2.Human Bile Collection and Implication of Acylglucuronide ... 02zdl.pdf · Human Bile Collection...
30
Human Bile Collection and Implication of Acylglucuronide Instability Donglu Zhang 1 Donglu Zhang Drug Metabolism and Pharmacokinetics Genentech, One DNA Way South San Francisco, CA 94080 At 2015 Nanjing International DMPK Symposium At 2015 Nanjing International DMPK Symposium June 25, 2015 June 25, 2015
Transcript of 2.Human Bile Collection and Implication of Acylglucuronide ... 02zdl.pdf · Human Bile Collection...
Human Bile Collection and Implication ofAcylglucuronide Instability
Donglu Zhang
1
Donglu ZhangDrug Metabolism and PharmacokineticsGenentech, One DNA WaySouth San Francisco, CA 94080
At 2015 Nanjing International DMPK SymposiumAt 2015 Nanjing International DMPK SymposiumJune 25, 2015June 25, 2015
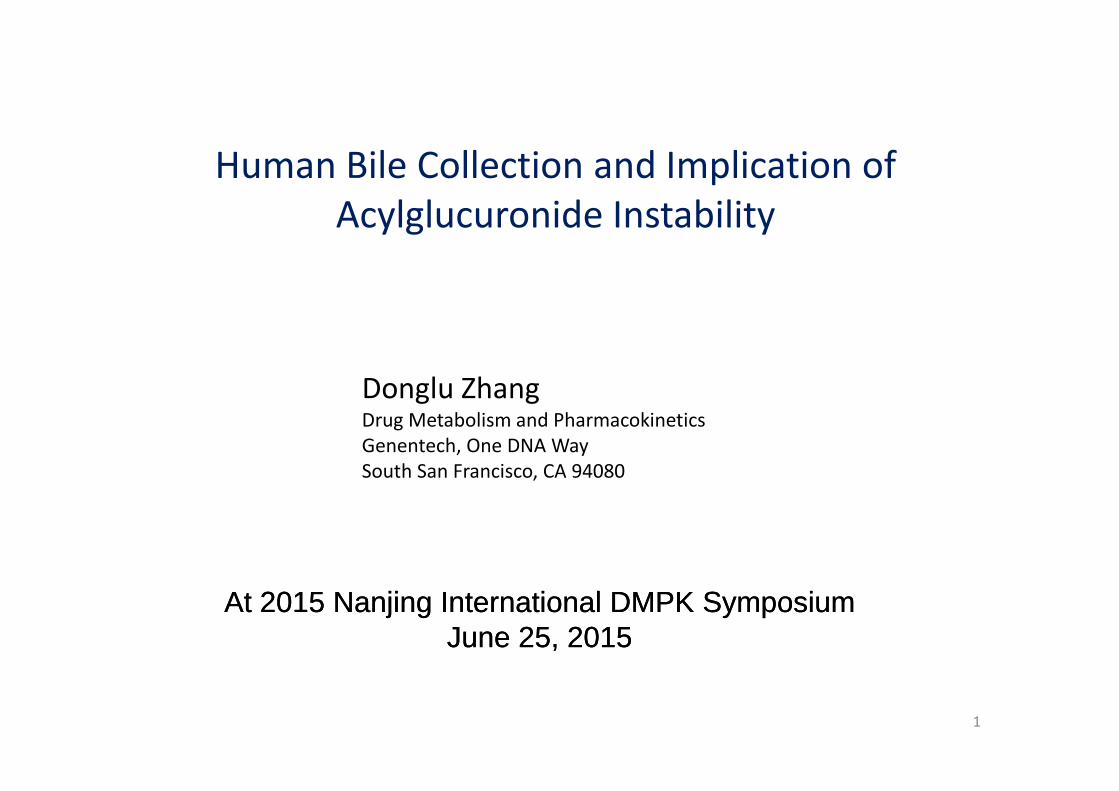
Bile Characteristics and Physiology
• Bile is a viscous, slightly alkaline, greenish-yellow liquid produced by hepatocytes in theliver.
• Bile contains bile salts, phospholipids, cholesterol, proteins, amino acids, nucleotides,vitamins, bile pigments…. The composition depends on species and nutrition withinspecies. Which can be altered under certain disease states, such as cholelithiasis,Crohn’s disease, cirrhosis, and malignancies of the hepatobiliary system.
• Bile is released from the gallbladder into the intestine in response to food consumption,acts as an emulsifying agent (facilitating digestion and the absorption of fats and fat-soluble substances), Serves as a carrier for removal of some drugs and toxins and theirsoluble substances), Serves as a carrier for removal of some drugs and toxins and theirmetabolites.
• In humans, approximately 1 liter of bile per day is produced by the liver. Bile, drainedinto common hepatic duct, is delivered via cystic duct to the gallbladder, where it isstored and concentrated up to 90% over time. When food enters the duodenum, thehormone cholecystokinin is released from the mucosal epithelium of duodenum,stimulating gall bladder contraction and ejection of bile as well as secretion ofpancreatic juice. The stored bile flows out of the gallbladder into the common bile duct,which joins with the pancreatic duct, and enters the duodenum at the ampulla of Vater.The flow of fluids from the common bile duct into the intestine is regulated by thesphincter of Oddi.
• The gallbladder is absent in some animals, like rat, pigeon and horse. 2
Bile Collection Techniques
• Rat, mouse, Dog, Monkey: Invasive Bile duct-cannulation.– The bile duct is surgically cannulated resulting in complete recovery of
the total biliary output. Bile can be collected for prolonged periods withsupplementation of bile acids. Bile collected via duct-cannulation is freeof gastric juices and other intestinal secretions.
• Human: Invasive and non-invasive techniques.– Invasive methods involve patients undergoing surgical procedures to– Invasive methods involve patients undergoing surgical procedures to
treat or diagnose underlying disease. - rare availability of patients
• Ultrasonically guided percutaneous, sub- or trans-hepatic fine-needle puncture of thegall bladder (Wee et al. 1995), hepaticojejunostomy (Brookman et al. 1997) or T-tubepercutaneous biliary drainage in patients after cholecystectomy (Rollins et al, 1979).
– Non-invasive methods in patients or healthy volunteers
3
Non-Invasive Human Bile Collection
• Naso/Ora-gastroduodenal aspiration– A naso/orogastric (NG) tube - suction of the fluids from from the stomach and
ampulla of Vater. e.g. [14C]montelukast (Singulair), (Balani et al. 1997).
– Modified: Miller-Abbott Type Intestinal Tube. e.g. [14C]muraglitazar , [14C]apixaban
• IV dose of Kinevac (sincalide, a synthetic cholecystokinin) 7 hours postdose tostimulate gallbladder contraction and maximize bile secretion
• Entero-Test®, String collection method (Guiney et.al., 2010)• Entero-Test®, String collection method (Guiney et.al., 2010)– It is also used in humans (poster on 29th ISSX)
– Snapshot of metabolic pathways in bile
4
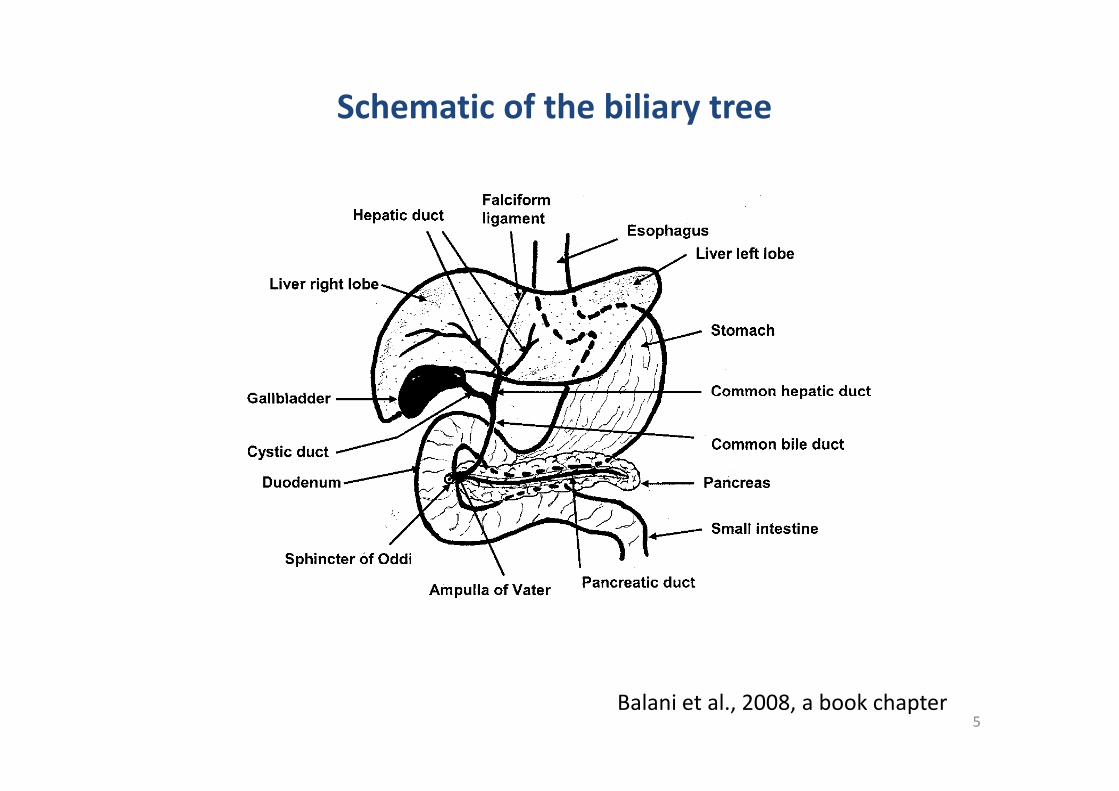
Schematic of the biliary tree
5Balani et al., 2008, a book chapter
Miller-Abbott type intestinal tube for bile collection
Amplified version
6
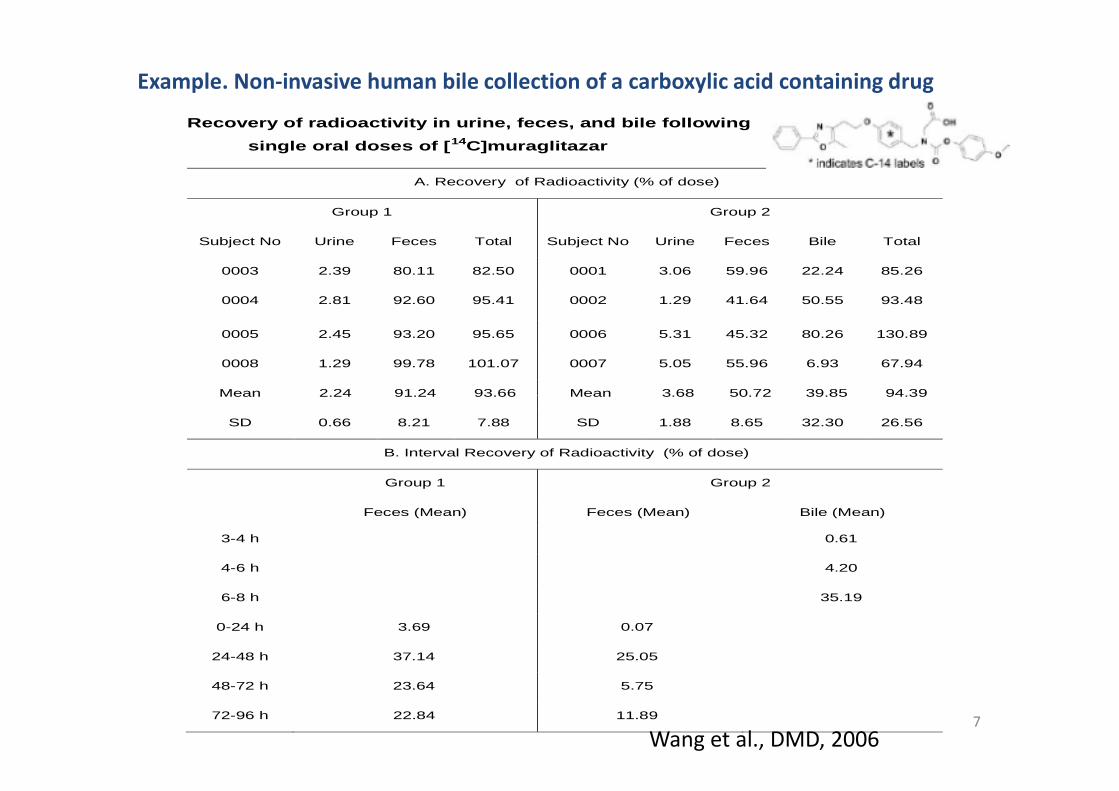
Example. Non-invasive human bile collection of a carboxylic acid containing drug
Recovery of radioactivity in urine, feces, and bile following
single oral doses of [14C]muraglitazar
A. Recovery of Radioactivity (% of dose)
Group 1 Group 2
Subject No Urine Feces Total Subject No Urine Feces Bile Total
0003 2.39 80.11 82.50 0001 3.06 59.96 22.24 85.26
0004 2.81 92.60 95.41 0002 1.29 41.64 50.55 93.48
0005 2.45 93.20 95.65 0006 5.31 45.32 80.26 130.89
0008 1.29 99.78 101.07 0007 5.05 55.96 6.93 67.94
Mean 2.24 91.24 93.66 Mean 3.68 50.72 39.85 94.39
7
Mean 2.24 91.24 93.66 Mean 3.68 50.72 39.85 94.39
SD 0.66 8.21 7.88 SD 1.88 8.65 32.30 26.56
B. Interval Recovery of Radioactivity (% of dose)
Group 1 Group 2
Feces (Mean) Feces (Mean) Bile (Mean)
3-4 h 0.61
4-6 h 4.20
6-8 h 35.19
0-24 h 3.69 0.07
24-48 h 37.14 25.05
48-72 h 23.64 5.75
72-96 h 22.84 11.89
Wang et al., DMD, 2006
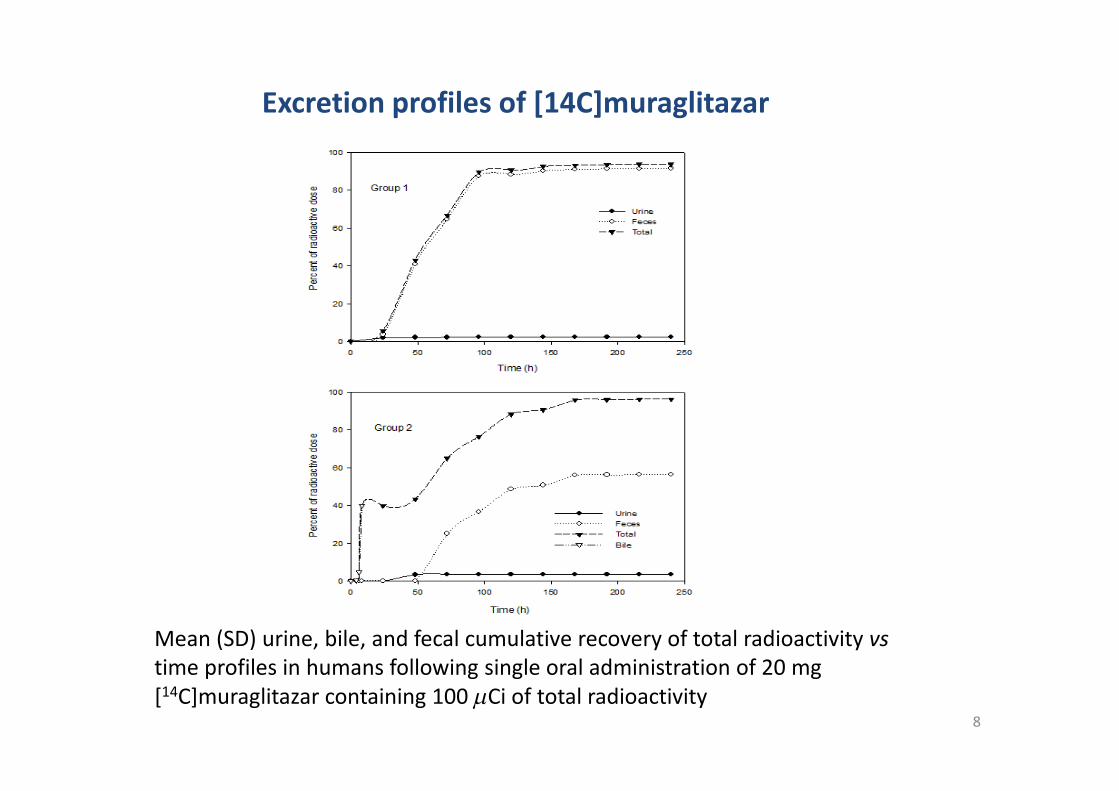
Excretion profiles of [14C]muraglitazar
8
Mean (SD) urine, bile, and fecal cumulative recovery of total radioactivity vstime profiles in humans following single oral administration of 20 mg[14C]muraglitazar containing 100 Ci of total radioactivity
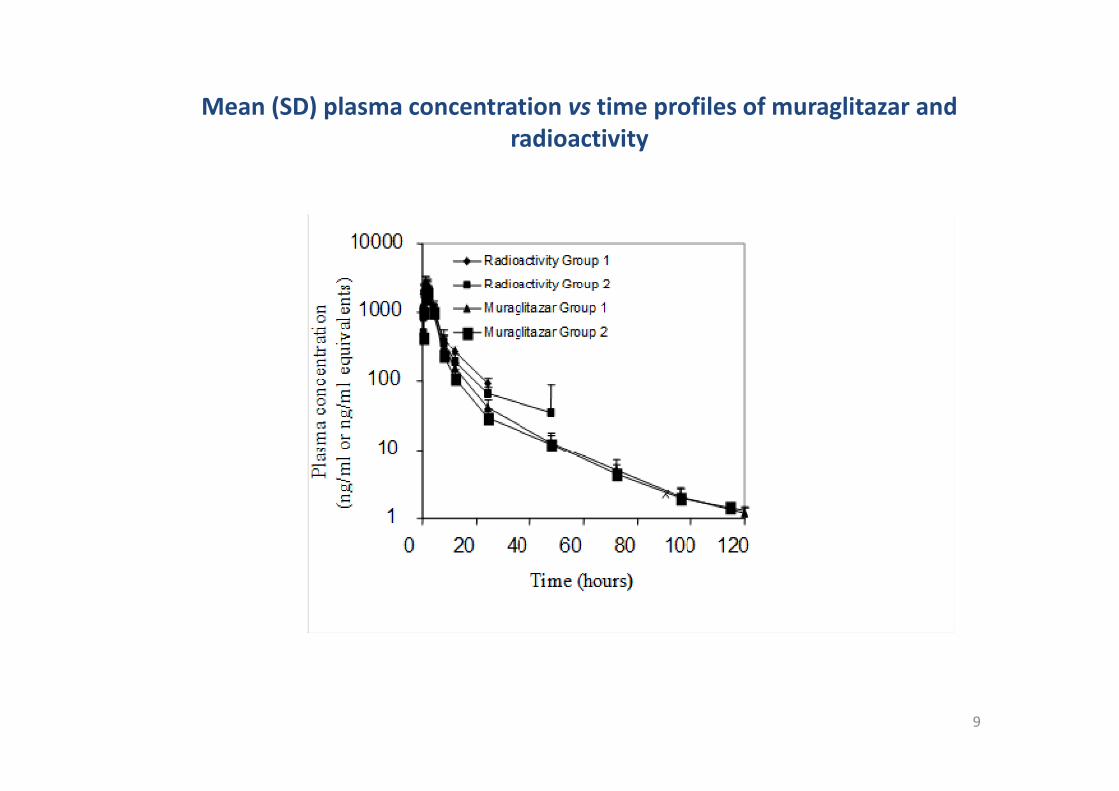
Mean (SD) plasma concentration vs time profiles of muraglitazar andradioactivity
9
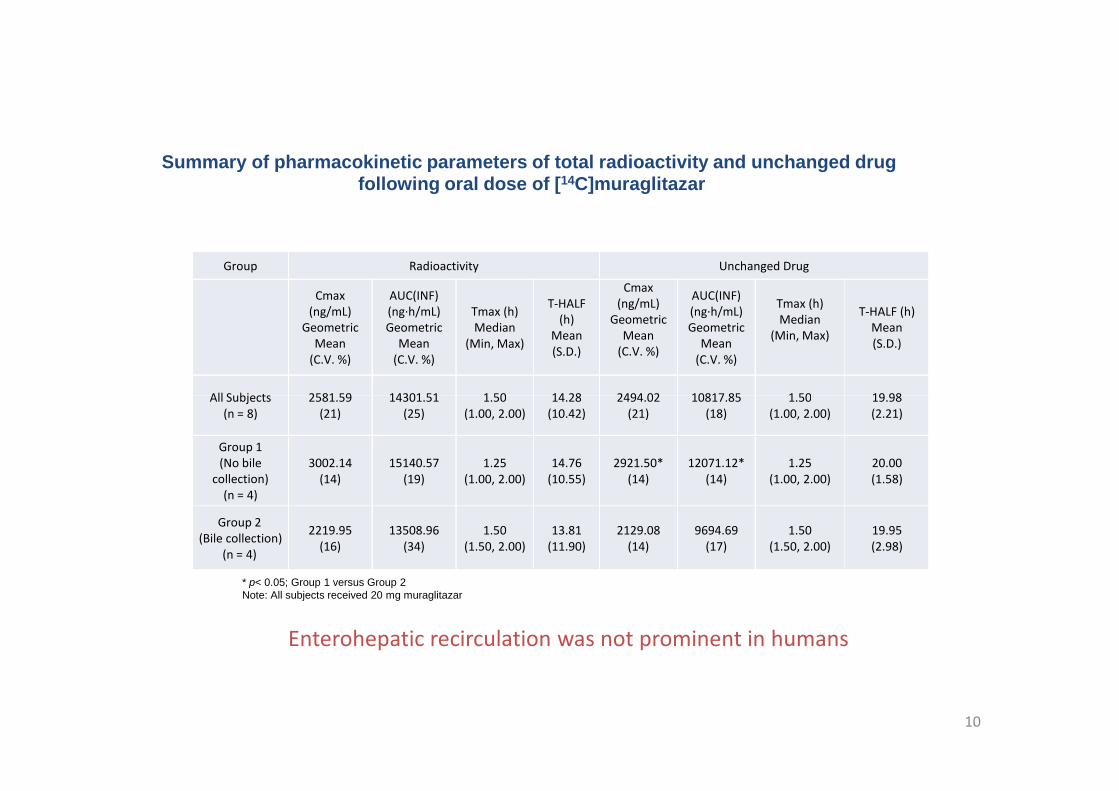
Group Radioactivity Unchanged Drug
Cmax(ng/mL)
GeometricMean
(C.V. %)
AUC(INF)(ng·h/mL)Geometric
Mean(C.V. %)
Tmax (h)Median
(Min, Max)
T-HALF(h)
Mean(S.D.)
Cmax(ng/mL)
GeometricMean
(C.V. %)
AUC(INF)(ng·h/mL)Geometric
Mean(C.V. %)
Tmax (h)Median
(Min, Max)
T-HALF (h)Mean(S.D.)
All Subjects 2581.59 14301.51 1.50 14.28 2494.02 10817.85 1.50 19.98
Summary of pharmacokinetic parameters of total radioactivity and unchanged drugfollowing oral dose of [14C]muraglitazar
10
All Subjects(n = 8)
2581.59(21)
14301.51(25)
1.50(1.00, 2.00)
14.28(10.42)
2494.02(21)
10817.85(18)
1.50(1.00, 2.00)
19.98(2.21)
Group 1(No bile
collection)(n = 4)
3002.14(14)
15140.57(19)
1.25(1.00, 2.00)
14.76(10.55)
2921.50*(14)
12071.12*(14)
1.25(1.00, 2.00)
20.00(1.58)
Group 2(Bile collection)
(n = 4)
2219.95(16)
13508.96(34)
1.50(1.50, 2.00)
13.81(11.90)
2129.08(14)
9694.69(17)
1.50(1.50, 2.00)
19.95(2.98)
Enterohepatic recirculation was not prominent in humans
* p< 0.05; Group 1 versus Group 2Note: All subjects received 20 mg muraglitazar
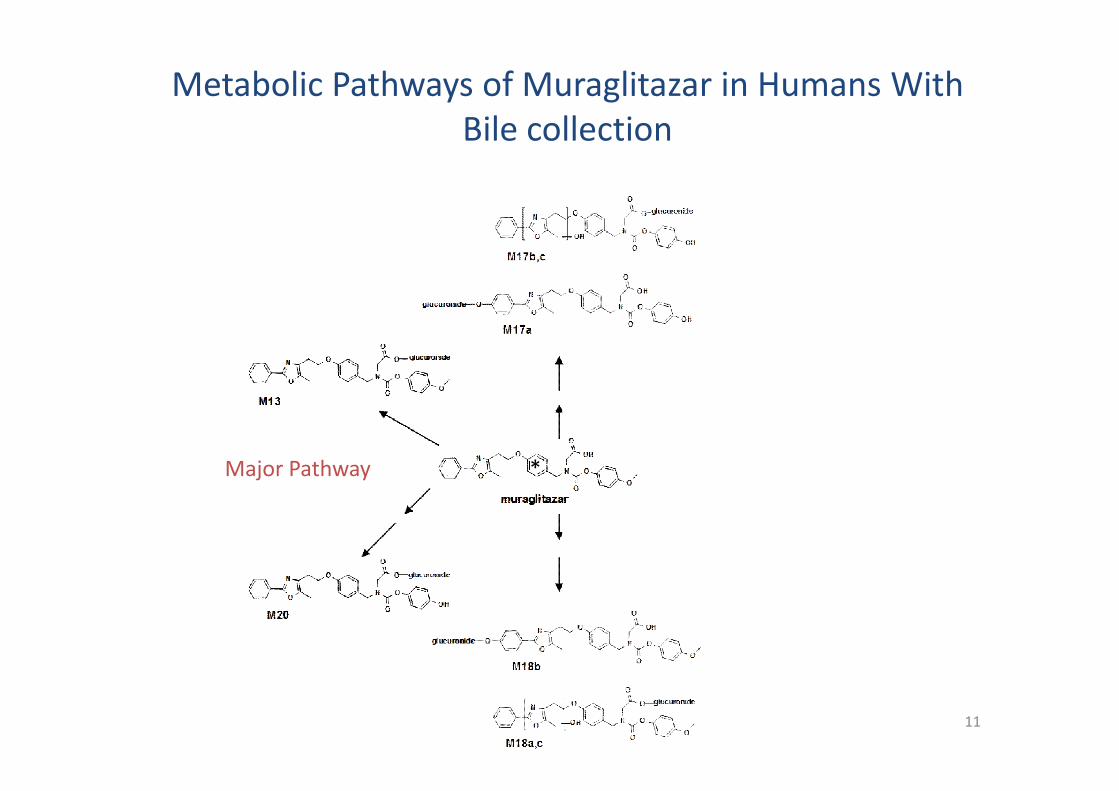
Metabolic Pathways of Muraglitazar in Humans WithBile collection
11
Major Pathway *
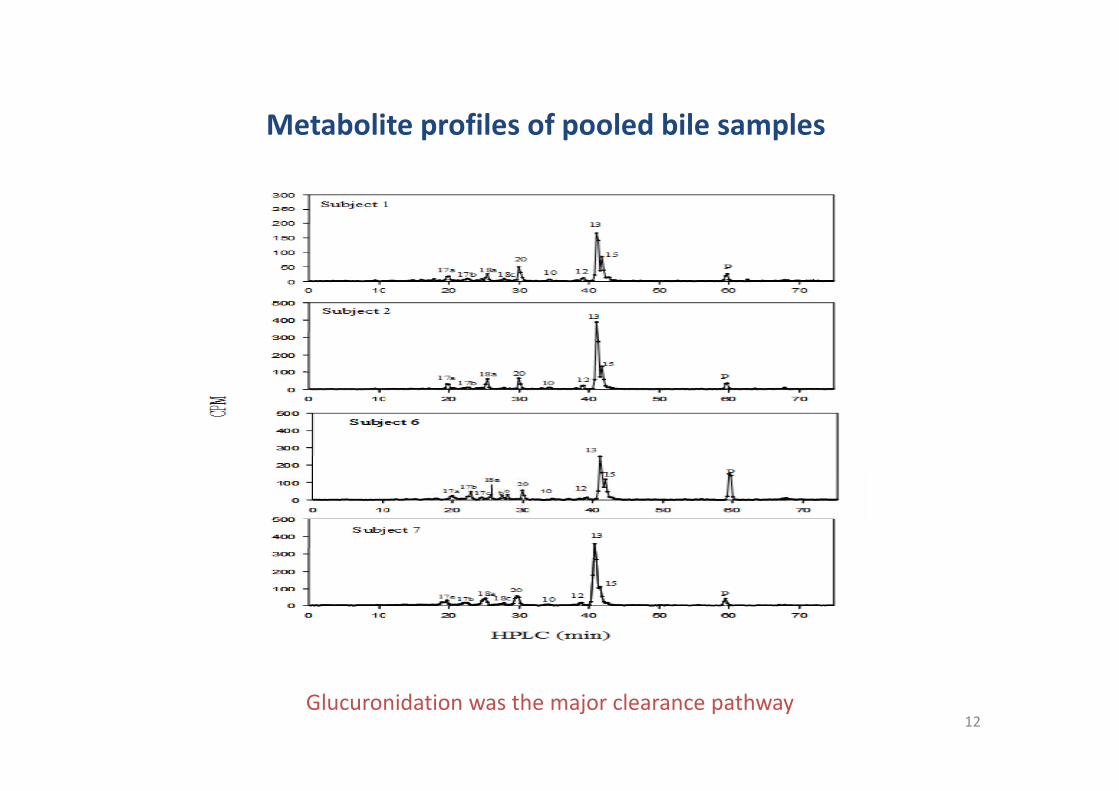
Metabolite profiles of pooled bile samples
12Glucuronidation was the major clearance pathway

No Glucuronide was identified in radioactivity profiles of pooled fecal homogenate
All are oxidative metabolites
13
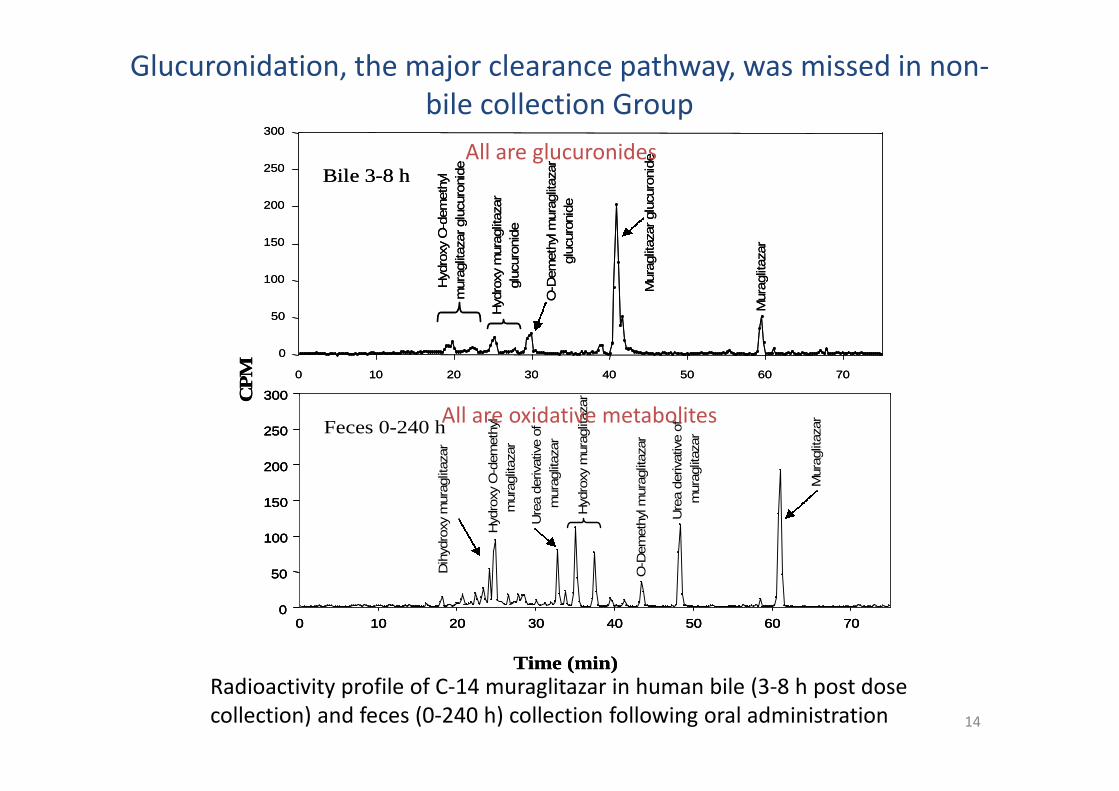
Glucuronidation, the major clearance pathway, was missed in non-bile collection Group
300CP
M 0 10 20 30 40 50 60 70
0
50
100
150
200
250
300
Bile 3-8 h
Mura
glit
aza
rglu
curo
nid
e
Mura
glit
aza
r
O-D
em
eth
ylm
ura
glit
aza
r
glu
curo
nid
e
Hyd
roxy
O-d
em
eth
yl
mura
glit
aza
rglu
curo
nid
e
Hyd
roxy
mura
glit
aza
r
glu
curo
nid
e
mura
glit
aza
r300300CP
M 0 10 20 30 40 50 60 70
0
50
100
150
200
250
300
Bile 3-8 h
Mura
glit
aza
rglu
curo
nid
e
Mura
glit
aza
r
O-D
em
eth
ylm
ura
glit
aza
r
glu
curo
nid
e
Hyd
roxy
O-d
em
eth
yl
mura
glit
aza
rglu
curo
nid
e
Hyd
roxy
mura
glit
aza
r
glu
curo
nid
e
mura
glit
aza
r
All are glucuronides
14
0 10 20 30 40 50 60 700
50
100
150
200
250
300
Feces 0-240 h
Time (min)
CP
M
Mura
glit
aza
r
Ure
aderiva
tive
of
mura
glit
aza
r
Ure
aderiva
tive
of
mura
glit
aza
r
Hyd
roxy
mura
glit
aza
r
O-D
em
eth
ylm
ura
glit
aza
r
Hyd
roxy
O-d
em
eth
yl
mura
glit
aza
r
Dih
ydro
xym
ura
glit
aza
r
0 10 20 30 40 50 60 700
50
100
150
200
250
300
Feces 0-240 h
0 10 20 30 40 50 60 700
50
100
150
200
250
300
Feces 0-240 h
Time (min)
CP
M
Mura
glit
aza
r
Ure
aderiva
tive
of
mura
glit
aza
r
Ure
aderiva
tive
of
mura
glit
aza
r
Hyd
roxy
mura
glit
aza
r
O-D
em
eth
ylm
ura
glit
aza
r
Hyd
roxy
O-d
em
eth
yl
mura
glit
aza
r
Dih
ydro
xym
ura
glit
aza
r
Radioactivity profile of C-14 muraglitazar in human bile (3-8 h post dosecollection) and feces (0-240 h) collection following oral administration
All are oxidative metabolites
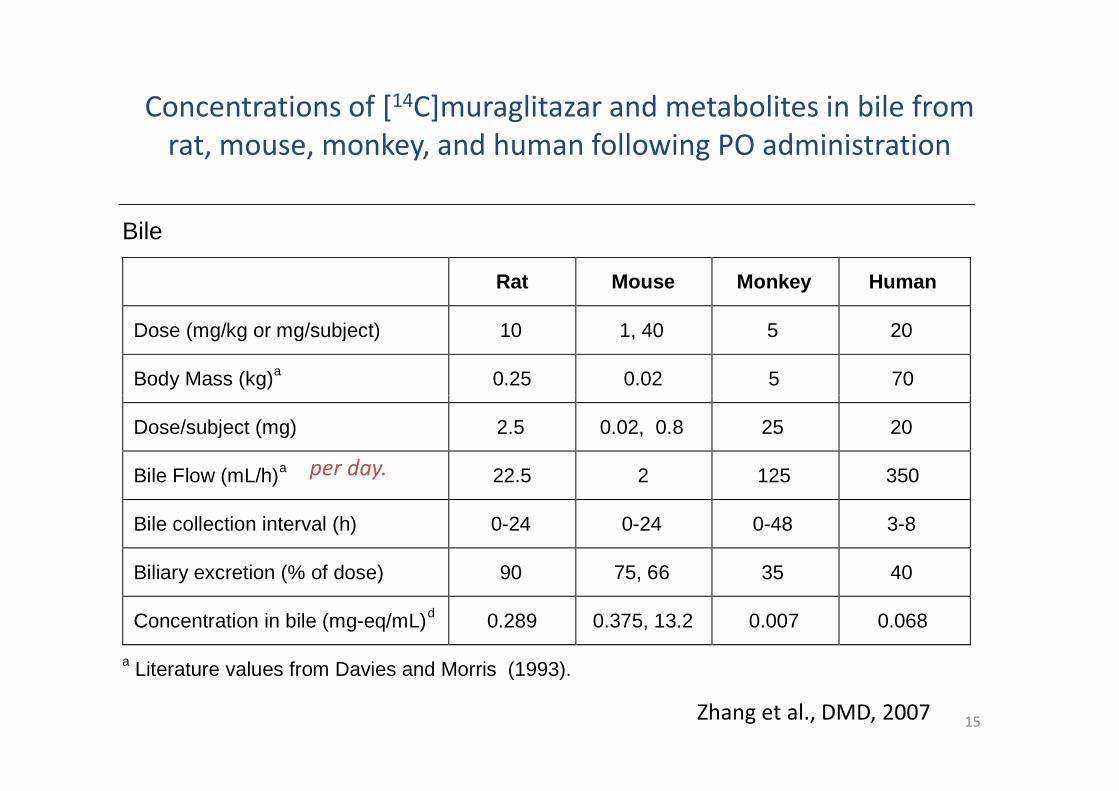
Concentrations of [14C]muraglitazar and metabolites in bile fromrat, mouse, monkey, and human following PO administration
Bile
Rat Mouse Monkey Human
Dose (mg/kg or mg/subject) 10 1, 40 5 20
Body Mass (kg)a
0.25 0.02 5 70
15
Dose/subject (mg) 2.5 0.02, 0.8 25 20
Bile Flow (mL/h)a
22.5 2 125 350
Bile collection interval (h) 0-24 0-24 0-48 3-8
Biliary excretion (% of dose) 90 75, 66 35 40
Concentration in bile (mg-eq/mL)d
0.289 0.375, 13.2 0.007 0.068
aLiterature values from Davies and Morris (1993).
Zhang et al., DMD, 2007
per day.
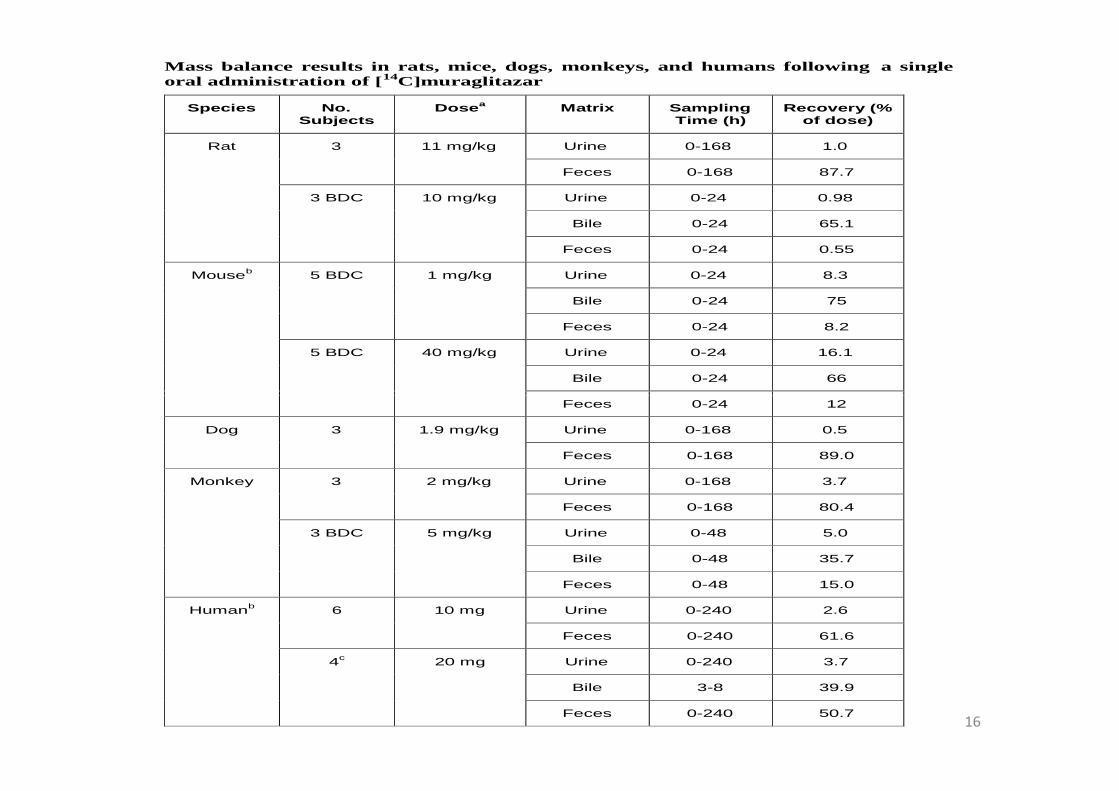
Mass balance results in rats, mice, dogs, monkeys, and humans following a singleoral administration of [14C]muraglitazar
Species No.Subjects
Dosea Matrix SamplingTime (h)
Recovery (%of dose)
Rat 3 11 mg/kg Urine 0-168 1.0
Feces 0-168 87.7
3 BDC 10 mg/kg Urine 0-24 0.98
Bile 0-24 65.1
Feces 0-24 0.55
Mouseb
5 BDC 1 mg/kg Urine 0-24 8.3
Bile 0-24 75
Feces 0-24 8.2
5 BDC 40 mg/kg Urine 0-24 16.1
Bile 0-24 66
16
Feces 0-24 12
Dog 3 1.9 mg/kg Urine 0-168 0.5
Feces 0-168 89.0
Monkey 3 2 mg/kg Urine 0-168 3.7
Feces 0-168 80.4
3 BDC 5 mg/kg Urine 0-48 5.0
Bile 0-48 35.7
Feces 0-48 15.0
Humanb
6 10 mg Urine 0-240 2.6
Feces 0-240 61.6
4c
20 mg Urine 0-240 3.7
Bile 3-8 39.9
Feces 0-240 50.7
0
2 0 0
4 0 0
6 0 0
8 0 0
1 0 0 0
0 . 0 0 1 0 . 0 0 2 0 . 0 0 3 0 . 0 0 4 0 . 0 0 5 0 . 0 0 6 0 . 0 0 7 0 . 0 0
8 0 0 0
P1 3
1 5
2 0
1 8 a , b , c1 7 a , b , c
R a t
M o n k e y
0
2 0 0
4 0 0
6 0 0
8 0 0
1 0 0 0
0 . 0 0 1 0 . 0 0 2 0 . 0 0 3 0 . 0 0 4 0 . 0 0 5 0 . 0 0 6 0 . 0 0 7 0 . 0 0
8 0 0 0
P1 3
1 5
2 0
1 8 a , b , c1 7 a , b , c
R a t
M o n k e y
8 0 0 0
P1 3
1 5
2 0
1 8 a , b , c1 7 a , b , c
R a t
M o n k e y
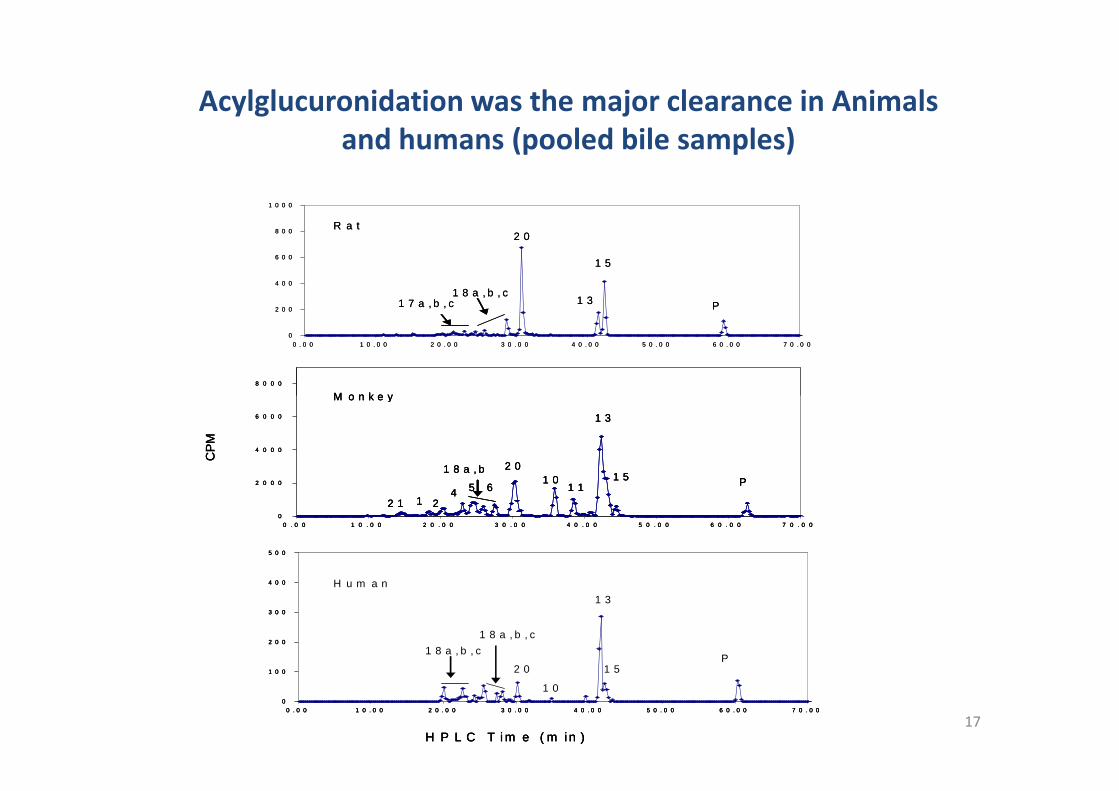
Acylglucuronidation was the major clearance in Animalsand humans (pooled bile samples)
17
0
2 0 0 0
4 0 0 0
6 0 0 0
0 . 0 0 1 0 . 0 0 2 0 . 0 0 3 0 . 0 0 4 0 . 0 0 5 0 . 0 0 6 0 . 0 0 7 0 . 0 0
0
1 0 0
2 0 0
3 0 0
4 0 0
5 0 0
0 . 0 0 1 0 . 0 0 2 0 . 0 0 3 0 . 0 0 4 0 . 0 0 5 0 . 0 0 6 0 . 0 0 7 0 . 0 0
P
P
1 3
1 3
1 5
1 5
2 0
2 0
1 8 a , b , c
1 8 a , b , c
1 0
1 8 a , b1 0
1 1
2 1 1
6
24 5
H P L C T i m e ( m in )
CP
M
M o n k e y
H u m a n
0
2 0 0 0
4 0 0 0
6 0 0 0
0 . 0 0 1 0 . 0 0 2 0 . 0 0 3 0 . 0 0 4 0 . 0 0 5 0 . 0 0 6 0 . 0 0 7 0 . 0 0
0
1 0 0
2 0 0
3 0 0
4 0 0
5 0 0
0 . 0 0 1 0 . 0 0 2 0 . 0 0 3 0 . 0 0 4 0 . 0 0 5 0 . 0 0 6 0 . 0 0 7 0 . 0 0
P
P
1 3
1 3
1 5
1 5
2 0
2 0
1 8 a , b , c
1 8 a , b , c
1 0
1 8 a , b1 0
1 1
2 1 1
6
24 5
H P L C T i m e ( m in )
CP
M
M o n k e y
H u m a n
0
2 0 0 0
4 0 0 0
6 0 0 0
0 . 0 0 1 0 . 0 0 2 0 . 0 0 3 0 . 0 0 4 0 . 0 0 5 0 . 0 0 6 0 . 0 0 7 0 . 0 0
0
1 0 0
2 0 0
3 0 0
4 0 0
5 0 0
0 . 0 0 1 0 . 0 0 2 0 . 0 0 3 0 . 0 0 4 0 . 0 0 5 0 . 0 0 6 0 . 0 0 7 0 . 0 0
P
P
1 3
1 3
1 5
1 5
2 0
2 0
1 8 a , b , c
1 8 a , b , c
1 0
1 8 a , b1 0
1 1
2 1 1
6
24 5
H P L C T i m e ( m in )
CP
M
M o n k e y
H u m a n
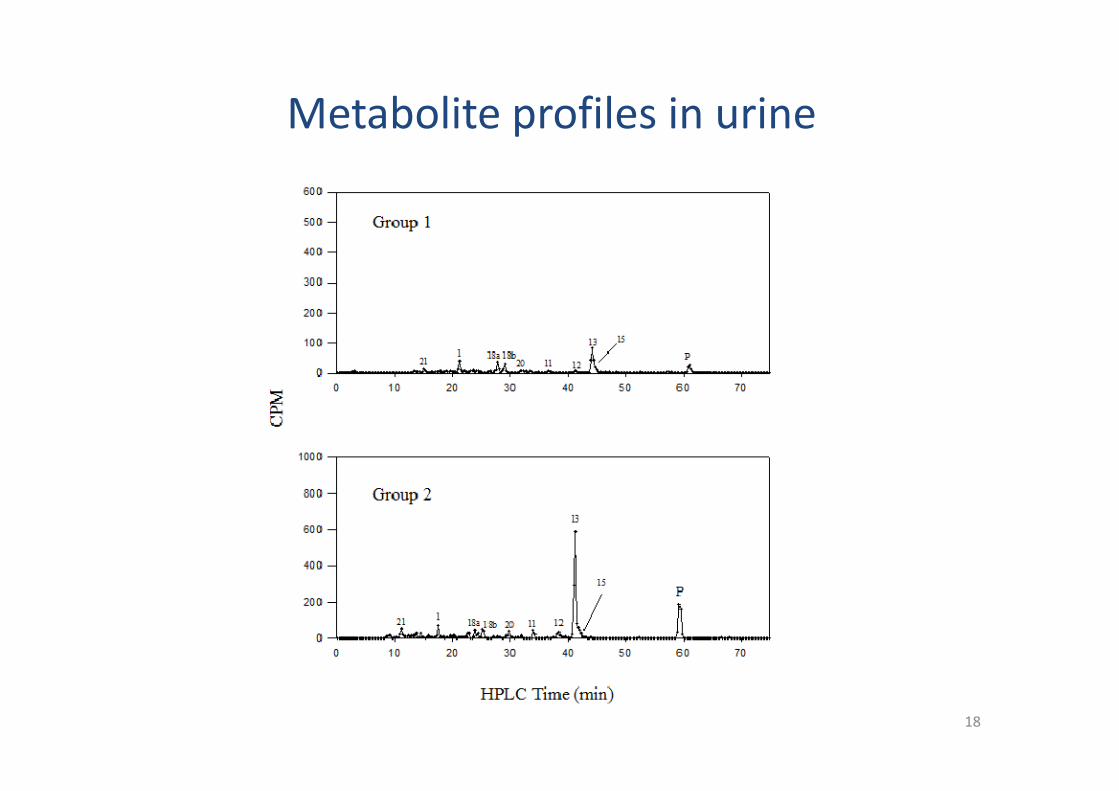
Metabolite profiles in urine
18
Utilities of Bile Data
• Biliary excretion data, in conjunction with urinary and fecal excretion data, to achieve amore thorough understanding of the ADME properties such as Fm determination.
– The metabolic profiles of fecal samples can be misleading: (1) acyl glucuronide, compounds that undergodirect glucuronidation in the liver and secretion in bile would be detected as aglycones but not asglucuronides in the fecal samples gut microbial hydrolysis. (2) N-oxides would likely undergo reduction inthe gut, and would be misinterpreted as unchanged parent compound in the feces. (3) For PO drugs,parent compound detected in feces could be the result of unabsorbed drug or systemic metabolitesexcreted in bile being converted back to the parent compound via gut microflora metabolism, confoundingthe interpretation of how much metabolism had occurred.
• The extent of human biliary excretion can aid in the planning for future clinical studies.(1) Hepatic impairment subjects (2) DDI based on the determined Fm.(1) Hepatic impairment subjects (2) DDI based on the determined Fm.
• Bile collection can be used to assess the extent of metabolism through conjugation orreactive metabolite(s) formation. These data suggested that the hydrolysis ofglucuronide metabolites by the gut microflora would have prevented accurateevaluation of the extent of glucuronidation in vivo.
• Biliary excretion studies can also help determine potential enterohepatic recirculation.
19
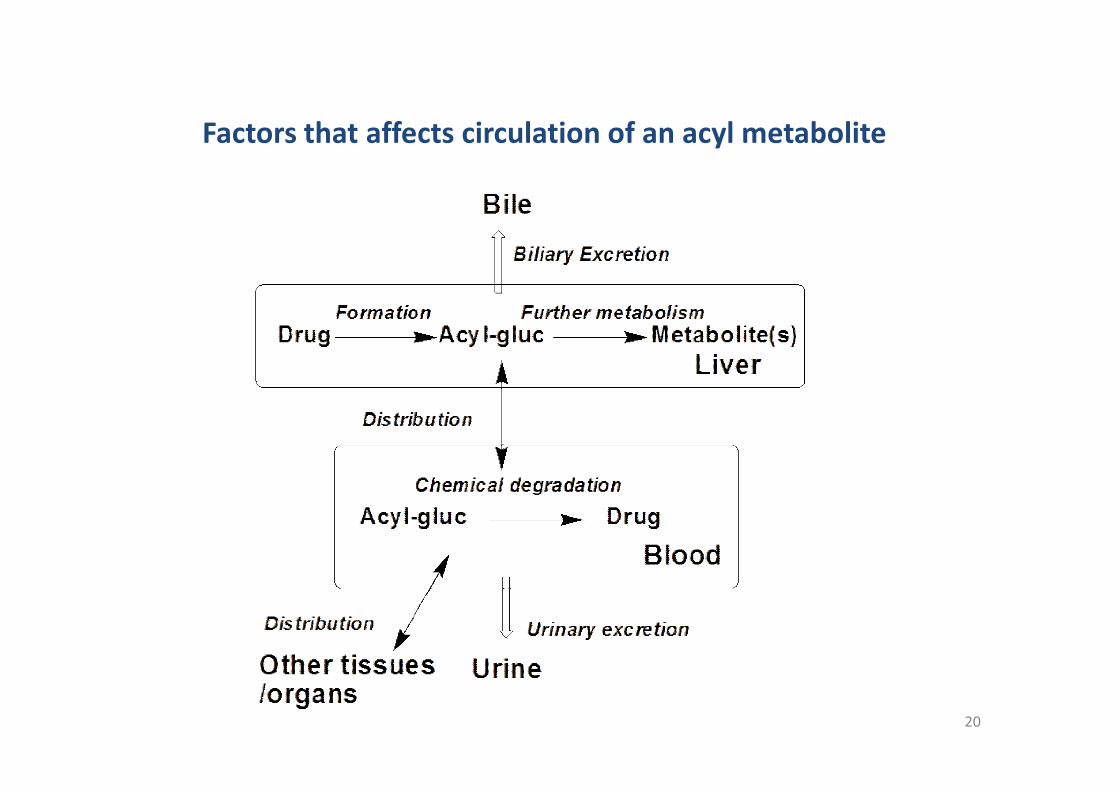
Factors that affects circulation of an acyl metabolite
20
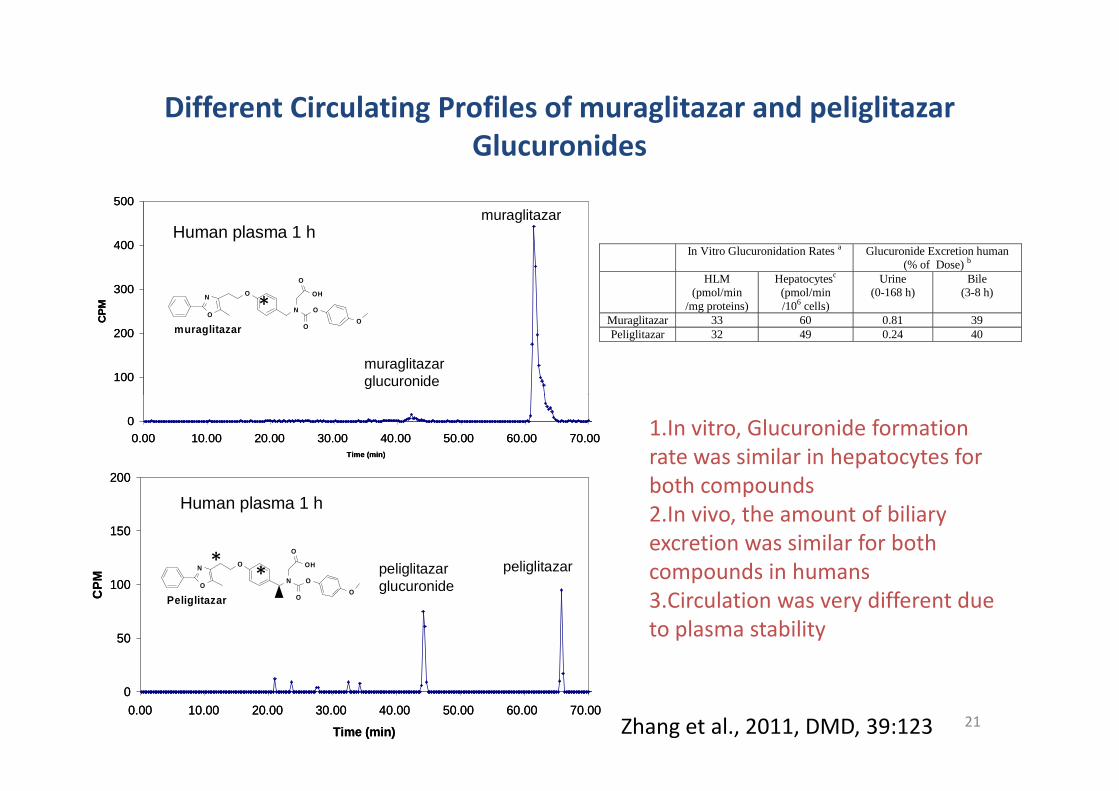
Different Circulating Profiles of muraglitazar and peliglitazarGlucuronides
100
200
300
400
500
CP
M
muraglitazarglucuronide
muraglitazarHuman plasma 1 h
O
NO
N
OH
O
O
OOmuraglitazar
100
200
300
400
500
CP
M
muraglitazarglucuronide
muraglitazarHuman plasma 1 h
O
NO
N
OH
O
O
OOmuraglitazar
In Vitro Glucuronidation Rates a Glucuronide Excretion human(% of Dose) b
HLM(pmol/min
/mg proteins)
Hepatocytesc
(pmol/min/106 cells)
Urine(0-168 h)
Bile(3-8 h)
Muraglitazar 33 60 0.81 39Peliglitazar 32 49 0.24 40
*
21
0
0.00 10.00 20.00 30.00 40.00 50.00 60.00 70.00
Time (min)
0
50
100
150
200
0.00 10.00 20.00 30.00 40.00 50.00 60.00 70.00
Time (min)
CP
M
peliglitazarglucuronide
peliglitazar
Human plasma 1 h
O
NO
N
OH
O
O
OOPeliglitazar
0
0.00 10.00 20.00 30.00 40.00 50.00 60.00 70.00
Time (min)
0
50
100
150
200
0.00 10.00 20.00 30.00 40.00 50.00 60.00 70.00
Time (min)
CP
M
peliglitazarglucuronide
peliglitazar
Human plasma 1 h
O
NO
N
OH
O
O
OOPeliglitazar
1.In vitro, Glucuronide formationrate was similar in hepatocytes forboth compounds2.In vivo, the amount of biliaryexcretion was similar for bothcompounds in humans3.Circulation was very different dueto plasma stability
Zhang et al., 2011, DMD, 39:123
**
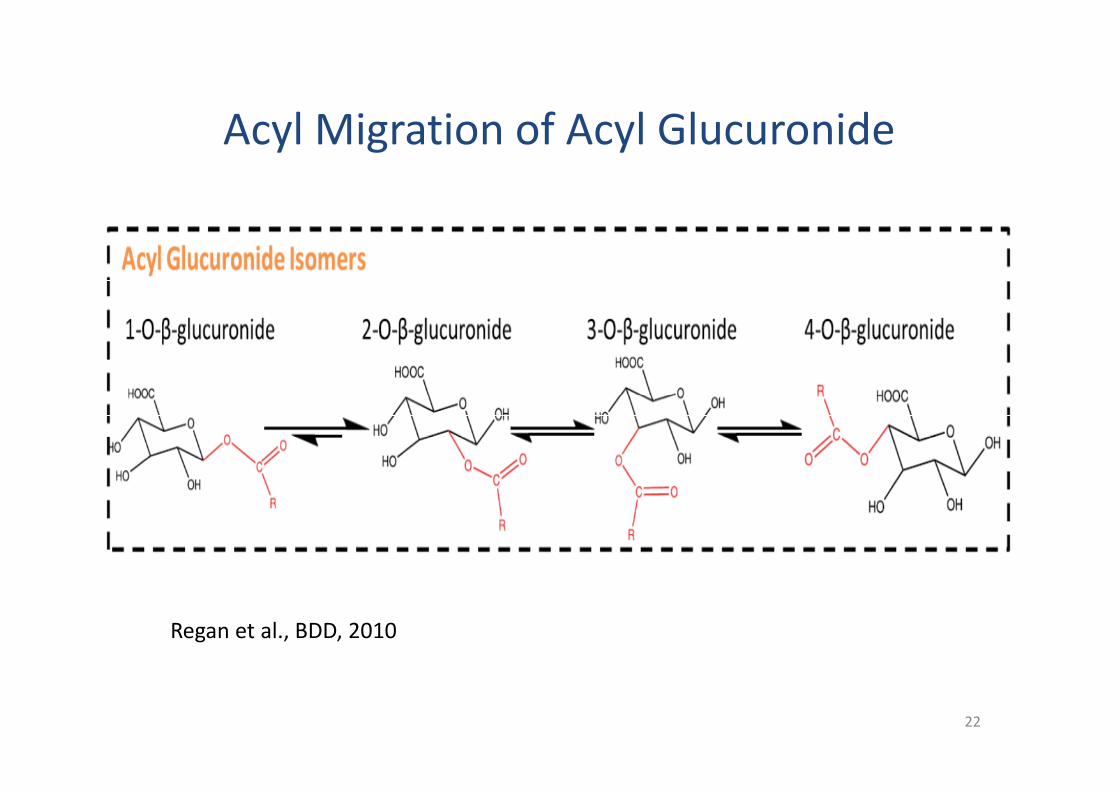
Acyl Migration of Acyl Glucuronide
22
Regan et al., BDD, 2010
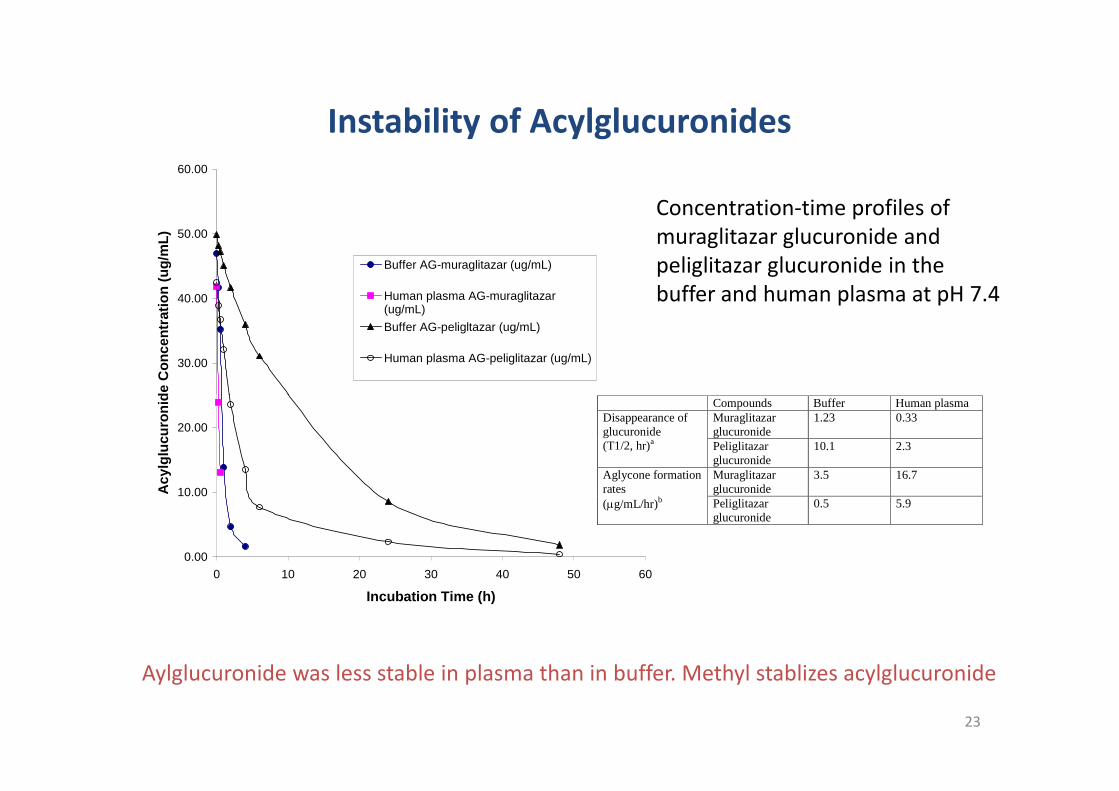
Instability of Acylglucuronides
30.00
40.00
50.00
60.00A
cy
lglu
cu
ron
ide
Co
nc
en
trati
on
(ug
/mL
)
Buffer AG-muraglitazar (ug/mL)
Human plasma AG-muraglitazar(ug/mL)
Buffer AG-peligltazar (ug/mL)
Human plasma AG-peliglitazar (ug/mL)
Concentration-time profiles ofmuraglitazar glucuronide andpeliglitazar glucuronide in thebuffer and human plasma at pH 7.4
23
0.00
10.00
20.00
0 10 20 30 40 50 60
Incubation Time (h)
Ac
ylg
lucu
ron
ide
Co
nc
en
trati
on
(ug
/mL
)
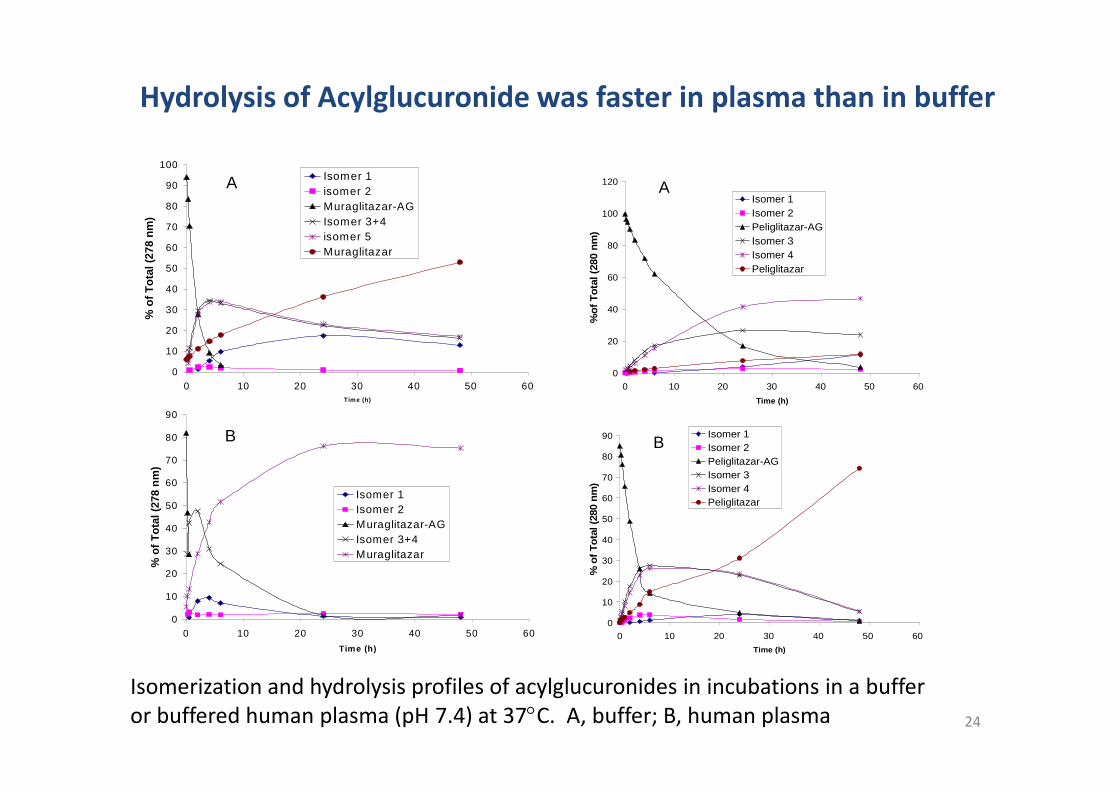
Aylglucuronide was less stable in plasma than in buffer. Methyl stablizes acylglucuronide
Compounds Buffer Human plasmaDisappearance ofglucuronide(T1/2, hr)a
Muraglitazarglucuronide
1.23 0.33
Peliglitazarglucuronide
10.1 2.3
Aglycone formationrates(g/mL/hr)b
Muraglitazarglucuronide
3.5 16.7
Peliglitazarglucuronide
0.5 5.9
0
10
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60
%o
fT
ota
l(2
78
nm
)
Isomer 1
isomer 2
Muraglitazar-AG
Isomer 3+4
isomer 5
Muraglitazar
A
Hydrolysis of Acylglucuronide was faster in plasma than in buffer
0
20
40
60
80
100
120
0 10 20 30 40 50 60
%o
fT
ota
l(2
80
nm
)
Isomer 1
Isomer 2
Peliglitazar-AG
Isomer 3
Isomer 4
Peliglitazar
A
24
Time (h)
0
10
20
30
40
50
60
70
80
90
0 10 20 30 40 50 60
Time (h)
%o
fT
ota
l(2
78
nm
)
Isomer 1
Isomer 2
Muraglitazar-AG
Isomer 3+4
Muraglitazar
B
Isomerization and hydrolysis profiles of acylglucuronides in incubations in a bufferor buffered human plasma (pH 7.4) at 37C. A, buffer; B, human plasma
Time (h)
0
10
20
30
40
50
60
70
80
90
0 10 20 30 40 50 60
Time (h)
%o
fT
ota
l(2
80
nm
)
Isomer 1
Isomer 2
Peliglitazar-AG
Isomer 3
Isomer 4
Peliglitazar
B
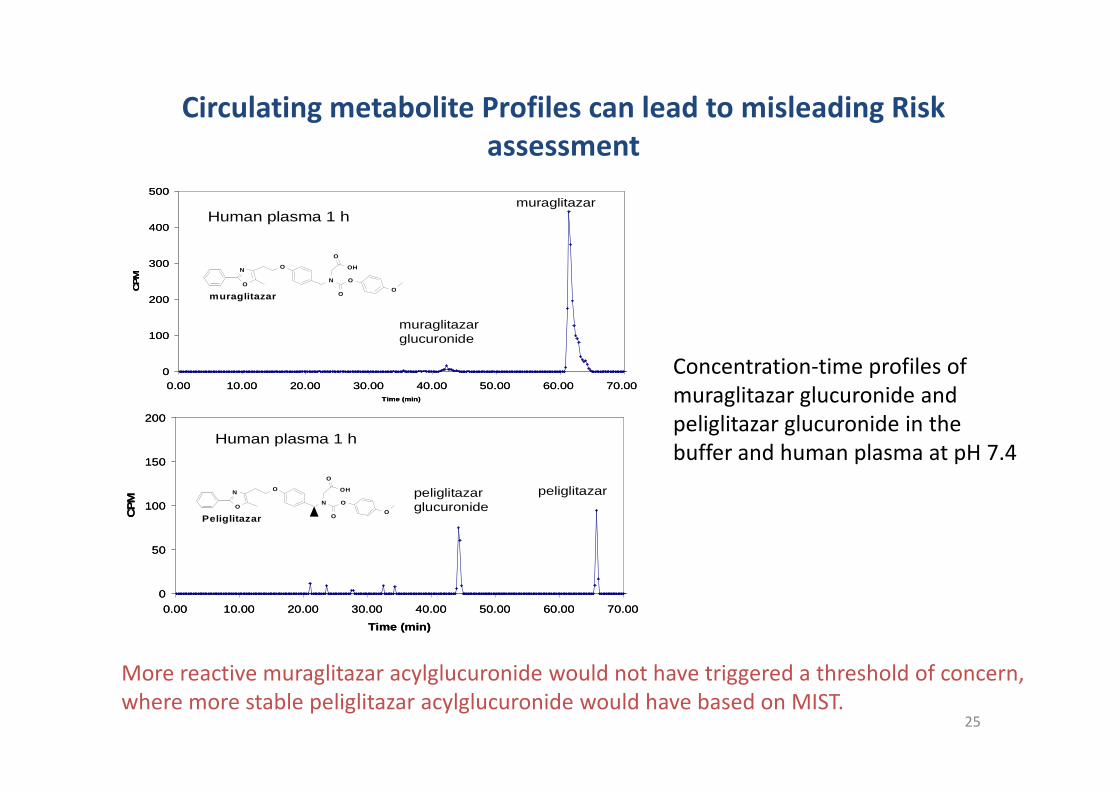
Circulating metabolite Profiles can lead to misleading Riskassessment
0
100
200
300
400
500
0.00 10.00 20.00 30.00 40.00 50.00 60.00 70.00
CPM
muraglitazarglucuronide
muraglitazarHuman plasma 1 h
O
NO
N
OH
O
O
OOmuraglitazar
0
100
200
300
400
500
0.00 10.00 20.00 30.00 40.00 50.00 60.00 70.00
CPM
muraglitazarglucuronide
muraglitazarHuman plasma 1 h
O
NO
N
OH
O
O
OOmuraglitazar
Concentration-time profiles ofmuraglitazar glucuronide and
25
Time (min)
0
50
100
150
200
0.00 10.00 20.00 30.00 40.00 50.00 60.00 70.00
Time (min)
CP
M
peliglitazarglucuronide
peliglitazar
Human plasma 1 h
O
NO
N
OH
O
O
OOPeliglitazar
Time (min)
0
50
100
150
200
0.00 10.00 20.00 30.00 40.00 50.00 60.00 70.00
Time (min)
CP
M
peliglitazarglucuronide
peliglitazar
Human plasma 1 h
O
NO
N
OH
O
O
OOPeliglitazar
muraglitazar glucuronide andpeliglitazar glucuronide in thebuffer and human plasma at pH 7.4
More reactive muraglitazar acylglucuronide would not have triggered a threshold of concern,where more stable peliglitazar acylglucuronide would have based on MIST.
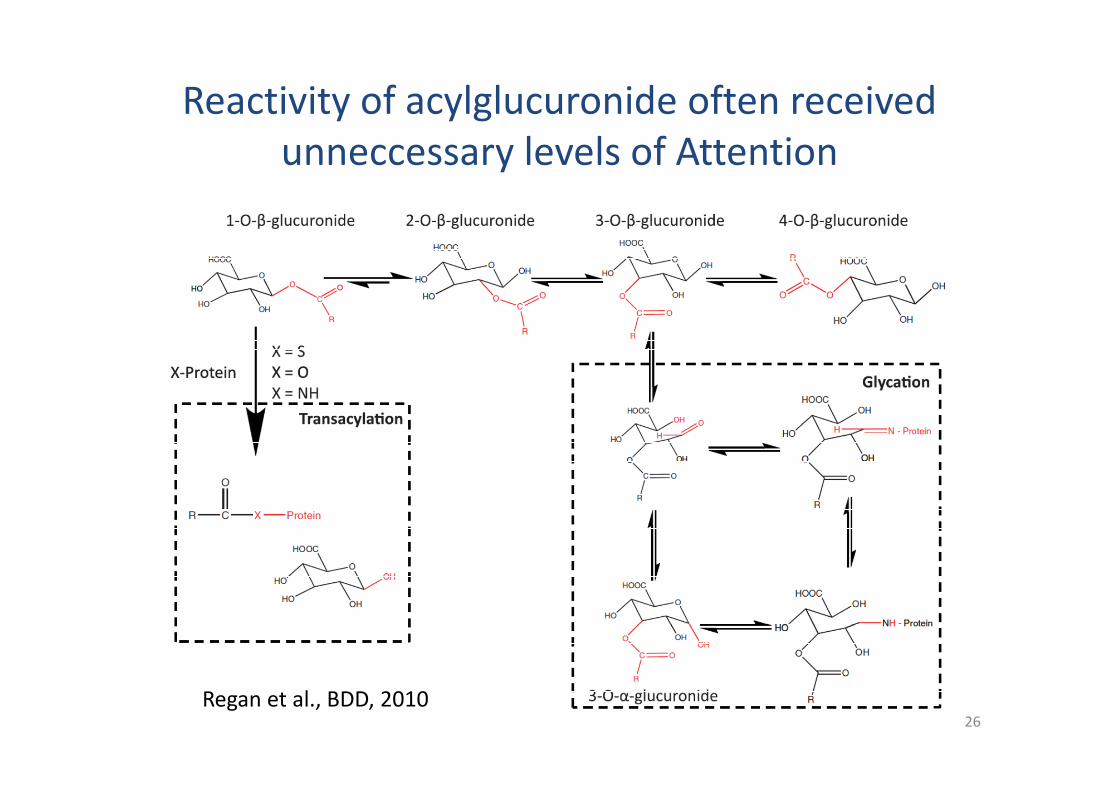
Reactivity of acylglucuronide often receivedunneccessary levels of Attention
26
Regan et al., BDD, 2010
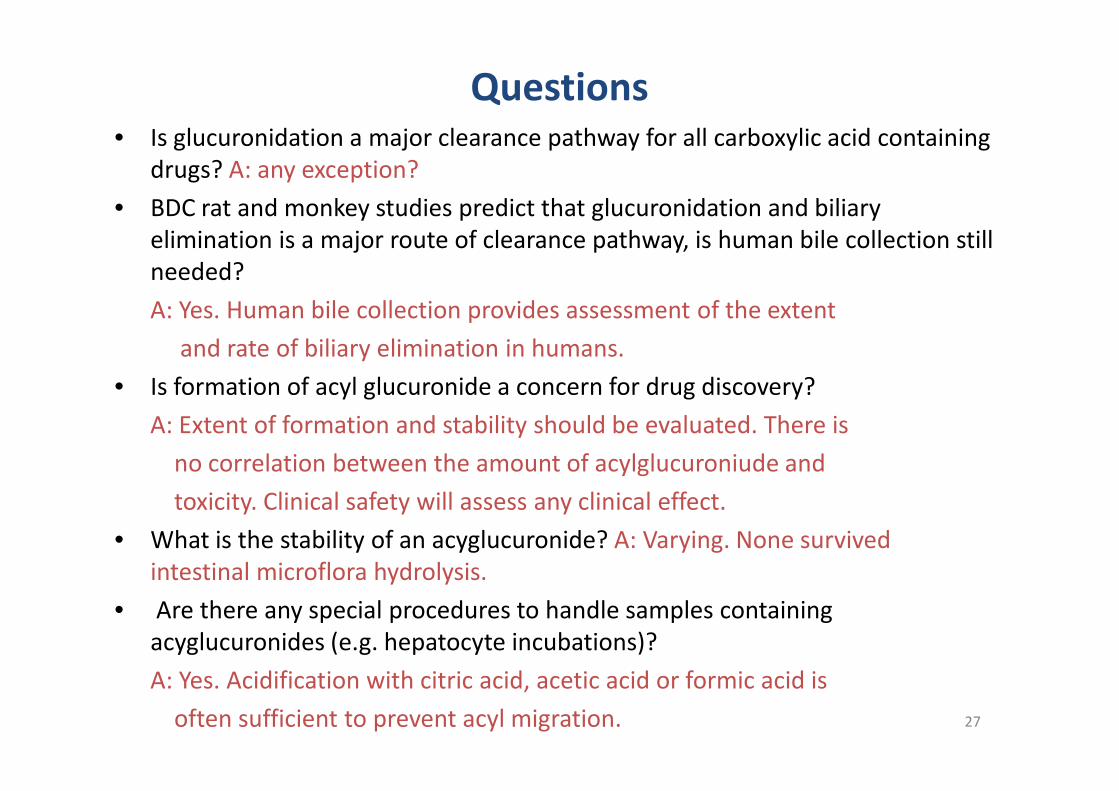
Questions• Is glucuronidation a major clearance pathway for all carboxylic acid containing
drugs? A: any exception?
• BDC rat and monkey studies predict that glucuronidation and biliaryelimination is a major route of clearance pathway, is human bile collection stillneeded?
A: Yes. Human bile collection provides assessment of the extent
and rate of biliary elimination in humans.
• Is formation of acyl glucuronide a concern for drug discovery?• Is formation of acyl glucuronide a concern for drug discovery?
A: Extent of formation and stability should be evaluated. There is
no correlation between the amount of acylglucuroniude and
toxicity. Clinical safety will assess any clinical effect.
• What is the stability of an acyglucuronide? A: Varying. None survivedintestinal microflora hydrolysis.
• Are there any special procedures to handle samples containingacyglucuronides (e.g. hepatocyte incubations)?
A: Yes. Acidification with citric acid, acetic acid or formic acid is
often sufficient to prevent acyl migration. 27
Summary• Human bile collection indicates that glucuronidation was the
major clearance pathway for the carboxylic acid-containingdrugs. The major clearance pathway would have been missedwithout bile collection.
• Bile collection help assess the extent of formation of thereactive metabolites.
• Acylglucuronides are not stable. Their circulation depends on• Acylglucuronides are not stable. Their circulation depends ontheir plasma stability. Acylglucuronide circulating profiles canmislead risk assessment based on MIST.
• Bile collection supports hepatic impairment study andprecludes P450 clinical DDI that would have been suggestedfrom fecal metabolite profile of subjects without bilecollection.
28
ReferencesBalani SK, Xu X, Pratha V, Koss MA, Amin RD, Dufresne C, Miller RR, ArisonBH, Doss GA, Chiba M, Freeman A, Holland SD, Schwartz JI, Lasseter K, GertzB, Isenberg JI, Rogers JD, Lin JH, and Baillie TA (1997) Metabolic profiles ofmontelukast sodium (Singulair), a potent leukotriene 1 receptor antagonist, inhuman plasma and bile. Drug Metab Disp 25:1282-1287.
Guiney WJ, Beaumont C, and Thomas SR (2010) Use of the Entero-Test®, anovel approach for the non-invasive capture of biliary metabolites in dogs. DrugMetab Dispos. 38:851-856.
Ghibellini G, Leslie EL, and Brouwer KLR (2006) Methods To Evaluate BiliaryExcretion of Drugs in Humans: An Updated Review. Mol Pharma 3: 198-211.
Raghavan N, Frost C, Yu Z, He K, Zhang H, Humphreys W, Pinto D, Chen S,Bonacorsi S, Wong P, Zhang D (2009) Apixaban metabolism andpharmacokinetics after oral administration to humans. Drug Metab Dispos 37:74-81.
Regan SL, Maggs JL, Hammond TG, Lambert C, Wiliams DP, Park BK (2010)
29
Regan SL, Maggs JL, Hammond TG, Lambert C, Wiliams DP, Park BK (2010)
Acyl glucuronides: The good, the bad and the ugly. Biopharm Drug Dispos 31:
367-395.
Wang L, Zhang D, Swaminathan A, Xue Y, Cheng PT, Wu S, Mosqueda-GarciaR, Aurang C, Everett DW, and Humphreys WG (2006) Glucuronidation as amajor clearance pathway of muraglitazar in humans: Different metabolic profilesin subjects with and without bile collection. Drug Metab Dispos 34: 427-439.
Zhang D, Wang L, Raghavan N, Zhang H, Li W, Cheng PT, Yao M, Zhang L, ZhuM, Bonacorsi S, Mitroka J, Hariharan N, Hosagrahara V, Chandrasena, Shyu W,and Humphreys GW (2007) Comparative metabolism of radiolabeledmuraglitazar in animals and humans by quantitative and qualitative metaboliteprofiling. Drug Metab Dispos 35: 150-167.
Zhang D, Raghavan N, Wang L, Xue Y, Obermeier M, Chen S, Tao S, Zhang H,
Cheng PT, Li W, Ramanathan R, Yang Z, Humphreys WG (2011) Plasma
stability-dependent circulation of acyl glucuronide metabolites in humans: how
circulating metabolite profiles of muraglitazar and peliglitazar can lead to
misleading risk assessment. Drug Metab Dispos 39: 123-131.
Acknowledgement
BMS
•Lifei Wang
•Nirmala Raghavan
•Griff Humphreys
Genentech
30
Genentech
•Cyrus Khojasteh
•Cornelis E.C.A. Hop