
2014 Health Care Professional Conference...
130
healthprofessionalconference.com 10th Annual Health Care Professional Conference September 12, 2014 | Vancouver, B.C.
Transcript of 2014 Health Care Professional Conference...
healthprofessionalconference.com
10th Annual
Health Care Professional Conference
September 12, 2014 | Vancouver, B.C.

CBI Health Group is a values-based, results-oriented and collaborative group of companies that is focused on providing improved access and better health outcomes to clients and communities across Canada.
better health begins here.
PART OF THE CBI HEALTH GROUP
www.cbi.ca
CAREPOINT
HEALTHCENTRE
* Note: Only attendees who have given their consent are on the list.
Health Care Professional Conference 3
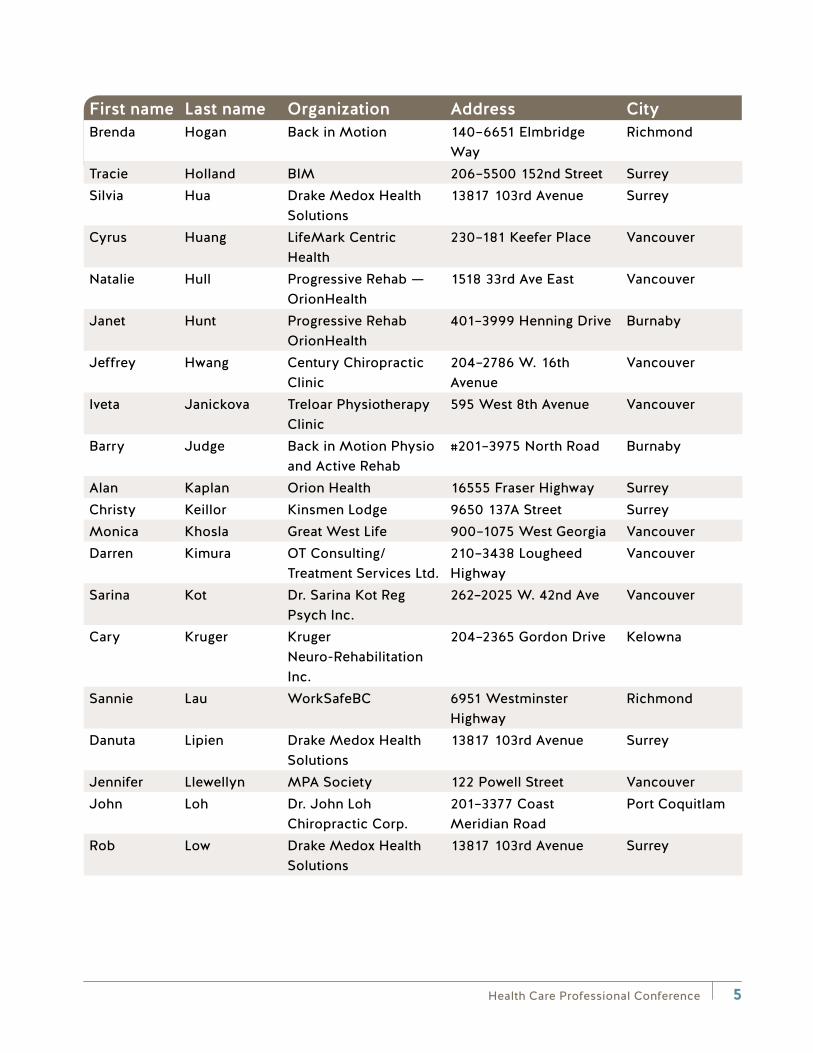
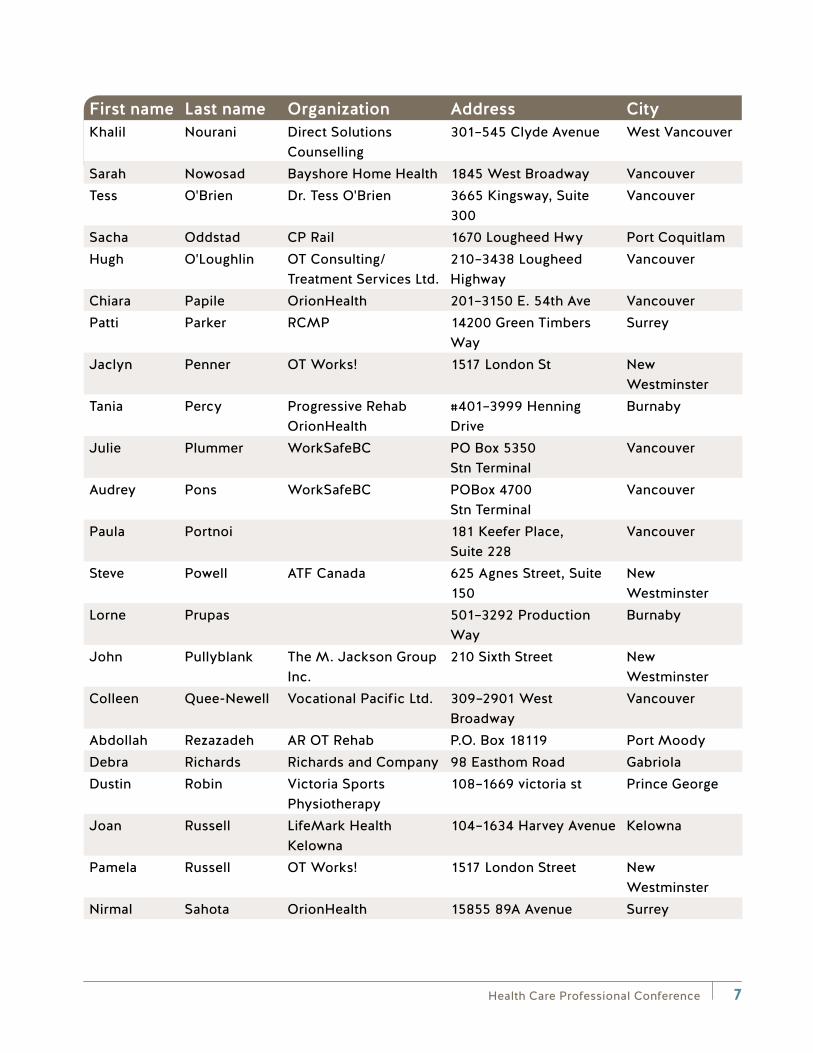
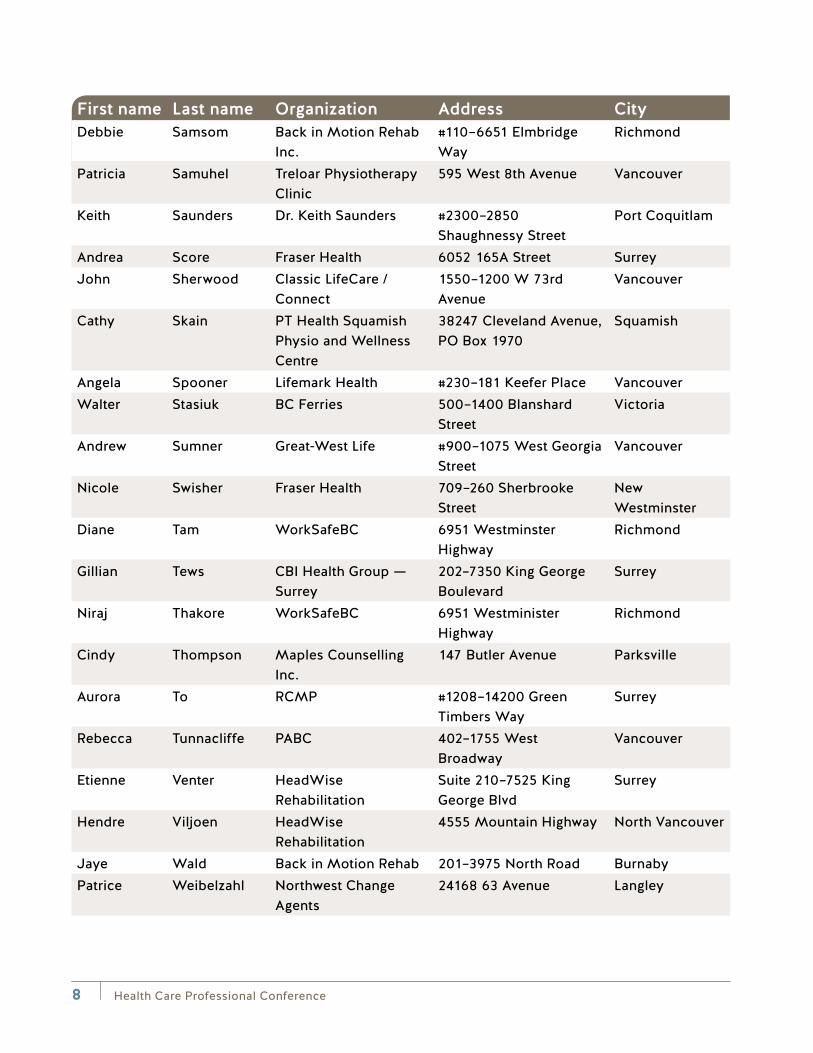
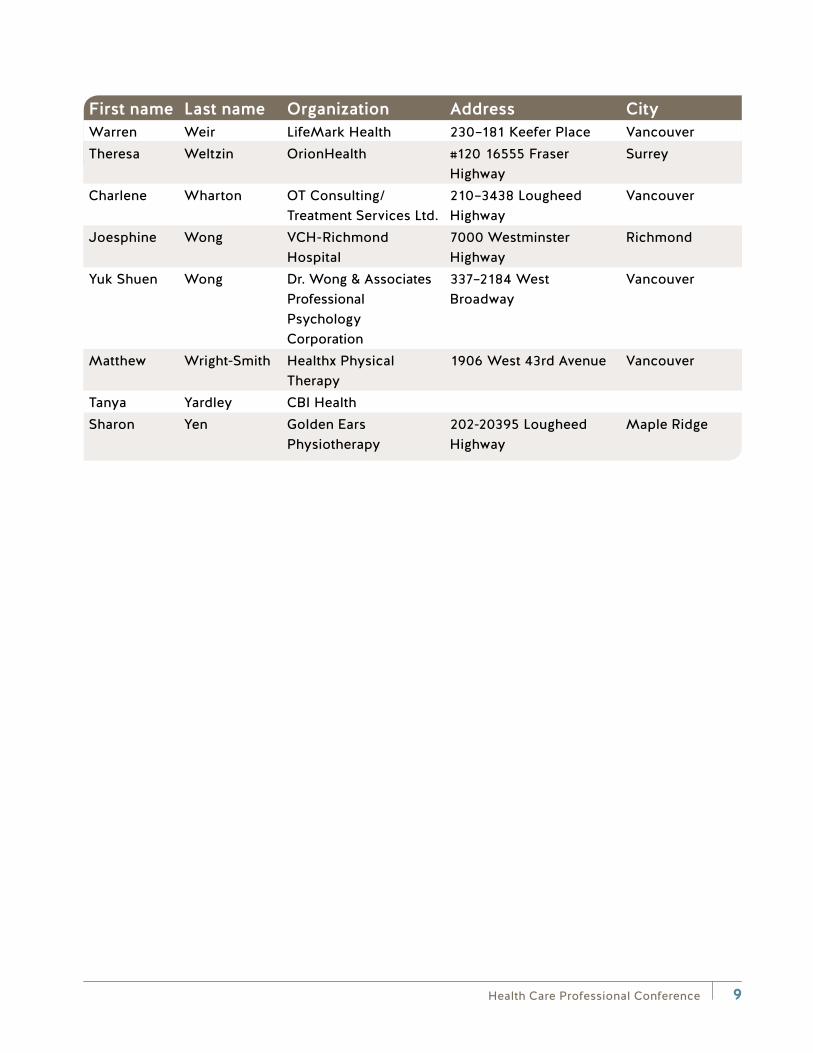
10th Annual Health Care Professional Conference Attendee List*
First name Last name Organization Address CityBrenda Adams Brenda Adams 200–321 Festubert Street DuncanMike Allegretto CBI Workplace
Solutions605 Discovery Street Victoria
Stephen Allen GWL 2nd Floor, 8700–200th Street
Langley
Manouch Amel Mountainview Kinesiology Ltd
1025 Robin Way Anmore
Nikki Anderson Drake Medox Health Solutions
13817 103rd Avenue Surrey
Kristan Ash CBI HealthJennifer Beck Progressive Rehab 401–3999 Henning Drive VancouverColleen Bell WorkSafeBC 157–3031 Williams Road RichmondDave Bernard Back In Motion Physio
and Active Rehab#201–3975 North Road Burnaby
Deepak Bhasin Centric/Lifemark Health
19073–68A Avenue Surrey
Nick Blackman MPA Society 122 Powell Street VancouverGerald Blomme Gerald Cyril Blomme
Psychology Services Professional Corp.
Box 2961 Prince George
Jeff Boniface Boniface |Consulting Occupational Therapy Services
2915 Panorama Drive North Vancouver
David Bruce Vocational Consulting Group
109–2059 Kaltasin Road Sooke
John Buchanan BC Public Service Agency
700–235 1st Avenue Kamloops
Pardeep Chatha Asha Counselling Services
#202–15388 24 Avenue Surrey
Ralph Cheesman Back in Motion Functional Assessments
Suite 110–6651 Elmbridge Way
Richmond
Health Care Professional Conference4
First name Last name Organization Address CityMinda Chittenden Meridian Rehabilitation 3007 28th Avenue VernonHazel Choy Back in Motion #140, 6651 Elmbridge
WayRichmond
Leanna Cousins RCMP 1208- 14200 Green Timbers Way
Surrey
Gordon Davidson 250-542-0660 114 3105 31 Street VernonPeter De Marchi Back in Motion 206–5500 152 Street SurreySuki Dhaliwal RCMP 6699 194st Street SurreyKimberley Dimayuga Progressive Rehab-
Orionhealth401-3999 Henning Drive Burnaby
Robert Douglas Private Hollyoaks #20 Haven Gardens, Crawley Down
West Sussex
Tricia Earl CBI Health Group 716 Rivers Edge Drive Nanoose BayDeb Edwards We Care Health
Services#1108–7330–137th Street Surrey
Philip Fahrni White Rock Orthopaedic & Sports Physio Clinic
#80–1959 152nd Street South Surrey
Roisin Flinn OT Consulting/Treatment Services Ltd.
210–3438 Lougheed Highway
Vancouver
Britney Foster Bayshore Home Health 1843 West Broadway VancouverNaomi Goffman Community Therapists 401–8750 Selkirk Street VancouverAlaina Guymer Burnaby Hospital
- Workplace Health3935 Kincaid Street Burnaby
Tamara Guzman Recabarren
Orion Health 210–555 Sixth Street New Westminster
Dr. Denise Hall Dragonfly Psychology Services
#215 1118 Homer Street Vancouver
Kris Hallenburg Back in Motion 1040 Parker Street #1 White RockMary Hamilton Able OT Consulting 185 Cambridge Road TrailSven Hartman VISTA Disability
Management#223–119 W. Pender Street
Vancouver
Paul Hatch 15081 86A Avenue SurreyKen Hemphill Back in Motion Rehab 300–5450 152 Street SurreyRobin Henery ATF Canada 150–625 Agnes Street New
WestminsterCarly Higgon
(Duggleby)Back in Motion Functional Assessments Inc.
6651 Elmbridge Way Richmond
Health Care Professional Conference 5
First name Last name Organization Address CityBrenda Hogan Back in Motion 140–6651 Elmbridge
WayRichmond
Tracie Holland BIM 206–5500 152nd Street SurreySilvia Hua Drake Medox Health
Solutions13817 103rd Avenue Surrey
Cyrus Huang LifeMark Centric Health
230–181 Keefer Place Vancouver
Natalie Hull Progressive Rehab — OrionHealth
1518 33rd Ave East Vancouver
Janet Hunt Progressive Rehab OrionHealth
401–3999 Henning Drive Burnaby
Jeffrey Hwang Century Chiropractic Clinic
204–2786 W. 16th Avenue
Vancouver
Iveta Janickova Treloar Physiotherapy Clinic
595 West 8th Avenue Vancouver
Barry Judge Back in Motion Physio and Active Rehab
#201–3975 North Road Burnaby
Alan Kaplan Orion Health 16555 Fraser Highway SurreyChristy Keillor Kinsmen Lodge 9650 137A Street SurreyMonica Khosla Great West Life 900–1075 West Georgia VancouverDarren Kimura OT Consulting/
Treatment Services Ltd.210–3438 Lougheed Highway
Vancouver
Sarina Kot Dr. Sarina Kot Reg Psych Inc.
262–2025 W. 42nd Ave Vancouver
Cary Kruger Kruger Neuro-Rehabilitation Inc.
204–2365 Gordon Drive Kelowna
Sannie Lau WorkSafeBC 6951 Westminster Highway
Richmond
Danuta Lipien Drake Medox Health Solutions
13817 103rd Avenue Surrey
Jennifer Llewellyn MPA Society 122 Powell Street VancouverJohn Loh Dr. John Loh
Chiropractic Corp.201–3377 Coast Meridian Road
Port Coquitlam
Rob Low Drake Medox Health Solutions
13817 103rd Avenue Surrey

Health Care Professional Conference6
First name Last name Organization Address CityBill Lyons LifeMark
Physiotherapy — Centric Health
209–12080 Nordel Way Surrey
Margaret Mallam RCMP Health Services 14200 Green Timbers Way
Surrey
Yenna Mansfield Community Therapists Unit 201–3997 Henning Drive
Burnaby
David Maxwell CBI Health VictoriaKerry Maxwell Burrard Physiotherapy #702–1190 Hornby Street VancouverMary Anne McLennan OrionHealth 201–3150 East 54th
AvenueVancouver
Marisol McRae Centre for Compassionate Change Inc
10458 Glenmoor Place Surrey
Larissa Mead-Wescott
North Shore Neurpsychology
#212–545 Clyde Avenue West Vancouver
Damaris Medina Community Therapists 14881 103A Avenue SurreyAnita Melin Open Door
Communications415 Baker Street, Suite B
Nelson
Hafeez Mian Psychotherapy & Counseling Clinic
17246 Fourth Avenue Surrey
Dr. Lawrence Miller Dr. Lawrence Miller, Professional Psychology Corporation
405–3551 Foster Avenue Vancouver
Anthony Milonas CBI HealthDev Mitra Drake Medox Health
Solutions164 Oriole Road Kamloops
Derek Monkman Fraser Valley Physiotherapist & Rehabilitation Centre
#2, 9145 Corbould Street Chilliwack
David Morosan Mountain Counselling & Mediation
34334 Forrest Terrace Abbotsford
Vanja Mudrinic LifeMark Health 230–181 Keefer Place VancouverMary Jo Mulgrew Focus Rehabilitation
and Consulting Inc.#305–1890 Cooper Road Kelowna
Michelle Noel Progressive Rehab — OrionHealth
#401–3999 Henning Drive
Burnaby
Colleen North Progressive Rehab, OrionHealth
3999 Henning Drive Burnaby
Health Care Professional Conference 7
First name Last name Organization Address CityKhalil Nourani Direct Solutions
Counselling301–545 Clyde Avenue West Vancouver
Sarah Nowosad Bayshore Home Health 1845 West Broadway VancouverTess O'Brien Dr. Tess O'Brien 3665 Kingsway, Suite
300Vancouver
Sacha Oddstad CP Rail 1670 Lougheed Hwy Port CoquitlamHugh O'Loughlin OT Consulting/
Treatment Services Ltd.210–3438 Lougheed Highway
Vancouver
Chiara Papile OrionHealth 201–3150 E. 54th Ave VancouverPatti Parker RCMP 14200 Green Timbers
WaySurrey
Jaclyn Penner OT Works! 1517 London St New Westminster
Tania Percy Progressive Rehab OrionHealth
#401–3999 Henning Drive
Burnaby
Julie Plummer WorkSafeBC PO Box 5350 Stn Terminal
Vancouver
Audrey Pons WorkSafeBC POBox 4700 Stn Terminal
Vancouver
Paula Portnoi 181 Keefer Place, Suite 228
Vancouver
Steve Powell ATF Canada 625 Agnes Street, Suite 150
New Westminster
Lorne Prupas 501–3292 Production Way
Burnaby
John Pullyblank The M. Jackson Group Inc.
210 Sixth Street New Westminster
Colleen Quee-Newell Vocational Pacific Ltd. 309–2901 West Broadway
Vancouver
Abdollah Rezazadeh AR OT Rehab P.O. Box 18119 Port MoodyDebra Richards Richards and Company 98 Easthom Road GabriolaDustin Robin Victoria Sports
Physiotherapy108–1669 victoria st Prince George
Joan Russell LifeMark Health Kelowna
104–1634 Harvey Avenue Kelowna
Pamela Russell OT Works! 1517 London Street New Westminster
Nirmal Sahota OrionHealth 15855 89A Avenue Surrey
Health Care Professional Conference8
First name Last name Organization Address CityDebbie Samsom Back in Motion Rehab
Inc.#110–6651 Elmbridge Way
Richmond
Patricia Samuhel Treloar Physiotherapy Clinic
595 West 8th Avenue Vancouver
Keith Saunders Dr. Keith Saunders #2300–2850 Shaughnessy Street
Port Coquitlam
Andrea Score Fraser Health 6052 165A Street SurreyJohn Sherwood Classic LifeCare /
Connect1550–1200 W 73rd Avenue
Vancouver
Cathy Skain PT Health Squamish Physio and Wellness Centre
38247 Cleveland Avenue, PO Box 1970
Squamish
Angela Spooner Lifemark Health #230–181 Keefer Place VancouverWalter Stasiuk BC Ferries 500–1400 Blanshard
StreetVictoria
Andrew Sumner Great-West Life #900–1075 West Georgia Street
Vancouver
Nicole Swisher Fraser Health 709–260 Sherbrooke Street
New Westminster
Diane Tam WorkSafeBC 6951 Westminster Highway
Richmond
Gillian Tews CBI Health Group — Surrey
202–7350 King George Boulevard
Surrey
Niraj Thakore WorkSafeBC 6951 Westminister Highway
Richmond
Cindy Thompson Maples Counselling Inc.
147 Butler Avenue Parksville
Aurora To RCMP #1208–14200 Green Timbers Way
Surrey
Rebecca Tunnacliffe PABC 402–1755 West Broadway
Vancouver
Etienne Venter HeadWise Rehabilitation
Suite 210–7525 King George Blvd
Surrey
Hendre Viljoen HeadWise Rehabilitation
4555 Mountain Highway North Vancouver
Jaye Wald Back in Motion Rehab 201–3975 North Road BurnabyPatrice Weibelzahl Northwest Change
Agents24168 63 Avenue Langley
Health Care Professional Conference 9
First name Last name Organization Address CityWarren Weir LifeMark Health 230–181 Keefer Place VancouverTheresa Weltzin OrionHealth #120 16555 Fraser
HighwaySurrey
Charlene Wharton OT Consulting/Treatment Services Ltd.
210–3438 Lougheed Highway
Vancouver
Joesphine Wong VCH-Richmond Hospital
7000 Westminster Highway
Richmond
Yuk Shuen Wong Dr. Wong & Associates Professional Psychology Corporation
337–2184 West Broadway
Vancouver
Matthew Wright-Smith Healthx Physical Therapy
1906 West 43rd Avenue Vancouver
Tanya Yardley CBI HealthSharon Yen Golden Ears
Physiotherapy202-20395 Lougheed Highway
Maple Ridge

Health Care Professional Conference10
10th Annual Health Care Professional Conference Agenda — September 12
Time Topic Presenter(s)7:45–8:30 am Registration and breakfast
8:30–8:35 am Introduction by emcee Dr. Brian Worth Psychologist, Health Care Services, WorkSafeBC
8:35–8:45 am Opening remarks Andrew Montgomerie Director of Financial Services and Health Care Programs, WorkSafeBC
8:45–9:45 am Demographic Effects: What demographic changes on a global and local basis mean for healthcare professionals
Terry Bogyo Independent researcher, speaker, and consultant
9:45–10:45 am Taking Action to Improve Psychological Health and Safety in the Workplace
Dr. Merv Gilbert Adjunct Professor, Centre for Applied Research in Mental Health and Addiction, Faculty of Health Sciences, Simon Fraser University
10:45–11:15 am Refreshment break/visit exhibitor booths
11:15 am–12 pm Breakout Session 1a
What About the Neck?: Identification and management of potential cervical contribution to concussion symptoms
Carol Kennedy Physiotherapist
Breakout Session 1b
Psychologically and Occupationally Responsive Treatment (PORT)
Dr. Merv Gilbert Adjunct Professor, Centre for Applied Research in Mental Health and Addiction, Faculty of Health Sciences, Simon Fraser University
12–1 pm Lunch/visit exhibitor booths
Health Care Professional Conference 11
Time Topic Presenter(s)12:20–1 pm Physiotherapy Agreement Q&A
Panel Informal Session (Optional)Gabi Jacobson Program Manager, Health Care Services, WorkSafeBC
Karen Takai Quality Assurance Supervisor, Health Care Services, WorkSafeBC
Jamie MacGregor Physiotherapist and Certified Hand Therapist PABC/WorkSafeBC Liaison
1–1:15 pm Sponsor afternoon introduction and draw
1:15–2 pm Breakout Session 2a
Mobile Apps for Quantifying Recovery: Current state and emerging opportunities
Dr. Kendall Ho Professor in Emergency Medicine, University of British Columbia
Breakout Session 2b
Life of a Claim — How Law and Policy Affects the Decision- Making Process in the Mental Health Claims Unit
WorkSafeBC Claims Panel: Scott Brent and Mental Health Claims Unit team
2–3 pm The Do’s and Don’ts of Engaging a Family Physician in a Return-to-Work Plan
Dr. Gurdeep Parhar Executive Associate Dean, Clinical Affairs, Faculty of Medicine, University of British Columbia
3–3:30 pm Refreshment break/visit exhibitor booths
3:30–4 pm Empowering Workers to Empower Themselves
Jessica Vliegenthart Paralympic injured worker
4–4:15 pm Closing and prize draws by emcee Dr. Brian Worth Psychologist, Health Care Services, WorkSafeBC

Health Care Professional Conference12
Exhibitor Floor Plan
25
24
23
22
21
2019
18 13
1417
16 15
Coffee/tea station
Coffee/tea station
8 7
69
10 5
4
1 2 3
1112
Booth Company
18 Clinicmaster
20 Edgewood
21, 22, and 23
WorkSafeBC
24 Quart Healthcare West
25Essential Medical Products
Booth Company
1 Connect
2Columbia Speech and Language Services Inc.
3 OT Works!
4 Community Therapists
5Angel Accessibility Solutions Ltd.
6 Chairlines
7Canadian Magnetic Imaging Inc.
8Centric Health (LifeMark)
9 Bayshore Home Health
10Canada Diagnostic Centres
11LifeLabs Medical Laboratory Services
12 and 19
CBI Health Centres/ We Care Home Health
13 CAOT-BC
14Advanced Health Care Products
15Back in Motion Rehab Inc.
16BC Medequip Home Health Care Ltd.
17 OrionHealth Services
Health Care Professional Conference 13
Speakers Disclosure statements
All presenters participating in these programs are expected to disclose to the program audiences any real or apparent conflict of interest related to the content of their presentation.
Guest Speaker The following information discloses my relationship with WorkSafeBC (Workers’ Compensation Board), and/or other corporate sponsors that might relate in some way to the presentation of my subject at this conference
Terry Bogyo Nothing additional to biography
Dr. Merv Gilbert Nothing additional to biography
Dr. Kendall Ho In discussion with Telus re: possible study in the future.
Used Blipcare equipment in a research study and paid them for their equipment. They have no interest with research design. This is purely a purchase.
Carol Kennedy Nothing additional to biography
Andrew Montgomerie Nothing additional to biography
Dr. Gurdeep Parhar Nothing additional to biography
Jessica Vliegenthart Nothing additional to biography

Health Care Professional Conference14

Health Care Professional Conference 15
Terry Bogyo
Terry is an independent researcher, speaker, and consultant who focuses on workers’ compensation and occupational safety and health.
Over his 30 year career at WorkSafeBC, he held a variety of positions including: executive assistant to the Chairman of the Board, director of Policy and Research, Vocational Rehabilitation, and Community Relations. He is a student of workers’ compensation systems and is frequently engaged in comparative performance analysis of workers’ compensation systems around the globe.
Terry’s academic interests include advanced studies in Occupational and Environmental Health, Health Care and Epidemiology, and Philosophy. He’s a Registered Rehabilitation Professional (RRP) and a Canadian Certified Rehabilitation Counselor (CCRC). He’s co-chaired the Research and Standards Committee for the International Association of Industrial Accident Boards and Commissions (IAIABC) and worked closely with the Association of Workers’ Compensation Boards of Canada (AWCBC) on emerging issues.
Terry also technically reviews papers on workers’ compensation issues and teaches online courses. He’s an avid writer and speaker, and conducts workshops on issues facing workers’ compensation systems and on future risks facing workplaces and society at events around the world.
Plenary session: Demographic Effects: What demographic changes on a global and local basis mean for healthcare professionals
The world is experiencing dramatic shifts in its population characteristics that are fundamentally changing our economies, labour force, and communities as never before. These “demographic effects” have profound implications for our society, healthcare system, and families. This plenary presentation connects demographic change and the impacts already reverberating through our professions and communities.
Learning objectives:
• Understanding a range of demographic changes and techniques
• Interpret demographic data on healthcare professions
• Identify the personal implications of changes in longevity
• Use demographic data to inform personal and family decisions
• Gain new perspectives on the pressures driving healthcare policy and practice

Health Care Professional Conference16
Health Care Professional Conference Vancouver Hyatt Regency– September 12, 2014
Terrance J. BogyoIndependent Researcher | Speaker | Consultant
Introduction: Who is this presenter? Terrance (Terry) J. Bogyo (BSc, MBA, CCRC, RRP) I n d epen d en t Researc h er | Speaker | C o n su l tan t 1665 58 A Street Delta, BC V4L 1X5 e-mail: [email protected] Blog: www.WorkersCompPerspectives.wordpress.com Phone: (604) 943-3545 Skype: terry.bogyo
Outline Demographic Effects: What we mean by demographics How workforce and population demographics are changing What demographic change means to you and me, our
families, our communities– and healthcare professionals in particular
Health Care Professional Conference 17
Demographic Effects: What demographic changes on a global and local basis mean for
healthcare professionals Learning objectives: The world is experiencing dramatic shifts in its population
characteristics that are fundamentally changing our economies, labour force, and communities as never before. These “demographic effects” have profound implications for our society, healthcare system and families. This plenary presentation connects demographic change and the impacts already reverberating through our professions and communities. The Learning Objectives for this session include:
· Understanding a range of demographic changes and techniques · Interpret demographic data on healthcare professions · Identify the personal implications of changes in longevity · Use demographic data to inform personal and family decisions · Gain new perspectives on the pressures driving healthcare policy and practice.
Demographics dem·o·graph·ics (dĕm'ə-grăf'ĭks) noun
shortened term for ‘population characteristics’ including race, age, income, educational attainment, home ownership, employment status, location ...
Common “Demographic” terms WASP YUPPIE OINK(Y) DINK(Y) SNAG WOOF(P) PIPPIE
White, anglo-saxon, protestant Young, urban, professional One income, no kids (yet) Double income, no kids (yet) Sensitive, new-age guy Well off, older folk (person) Person inheriting parents property
Health Care Professional Conference18

Common “Demographic” terms WASP YUPPIE OINK(Y) DINK(Y) SNAG WOOF(P) PIPPIE
White, anglo-saxon, protestant Young, urban, professional One income, no kids (yet) Double income, no kids (yet) Sensitive, new-age guy Well off, older folk (person) Person inheriting parents property
Top 10 Countries by Population
8http://sasweb.ssd.census.gov/idb/ranks.htmlViewed August 31, 2014
0
200,000,000
400,000,000
600,000,000
800,000,000
1,000,000,000
1,200,000,000
1,400,000,000
1,600,000,000 201420242034
Top 10 Countries by Population
9http://sasweb.ssd.census.gov/idb/ranks.htmlViewed August 31, 2014
0
200,000,000
400,000,000
600,000,000
800,000,000
1,000,000,000
1,200,000,000
1,400,000,000
1,600,000,000 201420242034
Health Care Professional Conference 19
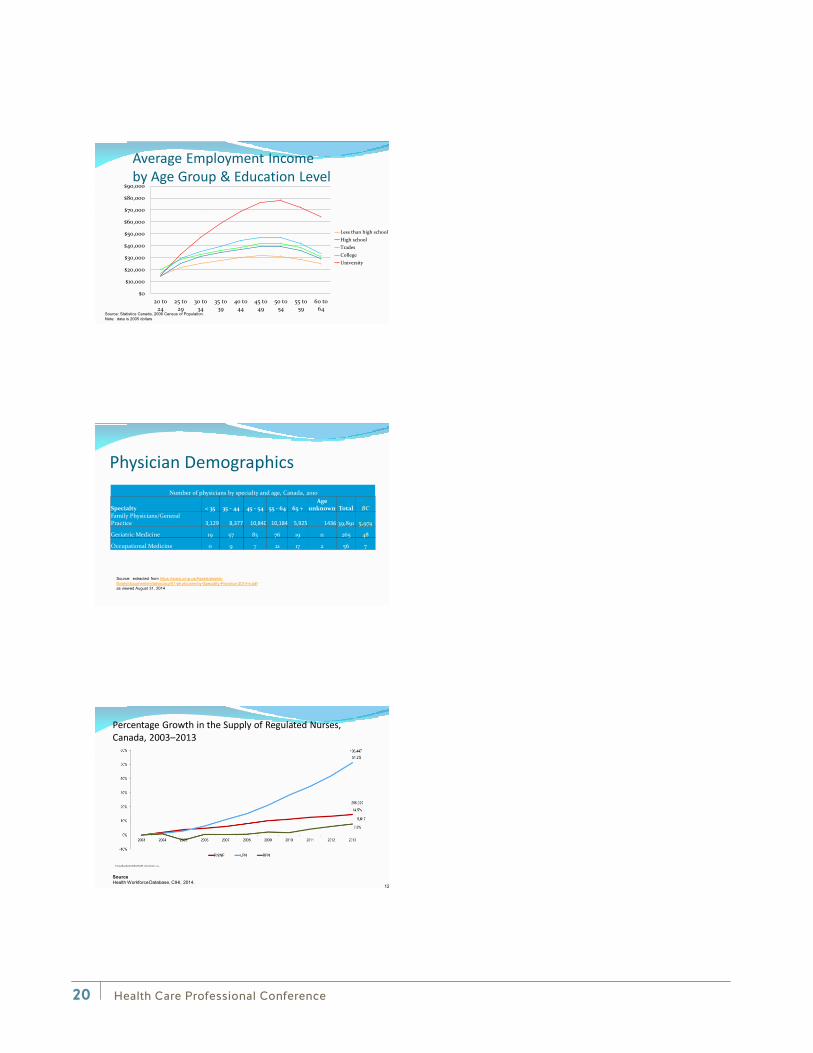
Average Employment Income by Age Group & Education Level
$0
$10,000
$20,000
$30,000
$40,000
$50,000
$60,000
$70,000
$80,000
$90,000
20 to24
25 to29
30 to34
35 to39
40 to44
45 to49
50 to54
55 to59
60 to64
Less than high schoolHigh schoolTradesCollegeUniversity
Source: Statistics Canada, 2006 Census of Population.Note: data is 2005 dollars
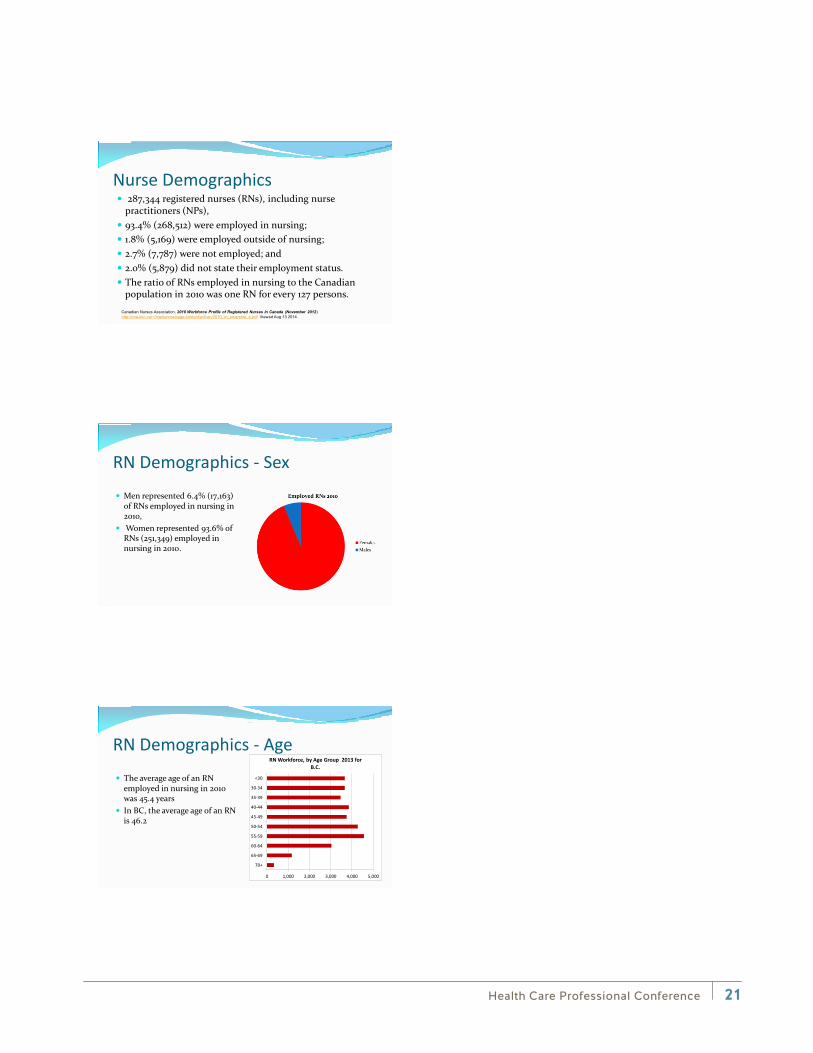
Physician Demographics Number of physicians by specialty and age, Canada, 2010
Specialty < 35 35 - 44 45 - 54 55 - 64 65 + Age
unknown Total BC Family Physicians/General Practice 3,129 8,377 10,840 10,184 5,925 1436 39,891 5,974
Geriatric Medicine 19 57 83 76 19 11 265 48
Occupational Medicine 0 9 7 21 17 2 56 7
Source: extracted from https://www.cma.ca/Assets/assets-library/document/en/advocacy/01-physicians-by-Specialty-Province-2014-e.pdf as viewed August 31, 2014
Percentage Growth in the Supply of Regulated Nurses, Canada, 2003–2013
12
SourceHealth Workforce Database, CIHI, 2014.
Health Care Professional Conference20
Nurse Demographics
Canadian Nurses Association, 2010 Workforce Profile of Registered Nurses in Canada (November 2012)http://cna-aiic.ca/~/media/cna/page-content/pdf-en/2010_rn_snapshot_e.pdf Viewed Aug 13 2014.
287,344 registered nurses (RNs), including nurse practitioners (NPs),
93.4% (268,512) were employed in nursing; 1.8% (5,169) were employed outside of nursing; 2.7% (7,787) were not employed; and 2.0% (5,879) did not state their employment status. The ratio of RNs employed in nursing to the Canadian
population in 2010 was one RN for every 127 persons.
RN Demographics - Sex Men represented 6.4% (17,163)
of RNs employed in nursing in 2010,
Women represented 93.6% of RNs (251,349) employed in nursing in 2010.
RN Demographics - Age The average age of an RN
employed in nursing in 2010 was 45.4 years
In BC, the average age of an RN is 46.2
0 1,000 2,000 3,000 4,000 5,000
70+
65-69
60-64
55-59
50-54
45-49
40-44
35-39
30-34
<30
RN Workforce, by Age Group 2013 for B.C.
Health Care Professional Conference 21
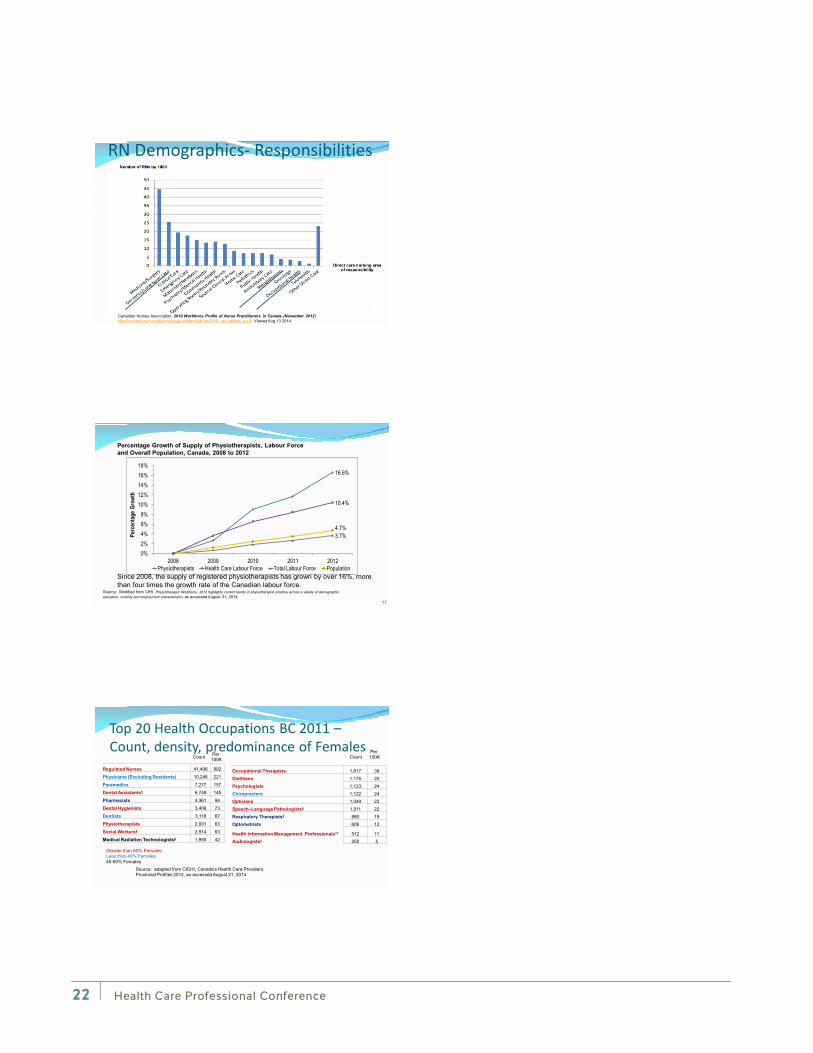
RN Demographics- Responsibilities
Canadian Nurses Association, 2010 Workforce Profile of Nurse Practitioners in Canada (November 2012)http://cna-aiic.ca/~/media/cna/page-content/pdf-en/2010_np_profiles_e.pdf Viewed Aug 13 2014.
16.6%
10.4%
3.7% 4.7%
0%2%4%6%8%
10%12%14%16%18%
2008 2009 2010 2011 2012
Perc
entag
e Gr
owth
Physiotherapists Health Care Labour Force Total Labour Force Population
17
Percentage Growth of Supply of Physiotherapists, Labour Force and Overall Population, Canada, 2008 to 2012
Since 2008, the supply of registered physiotherapists has grown by over 16%, more than four times the growth rate of the Canadian labour force.
Source: Modified from CIHI, Physiotherapist Workforce, 2012 highlights current trends in physiotherapist practice across a variety of demographic, education, mobility and employment characteristics as accessed August 31, 2014
Top 20 Health Occupations BC 2011 – Count, density, predominance of Females
Regulated Nurses 41,406 892
Physicians (Excluding Residents) 10,246 221
Paramedics 7,277 157
Dental Assistants§ 6,748 145
Pharmacists 4,361 94
Dental Hygienists 3,406 73
Dentists 3,118 67
Physiotherapists 2,931 63
Social Workers§ 2,914 63
Medical Radiation Technologists§ 1,955 42
Occupational Therapists 1,817 39Dietitians 1,175 25Psychologists 1,123 24Chiropractors 1,122 24Opticians 1,049 23Speech–Language Pathologists§ 1,011 22Respiratory Therapists§ 880 19Optometrists 606 13
Health Information Management Professionals** 512 11Audiologists§ 250 5
Source: adapted from CICHI, Canada's Health Care Providers: Provincial Profiles 2012, as accessed August 21, 2014
Count CountPer 100K
Per 100K
Greater than 60% FemalesLess than 40% Females40-60% Females
Health Care Professional Conference22
Let’s get personal On the top of the page write
The year you were born Your age on your birthday this year The age you expect to retire What do you think your life expectancy was at birth? If you were 65 today, how many more years do you think you might
live? Do you plan to work after you reach retirement age? If so, why?
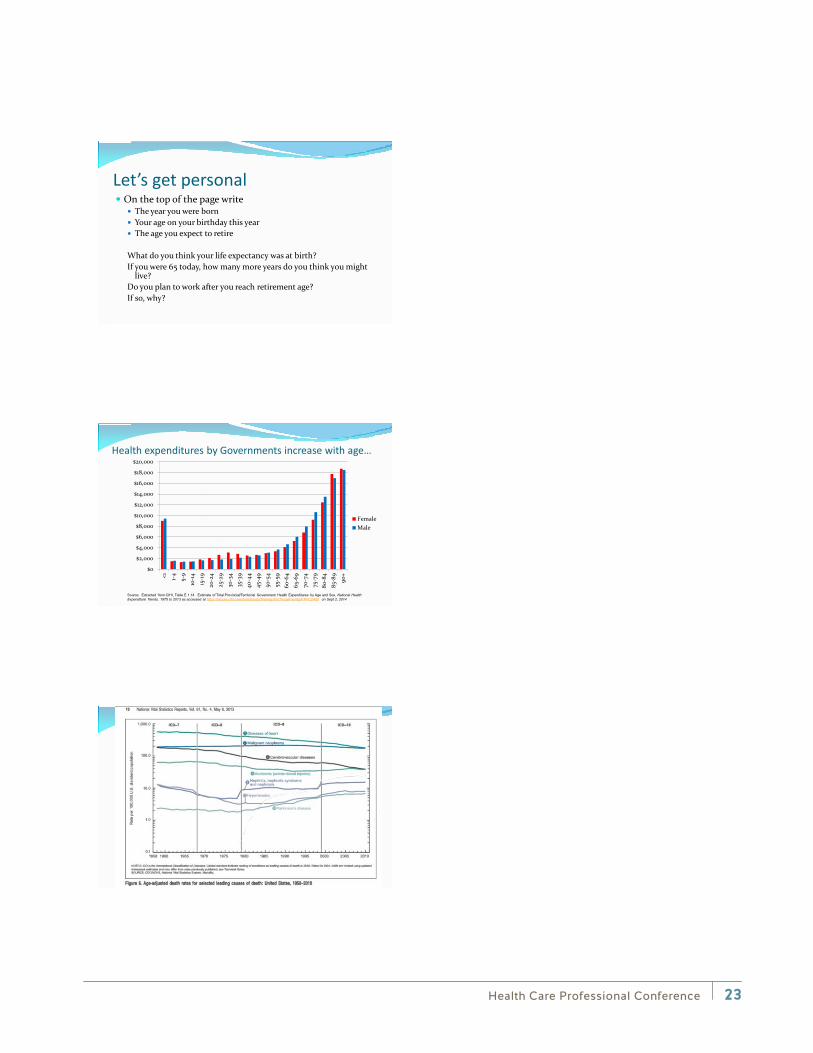
Health expenditures by Governments increase with age…
Source: Extracted from CIHI, Table E 1.14 Estimate of Total Provincial/Territorial Government Health Expenditures by Age and Sex, National Health Expenditure Trends, 1975 to 2013 as accessed at https://secure.cihi.ca/estore/productFamily.htm?locale=en&pf=PFC2400 on Sept 2, 2014
$0
$2,000
$4,000
$6,000
$8,000
$10,000
$12,000
$14,000
$16,000
$18,000
$20,000
<1 1-4
5-9
10-1
415
-19
20-2
425
-29
30-3
435
-39
40-4
445
-49
50-5
455
-59
60-6
465
-69
70-7
475
-79
80-8
485
-89
90+
FemaleMale
Health Care Professional Conference 23
New study ranks Alzheimer’s as third-leading cause of death, after heart disease and cancer Washington Post By Tara Bahrampour, Published:
March 5
Contribution of Alzheimer disease to mortality in the United States
Bryan D. James, PhD, Sue E. Leurgans, PhD, Liesi E. Hebert, ScD, Paul A. Scherr, PhD, ScD, Kristine Yaffe, MD and David A. Bennett, MD
Published online before print March 5, 2014, doi: 10.1212/WNL.0000000000000240
Neurology 10.1212/WNL.0000000000000240 Alzheimers
New study ranks Alzheimer’s as third-leading cause of death, after heart disease and cancer Washington Post By Tara Bahrampour, Published:
March 5, 2014
Contribution of Alzheimer disease to mortality in the United States
Bryan D. James, PhD, Sue E. Leurgans, PhD, Liesi E. Hebert, ScD, Paul A. Scherr, PhD, ScD, Kristine Yaffe, MD and David A. Bennett, MD
Published online before print March 5, 2014, doi: 10.1212/WNL.0000000000000240
Neurology 10.1212/WNL.0000000000000240
Alzheimer's
Alzheimer's
Health Care Professional Conference24
Headlines Health care worker shortage looms as staff retire Nova Scotia's health Minister, Leo Glavine, warned in briefing notes The Canadian Press Posted: Jan 02, 2014 7:25 AM AT Last Updated: Jan 02, 2014 10:51 AM AT
Nova Scotia's new health minister is being warned the province could face "alarming" shortages across a range of professions in the health-care system as workers approach retirement, which includes a shortage of 800 nurses within five years.
"Professions requiring close monitoring include physicians, registered nurses, licensed practical nurses, continuing care assistants and lab and diagnostic imaging staff to name a few."
Headlines Global health workforce shortage to reach 12.9 million in coming decades WHO News Release NOVEMBER 2013 | RECIFE, BRAZIL -
The world will be short of 12.9 million health-care workers by 2035; today, that figure stands at 7.2 million. A WHO report released today warns that the findings – if not addressed now – will have serious implications for the health of billions of people across all regions of the world.
Demand elsewhere GETHealth Summit- Leveraging ICTs to Close the Health Workforce Gap 14 August 14
The world is currently facing a global health worker shortage of almost 4.3 million doctors, midwives, nurses, and other healthcare professionals. There are fifty-seven countries worldwide which are suffering from a severe shortage of health workers; of these, thirty-six are in Africa.
Health Care Professional Conference 25

High Demand Occupations Healthcare occupations top the list in Canada Inspectors in public and
environmental health and occupational health and safety
Nursing co-coordinators and supervisors
Registered nurses and registered psychiatric nurses
Specialty physicians General practitioners and family
physicians Dietitians and nutritionists Audiologists and speech-language
pathologists
Physiotherapists Occupational therapists Respiratory therapists, clinical
perfusionists and cardiopulmonary technologists
Medical radiation technologists Medical sonographers Licensed practical nurses Paramedical occupations Psychologists
Headlines Crisis and Intervention Lessons From the Financial Meltdown and Recession Conference Board of Canada January 2011
Lesson 1: Sound Fiscal Policy Is Key to Keeping the Economy Afloat in Hard Times
Lesson 6: “Too Big to Fail” Means Too Big
Lesson 2: Recession Only Delayed the Inevitable Workplace Shortages
Lesson 7: Integrative Trade Can Pull Us Down and Up
Lesson 3: The Financial Sector is Unique and Needs New Standards
Lesson 8: Local Governments Can’t Provide the Solution
Lesson 4: Public Sector Financial Institutions Prove Their Worth
Lesson 9: Psychology Matters to How a Recession Unfolds
Lesson 5: Global Coordination Was Critical to a Speedy Recovery
Lesson 10: The Fiscal Bills Will Eventually Have to Be Paid
Unemployment Rates rose but remained low for high-demand occupations (percent)
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
Management Contractors & supervisors in trade &transport
Natural applied sciences & relatedoccupations
Health, nurse supervisor, registerednurses
Art, culture, recreation & sport
2006200720082009
Source: Statistic Canada as quoted in Crisis and Intervention: Lessons from the Financial Meltdown and Recession,Conference Board of Canada 2010, page 52 Chart 7
Health Care Professional Conference26
Headlines… Starting in April 2023, the age of eligibility for the Old Age Security
(OAS) pension and the Guaranteed Income Supplement (GIS) will gradually increase from 65 to 67. This change will affect people born in 1958 and later.
Canada Pension Plan changes provide incentives to work longer:
Age 60 Age 65 Age 70 Prior to 2011 $900-(30% of 900) = $630 $900 $900+(30% of 900) = $1170 $900-(36% of 900) = $576 $900 $900+(42% of 900) = $1278
(by 2016) (by 2013)
Headlines… BC announces end to Mandatory Retirement (Feb 13, 2007) Ontario moves to end mandatory retirement
Mandatory retirement already eliminated in US, Australia, New Zealand
Tony Blair proposes raising the retirement age to 70 for high-income earners
“White-collar professionals [should] retire later then lower-paid workers because they have more cash and a longer life expectancy.” Adair Turner, head of the UK Pensions Commission
German experts fuel debate about retirement at 70 By VERENA SCHMITT-ROSCHMANN (AP) August 11, 2010 BERLIN
Germans are famous for being hard workers — but retirement at 70? That's the prescription of two think tanks, which say years more toil are inevitable due to stubbornly low birthrates and the ballooning costs of the cradle-to-grave welfare system in a country that already has decided to bump up the retirement age from 65 to 67.
32
“Sweden considers raising retirement age to 75” Published 27 February 2013
http://www.euractiv.com/health/sweden-prime-minister-considers-news-518068
Swedes should be prepared to work until they are 75 and to change careers in the middle of their work life if they are to keep the welfare standards they expect, Swedish Prime Minister Fredrik Reinfeldt said.
Reinfeldt, who leads a centre-right government, also said half of today's children in Sweden can expect to become 100 years old and there has to be a change in the way the Swedes view their work life.
33
Health Care Professional Conference 27
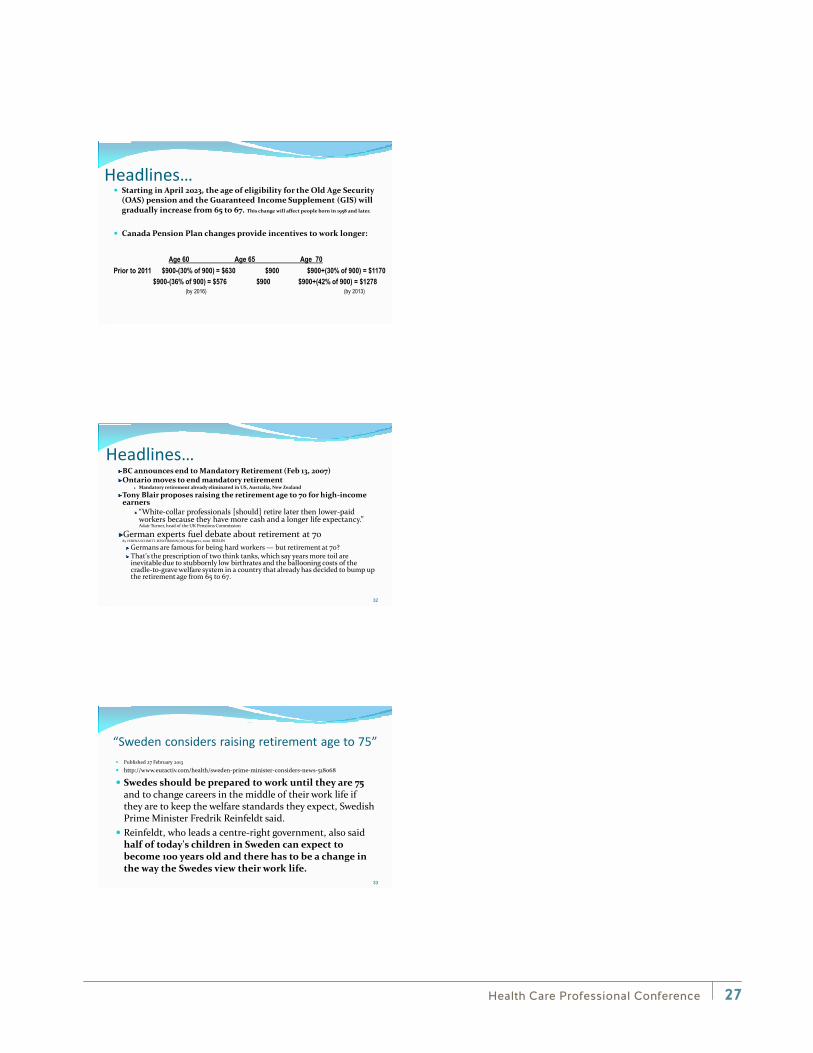
So, What’s Happening With Life Expectancy?
0 5 10 15 20 25 30 35 40 45 50
Prehistoric timesAncient Greece
Medieval EnglandRenaissance England
Canada 18311841185118611871188118911901
Life Expectancy at Birth
Source: attributed to The Urban Futures Institute as published in “Planning for Retirement, Canadian Bankers Association.
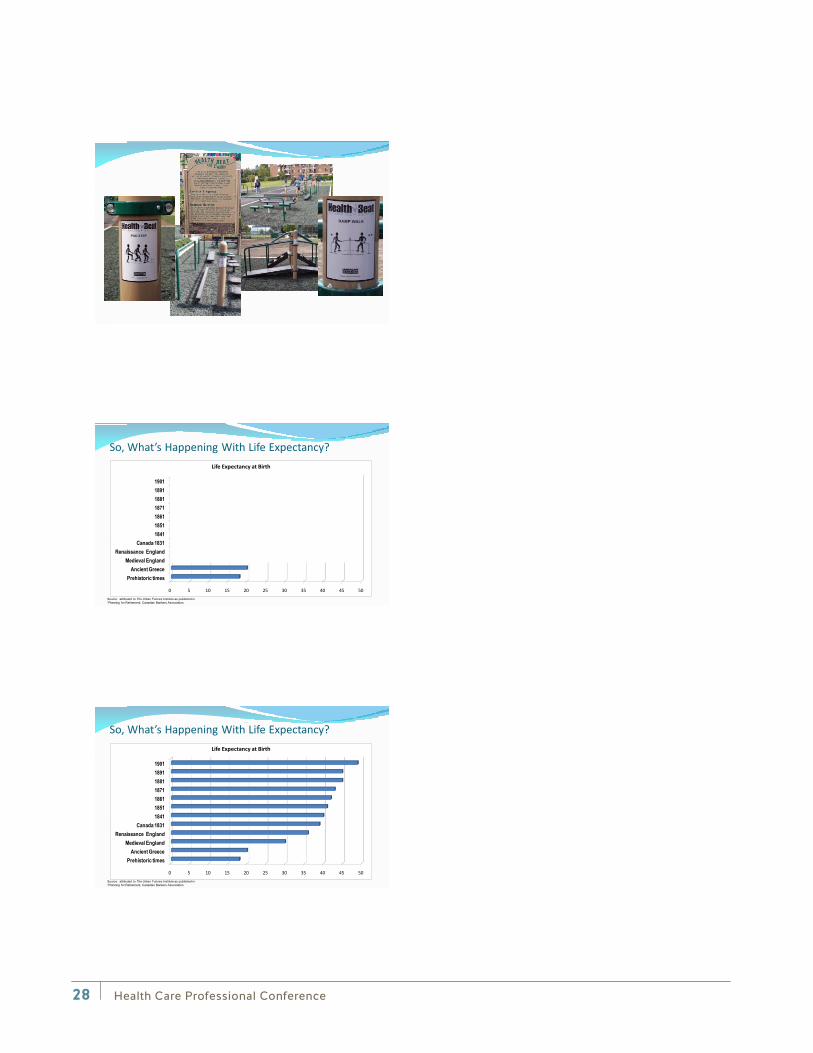
So, What’s Happening With Life Expectancy?
0 5 10 15 20 25 30 35 40 45 50
Prehistoric timesAncient Greece
Medieval EnglandRenaissance England
Canada 18311841185118611871188118911901
Life Expectancy at Birth
Source: attributed to The Urban Futures Institute as published in “Planning for Retirement, Canadian Bankers Association.
Health Care Professional Conference28
In 1900… Life expectancy at birth was:
In the US As recently as 1900, 48.3 years for men and 51.1 years for women
In Austria, Czechoslovakia, Greece, Hungary and Spain less than 40 years
Belgium, France, Great Britain, Italy, Japan Under 50
Australia 53.2 years at birth and a female would have 56.8 years.
-Source: Bruce Bartlett, “ Setting a realistic retirement age”,
Washington Times, May 25, 2005
And Today… If you retire at age 55 having worked for 30 years…
As a female, you will live nearly as many years longer as you worked.
If you are married at age 60… There is a 50% probability that at least one of you will be
alive at age 90 At age 65, having 35 years of work, your savings, SS
(CP/OAS), and pension will have to support yourself for another 20 years
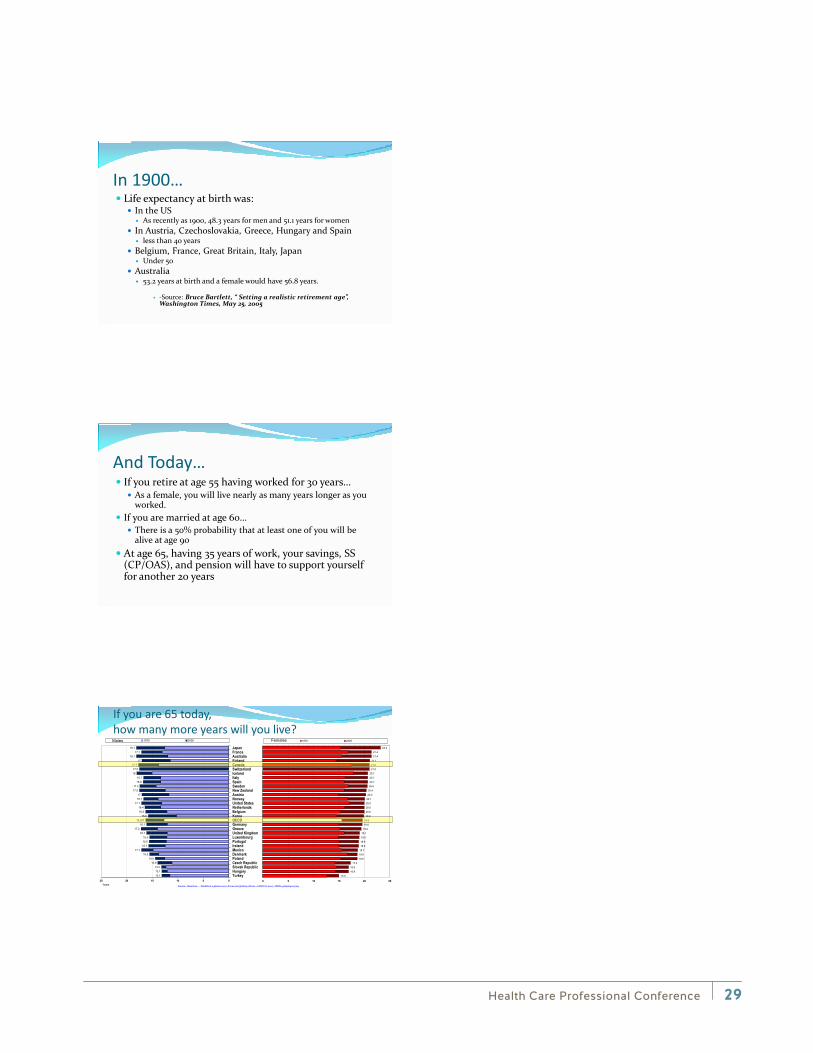
If you are 65 today, how many more years will you live?
15.0
16.9
16.917.3
18.6
18.618.7
18.9
18.9
19.0
19.1
19.419.6
19.6
19.9
20.020.0
20.0
20.120.3
20.4
20.620.7
20.7
20.721.0
21.0
21.1
21.4
21.4
23.2
0 5 10 15 20 25
1970 2005
13.113.113.2
13.914.4
15.517.1
15.715.615.5
16.117.2
16.116.257
15.816.316.4
17.116.717
17.517.4
16.816.7
1817.5
17.717
18.117.1
18.1
0510152025
TurkeyHungarySlovak RepublicCzech RepublicPolandDenmarkMexicoIrelandPortugalLuxembourgUnited KingdomGreeceGermanyOECDKoreaBelgiumNetherlandsUnited StatesNorwayAustriaNew ZealandSwedenSpainItalyIcelandSwitzerlandCanadaFinlandAustraliaFranceJapan
Years
1970 2005Males Females
Source: Based on Health at a glance 2007: Focus on Quality of Care - OECD © 2007 - ISBN 9789264027329
Health Care Professional Conference 29
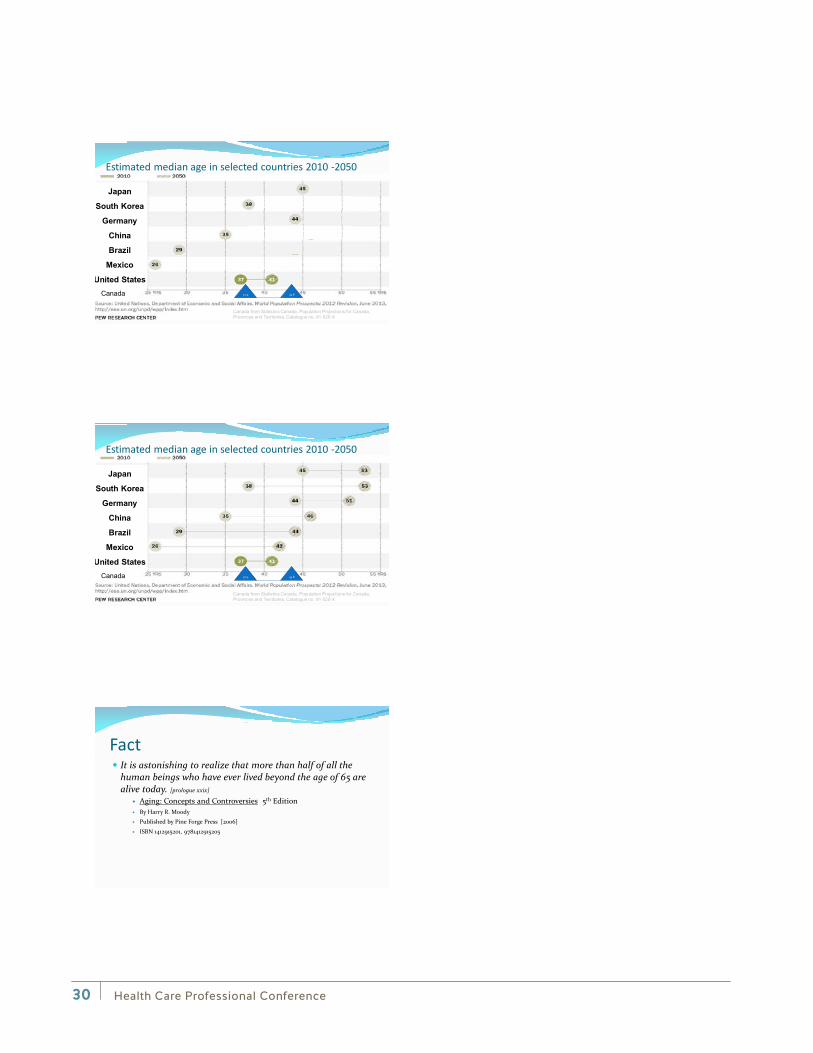
Estimated median age in selected countries 2010 -2050
Japan
South Korea
Germany
China
Brazil
Mexico
United States37.9 43.8 Canada
Canada from Statistics Canada, Population Projections for Canada, Provinces and Territories, Catalogue no. 91-520-X
Estimated median age in selected countries 2010 -2050
Japan
South Korea
Germany
China
Brazil
Mexico
United States37.9 43.8 Canada
Canada from Statistics Canada, Population Projections for Canada, Provinces and Territories, Catalogue no. 91-520-X
Fact It is astonishing to realize that more than half of all the
human beings who have ever lived beyond the age of 65 are alive today. [prologue xxix]
Aging: Concepts and Controversies 5th Edition By Harry R. Moody
Published by Pine Forge Press [2006]
ISBN 1412915201, 9781412915205
Health Care Professional Conference30
The Truth — An Inconvenient Inevitability The developed world – not just BC or Canada—is facing
an “Age Tsunami” a “Demographic Discontinuity” A “Population Predicament”
Chose your catch phrase… the truth is the same: A million people worldwide turn 60 every month over the next 25 years, around 70 million people will retire
in developed countries… …and will be replaced by just five million
Your “Demographic” baby boomer - People born between (and including)
1946 and 1964. generation X - a.k.a. GenX (pronounced: jen-X) 1963
and 1978 (or 1961 to 1981). generation Y - a.k.a. Gen M -or- millennials -or-
digital natives -or- echo boomers -or- millennial students -or- 21st century learners -or- Net Generation 1980 and 1995.
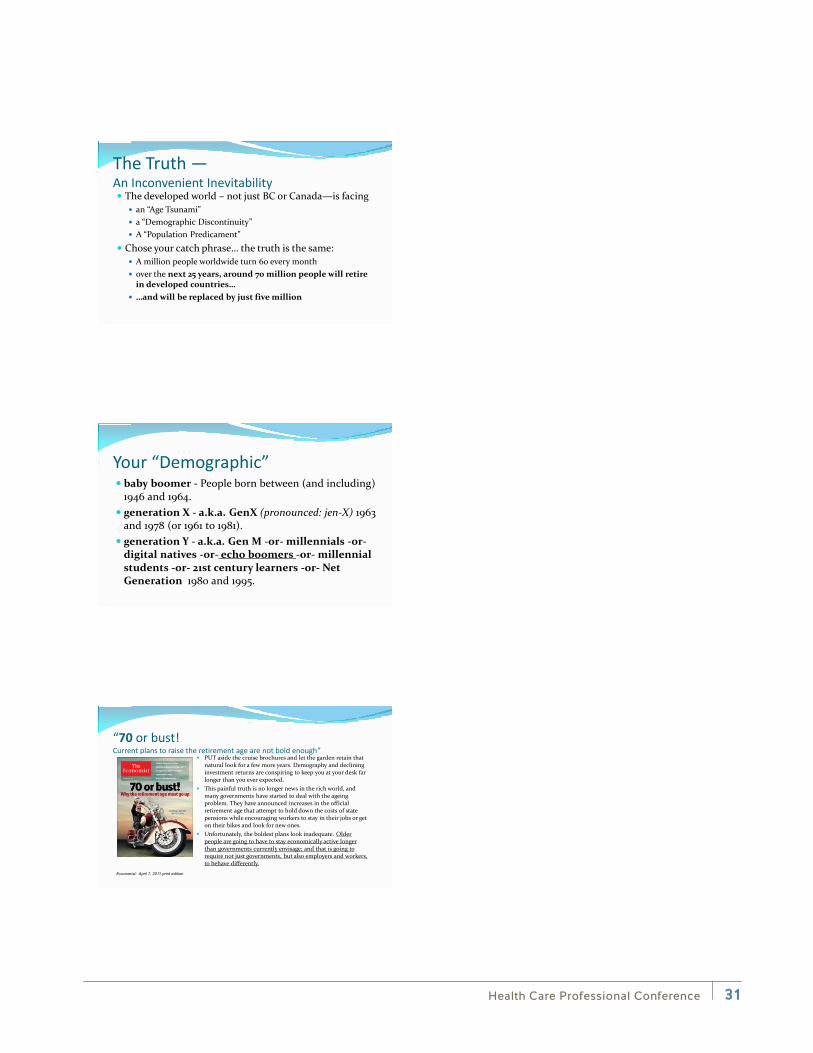
“70 or bust! Current plans to raise the retirement age are not bold enough”
PUT aside the cruise brochures and let the garden retain that natural look for a few more years. Demography and declining investment returns are conspiring to keep you at your desk far longer than you ever expected.
This painful truth is no longer news in the rich world, and many governments have started to deal with the ageing problem. They have announced increases in the official retirement age that attempt to hold down the costs of state pensions while encouraging workers to stay in their jobs or get on their bikes and look for new ones.
Unfortunately, the boldest plans look inadequate. Older people are going to have to stay economically active longer than governments currently envisage; and that is going to require not just governments, but also employers and workers, to behave differently.
Economist: April 7, 2011 print edition
Health Care Professional Conference 31
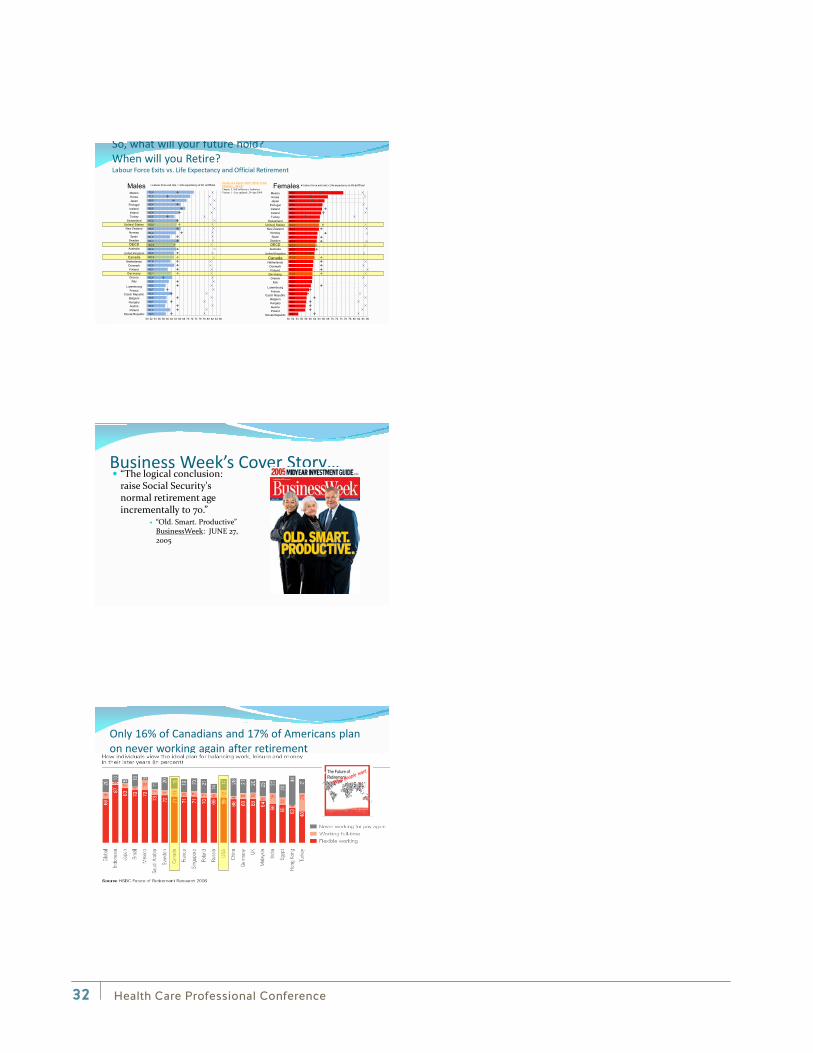
So, what will your future hold? When will you Retire? Labour Force Exits vs. Life Expectancy and Official Retirement
75.067.966.565.565.364.964.364.163.963.963.263.162.962.362.261.961.961.361.361.061.060.960.860.359.558.558.358.257.957.754.5
50 52 54 56 58 60 62 64 66 68 70 72 74 76 78 80 82 84 86
Labour force exit rate Life expectancy at 65 Official
73.071.269.566.668.965.663.565.264.666.564.261.465.763.564.463.263.361.663.560.262.162.460.859.258.762.259.659.758.961.459.3
50 52 54 56 58 60 62 64 66 68 70 72 74 76 78 80 82 84 86
Labour force exit rate Life expectancy at 65 Official
MexicoKoreaJapan
PortugalIcelandIrelandTurkey
SwitzerlandUnited StatesNew Zealand
NorwaySpain
SwedenOECDAustralia
United KingdomCanada
NetherlandsDenmarkFinland
GermanyGreece
Italy
LuxembourgFrance
Czech RepublicBelgiumHungaryAustriaPoland
Slovak Republic
MexicoKoreaJapan
PortugalIcelandIrelandTurkey
SwitzerlandUnited StatesNew Zealand
NorwaySpain
SwedenOECDAustralia
United Kingdom
CanadaNetherlands
DenmarkFinland
GermanyGreece
Italy
LuxembourgFrance
Czech RepublicBelgiumHungaryAustriaPoland
Slovak Republic
Society at a Glance 2009: OECD Social Indicators - OECDChapter 5. Self-sufficiency Indicators.Version 1 - Last updated: 29-Apr-2009
Males Females
Business Week’s Cover Story… “The logical conclusion:
raise Social Security's normal retirement age incrementally to 70.”
“Old. Smart. Productive” BusinessWeek: JUNE 27, 2005
Only 16% of Canadians and 17% of Americans plan on never working again after retirement
The Future of Retirement
Health Care Professional Conference32

Why will you work?
•Money (30% US 24% CDN)
•Mental Stimulation (15% US 18% CDN)
•Keep Physically active (22%US 21% CDN)
•Connect with others (7%US 11% CDN)
•Have something meaningful / valuable to with your time (21% US 23% CDN)
How individuals think governments should finance ageing populations (in percent)
14%
34%
17%
10%
22%
14%
34%
14%
6%
28%
0%
5%
10%
15%
20%
25%
30%
35%Increase Taxes
Enforced Additional PrivateSavings
Not Sure
Reduce Pensions
Increase Retirement Age
Source: HSBC Future of Retirement Research 2006US Canada
Gordon Waddell and A Kim Burton. Published by The Stationery Office, 2006.
ISBN 0-11-703694-3.
From the book by Gordon Waddell, A Kim Burton
Health Care Professional Conference 33
M Frese & G Mohr 1987, “Prolonged Unemployment And Depression In Older Workers: A Longitudinal Study Of Intervening Variables.” Soc Sci Med 25: 173-178
Re-employment in older workers can improve physical functioning and mental health.
Haynes SG, McMichael AJ, Tyroler HA. 1978. “Survival After Early And Normal Retirement.” Journal of Gerontology 33: 269-278.
Mortality after early retirement is higher than would be
expected in a corresponding working group: the only significant predictor is pre-retirement health status (i.e. a health selection effect). Taking all the data, no excess mortality was observed after normal retirement.
Morris JK, Cook DG, Shaper AG. 1992. “Non-employment And Changes In Smoking, Drinking, And Body-weight.” BMJ304: 536-541
Men who remained continuously employed had the lowest mortality, even after adjusting for socio-economic variables, manual/non-manual work and health-related behaviour. Even men who retired for reasons other than illness and who appeared to be relatively advantaged and healthy had a significantly increased risk (RR 1.87). The effect was non-specific: the increased risk of mortality from cancer was similar to that from cardiovascular disease.
Continue…
Health Care Professional Conference34
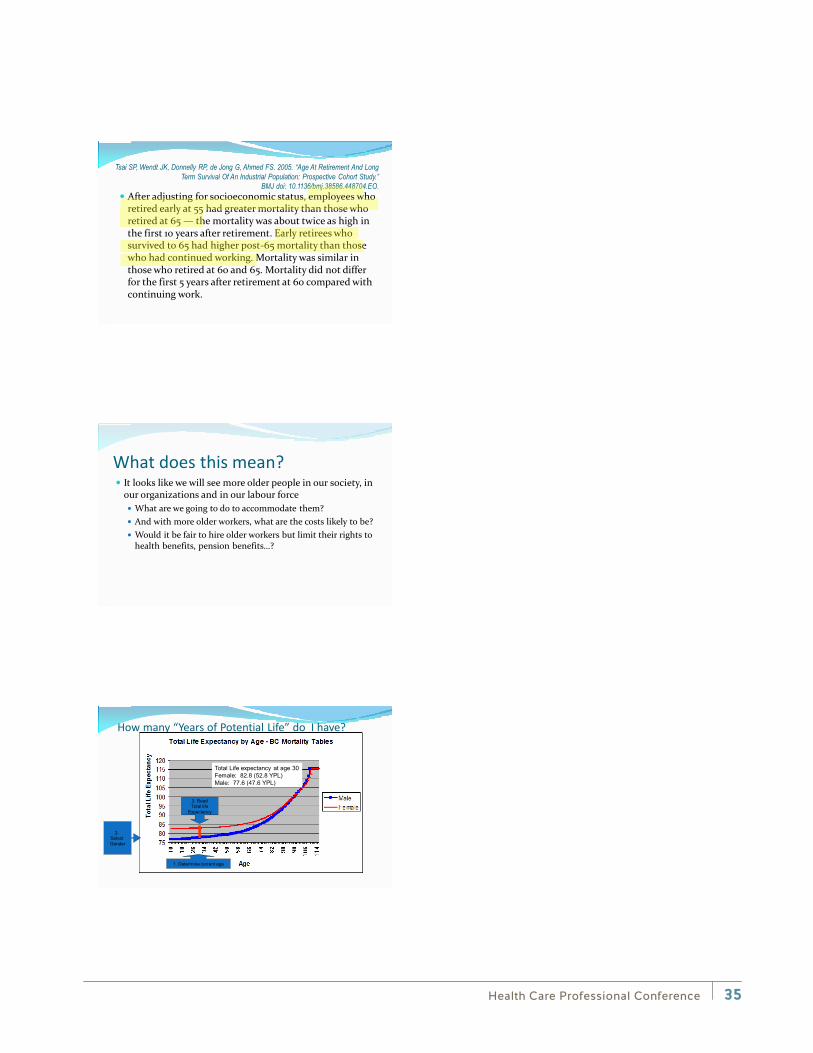
Tsai SP, Wendt JK, Donnelly RP, de Jong G, Ahmed FS. 2005. “Age At Retirement And Long Term Survival Of An Industrial Population: Prospective Cohort Study.”
BMJ doi: 10.1136/bmj.38586.448704.EO. After adjusting for socioeconomic status, employees who
retired early at 55 had greater mortality than those who retired at 65 — the mortality was about twice as high in the first 10 years after retirement. Early retirees who survived to 65 had higher post-65 mortality than those who had continued working. Mortality was similar in those who retired at 60 and 65. Mortality did not differ for the first 5 years after retirement at 60 compared with continuing work.
What does this mean? It looks like we will see more older people in our society, in
our organizations and in our labour force What are we going to do to accommodate them? And with more older workers, what are the costs likely to be? Would it be fair to hire older workers but limit their rights to
health benefits, pension benefits…?
How many “Years of Potential Life” do I have?
1. Determine current age
2.Select Gender
3. ReadTotal life
Expectancy
Total Life expectancy at age 30Female: 82.8 (52.8 YPL)Male: 77.6 (47.6 YPL)
Health Care Professional Conference 35

How long was my life expectancy when I was born?
Sources: Adapted from BC Stats, Ministry of Technology, Innovation and Citizens' Services 1921-1946:Longevity and Historical Life Tables, Dhruva Nagnur, Statistics Canada1950-2013: BC Stats, Ministry of Technology, Innovation and Citizens' Serviceshttp://www.bcstats.gov.bc.ca/StatisticsBySubject/Demography/VitalStatistics.aspxas accessed Set 2, 2014
50
55
60
65
70
75
80
85
90
1921
1936
1950
1953
1956
1959
1962
1965
1968 1971
1974
1977
1980
1983
1986
1989
1992
1995
1998
2001
2004
2007
2010
2013
Male
Female
Note: Population data after 1970 adjusted for non-permanent residents and undercount.Figures prepared through the use of single year of age life table.using deaths provided by Vital Statistics, Ministry of Health, and theaverage of consecutive years of population provided by Statistics Canada.Deaths are on a Census Year period basis (July 1, year 1, to June 30, year 2).Source population is date referenced July 1.
If I were 65 today, how long could I expect live?
1012141618202224
1950
1953
1956
1959
1962
1965
1968 1971
1974
1977
1980
1983
1986
1989
1992
1995
1998
2001
2004
2007
2010
2013
MaleFemale
Source: Data from BC Stats, Ministry of Technology, Innovation and Citizens' Serviceshttp://www.bcstats.gov.bc.ca/StatisticsBySubject/Demography/VitalStatistics.aspx
as accessed Set 2, 2014Note: Population data after 1970 adjusted for non-permanent residents and undercount.
Figures prepared through the use of single year of age life table.using deaths provided by Vital Statistics, Ministry of Health, and theaverage of consecutive years of population provided by Statistics Canada.Deaths are on a Census Year period basis (July 1, year 1, to June 30, year 2).Source population is date referenced July 1.
Life Tables Canadian Life BC Life Public Service
Pension Plan Age Male Female Male Female Male Female
55 80.01 84.11 81.20 84.84 83.22 86.62
60 80.84 84.72 81.98 85.41 83.80 86.99
65 81.98 85.52 83.01 86.16 84.96 87.61 Source: PensionsBC BC Pension Corp.
Health Care Professional Conference36
6050403020100
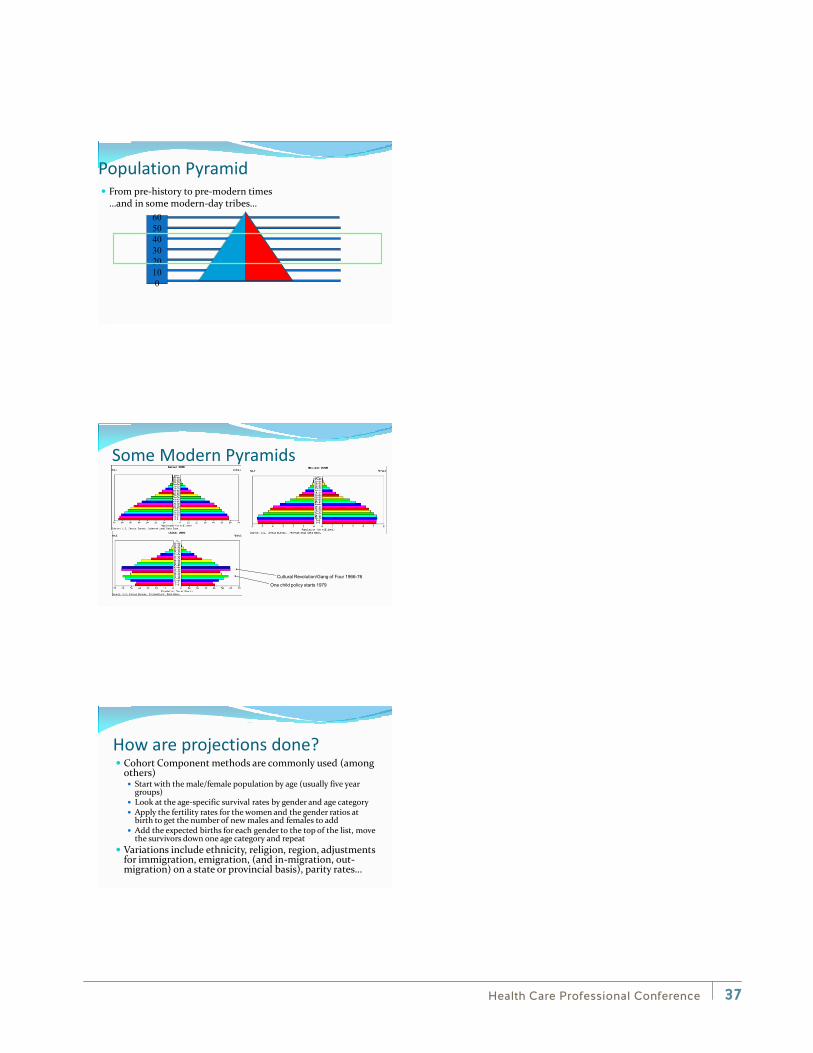
Population Pyramid From pre-history to pre-modern times
…and in some modern-day tribes…
Some Modern Pyramids
One child policy starts 1979
Cultural Revolution/Gang of Four 1966-76
How are projections done? Cohort Component methods are commonly used (among
others) Start with the male/female population by age (usually five year
groups) Look at the age-specific survival rates by gender and age category Apply the fertility rates for the women and the gender ratios at
birth to get the number of new males and females to add Add the expected births for each gender to the top of the list, move
the survivors down one age category and repeat Variations include ethnicity, religion, region, adjustments
for immigration, emigration, (and in-migration, out-migration) on a state or provincial basis), parity rates…
Health Care Professional Conference 37
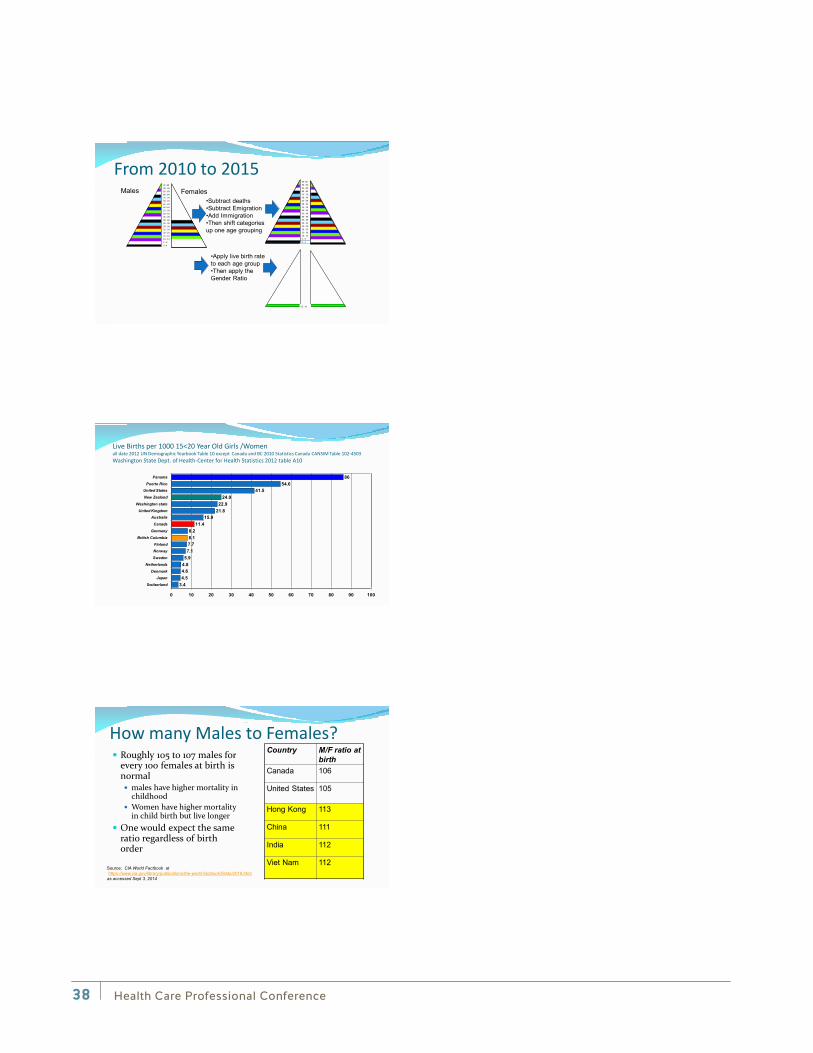
95 -99 90 - 94 85 - 89 80 - 84 75 - 79 70 - 74 65 - 69 60 - 64 55 - 59 50 - 54 45 - 49 40 - 44 35 - 39 30 - 34 25 - 29 20 - 24 15 - 19 10 - 14 5 - 9 0 - 4
From 2010 to 2015 •Subtract deaths•Subtract Emigration•Add Immigration•Then shift categories up one age grouping
????????????????????????????????????????????????????????????????????????????????????
95 -99 90 - 94 85 - 89 80 - 84 75 - 79 70 - 74 65 - 69 60 - 64 55 - 59 50 - 54 45 - 49 40 - 44 35 - 39 30 - 34 25 - 29 20 - 24 15 - 19 10 - 14 5 - 9 0 - 4
•Apply live birth rateto each age group•Then apply the Gender Ratio
0 - 4
Males Females
Live Births per 1000 15<20 Year Old Girls /Women all date 2012 UN Demographic Yearbook Table 10 except Canada and BC 2010 Statistics Canada CANSIM Table 102-4503 Washington State Dept. of Health-Center for Health Statistics 2012 table A10
3.44.54.64.85.97.17.78.18.2
11.415.9
21.822.9
24.941.5
54.686
0 10 20 30 40 50 60 70 80 90 100
Switzerland
JapanDenmark
Netherlands
Sweden
NorwayFinland
British Columbia
Germany
Canada
AustraliaUnited Kingdom
Washington state
New Zealand
United StatesPuerto Rico
Panama
How many Males to Females? Roughly 105 to 107 males for
every 100 females at birth is normal males have higher mortality in
childhood Women have higher mortality
in child birth but live longer One would expect the same
ratio regardless of birth order
Country M/F ratio at birth
Canada 106
United States 105
Hong Kong 113
China 111
India 112
Viet Nam 112Source: CIA World Factbook athttps://www.cia.gov/library/publications/the-world-factbook/fields/2018.html
as accessed Sept 3, 2014
Health Care Professional Conference38
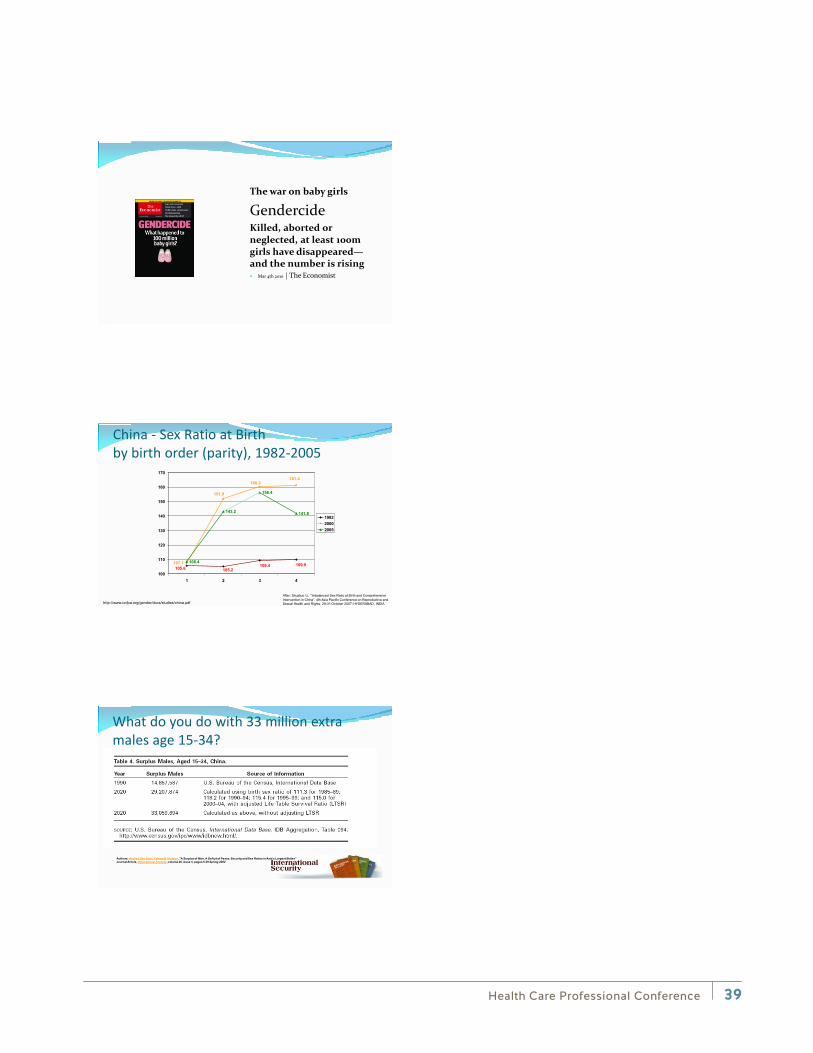
The war on baby girls
Gendercide Killed, aborted or neglected, at least 100m girls have disappeared—and the number is rising Mar 4th 2010 | The Economist
China - Sex Ratio at Birth by birth order (parity), 1982-2005
108.4
143.2
156.4
141.8
109.9109.4105.2105.6
161.4160.3
151.9
107.1
100
110
120
130
140
150
160
170
1 2 3 4
198220002005
http://www.unfpa.org/gender/docs/studies/china.pdf
After: Shuzhuo Li, “Imbalanced Sex Ratio at Birth and ComprehensiveIntervention in China”, 4th Asia Pacific Conference on Reproductive and Sexual Health and Rights, 29-31 October 2007; HYDERABAD, INDIA
What do you do with 33 million extra males age 15-34?
Authors: Andrea Den Boer, Valerie M. Hudson, "A Surplus of Men, A Deficit of Peace: Security and Sex Ratios in Asia's Largest States"Journal Article, International Security, volume 26, issue 4, pages 5-39 Spring 2002
Health Care Professional Conference 39
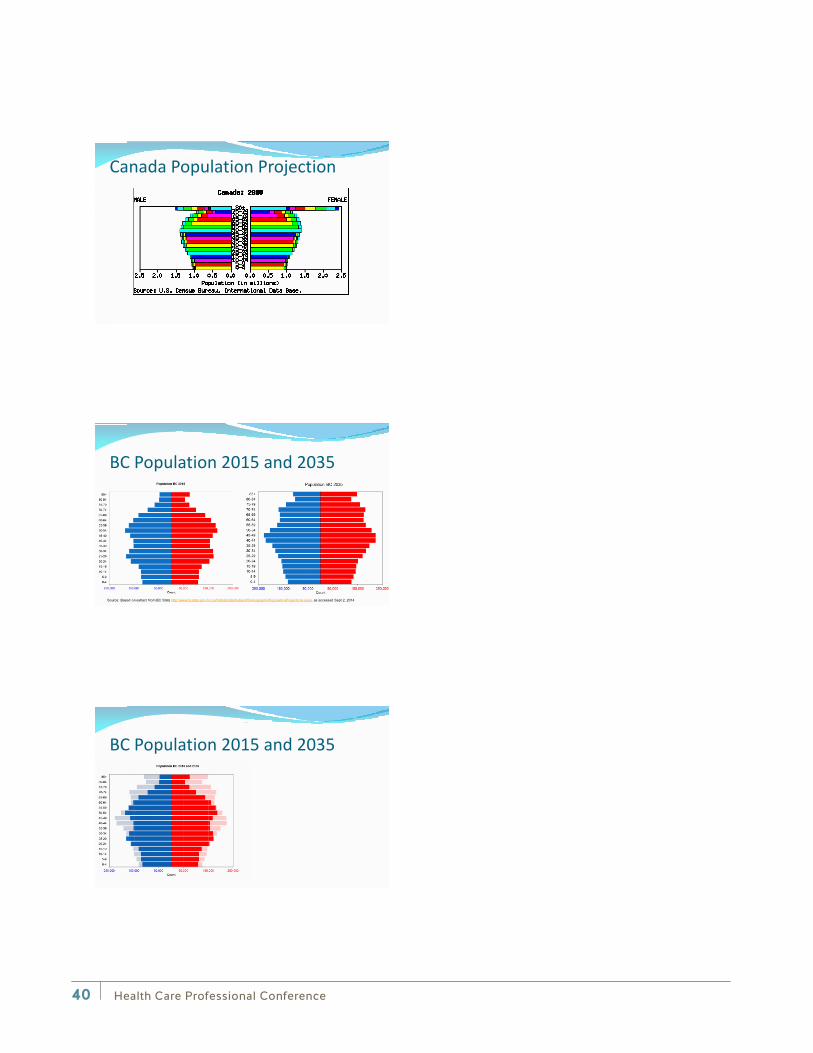
Canada Population Projection
BC Population 2015 and 2035
Source: Based on extract from BC Stats http://www.bcstats.gov.bc.ca/StatisticsBySubject/Demography/PopulationProjections.aspx as accessed Sept 2, 2014
BC Population 2015 and 2035
Health Care Professional Conference40
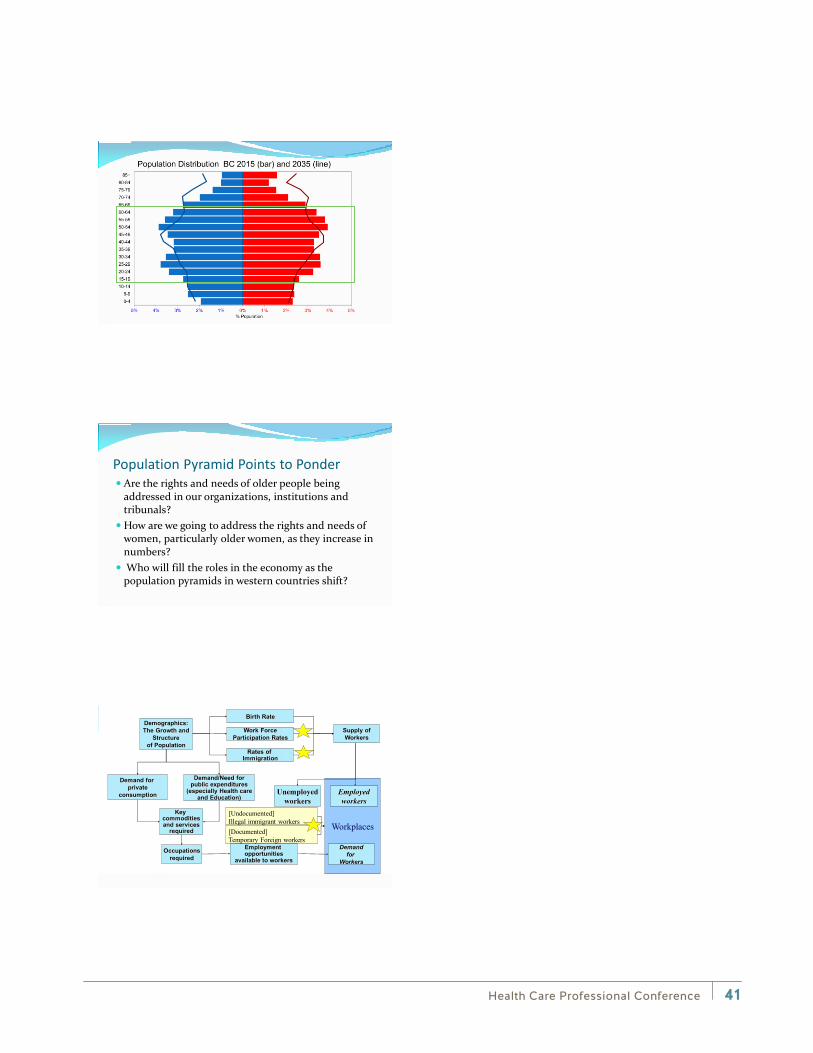
Population Pyramid Points to Ponder Are the rights and needs of older people being
addressed in our organizations, institutions and tribunals?
How are we going to address the rights and needs of women, particularly older women, as they increase in numbers?
Who will fill the roles in the economy as the population pyramids in western countries shift?
Workplaces
Demographics:The Growth and
Structure of Population
Key commoditiesand services
required
Employment opportunities
available to workers
Demandfor
Workers
Occupationsrequired
Rates of Immigration
Work ForceParticipation Rates
Birth Rate
Supply ofWorkers
Demand for private
consumption
Demand/Need forpublic expenditures
(especially Health careand Education)
Unemployedworkers
Employedworkers
[Undocumented]Illegal immigrant workers[Documented] Temporary Foreign workers
Health Care Professional Conference 41

Immigration? Possible source but…
We are competing with every other industrialized nations for the same skilled immigrants
New immigrants bring new challenges and may be more vulnerable to workplace injury, stress and adjustment
Canada Source: "Citizenship and Immigration Canada, Facts and Figures". Citizenship and Immigration Canada. 2013. Retrieved Dec 7, 2013.
Canada
Canadian Immigration
China 13%
Philippines 13%India 11%
Pakistan 4%USA 4%
USA
US ImmigrationMexico 14%
China 7%India 7%Philippines 5%Dominican Rep 4%
US Source: U.S. Lawful Permanent Residents: 2013" (PDF). Annual Flow Report, May 2014
Australian ImmigrationNew Zealand 18%India 12%China 12%UK 4%Philippines 4%
Australia Sourcehttps://www.immi.gov.au/media/fact-sheets/02key.htm /
Australia
UK
UK Source: https://www.gov.uk/government/publications/immigration-statistics-april-to-june-2014/immigration-statistics-april-to-june-2014#settlement-1
UK ImmigrationIndia 17%Pakistan 12%Nigeria 5%China 5%South Africa 4%
Immigration Trends: Canada(2012), US(2013), Australia(2012/13), UK(Q2 2014)
Temporary Foreign Workers? A growing source but…
We are competing with every other industrialized nations for the same skilled immigrants
Temporary foreign workers bring new challenges and may be more vulnerable to workplace injury, stress and adjustment
Health Care Professional Conference42
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
BC
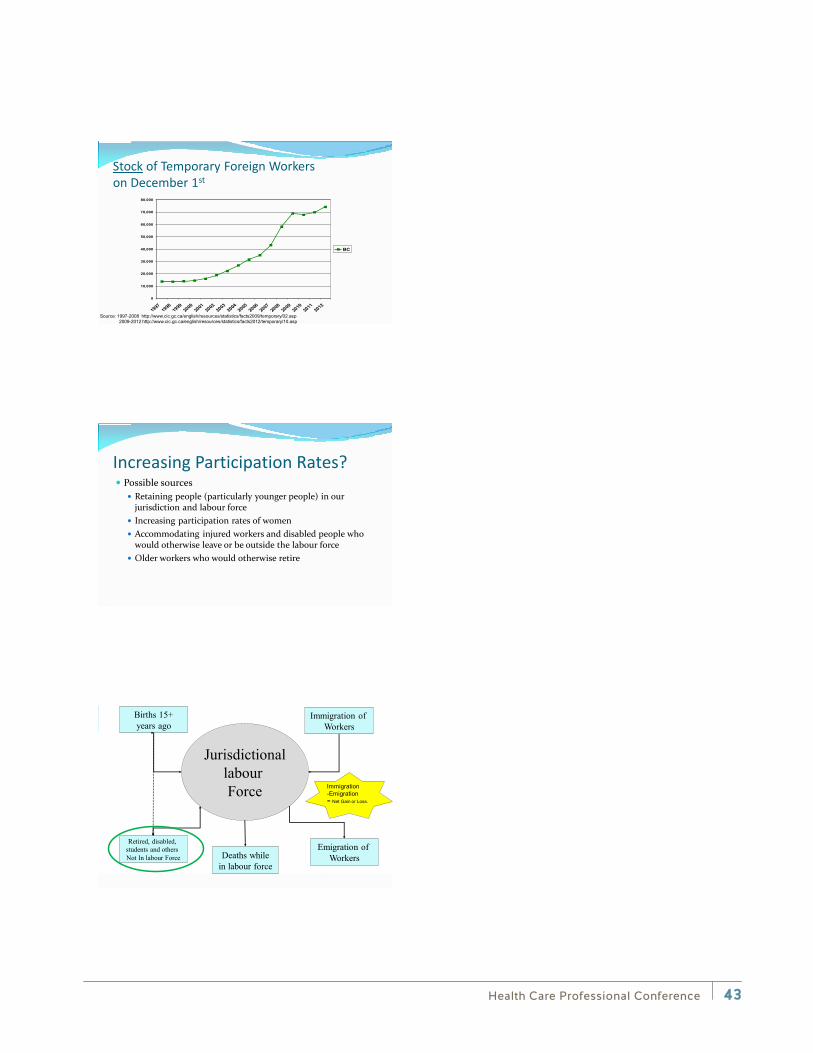
Stock of Temporary Foreign Workers on December 1st
Source: 1997-2008 http://www.cic.gc.ca/english/resources/statistics/facts2009/temporary/02.asp2009-2012 http://www.cic.gc.ca/english/resources/statistics/facts2012/temporary/10.asp
Increasing Participation Rates? Possible sources
Retaining people (particularly younger people) in our jurisdiction and labour force
Increasing participation rates of women Accommodating injured workers and disabled people who
would otherwise leave or be outside the labour force Older workers who would otherwise retire
JurisdictionallabourForce
Births 15+years ago
Retired, disabled, students and others Not In labour Force Deaths while
in labour force
Immigration of Workers
Emigration of Workers
Immigration -Emigration = Net Gain or Loss.
Health Care Professional Conference 43
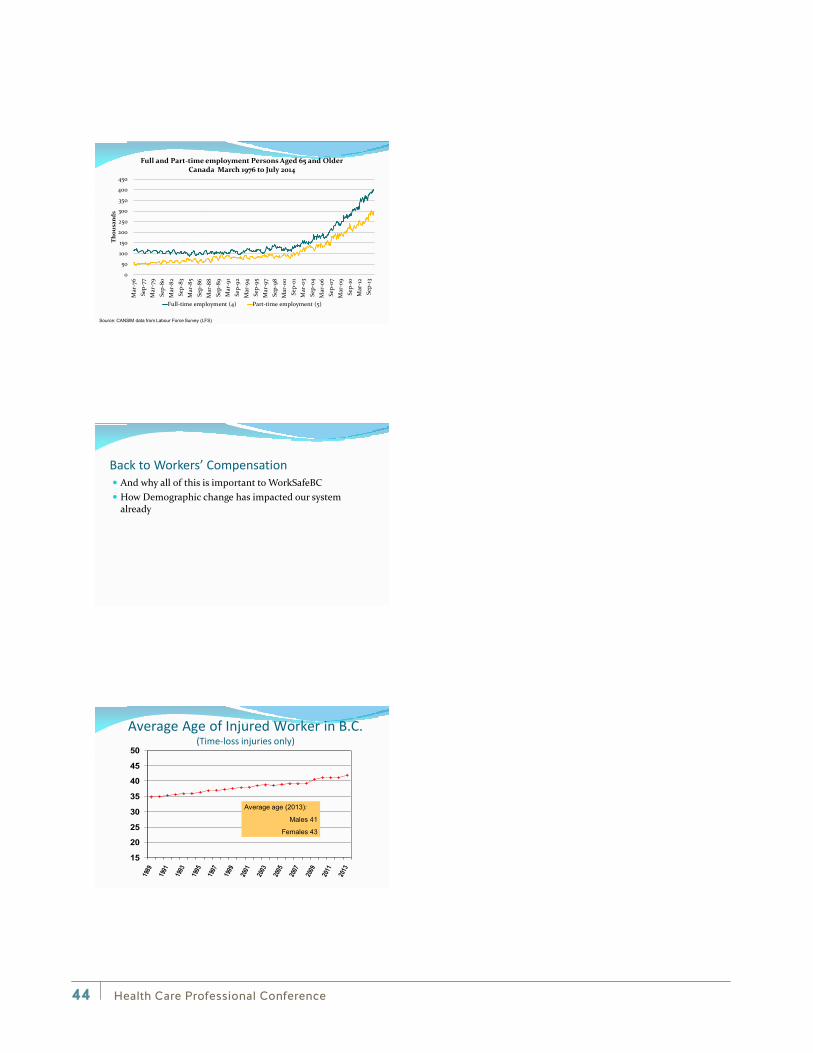
Source: CANSIM data from Labour Force Survey (LFS)
0
50
100
150
200
250
300
350
400
450
Mar
-76
Sep-
77M
ar-7
9Se
p-80
Mar
-82
Sep-
83M
ar-8
5Se
p-86
Mar
-88
Sep-
89M
ar-9
1Se
p-92
Mar
-94
Sep-
95M
ar-9
7Se
p-98
Mar
-00
Sep-
01M
ar-0
3Se
p-04
Mar
-06
Sep-
07M
ar-0
9Se
p-10
Mar
-12
Sep-
13
Thou
sand
s
Full and Part-time employment Persons Aged 65 and Older Canada March 1976 to July 2014
Full-time employment (4) Part-time employment (5)
Back to Workers’ Compensation And why all of this is important to WorkSafeBC How Demographic change has impacted our system
already
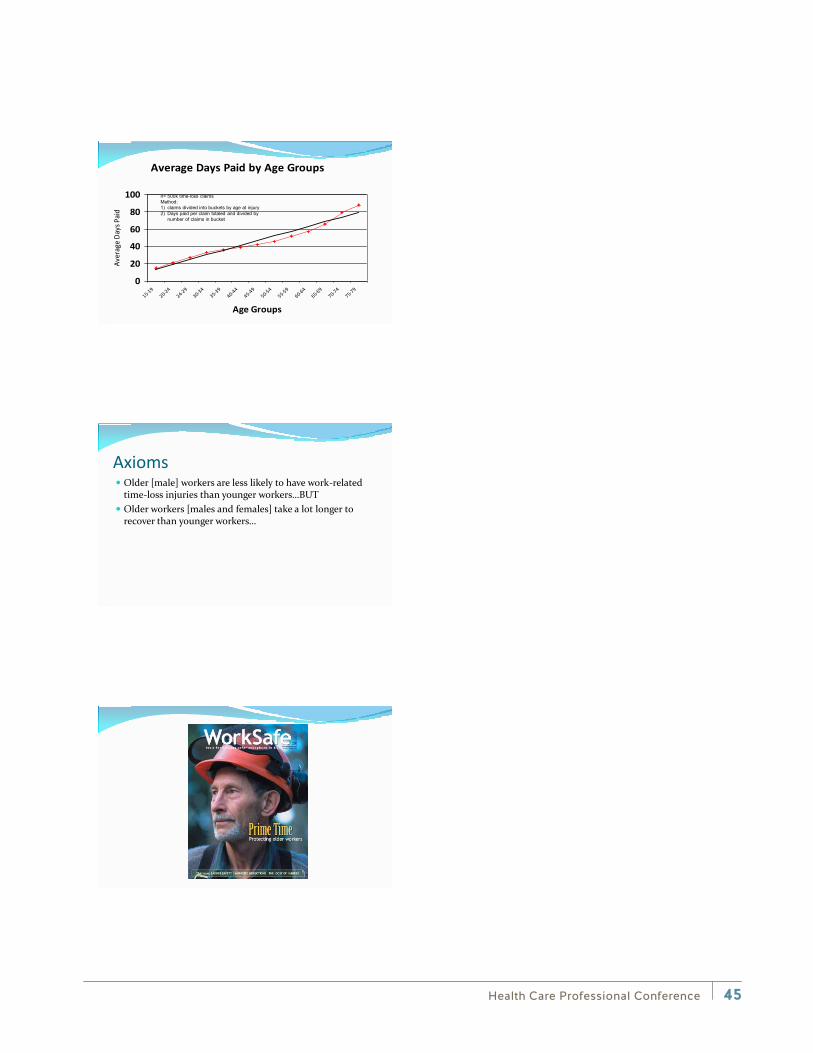
15
20
25
30
35
40
45
50
1989
1991
1993
1995
1997
1999
2001
2003
2005
2007
2009
2011
2013
Average age (2013):
Males 41
Females 43
Average Age of Injured Worker in B.C. (Time-loss injuries only)
Health Care Professional Conference44
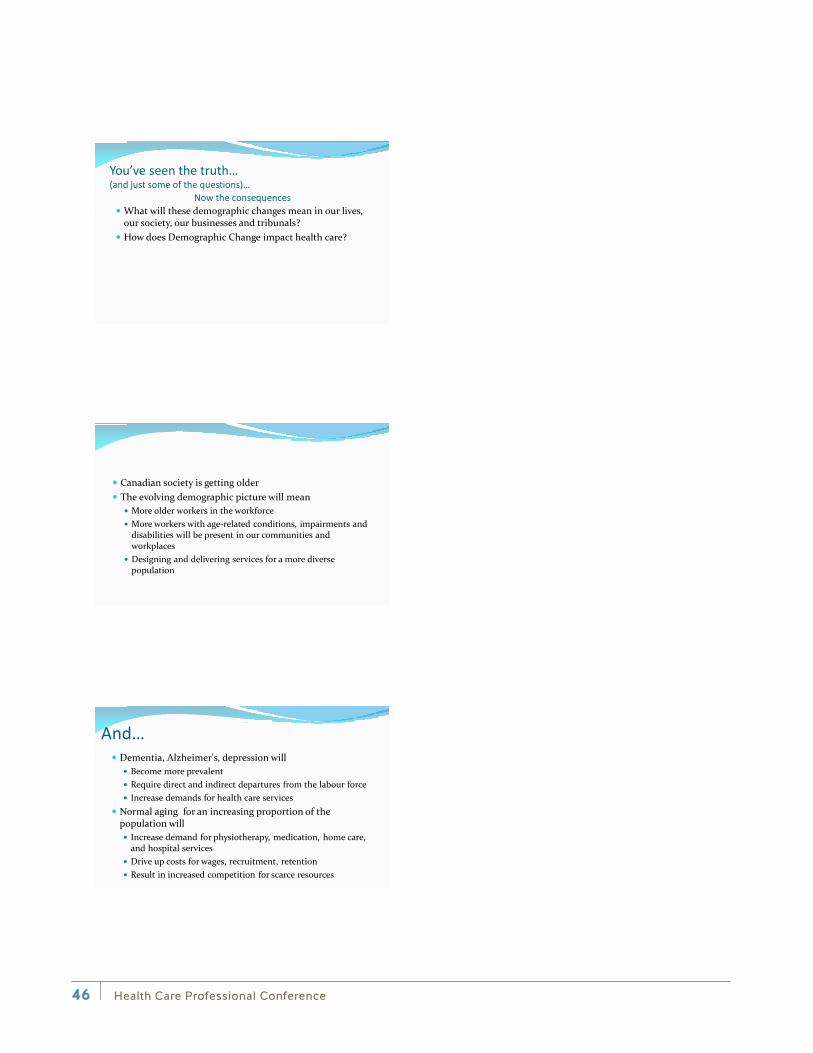
Average Days Paid by Age Groups
0
20
40
60
80
100
15-19
20-24
24-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
75-79
Age Groups
Aver
age D
ays P
aid
n= 500k time-loss claims Method: 1) claims divided into buckets by age at injury2) Days paid per claim totaled and divided by
number of claims in bucket
Axioms Older [male] workers are less likely to have work-related
time-loss injuries than younger workers…BUT Older workers [males and females] take a lot longer to
recover than younger workers…
Health Care Professional Conference 45
You’ve seen the truth… (and just some of the questions)…
What will these demographic changes mean in our lives, our society, our businesses and tribunals?
How does Demographic Change impact health care?
Now the consequences
Canadian society is getting older The evolving demographic picture will mean
More older workers in the workforce More workers with age-related conditions, impairments and
disabilities will be present in our communities and workplaces
Designing and delivering services for a more diverse population
And… Dementia, Alzheimer's, depression will
Become more prevalent Require direct and indirect departures from the labour force Increase demands for health care services
Normal aging for an increasing proportion of the population will Increase demand for physiotherapy, medication, home care,
and hospital services Drive up costs for wages, recruitment, retention Result in increased competition for scarce resources
Health Care Professional Conference46
Further… We will see more people from outside Canada come to live
permanently and temporarily to fill many occupations Older workers will become more prevalent in the labour
force More workers will be vulnerable due to
Age “newness” to the job Language and culture Economics Precariousness of employment
Some final thoughts Be sensitive… Take care of your health… Be very nice to your children… Be very generous to your retirement savings…
Health Care Professional Conference Vancouver Hyatt Regency– September 12, 2014
Terrance J. BogyoIndependent Researcher | Speaker | Consultant
Health Care Professional Conference 47

Health Care Professional Conference48
Health Care Professional Conference 49
Dr. Merv Gilbert, PhD, R Psych
Dr. Merv Gilbert is a psychologist with over thirty years experience in direct clinical and leadership roles at regional, provincial, and international levels. He has published and presented in a diverse array of forums on the importance of workplace psychological health and safety for individuals and organizations. Dr. Gilbert has also served on a number of professional and non-profit organizations and currently serves on the steering committee of the American Psychological Association’s Psychologically Healthy Workplace Network.
Dr. Gilbert is currently a principal partner with Psych Health + Safety, a consulting partnership, providing planning, training, implementation and evaluation services that enable organizations to foster psychologically healthy employees and workplace climates. He is an Adjunct Professor with the Centre for Applied Research in Mental Health and Addiction (CARMHA), a research centre within the Faculty of Health Sciences at Simon Fraser University. Dr. Gilbert is a primary participant in the development, evaluation and dissemination of resources for workplace mental health. His most recent work has been creating resources for the Mental Health Commission of Canada.
Plenary session: Taking Action to Improve Psychological Health and Safety in the Workplace
More and more employers recognize the legal, financial, and practical need to effectively address workplace psychological health and safety but are unsure where to start. Is their organization ready to change? What resources will they need? How will they know if their actions are effective? This session will provide an overview of Psychological health and safety: An action guide for employers. The guide is one of the key resources identified in the National Standard of Canada for Psychological Health and Safety in the Workplace. The session will take participants through a strategic, sequential planning process that will include identification of practical, evidence –informed actions that are readily accessible to all employers, regardless of size or sector. It will be of interest to health professionals, human resource practitioners, health and safety experts, employers, organized labour and employee representatives. Key learning objectives include:
• Introduction to Psychological Health and Safety: An Action Guide for Employers
• Determining the business case for your organization
• Selection the best actions for your organization
• Creating an action plan for your organization
Health Care Professional Conference50
Breakout session: Psychologically and Occupationally Responsive Treatment (PORT)
PORT is a training program that enhances the treatment and rehabilitation of workers with psychological conditions by presenting an approach that integrates psychological and work-related issues, focusing on barriers to successful coping with the work situation and recovery of occupational function.
Learning objectives:
• Improve understanding of the various factors that are critical to return-to-work (RTW) planning for clients with mental health disorders including preparation, planning, implementation and relapse prevention
• Become familiar with a workforce problem-solving model, and how it can be applied to improve communication and understanding between employers, healthcare providers, employees in order to achieve successful RTW
• Enhance awareness of effective interventions for sustained work return
• Learn about various tools that can facilitate RTW planning for individuals with mental health issues
Taking Action to improve Psychological Health & Safety in
the Workplace 10th Annual Health Care Professional Conference
Vancouver, September 12th, 2014
Merv Gilbert, PhD, RPsych
Partner, Psych Health + Safety Consulting Adjunct Professor, CARMHA, Simon Fraser University Chair, BCPA Psychologically Healthy Workplace Committee Steering Committee, APA Centre for Organizational Excellence
Love and work are the
cornerstones of our
humanness
But for too many adults, their work is experienced as compromising their
psychological (mental) health
Health Care Professional Conference 51
Impact of poor psychological health • Estimated to cost the Canadian economy $50
billion dollars/year (+) • Fastest rising cause of long term disability,
main cause in some (e.g. health care) • Longer periods of absence than most other
disorders (e.g. diabetes, back pain, cardiac disease)
• Raises the risk for other psychological and physical disorders
• Contributes to accidents, injuries and incidents
Why is this happening now? • The worker? • The workplace?
• The nature of work?
•OH&S movement triggered improvement in physical domain •PH&S aims to trigger action in psychological domain
Occupational Health & Safety
Psychological H&S
Physical H&S
Evolution of Health and Safety
Health Care Professional Conference52

FINANCIAL Big impact on productivity
LEGAL Regulators & courts demand it
PRAGMATIC It’s hard to solve problems with distressed workers
ETHICAL It’s the right thing to do …
The business case for addressing PH&S?
The Standard focuses on mental illness prevention and mental health promotion in the workplace. It is intended to help prevent harm to all people in the workplace, whether or not they have had a lived experience with mental illness.
“(A workplace) in which every practical effort is made to avoid
foreseeable injury to the mental health of employees.”
The National Standard for Canada: Psychological health and safety in the
workplace — Prevention, promotion, and guidance to staged implementation
Goal: Create psychologically healthy and safe workplaces that meet the needs of employers and employees
Health Care Professional Conference 53

The APA Psychologically Healthy Workplace Model
The choice for employers: • Do nothing: Outcome is increased
costs, decreased productivity/morale, loss of skilled workforce
• Act: Outcome is decreased costs, increased productivity/morale, recruitment/retention of skilled workers
But where do we start?
Introducing: Psychological Health & Safety: An Action Guide for Employers
Available at www.carmha.ca
Health Care Professional Conference54
POLICY
PLANNING
PROMOTION
PREVENTION
PROCESS
PERSISTENCE
The P6 Model
24 employer actions to enhance and protect PH&S. Actions are:
• Evidence-consistent • Practical • Stand-alone Includes stories, resources, references and topics of special interest (e.g. PH&S
for small business)
Some key actions to improve workplace PH&S
1. Take a strategic approach 2. Assess and address risks to PH&S 3. Train Managers in engaged performance
management 4. Train employees in psychological safety skills 5. Provide timely support to staff who are
struggling
Health Care Professional Conference 55
Take a Strategic Approach
Integrated into the organizational plan, vision & values
Meaningful leadership & employee involvement Based on a clear business case
E.g. Measure of Organizational Readiness for Psychological Health (MORPH)
Assess and address PH&S hazards &
risks
Workplace variables that impact employee
psychological health
Employee input (surveys, focus groups,…) Key indicators (absence, STD/LTD, benefits utilization, grievances…)
e.g. Guarding Minds @ Work
Train and support
managers
Appropriate skills to respond to staff with possible MH issues
Training may be are in-person, online, written materials
E.g. WorkSafeBC Bullying and Harassment Prevention toolkit
Health Care Professional Conference56

Train employees in PH&S skills
Adapted to fit the needs of the worker,
the workplace and the organization
E.g. Resiliency training, conflict resolution, active problem-solving,
stress management
E.g. Coaching Antidepressant Self-care Skills (CASS)
Support employees
who are struggling
Early intervention to prevent functional
impairment & disability
Support access to effective on-line
resources, psychological
treatment, SAW/RTW
E.g. Psychologically & Occupationally Responsive Treatment (PORT)
The BCPA Psychologically Healthy Workplace Program
• Mission: to enhance and ensure the health, productivity and sustainability of Canadian workers and workplaces
• Members: psychologists, business leaders, academics and informed professionals volunteering their time and expertise
• Actions: Provide education and recognition for British Columbia organizations to enhance psychologically healthy and safe workplaces
For more information: http://www.phwa.ca/
Health Care Professional Conference 57

An Example: Brookhaven Extended Care Facility
Questions? Comments?
Merv Gilbert [email protected]
Health Care Professional Conference58
Psychologically & Occupationally Responsive Treatment
PORT
10th Annual Health Care Professional Conference Vancouver, September 12th, 2014
1
Merv Gilbert, PhD, RPsych Partner, Psych Health + Safety Consulting Adjunct Professor, CARMHA, Simon Fraser University
Objectives • Understand key principles critical to providing treatment and
rehabilitation for employed clients with psychological issues • Understand an alternative to the medical model, a problem-focused
approach to occupational disability • Integrate into intervention planning a cognitive behavioral approach,
focused on enhancement of the individuals capacity for effective personal and interpersonal coping
• Learn strategies to enhance appropriate and timely participation and engagement by key participants (employers, employees, unions, healthcare providers)
• Learn about practical tools, resources and programs to facilitate efficient, effective and sustainable recovery and work return
2
What is PORT? PORT is designed to enhance provider effectiveness in treating working
adults with psychological conditions by integrating occupational and psychological perspectives. Treatment incorporates primary, secondary and tertiary actions to address employee psychological health and safety.
3
Occupational Perspective
Psychological Perspective
Effective & Efficient Treatment
Health Care Professional Conference 59
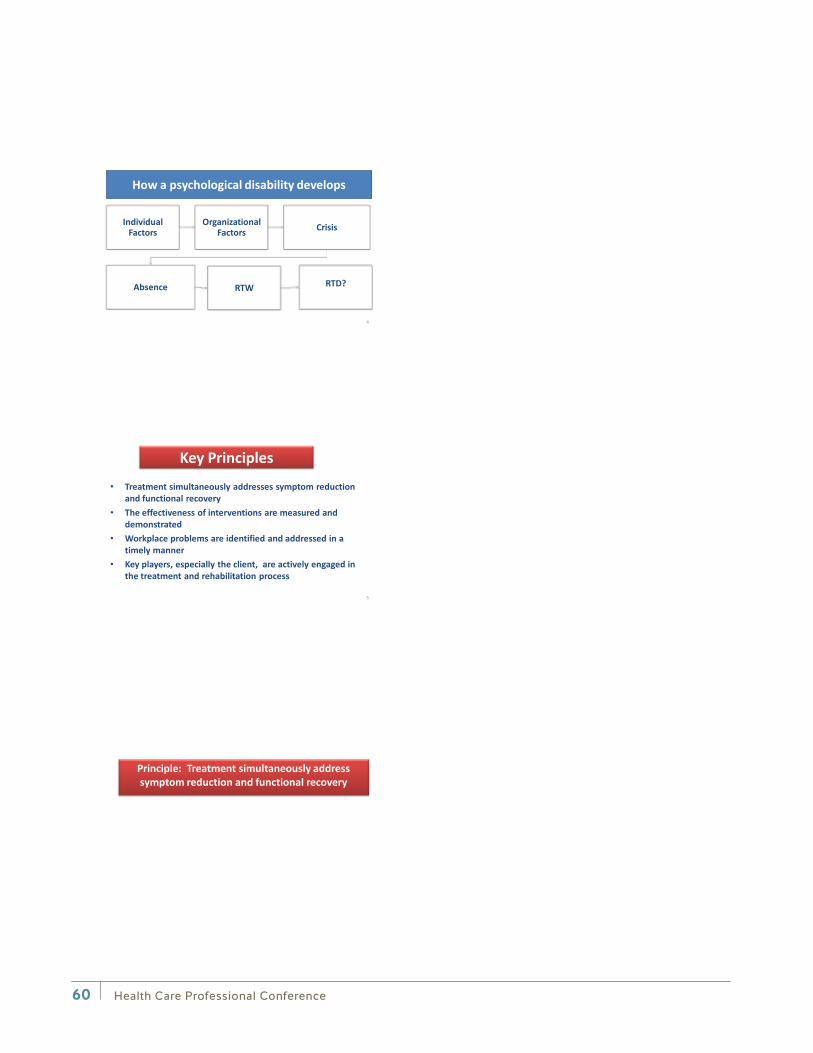
Individual Factors
Organizational Factors Crisis
Absence RTW RTD?
How a psychological disability develops
4
Key Principles • Treatment simultaneously addresses symptom reduction
and functional recovery • The effectiveness of interventions are measured and
demonstrated • Workplace problems are identified and addressed in a
timely manner • Key players, especially the client, are actively engaged in
the treatment and rehabilitation process
5
Principle: Treatment simultaneously address symptom reduction and functional recovery
Health Care Professional Conference60

FINANCIAL Big impact on productivity
LEGAL Regulators & courts demand it
PRAGMATIC It’s hard to solve problems with distressed workers
ETHICAL It’s the right thing to do …
The business case for addressing PH&S?
The Standard focuses on mental illness prevention and mental health promotion in the workplace. It is intended to help prevent harm to all people in the workplace, whether or not they have had a lived experience with mental illness.
“(A workplace) in which every practical effort is made to avoid
foreseeable injury to the mental health of employees.”
The National Standard for Canada: Psychological health and safety in the
workplace — Prevention, promotion, and guidance to staged implementation
Goal: Create psychologically healthy and safe workplaces that meet the needs of employers and employees
Health Care Professional Conference 61
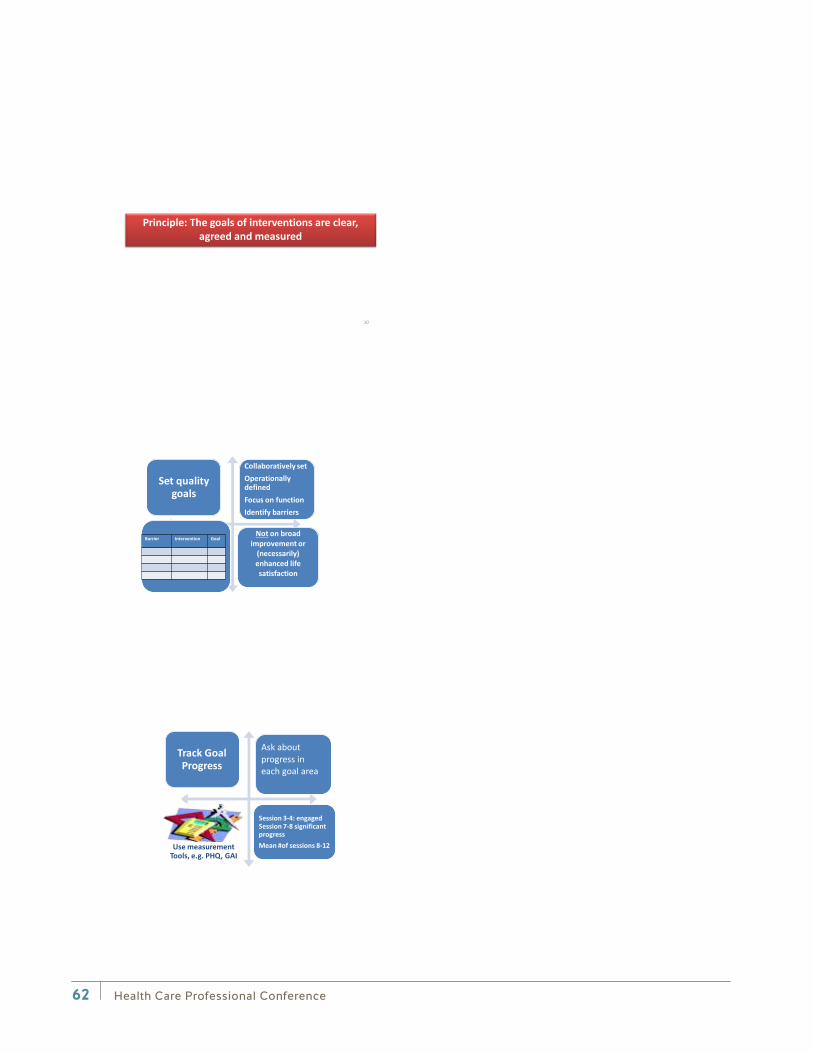
Principle: The goals of interventions are clear, agreed and measured
10
Set quality goals
Collaboratively set Operationally defined Focus on function Identify barriers
Not on broad improvement or
(necessarily) enhanced life satisfaction
Barrier Intervention Goal
Track Goal Progress
Ask about progress in each goal area
Session 3-4: engaged Session 7-8 significant progress Mean #of sessions 8-12
Use measurement Tools, e.g. PHQ, GAI
Health Care Professional Conference62
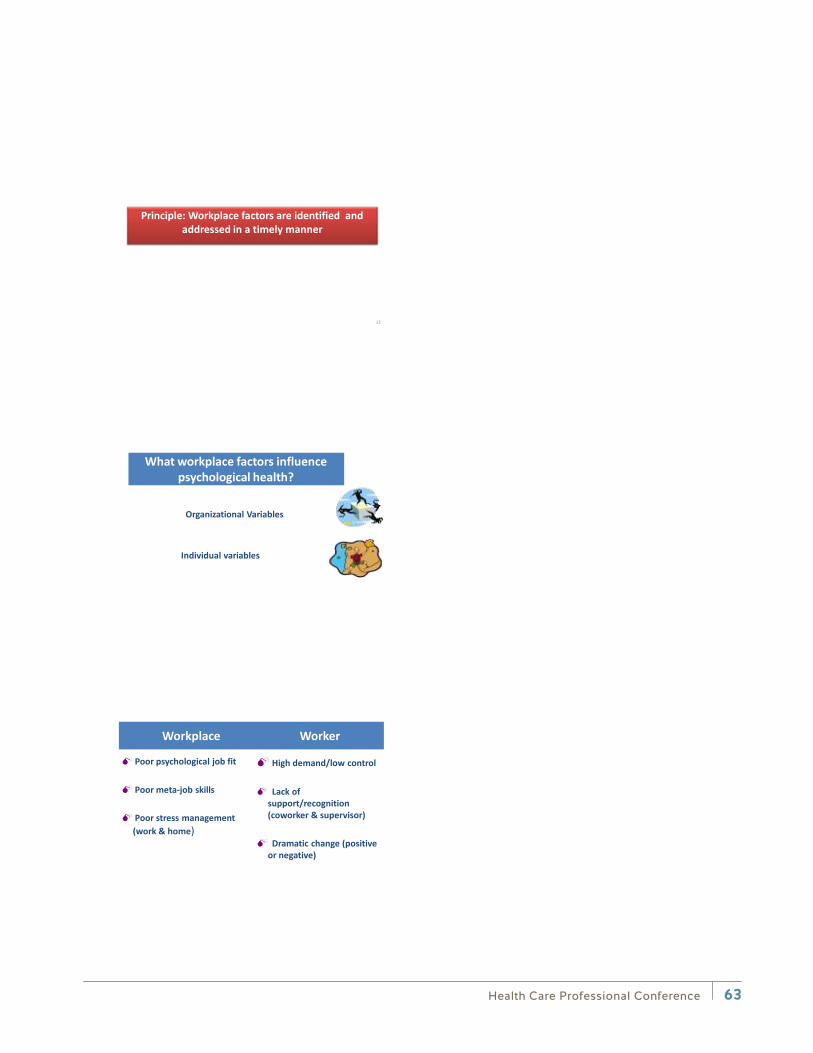
Principle: Workplace factors are identified and addressed in a timely manner
13
What workplace factors influence psychological health?
Individual variables
Organizational Variables
Workplace Worker
Poor psychological job fit Poor meta-job skills Poor stress management
(work & home)
High demand/low control Lack of
support/recognition (coworker & supervisor)
Dramatic change (positive
or negative)
Health Care Professional Conference 63
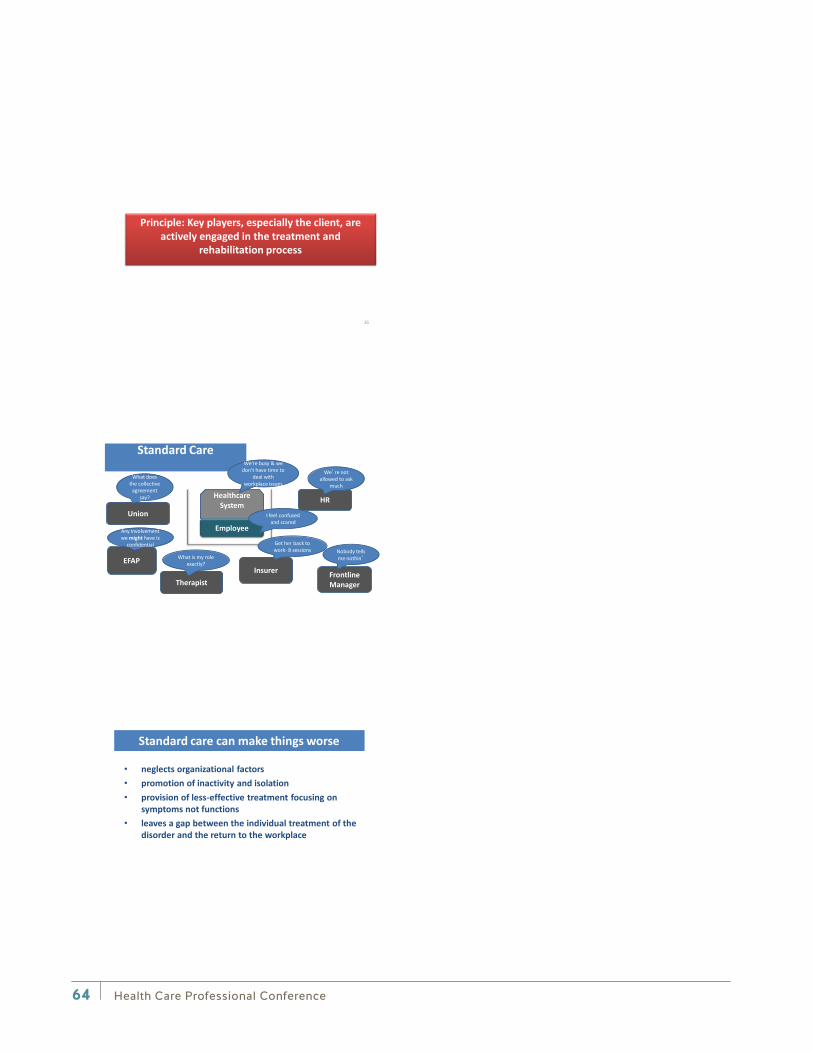
Principle: Key players, especially the client, are actively engaged in the treatment and
rehabilitation process
16
HR Healthcare System
Union
EFAP
Frontline Manager
Employee
Insurer
What does the collective
agreement say?
Any involvement we might have is
confidential
We’re not allowed to ask
much
Get her back to work- 8 sessions Nobody tells
me nothin’
Standard Care
Therapist
What is my role exactly?
I feel confused and scared
We’re busy & we don’t have time to
deal with workplace issues
• neglects organizational factors • promotion of inactivity and isolation • provision of less-effective treatment focusing on
symptoms not functions • leaves a gap between the individual treatment of the
disorder and the return to the workplace
Standard care can make things worse
Health Care Professional Conference64
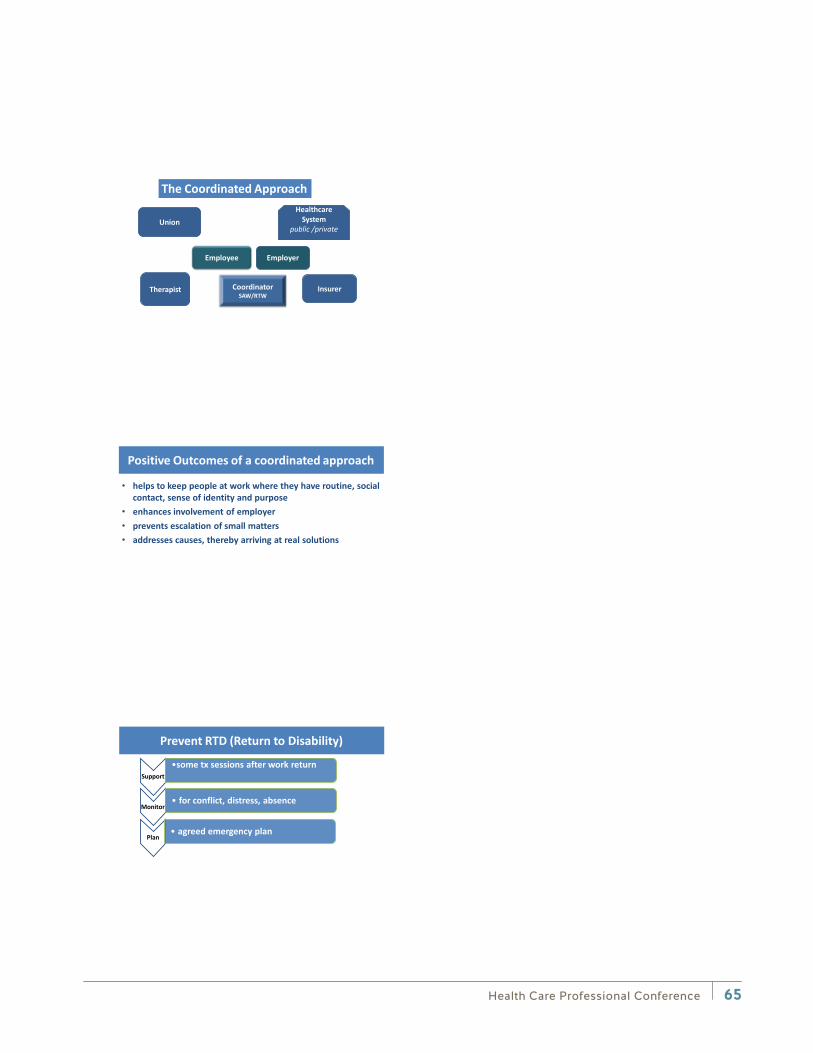
Insurer
Healthcare System
public /private
Union
Therapist
Employer Employee
Coordinator SAW/RTW
The Coordinated Approach
Positive Outcomes of a coordinated approach
• helps to keep people at work where they have routine, social contact, sense of identity and purpose
• enhances involvement of employer • prevents escalation of small matters • addresses causes, thereby arriving at real solutions
Support •some tx sessions after work return
Monitor • for conflict, distress, absence
Plan • agreed emergency plan
Prevent RTD (Return to Disability)
Health Care Professional Conference 65
Health Care Professional Conference 67
Dr. Kendall Ho, MD FRCPC
Dr. Kendall Ho, professor in Emergency Medicine at the University of British Columbia, practices clinically at the Vancouver General Hospital. Before this role, he was the founding director of the UBC Faculty of Medicine eHealth Strategy Office in 2008, and the associate dean of continuing professional development and knowledge translation.
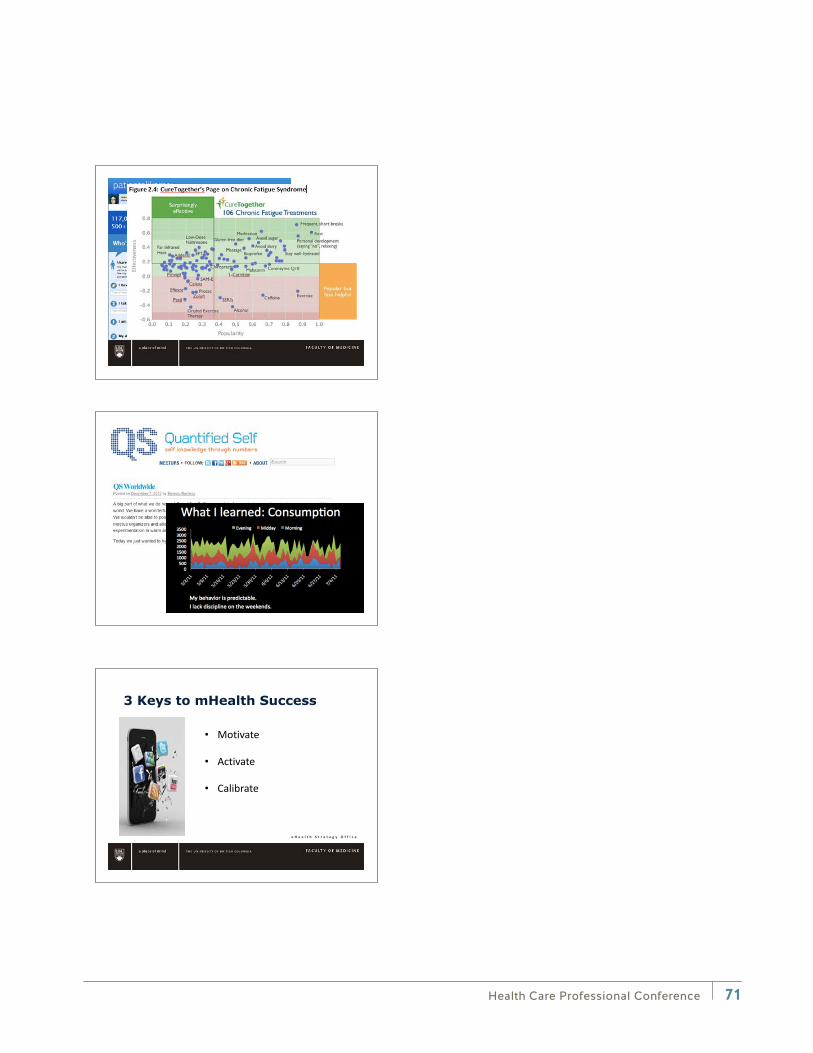
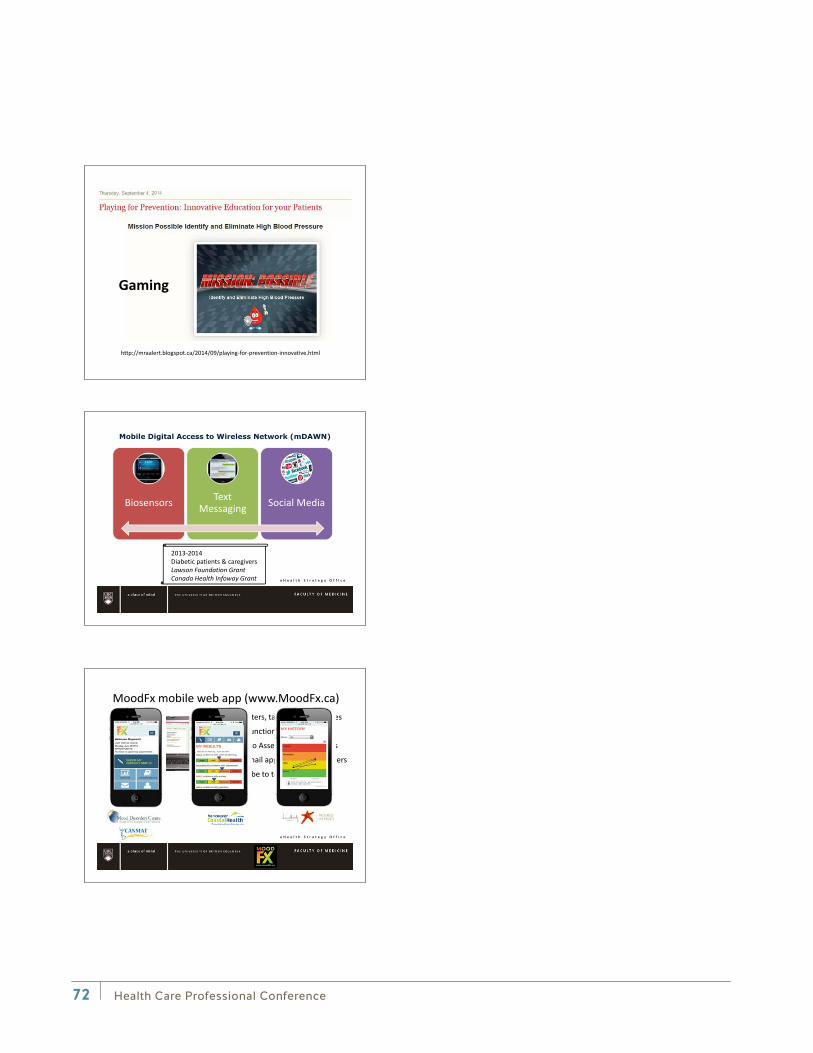
Dr. Ho’s area of academic interest is in eHealth — the innovative application and evaluation of modern information and communication technologies in health research, education, and health practice. Examples of his research include: the use of apps, social media, and biosensors to support patient self-management with health professional support; telehealth using technology-enabled academic detailing to connect pharmacists and physicians for evidence-based prescribing; multicultural patient and care provider engagement for chronic disease management through the inter-Cultural Online health Network (iCON); public education to raise eHealth literacy.
He’s a member of the Association of Faculties of Medicine eHealth Education Committee and the Royal College of Physicians and Surgeons of Canada Professional Development Committee, chairs the Royal College’s eHealth Expert Working Group in CanMEDS 2015 Renewal, and co-chairs the Universitas 21 Health Sciences Social Media for Health Education Committee. He is also a collaborator with the World Health Organization global eHealth Observatory and the Pan American Health Organization Knowledge Management and Communications unit.
Breakout session: Mobile Apps for Quantifying Recovery: Current state and emerging opportunities
Learning objectives:
• To understand the current trends in mobile apps and sensors developments, and how they apply to injured patients and their recovery
• To consider using these sensors in your patient population
• To follow the emerging trends and contributing to their evolution over time
Health Care Professional Conference68
e H e a l t h S t r a t e g y O f f i c e
Mobile Apps for Quantifying Recovery:Current state and emerging opportunities
WorkSafe BC10th Annual Healthcare Professional Conference
September 12th, 2014
Kendall Ho, MD FRCPCProfessor, Emergency Medicine
Director, eHealth Strategy Office
e H e a l t h S t r a t e g y O f f i c e
•
•
•
•
•
e H e a l t h S t r a t e g y O f f i c e
mHealthGlobal Market
$9 million in 2014
>50% annual growth
$10 Billion in 2018
Health Care Professional Conference 69
Health Care Professional Conference70
e H e a l t h S t r a t e g y O f f i c e
e H e a l t h S t r a t e g y O f f i c e
• Motivate
• Activate
• Calibrate
Health Care Professional Conference 71
http://mraalert.blogspot.ca/2014/09/playing-for-prevention-innovative.html
Gaming
e H e a l t h S t r a t e g y O f f i c e
Biosensors Text Messaging Social Media
2013-2014Diabetic patients & caregiversLawson Foundation GrantCanada Health Infoway Grant
e H e a l t h S t r a t e g y O f f i c e
MoodFx mobile web app (www.MoodFx.ca) Computers, tablets, smartphones
Work functioning & depression
Scales to Assess/track outcomes
Text/email appointment reminders
Subscribe to text/email tips
Health Care Professional Conference72
Health Care Professional Conference 73
Carol Kennedy, BScPT, MClSc(manip), FCAMPT
Carol graduated from Queen’s University in 1979, completed her Advanced Diploma of Orthopaedic and Manipulative Therapy in 1984, and her Clinical Masters of Science in Manipulative Therapy from UWO in 2010. She has been at Treloar since 1984 and became a partner in 1989. She’s taught extensively in the Canadian Manual Therapy Course System, as well as internationally, and is a chief examiner for the national exams. In 2005 Carol received an Award of Excellence for Clinical Contribution from the Physiotherapy Association of British Columbia for her work and teaching in the area of the cervical spine.
Carol treats neck pain patients almost exclusively, utilizing the evidence-based practice of manual therapy and specific exercise. She has written chapters on neck exercise in two textbooks. Carol was honoured to be involved in the Olympics as a speaker at the Medical Symposium and as a Clinical Specialist for the Athlete Physiotherapy Clinic. In 2012, Carol was one of the first physiotherapists to successfully complete the Specialization Program through the Canadian Physiotherapy Association in the field of musculoskeletal physiotherapy and also certified as an assessor for that process.
Breakout session: What About the Neck?: Identification and management of potential cervical contribution to concussion symptoms
Learning objectives:
• To be aware of the evidence supporting cervical spine involvement in concussion syndromes
• To be able to identify the features suggestive of cervicogenic headache and dizziness
• To have an awareness of management strategies for the treatment of the cervical spine for headache and dizziness
• Exposure to examples of manual therapy and exercise interventions to improve symptoms arising from the cervical spine

Health Care Professional Conference74
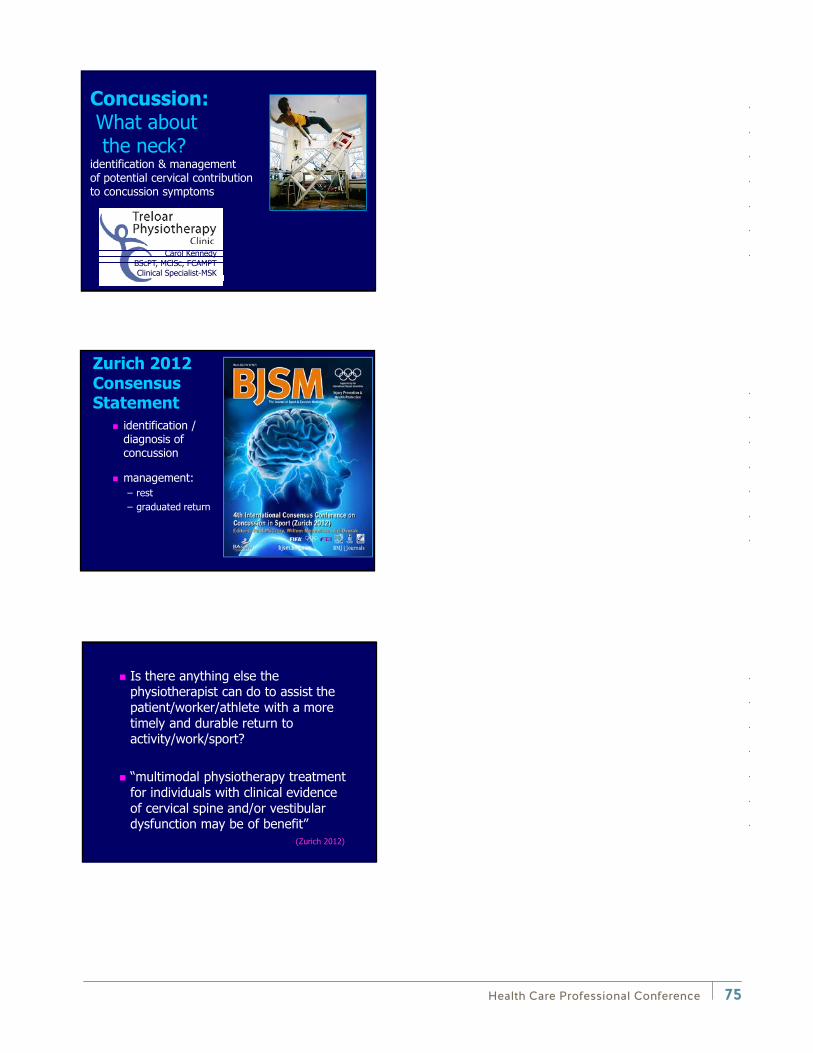
Health Care Professional Conference 75
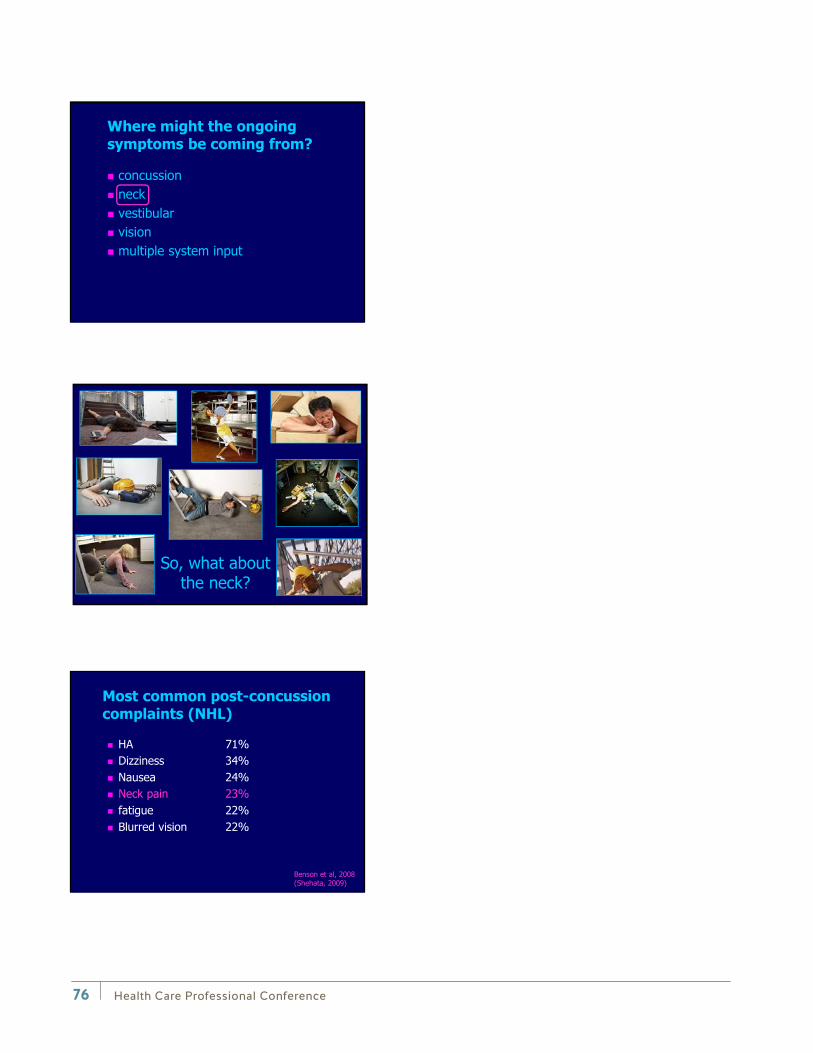
Health Care Professional Conference76

Health Care Professional Conference 77
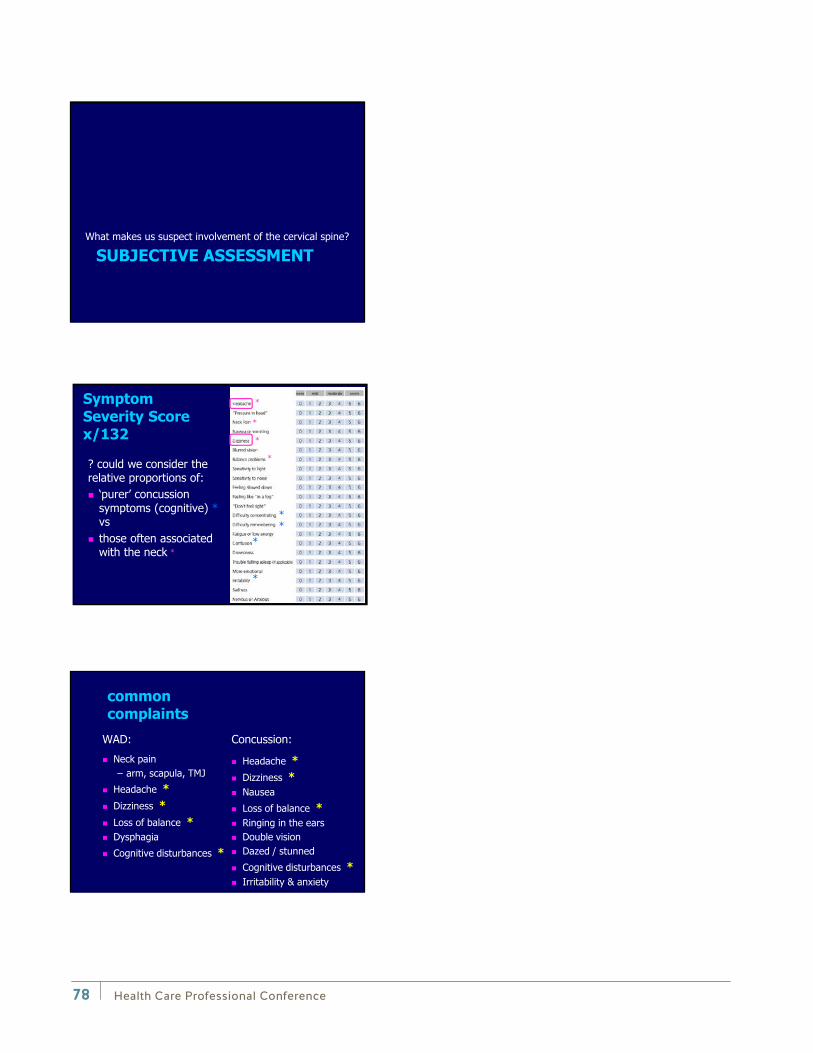
Health Care Professional Conference78
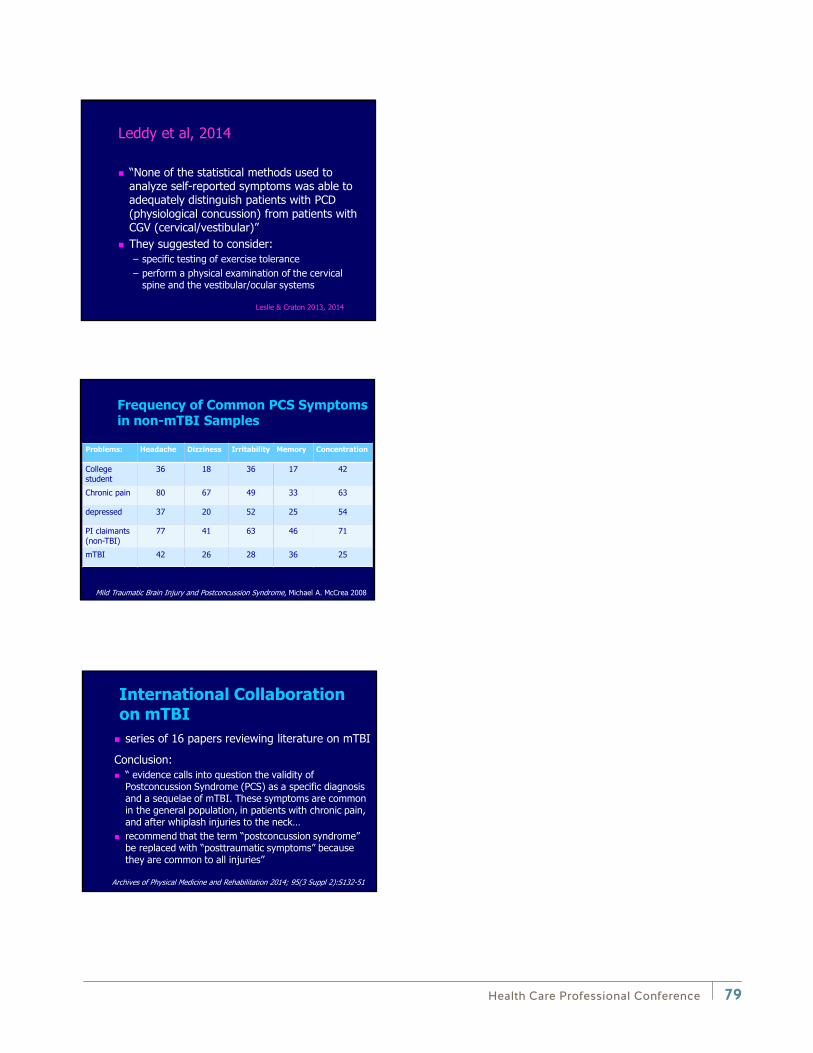
Health Care Professional Conference 79
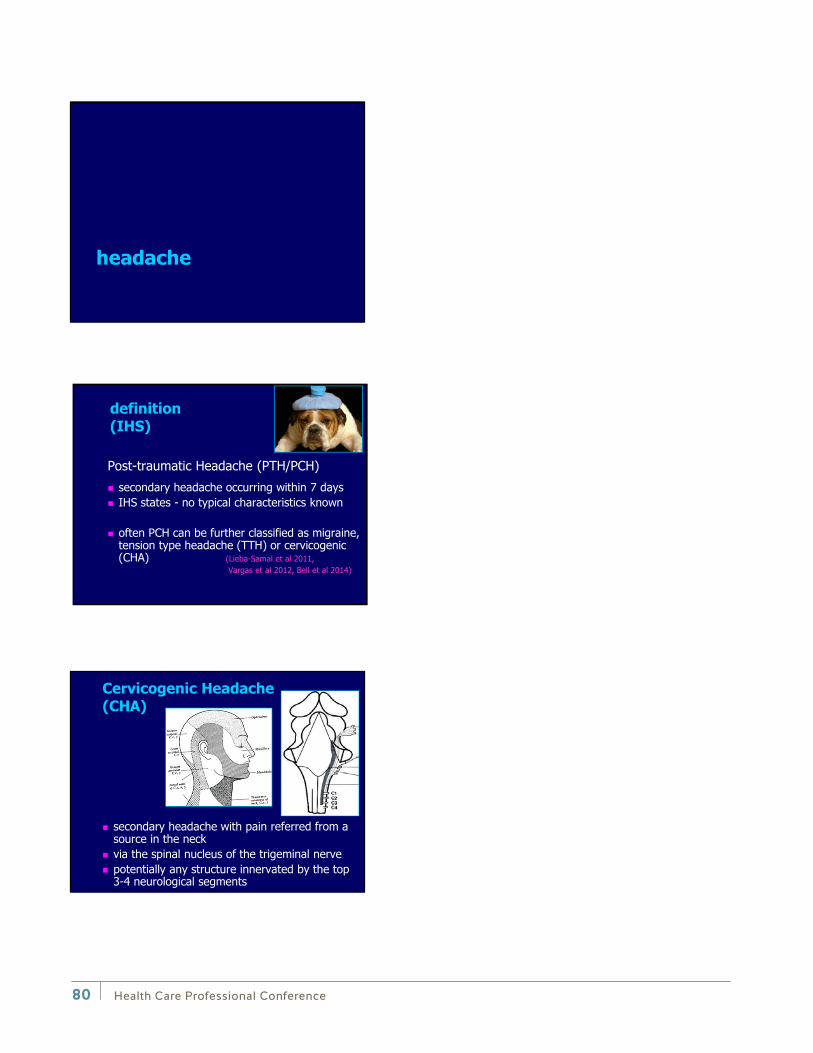
Health Care Professional Conference80
Health Care Professional Conference 81
Health Care Professional Conference82
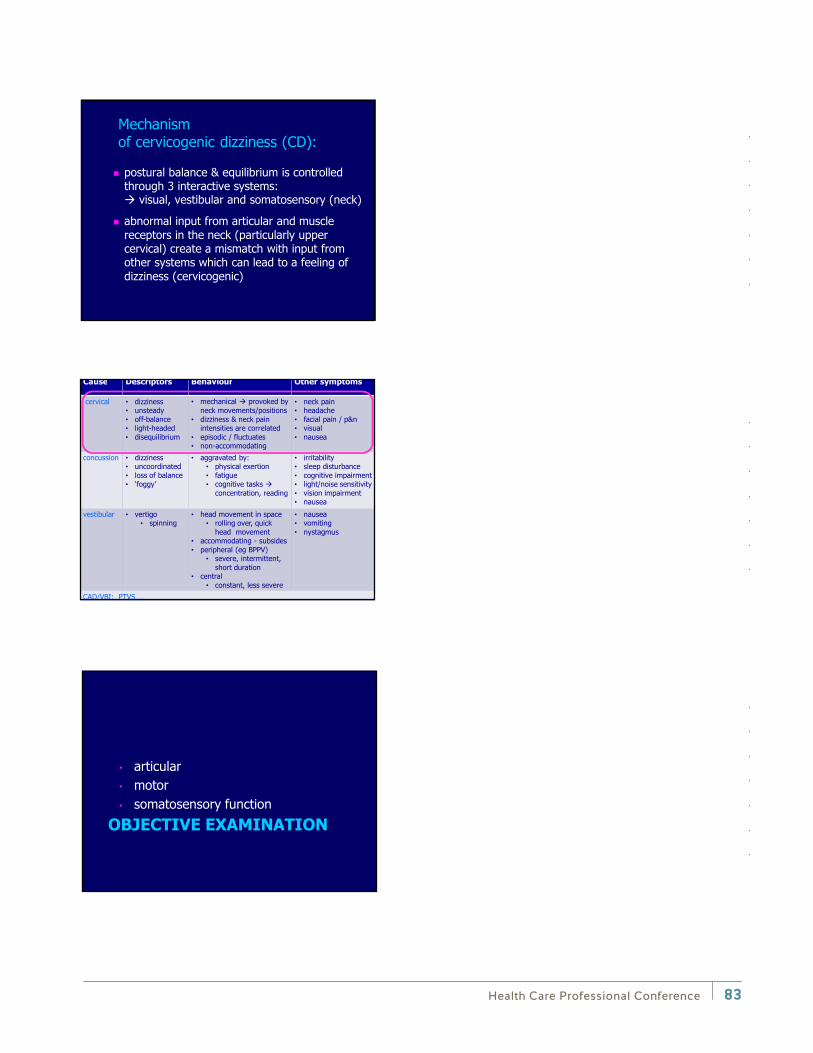
• • • • •
•
•
• •
• • • • •
• • • •
• • • •
• • • • • •
• •
• •
• •
•
• •
• • •
• • •
↓
↓
• • • • •
•
•
• •
• • • • •
• • • •
• • • •
• • • • • •
• •
• •
• •
•
• •
• • •
• • •
↓
↓
• • • • •
•
•
• •
• • • • •
• • • •
• • • •
• • • • • •
• •
• •
• •
•
• •
• • •
• • •
↓
↓
Health Care Professional Conference 83
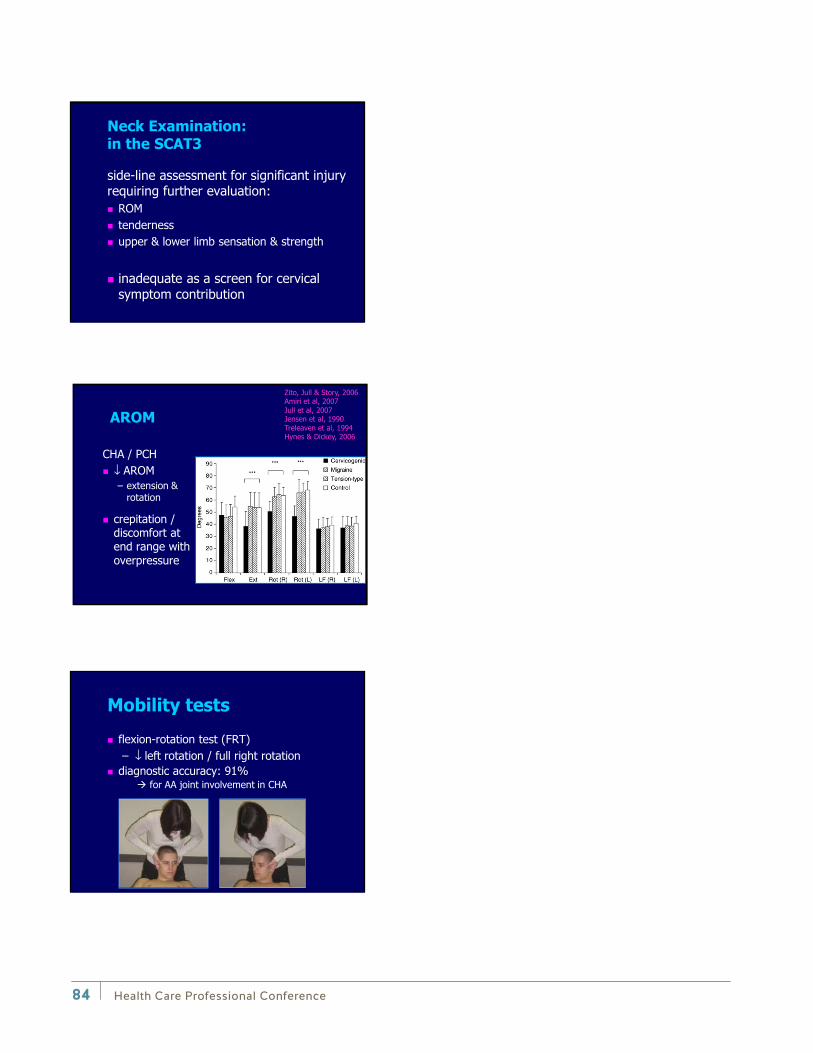
• • • • •
•
•
• •
• • • • •
• • • •
• • • •
• • • • • •
• •
• •
• •
•
• •
• • •
• • •
↓
↓
• • • • •
•
•
• •
• • • • •
• • • •
• • • •
• • • • • •
• •
• •
• •
•
• •
• • •
• • •
↓
↓
• • • • •
•
•
• •
• • • • •
• • • •
• • • •
• • • • • •
• •
• •
• •
•
• •
• • •
• • •
↓
↓
Health Care Professional Conference84
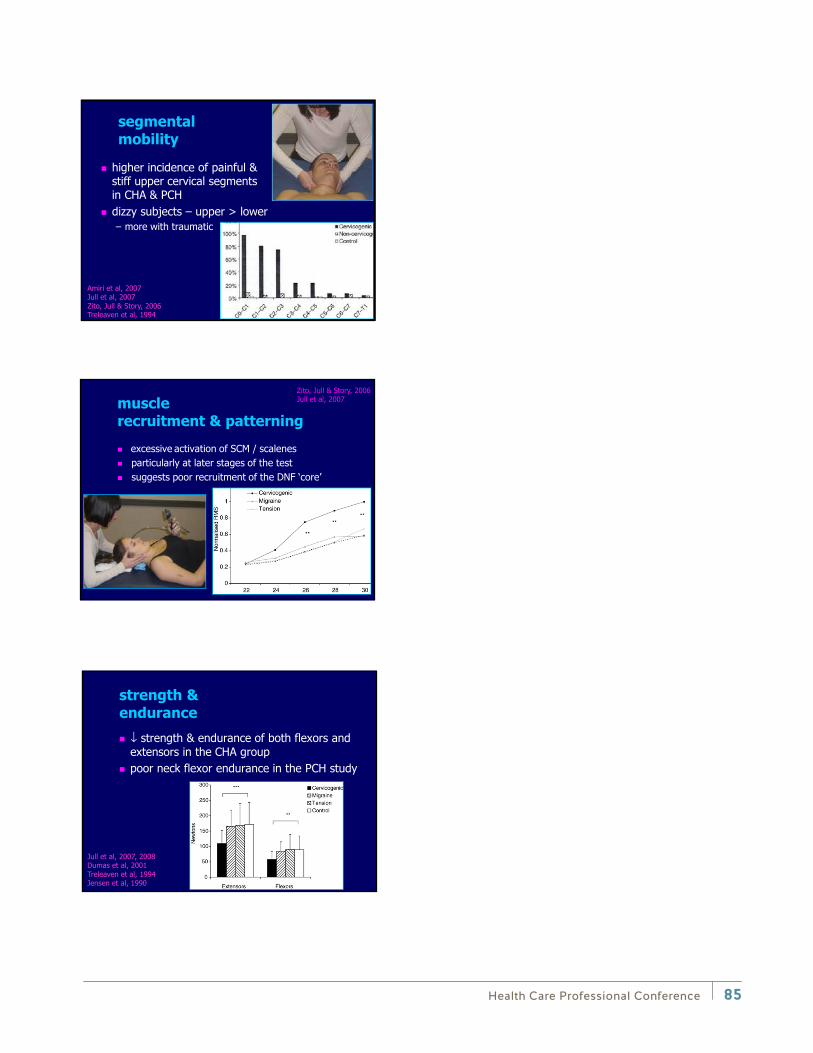
↓
↓
↓
Health Care Professional Conference 85
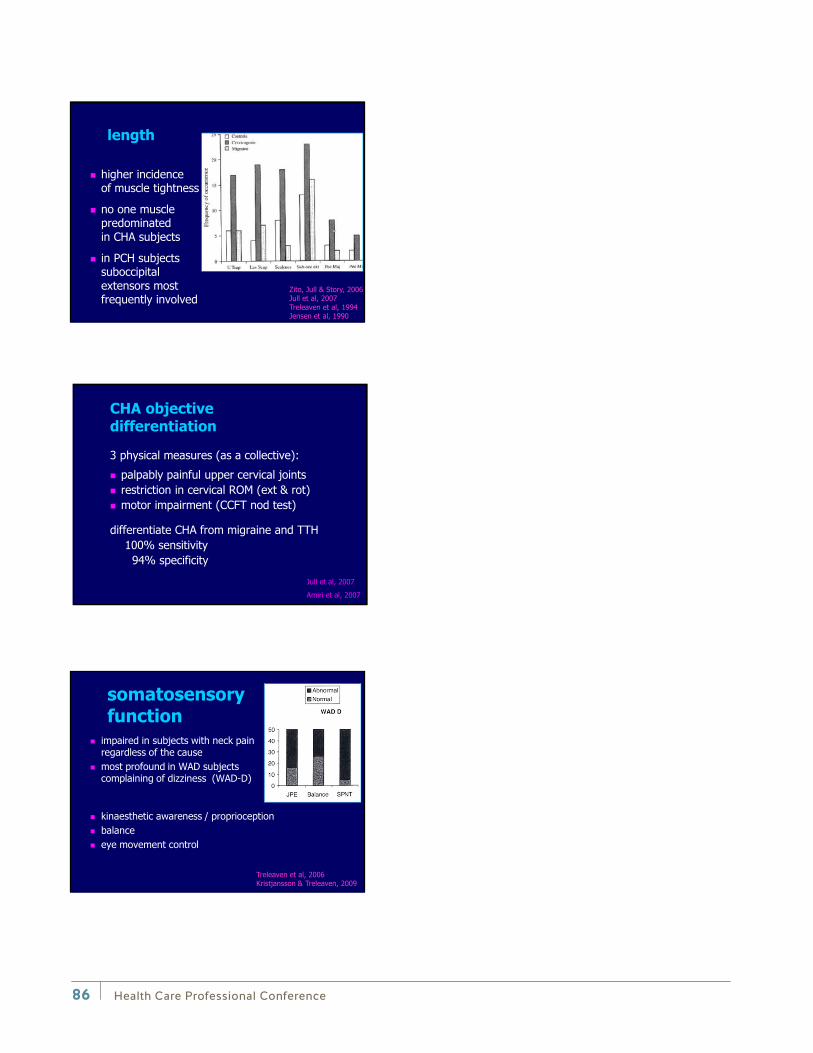
↓
↓
↓
Health Care Professional Conference86
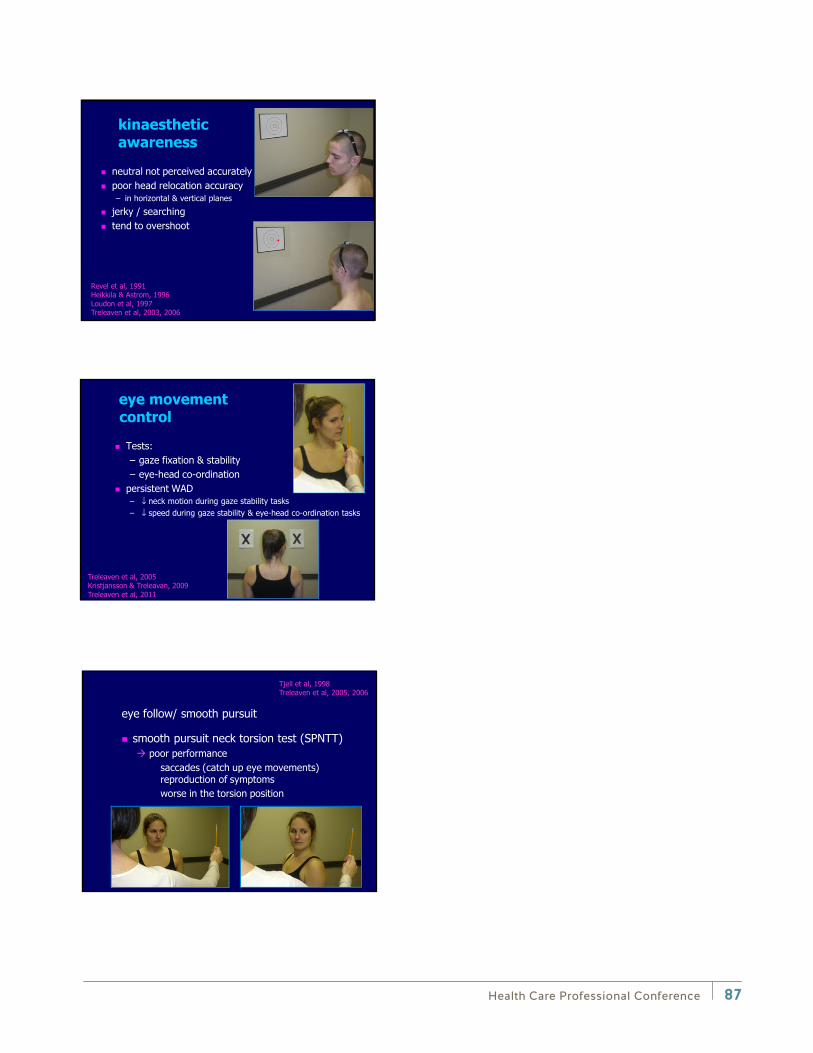
↓ ↓
↓ ↓
↓ ↓
Health Care Professional Conference 87
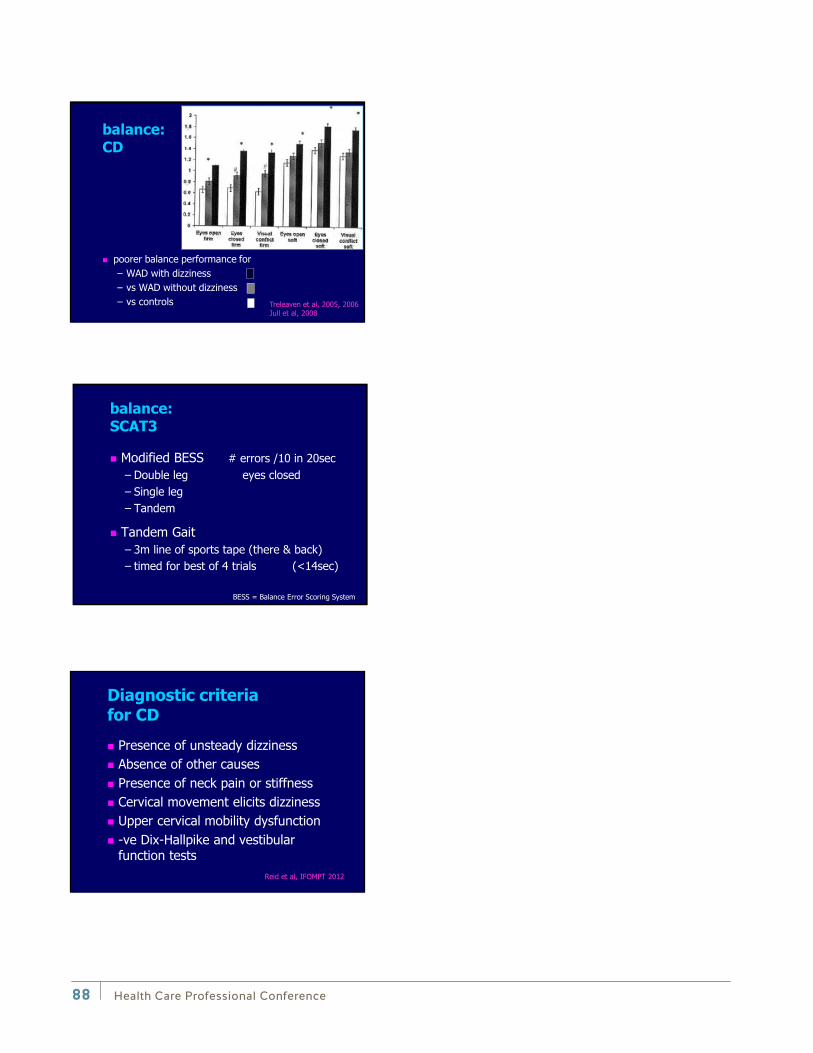
↓ ↓
↓ ↓
↓ ↓
Health Care Professional Conference88

Health Care Professional Conference 89
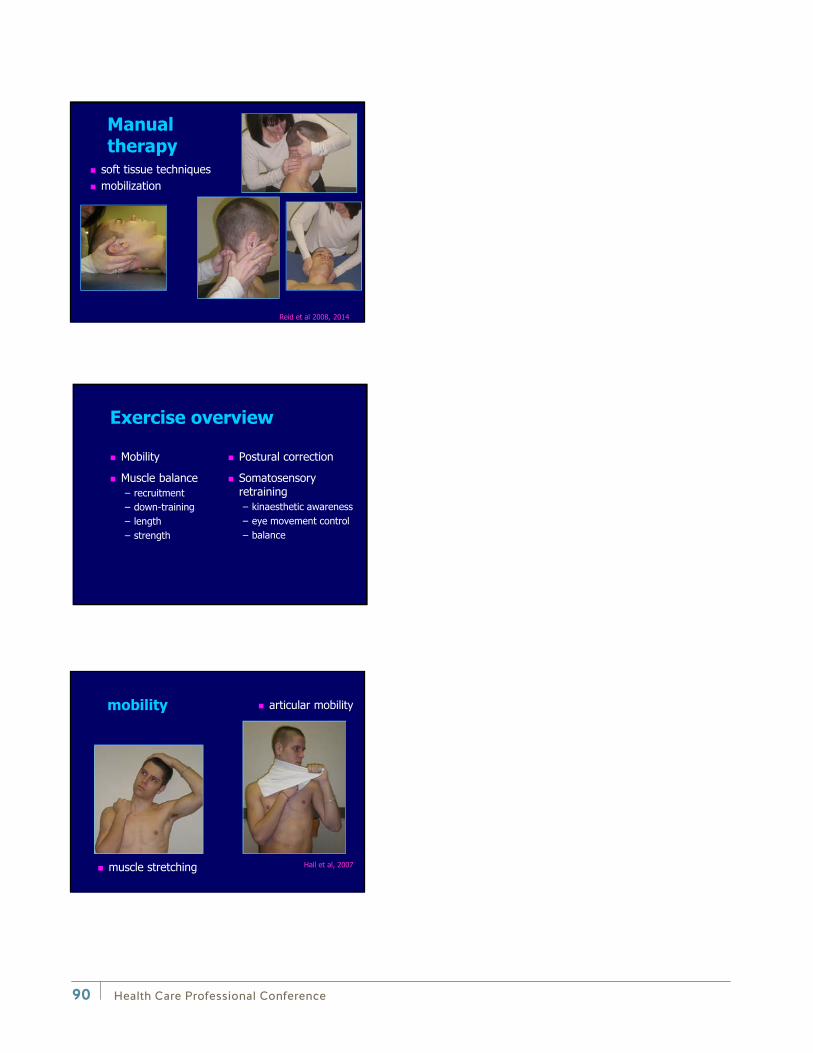
Health Care Professional Conference90
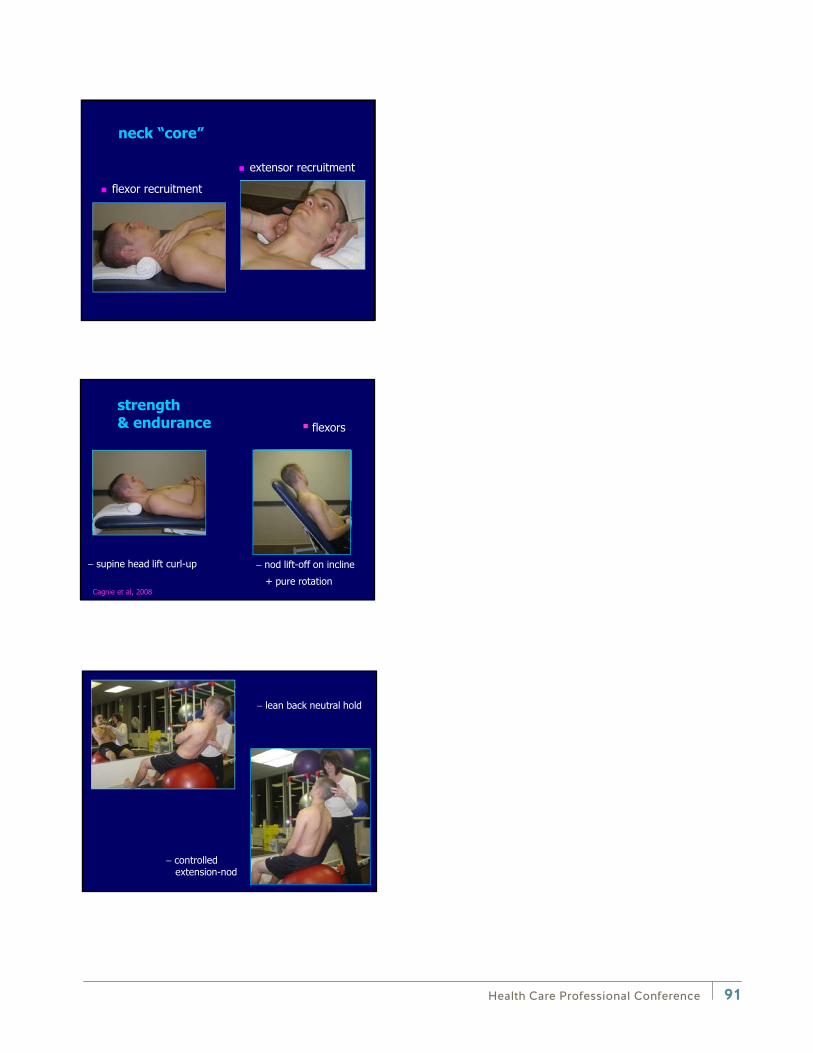
−
−
−
−
−
−
−
−
−
−
−
−
−
−
−
−
−
− Health Care Professional Conference 91
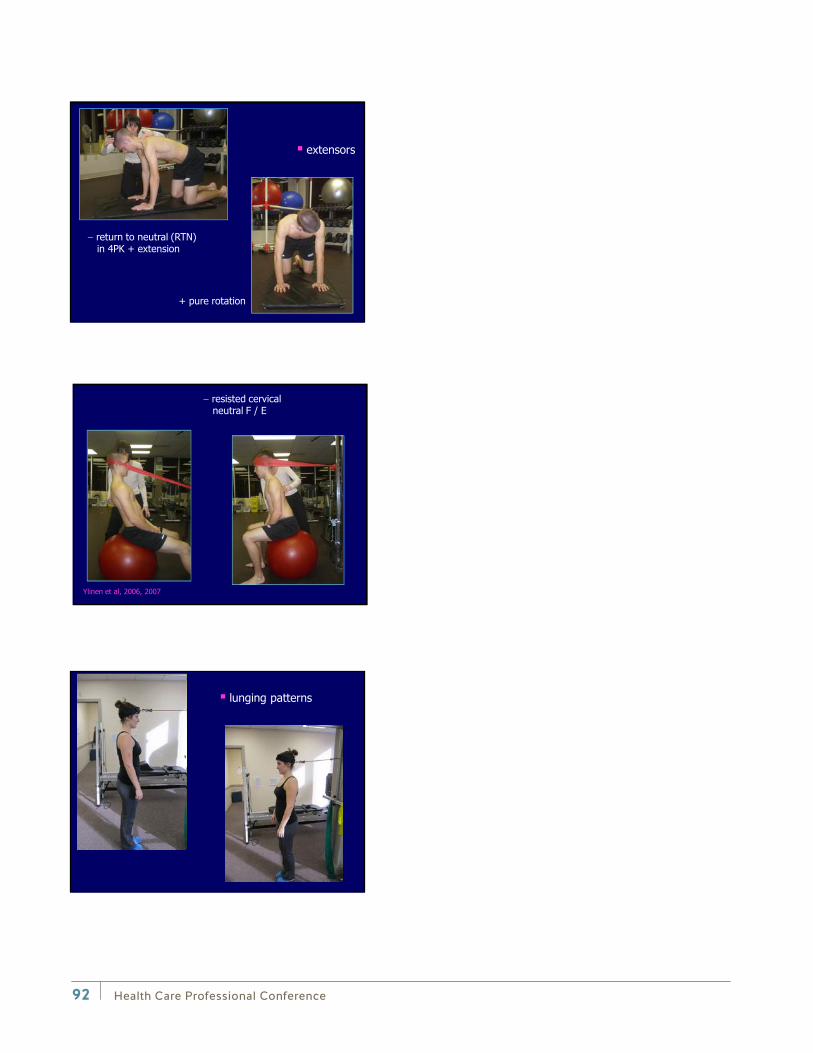
−
−
−
−
−
−
−
−
−
−
−
−
−
−
−
−
−
−
Health Care Professional Conference92

Health Care Professional Conference 93
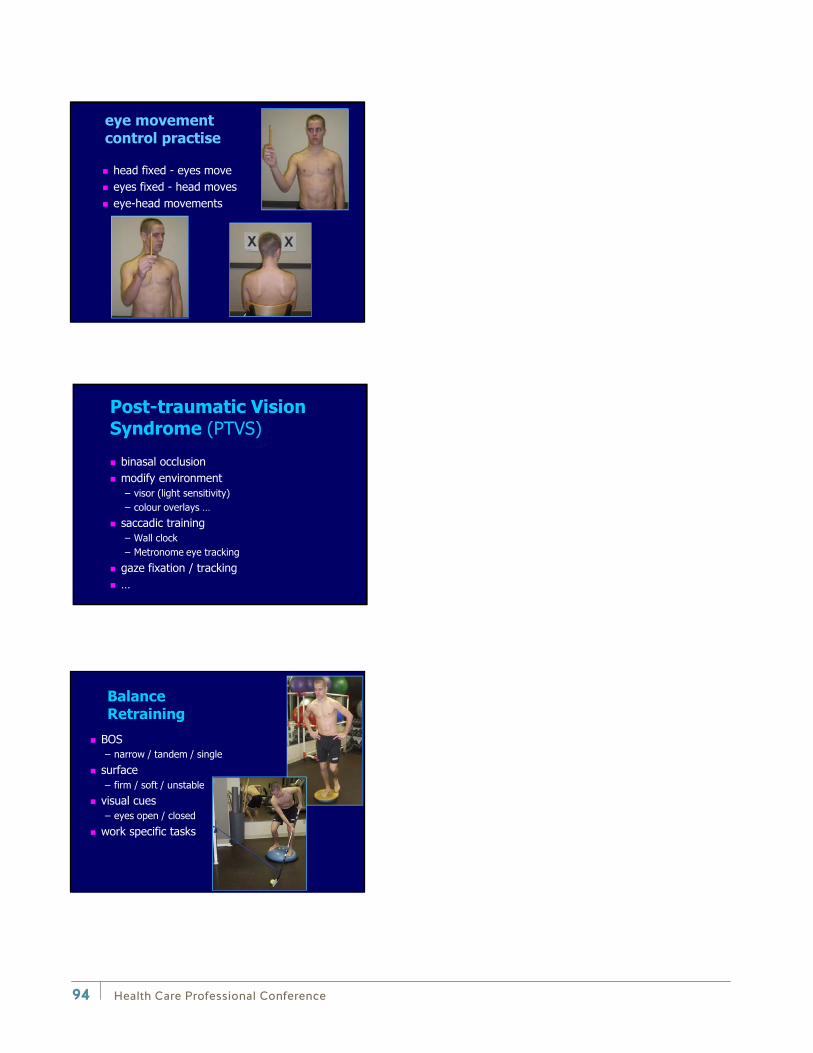
Health Care Professional Conference94
↓
↓
↓
Health Care Professional Conference 95

↓
↓
Health Care Professional Conference96

Health Care Professional Conference 97
Andrew Montgomerie
Andrew Montgomerie has been with Health Care Services at WorkSafeBC since 2004. Prior to that, Andrew worked in Vancouver as a kinesiologist, focused primarily on occupational rehabilitation and functional assessment. Andrew is currently the Director of Financial Services and Health Care Programs at WorkSafeBC. In his spare time, Andrew enjoys playing with his four children, and is working on achieving an accounting designation (CMA).
Plenary session: Opening remarks

Notes
Health Care Professional Conference98
Health Care Professional Conference 99
Dr. Gurdeep Parhar
Dr. Gurdeep Parhar is Executive Associate Dean — Clinical Affairs for UBC’s Faculty of Medicine. He has also served as Associate Dean, Equity and Professionalism, for UBC’s Faculty of Medicine and as Acting Associate Vice-President, for UBC’s Equity and Inclusion Office. Previously, he was Co-Acting Head and Associate Head of the UBC Department of Family Practice.
Dr. Parhar is Medical Director of CORE Occupational Health Centre providing Independent Medical Examinations (IME) in the field of Disability Medicine, Functional Capacity Evaluations (FCE), and Cost of Future Care (CFC) assessments. He provides consultation services to assist in the rehabilitation of injured or ill workers. In this capacity, he serves as the Medical Director of numerous corporations in British Columbia.
Dr. Parhar was a Medical Advisor at WorkSafeBC for five years and was the first Medical Coordinator for the BC Workers Compensation Appeal Tribunal (WCAT) for nine years, before retiring from this position in February 2014.
He teaches extensively in the areas of impairment, disability, occupational medicine, and the management of motor vehicle collision injuries at the Faculty of Medicine at UBC. He also created and teaches a course on Physical Aspects of Medical Disability at Simon Fraser University in a diploma program for case managers and disability managers. At the University of British Columbia, he created and taught a course entitled “Medical Aspects of Disability”, a mandatory course in the Masters of Vocational Rehabilitation Counseling Program.
He was the Occupational Physician for the City of Vancouver where he was responsible for reviewing the health of injured and ill workers in the various departments of the City of Vancouver including the City of Vancouver Fire Department, Parks and Recreation, and Engineering Department.
Dr. Parhar has served as the Occupational Physician for the Workplace Health and Safety (WHS) Program at the University of British Columbia. He is also a Marine Medical Examiner certified by Transport Canada and determined fitness to work for all seafarers who work in the marine industry. In addition, Dr. Parhar is currently the Chairperson of the Royal Canadian Mounted Police (RCMP) Medical Review Board.
He also co-hosts a weekly television program entitled “Pearls for Success”, targeting the well-being of new Canadians.
In 2010, Dr. Parhar was awarded the Trial Lawyers Association of British Columbia (TLABC) President’s Award and the BC College of Family Physicians’ Teacher of the Year Award. In 2011, Dr. Parhar was awarded a UBC Killam Teaching Prize and the University of Calgary’s, Faculty of Medicine Alumnus of Distinction Award. In 2012, Dr. Parhar made the key note address to the Medical University of Vienna entitled “Diversity — Recruiting, Supporting and Promoting Excellence”. In July 2013, Dr. Parhar was invited as a visiting professor to teach Professionalism in Saigon Medical School Vietnam.
Breakout session: The Do’s and Don’ts of Engaging a Family Physician in a Return-to-Work Plan
Health Care Professional Conference100
Learning objectives:
• To understand the role of the family physician in managing injured workers’ situations
• To understand the advantages of the longitudinal and contextual family physician-patient relationship to the injured worker
• To be aware of common errors made by the case managers and rehabilitation communities when attempting to engage family physicians
• To learn strategies on how best to communicate and thereby engage family physicians

Dr. Gurdeep ParharExecutive Associate Dean
Clinical Affairs Faculty of Medicine [email protected]
CORE Occupational Medical CentreIndependent Medical Examinations (IME)Functional Capacity Evaluations (FCE)Cost of Future Care (CFC)604.525.8604coremedicalcentre.com
The Do’s and Don’ts of Engaging a
Family Physician in a
Return-To-Work Plan
Top Difficult Family Doctor Situations(as reported to me by Health Professional Colleagues in the past 20 years)
1. The family doctor is not approving my rehabilitation plan.2. The family doctor is not approving my gradual return to
work plan.3. The family doctor is not sending my client for the
appropriate investigation –MRI4. The family doctor is not referring my patient to the
appropriate specialist5. The family doctor is missing the real diagnosis
Top 10 Difficult Family Doctor Situations(as reported to me by Health Professional Colleagues in the past 20 years)
6. The family doctor is not initiating the correct medication/treatment.
7. The family doctor will not meet with me or speak to me on the telephone.
8. I cannot find a family physician willing to accept my client into their practice.
9. The family doctor is refusing/delayed in responding to requests for copy of clinical records or form.
Health Care Professional Conference 101
10. The family doctor is not willing to offer an opinion as to future treatment and need for assistive devices and aids.
11. The family doctor is not appreciating or documenting the extent of my client’s injuries.
Top 10 Difficult Family Doctor Situations(as reported to me by Health Professional Colleagues in the past 20 years)
Learning objectives
• To understand the role of the family physician in managing injured workers’ situations
• To understand the advantages of the longitudinal and contextual family physician-patient relationship to the injured worker
• To be aware of common errors made by the case managers and rehabilitation communities when attempting to engage family physicians
• To learn strategies on how best to communicate and thereby engage family physicians
Outline
Family Practice Opportunities in Work Injuries
Family Practice Challenges in Work Injuries
Pearls for Dealing with the Family Physician
Health Care Professional Conference102

Family Practice Opportunities in Injured Worker Situations
• The Canadian College of Family Physicians of Canada has defined the following four principles of Family Medicine:
① The family physician is a skilled clinician.② Family medicine is a community-based discipline.③ The family physician is a resource to a defined
practice population.④ The patient-physician relationship is central to the
role of the family physician.
http://www.cfpc.ca/English/cfpc/about%20us/principles/default.asp?s=1
① The family physician is a skilled clinician
• demonstrate competence in the patient-centred clinical method
• develop a comprehensive approach to the management of disease and illness in patients and their families.
• are adept at working with patients to reach common ground on the definition of problems, goals of treatment, and roles of physician and patient in management.
• have an expert knowledge of the wide range of common problems of patients in the community, and of less common, but life threatening and treatable emergencies in patients in all age groups.
Family Physicians...
② Family medicine is a community-based discipline
• Family practice is based in the community
• Clinical problems presenting to a community-based family physician are not pre-selected and are commonly encountered at an undifferentiated stage.
• The family physician may care for patients in the office, the hospital, other health care facilities, or the home.
Health Care Professional Conference 103

③ The family physician is a resource to a defined practice population
• view their practice as a “population at risk”, and organize the practice to ensure that patients’ health is maintained whether or not they are visiting the office.
• have effective strategies for self-directed, lifelong learning.
• have the responsibility to advocate public policy that promotes their patients’ health.
• accept their responsibility in the health care system for wise stewardship of scarce resources.
• consider the needs of both the individual and the community.
Family Physicians...
④ The patient-physician relationship is central to the role of the family physician
• have an understanding and appreciation of the human condition, especially the nature of suffering and patients’ response to sickness.
• respect the privacy of the person.
• provide continuing care to their patients.
Family Physicians...
• Rather than intermittent “snap shots” from which specialist colleagues are forced to understand the patient, the family physician has the luxury of frequent visits over a greater length of time.
• The very scope of family practice – focusing on breadth and not depth – compels the family physician to recruit the assistance of other health professionals in managing the patient’s complete care.
• Thus the family physician is perfectly poised to provide the comprehensive, longitudinal, multidisciplinary and community based care that these patients require.
Family Practice Opportunities in Work Injury Situations:
Health Care Professional Conference104
Family Practice Challenges in Work Injury Situations:
• Despite the potential opportunities that family physicians have in dealing with patients with complex injuries, very often these opportunities are not taken advantage of due to significant challenges.
• Perhaps the main impediment faced by family physicians is that of time.
It is very difficult interviewing, examining, diagnosing and managing a patient within a family practice appointment time allotment.
Many family physicians either rush or outright refuse to manage patients with complex injuries.
Many family physicians resent the time required to complete forms, write reports, attend conferences, interact with other health professionals, and communicate with case managers/legal representatives.
• Some family physicians feel frustration at not being able to access the appropriate resources needed to properly manage complicated patients.
• There are family physicians that feel animosity towards the Work Safe BC and some are even cynical of their own patients’ motivation with respect to work injuries.
• This notion is supported by various negative experiences: Patients whose recovery course does not follow the expected
trajectory Advocates/Case Managers that ask for additional details The “system” provides independent medical examination reports
challenging the patients’ disability and credibility.
Family Practice Challenges in Work Injury Situations:
Pearls for Health Professionals on Dealing with the Family Physician in Injured
Worker Situations
DO NOT:1) Show up at my office unexpectedly2) Show up in the examination room with my patient, without my
prior approval3) Ask me for medical information when you have not attached or
pre-forwarded a signed consent from the patient4) Ask me for medical diagnoses when you do not need them5) Ask me for medical diagnoses repeatedly6) Ask me to complete unnecessary lengthy forms7) Ask me for medical limitations when you really want restrictions
or vice versa8) Send the same form 3 times –via patient, via fax, via mail9) Ask for forms to be completed without a mechanism for payment10) Ask me to arrange a medical service that is not
covered/approved or the patient has no way of covering
Health Care Professional Conference 105

Pearls for Health Professionals on Dealing with the Family Physician in Injured
Worker Situations
DO:1) Send simple/short forms2) Use, for doctors that do not respond, consider “silence means
approval” strategy forms3) Offer suggestions when you think we need to go in a different
direction4) Tell me what you can provide for the patient5) Tell me what you will lobby/advocate for, pending my
approval6) Send subsequent referral forms/authorizations for treatment
with the patient –eg. Active Rehab Program
Pearls for Health Professionals on Dealing with the Family Physician in Injured
Worker Situations
• Enhancing Communication is the single most important strategy in dealing with family physicians in complex medical legal cases. Some specific suggestions include:
1) Communicate Conveniently 2) Communicate Early3) Communicate Helpingly4) Communicate Exploringly5) Communicate Clearly
1) Communicate Conveniently
• The biggest challenge with busy family physicians is finding time to address administrative/paper work.
• When having to communicate volumes of material, it is best to send it in hard copy format by courier or mail.
• Ask the medical office assistant if the physician uses any form of encrypted electronic communication method
• When a written letter or report is not necessary, try to obtain medical information verbally.
• For a telephone consultation, pre-arrange an appropriate time with the medical office assistant
Health Care Professional Conference106
2) Communicate Early
• When you first become involved it is important that a letter be sent to the family physician as soon as possible.
• When requesting a report, meeting or attendance at ameeting, giving ample advanced notice respects the physician’s time and office resources required to complete the report and to alter scheduled patients.
• An early informal “fireside chat” with the family physician is often very valuable
• If the family physician does not understand the full array and severity of the patient’s symptoms you should remind your client to be very careful and detailed when visiting the family physician.
3) Communicate Helpingly
• One of the best methods to improve and solidify the relationship with the family physician is to offer them assistance with their management of the patient.
• If you can advocate for medical imaging, psychological assessments, medical assessments, or expedited surgery, offer it to the family physician.
• Communicate this offer of assistance verbally, by telephone or fax and ask the family physician to have the appropriate referral form faxed.
4) Communicate Exploringly
• Animosity between health professionals and family physicians usually arises from misunderstandings.
• The easiest method to avoid this disastrous situation is to have a telephone conversation with the family physician to explore how well their client’s injuries are understood to ensure that important pathology is not being overlooked.
Health Care Professional Conference 107
5) Communicate Clearly
• When requesting medical clearance, approval of programs or approval of a return to work plan, ensure that your documents are as concise and clear as possible.
• As noted, the family physician has extensive knowledge of the patient’s biological-psychological-social context. If this is important to your case, ask.
Conclusion
There are few more terrifying things in life than having to recover from complex and serious injuries.
Patients struggling with long rehabilitation programs, multiple health professionals, insurance companies, financial stresses, family turmoil, and social isolation reach out to the two people they feel will get them through this difficult time: all of the clinicians need to work together. manage the treatment plan.
It is crucial that communication between the patient’s therapists andphysician be ideal.
Learning objectives
To understand the role of the family physician in managing injured workers’ situations
To understand the advantages of the longitudinal and contextual family physician-patient relationship to the injured worker
To be aware of common errors made by the case managers and rehabilitation communities when attempting to engage family physicians
To learn strategies on how best to communicate and thereby engage family physicians
Health Care Professional Conference108

It is all about accurate communication…
• I would be happy to discuss or assist you with any challenging situation –at no cost to you or your client.
• Thank you for being such an important part of the recovery of injured workers.
Health Care Professional Conference 109

Notes
Health Care Professional Conference110
Health Care Professional Conference 111
Jessica Vliegenthart
In 2004, five days before her 21st birthday, Jessica Vliegenthart broke her back while working as a forest firefighter in the Northwest Territories, leaving her a paraplegic.
Following the accident, Jessica completed her undergraduate degree in communications from Simon Fraser University in 2008 and her law degree from the University of Victoria in 2011.
Always an athlete, Jessica competed for Canada in wheelchair basketball from 2007 to 2012, retiring after competing at the London 2012 Paralympics. Jessica is now a lawyer specializing in personal injury (plaintiff) law and is happiest when she is in the role of advocate. She’s also passionate about adapted sport and helping those with mobility impairments get playing again. Jessica is the president and co-founder, along with her husband Jon, of the Kamloops Adapted Sports Association which offers wheelchair basketball, wheelchair tennis, and handcycling to residents of the Thompson Okanagan.
Plenary session: Empowering Workers to Empower Themselves

Health Care Professional Conference112

Notes
Health Care Professional Conference 113

Notes
Health Care Professional Conference114
Health Care Professional Conference 115
WorkSafeBC Mental Health Claims Unit Panel
The Mental Health Claims Unit (MHCU) is a 30 member team, comprised of adjudicative, support, and clinical staff. It is responsible for adjudicating and managing WorkSafeBC claims where the sole injury is psychological. The MHCU was created in response to expanded coverage for mental disorder claims following the passage of Bill 14 into law on July 1, 2012. Members of the MHCU include Dr. David Eveleigh, Damian Gorman, Abha Sharma McDonell, Jason Jang, and Scott Brent.
Scott Brent, Client Services ManagerScott joined the MHCU as a client services manager in February 2014. He previously worked as a review officer in the Review Division and with the Fair Practices Office at WorkSafeBC. He holds a law degree from UBC.
Dr. David Eveleigh, Senior Psychology AdvisorDr. Eveleigh is one of the MHCU’s senior psychology advisors. He obtained his doctoral degree from SFU and has worked as a psychologist at WorkSafeBC since 1995, initially in the Rehabilitation Centre before moving to Clinical Services. He has been with the MHCU since its inception in 2012.
Damian Gorman, Case ManagerDamian is an occupational therapist and past WorkSafeBC service provider for multiple health care services including FCE, RTWSS, COT, OR2, HIATS, MARP and CMPA. He recently joined the MHCU as a case manager.
Jason Jang, Vocational Rehabilitation ConsultantJason has been a vocational rehabilitation consultant with WorkSafeBC since 2006 and joined the MHCU two years ago. Jason holds a degree in Human Kinetics in addition to his RRP.
Abha McDonell, Return-to-Work Specialist NurseAbha is a RTW specialist-nurse that currently supports the MHCU. She has been with WorkSafeBC for over eight years and brings with her over 11 years of experience working in acute psychiatric care and public health care teaching.
Breakout session: Life of a Claim — How Law and Policy Affects the Decision-Making Process in the Mental Health Claims Unit
From left back row: Scott Brent, Dr. David Eveleigh, Damian Gorman, Jason Jang; Front row: Abha McDonell

Learning objectives:
• To improve the understanding of the collaborative process between the various members of the mental health claims unit to effect early, durable and safe return to work.
• To explore and understand the life of a claim including the various paths that can be taken and the impact on the injured worker
• To increase awareness of the impact that the new legislation and policy has had on the decision-making process
Health Care Professional Conference116
WorkSafeBC Mental Health Claims Unit Panel Discussion 10th Annual Health Care Professional Conference
September 12, 2014
Life of a Claim
How Law & Policy Affects the Decision-Making Process
Introduction to the Team
A Brief History – Mental Health Claims Unit (MHCU)
• MHCU took effect on July 1, 2012.
• On July 3, 2012, a Centralized Richmond Team began to adjudicate and manage mental disorder claims.
• 6 Case Managers initially (now expanded to 15), with case loads aligned by major employer versus geography.
• Clinical support includes psychologists, physicians, nurse advisors and mental health specialists.
3
Health Care Professional Conference 117
Changes to the Legislation Section 5.1 of the Workers Compensation Act
• Under Bill 14, a worker may be entitled to compensation only if the mental disorder:
• is a reaction to one or more traumatic events arising out of and in the course of the worker’s employment; or
• is predominantly caused by a significant work-related stressor, or a cumulative series of significant work-related stressors, arising out of and in the course of the worker’s employment.
4
Additional Amendments Section 5.1 of the Workers Compensation Act
• Other key changes: • Replaced mental stress with mental disorder
• Replaced references to physician with psychiatrist or psychologist
• Included a definition of psychiatrist and psychologist
• Included bullying or harassment as an example of a significant work-related stressor
5
Section 5.1(1)(c) Exclusion Decisions of the Employer Examples in Legislation and WorkSafeBC’s policy: • a decision to change the work to be performed or the working
conditions
• to discipline the worker
• to terminate the worker’s employment
• decisions of the employer relating to workload and deadlines, work evaluation, performance management, transfers, changes in job duties, lay-offs, demotions and reorganizations
6
Health Care Professional Conference118

A collaborative and team based approach to adjudication and claim
management
Adjudication and Case Management Model • Only basic information taken when claim first registered.
• CM completes a comprehensive worker history interview.
• RTW Nurse Advisor is engaged to explore return to work opportunities even before claim is accepted.
• Early use of RTW NA and VRC allows CM to focus on claims management issues.
Taking a Proactive Approach
8
Adjudication and Case Management Model • New psych assessment contract stipulates 10 days turn-around
time (from date assessment is booked to report received)
• This assessment is reviewed by the CM with the assistance of a Senior PA in a team meeting setting.
• Both the Sr. PA and Board MA will provide guidance on the appropriateness of any treatment recommendations made, including medication or therapy.
Clinical Support
9
Health Care Professional Conference 119
Regular Team Meetings Charting a Recovery and RTW Strategy • Team meetings are held twice weekly. In attendance are:
• Case Manager
• Vocational Rehabilitation Consultant
• Return to Work Nurse Advisor
• Mental Health Specialist
• Sr. Psychology Advisor and Board Medical Advisor
• Case Manager Supervisor and Client Services Manager
• Recovery and RTW are explored simultaneously. All individuals present bring their specific skills and role to the table.
10
Regular Team Meetings Monitoring Progress & Supporting the Worker • Early Vocational Rehabilitation Consultant (VRC) involvement:
• No expectation that worker RTW where workplace or duties are unsafe or deemed unsuitable
• Early intervention to improve successful & durable RTW.
• Encourages the worker to start thinking about a RTW as part of their recovery, and not a separate phase or stage.
• MHS evaluates workers that self-identify as being fragile or express suicidal ideation. Completes a risk assessment and, where necessary, refers for CIR or to community resources.
11
Adjudication Process Map
12
Health Care Professional Conference120
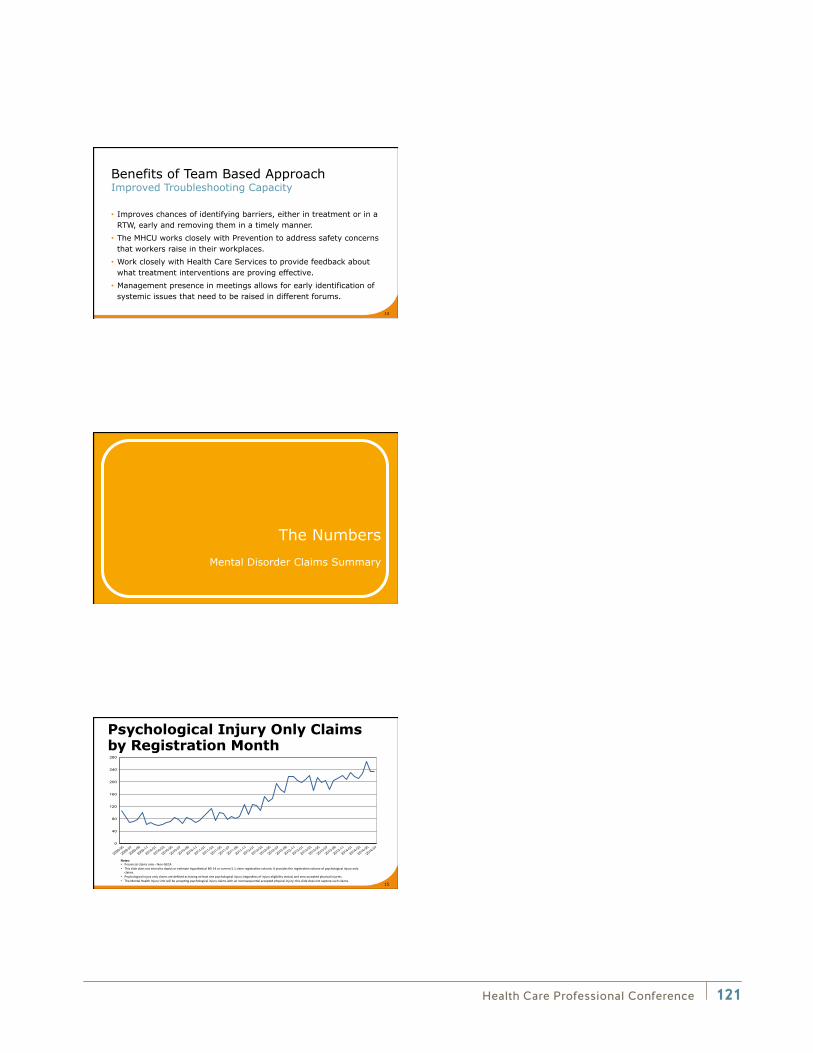
Benefits of Team Based Approach Improved Troubleshooting Capacity
• Improves chances of identifying barriers, either in treatment or in a RTW, early and removing them in a timely manner.
• The MHCU works closely with Prevention to address safety concerns that workers raise in their workplaces.
• Work closely with Health Care Services to provide feedback about what treatment interventions are proving effective.
• Management presence in meetings allows for early identification of systemic issues that need to be raised in different forums.
13
The Numbers
Mental Disorder Claims Summary
Psychological Injury Only Claims by Registration Month
15
• •
• •
0
40
80
120
160
200
240
280
2009-05
2009-07
2009-09
2009-11
2010-01
2010-03
2010-05
2010-07
2010-09
2010-11
2011-01
2011-03
2011-05
2011-07
2011-09
2011-11
2012-01
2012-03
2012-05
2012-07
2012-09
2012-11
2013-01
2013-03
2013-05
2013-07
2013-09
2013-11
2014-01
2014-03
2014-05
2014-07
Psychological Injury Only Claims by Registration Month
Health Care Professional Conference 121
Health Care and Social Services (7660) 1,336 26.68%
Transportation and Related Services (7320) 559 11.16%
Retail (7410) 445 8.89%
Accommodation, Food, and Leisure Service (7610) 406 8.11%
Public Administration (7530) 297 5.93%
Education (7650) 289 5.77%
Business Services (7620) 246 4.91%
Other Services (not elsewhere specified) (7640) 225 4.49%
Deposit Sector 11 (formerly Class 13) (8411) 165 3.30%
General Construction (7210) 140 2.80%
Wood and Paper Products (7140) 106 2.12%
Metal and Non-Metallic Mineral Products (7120) 94 1.88%
Professional, Scientific, & Tech Service (7630) 75 1.50%
Wholesale (7420) 53 1.06%
Food and Beverage Products (7110) 44 0.88%
Road Construction or Maintenance (7230) 44 0.88%
Other 259 5.17%
Not Specified (9999) 224 4.47%
MHCU Claims – Top Subsectors Claims registered July 1, 2012 – July 31, 2014 Subsector Count Percent
16
Acute Care (766001) 410 30.69%
Long-Term Care (766011) 226 16.92%
Ambulance or First Aid Services (766004) 151 11.30%
Counselling or Social Services (766007) 147 11.00%
Community Health Support Services (766006) 145 10.85%
Residential Social Service Facility (766017) 92 6.89%
Short-Term Care (766019) 30 2.25%
Life and Job Skills Training (766010) 27 2.02%
Medical Clinic or Medical Practice (766015) 22 1.65%
Retirement or Seniors' Home (accom only) (766018) 21 1.57%
Dentistry or Ancillary Dental Services (766008) 18 1.35%
Alcohol or Drug Treatment Centre (766002) 15 1.12%
Religious Organization (766016) 11 0.82%
Physiotherapy or Occupational Therapy (766014) 6 0.45%
Optometry (766013) 5 0.37%
Other 10 0.75%
MHCU Claims – Health Care Subsector
17
Claims registered July 1, 2012 – July 31, 2014 CU Count Percent
Allowed 747 14.92%
Disallowed 2,263 45.20%
No adjudication required 373 7.45%
Pending 307 6.13%
Rejected 27 0.54%
Suspended 1,290 25.76%
MHCU Claims – Eligibility Decisions
18
Claims registered July 1, 2012 – July 31, 2014
Claim Eligibility Decision Count Percent
Health Care Professional Conference122
Claim Scenarios
Scenario
• A manager in a retail store reports what she describes as a campaign of harassment by the new district manager (DM) since the latter’s appointment six months earlier.
• A detailed history is taken by the CM. The worker does not report any abusive or threatening behaviour, but indicates that she is having trouble sleeping and focusing because her continued employment is under review by the DM for the next 3 months.
• The manager describes feeling singled out and targeted by her DM for bi-weekly meetings. The meetings are tense and unfriendly, but there is no yelling or swearing or other abusive conduct.
20
Scenario Continued
• Both the worker and the employer agree that the subject-matter of the meetings is limited to the manager’s team’s sales, salary and overtime costs, its absenteeism and its contribution to corporate profits.
• The employer denies the manager has been singled out and says that she is one of three managers who receive “regular performance coaching” because their teams are performing below expectations.
• The DM acknowledges that the worker is exhibiting signs of being under intense pressure, but says the “coaching” sessions are necessary to ensure the success of the manager’s team.
21
Health Care Professional Conference 123

Questions & Answers
Health Care Professional Conference124
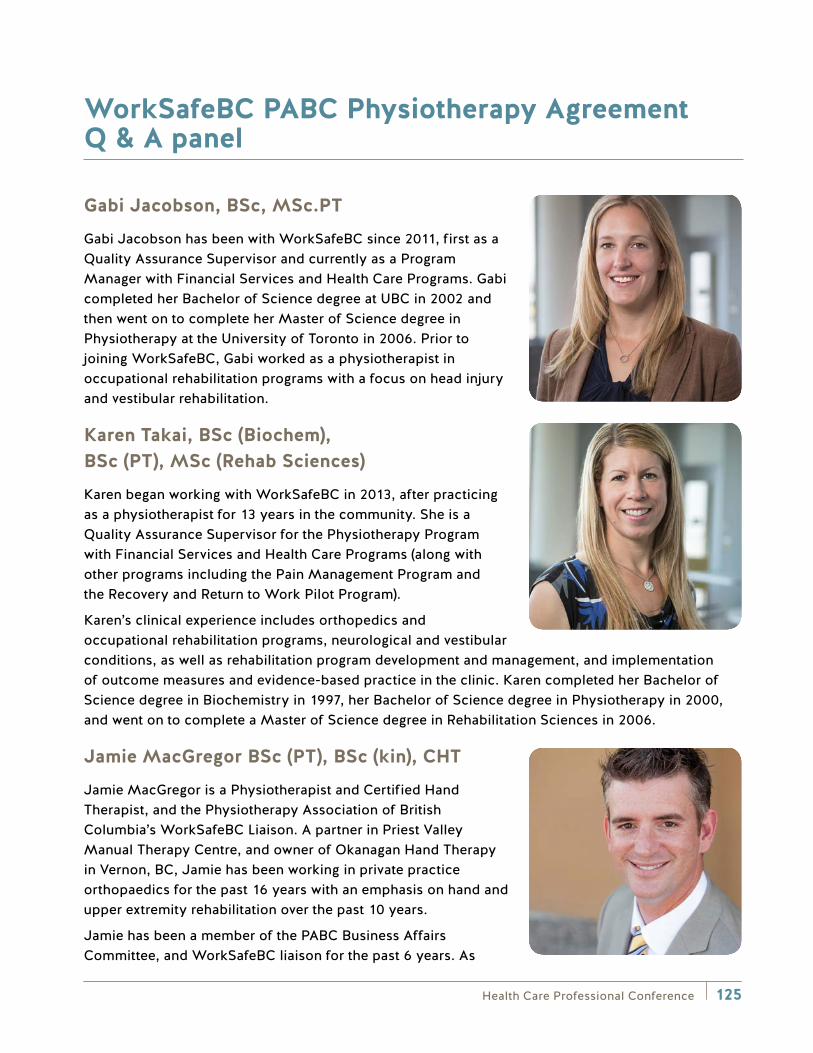
Health Care Professional Conference 125
WorkSafeBC PABC Physiotherapy Agreement Q & A panel
Gabi Jacobson, BSc, MSc.PT
Gabi Jacobson has been with WorkSafeBC since 2011, first as a Quality Assurance Supervisor and currently as a Program Manager with Financial Services and Health Care Programs. Gabi completed her Bachelor of Science degree at UBC in 2002 and then went on to complete her Master of Science degree in Physiotherapy at the University of Toronto in 2006. Prior to joining WorkSafeBC, Gabi worked as a physiotherapist in occupational rehabilitation programs with a focus on head injury and vestibular rehabilitation.
Karen Takai, BSc (Biochem), BSc (PT), MSc (Rehab Sciences)
Karen began working with WorkSafeBC in 2013, after practicing as a physiotherapist for 13 years in the community. She is a Quality Assurance Supervisor for the Physiotherapy Program with Financial Services and Health Care Programs (along with other programs including the Pain Management Program and the Recovery and Return to Work Pilot Program).
Karen’s clinical experience includes orthopedics and occupational rehabilitation programs, neurological and vestibular conditions, as well as rehabilitation program development and management, and implementation of outcome measures and evidence-based practice in the clinic. Karen completed her Bachelor of Science degree in Biochemistry in 1997, her Bachelor of Science degree in Physiotherapy in 2000, and went on to complete a Master of Science degree in Rehabilitation Sciences in 2006.
Jamie MacGregor BSc (PT), BSc (kin), CHT
Jamie MacGregor is a Physiotherapist and Certified Hand Therapist, and the Physiotherapy Association of British Columbia’s WorkSafeBC Liaison. A partner in Priest Valley Manual Therapy Centre, and owner of Okanagan Hand Therapy in Vernon, BC, Jamie has been working in private practice orthopaedics for the past 16 years with an emphasis on hand and upper extremity rehabilitation over the past 10 years.
Jamie has been a member of the PABC Business Affairs Committee, and WorkSafeBC liaison for the past 6 years. As
Health Care Professional Conference126
PABC-WorkSafeBC liaison Jamie works with physiotherapists and WorkSafeBC officers in addressing treatment model concerns, developing stronger relationships between physiotherapists and WorkSafeBC, and developing new treatment models for injured workers. Jamie has been very involved in the development, negotiations, and roll-out of the new Physiotherapy Treatment Services model with PABC and WorkSafeBC, and continues in his role as liaison to work on helping the model evolve.
Breakout session: Physiotherapy Agreement Q&A Panel Informal Session (Optional)

Notes
Health Care Professional Conference 127

Notes
Health Care Professional Conference128

Thank you to all conference sponsors, exhibitors, and attendees for your support of the conference.
Health Care Professional Conference 129
HealthCare
Better care for a better life
People with serious injuries often need a variety of health care services – attendant care and nursing for their daily needs and physiotherapy and other rehabilitative services to make the best possible recovery.
Bayshore Home Health and Bayshore Therapy & Rehab, the newest addition to the trusted Bayshore brand of health care offerings, can provide professional services in both areas.
A single source for your clients’ home care and rehab needs
Contact us today to learn more
1.877.289.3997 / www.bayshore.ca
For more information visit us:backinmotion.com
Helping people Work. Helping people Live.
We offer:Treatment Services
Assessment Services
Employment Services
Consulting Services
Back in Motion offers individualized
assessment and rehabilitation
programs since 1993
Chronic Pain Management Psychological Trauma and
Post Traumatic Stress Disorder (PTSD)
Medication (opioid) Management
Return-to-work Functional and Medical-legal
Assessments
Psychology Assessments and Counselling
Occupational Rehabilitation Work Conditioning Brain Injury Rehabilitation Community Occupational
and Physical Therapy Vocational Rehabilitation
“A shadow of darkness lifted from my mind. I received my family back in the nick of time. To say Thank You
underestimates the change you have all given me.”
Canmore client
Unlocking the potential in people
www.orionhealth.ca
Our Programs and Services
Partnering with you to keep workers in B.C. healthy.
Find valuable resources for health care professionals at worksafebc.com.














![0037-7856(75)90182-1] Lawrence G. Miller -- Negative Therapeutics (1)](https://static.fdocuments.net/doc/165x107/577cd7f81a28ab9e78a01e9d/0037-78567590182-1-lawrence-g-miller-negative-therapeutics-1.jpg)


