidence recognizing maggot therapy as a safe and effective treatment of wounds, with increased understanding of its mechanism of action for debridement, disinfection, and wound healing.[3] Maggot debridement therapy (MDT)
Journal of Global Infectious Diseases ¦ Volume 11 ¦ Issue 4 ¦ October-December 2019 165
Swati.Veer
Rectangle

Letters to Editor
is essentially debridement of necrotic tissue by biochemical and mechanical means.[3]
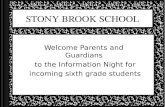
An 82-year-old Caucasian male with diabetes presented to our hospital with 4 days of febrile illness and upper back discomfort after sustaining a mechanical fall. On physical examination, temperature was 101.9°F and blood pressure was 87/50. There was no audible murmur. A 5 cm × 4 cm abscess with surrounding cellulitis was noted medial to the left scapula [Figure 1a]. During surgical debridement, a copious amount of pus was removed. Laboratory studies revealed the following: white blood cell count, 17,600/mm3 with 89% neutrophils and 2% bands; hemoglobin A1c 6.9%. A wound culture and four sets of blood cultures in 2 consecutive days revealed MRSA. Dual-antibiotic treatment was started: ceftaroline (renally adjusted due to serum creatinine of 4.4 mg/dL) intensified with daptomycin at 4 mg/Kg. Fever and leukocytosis resolved 72 h after initiation of antibiotics. A transthoracic echocardiogram did not show vegetations on any cardiac valve. Ten days after the initial debridement, the wound measured 7 cm × 4 cm, filled mostly with fibrinous material [Figure 1b]. It was decided to use maggots for the debridement. Figure 1c shows placement of the maggots, live larvae product BioBag® (BioMonde®, Gainesville, Florida, USA), which contains green bottle larvae from the fly Lucilia sericata. A heat-sealed porous polyester bag, containing the larvae, was applied on the wound. Video 1 shows the bagged larvae being removed from the wound after 3 days of continuous application. After two consecutive treatments with MDT, each one for 72 h of application [Figure 1d after one application and Figure 1e after second application], the wound had no fibrinous material and a pink-colored granulation tissue was present at wound edges. After 7 days of the combination antibiotic treatment, the patient completed an additional 4-week course with daptomycin, with continued improvement in wound healing.
This case report offers supporting evidence that MDT will hasten wound healing of deep and complex MRSA-infected cutaneous abscesses. A recent meta-analysis demonstrated that MDT shortened the healing time and improved healing rate of chronic ulcerations.[4] Bowling et al. were the first to demonstrate elimination of MRSA colonization in chronic
diabetic foot ulcers using MDT with an efficacy of 92%.[5] Nishijima et al. reported successful use of MDT to achieve limb salvage of MRSA-infected wound with critical ischemia.[6]
Initially, we chose to combine daptomycin and ceftaroline to treat the patient’s MRSA bacteremia and sepsis. Prior evidence showed that this combination can be used as salvage therapy for persistent bacteremia due to MRSA.[7] More recent data demonstrated that the same combination achieved shorter duration of MRSA bacteremia compared to the standard of care (monotherapy with vancomycin) and can possibly be associated with improved mortality.[8] The Patient’s bacteremia cleared quickly, and after of the ceftaroline–daptomycin combination, an additional 4-week course with daptomycin was given in accordance to treatment guidelines for complex MRSA infections.[9]
We believe that MDT hastened improvement of our patient’s wound through the removal of fibrinous debris without harming healthy tissue. The interdisciplinary collaboration of infectious diseases and surgical and wound care specialists led to an evidence-based approach to resolve a complex and large wound.
Declaration of patient consentThe authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
Olga Kaplun1, Magdalena Pupiales2, George Psevdos3,4
1Department of Infectious Diseases, Stony Brook University Hospital, 4Department of Infectious Diseases, Stony Brook University School of Medicine,
2Department of Surgery, Veterans Affairs Medical Center, 3Veterans Affairs Medical Center, NY, New York, USA
Figure 1: (a) The patient at presentation, large draining abscess medial to the left scapula. (b) The wound 10 days after initial debridement filled with fibrinous material. (c) Placement of BioBag® maggot debridement therapy. (d and e) Debridement of fibrinous material by maggot debridement therapy after 1st and 2nd application, respectively
dcba e
Journal of Global Infectious Diseases ¦ Volume 11 ¦ Issue 4 ¦ October-December 2019166

Letters to Editor
Address for correspondence: Dr. George Psevdos, Veterans Affairs Medical Center, 79 Middleville Road, Northport, NY 11768,
New York 11768, USA. E‑mail: [email protected]
RefeRences1. Boucher H, Miller LG, Razonable RR. Serious infections caused
by methicillin-resistant staphylococcus aureus. Clin Infect Dis 2010;51 Suppl 2:S183-97.
2. Whitaker IS, Twine C, Whitaker MJ, Welck M, Brown CS, Shandall A. Larval therapy from antiquity to the present day: Mechanisms of action, clinical applications and future potential. Postgrad Med J 2007;83:409-13.
3. Sherman RA. Mechanisms of maggot-induced wound healing: What do we know, and where do we go from here? Evid Based Complement Alternat Med 2014;2014:592419.
4. Sun X, Jiang K, Chen J, Wu L, Lu H, Wang A, et al. A systematic review of maggot debridement therapy for chronically infected wounds and ulcers. Int J Infect Dis 2014;25:32-7.
5. Bowling FL, Salgami EV, Boulton AJ. Larval therapy: A novel treatment in eliminating methicillin-resistant staphylococcus aureus from diabetic foot ulcers. Diabetes Care 2007;30:370-1.
6. Nishijima A, Yamamoto N, Yoshida R, Hozawa K, Yanagibayashi S, Takikawa M, et al. Maggot debridement therapy for a patient with critical limb ischaemia and severe cardiac dysfunction: Possibility of limb salvage. Case Reports Plast Surg Hand Surg 2017;4:42-7.
7. Sakoulas G, Moise PA, Casapao AM, Nonejuie P, Olson J, Okumura CY, et al. Antimicrobial salvage therapy for persistent staphylococcal bacteremia using daptomycin plus ceftaroline. Clin Ther 2014;36:1317-33.
8. Geriak M, Haddad F, Rizvi K, Rose W, Kullar R, LaPlante K, et al. Clinical data on daptomycin plus ceftaroline versus standard of care monotherapy in the treatment of methicillin-resistant Staphylococcus
How to cite this article: Kaplun O, Pupiales M, Psevdos G. Adjuvant maggot debridement therapy for deep wound infection due to methicillin-resistant Staphylococcus aureus. J Global Infect Dis 2019;11:165-7.Received: 13 March 2019 Accepted: 04 September 2019 Published: 26 November 2019© 2019 Journal of Global Infectious Diseases | Published by Wolters Kluwer - Medknow
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Access this article online
Quick Response Code:Website: www.jgid.org
DOI: 10.4103/jgid.jgid_30_19
Video available on: www.jgid.org
aureous bacteremia. Antimicrob Agents Chemother 2019;63: pii: e02483-18.
9. Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, et al. Clinical practice guidelines by the infectious diseases society of America for the treatment of methicillin-resistant staphylococcus aureus infections in adults and children. Clin Infect Dis 2011;52:e18-55.
Journal of Global Infectious Diseases ¦ Volume 11 ¦ Issue 4 ¦ October-December 2019 167













![Medication Safety 2013: Stony Brook Medicine · Medication Safety 2013: Stony Brook Medicine ... [FMEA]) •Make it difficult ... complete the admission medication reconciliation](https://static.fdocuments.net/doc/165x107/5af50b277f8b9a9e598d80c4/medication-safety-2013-stony-brook-medicine-safety-2013-stony-brook-medicine-.jpg)



