
2015 Otolaryngology Update Chuck Reese CAPT MC USN [email protected] 850-452-3256.
34
-
Upload
leilani-bodey -
Category
Documents
-
view
220 -
download
1
Transcript of 2015 Otolaryngology Update Chuck Reese CAPT MC USN [email protected] 850-452-3256.
2015 Otolaryngology Update
Chuck Reese
CAPT MC USN
850-452-3256

Hearing Loss
Tinnitus and Hearing loss are the two most common disability claims in the military.
Together, DoD and the VA spend more than $4 Billion a year on evaluation, treatment and disability payments related to tinnitus and hearing loss.
Hearing Loss
Although the financial burden and the potential for mission impact are significant, the effect on quality of life and an individual’s diminished ability to “connect” with family and friends is perhaps even more significant.
Hearing Loss
Two basic types of hearing loss:
Sensorineural
Conductive
Combination of sensorineural and conductive is referred to as Mixed Loss
Hearing Loss
Other less common types of hearing loss are:
Somatoform
Malingering
Central

What is sound?
Sound is a physical force that results in alternating movements of the molecules of air (or whatever medium is exposed to the
sound). Measured in cycles
per second, or Hertz (HZ)

dB Source 140 Jet Engine, Gun Shot
120 Car Horn
100 Pneumatic Drill 90 Subway 80 Noisy Restaurant 75 Busy Street 65 Conversation
50 Average Home 40 Quiet Office
30 Whisper 0 Threshold of Hearing

Tympano-Cochlear schematic
From Ear Diseases, Deafness and Dizziness; V Goodhill, 1979, Harper and Row, Publishers

Classic noise-induced notch at 4 kHz

Scanning E.M., Outer Hair Cells of Cochlea, I. Hunter-Duvar, in Schuknecht, 2nd Edition Pathology of the Ear
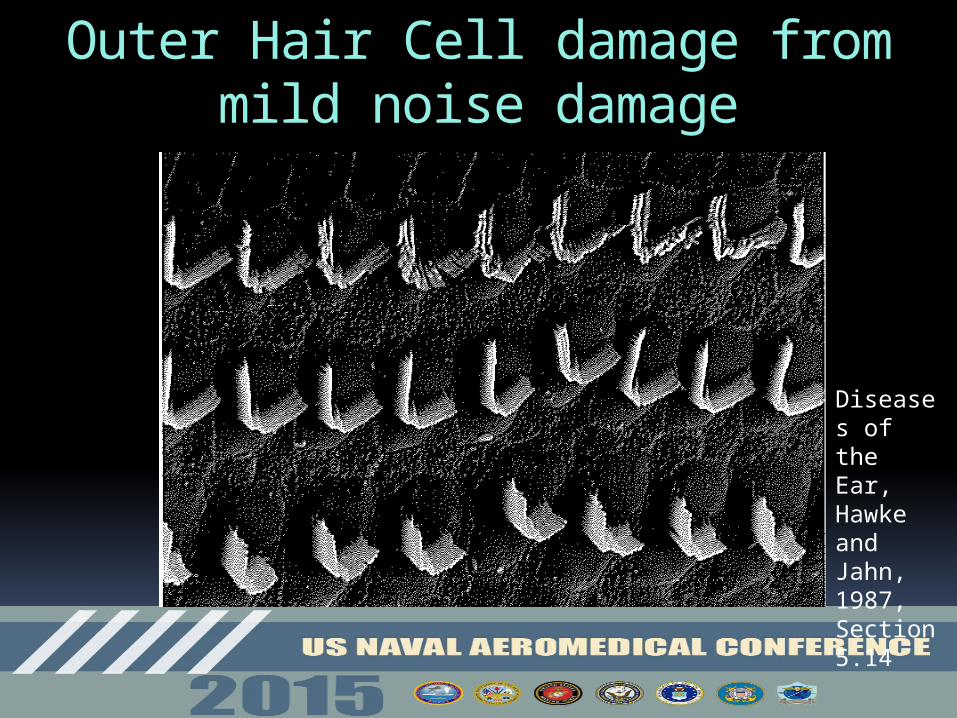
Outer Hair Cell damage from mild noise damage
Diseases of the Ear, Hawke and Jahn, 1987, Section 5.14
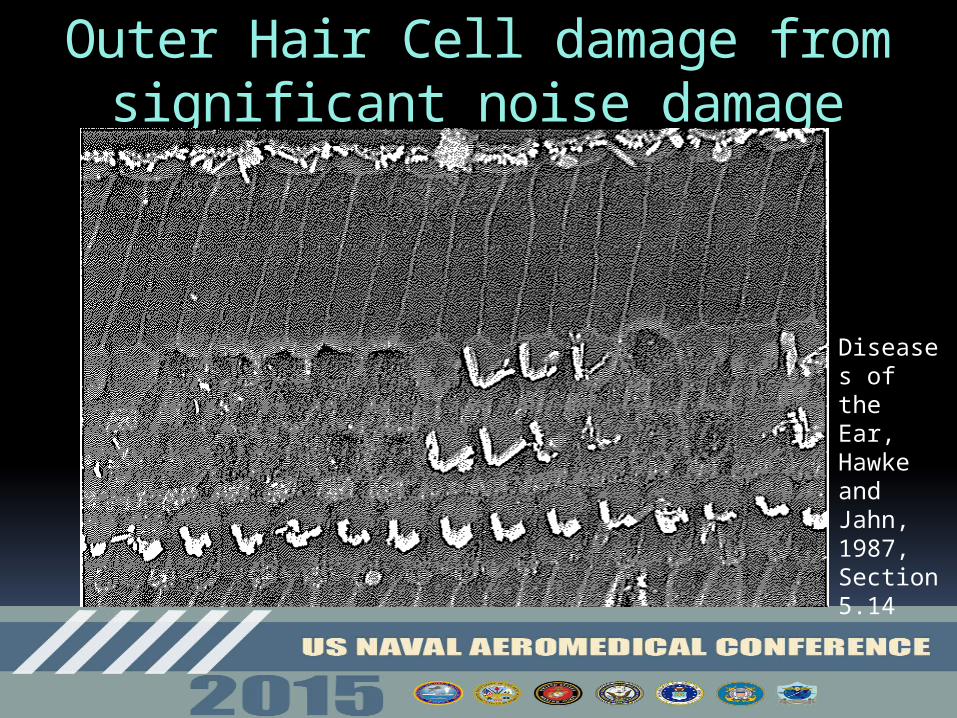
Outer Hair Cell damage from significant noise damage
Diseases of the Ear, Hawke and Jahn, 1987, Section 5.14
What did you say??
Components of Hearing Conservation Program
Noise measurements at job site
Engineering fixes if possible; otherwise, administrative controls on duration of exposure
Periodic audiograms (annual for aviation)
Hearing protection devices mandated and provided
Components of Hearing Conservation Program
New Reference Audiogram:Average of 10 dB shift at 2K, 3K and 4K HzRequires repeat testing after 14 hrs in noise free environmentSpecial reporting requirementsPossible ENT consultation
Education - counseling - motivation 15 dB drop between audiograms in single
frequency: may indicate a problem and member should be counseled

Role of the Flight Surgeon
From OPNAVINST 5100.19E:
“…..it is incumbent upon leadership to set the right example in their personal protective practices, to enforce compliance, and to ensure HCP receives their full support.”
Role of the Flight Surgeon
From OPNAVINST 5100.19E:
i. When an audiologist or a physician confirms the positive threshold shift is permanent, the individual shall be notified in writing within 21 days of such determination…….
Role of the Flight Surgeon
From OPNAVINST 5100.19E:
Supervisors shall be notified, in writing, that the worker has experienced a decrease in hearing.
Role of the Flight Surgeon
From OPNAVINST 5100.19E:
In accordance with subparagraph C7.2.1.5.4. of Reference (s), workers shall be informed, in writing, that their supervisors are notified that they have experienced a decrease in hearing.
Role of the Flight Surgeon
-Coordinate with division officers…. -Conduct training for all hands…. -Ensure annual refresher training….-Consult the command industrial hygiene survey……-Schedule personnel…. -…personnel who require hearing retests …-…ensure the certification of annual….-Report all permanent threshold shifts…-Enter into the web-enabled safety system…
From OPNAVINST 5100.19E:
(3) Any individual who has hearing loss in both ears in which the sum of thresholds at the frequencies of 3000, 4000 and 6000 Hz exceeds a total of 270 dB or has their reference hearing test (form DD 2215) re-established three times will not be assigned to duties involving exposure to hazardous noise until evaluated and waived by an audiologist, otologist, or occupational medicine physician.
Page B4-A-8

Role of the Flight Surgeon
The hearing conservation program is receiving increased scrutiny. There have been several working groups over the years and it continues to be a tough nut to crack.
The flight surgeon’s role is critical.
The AVTs and their entry of data into DOEHRS-HC is a critical component of the program. They are a crucial resource.
Sudden Idiopathic Sensorineural Hearing Loss
Incidence of 2-20 per 100,000 per year 30 dB threshold shift in 3 contiguous
frequencies occurring within 72 hours.~50% awaken with the loss
Idiopathic: Viral cochleitis, microvascular event, autoimmune
90% with tinnitus. 20-60% with vertigo
Sudden Idiopathic Sensorineural Hearing Loss Potentially a diagnostic challenge.
Patients frequently report that the ear feels blocked or plugged.Clinicians convince themselves that the drum looks retracted or red or………
You MUST remember how to use tuning forks, and more importantly, you must know where one is and you must use it!!
Sudden Idiopathic Sensorineural Hearing Loss
Approx two thirds will have some degree of spontaneous recovery
Prognosis is generally worse for a profound loss affecting all frequencies and in the presence of vertigo
Recovery most likely if treatment is initiated within days
Sudden Idiopathic Sensorineural Hearing Loss
Clinical Practice Guideline from AAO-HNSFOtolaryngol Head Neck Surg. 2012 Mar;146(3 Suppl):S1-35
-Delineate SNHL from Conductive loss.-Recommendation for offering treatment with oral glucocorticoids-Recommendation for consideration of trans-tympanic steroids for treatment failures-Recommend against treating with antivirals.-Recommend consideration of hyperbaric oxygen.-Obtain MRI of IACs to evaluate for retrocochlear lesions
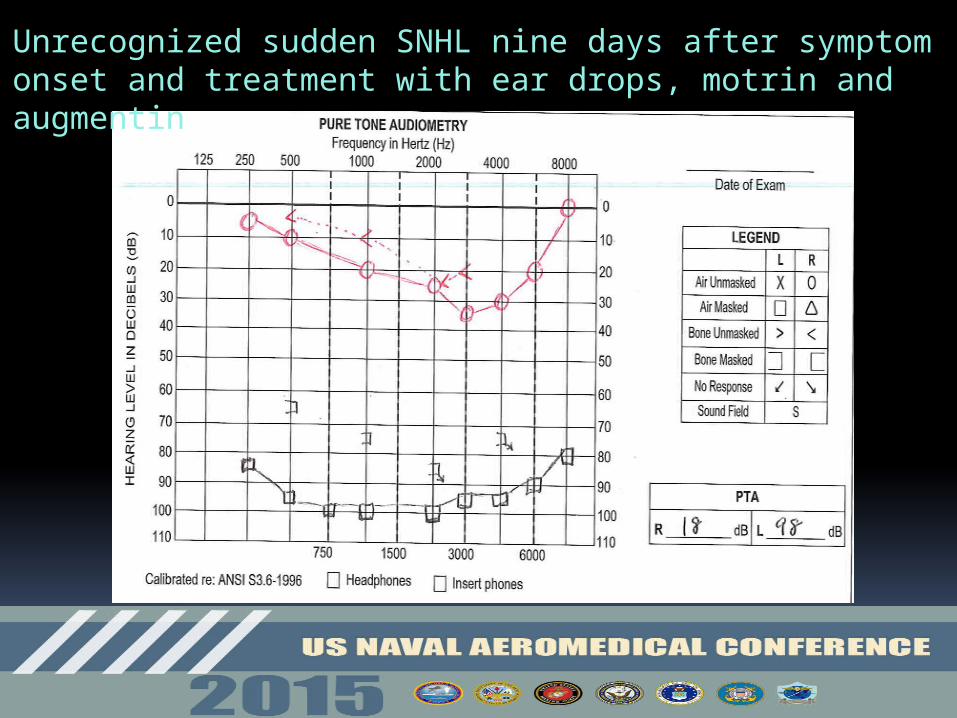
Unrecognized sudden SNHL nine days after symptom onset and treatment with ear drops, motrin and augmentin.
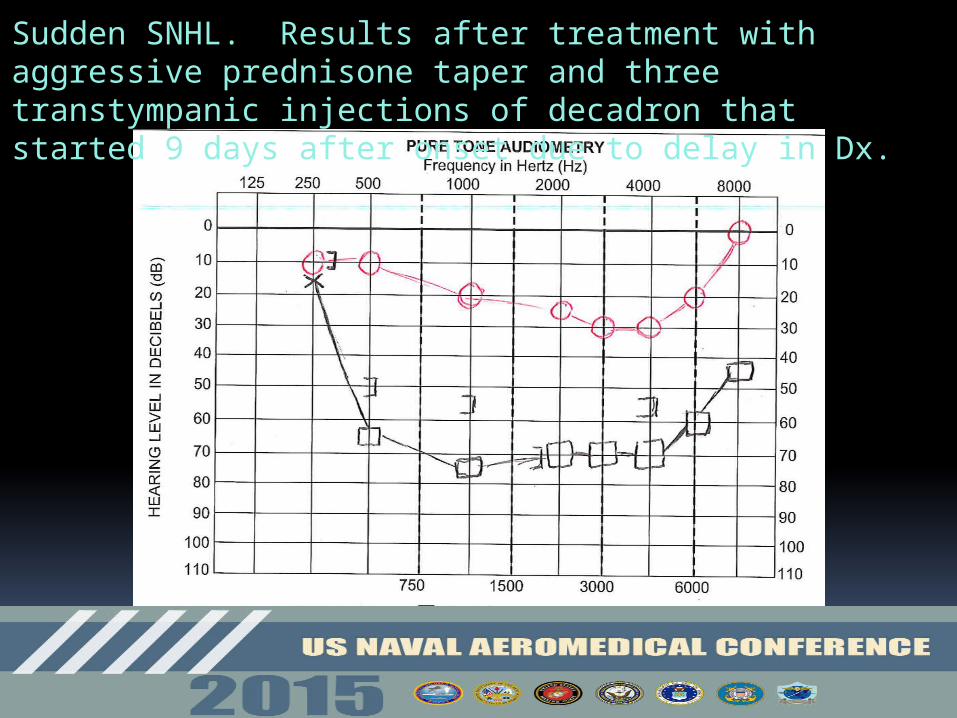
Sudden SNHL. Results after treatment with aggressive prednisone taper and three transtympanic injections of decadron that started 9 days after onset due to delay in Dx.
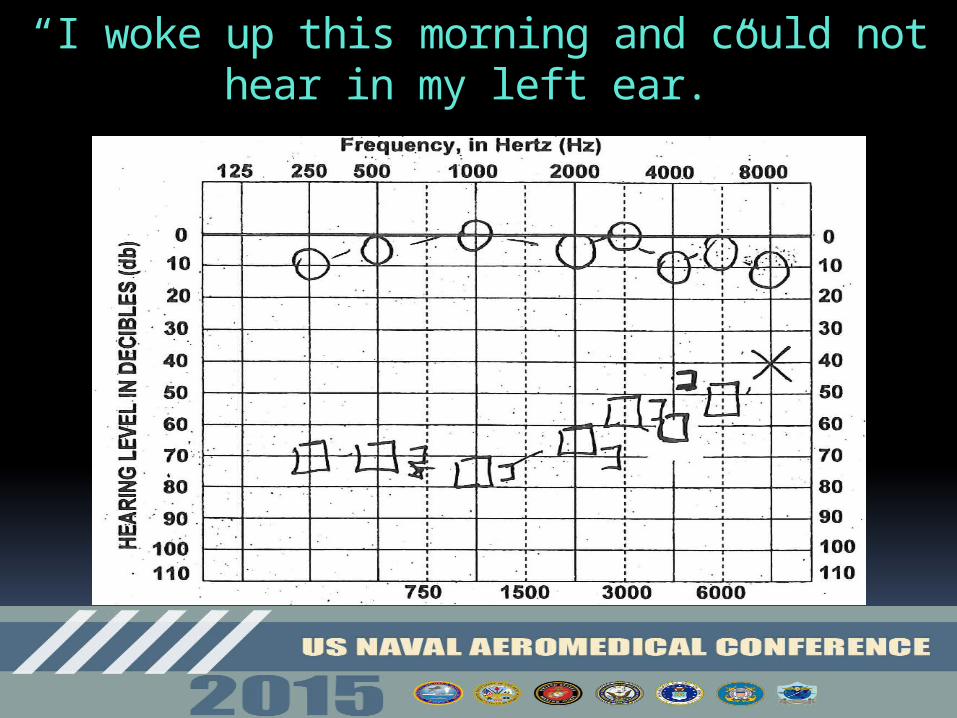
“I woke up this morning and could not hear in my left ear.”

Audiogram three weeks later after aggressive oral steroid taper.
Sudden Idiopathic Sensorineural Hearing Loss
Not everyone will have this good of a response, but you have to start with the correct diagnosis.
Simple use of tuning forks will work for you.
If in doubt, get a formal audiogram!

Finally, don’t forget to ignore the light reflex!!

Finally, don’t forget to ignore the light reflex!!

Questions?


















