2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT

of 36
-
Upload
christine-chambers -
Category
Documents
-
view
219 -
download
0
Transcript of 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
1/36
Accepted Manuscript
Perspectives on Treatment for Nonalcoholic Steatohepatitis
Guillaume Lassailly, Robert Caiazzo, François Pattou, Philippe Mathurin
PII: S0016-5085(16)00323-1
DOI: 10.1053/j.gastro.2016.03.004
Reference: YGAST 60356
To appear in: Gastroenterology Accepted Date: 8 March 2016
Please cite this article as: Lassailly G, Caiazzo R, Pattou F, Mathurin P, Perspectives on Treatment for
Nonalcoholic Steatohepatitis,Gastroenterology (2016), doi: 10.1053/j.gastro.2016.03.004.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to
our customers we are providing this early version of the manuscript. The manuscript will undergo
copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please
note that during the production process errors may be discovered which could affect the content, and all
legal disclaimers that apply to the journal pertain.
http://dx.doi.org/10.1053/j.gastro.2016.03.004
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
2/36
ACCEPTED MANUSCRIPT
Perspectives on Treatment for Nonalcoholic Steatohepatitis
Guillaume Lassailly1,2,3
, Robert Caiazzo4,5,6
, François Pattou4,5,6
, and Philippe Mathurin1,2,3*
.
1. Univ. Lille, U995 - LIRIC - Lille Inflammation Research International Center, F-
59000 Lille, France
2. Inserm, U995, F-59000 Lille, France
3. CHRU Lille, Service des Maladies de l’appareil digestif
4. Univ. Lille, U1190, EGID, F-59000 Lille, France
5. Inserm, U1190, F-59000 Lille, France
6.
CHRU Lille, Service de chirurgie endocrinienne
*Corresponding author:
Prof. Philippe Mathurin
2 rue Michel Polonovski
59037, Lille CEDEX
France
Phone : 03 20 44 53 21Email : [email protected]
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
3/36
ACCEPTED MANUSCRIPT
Abstract
It is important to provide treatment to patients with nonalcoholic steatohepatitis (NASH)
because one third of patients with the metabolic syndrome die from liver disease. Basic
research studies have elucidated mechanisms of NASH pathogenesis, which could lead to
therapeutic targets. Health agencies have confirmed strategies for the optimal management of
NASH and approved new drugs and treatments, which are urgently needed. The United States
Food and Drug Administration recently endorsed endpoints for NASH therapy. The reversal
of NASH with no evidence of progression to advanced fibrosis has been defined as the
endpoint for phase 2b and phase 3 trials in patients with NASH and early-stage fibrosis.
Although a decrease in the non-alcoholic fatty liver disease activity score could serve as an
endpoint in clinical trials, it is not clear whether patients with lower scores have a lower risk
of progression to advanced fibrosis. Endpoints for clinical trials of patients with NASH
cirrhosis are currently based on model for end-stage liver disease and Child-Pugh-Turcotte
scores, as well as the hepatic venous pressure gradient. Different strategies are being explored
to reduce liver diseases that are linked to a sedentary lifestyle, overeating, and genetic factors.
In association with insulin resistance and deregulation of the lipid metabolism (accumulation
of lipotoxins that promote hepatic lipogenesis, adipose tissue lipolysis, and impaired β-
oxidation), these factors could increase the risk of liver steatosis with necroinflammatory
lesions and fibrosis. We review the pathogenic mechanisms of NASH and therapeutic options,
as well as strategies that are being developed for treatment of injury to the liver and other
organs.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
4/36
ACCEPTED MANUSCRIPT
The optimal treatment for non-alcoholic steatohepatitis (NASH) would reduce liver-related
mortality, metabolic comorbidities, and the risk of cardiovascular events. Research aimed at
achieving these goals has received a large amount of support because NASH has been
declared a public health issue by public health authorities. The endorsement of therapeutic
endpoints for NASH by the United States (US) Food and Drug Administration (FDA) was
important and facilitates development of new agents. The reversal or resolution of NASH,
defined as the disappearance of necroinflammatory features (hepatocyte ballooning and portal
inflammation) in histologic analysis, along with an absence of evidence for disease
progression to advanced fibrosis, has been recognized as the endpoint for phase 2b and phase
3 trials of patients with NASH and early-stage fibrosis1. Although a decrease in the non-
alcoholic fatty liver disease (NAFLD) activity score (NAS) could be used as an endpoint in
clinical trials, studies are needed to determine whether patients with lower scores have a
reduced risk for progression to advanced fibrosis. Endpoints for clinical trials of patients with
NASH and cirrhosis are currently based on model for end-stage liver disease and Child-Pugh-
Turcotte scores, as well as the hepatic venous pressure gradient1. These new approaches
provide a foundation to develop treatments for NAFLD.
New therapeutic targets must be identified that can lead to development of agents to
reduce disease progression in patients with NASH. To limit liver-related complications, these
agents should target 1 of the several pathways in the complex process of liver injury in
patients with NASH. These are likely to involve agents that modify the metabolic profile,
because accumulation of hepatic fat and liver injury are associated with insulin resistance2.
We review the roles of weight loss, insulin sensitization, lipid metabolism, oxidative stress,
fibrosis, inflammation and the intestinal microbiota in development and treatment of NASH.
Weight Loss
Diet and physical activity
Patients with NAFLD have a higher daily caloric intake and are more sedentary3 than those
without. The first step in the management of NASH is to obtain significant and sustained
weight loss by changing the patient’s lifestyle through diet and physical activity. Weight loss
increases hepatic and peripheral insulin sensitivity, reduces oxidative stress, and improves the
lipid profile. A restricted calorie diet rapidly decreases steatosis, improves insulin sensitivity,
and optimizes endogenous glucose synthesis4
.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
5/36
ACCEPTED MANUSCRIPT
Hepatic triglyceride content decreases with a weight loss of 3%–5%, but further
weight loss is necessary to reduce necroinflammation. Peripheral (skeletal muscle) insulin
resistance improves with more than 7%4 of weight loss. In randomized trials with consecutive
biopsies, a decrease in the necroinflammatory process was mainly observed in the subgroup
that lost at least 7%–9% of body weight.5, 6
However, this did not affect the progression of
fibrosis. A prospective study of 293 patients with NASH showed that 90% of steatosis
disappeared and fibrosis regressed in 45% of patients with a weight reduction >10%7. Weight
loss of >7%–9% should therefore be the goal to reduce necroinflammation, whereas weigh
loss >10% should be the goal to induce regression of fibrosis in patients with NASH.
On the other hand, further studies are necessary before specific diets can be
recommended for patients with NASH. Low-carbohydrate and Mediterranean diets seem to be
effective alternatives to low-fat diets, with different metabolic effects. Low-carbohydrate diets
have a more positive effect on lipids whereas the Mediterranean diet improves control of
glycemia8. The daily maximum amount of fructose or sucrose has not been confirmed,
although there is increasing evidence for their negative effects (especially high-fructose corn
syrup), including increased visceral adipose tissue, liver fat accumulation, and insulin
resistance. A pilot study in 15 patients indicated that diets can reduce histologic markers of
NASH. The prescribed diet included 40%–45% carbohydrates (especially complex
carbohydrates with fiber), 30%–40% fat (especially mono- and polyunsaturated fatty acids),
and 15%–20% protein9. The Mediterranean diet is rich in mono-unsaturated fatty acid and
was more effective than a low-fat, high-carbohydrate diet in increasing insulin sensitivity in a
randomized cross-over study of patients with NAFLD. However, this study did not perform
histologic analyses10
. A study is underway to evaluate the effects of the Mediterranean diet in
patients with NASH (NCT01894438).
Increased coffee consumption has been inversely associated with the risk of cirrhosis
or progression of fibrosis in patients at risk of liver disease, including NAFLD11-13. However
biases might have led to overestimates of coffee intake and risk of fibrosis progression.
Moreover, differences in coffee intake could reflect differences in socioeconomic status, or
exposure to other variables could affect fibrosis progression. Little is known about the
mechanisms by which coffee protects the liver, although a study an animal model of NASH
found that coffee reduced the amount of fat in the liver, oxidative stress, and inflammation.
Although coffee consumption is not associated with increased cardiovascular mortality,14
not
enough data are available to recommend increased coffee intake for patients with NASH.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
6/36
ACCEPTED MANUSCRIPT
Besides diet, lifestyle change includes physical activity. The American Heart
Association recommends aerobic resistance activities, including at least 150 minutes
(preferably 300 minutes) of moderate-intensity physical activity per week, or at least 75
minutes (preferable 150 minutes) of intense cardiorespiratory activity. These
recommendations may be applied to patients with NASH, although they have not been
specifically evaluated in this subgroup. A recent study showed that a weekly combination of
250 min of moderate to vigorous exercise was more effective than 150 min in reducing
steatosis and liver stiffness. Like diet, physical activity must be based on realistic and
sustainable objectives15
. The major difficulty is obtaining long-term compliance—especially
in individuals who are not accustomed to regular intense exercise.
In conclusion, lifestyle therapy is insufficient to induce long-term weight loss and
resolve NASH. Only 10% of patients who commit to a lifestyle intervention lose more than
10% of their weight, even when innovative approaches, such as brief consults with coaches,
are provided to instruct patients and about behaviors that control weight provide structured
recommendations16
. These limits must be overcome for this strategy to be effective. A
therapeutic algorithm is needed to define 10% weight loss as the minimum goal for patients
with NASH and to offer alternative therapy to those who do not reach the goal or in whom
NASH persists despite successful weight loss.
Weight loss with pharmacologic agents
Weight loss medications induce a median loss of approximately 3%–9%17
A randomized
study of patients in primary care showed that a combination of lifestyle intervention and a
prescription of weight loss medication (orlistat or sibutramine) produced a ≥10% loss of
baseline weight in a significantly higher proportion of patients (17.8%) than of those
receiving brief lifestyle counseling alone (9.9%) or usual (6.2%)16
.
However, health agencies have discontinued or raised concerns about these
medications. Sibutramine, a serotonergic and noradrenergic reuptake inhibitor that promotes
satiety, was associated with a 16% increase in risk of serious cardiovascular events18
and was
taken off the market by the FDA. The European Medicine Agency (EMA) recommends
listing the risk for liver-related side effects, including severe liver injury and rare cases of
acute liver failure leading to death or liver transplantation, for orlistat—an inhibitor of gastric
and pancreatic lipase. Nevertheless, the benefits of these drugs are considered to outweigh
their risks by health agencies. Orlistat did not modify necroinflammation or fibrosis in
patients with NASH5, 19
.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
7/36
ACCEPTED MANUSCRIPT
Rimonabant20
, a selective antagonist of central and peripheral CB1 receptors,
promotes satiety, reduces weight and waist circumference, and improves the lipid profile
through by increasing high-density lipoprotein (HDL) and reducing triglycerides21, 22
. There
was great hope for this drug because targeting CB1 receptors in the liver reduces steatosis,
portal pressure, and the pathways of fibrogenesis23
. These results were the rationale to test
rimonabant in patients with NASH (NCT00577148; NCT00576667). Unfortunately the trial
was stopped due to serious psychiatric side effects—patients developed severe depression and
became suicidal21
. Research is underway to develop a peripherally restricted CB1 antagonist
that reduces liver injury without causing neuropsychiatric events23
.
Liragutide, an agonist of glucagon-like petide-1 (GLP1) is an anorectic incretin
hormone. It was found to be significantly more effective than orlistat in treating obese patients
24 and increasing weight loss in patients with type 2 diabetes
25. In addition to the benefits to
body weight and glycemic control, GLP1 pathways seem to interfere with other mechanisms
of liver injury. Because of this profile, this drug is being investigated for treatment of
NASH26
.
Bariatric surgery
In severely obese patients (those with a body mass index [BMI] ≥ 40 or 35–40 with
comorbidities), bariatric surgery induces sustained weight loss and has been recommended by
the National Institutes of Health for motivated candidates. Perioperative mortality varies from
0.1% to 0.3%, depending on the type of surgery and patient characteristics27, 28
. Regardless of
procedure type, bariatric surgery induces long-term weight loss (of 15%–25%), as well as
remission of diabetes29-31
and reduced overall long-term mortality32
—particularly from
diabetes33
, heart disease,34
and cancers35
.
The effects of bariatric surgery on the liver include reductions in steatosis—mainly
within the first year after surgery until 5 years later. The kinetics of the insulin resistance
profile parallel those of steatosis and ballooning, with the greatest reductions the first year
after surgery but continuing for up to 5 years. The long-term outcome can be predicted by
early improvement in insulin resistance following the procedure36
. Nevertheless, reduced
insulin resistance is often not enough to resolve NASH. At the same time, some patients with
improvement in NASH injuries remain insulin resistant. Moreover, despite the ability of
bariatric surgery to reduce steatosis, there is controversy over its effects on fibrosis and the
necroinflammation. Prospective studies are needed to resolve this issue.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
8/36
ACCEPTED MANUSCRIPT
Small, preliminary studies reported that NASH disappeared from approximately 85%–
90% of patients who underwent gastric banding or bypass surgeries37, 38
. A recent prospective
study that analyzed sequential liver biopsies from 1540 patients who underwent bariatric
surgery for morbid obesity provided strong evidence that the procedure resulted in the
disappearance of NASH. One hundred and nine patients had biopsy-proven NASH at
baseline; NASH had disappeared from the livers of approximately 85% of the patients 1 year
later. NASH resolved a greater proportion of patients with mild disease than from those with
moderate or severe disease at baseline. Bariatric surgery significantly reduced all the
histological components of NASH including fibrosis that was improved in about 30% of cases
39.
After bariatric surgery, the extent of weight loss appears to associate with the
reduction in liver injury. Gastric bypass seems to be more effective than gastric banding in
reducing liver injury—this specific benefit is believed to be due to the greater loss in weight40
.
However, larger studies of patients matched for disease severity and comorbidities are needed
to confirm these results. Beside the ability of gastric bypass to promote weight loss, it has
several other features that make it more effective than gastric banding. For example, more
rapid contact of nutrients with the ileum increases satiety by increasing secretion of anorectic
hormones such as PYY or incretins (GLP1 and GLP2). GLP1 is involved in the enteroinsular
axis, stimulating insulin secretion and decreasing hepatic glucose output and insulin resistance
in the liver and adipose tissues41
.
So, bariatric surgery appears to reduce fibrosis and necroinflammatory processes to
alter disease progression and prevent development of cirrhosis and its complications.
Cirrhosis is considered to be a contraindication to bariatric surgery—mortality increased 21-
fold in patients with decompensated cirrhosis and 2-fold in patients with compensated
cirrhosis42
. However, it is not clear whether this contraindication applies to patients with
cirrhosis or portal hypertension or liver dysfunction. Another important area for future
research is to determine whether bariatric surgery is effective for severely obese patients who
are candidates for liver transplantation43, 44
. A preliminary study of 7 patients reported that
sleeve gastrectomy performed at the same time than liver transplantation was more effective
to reduce weight of obese patients with end-stage liver disease that medical management.
Thus bariatric surgery could be of interest for the management of liver transplantation
candidates with severe obesity45
.
In conclusion, although bariatric surgery resolves NASH in patients in whom lifestyle
therapy has failed, perioperative risks limit its application. Because of the high rate of
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
9/36
ACCEPTED MANUSCRIPT
remission of NASH, bariatric surgery could be tested in randomized controlled trials of
moderately obese patients with extensive fibrosis and severe comorbidities.
Insulin Sensitization
Insulin-resistance is an important factor in the development of NASH. Excess fatty-acid
transport into hepatocytes is required for development of hepatic insulin resistance and
NAFLD (Figure 1). In rats fed high-fat diets, increased hepatic diacylglycerol content and the
translocation of protein kinase C epsilon (PRKCE) to the plasma membrane contributes to
development of insulin resistance. By binding the insulin receptor an inhibiting its activity,
translocated PRKCE2, 46
impairs the ability of insulin to activate glycogen synthesis and
inhibit gluconeogenesis2. These mechanisms have been also been observed in liver tissues
from obese patients with NAFLD; in these patients, hepatic diacylglycerol content,
cytoplasmic lipid droplets, and PRKCE activation correlated with reduced insulin signaling47
.
Accumulation of fat in the liver therefore seems to be the first step in the development of
hepatic insulin resistance.
Studies from animal models indicate that liver inflammation is not sufficient for
development of hepatic insulin resistance, regardless of the pathway48
. The severity of insulin
resistance was associated with more severe necroinflammation injury in liver tissues from
patients with NASH than those without NASH36. By increasing peripheral lipolysis, insulin
resistance increases delivery of free fatty acids to the liver,49
leading to excess fat and
increased β-oxidation, which worsens oxidative stress. Insulin resistance might be targeted
therapeutically, perhaps with insulin sensitizing agents.
Metformin
By reducing gluconeogenesis50
metformin, a biguanide agent, increases fasting levels of
glucose, as well as levels of postprandial glucose and glycosylated hemoglobin; it is
recommended for obese patients with type 2 diabetes51
. Metformin also reduces fat body mass
without changing lean body mass50
. In a proof of concept study of 20 patients with NASH,
metformin was associated with decreased levels of aminotransferases and insulin resistance52
.
These effects were confirmed in a randomized controlled trial and a non-controlled
prospective study. Histologic features of NASH were reduced in 30% of liver tissues
analyzed; a higher proportion of patients from who these tissues were obtained lost weight
during metformin treatment53, 54
. Nevertheless, other studies have not confirmed the ability of
metformin to reduce histologic features of NASH, and a meta-analysis concluded that
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
10/36
ACCEPTED MANUSCRIPT
metformin was not effective in patients with NASH55
. The 2012 American Association for the
Study of Liver Disease (AASLD) guidelines do not recommend the use of metformin in
adults with NASH56
.
More recent results have indicated that metformin could decrease the risk of
hepatocellular carcinoma, in a dose-dependent manner, in obese patients with type 2
diabetes57, 58
. Metformin might therefore be used to decrease the risk of liver cancer in
patients with diabetes, but this interesting strategy requires further study58
.
Peroxisome proliferator-activated receptors (PPARs)
Peroxisome proliferator-activated receptors (PPARγ) are nuclear receptors involved in lipid
and glucose homeostasis and regulation of inflammation and cellular differentiation.
Randomized studies of patients with type 2 diabetes have shown that PPARγ agonists
decrease glucose and glycosylated hemoglobin. Because PPARγ agonists such as
rosiglitazone and pioglitazone have multiple targets, they have been extensively tested in
patients with NASH. In a randomized study, patients with NASH given rosiglitazone had
significant reductions in levels of aminotransferases, insulin resistance, and steatosis, but no
changes in necroinflammation or fibrosis, compared with placebo group. However, there was
no additional benefit in extending rosiglitazone therapy up to 2 years.
In 2 randomized trials of pioglitazone,59, 60 patients with impaired glucose tolerance or
type 2 diabetes had significant reductions in levels of aminotransferases, steatosis (by 65%),
hepatocyte ballooning, necrosis, and lobular inflammation, along with increased hepatic
insulin sensitivity, compared to patients given placebo. However, a significant reduction in
fibrosis was only reported in only 1 study60
. A large randomized controlled trial of in non-
diabetic patients with NASH61
compared pioglitazone to placebo, as well as vitamin E to
placebo. Although the pioglitazone group did not reach the pre-specified statistical
significance for the primary outcome (that was a reduction of 2 point in NAS) compared to
the placebo group, patients given pioglitazone had significant reductions in steatosis,
inflammation, hepatocyte ballooning, insulin resistance, and levels of liver enzymes61
.
Pioglitazone seemed to be more effective than vitamin E in producing the secondary
outcome—resolution of NASH, although there was no statistical analysis performed in the
comparison of these agents61
.
Because of the promising results from these trials, pioglitazone is listed as a potential
treatment for NASH in the 2012 AASLD guidelines56
. However, there is concern about the
safety of PPARγ agonists. All large randomized controlled trials of pioglitazone and
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
11/36
ACCEPTED MANUSCRIPT
rosiglitzone have shown weight gain of 3–5 kg after patients took these drugs59, 61, 62
.
Furthermore, the FDA and EMA have warned about the cardiovascular risk related to the use
of PPARγ agonists63, 64
. Rosiglitazone has been associated with an increased risk of cardiac
ischemia and heart failure, and its prescription was restricted by the FDA. Data that indicate
that pioglitazone might induce congestive heart failure, although no increased risk of cardiac
death was found among the pioglitazone group. Expert guidelines have therefore approved the
prescription of pioglitazone for patients with NASH with safety and caution recommendations
on long-term use56
.
Elafibranor (GFT505)65
is an agonist of PPARα and PPARδ that has been tested in
patients with NASH because it increases hepatic insulin sensitivity, improves glucose
homeostasis and lipid metabolism, and reduces inflammation. In animal models of NAFLD or
NASH and liver fibrosis, elafibranor reduced steatosis, inflammation, and fibrosis as well as
markers of inflammation and fibrogenesis70
. In clinical trials, elafibranor (NCT01271751,
NCT01275469, NCT01275469, and NCT01271777) significantly improved patients’
metabolic profiles and reduced levels of aminotransferases. A recent randomized controlled
phase 2 study of 274 patients with NASH compared 2 doses of elafibranor to placebo. There
was no significant difference between the number of patients in each group who reached the
primary endpoint (resolution of NASH without the worsening of fibrosis). However, after
correction for baseline severity and the center effect, the highest dose of elafibranor (120 mg
per day)64
resolved NASH in significantly more patients than placebo. These results must be
confirmed in a well-designed phase 3 study of patients with severe NASH and fibrosis, which
seems to be the population who can receive the most benefit from this agent.
The GLP1 pathway
GLP1 is an incretin hormone that is secreted after nutrients come in contact with the ileum. It
increases insulin secretion, decreases hepatic glucose output and insulin resistance in the liver
and adipose tissues, and promotes satiety. The GLP1 pathway decreases liver fatty acid
accumulation through the activation of numerous genes such as PPARα / γ witch will enhance
hepatic fatty oxidation, lipid export, and insulin sensitivity. This pathway also stimulates
macro- and chaperon-mediated autophagy, and to reduce endoplasmic reticulum stress and
TNF, IL6, IL1β, and MCP1/CCL2 expression4, lipid export, and insulin sensitivity. This
pathway also stimulates macro- and chaperon-mediated autophagy and reduces endoplasmic
reticulum stress and expression of tumor necrosis factor (TNF), interleukin-6 (IL6), IL1B, and
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
12/36
ACCEPTED MANUSCRIPT
MCP1 (also called CCL2)4. All these GLP1-related mechanisms decrease liver inflammation
and apoptotic liver injuries66
.
As previously observed in patients with diabetes and obese patients24, 25
, liraglutide
reduces weight loss in patients with NAFLD, but also decreases levels of fasting glucose and
HbA1c, insulin resistance, and peripheral lipolysis, leading to lower levels of low-density
lipoprotein (LDL)–cholesterol, serum leptin, and adiponectin. The most frequent side effects
are gastrointestinal symptoms, which occur in approximately 20% of cases. Levels of
aminotransferases, gamma-glutamyl transferase, and steatosis also improved67
. Researchers
performed a phase 2 randomized controlled trial (LEAN study)26
of 52 patients with NASH
and type 2 diabetes; 46% of patients had Kleiner fibrosis stage F3 and 58% had fibrosis stage
F4. The authors observed NASH resolution in a significantly higher proportion of patients
who received liraglutide (39% of patients) than those given placebo (9% of patients), along
with reductions in fasting level of glucose and significantly less worsening of fibrosis in
patients who received liraglutide. In a post-hoc analysis, there was no difference in weight or
glycemic control in the liraglutide group between patients in whom NASH resolved vs those
without NASH resolution. Moreover, liraglutide reduced biomarkers of fibrosis, indicating
that in addition to studies of weight loss, larger studies should be performed to evaluate the
ability of this agent to reduce fibrosis. Large phase 3 randomized controlled studies are also
needed to determine the effects of liraglutide on NASH, considering there was no significant
difference in level of aminotransferase levels between groups, as well as the low spontaneous
resolution (9%) of NASH in patients who received the placebo. Exenatide, another agonist of
GLP1, is being evaluated in a trial of patients with NASH (NCT01208649), but no data are
available.
An alternative approach is to maintain activation of the GLP1 pathway. The incretin
inhibitor dipeptidyl peptidase 4 (DDP4), which is involved in the degradation of GLP1 and
induces a sustained metabolic effect, has been tested in patients with type 2 diabetes. Health
agencies have approved saxagliptin and sitagliptin for treatment of patients with type 2
diabetes, but cardiovascular safety is a subject of debate. Randomized clinical trials have
evaluated the vascular effects of saxaglitin in patients with type 2 diabetes and found an
acceptable level of cardiovascular risk, with no increase in mortality, although the rate of
hospitalization for heart failure increased among patients receiving this agent68
. There was no
increased risk of cardiovascular events or heart failure with sitagliptine69
. Steatosis decreased
in animal models following treatment with sitagliptine70
. Researchers are considering a
clinical trial of sitagliptine in patients with NASH (NCT01963845).
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
13/36
ACCEPTED MANUSCRIPT
Obeticholic acid
Obeticholic acid, a 6a-ethyl derivative of chenodeoxycholic acid, is an active ligand of
nuclear receptor subfamily 1 group H member 4 (NR1H4 or FXR), which regulates glucose,
lipid, and energy homeostasis71, 72
and acts in anti-inflammatory and anti-fibrosis pathways73,
74. In patients with type 2 diabetes and NAFLD, 25 and 50 mg of obeticholic acid per day
induced weight loss and decreased insulin resistance and serum markers of liver inflammation
and fibrosis75
. In an interim analysis of results from a phase 2b randomized controlled trial of
283 patients with NASH, 25 mg obeticholic acid was more effective than placebo at
producing a decrease in NAS of 2 points or more (the primary endpoint), with no worsening
of fibrosis. In fact, fibrosis was significantly reduced in patients who received obeticholic
acid, compared to patients given placebo; these patients also had reductions in steatosis,
hepatocellular ballooning, and lobular inflammation76
.
However, concerns were raised about the observation that patients who received
obeticholic acid had higher concentrations of total serum cholesterol and LDL–cholesterol,
but lower levels of HDL–cholesterol. This is a major issue due because these factors increase
the risk of cardiovascular events in this population. Therapeutic strategies that include this
agent might need to include a statin, to limit hyperlipemia. Another limitation of obeticholic
acid is that about 20% of patients who take it develop pruritus, which could reduce
compliance.
The optimal dose of obeticholic acid was evaluated in a phase 2 dose-range study of
200 patients with NASH that used a decrease in NAS of 2 points or more as the primary
endpoint. . A statistically significant difference was observed only in group that received 40
mg obeticholic acid, compared to placebo—not in the groups that received 10 or 20 mg
obeticholic acid77
. The long-term safety and efficacy of the 25 mg/day dose of obeticholic
acid will be evaluated in an international phase 3 randomized controlled trial
(NCT02548351). This trial will focus on reduction in liver-related morbidity and mortality, as
well as cardiovascular events.
Altering Lipid Metabolism
Polyunsaturated fatty acids (PUFAs) can either promote or inhibit inflammation, depending
on their structure78
. N‑6 PUFAs, such as linoleic acid and arachidonic acid have been shown
to promote inflammation and synthesis of eicosanoids79. Conversely, n‑3 PUFAs and omega3
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
14/36
ACCEPTED MANUSCRIPT
fatty acids, such as α‑linolenic acid, eicosapentaenoic acid (EPA), and docosahexaenoic acid
reduce inflammation. In animal models, a diet enriched in n‑3 PUFAs and omega3 fatty acids
reduced steatosis by inhibiting sterol regulatory element binding protein 1c (SREBF1), which
regulates expression of genes involved in glucose and lipid metabolism
80
.The ratio of n-6:n-3 is altered in serum samples from patients with NAFLD
81. A
randomized placebo-controlled trial of 243 patients with NASH or severe NAFLD (NAS
scores of 4 or more) showed that 1.8g–2.4g/day of ethyleicosapentanoic acid (EPA-E), a
synthetic n-3 PUFA, had no significant effect on liver enzymes, insulin resistance, steatosis,
or histologic features of NASH82
. Primary analysis of data from a randomized controlled trial
of 103 patients with NAFLD did not find any significant difference between the combination
of docosahexaenoic acid plus EPA vs placebo reducing amounts of liver fat83
.
Inhibition of stearoyl-CoA desaturase (SCD) activity by aramchol (arachidyl amido
cholanoic acid) lowers the amount of fat in the liver by decreasing synthesis and increasing β
oxidation84
. In addition to the reduction of fatty acid synthesis, the SD1 deficiency seems to
be associated with an increased activity of the carnitine palmitoyltransferase system, which
leads to long chain fatty acid β oxidation85
. In a randomized controlled trial of 60 patients
with NAFLD, 300 mg/day aramchol decreased the amount of fat in the liver but did not
significantly affect liver enzymes86
.
Leptin is an adipokine that inhibits food intake and decreases hepatic glucose
production and insulin resistance. Furthermore, leptin decreases steatosis, by reducing de
novo synthesis of fatty acids by inhibiting SCD, and increasing fatty acid β-oxidation87
.
Administration of a recombinant leptin (metreleptin) reduced fatty liver in patients with
general lipodystrophy, a genetic disorder that causes leptin deficiency88, 89
. Data from long-
term studies have shown that although metreleptin significantly reduced steatosis, lobular
inflammation, and hepatocellular ballooning, it did not reduce fibrosis89
. Resistance to leptin
contributes to the pathogenesis of obesity and could account for the correlation between the
amount of body fat and serum level of leptin in obese patients87
. However, the best
therapeutic strategy for modulation of the leptin pathway is uncertain, because of the different
effects of leptin on metabolism, the inflammatory processes, and fibrogenesis.
Combination treatment strategies that include a lipid-lowering agent have produced
some promising results. For example, the Niemann–Pick C1–like 1 (NPC1L1) protein
mediates intestinal absorption of cholesterol whereas the proprotein convertase
subtilisin/kexin type 9 (PCSK9) (inhibited by alirocumab and evolocumab) is involved in the
regulation of cholesterol homeostasis through modulation of the LDL receptor in hepatocytes.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
15/36
ACCEPTED MANUSCRIPT
The combination of ezetmibe (a NPC1L1 inhibitor), or PCSK9 inhibitor (alirocumab or
evolocumab) with statins decreases levels of LDL–cholesterol and improves cardiovascular
outcomes by reducing the risk of myocardial infarction and ischemic stroke90-94
. PCSK9-
knockout mice fed with high-fat diet are protected for the development of steatosis, compared
with controls95
. Mice given ezetimibe, which inhibits NPC1L1, have reduced inflammation
and fibrosis biomarkers96
. A randomized controlled trial of 50 patients with NASH (the
MOZART trial)97
compared the effects of ezetimibe with placebo and significant difference in
histologic markers of response, serum levels of aminotransferases, or changes in liver
stiffness (assessed by magnetic resonance elastography). Further studies are needed to
determine the effects of PCSK9 inhibitors.
Reducing Oxidative Stress
Oxidative stress causes chronic tissue injury, leading to increased cell death and fibrogenesis.
There are multiple sources of oxidative stress involved in NAFLD (Figure 1). Immune cells
such as peripheral mononuclear cells and macrophages produce excessive reactive oxygen
and nitrogen species under conditions of chronic liver inflammation. Reactive oxygen species
can disturb the intracellular redox system. Intracellular redox balance can also be disrupted by
metabolic abnormalities such as lipid β oxidation or endoplasmic reticulum stress, leading to
mitochondrial injury and cell death98. Numerous anti-oxidant agents have therefore been
tested in patients with liver disease. Except for Vitamin E, the effects of these agents in
patients with NASH have been disappointing.
Vitamin E or tocopherol
The vitamin E isoform rrr-alpha-tocopherol has been shown to have greater efficacy than the
other 7 isoforms of vitamin E in patients with NASH. Vitamin E is considered to be the first-
line pharmacotherapy for non-diabetic patients with NASH. However, further studies are
necessary before vitamin E can be recommended for diabetic patients with NASH or with
cirrhosis56
. In a randomized controlled trial (the PIVENS trial) of 247 non-diabetic patients
with NASH, a daily dose of 800 mg vitamin E for 96 weeks reduced steatosis, lobular
inflammation, hepatocellular ballooning, and NAS, compared to placebo61
. The safety profile
of vitamin E did not differ from that of placebo. Subjects receiving vitamin E had early and
continued decreases in levels of aminotransferases. Alkaline phosphatase and γ-glutamyl
transpeptidase levels progressed in a similar manner. However, after vitamin E was
discontinued, aminotransferase levels returned to the same range as that of placebo. This
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
16/36
ACCEPTED MANUSCRIPT
relapse after 96 weeks of vitamin E administration indicates that it might need to be given for
a longer time periods, or indefinitely, to patients with NASH, because in most cases, the
factors that contribute to liver injury persist.
This is an important consideration, because long-term vitamin E use was associated
with increased mortality99
. Long-term use of vitamin E was associated with a 22% increase in
risk of hemorrhagic stroke and a 10% reduction in thrombotic stroke. However the effect of
vitamin E on overall stroke events has not been clarified100
. Concerns about the safety profile
associated with long-term use of vitamin E were raised in a randomized controlled trial (the
SELECT study) of 32,500 men that investigated whether selenium and/or vitamin E could
prevent prostate cancer. After a preplanned 7-year interim analysis, the safety committee
recommended discontinuing the study because futility analysis did not find any evidence that
selenium or vitamin E affected risk for prostate cancer101
. This result was confirmed by the
Physicians' Health Study II, which followed 14,641 patients who were randomly assigned to
groups given placebo or vitamin E for 8 years and did not find any difference in the risk of
prostate cancer between groups102
. However, the study committee of the SELECT trial
recommended that the preplanned final analysis be performed 7 years after the last patient
was randomly assigned to their group, because there was a trend toward an increase in risk of
prostate cancer in the vitamin E group. The final analysis showed a 17% increase in the
incidence of prostate cancer among individuals with an average risk of prostate cancer who
received 400 mg/day of vitamin E103
. However, no firm conclusions can be drawn because of
the contradictory conclusions of meta-analyses evaluating the risk of vitamin E-related
mortality.
Non-vitamin E antioxidants
Ursodeoxycholic acid does not significantly affect histologic features of NASH56, 104, 105
.
Antioxidants such as silymarin, cysteamine bitartrate, or resveratrol have been studied in
proof-of-concept studies, but there is no evidence to support their further evaluation in
patients with NASH56
.
Preventing or Reducing Fibrosis
Anti-fibrotic agents are being developed to prevent progression of NASH106
. One strategy
targets factors that promote chronic liver inflammation, to prevent subsequent fibrogenesis
(such as antiviral agents)107
. Reduced fibrosis is therefore an endpoint for studies of the
effectiveness of these agents in patients with NASH. Another approach targets the
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
17/36
ACCEPTED MANUSCRIPT
pathogenesis of fibrosis, based on clinical evidence that NASH-related mortality is associated
with the severity of fibrosis106
.
Simtuzumab (GS-6624) is an antibody against enzyme lysyl oxidase-like-2 (LOXL2),
which is overexpressed during development of liver fibrosis and promotes cross-linking of
fibrillar collagen I. In animal models, an anti-LOXL2 agent reduced liver and lung fibrosis by
inhibiting fibroblasts and decreasing growth factors and the transforming growth factor-β
pathway108
. Patients with NASH and stage 3 and 4 fibrosis have been enrolled in a study of its
safety and efficacy (NCT00799578; NCT01672879). Data are not yet available.
Galectins are a family of proteins with binding specificities for β-galactoside sugars.
Galectin-3 has crosslinking and adhesive properties and is encoded by the lectin, galactoside-
binding, soluble, 3 gene ( LGALS3); it is a target of direct-acting anti-fibrotic agents. This
protein is mediates fibrogenesis in the liver and other organs. Lgals3–/–
mice are resistant to
induction of liver fibrosis by toxin administration109
. Phase 1 studies of galectin-3 inhibitors
have been completed (GR-MD-02, NCT01899859) (see Table 2) and the agent is being
evaluated in phase 2 studies of patients with NASH and cirrhosis (NCT02462967) or
advanced fibrosis (NCT02421094).
Reducing Cell Death and Inflammation
Pentoxifylline appears to prevent inflammation-related liver injury by decreasing production
of TNF, which reduces insulin resistance, oxidative stress,110
and cell death. Pilot studies
have reported beneficial effects of pentoxifylline, and a randomized controlled trial of 50
patients with NASH found that pentoxifylline reduced steatosis, lobular inflammation, and
NAS, but had no significant effect on hepatocyte ballooning or fibrosis111
. A meta-analysis
concluded that although pentoxifylline had a moderate effect in patients with NASH, there
was not enough robust evidence to show that it was better than placebo112
. Larger trials are
needed to evaluate the effectiveness of pentoxifylline.
Modulators of apoptotic signaling could reduce inflammation and liver cell injury in
patients with NASH. GS-9450, which has selective activity against caspases 1, 8, and 9, was
tested in a randomized controlled trial of 124 patients with NASH. Patients given GS-9450 for
4 weeks had reduced caspase-3–cleaved cytokeratin-18 fragments in liver tissues and lower
levels of alanine aminotransferase than patients given placebo113
. However, development of
this agent was discontinued because some patients developed liver injury. This should be
carefully evaluated because drug-induced liver injury has been associated with other caspase
inhibitors, indicating a possible class effect.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
18/36
ACCEPTED MANUSCRIPT
Agents that target chemokine (C-C motif) receptor 2 (CCR2) or CCR5 might
be developed for patients with NASH, because the chemokines they bind can increase insulin
resistance and recruit macrophages to the liver and adipose tissue114
. However, there is no
clear evidence for the role of CCR5 in the pathogenesis of NAFLD. This receptor regulates
CD8+ T-cell accumulation115
and the response to viral116
and bacterial infections117
.
Cenicriviroc, which inhibits CCR2 and CCR5, was initially developed for treatment of
patients with HIV infection. It will be evaluated in patients with NASH.
New Approaches
There are several drugs in phase 1 development with new targets and previously
undescribed mechanisms of action (see Table 2). One class is the apical sodium-dependent
bile acid transporter (ASBT) inhibitor. ASBT is an ileal bile acid transporter that reabsorbs
bile acids and seems to be required for enterohepatic recirculation and lipid homeostasis118
.
Recent research into the pathways activated by bile acids (such as FXR agonists) found that
bile acid sequestrants have interesting metabolic effects, such as reducing blood glucose and
LDL in patients with type 2 diabetes119
. Blocking bile acid absorption with ASBT inhibitors
could therefore reduce insulin sensitivity and potentially NAFLD.
The mitogen-activated protein kinase kinase kinase 5 (also known as apoptosis signal
kinase-1 [ASK1]) is involved in oxidative stress-induced apoptosis 120 . Although data are
limited, ASK1 inhibitors could be of interest for treatment of NASH.
The composition of the intestinal microbiota has been associated with obesity, insulin
resistance, and liver diseases including NAFLD121, 122
. NASH has been associated with
specific microbiota profiles, and inflammasome-mediated dysbiosis regulates progression of
NAFLD and obesity121, 122
. Transfer of intestinal microbiota from lean donors increased
insulin sensitivity in individuals with metabolic syndrome123
. Some studies have aimed to
alter the composition of microbiota in patients with NASH124. However, more studies are
needed to identify the microbes that affect insulin resistance, obesity, and liver cell injury125
and their mechanisms.
Future Directions
Although lifestyle intervention is still the first-line therapy for patients with NASH, only a
few patients are able to lose 10% of their body weight, which has been set as the threshold
required for NASH resolution. More efficient lifestyle and weight loss strategies are needed.
Bariatric surgery is highly effective in severely obese patients with NASH, and may be
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
19/36
ACCEPTED MANUSCRIPT
proposed for subjects who fulfill the validated criteria for this option. Expert guidelines
recommend vitamin E as the first-line therapy for non-diabetic patients with NASH.
However, many agents are in development for treatment of NASH, including obeticholic acid,
liraglutide, and elafibranor. Many studies are needed to determine the ability of these
molecules to resolve NASH and their long-term effects on liver-related mortality and
morbidity.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
20/36
ACCEPTED MANUSCRIPT
Table 1. Agents Available or in Development for Treatment of NASH or NAFLD
Drugs &
Therapy
Action Phase of
development
Histological Impact Pros & cons Ref
Weight loss
Lifestyle Reduces insulin
resistance,cardiovascular
risk; lipid profile reduces
oxidative stress
Recommended in
first-line
treatment
Depends on the level of
weight loss:
▪ >3%–5%: reduces
steatosis
▪ > 7%–9%: reduces
necroinflammation
▪ ≥10%: reduces fibrosis
Only 10% of patients reach the
10% weight loss threshold
required for an effect, and risk
weight gain relapse
6, 7, 56
Bariatric surgery Induces sustained weight
loss at least up to 10 years;
increases insulin resistance
and cardiovascular risk
Cohort studies Reverses NASH in 85%
of patients. Reduces
steatosis,
necroinflammation, and
fibrosis
Recommended for patients
with morbid obesity. Post-
operative morbidity limits
applicability to patients with
BMIs ≤ 35kg/m².
37-39
Insulin sensitizers
Pioglitazone PPARγ agonist, lipid
homeostasis, inflammation,
and cell differentiation
Phase 2
completed
Improves:
▪ steatosis
▪ necroinflammation
▪ fibrosis
Pros: effective for patients
with NASH
Cons: Weight gain
Risk of congestive heart
failure (no effect on mortality)
and bladder cancer
59, 61
Liraglutide GLP1 agonist, promotes
satiation, weight loss,
reduces insulin resistance
Phase 3 Reduces
▪ steatosis
▪ necroinflammation
No worsening of fibrosis
▪ resolution of NASH
Pros: marketed for patients
with diabetes, safety seems
acceptable
Cons: gastrointestinal side
effects, requires subcutaneous
administration
26
Agents with multiple targets
GFT505/
Elfibranor
PPARα and PPARδ
agonist;
reduces insulin resistance,
inflammation, and fibrosis;
improves lipid metabolism
Phase 3 Reduces
▪ steatosis
▪ necroinfammation
▪ fibrosis
Reverses NASH *
120 mg per day reduces
histologic features of NASH
65, 126
Obeticholic acid FXR agonist, increases
energy homeostasis and
lipid metabolism; reduces
insulin resistance,
inflammation, and fibrotic
pathways
Phase 3 Reduces
▪ steatosis
▪ necroinflammation
▪ fibrosis
▪ NAS without worsening
of fibrosis
Pros: reduces histologic
features in NASH.
Cons: side effects, with 20%
of patients developing pruritus
72,73
Agents that alter lipid metabolism
Aramchol Inhibition of stearoyl
coenzyme A desaturase 1
Phase 2 Decrease fat amount, no
effects on NASH
No effects on NASH, only
preliminary results available
83
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
21/36
ACCEPTED MANUSCRIPT
(SD1)
Anti-oxidants
Vitamin E Tocopherol, anti-oxydative
stress
Phase 2
completed
Significant effects on
▪ steatosis
▪ necroinflammation
▪ NAS
Pros: recommended as first
pharmacologic therapy
Cons: no data from patients
with diabetes or cirrhosis;
concerns for long-term use
1
Agents that reduce inflammation or cell death
Pentoxifylline Reduces inflammation
(potentially by inhibiting
TNF), blood viscosity, and
platelet aggregation
Phase 2
completed
Reduces
▪ steatosis
▪ necroinflammation
▪ NAS
Pros: pilot studies indicate
efficacy
Cons: lack of large
randomized controlled trials or
robust data sets
11
Cenicriviroc Inhibit CCR2 and
CCR5, reduces
insulin resistance and
recruitment of
inflammatory cells
Phase 2 No data Initially developed for
treatment of HIV infection.
Potentially interesting effects
in patients with NASH but
further studies are needed
*Did not achieve primary endpoint in large Phase 2 randomized controlled trial (resolution of NASH without worsening of
fibrosis). Statistical significance was obtained from subgroup analysis. Findings must be confirmed in phase 3 randomized
controlled trials.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
22/36
ACCEPTED MANUSCRIPT
Table 2. Agents in Development
Drug Target Potential Mechanism of
Action
ClinicalTrial.gov
identifier
GR-MD-02 Galectin-3 Anti-fibrotic NCT01899859
PX-102 FXR agonist Reduces insulin resistance NCT01998659
SHP-626 ASBT inhibitor Increases levels of GLP1 NCT02287779
GS-4997 ASK1 inhibitor Reduces consequences of
oxidative stress
NCT02466516
JKB-121 Toll-like receptor 4 Anti-inflammatory agent NCT02442687
Note: All agents are either in phase 1 trials or pre-clinical studies
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
23/36
ACCEPTED MANUSCRIPT
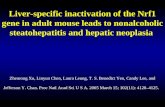
Figure 1. Pathophysiology of NASH and Therapeutic Targets
Legend:
Patients with NASH have a higher daily caloric intake (especially high fructose corn syrup)
and are more sedentary than those without. Those bad habits are also associated with obesity
and metabolic syndrome witch are highly prevalent in NASH. Thus, lifestyle therapy with diet
and increased physical activity to obtain 10% of weight loss is the first step for NASH
treatment. For a better efficacy, complementary weight loss strategies can be proposed as
bariatric surgery for severely obese patients. In NASH there is an excessive transport of sugar
and fatty-acids (from diet and increased lipogenesis) to the hepatocyte that leads to steatosis.
Fat absorption may be targeted to reduce steatosis, as for example NCP1L1 (Niemann–Pick
C1–like 1 protein) inhibitor (ezetimibe) that decreases the gut absorption of cholesterol.
However, steatosis is a key event for the development of hepatic insulin resistance. At a
molecular level, accumulation of fatty-acids in the hepatocytes enhances the translocation to
membrane of the primary novel PKC isoform epsilon that inhibits the insulin receptor
activity. Hepatic insulin resistance increases lipogenesis and reduces fatty acids β-oxidation
that lead to steatosis. This last mechanism can by reduced with aramchol, an inhibitor of
stearoyl coenzyme A desaturase (SCD) activity that promotes liver fat wash out through
increased β-oxidation and reduced lipogenesis. In the therapeutic landscape for NASH, many
agents target insulin resistance (liraglutide, PPARα agonist, metformin) that is a main
pathway of the pathogenesis of NASH. Insulin resistance can almost be consider as a
prerequisite target for the action of multiple hit drugs as obeticholic acid and elafibranor. But,
insulin resistance is not sufficient alone to induce NASH. Therefore macrovacuolar lipid
droplets accumulation in the hepatocyte drives major cellular stress and injuries through 3
main pathways: mitochondrial injury, oxidative and endoplasmic reticulum stress. Oxidative
stress reduces phosphorylation of FOXO1, a nuclear factor involved in glucose production
and adipose storage. The non-phosphorylate FOXO1 is translocated to the nucleus and
increases hepatic glucose production that occurs in insulin resistance and diabetes.
Furthermore the activation of the MAP kinase pathway through p38 promotes inflammatory
pathways and increases apoptosis. Thus, inflammation and apoptosis are two therapeutic
targets for NASH. For anti-inflammatory treatments, anti-oxidant therapies as vitamin E
reduces inflammatory injuries due to oxidative stress. Dual CCR2 and CCR5 antagonist
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
24/36
ACCEPTED MANUSCRIPT
(Cenicriviroc) reduces the recruitment of inflammatory cells. The apoptotic pathway may be
targeted with anti-caspase therapy. Decreasing inflammation and apoptosis might reduce
fibrogenesis. Finally, fibrosis can be considered as the last target for therapeutic agents, as an
example, anti-LOXL2 agents. (FFA:free fatty-acids, FA :fatty-acids, PKC: protein kinase C)
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
25/36
ACCEPTED MANUSCRIPT
References
1. Sanyal AJ, Friedman SL, McCullough AJ, et al. Challenges and opportunities in drug
and biomarker development for nonalcoholic steatohepatitis: findings and
recommendations from an American Association for the Study of Liver Diseases-U.S.Food and Drug Administration Joint Workshop. Hepatology 2015;61:1392-405.
2. Perry RJ, Samuel VT, Petersen KF, et al. The role of hepatic lipids in hepatic insulin
resistance and type 2 diabetes. Nature 2014;510:84-91.
3. Gerber L, Otgonsuren M, Mishra A, et al. Non-alcoholic fatty liver disease (NAFLD)
is associated with low level of physical activity: a population-based study. Aliment
Pharmacol Ther 2012;36:772-81.
4. Kim YO, Schuppan D. When GLP-1 hits the liver: a novel approach for insulin
resistance and NASH. Am J Physiol Gastrointest Liver Physiol 2012;302:G759-61.
5. Harrison SA, Fecht W, Brunt EM, et al. Orlistat for overweight subjects with
nonalcoholic steatohepatitis: A randomized, prospective trial. Hepatology 2009;49:80-
6.6. Promrat K, Kleiner DE, Niemeier HM, et al. Randomized controlled trial testing the
effects of weight loss on nonalcoholic steatohepatitis. Hepatology 2010;51:121-9.
7. Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, et al. Weight Loss Through
Lifestyle Modification Significantly Reduces Features of Nonalcoholic
Steatohepatitis. Gastroenterology 2015;149:367-78 e5; quiz e14-5.
8. Shai I, Schwarzfuchs D, Henkin Y, et al. Weight loss with a low-carbohydrate,
Mediterranean, or low-fat diet. N Engl J Med 2008;359:229-41.
9. Huang MA, Greenson JK, Chao C, et al. One-year intense nutritional counseling
results in histological improvement in patients with non-alcoholic steatohepatitis: a
pilot study. Am J Gastroenterol 2005;100:1072-81.
10. Ryan MC, Itsiopoulos C, Thodis T, et al. The Mediterranean diet improves hepatic
steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J
Hepatol 2013;59:138-43.
11. Anty R, Marjoux S, Iannelli A, et al. Regular coffee but not espresso drinking is
protective against fibrosis in a cohort mainly composed of morbidly obese European
women with NAFLD undergoing bariatric surgery. J Hepatol 2012;57:1090-6.
12. Molloy JW, Calcagno CJ, Williams CD, et al. Association of coffee and caffeine
consumption with fatty liver disease, nonalcoholic steatohepatitis, and degree of
hepatic fibrosis. Hepatology 2012;55:429-36.
13. Birerdinc A, Stepanova M, Pawloski L, et al. Caffeine is protective in patients with
non-alcoholic fatty liver disease. Aliment Pharmacol Ther 2012;35:76-82.14. Greenberg JA, Chow G, Ziegelstein RC. Caffeinated coffee consumption,
cardiovascular disease, and heart valve disease in the elderly (from the Framingham
Study). Am J Cardiol 2008;102:1502-8.
15. Oh S, Shida T, Yamagishi K, et al. Moderate to vigorous physical activity volume is
an important factor for managing nonalcoholic fatty liver disease: a retrospective
study. Hepatology 2015;61:1205-15.
16. Wadden TA, Volger S, Sarwer DB, et al. A two-year randomized trial of obesity
treatment in primary care practice. N Engl J Med 2011;365:1969-79.
17. Yanovski SZ, Yanovski JA. Long-term drug treatment for obesity: a systematic and
clinical review. JAMA 2014;311:74-86.
18. James WP, Caterson ID, Coutinho W, et al. Effect of sibutramine on cardiovascularoutcomes in overweight and obese subjects. N Engl J Med 2010;363:905-17.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
26/36
ACCEPTED MANUSCRIPT
19. Zelber-Sagi S, Kessler A, Brazowsky E, et al. A double-blind randomized placebo-
controlled trial of orlistat for the treatment of nonalcoholic fatty liver disease. Clin
Gastroenterol Hepatol 2006;4:639-44.
20. Despres JP, Golay A, Sjostrom L, et al. Effects of rimonabant on metabolic risk
factors in overweight patients with dyslipidemia. N Engl J Med 2005;353:2121-34.
21. Topol EJ, Bousser MG, Fox KA, et al. Rimonabant for prevention of cardiovascularevents (CRESCENDO): a randomised, multicentre, placebo-controlled trial. Lancet
2010;376:517-23.
22. Tam J, Liu J, Mukhopadhyay B, et al. Endocannabinoids in liver disease. Hepatology
2011;53:346-55.
23. Kunos G, Gao B. Endocannabinoids, CB1 receptors, and liver disease: hitting more
than one bird with the same stone. Gastroenterology 2008;134:622-5.
24. Astrup A, Rossner S, Van Gaal L, et al. Effects of liraglutide in the treatment of
obesity: a randomised, double-blind, placebo-controlled study. Lancet 2009;374:1606-
16.
25. Davies MJ, Bergenstal R, Bode B, et al. Efficacy of Liraglutide for Weight Loss
Among Patients With Type 2 Diabetes: The SCALE Diabetes Randomized ClinicalTrial. JAMA 2015;314:687-99.
26. Armstrong MJ, Gaunt P, Aithal GP, et al. Liraglutide safety and efficacy in patients
with non-alcoholic steatohepatitis (LEAN): a multicentre, double-blind, randomised,
placebo-controlled phase 2 study. Lancet 2015.
27. Chang SH, Stoll CR, Song J, et al. The effectiveness and risks of bariatric surgery: an
updated systematic review and meta-analysis, 2003-2012. JAMA Surg 2014;149:275-
87.
28. Longitudinal Assessment of Bariatric Surgery C, Flum DR, Belle SH, et al.
Perioperative safety in the longitudinal assessment of bariatric surgery. N Engl J Med
2009;361:445-54.
29. Gloy VL, Briel M, Bhatt DL, et al. Bariatric surgery versus non-surgical treatment for
obesity: a systematic review and meta-analysis of randomised controlled trials. BMJ
2013;347:f5934.
30. Schauer PR, Bhatt DL, Kirwan JP, et al. Bariatric Surgery versus Intensive Medical
Therapy for Diabetes - 3-Year Outcomes. N Engl J Med 2014.
31. Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric surgery versus conventional
medical therapy for type 2 diabetes. N Engl J Med 2012;366:1577-85.
32. Sjostrom L, Narbro K, Sjostrom CD, et al. Effects of bariatric surgery on mortality in
Swedish obese subjects. N Engl J Med 2007;357:741-52.
33. Eliasson B, Liakopoulos V, Franzen S, et al. Cardiovascular disease and mortality in
patients with type 2 diabetes after bariatric surgery in Sweden: a nationwide, matched,observational cohort study. Lancet Diabetes Endocrinol 2015;3:847-54.
34. Sjostrom L, Peltonen M, Jacobson P, et al. Bariatric surgery and long-term
cardiovascular events. JAMA 2012;307:56-65.
35. Sjostrom L, Gummesson A, Sjostrom CD, et al. Effects of bariatric surgery on cancer
incidence in obese patients in Sweden (Swedish Obese Subjects Study): a prospective,
controlled intervention trial. Lancet Oncol 2009;10:653-62.
36. Mathurin P, Hollebecque A, Arnalsteen L, et al. Prospective study of the long-term
effects of bariatric surgery on liver injury in patients without advanced disease.
Gastroenterology 2009;137:532-40.
37. Kral JG, Thung SN, Biron S, et al. Effects of surgical treatment of the metabolic
syndrome on liver fibrosis and cirrhosis. Surgery 2004;135:48-58.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
27/36
ACCEPTED MANUSCRIPT
38. Dixon JB, Bhathal PS, Hughes NR, et al. Nonalcoholic fatty liver disease:
Improvement in liver histological analysis with weight loss. Hepatology
2004;39:1647-54.
39. Lassailly G, Caiazzo R, Buob D, et al. Bariatric Surgery Reduces Features of
Nonalcoholic Steatohepatitis in Morbidly Obese Patients. Gastroenterology
2015;149:379-88; quiz e15-6.40. Caiazzo R, Lassailly G, Leteurtre E, et al. Roux-en-Y gastric bypass versus adjustable
gastric banding to reduce nonalcoholic fatty liver disease: a 5-year controlled
longitudinal study. Ann Surg 2014;260:893-8; discussion 898-9.
41. Lassailly G, Caiazzo R, Pattou F, et al. Bariatric surgery for curing NASH in the
morbidly obese? J Hepatol 2013;58:1249-51.
42. Mosko JD, Nguyen GC. Increased perioperative mortality following bariatric surgery
among patients with cirrhosis. Clin Gastroenterol Hepatol 2011;9:897-901.
43. Lazzati A, Iannelli A, Schneck AS, et al. Bariatric surgery and liver transplantation: a
systematic review a new frontier for bariatric surgery. Obes Surg 2015;25:134-42.
44. Charlton MR, Burns JM, Pedersen RA, et al. Frequency and outcomes of liver
transplantation for nonalcoholic steatohepatitis in the United States. Gastroenterology2011;141:1249-53.
45. Heimbach JK, Watt KD, Poterucha JJ, et al. Combined liver transplantation and
gastric sleeve resection for patients with medically complicated obesity and end-stage
liver disease. Am J Transplant 2013;13:363-8.
46. Samuel VT, Liu ZX, Wang A, et al. Inhibition of protein kinase Cepsilon prevents
hepatic insulin resistance in nonalcoholic fatty liver disease. J Clin Invest
2007;117:739-45.
47. Kumashiro N, Erion DM, Zhang D, et al. Cellular mechanism of insulin resistance in
nonalcoholic fatty liver disease. Proc Natl Acad Sci U S A 2011;108:16381-5.
48. Funke A, Schreurs M, Aparicio-Vergara M, et al. Cholesterol-induced hepatic
inflammation does not contribute to the development of insulin resistance in male
LDL receptor knockout mice. Atherosclerosis 2014;232:390-6.
49. Perry RJ, Camporez JP, Kursawe R, et al. Hepatic acetyl CoA links adipose tissue
inflammation to hepatic insulin resistance and type 2 diabetes. Cell 2015;160:745-58.
50. Stumvoll M, Nurjhan N, Perriello G, et al. Metabolic effects of metformin in non-
insulin-dependent diabetes mellitus. N Engl J Med 1995;333:550-4.
51. DeFronzo RA, Goodman AM. Efficacy of metformin in patients with non-insulin-
dependent diabetes mellitus. The Multicenter Metformin Study Group. N Engl J Med
1995;333:541-9.
52. Marchesini G, Brizi M, Bianchi G, et al. Metformin in non-alcoholic steatohepatitis.
Lancet 2001;358:893-4.53. Loomba R, Lutchman G, Kleiner DE, et al. Clinical trial: pilot study of metformin for
the treatment of non-alcoholic steatohepatitis. Aliment Pharmacol Ther 2009;29:172-
82.
54. Bugianesi E, Gentilcore E, Manini R, et al. A randomized controlled trial of
metformin versus vitamin E or prescriptive diet in nonalcoholic fatty liver disease. Am
J Gastroenterol 2005;100:1082-90.
55. Rakoski MO, Singal AG, Rogers MA, et al. Meta-analysis: insulin sensitizers for the
treatment of non-alcoholic steatohepatitis. Aliment Pharmacol Ther 2010;32:1211-21.
56. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-
alcoholic fatty liver disease: practice guideline by the American Gastroenterological
Association, American Association for the Study of Liver Diseases, and AmericanCollege of Gastroenterology. Gastroenterology 2012;142:1592-609.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
28/36
ACCEPTED MANUSCRIPT
57. Lee MS, Hsu CC, Wahlqvist ML, et al. Type 2 diabetes increases and metformin
reduces total, colorectal, liver and pancreatic cancer incidences in Taiwanese: a
representative population prospective cohort study of 800,000 individuals. BMC
Cancer 2011;11:20.
58. Chen HP, Shieh JJ, Chang CC, et al. Metformin decreases hepatocellular carcinoma
risk in a dose-dependent manner: population-based and in vitro studies. Gut2013;62:606-15.
59. Belfort R, Harrison SA, Brown K, et al. A placebo-controlled trial of pioglitazone in
subjects with nonalcoholic steatohepatitis. N Engl J Med 2006;355:2297-307.
60. Aithal GP, Thomas JA, Kaye PV, et al. Randomized, placebo-controlled trial of
pioglitazone in nondiabetic subjects with nonalcoholic steatohepatitis.
Gastroenterology 2008;135:1176-84.
61. Sanyal AJ, Chalasani N, Kowdley KV, et al. Pioglitazone, vitamin E, or placebo for
nonalcoholic steatohepatitis. N Engl J Med 2010;362:1675-85.
62. Ratziu V, Giral P, Jacqueminet S, et al. Rosiglitazone for nonalcoholic steatohepatitis:
one-year results of the randomized placebo-controlled Fatty Liver Improvement with
Rosiglitazone Therapy (FLIRT) Trial. Gastroenterology 2008;135:100-10.63. Home PD, Pocock SJ, Beck-Nielsen H, et al. Rosiglitazone evaluated for
cardiovascular outcomes in oral agent combination therapy for type 2 diabetes
(RECORD): a multicentre, randomised, open-label trial. Lancet 2009;373:2125-35.
64. Lincoff AM, Wolski K, Nicholls SJ, et al. Pioglitazone and risk of cardiovascular
events in patients with type 2 diabetes mellitus: a meta-analysis of randomized trials.
JAMA 2007;298:1180-8.
65. Presidential Plenary: Clinical. Hepatology 2015;62:261A-265A.
66. Li JV, Ashrafian H, Bueter M, et al. Metabolic surgery profoundly influences gut
microbial-host metabolic cross-talk. Gut 2011;60:1214-23.
67. Armstrong MJ, Hull D, Guo K, et al. Glucagon-Like Peptide 1 Decreases Lipotoxicity
in Non-Alcoholic Steatophepatitis. J Hepatol 2015.
68. Scirica BM, Bhatt DL, Braunwald E, et al. Saxagliptin and cardiovascular outcomes in
patients with type 2 diabetes mellitus. N Engl J Med 2013;369:1317-26.
69. Green JB, Bethel MA, Armstrong PW, et al. Effect of Sitagliptin on Cardiovascular
Outcomes in Type 2 Diabetes. N Engl J Med 2015;373:232-42.
70. Shirakawa J, Fujii H, Ohnuma K, et al. Diet-induced adipose tissue inflammation and
liver steatosis are prevented by DPP-4 inhibition in diabetic mice. Diabetes
2011;60:1246-57.
71. Lefebvre P, Cariou B, Lien F, et al. Role of bile acids and bile acid receptors in
metabolic regulation. Physiol Rev 2009;89:147-91.
72. Thomas C, Pellicciari R, Pruzanski M, et al. Targeting bile-acid signalling formetabolic diseases. Nat Rev Drug Discov 2008;7:678-93.
73. Verbeke L, Farre R, Trebicka J, et al. Obeticholic acid, a farnesoid X receptor agonist,
improves portal hypertension by two distinct pathways in cirrhotic rats. Hepatology
2014;59:2286-98.
74. Zhang S, Wang J, Liu Q, et al. Farnesoid X receptor agonist WAY-362450 attenuates
liver inflammation and fibrosis in murine model of non-alcoholic steatohepatitis. J
Hepatol 2009;51:380-8.
75. Mudaliar S, Henry RR, Sanyal AJ, et al. Efficacy and safety of the farnesoid X
receptor agonist obeticholic acid in patients with type 2 diabetes and nonalcoholic
fatty liver disease. Gastroenterology 2013;145:574-82 e1.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
29/36
ACCEPTED MANUSCRIPT
76. Neuschwander-Tetri BA, Loomba R, Sanyal AJ, et al. Farnesoid X nuclear receptor
ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): a
multicentre, randomised, placebo-controlled trial. Lancet 2015;385:956-65.
77. interceptpharma.
78. Wree A, Broderick L, Canbay A, et al. From NAFLD to NASH to cirrhosis-new
insights into disease mechanisms. Nat Rev Gastroenterol Hepatol 2013;10:627-36.79. Calder PC. n-3 polyunsaturated fatty acids, inflammation, and inflammatory diseases.
Am J Clin Nutr 2006;83:1505S-1519S.
80. Sekiya M, Yahagi N, Matsuzaka T, et al. Polyunsaturated fatty acids ameliorate
hepatic steatosis in obese mice by SREBP-1 suppression. Hepatology 2003;38:1529-
39.
81. Arendt BM, Comelli EM, Ma DW, et al. Altered hepatic gene expression in
nonalcoholic fatty liver disease is associated with lower hepatic n-3 and n-6
polyunsaturated fatty acids. Hepatology 2015;61:1565-78.
82. Sanyal AJ, Abdelmalek MF, Suzuki A, et al. No significant effects of ethyl-
eicosapentanoic acid on histologic features of nonalcoholic steatohepatitis in a phase 2
trial. Gastroenterology 2014;147:377-84 e1.83. Scorletti E, Bhatia L, McCormick KG, et al. Effects of purified eicosapentaenoic and
docosahexaenoic acids in nonalcoholic fatty liver disease: results from the Welcome*
study. Hepatology 2014;60:1211-21.
84. Dobrzyn A, Ntambi JM. Stearoyl-CoA desaturase as a new drug target for obesity
treatment. Obes Rev 2005;6:169-74.
85. Dobrzyn P, Dobrzyn A, Miyazaki M, et al. Stearoyl-CoA desaturase 1 deficiency
increases fatty acid oxidation by activating AMP-activated protein kinase in liver.
Proc Natl Acad Sci U S A 2004;101:6409-14.
86. Safadi R, Konikoff FM, Mahamid M, et al. The fatty acid-bile acid conjugate
Aramchol reduces liver fat content in patients with nonalcoholic fatty liver disease.
Clin Gastroenterol Hepatol 2014;12:2085-91 e1.
87. Marra F, Bertolani C. Adipokines in liver diseases. Hepatology 2009;50:957-69.
88. Javor ED, Ghany MG, Cochran EK, et al. Leptin reverses nonalcoholic steatohepatitis
in patients with severe lipodystrophy. Hepatology 2005;41:753-60.
89. Safar Zadeh E, Lungu AO, Cochran EK, et al. The liver diseases of lipodystrophy: the
long-term effect of leptin treatment. J Hepatol 2013;59:131-7.
90. Cannon CP, Blazing MA, Braunwald E. Ezetimibe plus a Statin after Acute Coronary
Syndromes. N Engl J Med 2015;373:1476-7.
91. Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe Added to Statin Therapy
after Acute Coronary Syndromes. N Engl J Med 2015;372:2387-97.
92. Robinson JG, Farnier M, Krempf M, et al. Efficacy and safety of alirocumab inreducing lipids and cardiovascular events. N Engl J Med 2015;372:1489-99.
93. Robinson JG, Kastelein JJ. PCSK9 Inhibitors and Cardiovascular Events. N Engl J
Med 2015;373:774.
94. Sabatine MS, Giugliano RP, Wiviott SD, et al. Efficacy and safety of evolocumab in
reducing lipids and cardiovascular events. N Engl J Med 2015;372:1500-9.
95. Zaid A, Roubtsova A, Essalmani R, et al. Proprotein convertase subtilisin/kexin type 9
(PCSK9): hepatocyte-specific low-density lipoprotein receptor degradation and critical
role in mouse liver regeneration. Hepatology 2008;48:646-54.
96. Van Rooyen DM, Gan LT, Yeh MM, et al. Pharmacological cholesterol lowering
reverses fibrotic NASH in obese, diabetic mice with metabolic syndrome. J Hepatol
2013;59:144-52.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
30/36
ACCEPTED MANUSCRIPT
97. Loomba R, Sirlin CB, Ang B, et al. Ezetimibe for the treatment of nonalcoholic
steatohepatitis: assessment by novel magnetic resonance imaging and magnetic
resonance elastography in a randomized trial (MOZART trial). Hepatology
2015;61:1239-50.
98. Stauffer JK, Scarzello AJ, Jiang Q, et al. Chronic inflammation, immune escape, and
oncogenesis in the liver: a unique neighborhood for novel intersections. Hepatology2012;56:1567-74.
99. Miller ER, 3rd, Pastor-Barriuso R, Dalal D, et al. Meta-analysis: high-dosage vitamin
E supplementation may increase all-cause mortality. Ann Intern Med 2005;142:37-46.
100. Schurks M, Glynn RJ, Rist PM, et al. Effects of vitamin E on stroke subtypes: meta-
analysis of randomised controlled trials. BMJ 2010;341:c5702.
101. Lippman SM, Klein EA, Goodman PJ, et al. Effect of selenium and vitamin E on risk
of prostate cancer and other cancers: the Selenium and Vitamin E Cancer Prevention
Trial (SELECT). JAMA 2009;301:39-51.
102. Gaziano JM, Glynn RJ, Christen WG, et al. Vitamins E and C in the prevention of
prostate and total cancer in men: the Physicians' Health Study II randomized
controlled trial. JAMA 2009;301:52-62.103. Klein EA, Thompson IM, Jr., Tangen CM, et al. Vitamin E and the risk of prostate
cancer: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA
2011;306:1549-56.
104. Lindor KD, Kowdley KV, Heathcote EJ, et al. Ursodeoxycholic acid for treatment of
nonalcoholic steatohepatitis: results of a randomized trial. Hepatology 2004;39:770-8.
105. Ratziu V, de Ledinghen V, Oberti F, et al. A randomized controlled trial of high-dose
ursodesoxycholic acid for nonalcoholic steatohepatitis. J Hepatol 2011;54:1011-9.
106. Angulo P, Kleiner DE, Dam-Larsen S, et al. Liver Fibrosis, but No Other Histologic
Features, Is Associated With Long-term Outcomes of Patients With Nonalcoholic
Fatty Liver Disease. Gastroenterology 2015;149:389-97 e10.
107. Marcellin P, Gane E, Buti M, et al. Regression of cirrhosis during treatment with
tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up
study. Lancet 2013;381:468-75.
108. Barry-Hamilton V, Spangler R, Marshall D, et al. Allosteric inhibition of lysyl
oxidase-like-2 impedes the development of a pathologic microenvironment. Nat Med
2010;16:1009-17.
109. Henderson NC, Mackinnon AC, Farnworth SL, et al. Galectin-3 regulates
myofibroblast activation and hepatic fibrosis. Proc Natl Acad Sci U S A
2006;103:5060-5.
110. Zein CO, Lopez R, Fu X, et al. Pentoxifylline decreases oxidized lipid products in
nonalcoholic steatohepatitis: new evidence on the potential therapeutic mechanism.Hepatology 2012;56:1291-9.
111. Zein CO, Yerian LM, Gogate P, et al. Pentoxifylline improves nonalcoholic
steatohepatitis: a randomized placebo-controlled trial. Hepatology 2011;54:1610-9.
112. Du J, Ma YY, Yu CH, et al. Effects of pentoxifylline on nonalcoholic fatty liver
disease: a meta-analysis. World J Gastroenterol 2014;20:569-77.
113. Ratziu V, Sheikh MY, Sanyal AJ, et al. A phase 2, randomized, double-blind, placebo-
controlled study of GS-9450 in subjects with nonalcoholic steatohepatitis. Hepatology
2012;55:419-28.
114. Miura K, Yang L, van Rooijen N, et al. Hepatic recruitment of macrophages promotes
nonalcoholic steatohepatitis through CCR2. Am J Physiol Gastrointest Liver Physiol
2012;302:G1310-21.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
31/36
ACCEPTED MANUSCRIPT
115. Castellino F, Huang AY, Altan-Bonnet G, et al. Chemokines enhance immunity by
guiding naive CD8+ T cells to sites of CD4+ T cell-dendritic cell interaction. Nature
2006;440:890-5.
116. Ramaley PA, French N, Kaleebu P, et al. HIV in Africa (Communication arising):
chemokine-receptor genes and AIDS risk. Nature 2002;417:140.
117. Alonzo F, 3rd, Kozhaya L, Rawlings SA, et al. CCR5 is a receptor for Staphylococcusaureus leukotoxin ED. Nature 2013;493:51-5.
118. Chen L, Yao X, Young A, et al. Inhibition of apical sodium-dependent bile acid
transporter as a novel treatment for diabetes. Am J Physiol Endocrinol Metab
2012;302:E68-76.
119. Staels B, Handelsman Y, Fonseca V. Bile acid sequestrants for lipid and glucose
control. Curr Diab Rep 2010;10:70-7.
120. Brenner C, Galluzzi L, Kepp O, et al. Decoding cell death signals in liver
inflammation. J Hepatol 2013;59:583-94.
121. Henao-Mejia J, Elinav E, Jin C, et al. Inflammasome-mediated dysbiosis regulates
progression of NAFLD and obesity. Nature 2012;482:179-85.
122. Mouzaki M, Comelli EM, Arendt BM, et al. Intestinal microbiota in patients withnonalcoholic fatty liver disease. Hepatology 2013;58:120-7.
123. Vrieze A, Van Nood E, Holleman F, et al. Transfer of intestinal microbiota from lean
donors increases insulin sensitivity in individuals with metabolic syndrome.
Gastroenterology 2012;143:913-6 e7.
124. Smits LP, Bouter KE, de Vos WM, et al. Therapeutic potential of fecal microbiota
transplantation. Gastroenterology 2013;145:946-53.
125. Le Chatelier E, Nielsen T, Qin J, et al. Richness of human gut microbiome correlates
with metabolic markers. Nature 2013;500:541-6.
126. Staels B, Rubenstrunk A, Noel B, et al. Hepatoprotective effects of the dual
peroxisome proliferator-activated receptor alpha/delta agonist, GFT505, in rodent
models of nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. Hepatology
2013;58:1941-52.
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
32/36
ACCEPTED MANUSCRIPT
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
33/36
ACCEPTED MANUSCRIPT
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
34/36
ACCEPTED MANUSCRIPT
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
35/36
ACCEPTED MANUSCRIPT
-
8/18/2019 2016 Perspectives on Treatment for Nonalcoholic Steatohepatitis. GASTROENT
36/36
ACCEPTED MANUSCRIPT