
2015-2016 PGY1 Pharmacy Residency Manual
69
Page 1 revised 7/22/15 2015-2016 PGY1 Pharmacy Residency Manual Community Regional Medical Center Department of Pharmacy Services Fresno, California
Transcript of 2015-2016 PGY1 Pharmacy Residency Manual

Page 1 revised 7/22/15
2015-2016
PGY1 Pharmacy Residency Manual
Community Regional Medical Center Department of Pharmacy Services
Fresno, California
Page 2 revised 7/22/15
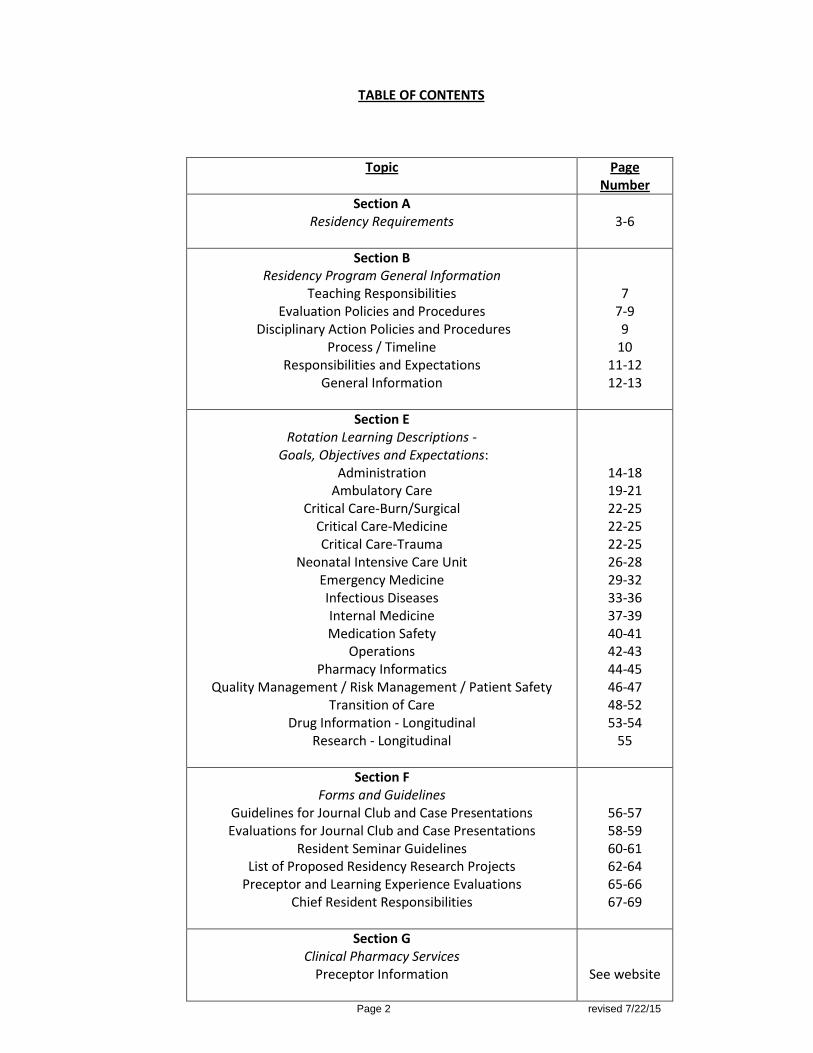
TABLE OF CONTENTS
Topic Page Number
Section A Residency Requirements
3-6
Section B Residency Program General Information
Teaching Responsibilities Evaluation Policies and Procedures
Disciplinary Action Policies and Procedures Process / Timeline
Responsibilities and Expectations General Information
7 7-9 9
10 11-12 12-13
Section E Rotation Learning Descriptions -
Goals, Objectives and Expectations: Administration
Ambulatory Care Critical Care-Burn/Surgical
Critical Care-Medicine Critical Care-Trauma
Neonatal Intensive Care Unit Emergency Medicine Infectious Diseases Internal Medicine Medication Safety
Operations Pharmacy Informatics
Quality Management / Risk Management / Patient Safety Transition of Care
Drug Information - Longitudinal Research - Longitudinal
14-18 19-21 22-25 22-25 22-25 26-28 29-32 33-36 37-39 40-41 42-43 44-45 46-47 48-52 53-54
55
Section F Forms and Guidelines
Guidelines for Journal Club and Case Presentations Evaluations for Journal Club and Case Presentations
Resident Seminar Guidelines List of Proposed Residency Research Projects
Preceptor and Learning Experience Evaluations Chief Resident Responsibilities
56-57 58-59 60-61 62-64 65-66 67-69
Section G Clinical Pharmacy Services
Preceptor Information
See website
Page 3 revised 7/22/15
SECTION A – RESIDENCY REQUIREMENTS Orientation Program and Residency meetings. A formal orientation program for all residents is
scheduled in July of each year. Attendance is mandatory. The orientation is designed to introduce the incoming residents to Community Regional Medical Center (CRMC) Pharmacy Services and to outline the expectations of the residency year. Residents must also attend the University of California, San Francisco (UCSF) Advanced Pharmacy Practice Experiences (APPEs) Preceptor Orientation, in order to serve as a co-preceptor.
Effective Communication. Residents are expected to effectively communicate with other health care
professionals in all methods of communication (e.g. verbal, phone, written, fax). Residents are expected to write progress notes in the medical record if they cannot reach the health care provider. Residents must give preceptors a minimum of 2 business days (48 hours) to review items, as a courtesy.
Drug Information / Ask the Pharmacist. Residents will become efficient in providing drug information
through comprehensive literature searches. Residents will become familiar with various references to expedite information retrieval, including dosing, adverse effects, therapeutic classes and uses, formulary drugs and alternatives to non-formulary drugs. In addition, residents will apply their skills in a service called “Ask the Pharmacist” throughout their residency year. Each resident will take turns answering questions. The Clinical Manager and the RPD are the contact persons for this service.
Presentations. Residents will participate in Journal Club, Case Presentations (or optional project), and
Resident Seminars to enhance presentation skills. A minimum of 3 presentations to the pharmacy department per year is required.
Teaching. Residents will be involved in various teaching activities, including in-services for the medical,
nursing, and/or pharmacy staff, case presentations, precepting students, and providing continuing education lectures.
Precept Pharmacy Students. Residents will serve as co-preceptors with faculty members for University
of California, San Francisco (UCSF), University of the Pacific (UOP) and other school of pharmacy students.
Residency Research Project. Each resident is expected to complete a research project, during their
residency year, designed to improve pharmacy practice. A list of potential research projects will be provided to the residents. The residents can pick a project from the list, or discuss one directly with a preceptor, and submit his/her research proposal to the Residency Program Director, Director of Pharmacy Services and preceptor(s) for approval. All projects must include a cost savings component that must be monitored. At least one preceptor must be chosen as a co-investigator for the project. All projects must be presented at the ASHP Midyear Clinical Meeting and Western States Conference, presumed publishable in a peer reviewed journal, and a CRMC “Define, Measure, Analyze, Improve and Control” (DMAIC) must be submitted.
Project selection / Scope of projects/ Approval o Each year a list of potential projects will be generated and distributed to the residents for
selection. This will allow all residents an opportunity to review all potential projects. Projects may be submitted by Pharmacy Services staff members, Clinical Pharmacists, Residents, and others, as appropriate.
o The Residency Preceptors will evaluate all project submissions for appropriateness and feasibility.

Page 4 revised 7/22/15
o Many of the projects will be conducted in support of the CRMC Department of Pharmacy Services. Residents participating in service projects originating in the Department of Pharmacy Services will follow the policies and procedures of the department.
o Each resident must submit a written research project proposal, which must be signed by the resident and preceptor and handed in to the RPD. An electronic version must also be emailed to the RPD.
Status Reports o The resident will complete a Quarterly longitudinal project evaluation form (e-value); status
reports will be emailed before the preceptor and resident meetings each month to the project preceptor and RPD to be reviewed at the Residency Preceptor Meetings.
Project Completion o The project will be considered complete when the stated objectives have been met. A
description of the results (manuscript) of the project must be written and submitted no later than the final quarterly evaluation (June 10th) before the project is considered complete. A DMAIC poster and PowerPoint must also be completed by June 10th. Projects must be reviewed before submission by the preceptors / co-investigators. A residency certificate will not be awarded until the project is completed.
Operations. All residents must participate in operational activities designed to ensure that residents
gain operational experience and understand the distribution process. To achieve this, residents are scheduled approximately 30 hours per month, in the inpatient pharmacy. If a resident misses any days of the operations staffing component due to illness or time off, then they must make up the time. If making a switch, this must be conveyed to the inpatient supervisor and RPD, and ensure all ACGME requirements are upheld -see www.acgme.org The month of December (including ASHP Midyear) and the weekend of CSHP Seminar, October 8-11, 2015 are excluded.
Journal Club and Case Presentation Discussions. Residents will present one Journal Club (JC) and one
Case Presentation (CP) during each Core Clinical rotation. It is mandatory to attend all resident JC and CP. Topics and format are up to the discretion of the preceptor. See the specific guidelines in section F. Residents are encouraged to attend student’s JC and CP, under the discretion of the preceptor.
Manuscript for Publication. Residents will prepare a manuscript of their Research Project in a format
acceptable for publication in a peer reviewed journal. The topic of this manuscript will be determined by the resident and his/her Preceptor/RPD based on the resident's background, experience and goals. Editorial assistance by a preceptor is required. Deadline is June 10th to email this to the RPD.
Pharmacy Services Documentation i-Vent. Each resident will document his/her daily interventions as i-
Vents in Epic. This is extremely important to the program to document a cost savings and improved patient care. A minimum requirement of 125 i-Vents per inpatient clinical rotation is required.
Med Checks. All CRMC inpatient rotations will have a minimum of 3 Med Checks per week completed,
and entered into i-Vents. One Med Check per patient is documented. Preceptor must observe and approve one Med Check and document into E-Value during the rotation evaluation. In addition, the “script” must be utilized. Please discuss with Rotation Preceptor for more information.
IV-to-PO Conversion. Residents are responsible for evaluating patients on the 1st floor for possible
conversion of IV medications to PO, in accordance with the IV-to-PO conversion policies and procedures (e.g. Nexium and Pepcid). This is also documented as an intervention in i-Vents in Epic.
Page 5 revised 7/22/15
Certification for Basic Life Support (BLS) and Advanced Cardiovascular Life Support (ACLS). Each resident is expected to successfully complete the BLS and ACLS curriculum within the first month of the residency. The goal is to ensure the resident is familiar with and capable of providing BLS, in the event of an emergency. ACLS is preferred prior to attending any Critical Care, or Emergency Medicine Rotations. Please access Healthstream Learning Center (HLC) or contact the Education Department to access course materials and information.
Resident Meetings. Residents will attend mandatory scheduled resident meetings to discuss upcoming
resident events, other issues pertaining to the residency program, and actions/recommendations made at preceptor meetings, etc. Meetings will be scheduled by the Chief Resident / RPD on a monthly basis.
Recruitment. Each resident will assist with the residency recruitment efforts of the department. Each
resident is a valuable source of information and advice for potential candidates. These are mandatory. o ASHP: Each resident is required to spend time providing information to interested parties during
the ASHP Midyear Clinical Meeting. Residents will staff the residency showcase. o CSHP: Same as above. o Interviews: Time will be scheduled during the interview process for interviewees to interact
with current residents. Resident interviews will be 2/4/16 and 2/11/16. Mark your calendars. o Western States Conference- Residents will help staff the recruitment table.
Pharmacy and Therapeutics (P&T). The Chief Resident is required to attend monthly P&T on the 4th
Wednesday of each month (location may vary), and disseminate the information to the residents during the monthly resident meetings. Residents are required to attend, write a monograph and present at selected P&T meetings and/or Formulary Subcommittee meetings:
o If medication is added to formulary, develop a concise, written summary of the monograph and final formulary decisions for inclusion in physician and pharmacy newsletters.
o If medication is added to formulary, assist with implementation of formulary recommendations. This may require development and follow-up of a medication use evaluation, protocol/order set development, pilot trial implementation, optimizing medical informatics and/or developing additional health care provider education.
o Contact the Clinical Manager or RPD with any questions.
Other Administrative Meetings. Residents are encouraged to attend all meetings that the current preceptor attends.
Newsletter Articles. Residents will participate in writing for the CRMC Pharmacy Newsletter. A
minimum of one Newsletter per year is required. Resident will select topic, with advice from preceptors or the Clinical Manager. Submissions and editing of the Pharmacy Newsletter articles are completed by the Clinical Manager. Residents will each choose a separate month for submission and inform the RPD of the dates.
Resident Seminar. Each resident will present one formal seminar during the residency program. See
Section F for more information. Dates scheduled for presenting are 2/18/16, 2/25/16, and 3/3/16- (from 1600-1800)
Chief Resident. Each resident will rotate through this position. See Section F for more details.
Overtime - Is required to be conveyed to the RPD via email- with the reason why, as soon as it occurs.
Please see RPD for more details.
Page 6 revised 7/22/15
Requirements for the Completion of the Residency Program
Residents are expected to satisfactorily complete all requirements of the CRMC Residency Program as listed above, adhere to the ASHP Accreditation Standards, and achieve all of the required educational Outcomes, Goals and Objectives. Residents who achieve and complete the residency requirements will receive their Residency Certificate as evidence of program completion.
Evaluation of the resident's progress in completing the requirements is done as part of the rotation and
quarterly evaluation tracking and review process.
The Resident Preceptor, in combination with the Residency Program Director and the Director of Pharmacy Services, shall assess the ability of the resident to meet the requirements and work with the resident to assure their satisfactory completion.
Completion of the Resident Research Project, subsequent manuscript, and DMAIC.
Fulfillment of essential accountabilities as defined in the Pharmacist Resident Grad Intern Job
Description 41561 and Pharmacist Resident Job Description 40741 under the Human Resources policy.

Page 7 revised 7/22/15
SECTION B – RESIDENCY PROGRAM GENERAL INFORMATION Residency Program Director (RPD): Alice Robbins, PharmD, BCPS Preceptor: Individual assigned to train, educate, and evaluate the resident in their practice area of expertise. Also may serve as a preceptor by lecturing or mentoring special projects.
Teaching Responsibilities Purpose Residents will participate in the teaching activities of the Department of Pharmacy Services. The purpose of such activities is to develop and refine the resident's communication skills, to build confidence, and to promote the effectiveness of the resident as a teacher. Procedure Teaching responsibilities may include clinical and didactic teaching for pharmacy students, medical staff and residents, hospital personnel, and pharmacy departmental staff. All residents act as co-preceptors for UCSF, UOP, or other schools of pharmacy students APPE’s (pharmacy student rotations). In addition, teaching activities may involve formal lectures, in-service presentations, or discussion sessions. Specific responsibilities will vary by service.
Residency Evaluation Policies and Procedures 1. Resident’s Self-assessment Evaluation
Each resident will assess his or her progress for the rotation by completing the assigned electronic SELF Midpoint and Summative Evaluation form online at E-Value, 3 days prior to the scheduled evaluation meeting with the preceptor. Written comments exampling the objectives with qualitative comments (How you can improve) are mandatory. This teaches the art of self reflection and self assessment.
2. Resident's Evaluation of Preceptor and Rotation
Each resident will complete a Resident's Evaluation of the Preceptor and Rotation before the end of each rotation. These evaluations will be completed on E-value.
3. Preceptor's Evaluation of the Resident’s Rotation Performance
Each Preceptor will review and electronically “sign off” on the resident’s SELF evaluation before completing their evaluation of the resident.
Each preceptor will complete an electronic Midpoint and Summative evaluation for each resident with mandatory qualitative comments (How can the resident improve). The preceptor will review and compare it to the resident’s self evaluation, electronically sign off on it within E-Value, and then will discuss it with the resident to help improve their future performance.
After this discussion, the preceptor will submit the evaluation. Residents will electronically “sign off” on the preceptors’ evaluation on their performance. Evaluations will be completed and submitted on E-Value.
4. Quarterly Evaluations
Quarterly Longitudinal Evaluation Process for All Residents The following longitudinal activities will be evaluated at least once each quarter: Operational
Pharmacy Experience, Drug Information, and Residency Projects. These are completed by the respective preceptors / evaluators.
Page 8 revised 7/22/15
Completed electronic evaluations must be completed on E-value by the following dates: October 10, January 10, April 10, and June 10. By submitting the evaluation on these dates, the Residency Program Director (RPD) can incorporate these comments into the resident's quarterly evaluation.
Resident Quarterly Progress Report All residents will complete a quarterly progress tracking report (electronically) detailing their residency
activities for the designated time period, and email the report to the RPD. The report includes progress made toward meeting goals and objectives established at the beginning of
the residency year. The quarterly report should also contain, in chronological order, a summary of the rotations completed
by the residents in that quarter. Any comments the resident would like to make regarding their achievements toward these goals should also be included.
Each resident is responsible for performing a self-evaluation on their Longitudinal Experiences on E-value. This includes the Operational Pharmacy Experience, Drug Information, and Residency Projects.
The resident will submit the quarterly progress report to the RPD and the self evaluations to E-Value by the dates designated below, or as requested. The quarterly progress report will be reviewed by the RPD and applied towards the preparation of the resident's quarterly evaluation. The RPD has the option to add a summary of overall progress.
Residency Program Director Quarterly Evaluations The RPD will evaluate the resident quarterly based upon the resident's progress and tracking report, and
overall residency performance. This evaluation will also take into account the rotation evaluations from prior preceptors. This report will evaluate the progress towards meeting goals and objectives established by the resident and RPD at the start of the residency year.
The quarterly report will be discussed with the resident and signed by both the RPD and the resident. Resident Quarterly Progress Report and Quarterly Evaluation Submission Dates Quarter Resident Quarterly Report Submission Date 1st Qtr: July 1 - September 30 October 10 2nd Qtr: October 1 - December 31 January 10 3rd Qtr: January 1 - March 30 April 10 4th Qtr: April 1 - June 30 June 10 Compliance with the Evaluation Policy
Residents must comply with the evaluation policy. This is essential for the advancement of the resident and the residency program. Failure to comply with this policy will be addressed and may result in disciplinary action by the RPD.
Summary of Residency Evaluation Responsibilities Residents Submit all Electronically (E-value)
1. Rotation Residency Learning System (RLS)-based self-assessment –Midpoint and Summative. 2. Rotation evaluation of the preceptor and rotation. 3. Quarterly progress report and Quarterly Longitudinal Evaluations on Operations, Ask the Pharmacist,
and Research Projects.
Page 9 revised 7/22/15
Preceptors (Submit all Electronically) (E-Value): 1. RLS-based resident rotation evaluations –Midpoint and Summative with qualitative commentary. 2. Case Presentations and Journal Club Evaluations - each preceptor that attends is individually responsible
for completing this on E-value. 3. Quarterly longitudinal evaluations for those preceptors in: Operations (Pharmacy Supervisor), Ask The
Pharmacist (Clinical Manager), and Research (Preceptor specific). Residency Program Director
1. Quarterly evaluation of resident, tracking progress of all educational goals and objectives.
Resident Disciplinary Action Summary Residents are expected to conduct themselves in a professional manner at all times and to follow all relevant CRMC and Residency Program policies. Disciplinary action will be taken if a resident:
Does not follow policies and procedures of CRMC, Department of Pharmacy Services, or Residency Program
Does not present him/herself in a professional manner Does not earn satisfactory progress on any of the residency goals or objectives Does not make adequate progress towards the completion of residency requirements (e.g. project,
manuscript, lecture, seminar) Performs gross negligence
Resident Disciplinary Action Policies and Procedures
Please see Human Resources Policies and Procedures in Lucidoc 1. Introductory Period Policy 2. Performance Evaluation 3. Corrective Action Policy 4. Employment Termination
Exempt employees, RN's, LVN's and Pharmacists have an introductory period of 6 months from the date of employment. Failure of an employee to meet acceptable standards of performance and/or behavior during the introductory period will result in termination. Employees in their introductory period are not eligible to utilize the grievance procedure.
Other related and pertinent policies specific to the Residency Program are also found in Lucidoc under: Human Resources Leave of Absence – Pregnancy Policy 10021 Human Resources Leave of Absence – Personal Leave 21124 Human Resources Family and Medical Leave Act / California Family Rights Act Policy 10045 Resident Guidelines for Leave of Absence 18275 Pharmacist Resident Job Description, Job Code 40741- regarding resident licensure Pharmacist Resident Grad Intern Job Description, Job Code 41561- regarding resident licensure Resident Candidate Selection 18273

Page 10 revised 7/22/15
Process / Timeline
July
1. Make arrangements for NAPLEX and CPJE exams (if not done already). 2. Residents choose a research project from an approved list and preceptor(s). 3. The resident, in conjunction with his/her potential project preceptor(s), will identify a
research project from the list of possible projects provided to the residents. A written summary of the project's goals, methods, and anticipated impact on services, signed by the project preceptor must be submitted to the residency director by August 1st.
4. Planned “Research Day” where residents get Institutional Review Board (IRB) training. July 2nd, UCSF building, room 218 from 10:30 - 11:30 AM
August
1. Residents make final decision and proposal on residency projects by August 1. 2. Choose dates for submission of Newsletter article, P&T monograph submission and
presentation to P&T and communicate these to the Clinical Manager and RPD.
September
1. Choose a topic, date and mentor for Resident Seminar. 2. Residents present the following information for research projects:
Background information, Hypothesis, Methods, Objectives / Outcomes, Statistics, Data collection tools, Timeline for completion, in preparation for IRB.
3. Start IRB submission forms (see Research Day in July). 4. Deadline for IRB submission: Completed by September 15th for IRB review on 1st
Thursday of October. 5. Complete “Needs Assessment” for Resident Seminar by September 15.
October 1. ASHP Abstract Deadline (Aug 15 to Oct 1) (see www.ashp.org for details) 2. Topic and date for Resident Seminar due on October 1st
. 3. CSHP Seminar 10/8/15 – 10/11/15 (San Diego).
November
1. Begin data collection following IRB approval. 2. Resident Seminar documentation due November 13th. If you need review, submit to
Dr. Assemi earlier for ACPE requirements (see page 61 for more information). 3. Present poster to preceptors as a lunch seminar. 4. Prepare, mock-present, and print poster for ASHP Clinical Midyear Meeting.
December
1. Present posters at ASHP Clinical Midyear Meeting 12/6-12/11/15 (New Orleans). 2. Continue data collection. 3. Reminder to work on Resident Seminar Draft and discuss with a preceptor.
February
1. Abstracts due for Western States Conference. 2. Start writing the manuscript of the Resident Research Project. 3. Resident Seminars presented 2/18/16, 2/25/16, and 3/3/16 -locations TBD. 4. Next residency class interviews –keep your schedule open (2/4/16 and 2/16/16). 5. ASHP Re-Accreditation Site Survey –February 2016, Date TBD
April/May
1. Finish data collection. 2. Prepare statistical results. 3. Present at Western States Conference (May 22 - May 25, 2016) at Paradise Point Hotel 4. Prepare research manuscript.
June
1. Prepare for end of year. 2. June 10th -Final submission of all required materials (Manuscript, DMAIC PPT, DMAIC
poster etc.)

Page 11 revised 7/22/15
Responsibilities and Expectations Professional Conduct It is the responsibility of all residents of Community Regional Medical Center (CRMC) and the profession of pharmacy to uphold the highest degree of professional conduct at all times. The resident will display an attitude of professionalism in all aspects of his/her daily practice. Time Management Each resident will learn time management techniques during their residency year. One area to highlight is adding “buffer” times to deadlines. This will allow adequate time for review of a project by a preceptor or outside party, as well as allowing time to make changes to a project. Dress Code All residents are expected to dress in appropriate professional attire when present in the institution or attending any function as a representative of CRMC. Men are expected to wear a collared shirt. All residents are expected to wear a clean, white, full length lab coat when in patient care areas (except the Emergency Department). Open-toed shoes are not to be worn within CRMC facilities. Attire should conform to the dress code stated in the CRMC policy and procedures in Lucidoc. Any specific problems with dress attire will be addressed by the resident's Preceptor or Residency Program Director. Patient Confidentiality Patient confidentiality will be strictly maintained by all residents. Any consultations concerning patients will be held in privacy with the highest concern for the patients' and families' emotional as well as physical well-being. All residents will undergo Health Insurance Portability and Accountability Act (HIPPA) training during orientation and abide by HIPPA regulations during practice. Employee Identification Badges All employees (including residents) are required to wear his/her identification badge at all times within CRMC facilities. Attendance
Residents are expected to attend all functions as required by the Residency Program, the RPD, and preceptors. The residents are responsible for their assigned operational pharmacy practice duties, and for assuring that these commitments are met in the event of an absence.
If a resident is scheduled for operational pharmacy practice for a weekend shift and calls in sick, he/she must make up the absence by working an additional weekend, or switching with a co-resident.
Residents are expected to complete all their work relating to patient care before leaving the facility. Residents are required to be on-site for a minimum of 8 hours per day.
Days Off requests should be discussed in advance with the involved preceptor and the RPD at least 2 business days in advance to assure that residency responsibilities can be fulfilled.
An excused absence is defined as a sick leave or professional leave. This must be discussed with and signed off by the rotation preceptor and RPD.
Residents are encouraged to attend UCSF pharmacy student presentations (Big Talks) scheduled at UCSF building, but are not mandatory.
Prior to licensure
Verbal Orders: Please be advised that under current pharmacy law, if a resident is NOT a CA licensed pharmacist or have a CA Intern license, they cannot take verbal orders, period. Only licensed personnel (whether it be CA licensed pharmacists or CA licensed interns) can take verbal orders. If a resident has a CA Intern License, then they can take verbal orders, but it must be co-signed by the preceptor, or a licensed pharmacist.
Page 12 revised 7/22/15
Notes in the Chart: Residents can leave progress notes in the patient chart, but it must be reviewed by the preceptor before placing in Epic per the preceptor’s discretion. If the resident is not licensed, the resident must complete an I-vent, communicate to the preceptor that an I-vent has been completed, and the preceptor will copy this into a progress note.
General Information Benefits
1. Resident Base Stipends: $20.00/hr, approximately $41,600/yr, not including overtime on weekends. 2. Paid time off (PTO): Accrued time includes 2 weeks of vacation, 9 paid holidays, and 6 discretionary
days. PTO includes personal days, vacation days, sick days, and holidays. 3. Holidays: Residents are expected to work on some designated holidays. 4. Funds for Professional Meetings: There are adequate funds available to compensate the residents
attending CSHP Seminar, ASHP Midyear, and Western States Residency Conference. 5. Health Insurance: Health insurance (medical, dental and vision) is effective Day 1 of the residency. 6. Long Term Disability: Coverage equal to 50% of your salary with elective for higher coverage. 7. Term Life Insurance: $10,000 effective the first of the month following 30 days of employment.
CRMC Employee Identification Cards
Identification of CRMC employees is necessary in order to promote recognition and communications among employees, students, patients and visitors.
While at CRMC, all employees are required to wear identification cards in a manner such that name, picture, and department are clearly visible. The ID card issued by Human Resources is the official ID card for all employees, and the employee is the only individual authorized to wear his/her ID card.
It is the responsibility of an employee who has lost his/her ID to have it replaced. The ID card is the property of CRMC, and must be surrendered upon termination of employment.
Residents are required to report the loss of their ID cards to Human Resources. Employee ID cards will be replaced by Human Resources at a cost of $5.00. This cost will be paid for by
the resident losing the card. Any employee reporting to work at CRMC without his/her official I.D. card must punch out, go home and
acquire it.
Parking
Each resident will have access to free parking in the CRMC parking structure with badge access.
Time Off Requests Requests for Days Off
Requests for days off must be emailed to the Preceptor and Residency Program Director 2 business days in advance, at minimum. Both the Preceptor and RPD must approve.
In order to maximize your learning experience in each rotation, residents are limited to 2 days off per rotation, under the discretion of the preceptor or RPD (this includes sick or personal time off).
Sick Leave
If a resident needs to take sick time, the resident must email/text/call the preceptor and notify the RPD in writing (via email).
Page 13 revised 7/22/15
Resident Holidays (8) The following are CRMC holidays. Residents can work Holidays if specifically requested by their preceptor (and approved by the RPD). Residents may also choose to work to save their PTO by staffing in the Inpatient Pharmacy. A resident may submit for time off on a holiday. The holidays are deducted from PTO. New Year's Day President’s Day Memorial Day Independence Day Labor Day Thanksgiving Day Day after Thanksgiving Christmas Day Photocopying
Copies made are only for use in the residency program. Residents may use the Department of Pharmacy Services photocopy machines located at CRMC
Pharmacy in the basement. Pharmacy Licensure for Residents
All residents must have a current and valid California intern license and subsequent Pharmacist license. For more information, please see Resident Pharmacist Job Description, Job Code 40741 regarding
resident licensure. Once licensed, a Pharmacy Resident must get a new employee badge (to reflect their current job
description). Elective Rotation requests
Rotation requests for Electives, or request for changes must be requested at least one month prior to the start of the rotation. This is to allow adequate preparation by the preceptor to accommodate any requests or changes.
Office Offices for residents are located at CRMC in the second floor annex. Please ask RPD for the code. Outside Employment Policy (Moonlighting)
The residency program is considered the primary priority of each resident. Outside employment is discouraged, but if desired, must not interfere with the resident’s
responsibilities or requirements. The responsibilities of the resident do not correspond with the normal 9:00 AM to 5:00 PM scheduled
forty-hour work week. At times, extra hours of coverage (weekends, evenings) are necessary to maintain residency requirements. Fluctuations in workload, unusual service demands or patient loads, or cross-coverage may all determine the hours of the residents’ service.
Working additional hours for CRMC in Operations outside of the residency program is considered outside employment. All outside employment must be approved by the Residency Program Director.
You must comply with ASHP duty hours: http://www.ashp.org/DocLibrary/Accreditation/Regulations-Standards/Duty-Hours.aspx
Pagers Residents will be held financially responsible for their assigned pagers (in case of loss, damage due to
neglect, etc.). Pagers must be turned in at the termination of the residency.

Page 14 revised 7/22/15
SECTION E – ROTATION GOALS/OBJECTIVES AND EXPECTATIONS Administration Rotation -Operational Activities PGY1 Resident Expectations and Responsibilities Preceptor: Tim Lopez, PharmD, Inpatient Pharmacy Manager Office: Inpatient Pharmacy Contact Information: Office x33828 General Description
Under the general management of the pharmacy manager, provide advanced and specialized administrative services to a department or division. Perform a variety of duties that require detailed functional and organizational knowledge. Coordinate administrative processes and assume a lead role on administrative projects.
Activity Goals Covered
Look up and review regulatory compliance guidelines/statutes related to:
Joint Commission National Patient Safety Goals (NPSG)
Joint Commission Medication Management (MM)
Title 22, California Board of Pharmacy Pharmacist in Charge Inpatient Self Assessment
Centers for Medicare/Medicaid Services (Conditions of Participation). The resident will identify areas for improvement for the organization after reviewing these guidelines/statutes. Lastly, the resident will recommend and write up a design to implement the changes.
R1.1
Develop a potential work flow system that would optimize the organizations ability to meet criteria according to regulatory compliance guidelines/statutes that would improve the organization from an accreditation, legal, and/or financial perspective.
R3.2

Page 15 revised 7/22/15
Administration Rotation -Medication Safety Activities PGY1 Resident Expectations and Responsibilities Preceptor: Curtis Takemoto, PharmD, Medication Safety Specialist Office: 5th Floor Annex Hours: 0800-1600 (Monday through Friday) Contact Information: x52522 or webnotify General Description The activities will emphasize concepts including but not limited to:
Introduction to Just Culture and Safety Culture
Risk management and error prevention /minimization
Reporting and analyzing medication related events (e.g. medication errors, adverse drug reactions)
Interdisciplinary systems approaches to address medication and patient safety GOALS and OBJECTIVES:
To understand the foundation of medication safety principles to facilitate patient safety.
To understand how interdisciplinary relationships involving medication safety are vital to patient care.
Understand the intercalation of the culture of safety and regulatory compliance.
To inculcate the concepts of Just Culture, medication and patient safety throughout the facility. ACTIVITIES:
Activity Goals Covered
Daily review of trigger tool and evaluation of potential medication safety events R1.1, R1.2
Identify medication errors, close calls (near misses) and adverse drug reactions R1.1, R1.2
Entering Incident Reporting Intranet System (IRIS) reports and follow up R1.1, R6.1
Attending Medication Safety related meetings including but not limited to:
CRMC Medication Management Committee meeting (monthly)
Clovis Community Medical Center (CCRMC) Medication Management Committee meeting (monthly as needed)
CRMC Quality Safety Committee (QPSC) (monthly)
Corporate Pharmacy and Therapeutics Committee (monthly as needed)
Community Behavioral Health Center (CBHC) Medication and Patient Safety Committee meeting (monthly to quarterly)
Acute Care, Home Health and Ambulatory Practice and Compliance Committee meetings (monthly as needed)
Medical-Surgical Safety Committee meeting (monthly)
Medical Staff advisory committee meetings as needed
CRMC Medication Event Subcommittee (monthly)
R3.3
Data analysis and development of medication error report for CRMC MMC, CBHC, Medication Event Subcommittee report (bi-monthly to monthly)
R1.1 R6.1
Annual revision of Medication Error Reduction and Prevention (MERP) Plan R3.2, R3.3
Participation in Medication Safety Specialist Rounds (weekly) R3.3
Contributing to the Corporate C-Safe Journal (quarterly) R4.1
Development of education tools for physicians, pharmacists, nurses, and other healthcare professionals
E2.1, E2.4
Page 16 revised 7/22/15
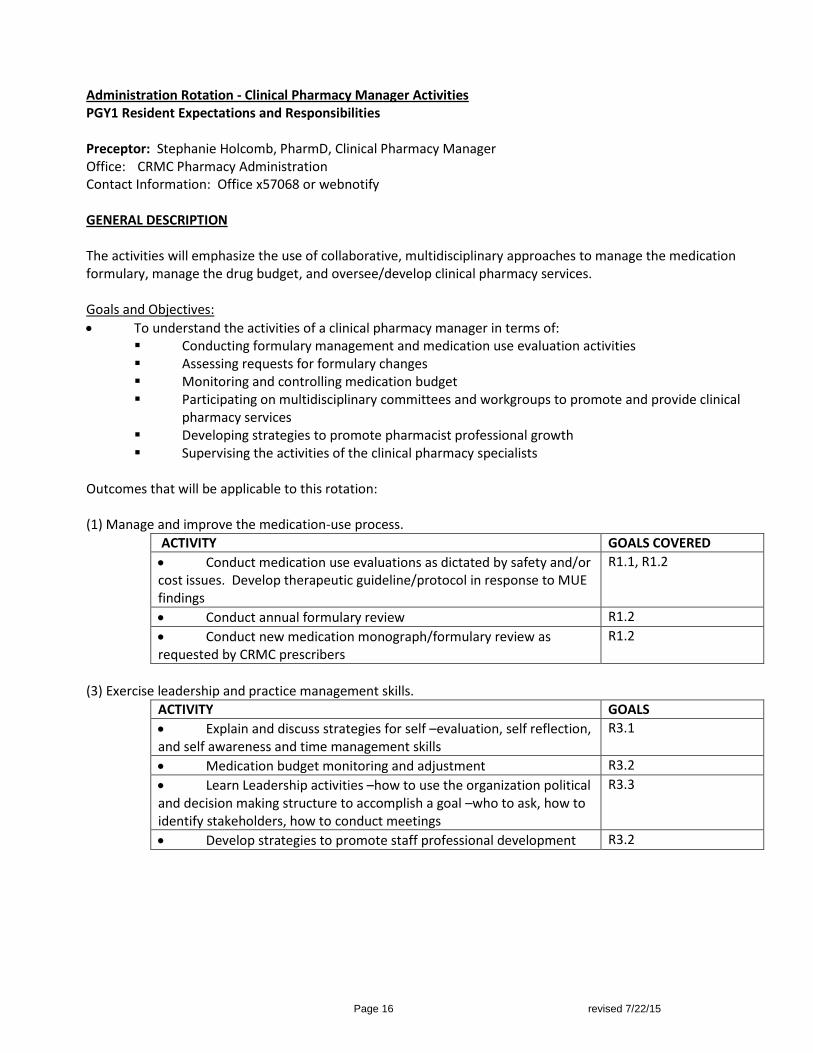
Administration Rotation - Clinical Pharmacy Manager Activities PGY1 Resident Expectations and Responsibilities Preceptor: Stephanie Holcomb, PharmD, Clinical Pharmacy Manager Office: CRMC Pharmacy Administration Contact Information: Office x57068 or webnotify GENERAL DESCRIPTION The activities will emphasize the use of collaborative, multidisciplinary approaches to manage the medication formulary, manage the drug budget, and oversee/develop clinical pharmacy services. Goals and Objectives:
To understand the activities of a clinical pharmacy manager in terms of: Conducting formulary management and medication use evaluation activities Assessing requests for formulary changes Monitoring and controlling medication budget Participating on multidisciplinary committees and workgroups to promote and provide clinical
pharmacy services Developing strategies to promote pharmacist professional growth Supervising the activities of the clinical pharmacy specialists
Outcomes that will be applicable to this rotation: (1) Manage and improve the medication-use process.
ACTIVITY GOALS COVERED
Conduct medication use evaluations as dictated by safety and/or cost issues. Develop therapeutic guideline/protocol in response to MUE findings
R1.1, R1.2
Conduct annual formulary review R1.2
Conduct new medication monograph/formulary review as requested by CRMC prescribers
R1.2
(3) Exercise leadership and practice management skills.
ACTIVITY GOALS
Explain and discuss strategies for self –evaluation, self reflection, and self awareness and time management skills
R3.1
Medication budget monitoring and adjustment R3.2
Learn Leadership activities –how to use the organization political and decision making structure to accomplish a goal –who to ask, how to identify stakeholders, how to conduct meetings
R3.3
Develop strategies to promote staff professional development R3.2
Page 17 revised 7/22/15
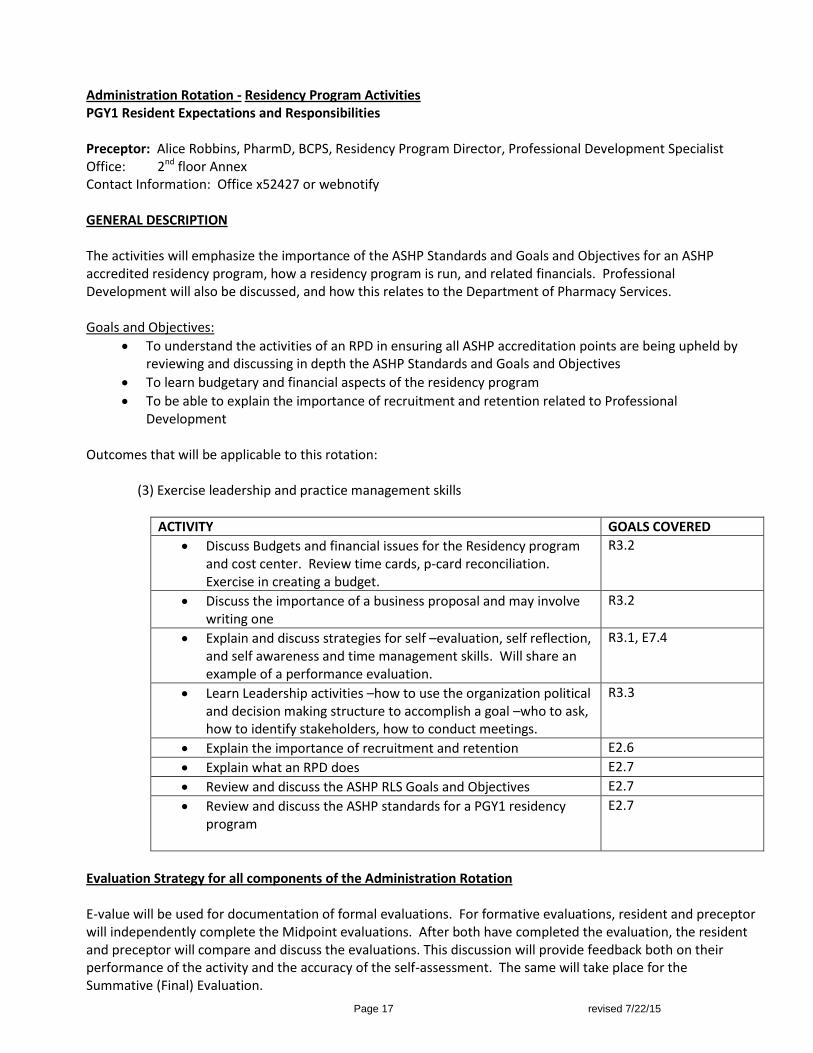
Administration Rotation - Residency Program Activities PGY1 Resident Expectations and Responsibilities Preceptor: Alice Robbins, PharmD, BCPS, Residency Program Director, Professional Development Specialist Office: 2nd floor Annex Contact Information: Office x52427 or webnotify GENERAL DESCRIPTION
The activities will emphasize the importance of the ASHP Standards and Goals and Objectives for an ASHP accredited residency program, how a residency program is run, and related financials. Professional Development will also be discussed, and how this relates to the Department of Pharmacy Services.
Goals and Objectives:
To understand the activities of an RPD in ensuring all ASHP accreditation points are being upheld by reviewing and discussing in depth the ASHP Standards and Goals and Objectives
To learn budgetary and financial aspects of the residency program
To be able to explain the importance of recruitment and retention related to Professional Development
Outcomes that will be applicable to this rotation:
(3) Exercise leadership and practice management skills
ACTIVITY GOALS COVERED
Discuss Budgets and financial issues for the Residency program and cost center. Review time cards, p-card reconciliation. Exercise in creating a budget.
R3.2
Discuss the importance of a business proposal and may involve writing one
R3.2
Explain and discuss strategies for self –evaluation, self reflection, and self awareness and time management skills. Will share an example of a performance evaluation.
R3.1, E7.4
Learn Leadership activities –how to use the organization political and decision making structure to accomplish a goal –who to ask, how to identify stakeholders, how to conduct meetings.
R3.3
Explain the importance of recruitment and retention E2.6
Explain what an RPD does E2.7
Review and discuss the ASHP RLS Goals and Objectives E2.7
Review and discuss the ASHP standards for a PGY1 residency program
E2.7
Evaluation Strategy for all components of the Administration Rotation E-value will be used for documentation of formal evaluations. For formative evaluations, resident and preceptor will independently complete the Midpoint evaluations. After both have completed the evaluation, the resident and preceptor will compare and discuss the evaluations. This discussion will provide feedback both on their performance of the activity and the accuracy of the self-assessment. The same will take place for the Summative (Final) Evaluation.
Page 18 revised 7/22/15
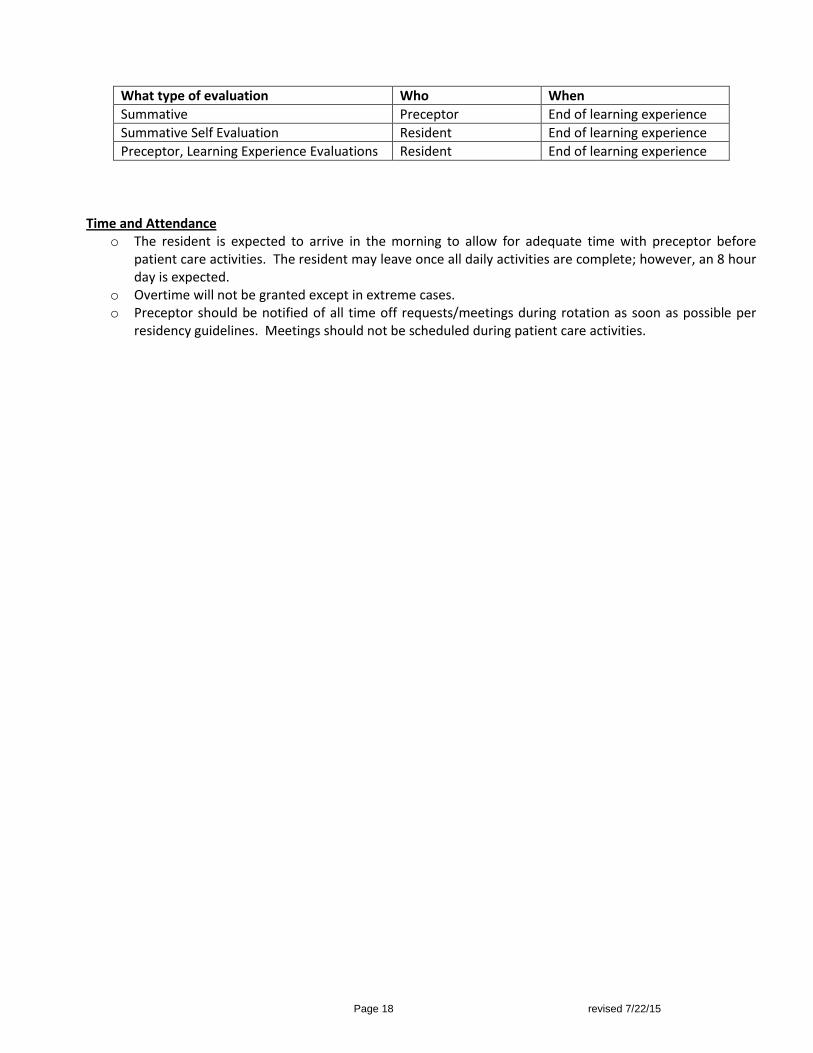
What type of evaluation Who When
Summative Preceptor End of learning experience
Summative Self Evaluation Resident End of learning experience
Preceptor, Learning Experience Evaluations Resident End of learning experience
Time and Attendance
o The resident is expected to arrive in the morning to allow for adequate time with preceptor before patient care activities. The resident may leave once all daily activities are complete; however, an 8 hour day is expected.
o Overtime will not be granted except in extreme cases. o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per
residency guidelines. Meetings should not be scheduled during patient care activities.

Page 19 revised 7/22/15
Ambulatory Care Rotation PGY1 Resident Expectations and Responsibilities Preceptors: Giovanni Lares, PharmD, BCACP (office x35193) Linda Kimura, PharmD, BCPS (pager 488-5267 / office x35030) Mallory Cruz, PharmD, BCPS (pager 488-0727 / office x35030) General Description Ambulatory Care is a core rotation for the Community Medical Center PGY1 pharmacy residency program. The Ambulatory Care Clinical Pharmacy Clinic is located at the Deran Koligian Ambulatory Care Center (ACC), and it is part of the ACC Internal Medicine Clinic. The ambulatory care clinical pharmacists, pharmacy residents, and students through a collaborative drug therapy and disease management agreement work as part of the interdisciplinary team that also includes the attending physicians, medical residents, interns, students, nurses, nurse practitioners, and physician assistants. The ambulatory care clinical pharmacy program focuses primarily on the following areas: anticoagulation, chronic pain, diabetes management, smoking cessation, hypertension, and dyslipidemia, but also provides pharmaceutical care supports for both internal medicine clinic and other specialty clinics. The pharmacy residents, under the supervision of the ambulatory care clinical pharmacists, are expected to participate in the management of chronic drug therapies and disease states, document all patient encounters in the medical charts, and provide education to patients as well as the clinical staff. They are also expected to identify and make recommendations for drug-related problems and cost-effective therapy. Development of time management, organizational, communication, and interview skills are essential for a successful experience in the ambulatory care pharmacy rotation. Disease States Common disease states in which a resident will be expected to gain knowledge and proficiency through self-directed learning, literature review, topic discussions and/or direct patient care experience include, but are not limited to: cardiovascular, cerebrovascular, diabetes, pain management, asthma, COPD, thyroid diseases, peptic ulcer disease, GERD, osteoarthritis, rheumatoid arthritis, gout, psychiatric disorders, dermatology, and infectious diseases.
Activity Goals Covered
Outcome R1: Manage and improve the medication-use process.
Identify opportunities for improving the organizations’ medication use system
Provide drug information to physicians, physician assistants, nurses, and other health care professionals at the internal medicine clinic
R1.1 R1.5
Outcome R2: Provide evidence-based, patient-centered medication therapy management with interdisciplinary teams
The pharmacy resident is expected to function as an integral member of the interdisciplinary team in the internal medicine clinic during his/her rotation
Perform medication therapy management (review of medications for drug-drug interactions, duplicate therapy, side effect; medication therapy monitoring; adherence; patient education) for chronic diseases such as diabetes and chronic pain
R2.1 R2.3 R2.4 R2.5 R2.6 R2.7 R2.8
Page 20 revised 7/22/15
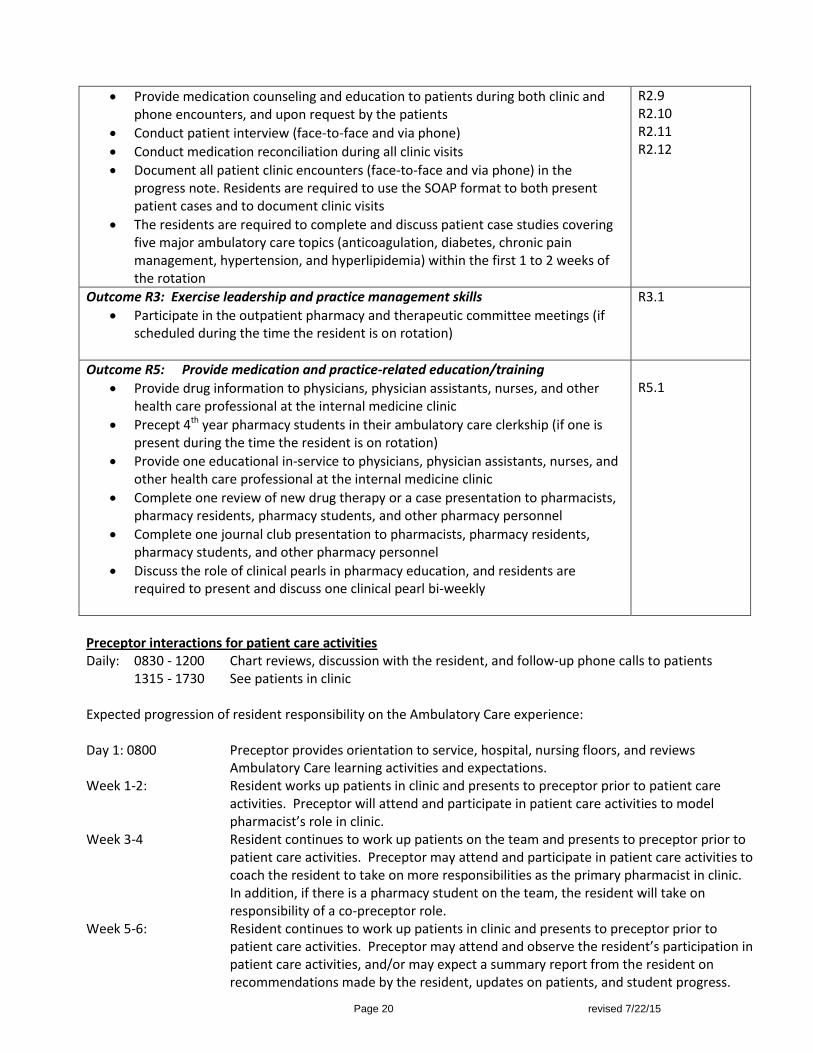
Provide medication counseling and education to patients during both clinic and phone encounters, and upon request by the patients
Conduct patient interview (face-to-face and via phone)
Conduct medication reconciliation during all clinic visits
Document all patient clinic encounters (face-to-face and via phone) in the progress note. Residents are required to use the SOAP format to both present patient cases and to document clinic visits
The residents are required to complete and discuss patient case studies covering five major ambulatory care topics (anticoagulation, diabetes, chronic pain management, hypertension, and hyperlipidemia) within the first 1 to 2 weeks of the rotation
R2.9 R2.10 R2.11 R2.12
Outcome R3: Exercise leadership and practice management skills
Participate in the outpatient pharmacy and therapeutic committee meetings (if scheduled during the time the resident is on rotation)
R3.1
Outcome R5: Provide medication and practice-related education/training
Provide drug information to physicians, physician assistants, nurses, and other health care professional at the internal medicine clinic
Precept 4th year pharmacy students in their ambulatory care clerkship (if one is present during the time the resident is on rotation)
Provide one educational in-service to physicians, physician assistants, nurses, and other health care professional at the internal medicine clinic
Complete one review of new drug therapy or a case presentation to pharmacists, pharmacy residents, pharmacy students, and other pharmacy personnel
Complete one journal club presentation to pharmacists, pharmacy residents, pharmacy students, and other pharmacy personnel
Discuss the role of clinical pearls in pharmacy education, and residents are required to present and discuss one clinical pearl bi-weekly
R5.1
Preceptor interactions for patient care activities Daily: 0830 - 1200 Chart reviews, discussion with the resident, and follow-up phone calls to patients
1315 - 1730 See patients in clinic Expected progression of resident responsibility on the Ambulatory Care experience: Day 1: 0800 Preceptor provides orientation to service, hospital, nursing floors, and reviews
Ambulatory Care learning activities and expectations. Week 1-2: Resident works up patients in clinic and presents to preceptor prior to patient care
activities. Preceptor will attend and participate in patient care activities to model pharmacist’s role in clinic.
Week 3-4 Resident continues to work up patients on the team and presents to preceptor prior to patient care activities. Preceptor may attend and participate in patient care activities to coach the resident to take on more responsibilities as the primary pharmacist in clinic. In addition, if there is a pharmacy student on the team, the resident will take on responsibility of a co-preceptor role.
Week 5-6: Resident continues to work up patients in clinic and presents to preceptor prior to patient care activities. Preceptor may attend and observe the resident’s participation in patient care activities, and/or may expect a summary report from the resident on recommendations made by the resident, updates on patients, and student progress.

Page 21 revised 7/22/15
Preceptor will always be available via pager, phone or cell for questions, and may follow patients independently to monitor resident skill development in all aspects of the learning experience to help facilitate the resident as the pharmacist in the clinic.
[The length of time the preceptor spends in each of the phases of learning will depend BOTH on the resident’s progression in the current rotation and where the rotation occurs in the residency program] Evaluation Strategy E-value will be used for documentation of formal evaluations. For formative evaluations, resident and preceptor will independently complete the Midpoint evaluations. After both have completed the evaluation, the resident and preceptor will compare and discuss the evaluations. This discussion will provide feedback both on their performance of the activity and the accuracy of the self-assessment. The same will take place for the Summative (Final) Evaluation.
What type of evaluation Who When
Formative (Midpoint) Self Evaluation Resident End of week 3
Formative (Midpoint) Preceptor End of week 3
Summative Preceptor End of learning experience
Summative Self Evaluation Resident End of learning experience
Preceptor, Learning Experience Evaluations Resident End of learning experience
Time and Attendance
o The resident is expected to arrive in the morning to allow for adequate time with preceptor before patient care activities. The resident may leave once all daily activities are complete; however, an 8 hour day is expected.
o Overtime will not be granted except in extreme cases. o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per
residency guidelines. Meetings should not be scheduled during patient care activities.
Page 22 revised 7/22/15
Critical Care Rotation (Burn/Surgery, Medicine, or Trauma) PGY1 Resident Expectations and Responsibilities Preceptors: Burn/Surgery - Melissa Reger, PharmD, BCPS (Pager 488-5567/ Office x33788) Medicine Blue / Gold - Tou Bee Thao, PharmD, BCPS (Pager 488-0079 / Office x57205) Trauma - Ann Vu, PharmD, BCPS (Pager 488-0502 / Office x57231)
General Description
The Critical Care Rotation is a core rotation for the Community Regional Medical Center PGY1 pharmacy residency program. Each resident will choose one area of critical care before the start of the residency program, on a first come, first served basis. There are six mixed medical-surgical intensive care units (ICU; 4 South, 4 North, Cardiovascular Care Unit, 5South, 5 North and the Burn Unit). Approximate average medicine ICU (MICU) daily census of 12 patients per team (2 MICU teams – MICU Blue and MICU Gold), surgical ICU (SICU) daily census of 5 - 10 patients, trauma ICU (TICU) daily census of 10 - 20 patients and Burn daily census of 5 - 10 patients . Rotations are associated with academic medical or surgical teams in a “closed” ICU setting. Thus patients are cared for by an intensivist-run critical care medicine service or a surgical service with multidisciplinary input from nursing, pharmacy, respiratory therapy, dietary, physical therapy, social work and others. Disease States
Understand and be able to effectively discuss ICU disease states and pharmacotherapy. Common disease states in which a resident will be expected to gain knowledge and proficiency through self-directed learning, literature review, topic discussions and/or direct patient care experience include, but are not limited to:
Cardiovascular dysfunction (e.g. hypertensive emergency, shock syndromes, hemodynamics, acute coronary syndromes, heart failure, cardiac arrest);
Respiratory dysfunction (e.g. asthma exacerbations, chronic obstructive pulmonary disease, pulmonary embolism, acute respiratory distress syndrome);
Metabolic and endocrine derangement (e.g. fluid and electrolyte management, nutrition support, renal failure, diabetic ketoacidosis, adrenal insufficiency, acid/base disorders);
Infectious diseases (e.g. pneumonia, severe sepsis, others);
Gastrointestinal dysfunction (e.g. gastrointestinal bleeding, stress ulcer prophylaxis, liver failure and complications);
Nervous system (e.g. seizure disorders, intracranial hemorrhages, subarachnoid hemorrhages, pain and sedation, neuromuscular blockade).
Trauma and Burn/Surgery topics (in addition to or in replacement of the above topics- per preceptor discretion)
Traumatic brain injury, spinal cord injury, post-trauma vaccinations, drug/food interactions, patient-controlled analgesia (PCA), compartment syndrome, antibiotic prophylaxis (in the operating room (OR)), blunt vascular injury, open fracture management, burn wound management.
Activity Goals Covered
Collect and organize all necessary patient-specific information to develop therapeutic assessment and plan (as described below)
R2.4
Review patient past medical history, current compliance, radiology results, laboratory results, vital signs, etc to:
o Identify and prioritize patient problem list (commonly organized by organ system)
R2.6 R2.7
Page 23 revised 7/22/15
o Identify potential drug-induced problems o Develop therapeutic care plan (pharmaceutical and non-pharmaceutical) to treat
high-priority problems. o Evaluate follow-up medication levels, laboratory values and/or vitals and modify
therapeutic plan as needed.
Review patient medication profiles for: o Medications used with no medical indication o Medical conditions for which there is no medication prescribed o Appropriate medication selection and dosing for allergies, co-morbidities and
drug-drug interactions o Appropriate prescribing (i.e. correct dose, dosage form, duration, schedule, route
of administration, method of administration, etc.) o Therapeutic duplications o Drug-drug interactions, drug-nutrient interactions and/or drug-device interactions
(including social, recreational, nonprescription or nontraditional medications potentially used prior to admission)
o Anticipated duration of therapy o Necessary monitoring parameters o Compliance with institution’s medication formulary. Cost-effectiveness
considerations
R2.4
Pre-rounding: o Gain expertise in developing and verbalizing patient-specific active problem list as
well as therapeutic goals o Design a patient-centered regimen to achieve evidence-based therapeutic goals
(considered all items listed above) o Design a patient-centered monitoring plan to ensure achievement of therapeutic
goals. Redesign care plan as necessary based on monitoring data and therapeutic outcomes
o Identify high priority recommendations and appropriate time course to intervene o Identify relevant literature to support therapeutic recommendations o Anticipate health care team therapeutic disagreements and develop convincing,
evidence-based arguments in support of recommendations
R1.5 R2.2 R2.7 R2.8 R2.9 R2.10 R2.11
Rounding with multi-disciplinary team: o Establish collaborative working relationship with members of a multidisciplinary
health care team o Learn appropriate strategies to implement different types of recommendations
(e.g. via intern versus resident versus fellow versus attending physicians) o Adjust recommendations based on additional information provided at point of
care o Serve as drug information resource o Discriminate between requestor’s statement of need and the actual drug
information need by asking for appropriate additional information o Identify urgency of question, appropriate literature resource, and appropriate
method of response o Evaluate the utility of the literature gathered and formulate a response based on
highest quality, applicable literature o Follow up on patient-specific outcomes of drug information provided o Possible order entry at point of care o Take over responsibilities as the primary pharmacist on service
R1.3 R1.4 R1.5 R2.1 R2.7 R2.8 R2.10 R2.12 R3.1
Page 24 revised 7/22/15
Topic discussions: o Review discovered and/or provided literature o Participate in preceptor-facilitated discussion of literature o Learn fluency in critical care controversies
R2.7
Educational activities (journal clubs, case presentations, in-services, topic discussions): o Identify current controversies in literature (journal club) or in a specific patient
care (case presentation) o Identify relevant literature o Critically evaluate literature and how they add information/clarity to area of
controversy o Use public speaking skills to effectively communicate educational goals o Use audio-visual aids and handouts to enhance communication of educational
goals
R5.1
Precept pharmacy students (when applicable) o Serve as pre-rounding preceptor o Facilitate/Lead topic discussions o Assist the student in following up on patient issues following rounds o Identify and implement the four preceptor roles as appropriate for the student
and the activity (direct instruction, modeling, coaching and facilitation) o Contribute to the students’ evaluations
R5.1
Appropriately select direct patient-care activities for documentation
R2.12
Possibly participate in the management of medical emergencies
R5.1
Conduct periodic self-assessments to practice self-managed professional development
R3.1
Character: o Demonstrate pride in and commitment to the profession through appearance and
professional personal contacts o Act ethically in the conduct of all job-related activities
R3.1
Preceptor interactions for rounding services -(these are guidelines and may be modified as needed by the preceptor) Burn/Surgery: Daily: 0830 Pre-rounds with resident
0930 Team Rounds -will vary depending on the OR schedule and other responsibilities of the SICU and Burn teams
After rounds-TBD Preceptor office hours: See topic discussion schedule (provided on day 1) for list of dates/times of topic discussions, and preceptor is available at other times as needed for reviewing progress notes, patient updates, etc.
MICU: Daily: 0800 Pre-rounds with resident 0930 Team Rounds
TBD Preceptor office hours: See topic discussion schedule (provided on day 1) for list of dates/times of topic discussions, and preceptor is available at other times as needed for reviewing progress notes, patient updates, etc.
TICU: Daily: 0830 Pre-rounds with resident
Page 25 revised 7/22/15
0930 Team Rounds -will vary depending on the OR schedule and other responsibilities of the trauma team
After rounds-TBD Preceptor office hours: See topic discussion schedule (provided on day 1) for list of dates/times of topic discussions, and preceptor is available at other times as needed for reviewing progress notes, patient updates, etc.
Expected progression of resident responsibility on the Critical Care experience: Day 1: 0800 Preceptor provides orientation to service, hospital, nursing floors, and reviews Critical
Care learning activities and expectations. Week 1-2: Resident works up patients on the team and presents to preceptor prior to team
rounds. Preceptor will attend and participate in team rounds to model pharmacist’s role on the team.
Week 3-4 Resident continues to work up patients on the team and presents to preceptor prior to team rounds. Preceptor may attend and participate in team rounds to coach the resident to take on more responsibilities as the primary pharmacist on the team. In addition, if there is a pharmacy student on the team, the resident will take on responsibility of a co-preceptor role.
Week 5-6: Resident continues to work up patients on the team and presents to preceptor prior to team rounds. Preceptor may attend and observe the resident’s participation in team rounds, and/or may expect a summary report from the resident on recommendations made by the resident, updates on patients, and student progress. Preceptor will always be available via pager, phone or cell for questions, and may follow patients independently to monitor resident skill development in all aspects of the learning experience to help facilitate the resident as the pharmacist on the team.
[The length of time the preceptor spends in each of the phases of learning will depend BOTH on the resident’s progression in the current rotation and where the rotation occurs in the residency program] Evaluation Strategy E-Value will be used for documentation of formal evaluations. For formative evaluations, resident and preceptor will independently complete the Midpoint evaluations that are Qualitative and Quantitative. After both have completed the evaluation, the resident and preceptor will compare and discuss the evaluations. This discussion will provide feedback both on their performance of the activity and the accuracy of the self-assessment. The same will take place for the Summative (Final) Evaluation.
What type of evaluation Who When
Formative (Midpoint) Self Evaluation Resident End of week 3
Formative (Midpoint) Preceptor End of week 3
Summative Preceptor End of learning experience
Summative Self-Evaluation Resident End of learning experience
Preceptor, Learning Experience Evaluations Resident End of learning experience
Time and Attendance
o The resident is expected to arrive in the morning to allow for adequate pre-rounding time with preceptor before rounds. The resident may leave once all daily activities are complete; however, an 8 hour day is expected.
o Overtime will not be granted except in extreme cases. o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per
residency guidelines. Meetings should not be scheduled during patient care activities.
Page 26 revised 7/22/15
Neonatal Intensive Care Unit Learning Activities: PGY1 Resident Expectations and Responsibilities Preceptors: Harlan Husted, PharmD, BCPS (Pager 488-5463 / Office x56295) George Lien, M.S., PharmD, BCPS (Pager 488-0467 / Office x56295) Hours: 8 - 4:30
1) General Description Neonatal Intensive Care Unit (NICU) is an elective, four week learning experience at Community Regional Medical Center and is offered in the Spring for all PGY1 Pharmacy Residents. There are 84 NICU beds in the hospital. There is one NICU teaching team, which includes an attending physician, a PGY2 or PGY3 medical resident, a PGY1 medical intern, and medical students (MSIII or MSIV). Other disciplines on the team include the clinical pharmacy specialist, pharmacy students, a respiratory therapist, a clinical dietitian and the primary nurse. Non-teaching teams are primarily hospitalist-based and pharmacists work regularly with them to identify and resolve medication-related problems for all patients. The pharmacy resident is responsible for identifying and resolving medication therapy issues for patients and will work toward assuming care of all patients on the unit throughout the learning experience. The resident will provide and document therapeutic drug monitoring services for patients on their team receiving drugs requiring monitoring including, but not limited to, aminoglycosides and vancomycin. Documentation must be completed on the day service was provided. The resident is responsible for providing and documenting discharge medication education to patients on their team who are pending discharge. Education and documentation must be provided no later than the day of discharge. The resident is responsible for completing non-formulary drug consults, within 48 hours of the request. Good communication and interpersonal skills are vital to success in this experience. The resident must devise efficient strategies for accomplishing the required activities in a limited time frame. 2) Disease States Common disease states in which the resident will be expected to gain proficiency through literature review, topic discussion, and/or direct patient care experience include, but are not limited to:
Cardiovascular disorders o Anatomic complications/surgical interventions, patent ductus arteriosus, transposition
of great vessels, hypoplastic left heart, Tetrology of Fallot
Critical care pharmacotherapy o Pressor agents, glycemic control, respiratory therapy (including ventilator support and
types), Neonatal Resuscitation Protocol
Gastrointestinal disorders o Gastroschisis/omphalocele, short-gut syndrome, nutrition overview including breast-
feeding, impact of medications on pregnancy/lactation, fortified nutritional supplements and total parenteral nutrition
Infectious diseases o Sepsis, meningitis, necrotizing enterocolitis, immunizations
Organ dysfunction o Retinopathy of prematurity, anemia of prematurity
Respiratory disorders o Apnea of prematurity, bronchopulmonary dysplasia/chronic lung disease, persistent
pulmonary hypertension

Page 27 revised 7/22/15
3) Goals and Objectives See Neonatal Intensive Care Unit summative evaluation for goals and objectives assigned to this learning experience.
4) Activities
Activity Goals Covered
Accurately gather, organize, and analyze patient specific information on assigned patients prior to pre-rounds with preceptor. For non-teaching services, review profiles to identify medication-related problems to discuss with hospitalist
R1.4 R2.2 R2.4 R2.6
Meet with preceptor for pre-rounds @ 10:00 daily for teaching services. For non-teaching services, meet with preceptor for pharmacy rounds @10:00 daily
R2.6 R2.7
Actively participate in NICU teaching service team rounds @ 11:00 daily. For non-teaching services, call or meet with each hospitalist covering services to resolve issues. (May round with them when feasible)
R2.3 R2.6 R2.11
Compose an accurate, concise progress note documenting direct patient care activities within time frame to be useful
R2.12
Complete consults for non-formulary drugs, recommending formulary, cost-effective alternative drug therapy to health care providers when possible
R1.2 R1.4
Provide and document therapeutic drug monitoring services for patients receiving drugs requiring monitoring including, but not limited to, aminoglycosides, vancomycin and erythropoietin
R2.7 R2.8 R2.9 R2.10
Identify and report medication events (ADE or medication errors). May be initiated by pharmacy personnel or by other health care professionals
R1.1
Participate in MUE activities or other outcome measures for patients on service
R1.1
Attend teaching discussion sessions in afternoons when applicable E7.4 R3.1
Respond to team, patient or family requests for drug information, and document question and response in the DI database on a timely basis
R1.5
Provide weekly “mini-in-service” drug information on rounds on topics requested by the team
R1.5 R5.1
5) Preceptor Interaction for rounding services Daily: 8:00 Assignment delegation for daily tasks 10:00 Pre-rounding with resident
11:00 Team rounds with resident and team 13:00 – 16:00 Preceptor office hour available for topic discussions, reviewing progress notes,
patient updates, etc.

Page 28 revised 7/22/15
Expected progression of resident responsibility on this learning experience: Day 1: 8:00 Preceptor to review NICU learning activities and expectations with resident. Week 1: Resident to work up assigned patients and present to preceptor prior to team rounds.
Preceptor will attend and participate in team rounds (modeling pharmacist’s role on the health care team).
Weeks 2-3: Resident to work up assigned patients and present to preceptor prior to team rounds. Preceptor may attend and participate in team rounds (coaching the resident to take on more responsibilities as the pharmacist on the team).
Week 4: Resident to work up assigned patients and present to preceptor prior to team rounds. Preceptor may attend and observe the resident’s participation in team rounds, and/or may expect a summary report from the resident regarding rounding activities and use of recommendations made by the resident. Preceptor will always be available for questions and will follow patients independently to monitor resident skill development in all aspects of the learning experience (facilitating the resident as the pharmacist on the team).
[The length of time the preceptor spends in each of the phases of learning will depend BOTH on the resident’s progression in the current rotation and where the rotation occurs in the residency program]
6) Evaluation Strategy E-value will be used for documentation of formal evaluations. For formative evaluations, resident and preceptor will independently complete the Midpoint evaluations that are Qualitative and Quantitative. After both have completed the evaluation, the resident and preceptor will compare and discuss the evaluations. This discussion will provide feedback both on their performance of the activity and the accuracy of the self-assessment. The same will take place for the Summative (Final) Evaluation.
What type of evaluation Who When
Formative (Midpoint) Self Evaluation Resident End of week 2
Formative (Midpoint) Preceptor End of week 2
Summative Preceptor End of learning experience
Summative Self Evaluation Resident End of learning experience
Preceptor, Learning Experience Evaluations Resident End of learning experience
Time and Attendance
o The resident is expected to arrive in the morning to allow for adequate pre-rounding time with preceptor before rounds. The resident may leave once all daily activities are complete; however, an 8 hour day is expected.
o Overtime will not be granted except in extreme cases. o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per
residency guidelines. Meetings should not be scheduled during patient care activities.
Page 29 revised 7/22/15
Emergency Medicine Rotation PGY1 Resident Expectations and Responsibilities Preceptors: Gillian Pineda, PharmD, BCPS (Pager 488-5268 / Office x35132) Leonard Valdez, PharmD, BCPS (Pager 488-5070 / Office x35132) Hours: 1000 – 1830 General Description Emergency Medicine (EM) is a core rotation for the Community Regional Medical Center PGY1 pharmacy residency program. The primary goal of this rotation is to provide a clinical pharmacy practice environment for the resident to apply the clinical, communication, and teaching skills necessary to interact in a multidisciplinary emergency medicine environment. The practice environment will require daily interactions with physicians, mid-level practitioners, nursing staff, pharmacy staff and other healthcare professionals as necessary to optimize pharmacotherapy for patients. The major challenges for this rotation is the dynamic and often chaotic environment in the emergency department, time management, and experiencing a broad variety of patients and disease states. Disease States Common disease states in which a resident will be expected to gain knowledge and proficiency through self-directed learning, literature review, topic discussions and/or direct patient care experience include, but are not limited to:
Cardiovascular ACS (AMI vs. unstable angina) Acute CHF CPR/ACLS Dysrhythmias Hypertensive urgency/emergency
CNS CVA/TIA (Thromboembolic vs. ischemic) Elevated intracranial pressure Meningitis Seizures Spinal cord injury Endocrine Adrenal insufficiency DKA Myxedema Thyrotoxicosis GI Appendicitis Cholecystitis Constipation Diarrhea Obstruction Pancreatitis Ulceration
Pulmonary Asthma COPD Pneumonia (Aspiration vs. CAP vs. HAP) Pulmonary edema Pulmonary embolus Rapid sequence intubation
Renal UTI vs. pyelonephritis Renal calculi Toxicology Acetaminophen Alcohol Aspirin Opiates Sympathomimetics/Hallucinogenics
(amphetamines/phencyclidine/cocaine) Tricyclic antidepressants Antidotes
Decontamination

Page 30 revised 7/22/15
Activity Goals Covered
1. Demonstrate knowledge of therapeutic principles related to emergency medicine topics, including, but not limited to: A. Advanced cardiac life support (ACLS) B. Cardiovascular system [e.g. acute myocardial infarction (MI), unstable angina,
acute congestive heart failure (CHF), arrhythmias, hypertensive crisis] C. Central nervous system [e.g. CVA, TIA (thromboembolic versus ischemic)] D. Pulmonary system [e.g. asthma, COPD, pneumonia, pulmonary edema,
pulmonary embolus] E. Endocrine system [e.g. adrenal insufficiency, diabetic ketoacidosis (DKA),
myxedema, coma, thyrotoxicosis] F. GI system [e.g. obstruction, appendicitis, cholecystitis, pancreatitis] G. Renal system [e.g. UTI, pyelonephritis, renal calculi] H. Toxicology [e.g. medication overdoses, poisonings, antidotes]
R2.4 R2.6 R2.7
2. Understand and communicate effectively about commonly used diagnostic, monitoring, and therapeutic procedures used in an emergency department
R2.6, R2.7, R2.8, R2.9, R2.10
3. Given a patient’s medical history (symptoms, physical examination, laboratory values, current medications, and diagnosis): A. Identify, list and prioritize the significant active and inactive medical problems
significant to ED visit and possible hospital admission B. Identify which of the above problems require drug therapy or drug therapy
adjustment in the ED setting C. List and discuss risks versus benefits and considerations important in selecting
appropriate drug(s) for a given disease state D. Identify the drug of choice, dose, frequency, and duration of therapy as well
as alternative drug or treatment choices for a given disease state E. Identify, list and assess the appropriate parameters (physical, lab, etc.) for
monitoring the progress of drug therapy for the stated disease states F. Identify the effects of drugs on physically measurable parameters and
laboratory test results G. Identify and discuss the significance and incidence of common adverse
reactions, predisposing patient risk factors, and strategies for minimizing or avoiding them
H. Identify and discuss common adverse drug interactions and strategies for minimizing or avoiding them
R2.2 R2.4 R2.6 R2.7 R2.8 R2.9 R2.10
4. For a given drug: A. Identify the drug class and its mechanism of action B. Select and utilize appropriate biopharmaceutic (dosage form, palatability, cost,
etc.) and pharmacokinetic (t½, elimination, etc.) parameters to establish a drug regimen
C. Predict and establish the therapeutic and toxic endpoints of therapy
R2.6
5. During a patient/family/caregiver interview, obtain all of the following: A. The patient’s chief complaint B. List of current medications and/or supplements and their dosing regimens C. List of pertinent past medication(s) and supplement(s) D. List and description of allergies, adverse side effects and drug interactions E. When applicable, elicit a description of any symptoms from the patient that
R1.4 R2.4

Page 31 revised 7/22/15
may relate to drug allergies/sensitivities, incorrect drug/supplement administration, or drug interaction
F. Social history, including cultural aspects (e.g. health beliefs, expectations of drug therapy, healing traditions, language barriers), which may impact health-care, medication delivery, and patient compliance or adherence
G. Patient adherence H. Patient reliability
6. Interact with patients, their families, and the health-care team in a culturally-sensitive manner A. Effectively utilize a skilled and/or unskilled interpreter for patient interviews
and education
E7.1 E7.2
7. Demonstrate competence in counseling patients on medications and/or devices and adherence (compliance) A. Effectively develop and utilize patient counseling aids for patient education
regarding medication usage and storage (e.g. inhalers, insulin) B. Explain the indication for each medication, common side effects and
strategies to mitigate them C. Emphasize and discuss strategies for mitigating patient adherence
R5.1
8. Provide drug information to the house staff, nurses, and other health-care professionals or patients as needed
R1.5, R2.1
9. Evaluate and critique the drug literature, new drug information and published protocols and point out strengths and weaknesses and develop conclusions for their role in acute care emergency medicine management
R1.5
10. Precept pharmacy students (when applicable) A. Serve as co-preceptor B. Facilitate/lead topic discussions C. Contribute to students’ evaluations
R3.1 R5.1
11. Review patient medication profiles for drug-related problems (Strand et al. Drug-related problems: Their structure and function. DICP: the annals of pharmacotherapy 1990;24(11):1093-7): A. Existing medical condition but not receiving drug for that indication B. Medication with wrong indication C. Subtherapeutic dosing for medical condition D. Supratherapeutic dosing for medication condition E. Medication condition resulting from an adverse drug reaction F. Medical condition resulting from drug-drug, drug-food, or drug-lab
interaction G. Medical condition that is a result of not receiving prescribed drug H. Medical condition that is a result of taking a drug for which there is no valid
medical indication
R2.2 R2.4
Preceptor Interactions Variable and resident-specific.
Page 32 revised 7/22/15
Evaluation Strategy E-value will be used for documentation of formal evaluations. For formative evaluations, resident and preceptor will independently complete the Midpoint evaluations that are Qualitative and Quantitative. After both have completed the evaluation, the resident and preceptor will compare and discuss the evaluations. This discussion will provide feedback both on their performance of the activity and the accuracy of the self-assessment. The same will take place for the Summative (Final) Evaluation.
What type of evaluation Who When
Formative (Midpoint) Self Evaluation Resident End of week 3
Formative (Midpoint) Preceptor End of week 3
Summative Preceptor End of learning experience
Summative Self Evaluation Resident End of learning experience
Preceptor, Learning Experience Evaluations Resident End of learning experience
Time and Attendance
o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per residency guidelines. Meetings should not be scheduled during patient care activities.

Page 33 revised 7/22/15
Infectious Diseases Rotation PGY1 Resident Expectations and Responsibilities Preceptor: TBD General Description The Infectious Diseases (ID) Service is a consulting service. Hospitalized patients are seen at the request of the primary physicians (private or teaching service). Patient population includes adults and pediatrics located in an area of CRMC - rehabilitation floor, medical/surgery units, step down units, intensive care units. Consultations are provided by the residents and students on the ID service under the guidance and supervision of the ID attending physician. The ID Service consists of the attending physician, ID pharmacist, ID/Pulmonary-Critical Care fellow(s), medical and pharmacy residents and students. This section will be updated, once the ID pharmacist has had a chance to review and revise. Disease States The resident will be expected to gain knowledge and proficiency in the principles of infectious diseases through self-directed learning, literature review, topic discussions and/or direct patient care experience including, but not limited to:
A. Signs and symptoms consistent with infection B. Disease states which can mimic infection C. Host factors which may predispose patients to infection D. The most likely anatomic sites for infectious processes E. Common pathogens and symptoms associated with infection for each of the following sites:
central nervous system, lung, heart, abdomen, genitourinary, skin/soft tissue, bone, intravenous catheter site
F. All common bacteria on the basis of Gram stain (e.g. Gram-positive versus Gram-negative, rod versus cocci) and oxygen requirements (aerobic versus anaerobic)
G. Signs, symptoms, complications, and monitoring parameters in HIV positive patients H. Monitoring parameters in a patient with infectious disease(s) I. For a given antimicrobial agent identify the drug class, mechanism of action, therapeutic and
toxic endpoints, adverse effects, dosing and administration considerations, monitoring, biopharmaceutic (dosage form, palatability, cost, etc.), pharmacokinetic and pharmacodynamic parameters.
Activity Goals Covered
Identify adverse effects associated with drug therapy and make necessary interventions
Complete online Incident Reporting Intranet System (IRIS) report on all medication errors, adverse drug reactions resulting from medication administration or causing admission to the hospital
Identify relevant literature to support therapeutic recommendations
Assist pharmacy in clarifying medication orders written by medical team, and answering medication questions about patients on the team
R1.1 R1.4 R1.5
Monitor assigned patients on ID Medical Service and formulate a drug regimen and appropriate monitoring parameters based on patient specific characteristics (as described below)
R2.1 R2.2 R2.3
Page 34 revised 7/22/15
Review patient medication profiles for: Medications used with no medical indication; Medical conditions for which there is no medication prescribed; Appropriate medication selection and dosing for allergies, comorbidities and drug-drug interactions; Appropriate prescribing (i.e. correct dose, dosage form, duration, schedule, route of administration, method of administration, etc.); Therapeutic duplications; Drug-drug interactions, drug-nutrient interactions and/or drug-device interactions (including social, recreational, nonprescription or nontraditional medications potentially used prior to admission); Anticipated duration of therapy; Necessary monitoring parameters; Compliance with institution’s medication formulary; Cost-effectiveness considerations
Design a patient-centered regimen to achieve evidence-based therapeutic goals (considered all items listed above)
Design a patient-centered monitoring plan to ensure achievement of therapeutic goals. Redesign care plan as necessary based on monitoring data and therapeutic outcomes
Establish collaborative working relationship with members of a multidisciplinary health care team
Assist in providing pharmacokinetic monitoring for services without a designated clinical pharmacist and document recommendations appropriately
Appropriately select direct patient-care activities for documentation
Attend daily rounds; actively participate in patient discussions and present therapeutic recommendations
Provide patient education and drug information to ID service
Communicate patient information to other clinical pharmacist specialists if patients are transferred to another service
R2.4 R2.6 R2.7 R2.8 R2.9 R2.10 R2.11 R2.12
Outcome R3: Exercise leadership and practice management skills
Take over responsibilities as the primary pharmacist on service
Conduct periodic self-assessments to practice self-managed professional development
Character: Demonstrate pride in and commitment to the profession through appearance and professional personal contacts; Act ethically in the conduct of all job-related activities
Not formally evaluated
Outcome R5: Provide medication and practice-related education/training
Prepare for and participate in topic discussions with preceptor; lead at least two topic discussions with pharmacy students (if applicable)
One formal journal club presentation to pharmacy department
One formal case presentation to pharmacy department
Set up a time and date for journal club and case presentations; email chief resident to notify pharmacy department at least one week in advance of presentation date; journal club article should be available one week prior to presentation date
Perform Med Checks on a regular basis and document as i-Vents
Document all therapeutic interventions in i-Vents
Educational activities (journal clubs, case presentations, in-services, topic discussions): Identify current controversies in literature (journal club) or in a specific patient care (case presentation); Identify relevant literature; Critically evaluate literature and how they add information/clarity to area of controversy; Use public speaking skills to effectively communicate educational goals; Use
R5.1 E7.4
Page 35 revised 7/22/15
audio-visual aids and handouts to enhance communication of educational goals
Precept pharmacy students (when applicable): Serve as pre-rounding preceptor; Facilitate/Lead topic discussions; Assist the student in following up on patient issues following rounds; Identify and implement the four preceptor roles as appropriate for the student and the activity (direct instruction, modeling, coaching and facilitation); Contribute to the students’ evaluations
Preceptor interactions for rounding services Daily activities are dependent on the time of rounds with the team, which is dependent on the attending physician. In general rounds will be in the afternoon on Monday and as listed below on Tuesday through Friday, depending on the attending. Daily: 0900 or 1100 Pre-rounds with resident 1030 or 1300 Team Rounds
Office hours: The preceptor does not have set office hours, but is always available to the resident via
pager. Time to discuss topics, review progress notes, patient updates, pharmacokinetic calculations, etc will be arranged with the preceptor at the beginning of the rotation or as needed on a daily basis.
Expected progression of resident responsibilities on the Infectious Diseases experience: Day 1: 0900 Resident reviews material provided by preceptor.
1230 Preceptor provides orientation to service, hospital, nursing floors, and reviews ID learning activities and expectations.
Week 1-2: Resident works up patients on the team and presents to preceptor prior to team rounds. Preceptor will attend and participate in team rounds to model pharmacist’s role on the team.
Week 3-4 Resident continues to work up patients on the team and presents to preceptor prior to team rounds. Preceptor may attend and participate in team rounds to coach the resident to take on more responsibilities as the primary pharmacist on the team. In addition, if there is a pharmacy student on the team, the resident will take on responsibility of a co-preceptor role. Resident will complete a preceptor approved journal club as per the Pharmacy Residency Manual.
Week 5-6: Resident continues to work up patients on the team and presents to preceptor prior to team rounds. Preceptor may attend and observe the resident’s participation in team rounds, and/or may expect a summary report from the resident on recommendations made by the resident, updates on patients, and student progress. Preceptor will always be available via pager or phone for questions, and may follow patients independently to monitor resident skill development in all aspects of the learning experience to help facilitate the resident as the pharmacist on the team. Resident will complete a case presentation, based on an actual patient on the ID Service, as per the Pharmacy Resident Manual.
[The length of time the preceptor spends in each of the phases of learning will depend BOTH on the resident’s progression in the current rotation and where the rotation occurs in the residency program]

Page 36 revised 7/22/15
Evaluation Strategy E-value will be used for documentation of formal evaluations. For formative evaluations, resident and preceptor will independently complete the Midpoint evaluations that are Qualitative and Quantitative. After both have completed the evaluation, the resident and preceptor will compare and discuss the evaluations. This discussion will provide feedback both on their performance of the activity and the accuracy of the self-assessment. The same will take place for the Summative (Final) Evaluation.
What type of evaluation Who When
Formative (Midpoint) Self Evaluation Resident End of week 3
Formative (Midpoint) Preceptor End of week 3
Summative Preceptor End of learning experience
Summative Self Evaluation Resident End of learning experience
Preceptor, Learning Experience Evaluations Resident End of learning experience
Time and Attendance
o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per residency guidelines. Meetings should not be scheduled during patient care activities.
o The resident is expected to arrive in the morning to allow for adequate pre-rounding time with
preceptor before rounds. The resident may leave once all daily activities are complete; however, an 8 hour day is expected.
o Overtime will not be granted except in extreme cases and should be discussed with the residency director.
o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per residency guidelines. Meetings should not be scheduled during patient care activities.
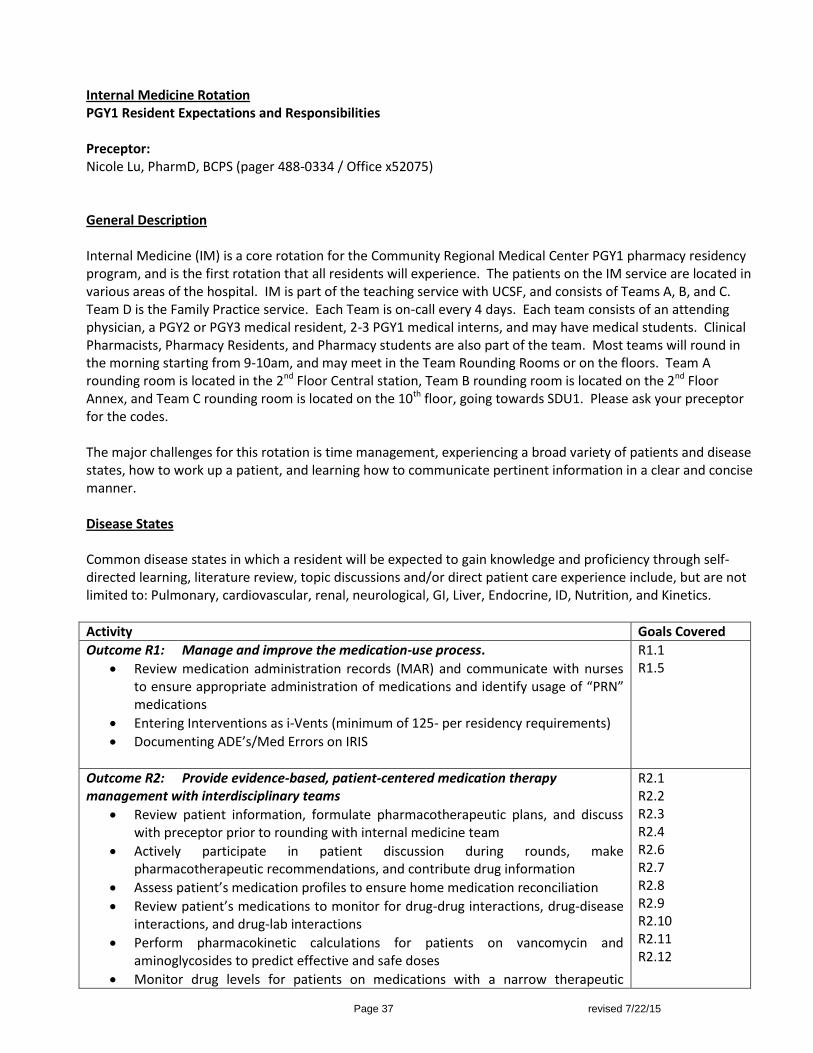
Page 37 revised 7/22/15
Internal Medicine Rotation PGY1 Resident Expectations and Responsibilities Preceptor: Nicole Lu, PharmD, BCPS (pager 488-0334 / Office x52075) General Description Internal Medicine (IM) is a core rotation for the Community Regional Medical Center PGY1 pharmacy residency program, and is the first rotation that all residents will experience. The patients on the IM service are located in various areas of the hospital. IM is part of the teaching service with UCSF, and consists of Teams A, B, and C. Team D is the Family Practice service. Each Team is on-call every 4 days. Each team consists of an attending physician, a PGY2 or PGY3 medical resident, 2-3 PGY1 medical interns, and may have medical students. Clinical Pharmacists, Pharmacy Residents, and Pharmacy students are also part of the team. Most teams will round in the morning starting from 9-10am, and may meet in the Team Rounding Rooms or on the floors. Team A rounding room is located in the 2nd Floor Central station, Team B rounding room is located on the 2nd Floor Annex, and Team C rounding room is located on the 10th floor, going towards SDU1. Please ask your preceptor for the codes. The major challenges for this rotation is time management, experiencing a broad variety of patients and disease states, how to work up a patient, and learning how to communicate pertinent information in a clear and concise manner. Disease States Common disease states in which a resident will be expected to gain knowledge and proficiency through self-directed learning, literature review, topic discussions and/or direct patient care experience include, but are not limited to: Pulmonary, cardiovascular, renal, neurological, GI, Liver, Endocrine, ID, Nutrition, and Kinetics.
Activity Goals Covered
Outcome R1: Manage and improve the medication-use process.
Review medication administration records (MAR) and communicate with nurses to ensure appropriate administration of medications and identify usage of “PRN” medications
Entering Interventions as i-Vents (minimum of 125- per residency requirements)
Documenting ADE’s/Med Errors on IRIS
R1.1 R1.5
Outcome R2: Provide evidence-based, patient-centered medication therapy management with interdisciplinary teams
Review patient information, formulate pharmacotherapeutic plans, and discuss with preceptor prior to rounding with internal medicine team
Actively participate in patient discussion during rounds, make pharmacotherapeutic recommendations, and contribute drug information
Assess patient’s medication profiles to ensure home medication reconciliation
Review patient’s medications to monitor for drug-drug interactions, drug-disease interactions, and drug-lab interactions
Perform pharmacokinetic calculations for patients on vancomycin and aminoglycosides to predict effective and safe doses
Monitor drug levels for patients on medications with a narrow therapeutic
R2.1 R2.2 R2.3 R2.4 R2.6 R2.7 R2.8 R2.9 R2.10 R2.11 R2.12
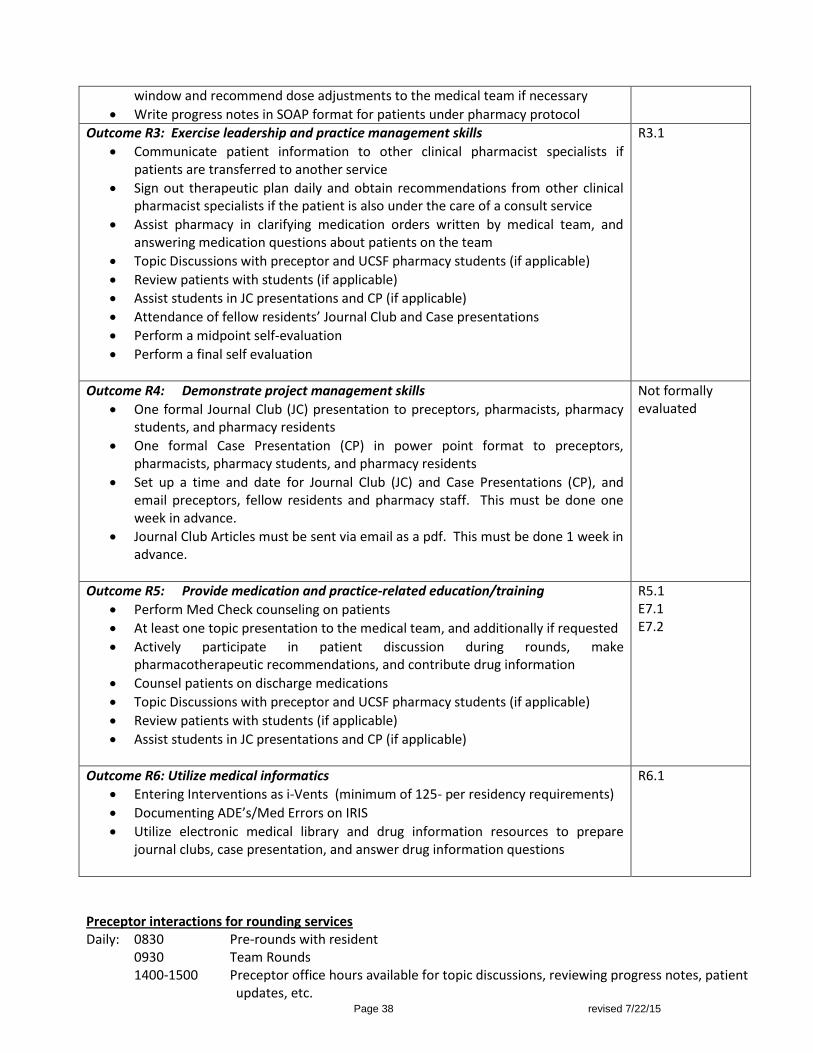
Page 38 revised 7/22/15
window and recommend dose adjustments to the medical team if necessary
Write progress notes in SOAP format for patients under pharmacy protocol
Outcome R3: Exercise leadership and practice management skills
Communicate patient information to other clinical pharmacist specialists if patients are transferred to another service
Sign out therapeutic plan daily and obtain recommendations from other clinical pharmacist specialists if the patient is also under the care of a consult service
Assist pharmacy in clarifying medication orders written by medical team, and answering medication questions about patients on the team
Topic Discussions with preceptor and UCSF pharmacy students (if applicable)
Review patients with students (if applicable)
Assist students in JC presentations and CP (if applicable)
Attendance of fellow residents’ Journal Club and Case presentations
Perform a midpoint self-evaluation
Perform a final self evaluation
R3.1
Outcome R4: Demonstrate project management skills
One formal Journal Club (JC) presentation to preceptors, pharmacists, pharmacy students, and pharmacy residents
One formal Case Presentation (CP) in power point format to preceptors, pharmacists, pharmacy students, and pharmacy residents
Set up a time and date for Journal Club (JC) and Case Presentations (CP), and email preceptors, fellow residents and pharmacy staff. This must be done one week in advance.
Journal Club Articles must be sent via email as a pdf. This must be done 1 week in advance.
Not formally evaluated
Outcome R5: Provide medication and practice-related education/training
Perform Med Check counseling on patients
At least one topic presentation to the medical team, and additionally if requested
Actively participate in patient discussion during rounds, make pharmacotherapeutic recommendations, and contribute drug information
Counsel patients on discharge medications
Topic Discussions with preceptor and UCSF pharmacy students (if applicable)
Review patients with students (if applicable)
Assist students in JC presentations and CP (if applicable)
R5.1 E7.1 E7.2
Outcome R6: Utilize medical informatics
Entering Interventions as i-Vents (minimum of 125- per residency requirements)
Documenting ADE’s/Med Errors on IRIS
Utilize electronic medical library and drug information resources to prepare journal clubs, case presentation, and answer drug information questions
R6.1
Preceptor interactions for rounding services Daily: 0830 Pre-rounds with resident 0930 Team Rounds
1400-1500 Preceptor office hours available for topic discussions, reviewing progress notes, patient updates, etc.
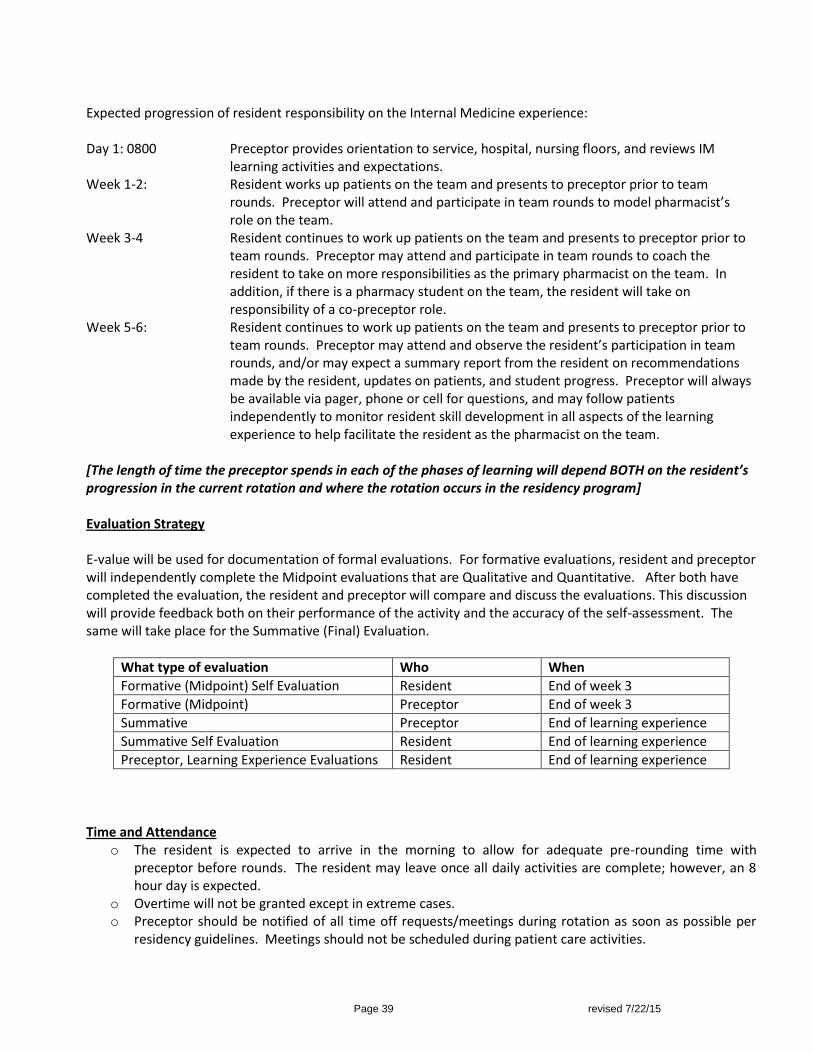
Page 39 revised 7/22/15
Expected progression of resident responsibility on the Internal Medicine experience: Day 1: 0800 Preceptor provides orientation to service, hospital, nursing floors, and reviews IM
learning activities and expectations. Week 1-2: Resident works up patients on the team and presents to preceptor prior to team
rounds. Preceptor will attend and participate in team rounds to model pharmacist’s role on the team.
Week 3-4 Resident continues to work up patients on the team and presents to preceptor prior to team rounds. Preceptor may attend and participate in team rounds to coach the resident to take on more responsibilities as the primary pharmacist on the team. In addition, if there is a pharmacy student on the team, the resident will take on responsibility of a co-preceptor role.
Week 5-6: Resident continues to work up patients on the team and presents to preceptor prior to team rounds. Preceptor may attend and observe the resident’s participation in team rounds, and/or may expect a summary report from the resident on recommendations made by the resident, updates on patients, and student progress. Preceptor will always be available via pager, phone or cell for questions, and may follow patients independently to monitor resident skill development in all aspects of the learning experience to help facilitate the resident as the pharmacist on the team.
[The length of time the preceptor spends in each of the phases of learning will depend BOTH on the resident’s progression in the current rotation and where the rotation occurs in the residency program] Evaluation Strategy E-value will be used for documentation of formal evaluations. For formative evaluations, resident and preceptor will independently complete the Midpoint evaluations that are Qualitative and Quantitative. After both have completed the evaluation, the resident and preceptor will compare and discuss the evaluations. This discussion will provide feedback both on their performance of the activity and the accuracy of the self-assessment. The same will take place for the Summative (Final) Evaluation.
What type of evaluation Who When
Formative (Midpoint) Self Evaluation Resident End of week 3
Formative (Midpoint) Preceptor End of week 3
Summative Preceptor End of learning experience
Summative Self Evaluation Resident End of learning experience
Preceptor, Learning Experience Evaluations Resident End of learning experience
Time and Attendance
o The resident is expected to arrive in the morning to allow for adequate pre-rounding time with preceptor before rounds. The resident may leave once all daily activities are complete; however, an 8 hour day is expected.
o Overtime will not be granted except in extreme cases. o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per
residency guidelines. Meetings should not be scheduled during patient care activities.
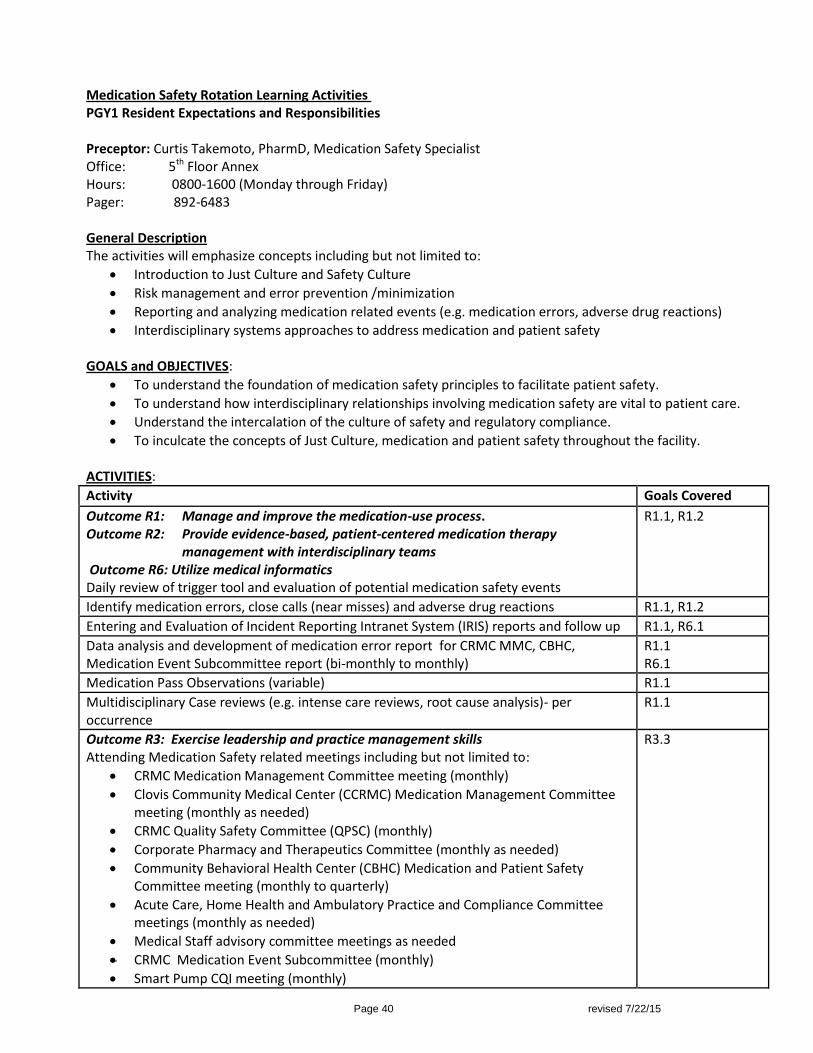
Page 40 revised 7/22/15
Medication Safety Rotation Learning Activities PGY1 Resident Expectations and Responsibilities Preceptor: Curtis Takemoto, PharmD, Medication Safety Specialist Office: 5th Floor Annex Hours: 0800-1600 (Monday through Friday) Pager: 892-6483 General Description The activities will emphasize concepts including but not limited to:
Introduction to Just Culture and Safety Culture
Risk management and error prevention /minimization
Reporting and analyzing medication related events (e.g. medication errors, adverse drug reactions)
Interdisciplinary systems approaches to address medication and patient safety GOALS and OBJECTIVES:
To understand the foundation of medication safety principles to facilitate patient safety.
To understand how interdisciplinary relationships involving medication safety are vital to patient care.
Understand the intercalation of the culture of safety and regulatory compliance.
To inculcate the concepts of Just Culture, medication and patient safety throughout the facility. ACTIVITIES:
Activity Goals Covered
Outcome R1: Manage and improve the medication-use process. Outcome R2: Provide evidence-based, patient-centered medication therapy
management with interdisciplinary teams Outcome R6: Utilize medical informatics Daily review of trigger tool and evaluation of potential medication safety events
R1.1, R1.2
Identify medication errors, close calls (near misses) and adverse drug reactions R1.1, R1.2
Entering and Evaluation of Incident Reporting Intranet System (IRIS) reports and follow up R1.1, R6.1
Data analysis and development of medication error report for CRMC MMC, CBHC, Medication Event Subcommittee report (bi-monthly to monthly)
R1.1 R6.1
Medication Pass Observations (variable) R1.1
Multidisciplinary Case reviews (e.g. intense care reviews, root cause analysis)- per occurrence
R1.1
Outcome R3: Exercise leadership and practice management skills Attending Medication Safety related meetings including but not limited to:
CRMC Medication Management Committee meeting (monthly)
Clovis Community Medical Center (CCRMC) Medication Management Committee meeting (monthly as needed)
CRMC Quality Safety Committee (QPSC) (monthly)
Corporate Pharmacy and Therapeutics Committee (monthly as needed)
Community Behavioral Health Center (CBHC) Medication and Patient Safety Committee meeting (monthly to quarterly)
Acute Care, Home Health and Ambulatory Practice and Compliance Committee meetings (monthly as needed)
Medical Staff advisory committee meetings as needed
CRMC Medication Event Subcommittee (monthly)
Smart Pump CQI meeting (monthly)
R3.3
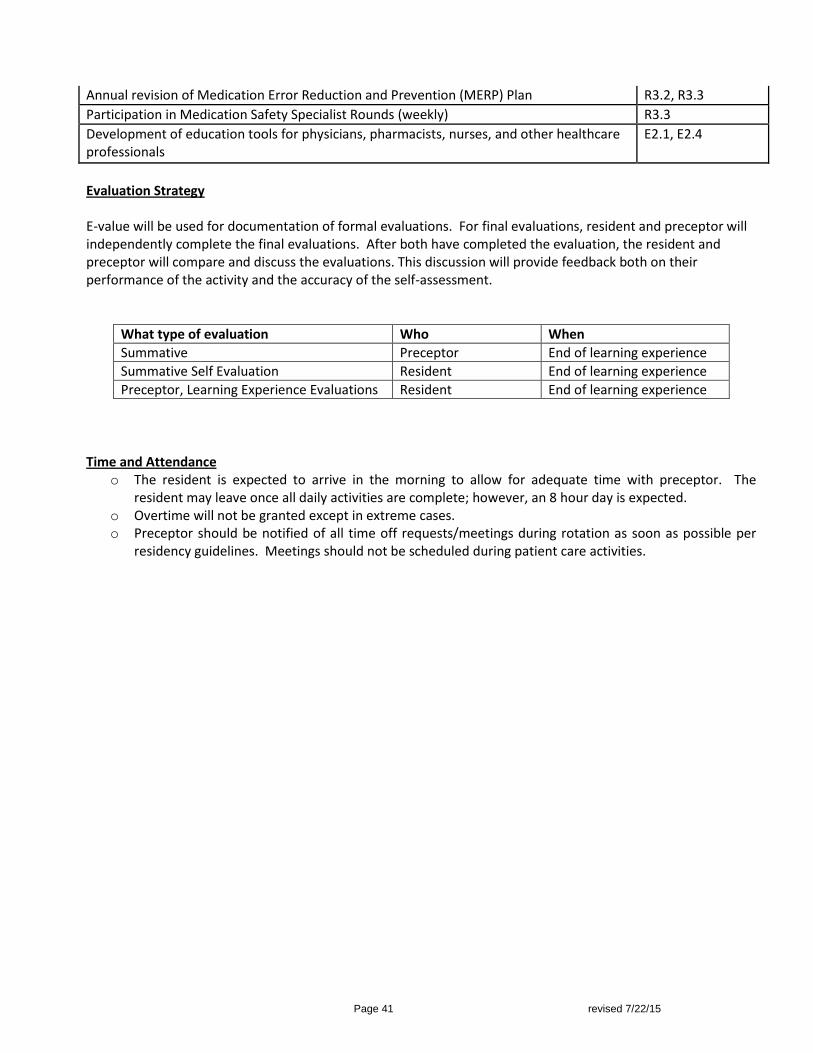
Page 41 revised 7/22/15
Annual revision of Medication Error Reduction and Prevention (MERP) Plan R3.2, R3.3
Participation in Medication Safety Specialist Rounds (weekly) R3.3
Development of education tools for physicians, pharmacists, nurses, and other healthcare professionals
E2.1, E2.4
Evaluation Strategy E-value will be used for documentation of formal evaluations. For final evaluations, resident and preceptor will independently complete the final evaluations. After both have completed the evaluation, the resident and preceptor will compare and discuss the evaluations. This discussion will provide feedback both on their performance of the activity and the accuracy of the self-assessment.
What type of evaluation Who When
Summative Preceptor End of learning experience
Summative Self Evaluation Resident End of learning experience
Preceptor, Learning Experience Evaluations Resident End of learning experience
Time and Attendance
o The resident is expected to arrive in the morning to allow for adequate time with preceptor. The resident may leave once all daily activities are complete; however, an 8 hour day is expected.
o Overtime will not be granted except in extreme cases. o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per
residency guidelines. Meetings should not be scheduled during patient care activities.
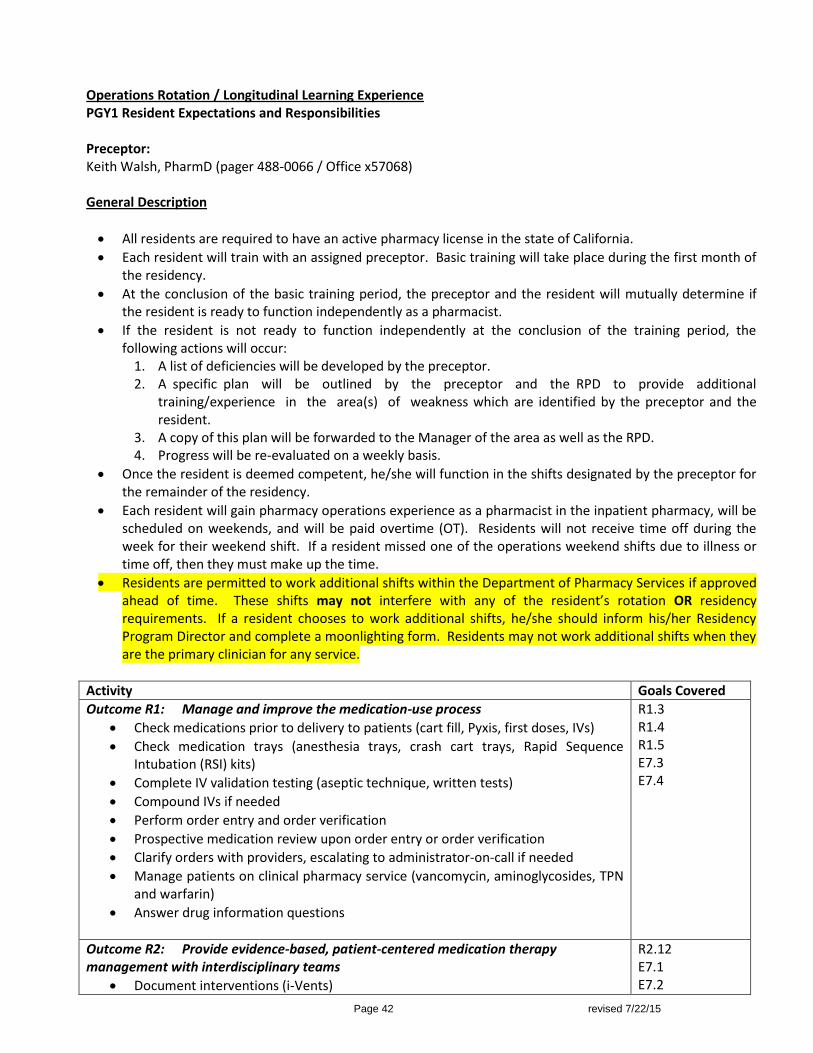
Page 42 revised 7/22/15
Operations Rotation / Longitudinal Learning Experience PGY1 Resident Expectations and Responsibilities Preceptor: Keith Walsh, PharmD (pager 488-0066 / Office x57068) General Description
All residents are required to have an active pharmacy license in the state of California.
Each resident will train with an assigned preceptor. Basic training will take place during the first month of the residency.
At the conclusion of the basic training period, the preceptor and the resident will mutually determine if the resident is ready to function independently as a pharmacist.
If the resident is not ready to function independently at the conclusion of the training period, the following actions will occur:
1. A list of deficiencies will be developed by the preceptor. 2. A specific plan will be outlined by the preceptor and the RPD to provide additional
training/experience in the area(s) of weakness which are identified by the preceptor and the resident.
3. A copy of this plan will be forwarded to the Manager of the area as well as the RPD. 4. Progress will be re-evaluated on a weekly basis.
Once the resident is deemed competent, he/she will function in the shifts designated by the preceptor for the remainder of the residency.
Each resident will gain pharmacy operations experience as a pharmacist in the inpatient pharmacy, will be scheduled on weekends, and will be paid overtime (OT). Residents will not receive time off during the week for their weekend shift. If a resident missed one of the operations weekend shifts due to illness or time off, then they must make up the time.
Residents are permitted to work additional shifts within the Department of Pharmacy Services if approved ahead of time. These shifts may not interfere with any of the resident’s rotation OR residency requirements. If a resident chooses to work additional shifts, he/she should inform his/her Residency Program Director and complete a moonlighting form. Residents may not work additional shifts when they are the primary clinician for any service.
Activity Goals Covered
Outcome R1: Manage and improve the medication-use process
Check medications prior to delivery to patients (cart fill, Pyxis, first doses, IVs)
Check medication trays (anesthesia trays, crash cart trays, Rapid Sequence Intubation (RSI) kits)
Complete IV validation testing (aseptic technique, written tests)
Compound IVs if needed
Perform order entry and order verification
Prospective medication review upon order entry or order verification
Clarify orders with providers, escalating to administrator-on-call if needed
Manage patients on clinical pharmacy service (vancomycin, aminoglycosides, TPN and warfarin)
Answer drug information questions
R1.3 R1.4 R1.5 E7.3 E7.4
Outcome R2: Provide evidence-based, patient-centered medication therapy management with interdisciplinary teams
Document interventions (i-Vents)
R2.12 E7.1 E7.2

Page 43 revised 7/22/15
Document Adverse Drug Event (ADE) and medication errors in Incident Reporting Intranet System (IRIS)
Document pharmacy-managed protocol activities appropriately (monitoring sheets, i-Vents)
Expected progression of resident responsibility on the Operational experience: Week 1: Preceptor(s) provide orientation and tour of inpatient pharmacy and facility with introduction
and orientation to EPIC, Talyst, and Community Forum. Resident observes and participates in the process of cart and Pyxis fill and delivery. Start working on required HLCs.
Week 2-4: Resident will progress to checking cart and anesthesia trays. Resident will orient to IV room
workflow and perform aseptic technique competency test. Resident continues to learn the navigation, search, verification and retrieval of orders in Epic. Residents begin learning process of order clarification, dose adjustment, therapeutic substitution or intervention. Resident will begin participating in pharmacy approved protocols of pharmacokinetic dosing and warfarin monitoring. If licensed, resident will be verifying and entering orders independently in Epic. Continue progress on required HLCs.
Quarterly: Resident will complete all required HLCs within the first 60 days. Resident will continue progress
in regards to EPIC verification and order entry ability, problem solving, organizational skills, and checking functions in regards to drug delivery system. Resident will progress in covering various operational pharmacy shifts as licensure allows.
[The length of time the preceptor spends in each of the phases of learning will depend BOTH on the resident’s progression in the current rotation and where the rotation occurs in the residency program] Evaluation Strategy E-value will be used for documentation of formal evaluations. For formative evaluations, resident and preceptor will independently complete the Midpoint evaluations that are Qualitative and Quantitative. After both have completed the evaluation, the resident and preceptor will compare and discuss the evaluations. This discussion will provide feedback both on their performance of the activity and the accuracy of the self-assessment. The same will take place for the Summative (Final) Evaluation.
What type of evaluation Who When
Summative Preceptor End of learning experience
Summative Self Evaluation Resident End of learning experience
Preceptor, Learning Experience Evaluations Resident End of learning experience
Quarterly Longitudinal Self Evaluation Resident Quarterly
Quarterly Longitudinal Evaluation Preceptor Quarterly
Time and Attendance
o The resident is expected to arrive on time for their scheduled shift. o Overtime will not be granted except in extreme cases. o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per
residency guidelines.
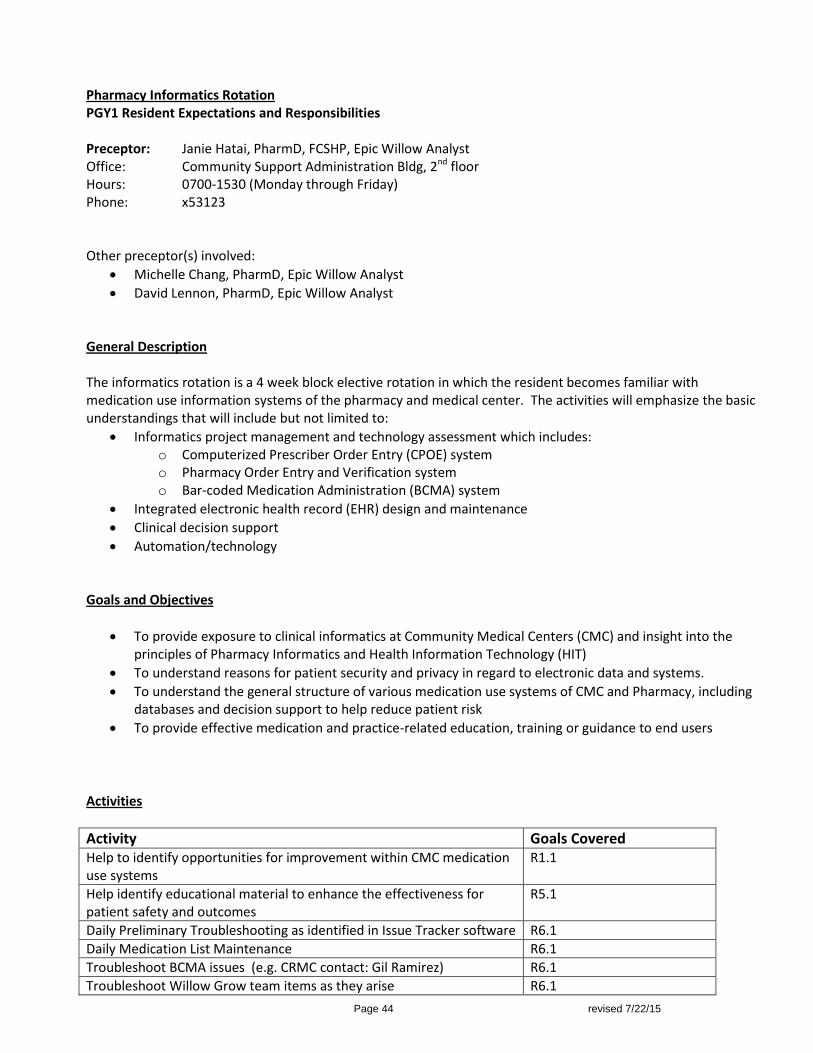
Page 44 revised 7/22/15
Pharmacy Informatics Rotation PGY1 Resident Expectations and Responsibilities Preceptor: Janie Hatai, PharmD, FCSHP, Epic Willow Analyst Office: Community Support Administration Bldg, 2nd floor Hours: 0700-1530 (Monday through Friday) Phone: x53123 Other preceptor(s) involved:
Michelle Chang, PharmD, Epic Willow Analyst
David Lennon, PharmD, Epic Willow Analyst General Description The informatics rotation is a 4 week block elective rotation in which the resident becomes familiar with medication use information systems of the pharmacy and medical center. The activities will emphasize the basic understandings that will include but not limited to:
Informatics project management and technology assessment which includes: o Computerized Prescriber Order Entry (CPOE) system o Pharmacy Order Entry and Verification system o Bar-coded Medication Administration (BCMA) system
Integrated electronic health record (EHR) design and maintenance
Clinical decision support
Automation/technology Goals and Objectives
To provide exposure to clinical informatics at Community Medical Centers (CMC) and insight into the principles of Pharmacy Informatics and Health Information Technology (HIT)
To understand reasons for patient security and privacy in regard to electronic data and systems.
To understand the general structure of various medication use systems of CMC and Pharmacy, including databases and decision support to help reduce patient risk
To provide effective medication and practice-related education, training or guidance to end users
Activities
Activity Goals Covered Help to identify opportunities for improvement within CMC medication use systems
R1.1
Help identify educational material to enhance the effectiveness for patient safety and outcomes
R5.1
Daily Preliminary Troubleshooting as identified in Issue Tracker software R6.1
Daily Medication List Maintenance R6.1
Troubleshoot BCMA issues (e.g. CRMC contact: Gil Ramirez) R6.1
Troubleshoot Willow Grow team items as they arise R6.1
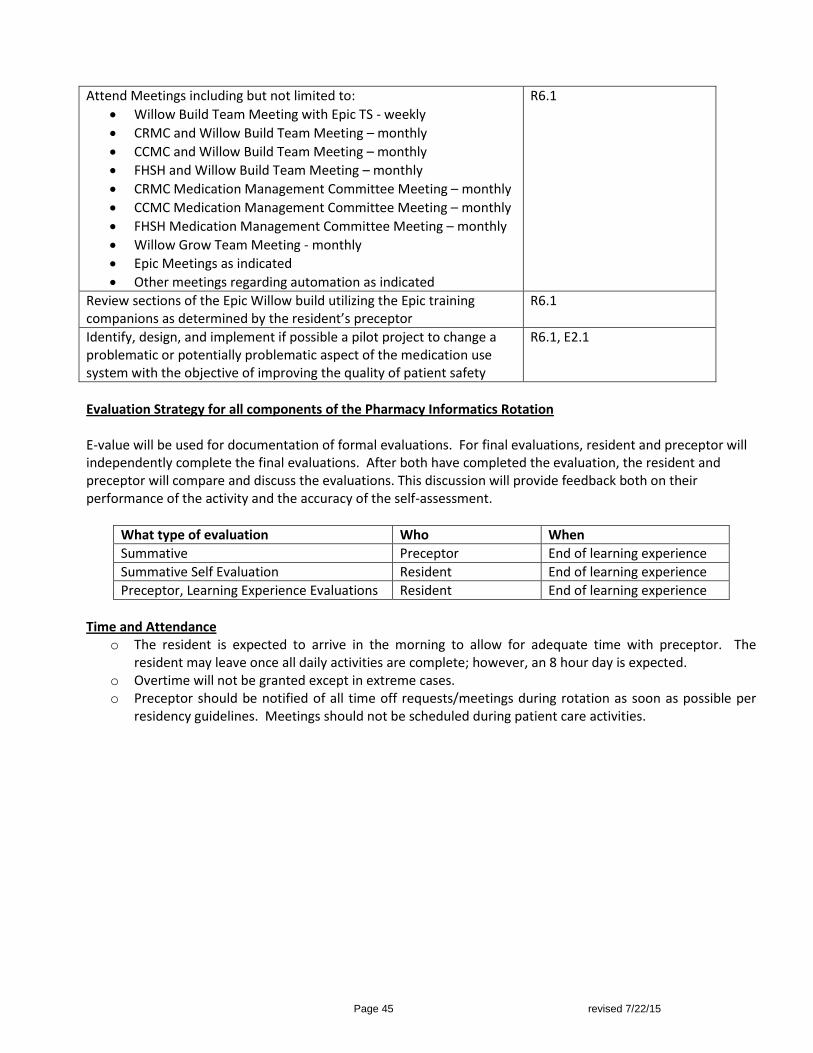
Page 45 revised 7/22/15
Attend Meetings including but not limited to:
Willow Build Team Meeting with Epic TS - weekly
CRMC and Willow Build Team Meeting – monthly
CCMC and Willow Build Team Meeting – monthly
FHSH and Willow Build Team Meeting – monthly
CRMC Medication Management Committee Meeting – monthly
CCMC Medication Management Committee Meeting – monthly
FHSH Medication Management Committee Meeting – monthly
Willow Grow Team Meeting - monthly
Epic Meetings as indicated
Other meetings regarding automation as indicated
R6.1
Review sections of the Epic Willow build utilizing the Epic training companions as determined by the resident’s preceptor
R6.1
Identify, design, and implement if possible a pilot project to change a problematic or potentially problematic aspect of the medication use system with the objective of improving the quality of patient safety
R6.1, E2.1
Evaluation Strategy for all components of the Pharmacy Informatics Rotation E-value will be used for documentation of formal evaluations. For final evaluations, resident and preceptor will independently complete the final evaluations. After both have completed the evaluation, the resident and preceptor will compare and discuss the evaluations. This discussion will provide feedback both on their performance of the activity and the accuracy of the self-assessment.
What type of evaluation Who When
Summative Preceptor End of learning experience
Summative Self Evaluation Resident End of learning experience
Preceptor, Learning Experience Evaluations Resident End of learning experience
Time and Attendance
o The resident is expected to arrive in the morning to allow for adequate time with preceptor. The resident may leave once all daily activities are complete; however, an 8 hour day is expected.
o Overtime will not be granted except in extreme cases. o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per
residency guidelines. Meetings should not be scheduled during patient care activities.
Page 46 revised 7/22/15
Quality Management/ Risk Management/Patient Safety Rotation -Elective PGY1 Resident Expectations and Responsibilities Preceptors: Jennifer Trytten, PharmD, BCPS; Amy Royston, PharmD, BCPS, CPHQ Office: 1234 P Street, Fresno, CA 93721 Hours: 0700-1530 (Monday through Friday) Phone: x52926 (Jennifer) / x57067 (Amy) General Description The Quality Management/Risk Management/ Patient Safety (QM/RM/PS) rotation is a 4 week block elective rotation in which the resident becomes familiar with quality improvement planning and measurement as well as risk mitigation strategies in a complex medical center. Activities will largely target improvements in patient safety and may include medication safety, infection control, National Patient Safety Goals and Health Care Associated Conditions. The activities will emphasize basic understanding that will include but not limited to:
Performance improvement models (e.g. DMAIC);
Data collection and analysis techniques associated with quality management;
Risk mitigation strategies (e.g. Failure Mode and Effects Analysis, Root Cause Analyses);
Public reporting and pay-for-performance metrics;
Regulatory compliance (especially related to National Patient Safety Goals and Quality Assurance Performance Improvement (QAPI) standards);
Compliance with Joint Commission, Medicare Conditions of Participation, California Department of Public Health, California Code of Regulations, and California Business and Profession Code regulations;
Patient safety processes, focusing on medication safety. Goals and Objectives
To provide exposure to quality management and risk management activities, especially as related to
patient safety;
To provide exposure to processes required for identification, pursuit, measurement and refinement of quality improvement initiatives;
To understand the regulatory requirements for quality measurement and performance improvement;
To understand the general structure of quality and patient safety reporting at Community Regional Medical Center;
To develop multidisciplinary relationships to foster collaborative patient safety initiatives.

Page 47 revised 7/22/15
Activities
Activity
Goals Covered
Literature review and discussion related to Quality Management and Risk Management definitions and responsibilities.
R3.1
Identify performance improvement opportunities based on regulations, public reporting and pay-for-performance initiatives.
R1.1
Define scope of performance improvement work through baseline data analysis, FMEA, brainstorming and/or RCA techniques, as appropriate.
R1.1, R1.2
Formally define the scope and plan of performance improvement work by using a project charter.
R1.1, R1.2
Identify and develop monitoring strategies to assess effectiveness of performance improvement efforts.
R1.1, R6.1
Develop educational material to enhance patient safety initiatives. R5.1
Attend Meetings including but not limited to:
Quality/Patient Safety Committee (CRMC) – monthly
Medication Management Committee (CRMC) – monthly
Quality Council (Corporate) – monthly
Nursing Professional Practice Committee(Corporate) – monthly
Core Measure Workgroups (CRMC) – monthly
Practice and Compliance Meeting (CRMC) - monthly
R2.1
Evaluation Strategy for all components of the Quality Management/Risk Management/Patient Safety Rotation: E-value will be used for documentation of formal evaluations. For final evaluations, resident and preceptor will independently complete the final evaluations. After both have completed the evaluation, the resident and preceptor will compare and discuss the evaluations. This discussion will provide feedback both on their performance of the activity and the accuracy of the self-assessment.
What type of evaluation Who When
Summative Preceptor End of learning experience
Summative Self Evaluation Resident End of learning experience
Preceptor, Learning Experience Evaluations Resident End of learning experience
Time and Attendance
o The resident is expected to arrive in the morning to allow for adequate time with preceptor. The resident may leave once all daily activities are complete; however, an 8 hour day is expected.
o Overtime will not be granted except in extreme cases. o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per
residency guidelines. Meetings should not be scheduled during patient care activities.
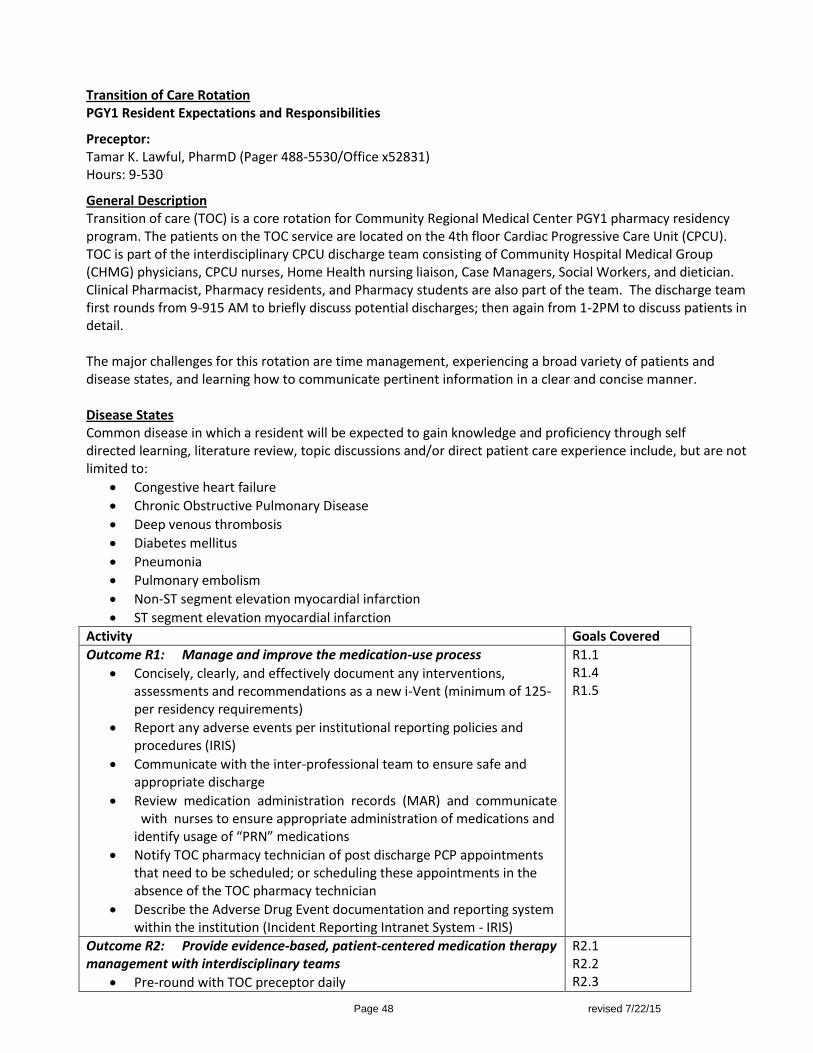
Page 48 revised 7/22/15
Transition of Care Rotation PGY1 Resident Expectations and Responsibilities
Preceptor: Tamar K. Lawful, PharmD (Pager 488-5530/Office x52831) Hours: 9-530
General Description Transition of care (TOC) is a core rotation for Community Regional Medical Center PGY1 pharmacy residency program. The patients on the TOC service are located on the 4th floor Cardiac Progressive Care Unit (CPCU). TOC is part of the interdisciplinary CPCU discharge team consisting of Community Hospital Medical Group (CHMG) physicians, CPCU nurses, Home Health nursing liaison, Case Managers, Social Workers, and dietician. Clinical Pharmacist, Pharmacy residents, and Pharmacy students are also part of the team. The discharge team first rounds from 9-915 AM to briefly discuss potential discharges; then again from 1-2PM to discuss patients in detail. The major challenges for this rotation are time management, experiencing a broad variety of patients and disease states, and learning how to communicate pertinent information in a clear and concise manner. Disease States Common disease in which a resident will be expected to gain knowledge and proficiency through self directed learning, literature review, topic discussions and/or direct patient care experience include, but are not limited to:
Congestive heart failure
Chronic Obstructive Pulmonary Disease
Deep venous thrombosis
Diabetes mellitus
Pneumonia
Pulmonary embolism
Non-ST segment elevation myocardial infarction
ST segment elevation myocardial infarction
Activity Goals Covered
Outcome R1: Manage and improve the medication-use process
Concisely, clearly, and effectively document any interventions, assessments and recommendations as a new i-Vent (minimum of 125-per residency requirements)
Report any adverse events per institutional reporting policies and procedures (IRIS)
Communicate with the inter-professional team to ensure safe and appropriate discharge
Review medication administration records (MAR) and communicate with nurses to ensure appropriate administration of medications and identify usage of “PRN” medications
Notify TOC pharmacy technician of post discharge PCP appointments that need to be scheduled; or scheduling these appointments in the absence of the TOC pharmacy technician
Describe the Adverse Drug Event documentation and reporting system within the institution (Incident Reporting Intranet System - IRIS)
R1.1 R1.4 R1.5
Outcome R2: Provide evidence-based, patient-centered medication therapy management with interdisciplinary teams
Pre-round with TOC preceptor daily
R2.1 R2.2 R2.3
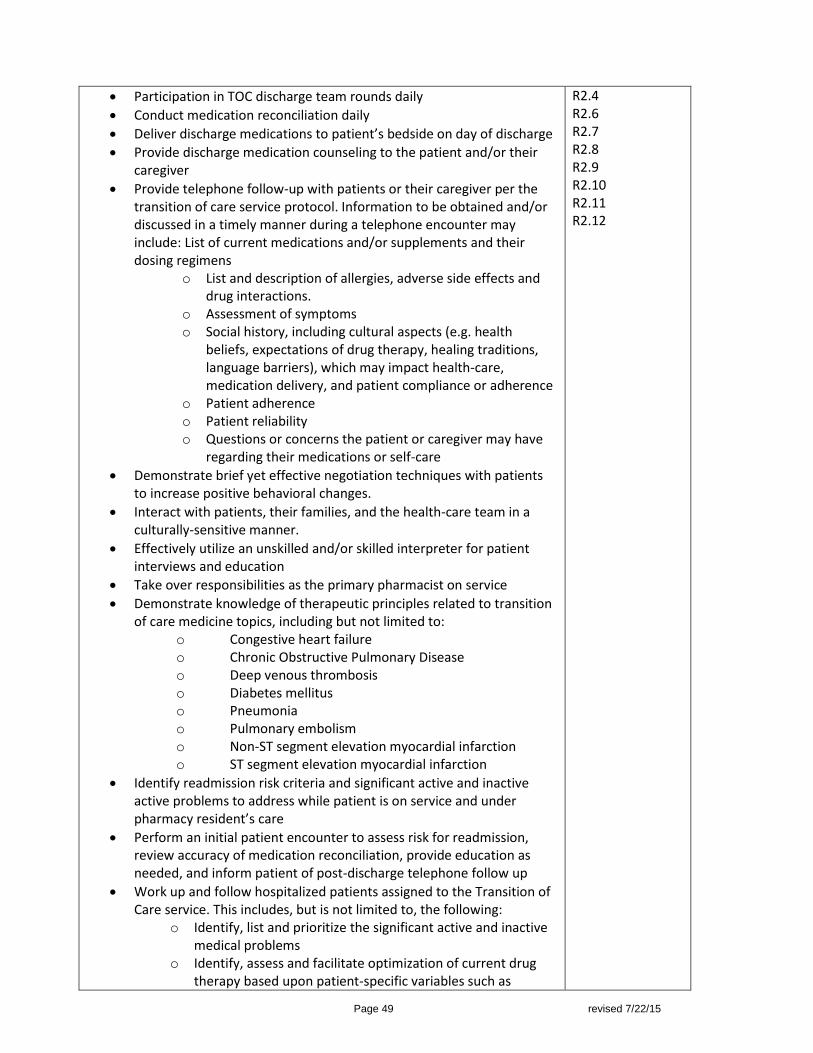
Page 49 revised 7/22/15
Participation in TOC discharge team rounds daily
Conduct medication reconciliation daily
Deliver discharge medications to patient’s bedside on day of discharge
Provide discharge medication counseling to the patient and/or their caregiver
Provide telephone follow-up with patients or their caregiver per the transition of care service protocol. Information to be obtained and/or discussed in a timely manner during a telephone encounter may include: List of current medications and/or supplements and their dosing regimens
o List and description of allergies, adverse side effects and drug interactions.
o Assessment of symptoms o Social history, including cultural aspects (e.g. health
beliefs, expectations of drug therapy, healing traditions, language barriers), which may impact health-care, medication delivery, and patient compliance or adherence
o Patient adherence o Patient reliability o Questions or concerns the patient or caregiver may have
regarding their medications or self-care
Demonstrate brief yet effective negotiation techniques with patients to increase positive behavioral changes.
Interact with patients, their families, and the health-care team in a culturally-sensitive manner.
Effectively utilize an unskilled and/or skilled interpreter for patient interviews and education
Take over responsibilities as the primary pharmacist on service
Demonstrate knowledge of therapeutic principles related to transition of care medicine topics, including but not limited to:
o Congestive heart failure o Chronic Obstructive Pulmonary Disease o Deep venous thrombosis o Diabetes mellitus o Pneumonia o Pulmonary embolism o Non-ST segment elevation myocardial infarction o ST segment elevation myocardial infarction
Identify readmission risk criteria and significant active and inactive active problems to address while patient is on service and under pharmacy resident’s care
Perform an initial patient encounter to assess risk for readmission, review accuracy of medication reconciliation, provide education as needed, and inform patient of post-discharge telephone follow up
Work up and follow hospitalized patients assigned to the Transition of Care service. This includes, but is not limited to, the following:
o Identify, list and prioritize the significant active and inactive medical problems
o Identify, assess and facilitate optimization of current drug therapy based upon patient-specific variables such as
R2.4 R2.6 R2.7 R2.8 R2.9 R2.10 R2.11 R2.12
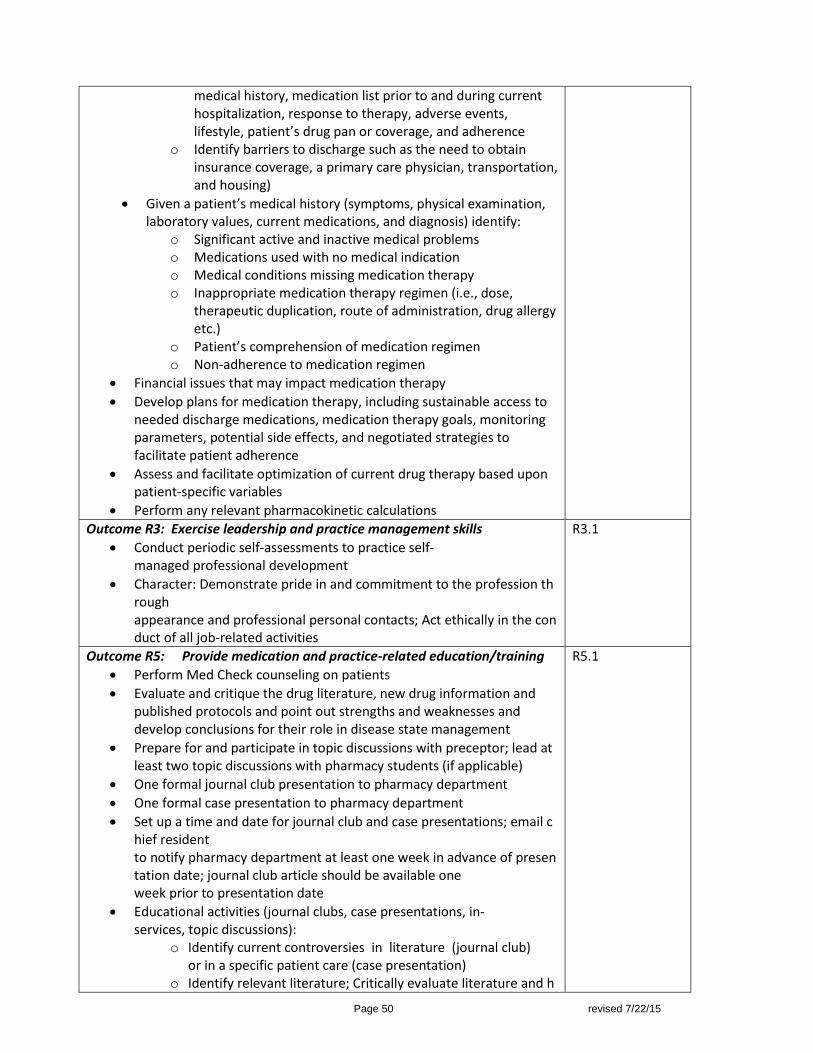
Page 50 revised 7/22/15
medical history, medication list prior to and during current hospitalization, response to therapy, adverse events, lifestyle, patient’s drug pan or coverage, and adherence
o Identify barriers to discharge such as the need to obtain insurance coverage, a primary care physician, transportation, and housing)
Given a patient’s medical history (symptoms, physical examination, laboratory values, current medications, and diagnosis) identify:
o Significant active and inactive medical problems o Medications used with no medical indication o Medical conditions missing medication therapy o Inappropriate medication therapy regimen (i.e., dose,
therapeutic duplication, route of administration, drug allergy etc.)
o Patient’s comprehension of medication regimen o Non-adherence to medication regimen
Financial issues that may impact medication therapy
Develop plans for medication therapy, including sustainable access to needed discharge medications, medication therapy goals, monitoring parameters, potential side effects, and negotiated strategies to facilitate patient adherence
Assess and facilitate optimization of current drug therapy based upon patient-specific variables
Perform any relevant pharmacokinetic calculations
Outcome R3: Exercise leadership and practice management skills
Conduct periodic self-assessments to practice self-managed professional development
Character: Demonstrate pride in and commitment to the profession through appearance and professional personal contacts; Act ethically in the conduct of all job-related activities
R3.1
Outcome R5: Provide medication and practice-related education/training
Perform Med Check counseling on patients
Evaluate and critique the drug literature, new drug information and published protocols and point out strengths and weaknesses and develop conclusions for their role in disease state management
Prepare for and participate in topic discussions with preceptor; lead at least two topic discussions with pharmacy students (if applicable)
One formal journal club presentation to pharmacy department
One formal case presentation to pharmacy department
Set up a time and date for journal club and case presentations; email chief resident to notify pharmacy department at least one week in advance of presentation date; journal club article should be available one week prior to presentation date
Educational activities (journal clubs, case presentations, in-services, topic discussions):
o Identify current controversies in literature (journal club) or in a specific patient care (case presentation)
o Identify relevant literature; Critically evaluate literature and h
R5.1

Page 51 revised 7/22/15
ow they add information/clarity to area of controversy o Use public speaking skills to effectively communicate educatio
nal goals; Use audio-visual aids and handouts to enhance communication of educational goals
Provide drug information to other health-care professionals as needed.
Precept pharmacy students (when applicable): o Serve as prerounding preceptor; Facilitate/Lead topic discuss
ions o Assist the student in following
up on patient issues following rounds o Identify and implement the four preceptor roles as appropri
ate for the student and the activity (direct instruction, modeling, coaching and facilitation)
Contribute to the students’ evaluations Outcome R6: Utilize medical informatics
Concisely, clearly, and effectively document any interventions, assessments and recommendations as a new i-Vent (minimum of 125- per residency requirements)
Report any adverse events per institutional reporting policies and procedures (IRIS)
R6.1
Preceptor Interactions-Variable and resident-specific. 0900:0930: Morning discharge rounds (week 1 only) 0930-1200: Review potential daily discharges, chart review, follow-up phone calls, medication reconciliation 1200-1300: Pre-round with resident, topic discussion (Fridays)
1300-1400: Discharge rounds with resident and discharge team 1430-1730: Follow up phone calls to patients, discharge counseling, medication reconciliation, patient updates Expected progression of resident responsibility on the Transition of Care experience: Day1: 0900: Preceptor provides orientation to service, hospital, nursing floors, and reviews Transition of Care
learning activities and expectations. Week 1-2: Resident works up patients and presents to preceptor prior to rounds and patient care activities.
Preceptor will attend and participate in patient care activities to model pharmacist’s role. Week 3-4: Resident continues to work up patients and presents to preceptor prior to rounds and patient
care activities. Preceptor may attend and participate in patient care activities to coach the resident to take on more responsibilities as the primary pharmacist. In addition, if there is a pharmacy student on the team, the resident will take on the responsibility of a co-preceptor role.
Week 5-6: Resident continues to work up patients and presents to preceptor prior to rounds and patient care activities. Preceptor may attend and observe the resident’s participation in patient care activities, and/or may expect a summary report from the resident on recommendations made by the resident, updates on patients, and student progress. Preceptor will always be available via pager, phone, or cell for questions, and may follow patients independently to monitor resident skill development in all aspects of the learning experience to help facilitate the resident as the pharmacist.
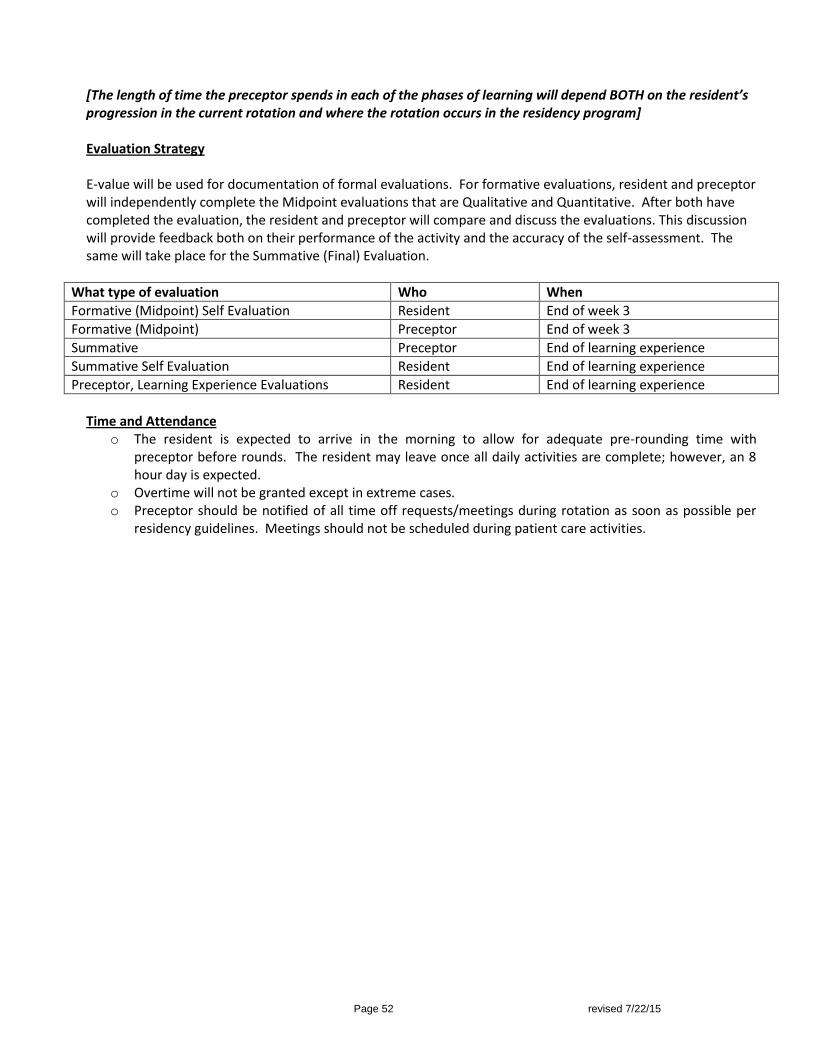
Page 52 revised 7/22/15
[The length of time the preceptor spends in each of the phases of learning will depend BOTH on the resident’s progression in the current rotation and where the rotation occurs in the residency program] Evaluation Strategy E-value will be used for documentation of formal evaluations. For formative evaluations, resident and preceptor will independently complete the Midpoint evaluations that are Qualitative and Quantitative. After both have completed the evaluation, the resident and preceptor will compare and discuss the evaluations. This discussion will provide feedback both on their performance of the activity and the accuracy of the self-assessment. The same will take place for the Summative (Final) Evaluation.
What type of evaluation Who When
Formative (Midpoint) Self Evaluation Resident End of week 3
Formative (Midpoint) Preceptor End of week 3
Summative Preceptor End of learning experience
Summative Self Evaluation Resident End of learning experience
Preceptor, Learning Experience Evaluations Resident End of learning experience
Time and Attendance
o The resident is expected to arrive in the morning to allow for adequate pre-rounding time with preceptor before rounds. The resident may leave once all daily activities are complete; however, an 8 hour day is expected.
o Overtime will not be granted except in extreme cases. o Preceptor should be notified of all time off requests/meetings during rotation as soon as possible per
residency guidelines. Meetings should not be scheduled during patient care activities.
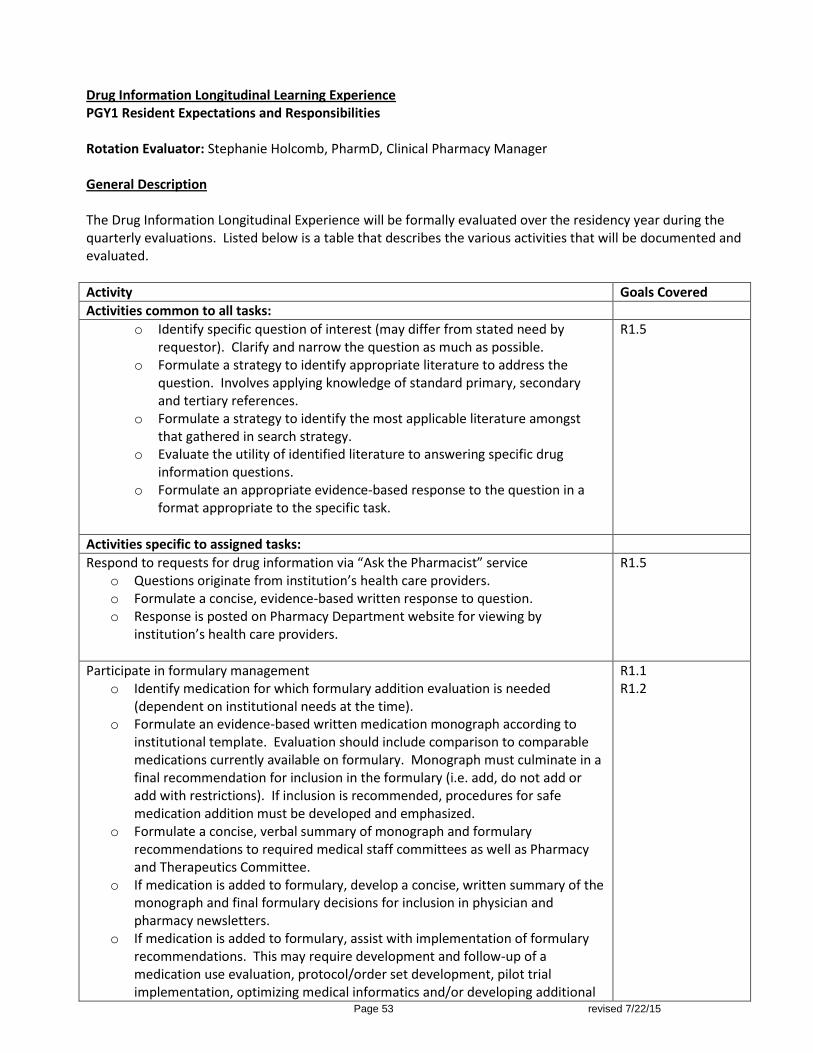
Page 53 revised 7/22/15
Drug Information Longitudinal Learning Experience PGY1 Resident Expectations and Responsibilities Rotation Evaluator: Stephanie Holcomb, PharmD, Clinical Pharmacy Manager General Description The Drug Information Longitudinal Experience will be formally evaluated over the residency year during the quarterly evaluations. Listed below is a table that describes the various activities that will be documented and evaluated.
Activity Goals Covered
Activities common to all tasks:
o Identify specific question of interest (may differ from stated need by requestor). Clarify and narrow the question as much as possible.
o Formulate a strategy to identify appropriate literature to address the question. Involves applying knowledge of standard primary, secondary and tertiary references.
o Formulate a strategy to identify the most applicable literature amongst that gathered in search strategy.
o Evaluate the utility of identified literature to answering specific drug information questions.
o Formulate an appropriate evidence-based response to the question in a format appropriate to the specific task.
R1.5
Activities specific to assigned tasks:
Respond to requests for drug information via “Ask the Pharmacist” service o Questions originate from institution’s health care providers. o Formulate a concise, evidence-based written response to question. o Response is posted on Pharmacy Department website for viewing by
institution’s health care providers.
R1.5
Participate in formulary management o Identify medication for which formulary addition evaluation is needed
(dependent on institutional needs at the time). o Formulate an evidence-based written medication monograph according to
institutional template. Evaluation should include comparison to comparable medications currently available on formulary. Monograph must culminate in a final recommendation for inclusion in the formulary (i.e. add, do not add or add with restrictions). If inclusion is recommended, procedures for safe medication addition must be developed and emphasized.
o Formulate a concise, verbal summary of monograph and formulary recommendations to required medical staff committees as well as Pharmacy and Therapeutics Committee.
o If medication is added to formulary, develop a concise, written summary of the monograph and final formulary decisions for inclusion in physician and pharmacy newsletters.
o If medication is added to formulary, assist with implementation of formulary recommendations. This may require development and follow-up of a medication use evaluation, protocol/order set development, pilot trial implementation, optimizing medical informatics and/or developing additional
R1.1 R1.2
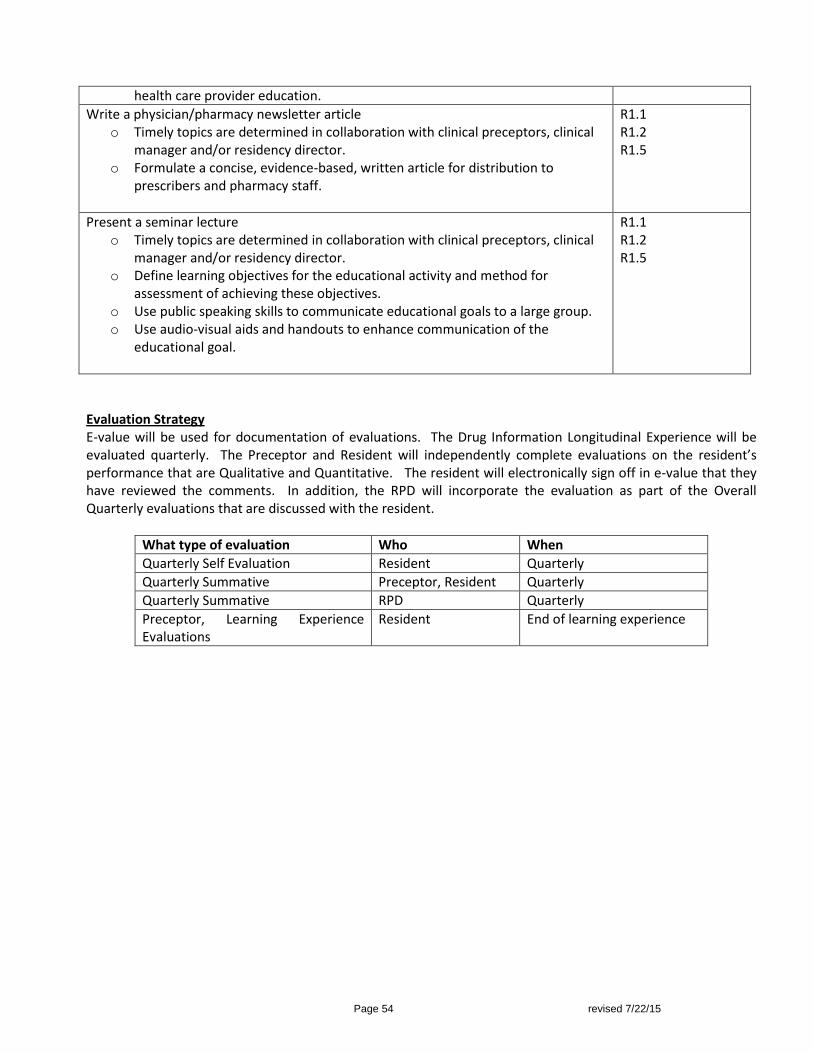
Page 54 revised 7/22/15
health care provider education.
Write a physician/pharmacy newsletter article o Timely topics are determined in collaboration with clinical preceptors, clinical
manager and/or residency director. o Formulate a concise, evidence-based, written article for distribution to
prescribers and pharmacy staff.
R1.1 R1.2 R1.5
Present a seminar lecture o Timely topics are determined in collaboration with clinical preceptors, clinical
manager and/or residency director. o Define learning objectives for the educational activity and method for
assessment of achieving these objectives. o Use public speaking skills to communicate educational goals to a large group. o Use audio-visual aids and handouts to enhance communication of the
educational goal.
R1.1 R1.2 R1.5
Evaluation Strategy E-value will be used for documentation of evaluations. The Drug Information Longitudinal Experience will be evaluated quarterly. The Preceptor and Resident will independently complete evaluations on the resident’s performance that are Qualitative and Quantitative. The resident will electronically sign off in e-value that they have reviewed the comments. In addition, the RPD will incorporate the evaluation as part of the Overall Quarterly evaluations that are discussed with the resident.
What type of evaluation Who When
Quarterly Self Evaluation Resident Quarterly
Quarterly Summative Preceptor, Resident Quarterly
Quarterly Summative RPD Quarterly
Preceptor, Learning Experience Evaluations
Resident End of learning experience
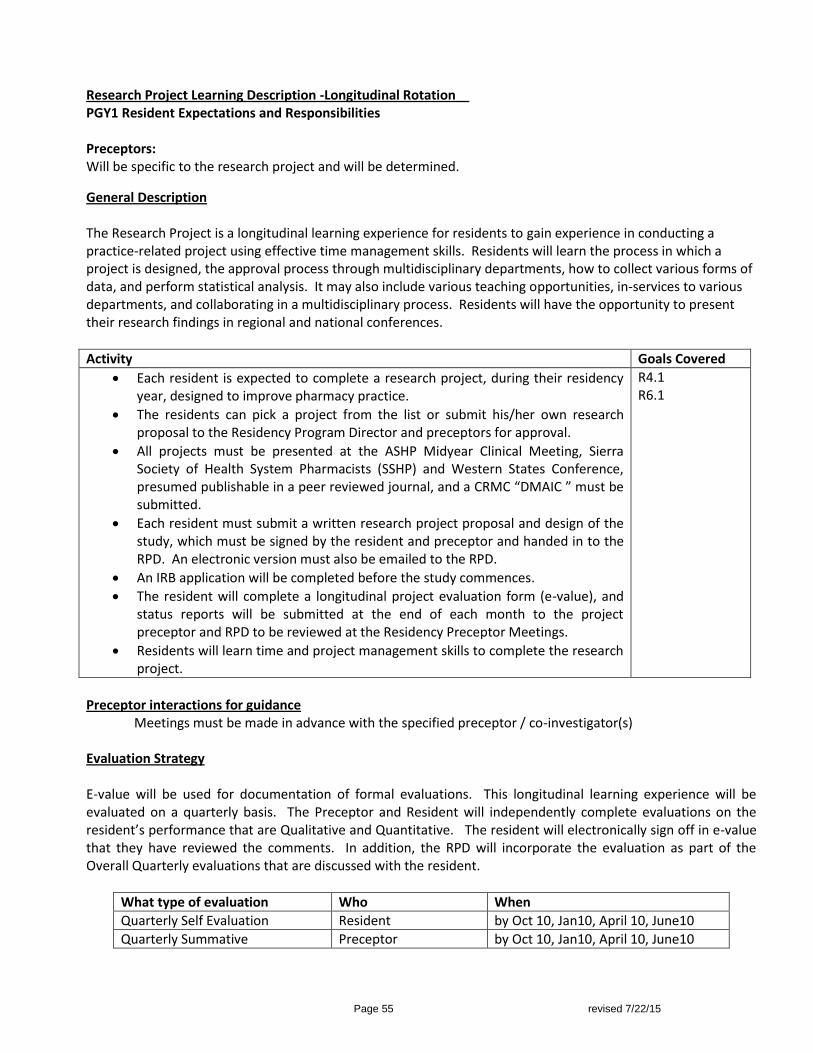
Page 55 revised 7/22/15
Research Project Learning Description -Longitudinal Rotation PGY1 Resident Expectations and Responsibilities Preceptors: Will be specific to the research project and will be determined.
General Description The Research Project is a longitudinal learning experience for residents to gain experience in conducting a practice-related project using effective time management skills. Residents will learn the process in which a project is designed, the approval process through multidisciplinary departments, how to collect various forms of data, and perform statistical analysis. It may also include various teaching opportunities, in-services to various departments, and collaborating in a multidisciplinary process. Residents will have the opportunity to present their research findings in regional and national conferences.
Activity Goals Covered
Each resident is expected to complete a research project, during their residency year, designed to improve pharmacy practice.
The residents can pick a project from the list or submit his/her own research proposal to the Residency Program Director and preceptors for approval.
All projects must be presented at the ASHP Midyear Clinical Meeting, Sierra Society of Health System Pharmacists (SSHP) and Western States Conference, presumed publishable in a peer reviewed journal, and a CRMC “DMAIC ” must be submitted.
Each resident must submit a written research project proposal and design of the study, which must be signed by the resident and preceptor and handed in to the RPD. An electronic version must also be emailed to the RPD.
An IRB application will be completed before the study commences.
The resident will complete a longitudinal project evaluation form (e-value), and status reports will be submitted at the end of each month to the project preceptor and RPD to be reviewed at the Residency Preceptor Meetings.
Residents will learn time and project management skills to complete the research project.
R4.1 R6.1
Preceptor interactions for guidance
Meetings must be made in advance with the specified preceptor / co-investigator(s) Evaluation Strategy E-value will be used for documentation of formal evaluations. This longitudinal learning experience will be evaluated on a quarterly basis. The Preceptor and Resident will independently complete evaluations on the resident’s performance that are Qualitative and Quantitative. The resident will electronically sign off in e-value that they have reviewed the comments. In addition, the RPD will incorporate the evaluation as part of the Overall Quarterly evaluations that are discussed with the resident.
What type of evaluation Who When
Quarterly Self Evaluation Resident by Oct 10, Jan10, April 10, June10
Quarterly Summative Preceptor by Oct 10, Jan10, April 10, June10

Page 56 revised 7/22/15
SECTION F – FORMS AND GUIDELINES
Residency Guidelines for Journal Club (JC) and Case Presentations (CP) - The intent of Journal Club is to review how the article will impact clinical practice. In order to do this, you need to critically evaluate the article against current clinical practice and use your judgment if this will change or impact clinical practice. **These are guidelines for both JC and CP and may be changed under the discretion of the preceptor**
Topic to be chosen and announced 1 week PRIOR to the presentation, by the Chief Resident, to allow time for preceptors to review and participate.
Journal Club and Case Presentations will be held on the 3rd and 5th weeks, respectively, of the core rotation on Tuesday or Wednesday from 12:30-1:30 pm. If there is a resident on Ambcare rotation or there are conflicting meetings, then the times and dates may change.
Due to time constraints, do not go over your 30 minute allotted time (20 minutes maximum to present and 10 minutes for Questions)***** You will be timed.
Please be courteous and be aware if there is another meeting scheduled afterwards. Journal Club (JC): 20 minutes to present and 10 minutes for Questions = 30 minutes maximum
Article must be from a peer-reviewed journal.
Article must be published within the last 3-6 months.
Topic must be related to the current rotation.
Email a copy of the article to CRMC_RX with the date/time 1 week before presentation.
A handout must accompany the presentation—optional per preceptor.
One journal club to be presented per Core clinical rotation. Case Presentations (CP) or New Drug presentation –Power Point presentation: 20 minutes to present and 10 minutes for Questions = 30 minutes maximum (Think of the presentation as “The use of ____in the treatment of ____”, or like “clinical pearls”)
3 - 5 minutes for patient case.
15 minutes on topic/disease state and a literature review.
10 Minutes for questions.
**Topic to be approved by rotation preceptor and reviewed prior to the actual presentation***
Handout of Power Point slides to be provided
One case presentation OR new drug presentation per Core clinical rotation. Choice of cases: must be a narrow topic
1. Rare or interesting disease states – Broad disease states are NOT appropriate (Examples: Lung cancer, hepatic encephalopathy, Community Acquired Pneumonia, Pulmonary Embolism). Broad disease states must have a focus.
If disease states are chosen, then focus on the evaluation of the treatments available or treatment-induced side effects. Examples are: -Lung Cancer: Non-standard of care treatment or severe chemotherapy induced side effects -Hepatic Encephalopathy: Treatment controversies or lactulose versus antibiotics. -Pulmonary embolism: Treatment with LMWH vs. unfractionated heparin or thrombolytic therapy.
Narrow topic examples are: Pulmonary hypertension, cryptococcal meningitis, tetanus, disseminated histoplasmosis, ethylene glycol overdose, heparin induced thrombocytopenia with thrombosis.
Page 57 revised 7/22/15
2. New Drug or Controversial Treatments
Examples are: Use of Aspirin for VTE prophylaxis in orthopedic patients, or Phenytoin versus Levetiracetam for Post-traumatic brain injury early seizure prophylaxis.
Literature Evaluation
The best 2 – 3 studies from primary literature should be presented.
Resident should evaluate the articles and formulate conclusions for each and then apply those to the patient case.
Articles should be clinically relevant to the case. **Upon discretion of the preceptors, case presentations or journal club will be repeated with a new case or new article if done inadequately**
Alternative project presentation guidelines Discussion - suggestion to replace a Case Presentation (CP) with a project.
Rationale -resident will serve as an extension to help their preceptor complete a rotation appropriate project
that adds value to the resident’s learning experience and institutional practice.
Resident will continue to present on the project instead of a normal CP during scheduled CP times. Current CP
rules will apply: Power Point presentation, 20 minute time limit, and preceptors will complete
evaluations. Project must be something that can be completed during the time on rotation, before week 5
(normal CP times).
Process:
Will consider a minimum of 2 CP per year, based on resident’s performance. If the resident exhibits exceptional CP skills on their first one, then the resident may not have to complete the second one. This will provide flexibility.
The resident will not be provided this option for Rotation 1 (to evaluate performance and determine baseline presentation skills).
If a resident wants to pursue this option, the resident must complete an email “request” to the Preceptor and RPD for documentation.
o Request must be completed either before the rotation begins or during week 1 of the rotation. o Request will include at minimum: Title, topic, rationale or objectives for project.
RPD and preceptor will have a discussion before a decision is made. The RPD will notify the resident of the decision.
Preceptors can require CP on their rotation (preceptor preference). Other Information: Chief Resident will send an email out to all preceptors, residents and other pharmacists to attend the presentation (send email to CRMC_RX and CRMC Clinical Pharmacy Specialists distribution lists)
Copies of the journal club articles will be made available to preceptors and guests at least 1 week prior
to the presentation (pdf attachments are appreciated).
All residents and preceptors are expected to complete the evaluations and submit them electronically on E-value.
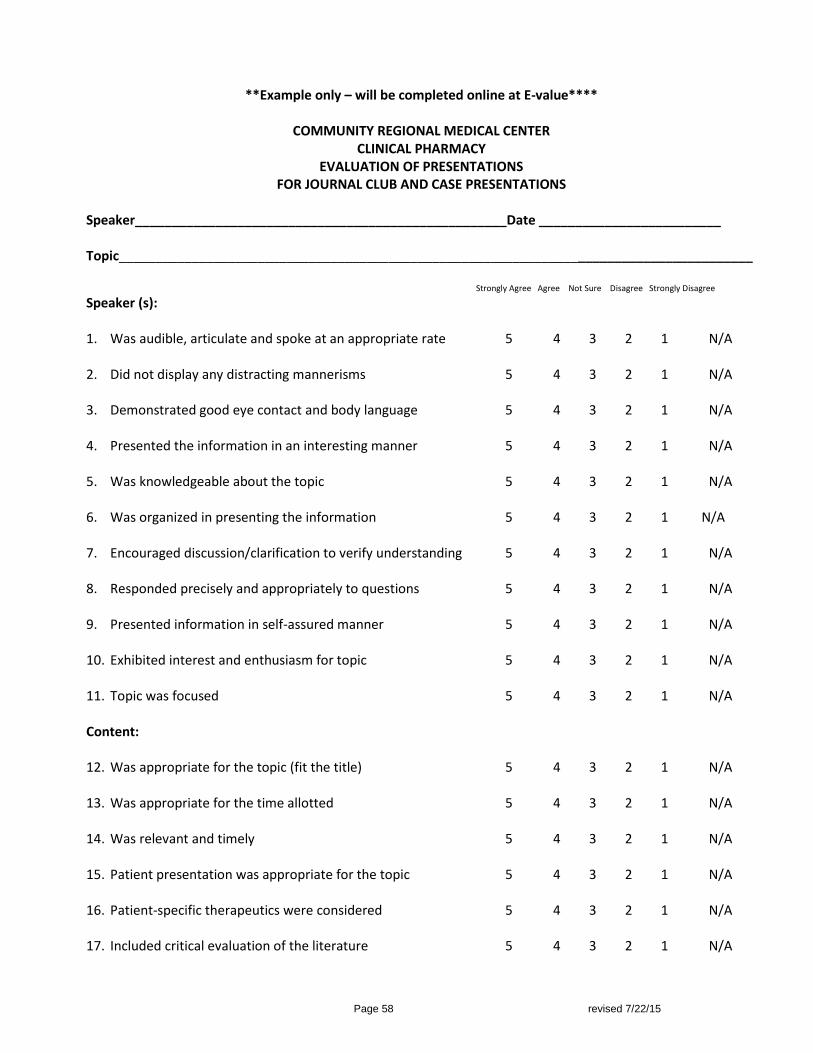
Page 58 revised 7/22/15
**Example only – will be completed online at E-value****
COMMUNITY REGIONAL MEDICAL CENTER CLINICAL PHARMACY
EVALUATION OF PRESENTATIONS FOR JOURNAL CLUB AND CASE PRESENTATIONS
Speaker___________________________________________________Date _________________________ Topic_______________________________________________________________________________________ Strongly Agree Agree Not Sure Disagree Strongly Disagree
Speaker (s): 1. Was audible, articulate and spoke at an appropriate rate 5 4 3 2 1 N/A 2. Did not display any distracting mannerisms 5 4 3 2 1 N/A 3. Demonstrated good eye contact and body language 5 4 3 2 1 N/A 4. Presented the information in an interesting manner 5 4 3 2 1 N/A 5. Was knowledgeable about the topic 5 4 3 2 1 N/A 6. Was organized in presenting the information 5 4 3 2 1 N/A 7. Encouraged discussion/clarification to verify understanding 5 4 3 2 1 N/A 8. Responded precisely and appropriately to questions 5 4 3 2 1 N/A 9. Presented information in self-assured manner 5 4 3 2 1 N/A 10. Exhibited interest and enthusiasm for topic 5 4 3 2 1 N/A 11. Topic was focused 5 4 3 2 1 N/A
Content: 12. Was appropriate for the topic (fit the title) 5 4 3 2 1 N/A 13. Was appropriate for the time allotted 5 4 3 2 1 N/A 14. Was relevant and timely 5 4 3 2 1 N/A 15. Patient presentation was appropriate for the topic 5 4 3 2 1 N/A
16. Patient-specific therapeutics were considered 5 4 3 2 1 N/A 17. Included critical evaluation of the literature 5 4 3 2 1 N/A
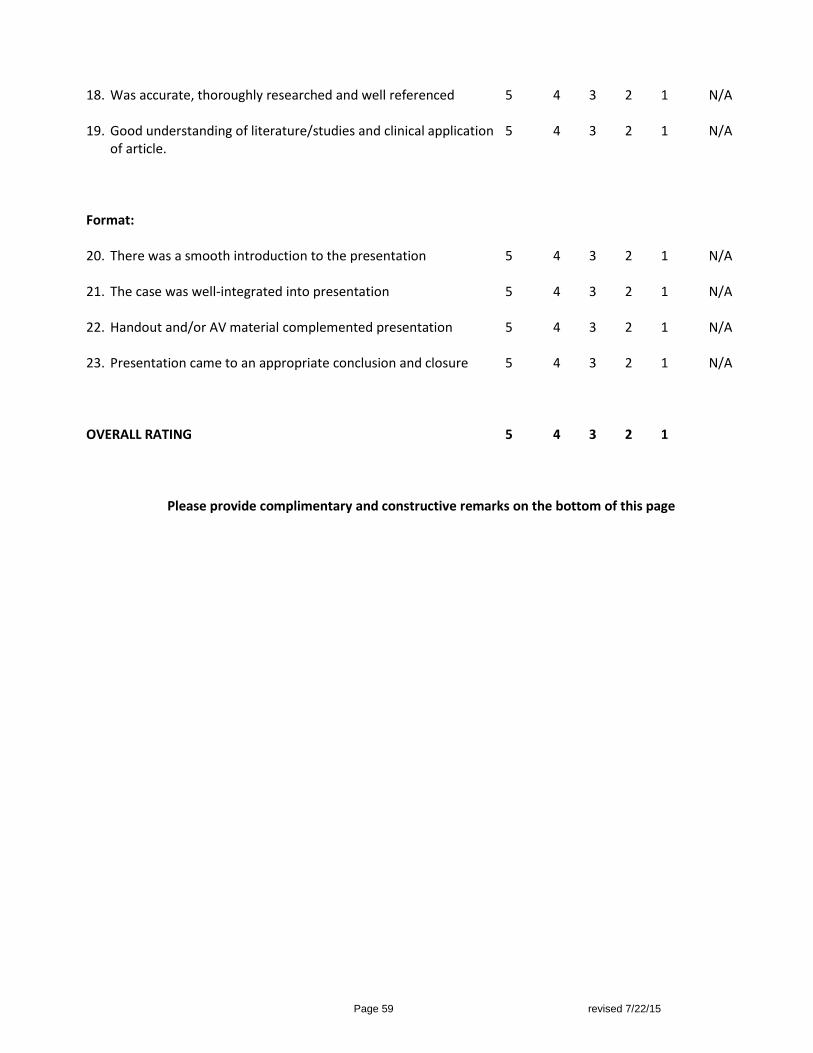
Page 59 revised 7/22/15
18. Was accurate, thoroughly researched and well referenced 5 4 3 2 1 N/A 19. Good understanding of literature/studies and clinical application 5 4 3 2 1 N/A
of article. Format: 20. There was a smooth introduction to the presentation 5 4 3 2 1 N/A 21. The case was well-integrated into presentation 5 4 3 2 1 N/A 22. Handout and/or AV material complemented presentation 5 4 3 2 1 N/A 23. Presentation came to an appropriate conclusion and closure 5 4 3 2 1 N/A OVERALL RATING 5 4 3 2 1
Please provide complimentary and constructive remarks on the bottom of this page

Page 60 revised 7/22/15
Resident Seminar Guidelines Each resident will present one formal Resident Seminar during the residency program. The goal of the Resident Seminar is to expand the resident's communication skills, critical evaluation of literature, and formal presentation techniques. The Resident Seminar topic will be chosen by the resident, with guidance from a Preceptor/Mentor, (who will ensure the integrity of the seminar is intact, and must be consulted with all aspects of the Resident Seminar), and involve a therapeutic or practice management topic that fits the needs of the department. This will be done with a “needs assessment”. The resident will be responsible for identifying and requesting a preceptor for their seminar. Together, the preceptor and resident will choose a timeline for seminar completion, in accordance with ACPE requirements. The location of the seminar will be at the discretion of the RPD. The CE seminar will be in conjunction with the UCSF School of Pharmacy, and the resident will work with the UCSF PEP for ACPE CE accreditation of their seminar. Please see table with timelines for reference on page 61 (will be updated) and contact Mitra Assemi to schedule an appointment for requirements in July. The objectives of the Resident Seminar include the following:
1. Critical evaluation of the literature. 2. Advancement of presentation, teaching, and communication skills. 3. Provision of continuing education for pharmacists and other health care professionals. 4. Development of skills in responding to audience questions and comments. 5. Familiarization with different audiovisual equipment and techniques.
The length of the Resident Seminar will be 50 minutes, with 10 minutes afterwards reserved for
questions and/or comments from the audience. Each Seminar will incorporate a patient case to exemplify the objectives of the seminar. Each Seminar will require a slide or handout pertaining to dosing considerations for drug therapy Each resident will receive a critique of the seminar from a minimum of two preceptors who will
evaluate the presentation on the basis of content, presentation style, and overall quality. The resident must request the preceptors at least one day in advance of the seminar. The evaluations will be handed to the preceptors picked by the resident, and will be discussed with the resident immediately after the presentation.
The audience will also be encouraged to submit written comments to the resident using the seminar evaluation form provided. Preceptors will complete evaluations via E-value.
The title of all the Resident Seminars will be submitted to the RPD by October 1st of each year. Residents will present their seminars during the month of February. The RPD will schedule the time. All residents are required to attend all of the Resident Seminar series.
After the Seminar:
1. Review the audience evaluation forms with your seminar preceptor. 2. Audience Evaluations will be completed electronically. 3. UCSF will collate evaluations and send to the resident and RPD.
Seminar presentation room -Residents are to assume that no podium or microphone will be provided. It is strongly suggested to visit your presentation room before you present.

Page 61 revised 7/22/15
Page 62 revised 7/22/15
Research projects for 2015-2016 ***all must include a cost savings component***
Administration: 1. Development and implementation of comprehensive medication safety plan for pharmacy services.
Preceptor: Curtis Takemoto 2. Evaluation of effectiveness of CRMC formulary usage and non-usage patterns and non-formulary usage.
Determine cost of non-formulary usage and missed cost savings if formulary alternative was used. Preceptor: Stephanie Holcomb
3. Development and implementation of antimicrobial stewardship program for Patient Centered Integrated Practice (PCIP) pharmacists. Preceptor: Stephanie Holcomb
Ambulatory Care / Inpatient: Preceptors: Mallory Cruz, Giovanni Lares, and Linda Kimura 1. Incidence of venous thromboembolism among inpatients with chronic liver disease at CRMC 2. Effect of free medications at hospital discharge on patient outcomes 3. Incidence of thrombosis in patients with new heart valves with lower INR goal 4. Effectiveness of a Pharmacist involvement in a Smoking-Cessation Program 5. Identifying and Quantifying Ambulatory Care Pharmacists Interventions in the Amb Care Setting
Critical Care: Preceptor: Melissa Reger (Burn/Surgery)
1. Evaluation of IVC filter use on DVT prophylaxis and rate of complications and associated costs (heparin infusions, lab costs).
2. Incidence of VTE events in the face of appropriate prophylaxis in trauma, surgery and burn patients and associated costs (heparin infusions, lab costs).
3. Assessment of IV acetaminophen intake in hospitalized patients (MUE) 4. Limiting of epogen use in acute renal failure- a cost savings analysis. 5. Safety and timing of chemical VTE prophylaxis in patients with traumatic brain injury (does early VTE
prophylaxis lead to a higher incidence of rebleeding?) 6. Correlation of anti-Xa levels and incidence of VTE in Burn patients (funding required) 7. Blood utilization in THA/TKA patients that have received tranexamic acid. 8. Incidence of bacteremia with TPN with a new line vs. used line 9. Audit of TPN prescribing practice similar to one performed prior: are our patients achieving nutrition
goals with pharmacist vs. physician prescribing 10. Mortality benefit/blood product utilization in trauma patients receiving tranexamic acid as part of the
massive transfusion protocol (continuation of Teresa’s project). 11. Vitamin D levels in burn patients should we be supplementing? Adverse effects from low vitamin D
levels? 12. Evaluation of safety and efficacy of FEIBA in trauma patients (continuation of Dr. Hubbard project) 13. Vancomycin/aminoglycoside/antibiotic dosing protocol in burn patients
Preceptor: Tou Bee Thao 1. Retrospective review of the efficacy and safety of FEIBA in reversing coagulopathy in warfarin associated
intracerebral hemorrhages.
2. Retrospective review of efficacy of phenytoin versus levetiracetam for seizure prophylaxis in
spontaneous intracerebral hemorrhages (and/or subarachnoid hemorrhages).
Preceptor Ann Vu: 1. Efficacy and safety of 7.5% hypertonic saline as primary therapy for management of intracranial
hypertension. 2. Safety and efficacy of valproic acid for refractory agitation after traumatic brain injury. 3. Use of quetiapine versus risperidone for ICU agitation. 4. Venous Thromboembolism Prophylaxis following neurosurgery in Critically Ill patients 5. Consult with preceptor for additional project ideas.

Page 63 revised 7/22/15
Joint ED/Critical Care: Preceptors: Ann Vu, Gillian Pineda and Leonard Valdez 6. Safety and efficacy of liposomal bupivacaine for pain management of rib fractures (Dr. Parks) 7. Retrospective review of the efficacy and safety of FEIBA versus FFP in reversing non-warfarin associated
supra-therapeutic INR (Dr. Hubbard)
Emergency Medicine: Preceptors: Gillian Pineda and Leonard Valdez 1. Treatment of acute decompensated heart failure with intravenous nitroglycerin: high-dose bolus dosing
versus conventional bolus with continuous infusion dosing. 2. Safety and efficacy of 3% hypertonic saline boluses versus continuous infusion in symptomatic, severe
hyponatremia. 3. Medication use evaluation (MUE) of propofol in procedural sedation (specifically, was an analgesic agent
used in combination with propofol)? a. Develop and implement usage guidelines for procedural sedation.
4. Medication use evaluation of hyperinsulinemia euglycemia therapy in calcium channel blocker or beta blocker overdose.
a. Develop and implement usage guidelines for calcium channel blocker or beta blocker overdose. 5. MUE of calcium gluconate or calcium chloride in hyperkalemia.
a. Develop and implement usage guidelines for hyperkalemia. 6. Safety of propofol use in pediatric patients. 7. Consult with preceptors for additional project ideas.
Internal Medicine: Preceptor Nicole Lu 1. Targeted medication use evaluations: appropriateness of use, safety, and cost effectiveness. Develop
and implement usage guidelines. Possible medications for review:
Filgrastim/pegfilgrastim
Dabigatran
Rivaroxaban
Stress ulcer prophylaxis - (Alice Robbins co-preceptor)
DVT prophylaxis (Alice Robbins co-preceptor)
TPN/PPN
Factor VII (Novoseven)
Rasburicase
2. Monitor safety and order accuracy of heparin infusions (pharmacy accuracy of nomogram completion, nursing adherence to nomogram, bleeding and thrombosis outcomes).
3. Appropriate use of antibiotics and steroids in asthma/COPD exacerbation. 4. Develop order set for management of hypertensive urgency/emergency. 5. Develop order set for management of cirrhotic patients including management of ascites, SBP, hepatic
encephalopathy, and variceal hemorrhage. 6. Evaluate the appropriateness of phenytoin dosing and management (Alice Robbins co-preceptor). 7. See preceptor for additional project ideas.
Neonatal Intensive Care Unit: Preceptors Harlan Husted and George Lien 1. Implementation of a pharmacy-managed erythropoietin protocol service in a neonatal intensive care
unit (NICU). a. Develop an official protocol to manage EPO therapy in the neonatal population to allow a
pharmacist to adjust dosage, monitor and order pertinent labs and to discontinue EPO therapy once eligibility criteria is satisfied.
b. Evaluate the cost-savings benefit to implementing this clinical pharmacy service in terms of drug cost utilization in patients not satisfying eligibility criteria, increasing/reducing lab draw frequency and assessing physician satisfaction scoring.
2. Implementation of a pharmacy-managed total parenteral nutrition protocol in a NICU. a. Develop an official protocol to manage TPN therapy in the neonatal population to allow a
pharmacist to evaluate and adjust nutrient dosages, monitor and order pertinent labs and to ensure adherence to ASPEN nutrition guidelines.

Page 64 revised 7/22/15
b. Evaluate the cost-savings benefit to implementing this clinical pharmacy service in terms of drug cost utilization in patients not satisfying eligibility criteria, increasing/reducing lab draw frequency and assessing physician satisfaction scoring.
c. Secondary goal to survey need for expansion of this service to the pediatric population at CRMC. 3. Improving pediatric medication safety in a primarily adult-population regional medical center
a. Review recommendations from Institution of Safe Medical Practices (ISMP), American Academy of Pediatrics (AAP), American Society of Health-System Pharmacists (ASHP) and compile common measures to improve pediatric and infant medication safety
b. From the information collected, identify some of the most common pediatric medication errors reported and identify outcomes and costs associated with those outcomes
c. Review CMC data from 2008 onward (when California Children’s Services approved NICU expansion) for IRIS data, safe practices, staff education, capital equipment purchased to gauge increase in medication errors in pediatric/infant population and safety measures to reduce those numbers.
d. Pathways: Conduct a survey of all CCS-approved hospitals (180 as of May 2014) with similar bed size/patient population to see what safety measures implemented in past 5 years, possible number of adverse events reported or prevented, types of education, specialist recruitment, equipment, etc.
e. Pathways: Assess the value of implementing measures, in terms of cost to institution to prevent errors, mitigate risk/damages, assess multidisciplinary staff comfort in different areas of competency and support of pediatric/infant populations.
f. Goal of study is 2-fold: Present poster of strategies that other facilities have implemented to improve specific population safety, gauging performance of those strategies and offer guides on feasible implementation at other facilities, with potential cost-risk/benefit component assessed.
g. Potential for publication to medical journals as an editorial/how-to guide, or case report type article.
Transition of Care: Preceptor Tamar Lawful
1. Cost Savings Associated with Transition of Care Pharmacy Interventions. 2. The Impact of Pharmacist-led Discharge Counseling on 30-day Readmissions. 3. Pharmacy Evaluation of Medication Discrepancies at Hospital Discharge. 4. Expansion of Transition of Care Pharmacy Services (Alice Robbins co-preceptor)

Page 65 revised 7/22/15
*Example only – will be completed on line at E-value**** PRECEPTOR AND LEARNING EXPERIENCE EVALUATION
Resident:
Preceptor:
Learning Experience: Evaluation Period: through
Please check one of the following for each category.
1 - ALWAYS 2 - FREQUENTLY 3 - SOMETIMES 4 - NEVER
Part 1 - Evaluation of the Preceptor
1
2
3
4
1.
The preceptor was a pharmacy practice role model.
2.
The preceptor gave me feedback on a regular basis.
3.
The preceptor's feedback helped me improve my performance.
4.
The preceptor was available when I needed him or her.
5.
When possible, the preceptor arranged the necessary learning opportunities to meet my objectives.
6.
The preceptor displayed enthusiasm for teaching.
7.
The preceptor gave clear explanations.
8.
The preceptor asked questions that caused me to do my own thinking.
9.
The preceptor answered my questions clearly.
10.
The preceptor modeled for me, coached my performance, or facilitated my independent work as appropriate.
11.
The preceptor displayed interest in me as a resident.
12.
The preceptor displayed dedication to teaching.
Comments:
Page 66 7/22/2015 updated AR
Please check one of the following for each category. 1 - CONSISTENTLY TRUE 2 - PARTIALLY TRUE 3 - FALSE
Part II: Evaluation of the Learning Experience
1
2
3
1.
I understood the objectives for this learning experience prior to beginning.
2.
The learning opportunities afforded me during this learning experience matched the objectives specified for this experience.
3.
Resources I needed were available to me.
4.
I feel that the preceptor's assessment of my performance on the objectives was fair.
5.
I was encouraged to further develop my ability to self-assess during this learning experience.
6.
This learning experience provided me opportunities to provide pharmaceutical care in a responsible way to my patients.
What were the strengths of this learning experience? What were the weaknesses of this learning experience? What suggestions can you make to improve this learning experience?
Resident's Signature/Date Preceptor's Signature/Date Forward completed evaluation to Residency Program Director

Page 67 7/22/2015 updated AR
Chief Resident Responsibilities: Each resident will rotate through this role. The Chief Resident role will encourage leadership, practice management skills, and practice responsibilities for the residency program. The Chief Resident will act as the liaison between the residents and the RPD to help clarify issues and understand all policies and procedures of the residency program. Responsibilities will vary depending on the period. If a resident leaves the residency program before the end of the year, the Chief Resident Responsibilities will be divided and assigned amongst the remaining residents by the RPD. General Responsibilities - All Year for Each Chief Resident
Coordinate changes in the resident rotation schedule with the RPD and residents Coordinate and schedule Resident and Student JC and CP on the RX Conference Room Calendar, and
disseminate the information -please email an announcement to CRMC_RX, CRMC Clinical Pharmacy Specialists, pharmacy students on rotations, and RPD with the dates and topics
Set up laptop and projector for Friday Seminars and Resident Case Presentations Prepare agenda, take minutes, and schedule monthly resident meetings with the RPD Ensure co-residents are on time for deadlines for projects, conferences, Seminar, etc. A weekly
email with a calendar of events is highly suggested. Responsible for collecting signatures on attendance sheets at all educational functions related to the
residency program, or student program (JC, CP, and lunch seminars) and filing it in the Education binder in the RX conference room. Ensure the topic / speaker is entered on the form.
Helps with any E-value issues Notify RPD to order office supplies as needed, and keep the resident office orderly and neat Chief Resident is responsible for attending P&T each month and disseminating the information at the
monthly Resident Meetings or via email Will check “Ask the Pharmacist” web page on Community Forum daily and keep track of which
resident’s turn it is to answer the question. Reminds co-residents to review P-cards monthly.
Period 1 (July 1 –October 31): Specific Responsibilities will include:
General responsibilities listed above Organize resident contact information for the RPD Coordinate and take group and individual resident photos for website in July (and preceptors) Ensure resident chooses a research project with a cost-savings component, writes a proposal, and
submits to IRB Ensure residents choose a Seminar topic and date Prepare a lecture list and schedule for Lunch Seminars through the end of November, and email list
to RPD for entry into E-value (and email distribution lists above) Schedule residents to present Midyear posters to preceptors before end of November as a Lunch
Seminar Ensure that all residents submit their ASHP abstracts on time (recommend all residents submit
abstracts at the same time to ensure your posters will be close to each other at ASHP) Help coordinate training for E-value software program Help plan resident recruitment, and responsible for CSHP Seminar residency showcase
o Ensure all residents are current members of CSHP and change their local chapter to Sierra Society of Health System Pharmacists (SSHP) for the duration of the residency
Page 68 7/22/2015 updated AR
o Ensure all residents are registered for the CSHP conference and coordinate travel arrangements
o Responsible for the set up and breakdown of the residency showcase - decorations, folders, advertisements for residency program, residency recruitment poster, and giveaways. Arranges for delivery of materials and reshipment if needed
o Responsible for taking photos of the residents at the residency showcase for website Make appointment for UCSF CE accreditation of the Resident Seminar, if not already completed
Period 2 (November 1-February 28) Specific Responsibilities will include:
General responsibilities listed above on previous page Ensure all residents prepare and print their posters for Midyear Help RPD with residency recruitment activities before and at Midyear
o Responsible for the set up and breakdown of the residency showcase at Midyear -decorations, folders, advertisements for residency program, residency recruitment poster, and giveaways. Arranges for delivery of materials and reshipment if needed
o Responsible for taking or ensuring there are photos of each resident with their poster, and residency showcase for website
o Ensure all residents are/must be members of ASHP, registered to go to ASHP and to coordinate travel plans with RPD (typically done in July with collaboration with Chief Resident Period 1)
Organization and communication for the Resident Open House -ensure office is clean and rug shampooed
Prepare a lecture list and schedule for lunch seminars, from January to June (please coordinate with period 3 Chief Resident for date of pre-WSC presentation)
Ensure residents are ready for their Resident Seminars in February Help plan and coordinate the Resident Seminar Residency Interviews:
o Help RPD coordinate the schedules of incoming resident candidates for interviews o Provide the tour of CRMC facilities o Help coordinate plans with RPD, candidates, and current residents o Responsible for meeting with co-residents to evaluate residency candidates,
summarize comments and scores, and final group consensus / submission of evaluation forms to RPD
Ensure WSC abstract submission and WSC registration
Period 3 (March 1-June 30th) Specific Responsibilities will include:
General responsibilities listed above on previous page Coordinate WSC registration and travel plans with RPD Schedule a “pre WSC” presentation to the preceptors by the end of April during the Lunch Seminar
(work with Chief Resident for period 2) Coordinate with SSHP CE board member to present WSC presentation in May
o Ensure all deadlines and materials for CE submission are completed by each resident Ensure ALL deadlines (evaluations, submission of manuscript, submission of DMAIC project, etc.)
and “end of year items” have been met for residents before end of year (see below) Responsible for “end of resident year” items
o Responsible for gathering all pagers and badges o Empty all desks, and remove all personal belongings and files

Page 69 7/22/2015 updated AR
o Schedule exit interviews for each resident and RPD Ensure that the Resident office is clean -floors are vacuumed, refrigerator is cleaned and de-iced,
microwave is cleaned, and all work surfaces are clean Help plan end of residency year (graduation) party Help RPD with tasks needed for next year’s class
SECTION G – CLINICAL PHARMACY SERVICES Preceptor Information -please see website Clinical Pharmacy Services
Clinical pharmacists are available to provide consultations concerning treatment plans, drug dosing, adverse drug effects, etc. Please refer to the in-house telephone and pager list.


















