
2SummaryAnnual-Report-2014-15.WEB_
16
Annual Report Summary 2014-2015 NHS EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP
-
Upload
joe-mccrea -
Category
Documents
-
view
291 -
download
0
Transcript of 2SummaryAnnual-Report-2014-15.WEB_

Annual Report Summary 2014-2015
NHS EAST LEICESTERSHIRE AND RUTLANDCLINICAL COMMISSIONING GROUP

WHO WE ARE
We are East Leicestershire and Rutland Clinical Commissioning Group (ELR CCG) - an NHS organisation set up by the Health and Social Care Act 2012 to plan, organise and pay for local NHS care. We operate from offices at Thurmaston in Leicester and employed 84 staff as at the end of March 2015.
During 2014-15, we served 321,580 patients registered with 32 GP practices in Blaby, Lutterworth, Market Harborough, Rutland, Melton Mowbray, Oadby and Wigston and the surrounding areas.
There is no doubt that 2014-15 has been a challenging year for everyone involved in organising and delivering health and social care to the people of East Leicestershire and Rutland. This summary sets out how we’ve risen to this challenge. We hope you’ll agree that, while there is plenty we still need to do, there is already plenty of which we can be proud.
WHAT WE DO
We commission - or buy in - health and care services including:• Primary Care;• Planned hospital care;• Urgent Care;• Rehabilitation care;• Community health services; and• Non-urgent patient transport.
Our area of operations contains:• 5 community hospitals;• 1 large acute provider;• 1 large non-acute provider;• 2 local authorities; and• 4 district/borough councils.
During 2014-15, we commissioned health services totalling £328 million for people registered with our GP practices. We do this by agreeing contracts with providers, ranging from small grants to the voluntary sector to a £126 million contract with University Hospitals of Leicester NHS Trust.
We also act as the co-ordinating commissioning body to manage the followingcontracts on behalf of all three Leicester, Leicestershire and Rutland CCGs:
• Out-of-county contracts for acute hospital care;• Out-of-county community health services;• East Midlands Ambulance Service;• Non-emergency patient transport services – Arriva Transport Solutions;• ‘Any qualified provider’ contracts – the list of approved providers for
some care services;• Leicester, Leicestershire and Rutland voluntary sector arrangements;• Community based elective care, using an alliance of commissioners and
providers; and• Home oxygen service contract for people with severe breathing problems.
East Leicestershire and Rutland CCG Annual Report Summary | 2014-151

2Annual Report Summary | 2014-15
WHERE OUR CARE IS DELIVERED

WHAT WE BELIEVE IN
Our vision and values guide what we are trying to achieve and how we wish go about it.
Our vision is “to improve health by meeting our patients’ needs with high quality and efficient services, led by clinicians and delivered closer to home.”
In pursuing this vision, we are guided by nine values:
• Quality - ensuring quality underpins everything we do;• Involvement - involving our patients, practices, staff, partners and the public in all aspects of our work, with a strong commitment to listen, learn and act on their views;• Innovation - embracing new ideas, seeking creative solutions to deliver the
best results;• Progression - looking ahead to identify and seize opportunities;• Inspiration - striving for excellence, inspiring confidence and trust in others;• Respect - championing equality, treating our patients and each other with
respect, dignity and professionalism;• Education - improving services and quality through effective training and
development for staff and clinicians;• Economy - spending wisely and preventing waste; and• People - developing a team people want to work with, where staff are valued and involved.
THE PEOPLE WE SERVE
50.6% of our population is female, which is similar to the England average of 50.2%
The average life expenctancy within East Leicestershire and Rutland is 80.5 years for men, and 83.9 years for women, both of which are higher than the England average.
The number of people aged 60 and over is higherthan the England average (22.6%), and our older population is predicted to increase over the next 10 years, with an estimated 19,000 additional people aged 60 years and over.
I In NHS East Leicestershire and Rutland, only a small proportion of people live in deprived areas Nevertheless, there are significant pockets of disadvantage i in areas on the edges of Leicester City and within the market towns. We have to ensure this deprivation is not overlooked.
Accounting for more than two-thirds of all deaths, the major killers in East Leicestershire and Rutland are:
• cancer (29%)• cardiovascular disease – CVD - (27%)• respiratory disease (13%).
The health of our local population is generally better than the overall population of England. However, there is a significant number of people affected by ill health, including coronary heart disease (10,739 people), hypertension – high blood pressure - (47,770 people) and diabetes (16,625 people).
East Leicestershire and Rutland CCG Annual Report Summary | 2014-153

4Annual Report Summary | 2014-15
“WE ARE A ‘CLINICALLY LED’ ORGANISATION”
That’s not simply a phrase we use. It’s central to what we’re about and how we do things. It means that our aims and priorities are driven by local family doctors and other clinicians, rooted in their own local communities across East Leicestershire and Rutland.
Clinicians are in the majority in our decision makers. They are trusted by local people and their families to have their best interests at heart and are deeply committed to helping them get healthy and stay healthy. Or when people fall ill, to make sure they get the very best treatment and care possible, in the right place at the right time, and delivered with compassion and respect.
We estimate that during a typical year, well over two million individual consultations take place in doctors’ surgeries in our area. That’s an average of around 5,500 a day.
The insight gleaned from family doctors and other health professionals carrying out these consultations gives them a powerful and unique insight into the real health needs of local people and their families, as well as how the healthcare system works in day-to-day reality. Together with their colleagues working in hospitals and other healthcare settings, they hold unique knowledge that cannot be obtained elsewhere.
WE DO NOT WORK ALONE
Partnership working is vital to how we work and it is the best way to bring about many of the changes we wish to see. Over the last year we have actively engaged with partner organisations to build on existing relationships and develop new and improved relations with clinicians, patients and carers, public members, staff, partner organisations including local authorities, and other commissioning agencies.
We have many partners, and have established key working relationships with the following:
• Leicester City and West Leicestershire CCGs;• Leicestershire County Council and Rutland County Council, particularly with social service commissioners and through Health and Wellbeing Boards, as well as the borough and district councils within our CCG boundaries;• Our providers including University Hospitals of Leicester NHS Trust, Leicestershire Partnership NHS Trust, East Midlands Ambulance Service, voluntary sector providers and charities;• Healthwatch Leicestershire, Healthwatch Rutland, and other patient and carer representative bodies;• Leicestershire Police and Leicestershire Fire and Rescue Service;• De Montfort University and the University of Leicester;• NHS Arden and Greater East Midlands Commissioning Support Unit; and• Health Education East Midlands.
We are an active partner key in the Better Care Together (BCT) programme. This is a significant programme of work which will transform the health and social care system in Leicester, Leicestershire and Rutland (LLR) by 2019. BCT brings together partners, including local NHS organisations and councils, to ensure that services change to meet the needs of local people.
Dr Richard HurwoodGP Locality Lead, Melton, Rutland and Harborough
Dr Richard PalinClinical Chair
Dr Andy KerClinical Vice Chair
Dr Vivek VarakantamGP Locality Lead, Oadby and Wigston
Dr Girish PurohitGP Locality Lead, MeltonRutland and Harborough
Dr Hilary FoxGP Locality Lead, MeltonRutland and Harborough
Dr Graham JohnsonGP Locality Lead, Blaby and Lutterworth
Dr Nick GloverGP Locality Lead, Blaby and Lutterworth
Dr Tabitha RandellSecondary Care Clinician

WE ARE A LISTENING ORGANISATION
We’re constantly looking for ways, new and old, to listen to people’s concerns and views, then do something about what they tell us and – crucially - be seen to do so. That’s not just good in principle, it’s good in practice. It means we’re much more likely to get things right first time or be able to put things right if they’re not working as they should.
As this summary hopefully shows, we’ve had some real successes over the past year in this regard, including:
• Taking a ‘Listening Booth’ – a portable kiosk - to more than 25 locations to enable our patients, the public and carers to tell us in their own words how they feel about local healthcare ;
• Collating ‘patient stories’ – their own experiences of healthcare – recorded on video from individual patients and discussed at our Governing Body meetings to improve our understanding; and
• Conducting detailed public engagement work on urgent care and community services.
We intend to build on this listening work with an integrated web, social media and mobile engagement strategy – to put us right at the forefront of the NHS digital revolution.
We are always looking for ways to refine and/or improve how we listen. Anyone can let us have their ideas and views by e-mailing us at:[email protected]
WHAT OUR GPS, PATIENTS AND STAFF HAVE TOLD US
During 2014-15 we also carried out detailed Practice Member engagement - visiting our practices and hearing their views, ideas and concerns. This engagement clarified many of the challenges encountered by patients, carers and GPs. Our programme of change and improvement during 2015-16 is designed to address these challenges.
These include:• Patients find accessing care confusing, and setting up a ‘care package’ for a
patient is confusing and time consuming for GPs;• GPs will need to manage more patients with complex medical care needs at
home;• Significant recruitment and retention issues in community nursing with a high vacancy rate;• Community services set up to deliver care aimed at avoiding hospital
admissions are affected by the inability to recruit staff and the pace of major changes taking place in the organisation of health and social care services across Leicester, Leicestershire and Rutland;
• Small numbers of physical beds are spread across four sites, which risks compromising clinical quality and is not cost-effective; and
• Under-use of current Intensive Community Support ‘beds’ – ie, care at home or in care homes.
In all that GPs, patients, staff, carers and families have told us, the key messages are that they would like to be able to deliver better quality and more effective services, with:
• More care delivered closer to home including access to services in patients’ own homes and other alternatives to hospital admissions;
• Closer working with social care to improve care pathways – ie, the courses of treatment, rehabilitation and after-care; and• More work on prevention, reducing diseases through screening, advice and
health checks.
East Leicestershire and Rutland CCG Annual Report Summary | 2014-155
Listening Booth Word Cloud

6Annual Report Summary | 2014-15
LISTENING, RESPONDING, DELIVERING…
Over the last year our priorities for new investment were:• Transforming primary care;• Redesigning community services;• Delivering an effective urgent care system;• Improving mental health and giving it equal importance to physical health;• Developing services for people with long-term conditions; and• Delivering maternity, children and young people’s services.
Overall, we believe our CCG has made good progress during our first two years. In particular, our clinical leaders highlight the following achievements and new services that have particularly benefited local patients and clinicians:
• The introduction of new Urgent Care Centres in Oadby, Market Harborough, Oakham and Melton Mowbray – offering increased access to care for patients at weekends, evenings and bank holidays;• Improving services for patients with mental health needs, through redesign
of the acute mental health pathway, plus a new crisis house for those finding themselves in immediate need of support;• Advanced care planning, with everyone proactively planning and working
together to meet the needs of people in care homes and those approaching the end of their lives;
• Expansion of Increasing Access to Psychological Treatment services – ‘talking therapies’ - with more patients requesting such care, resulting in improved uptake of the service;
• Strengthening the crisis pathway for patients with mental health needs, particularly for those with urgent needs, but who are not in crisis, so they are now seen within five days;• Working with our colleagues in Leicestershire Partnership NHS Trust (LPT) to reduce out-of-area places from 37 down to single figures so patients and their families and friends do not have to travel so far;
• Introducing a training programme for GPs in all practices in atrial fibrillation - abnormal heart rate - reducing the chance of patients suffering from blood clots or strokes;• Developing the first Alliance Partnership agreement in the country to bring together outpatient, day-case and diagnostic services in the community, closer to patients and their homes, and freeing up beds in major hospitals for other patients who need them;• Extending patient choice, reducing waiting times and backlogs by achieving
national standards for Referral to Treatment (ie, waiting) times • Ensuring the voice of children and young people is heard in decisions over
local health and care strategies and delivery, recognising that the children of today are the adults of the future;
• Improving services for children and young people with eating disorders;• Coming below the national average for antibiotic prescribing, helping avoid
unnecessary use of antibiotics, which risks reducing their effectiveness; and• Development of the Intensive Community Support service, provided by
LPT, with 48 at-home places across our area.The service is able to respond promptly to unscheduled care requests and is integrated into the Intensive Community Response Service and night assessment at-home service by nurses.
During 2014-15 the CCG worked closely with all service providers and partners across health and social care to support the implementation of plans to drive up quality of care and performance.
Planned care Urgent care
Community care
Primary care
Mental health Maternity and neonates /Children and young people
Long termconditions
Rehabilitation care Non-urgentpatient transfer

THE CHALLENGE OF CHANGE
We are embarking upon significant change to commissioning future community and primary care services which has been clearly laid out in a number of reports including the CCG’s Integrated Community Services Strategy, and the Primary Care Operating Framework: A GP Guide November 2014.
We were particularly pleased in February 2015 to be selected by NHS England to be one of the first wave of CCGs in the country to take on responsibility for jointly commissioning GP services with NHS England from April 2015. This will give patients, communities and clinicians more scope in deciding how local services are developed.
The emergence of ‘GP Federated models’ – GP practices working together in new groups - is also underway and offers the opportunity for partnership working to strengthen any new community services model that is commissioned.
To achieve our proposed model for the future of community services we have spent time engaging with local stakeholders including providers, local authorities, voluntary sector and GP locality groups.
Our engagement process has enabled us to understand current issues and the potential for bringing together community and primary care services. We have
identified a number of areas which need to be addressed to ensure a solid foundation for community services.
We will be embarking on a further round of engagement in the autumn to ensure we get things absolutely right. We will be asking what works best for patients and what will work best.
The following ways forward are not exhaustive and include:• Changing the current model of community services commissioning to give the CCG and its GPs more accountability to influence how services are delivered• Creation of joint GP/provider posts to enhance accountability;• Delivery of a rehabilitation system that moves services from a hospital to recovery at home with the right support;• Improving access to community services that are currently considered less than perfect, including physiotherapy;• Expanding the times when care is available both at home and in health facilities;• Establishing clinical support networks and services in acute and primary care to identify, enable and manage both complex care, frail elderly and sub-acute care locally;• Making the most of the land and buildings available to deliver local services, avoiding unnecessary travel to major hospitals;• Minimising the procedural barriers to more effective health and social care by simplifying the specifications, and by the joint commissioning of primary, social and community services; and• Changing the model of community services commissioning to focus on the actual outcomes of treatment and care rather than the inputs.
East Leicestershire and Rutland CCG Annual Report Summary | 2014-157
What’s the real challenge?
What’s the real need?
Will it deliverfor patients?
Will itwork?

8Annual Report Summary | 2014-15
WHAT WE’LL DO NEXT
Everybody knows money is tight - exceptionally so - and the financial challenge is not going to go away soon. Our health economy in Leicester, Leicestershire and Rutland faces a deficit of almost £400 million by 2018-19 if we do not fundamentally redesign and transform the way we do things.
That gives us an opportunity to design services that are more convenient for patients, while making the best use of every penny of taxpayers’ money we receive.
So our plans concentrate on transforming from a system that overly relies on too many people having to stay in hospital beds to one that supports and manages more people within their local communities and in their own homes.
Building on these foundations, our Two Year Operational Plan focuses on transforming services to enhance the quality of life for people with long-term health conditions, improve quality of care, reduce inequalities in access to healthcare and improve joint working and integration with social care.
In particular, in 2015-16, we plan to:• Lay strong foundations for the delivery of new and integrated systems of care in line with the Better Care Together programme and our Better Care Fund to bring about necessary changes and improve the health outcomes for our population;• Prioritise programmes of work which offer the best patient outcomes, and deliver quality changes ‘at pace’ across our health and social care economy; and• Focus on affordable developments that deliver value-for-money redesign which make the most of modern healthcare methods and technologies.
In practical terms, this will include:• Improved performance in waiting times at A&E;• Introduction of seven-day working in primary care and improved integration with community services;• Improved access to psychological services, through more investment and joint working with colleagues in West Leicestershire CCG;• Improved patient choice and delivery of national standards in the time taken between referral to treatment, cancer and diagnostic standards;• Increased investment in dementia care management;• Better home-visiting services for people with complex or multiple needs;• Rapid access to diagnostics for our frail older people;• Reduction in avoidable admissions to hospital;• Improved end-of-life care, with more people dying in their place of choice; and• Implementation of a unified ill-health prevention scheme for patients, including weight management, physical activity and sexual health.

East Leicestershire and Rutland CCG Annual Report Summary | 2014-159
QUALITY AND EXCELLENCE
We continue to be committed to improving the quality of patient care, by a focus on clinical effectiveness, patient safety and patient experience with specific goals to deliver excellent health services and improve the quality of patient care.
This will be achieved by: • Continuously improving the quality of care within providers, including acute, mental health and community services using contractual processes as a lever;• Combining commissioning and provider data with patient safety data and carer feedback, including complaints, reference groups and engagement events, to inform areas requiring improvement and attention and to ensure on-going improvement;• Reducing variations in primary care, for example, access to primary care services, appropriate prescribing, equitable access to health checks for all patients including hard to reach groups; • Extending patient choice of provider for a range of community and mental health services through the use of local and national AQP processes; • Delivering efficiency by maximising the use of community services through an integrated care approach with health and social care, to provide a seamless service for patients; and• Assuring delivery through collaboration with main providers ensuring ‘value for money’ for all partners.
Our plans for 2015-16 include a review of all quality schedules and local Commissioning for Quality and Innovation (CQUIN) schemes to ensure improvements areas have a greater focus.
We routinely review data published by the Care Quality Commission (CQC) to inform our quality monitoring arrangements. Where providers have received action plans following inspection visits, we monitor progress against these through our quality contracting processes. During 2015-16 we will be extending this to include CQC intelligence within our quality data sets for care homes and primary GP practices.
We have built positive relationships with our local CQC inspectors and have developed joint meetings with local authority colleagues to ensure intelligence sharing around providers; this supports our responsibility following the Francis Report of the NHS Mid Staffordshire Foundation Trust Public Enquiry in 2013.
Improving quality of patient care
Excellent Community Health Services
Improving quality of acute services
Improving quality of Mental Health Services
High Quality ResponsivePatient Care
Patient Safety Clinical Effectiveness
Patient Experience

10Annual Report Summary | 2014-15
SAFEGUARDING
The CCG continues to have a strong focus on safeguarding vulnerable people. We have developed and adopted a range of policies which underpin how we approach safeguarding arrangements. The Quality and Performance Committee of the Governing Body has oversight and scrutiny of safeguarding arrangements for the CCG. The Chief Nurse and Quality Officer is the Executive Lead for safeguarding and is a member of the Leicestershire and Rutland Local Safeguarding Children Board (LSCB) and Safeguarding Adults Board (SAB). The CCG is supported in its statutory duties by Designated Nurses and a Designated Doctor for safeguarding.
The CCG uses the Markers of Good Practice for Children and Safeguarding Adults Framework which meets the requirements set out in Safeguarding Vulnerable people in the reformed NHS - accountability and assurance framework published in March 2013 to assess provider compliance against statutory safeguarding duties.
During 2014-15 the CCG along with NHS England Area Team and the two other Leicester and Leicestershire CCGs, commissioned a review of the designated function to ensure capacity and capability of this function in supporting the CCG with delivering its statutory duties.
This review has confirmed that the CCG has commissioned the appropriate level of Designated Doctor and Nurse time and we are reviewing local service level agreements to ensure the quality of the service provision for 2015-16.
There have been no serious case reviews commissioned by the Leicestershire and Rutland Safeguarding Board for people within East Leicestershire and Rutland CCG area during 2014-15. However the GP Locality forums have adopted a standardised approach to bringing any issues relating to safeguarding issues on a monthly basis. In the last year we have supported the partnership arrangements by contributing to the Child Sexual Exploitation campaign and we have a local Practice Nurse supporting the work of the multi-agency sub-group within the LSCB.
The CCG has completed and submitted to the LSCB and SAB a self-assessment against Section 11 audit and the Safeguarding Adults Assurance Framework .
East Leicestershire and Rutland CCG Annual Report Summary | 2014-1511
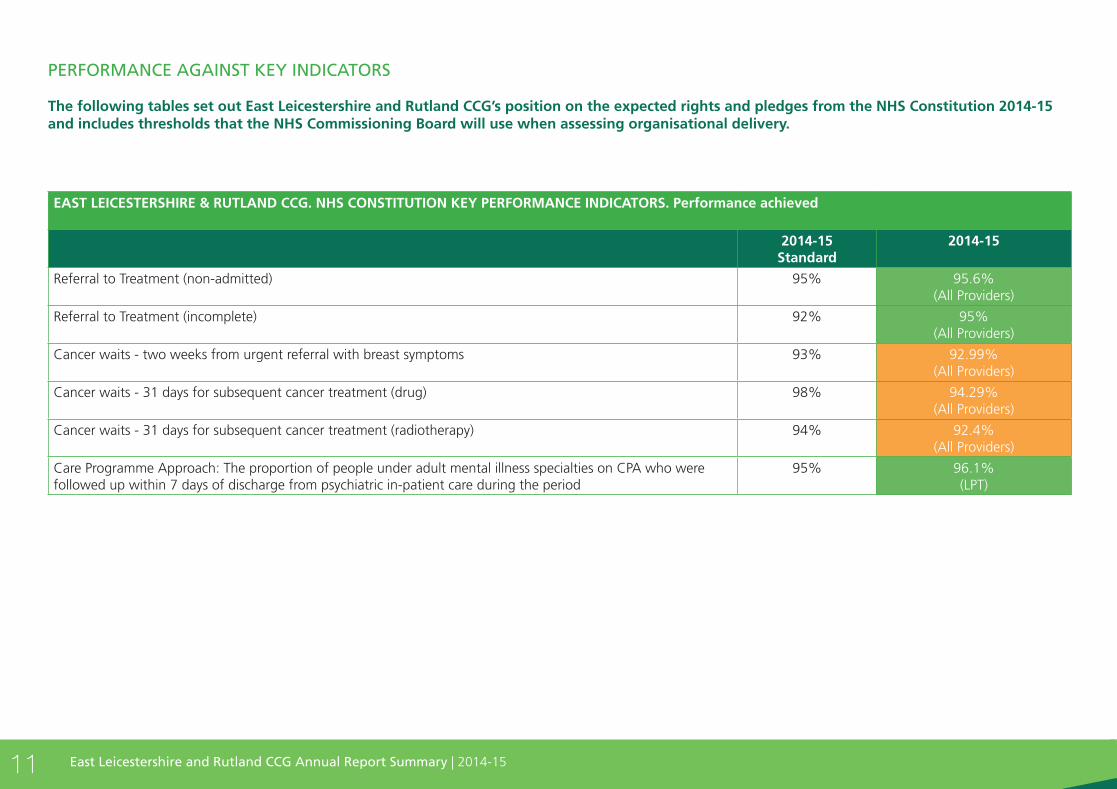
PERFORMANCE AGAINST KEY INDICATORS
The following tables set out East Leicestershire and Rutland CCG’s position on the expected rights and pledges from the NHS Constitution 2014-15 and includes thresholds that the NHS Commissioning Board will use when assessing organisational delivery.
EAST LEICESTERSHIRE & RUTLAND CCG. NHS CONSTITUTION KEY PERFORMANCE INDICATORS. Performance achieved
2014-15Standard
2014-15
Referral to Treatment (non-admitted) 95% 95.6%(All Providers)
Referral to Treatment (incomplete) 92% 95%(All Providers)
Cancer waits - two weeks from urgent referral with breast symptoms 93% 92.99%(All Providers)
Cancer waits - 31 days for subsequent cancer treatment (drug) 98% 94.29%(All Providers)
Cancer waits - 31 days for subsequent cancer treatment (radiotherapy) 94% 92.4%(All Providers)
Care Programme Approach: The proportion of people under adult mental illness specialties on CPA who were followed up within 7 days of discharge from psychiatric in-patient care during the period
95% 96.1%(LPT)

12Annual Report Summary | 2014-15
EAST LEICESTERSHIRE & RUTLAND CCG. NHS CONSTITUTION KEY PERFORMANCE INDICATORS. Performance achieved
2014-15Standard
2014-15
Referral to Treatment (admitted) 90% 86.4%(All Providers)
Cancer waits - two weeks from urgent GP referral 93% 92.9%(All Providers)
Cancer waits - 31 days to first definitive treatment
96% 94.2% (All Providers)
Cancer waits - 31 days for subsequent cancer treatment (surgery) 94% 92.4% (All Providers)
Cancer waits – 62 days from urgent GP referral to treatment 85% 82.8% (All Providers)
Cancer waits - 62 days from NHS screening service to treatment 90% 80.8% (All Providers)
Cancer waits - 62 days for treatment following a consultant’s decision to upgrade the priority of the patient
100% 92.3% (All Providers)
Diagnostic waiting times 99% 98.5%(All Providers)
Patients should be admitted, transferred or discharged within 4 hours of their arrival at an A&E department
95% 92% (UHL only)
Category A Red 1 incidents response within 8 minutes - (conditions that may be immediately life threatening and the most time critical)
75% 73.2% EMAS
Category A Red 2 incidents, response within 8 minutes - (conditions which may be life threatening but less time critical than Red 1)
75% 70.09% EMAS
Category A calls resulting in an ambulance arriving at the scene within 19 minutes 95% 93.2% EMAS
Cancelled ops - All patients who have operations cancelled, for non-clinical reasons, to be offered date within 28 days, or funded at the time and hospital of the patient’s choice.
100% 95.6%(UHL Only)
Mixed Sex Accommodation Breaches 0 breaches 5(All Providers)
NB: Indicators rated as ‘amber’ meet the lower threshold, but do not meet the nationally set target. For example: Referral to treatment (admitted) has a target of 90%, the lower threshold is 85%, therefore a position of 88.7% is between the target and the lower threshold, giving an amber indicator.
Table 5: Key Performance Indicators

WHAT WE SPENT
This summary shows how we’ve done during 2014-15, both in terms of health and social care development as well as in hitting all our financial targets, as follows:
• Achieving our planned expenditure against budget• Producing a planned surplus of £3.3m• Achievement of in-year financial savings plan of £9m.
For more detailed information please see our website, www.eastleicestershireandrutlandccg.nhs.uk where you can also download our full Annual Report and Accounts for 2014-2015.
East Leicestershire and Rutland CCG Annual Report Summary | 2014-1513
East Leicestershire and Rutland Clinical Commissioning GroupSummary Financial Performance
Budget£
Actual£
Variance - Under/Overspend£
Total Allocation 338,493,000 338,493,000 0
Total Acute Commissioning 154,290,935 160,217,997 5,927,062
Total Non-Acute Commissioning 105,584,715 109,084,218 3,499,504
Total Practice Prescribing 46,063,205 46,494,454 431,249
Total Primary Care Services 6,173,187 5,830,086 -343,101
Miscellaneous (inc reserves) 16,134,753 6,394,161 -9,740,592
Total Commissioned Healthcare Expenditure 328,246,795 328,020,917 -225,878
Total Running Costs 6,938,205 7,162,073 223,868
Total Expenditure 335,185,000 335,182,989 -2,011
Surplus £ £ £
Programme control total 2,308,000 2,512,083 204,083
Running Costs control total 1,000,000 797,927 -202,073
Total control total 3,308,000 3,310,011 2,011

14Annual Report Summary | 2014-15
We can provide versions of this plan summary in other languages and formats such as Braille and large print on request. Please contact the Engagement Team, telephone 0116 295 1486.
SomaliWaxaan ku siin karnaa bug-yarahaan oo ku qoran luqado iyo habab kale sida farta indhoolaha Braille iyo daabacad far waa-wayn markii aad soo codsato. Fadlan la soo xiriir qaybta Ka-qaybgalka iyo Dhex-gelidda, lambarka telefoonka waa 0116 295 1486.
PolishJeżeli chcieliby Państwo otrzymać kopię niniejszej ulotki w tłumaczeniu na język obcy lub w innym formacie, np. w alfabecie Braille’a lub w powiększonym druku, prosimy skontaktować się telefonicznie z zespołem ds. zaangażowania (Engagement and Involvement) pod numerem telefonu 0116 295 1486.
Cantonese
Gujarati
Hindi
Urdu
Arabic

Published by NHS East Leicestershire and Rutland Clinical Commissioning Group
Unit 2-3 (Ground Floor)Bridge Business Park674 Melton RoadThurmastonLeicestershireLE4 8BL


















