
2012 SNS Program Coordinator Meeting - acgme
35
1 Accreditation Council for Graduate Medical Education Neurosurgery Program Coordinator Workshop Pamela L. Derstine, PhD, MHPE Executive Director Atlanta, Georgia May 18, 2012 Accreditation Council for Graduate Medical Education Neurosurgery Program Coordinator Workshop Session 1: What’s New at ACGME?
Transcript of 2012 SNS Program Coordinator Meeting - acgme

1
Accreditation Council for Graduate Medical Education
Neurosurgery Program Coordinator Workshop
Pamela L. Derstine, PhD, MHPE Executive Director
Atlanta, GeorgiaMay 18, 2012
Accreditation Council for Graduate Medical Education
Neurosurgery Program Coordinator Workshop
Session 1:What’s New at ACGME?

2
Overview
• Department of Accreditation Services
• RRC Update
• Program Requirements
• Case Log System
• Announcements
DAS Reorganization

3
Department of Accreditation Services
• Surgical SectionJohn R. Potts III, MD, Senior Vice President Derstine Team: Colon & Rectal Surgery;
Neurological Surgery; Orthopaedic Surgery; Otolaryngology
Johnston Team: Obstetrics & Gynecology; Committee of Review Committee Chairs
Levenberg Team: Ophthalmology; Urology
Simpson Team: Plastic Surgery; General Surgery; Thoracic Surgery
Department of Accreditation Services
• Medical SectionMary Lieh-Lai, MD, Senior Vice President Anthony Team: Dermatology; Family Medicine
Fischer Team: Pediatrics; Physical Medicine & Rehabilitation
King Team: Allergy & Immunology; Neurology; Psychiatry
Vasilias Team: Internal Medicine

4
Department of Accreditation Services
• Hospital-based SectionLouis J. Ling, MD, Senior Vice President Lewis Team: Anesthesiology; Preventive
Medicine; Transitional Year
Meyer Team: Diagnostic Radiology; Emergency Medicine; Nuclear Medicine
Thorsen Team: Medical Genetics; Pathology; Radiation Oncology
Derstine Team
• Pamela L. Derstine, PhD, MHPEExecutive Director(312) 755-5083 – [email protected]
• Susan ManskerAssociate Executive Director(312) 755-5028 – [email protected]
• Jennifer LunaAccreditation Administrator(312) 755-5036 – [email protected]
• Deidra WilliamsAccreditation Assistant(312) 755-5055 – [email protected]

5
Review Committee Members
• H. Hunt Batjer, MDChair
• Kim J. Burchiel, MDVice Chair
• Ralph G. Dacey, Jr. MD(Term ends 6/30/12)
• Alexander A. Khalessi, MD, MS (Resident)(Term ends 6/30/12)
• Nelson M. Oyesiku, MD, PhD• A. John Popp, MD• Volker K.H. Sonntag, MD
(Term ends 6/30/12) • Patrice Blair, MPH
Ex-Officio (ACS)• Fredric Meyer, MD
Ex-Officio (ABNS)
New Members as of July 1, 2012 • Nicholas M. Barbaro, MD• Michael Sean Grady, MD• Melanie G. Hayden Gephart, MD (Resident)
Upcoming RRC Meetings
• June 28-30, 2012 Agenda closed April 20, 2012
• January 18-19, 2013 (tentative) Agenda closing date November 9, 2012
• June 28-29, 2013 (tentative) Agenda closing date April 19, 2013

6
April Newsletter
• Photos!
• Statistics!
• Reminders!
• Announcements!
Program Requirements

7
Duty Hour Requirements Update
Duty Hour requirements for PGY1 residents:
80 hours/week
1 day off in 7
Maximum duty period 16 hours
8-10 hours between duty periods
No home call
No in-house call (does not include night float or regularly scheduled overnight duties)
No moonlighting
No duty hour exception
Duty Hour Requirements Update
Duty Hour requirements for PGY2 residents:
80 hours/week (DHE allowed)
1 day off in 7
Maximum duty period 24+4 hours
8-10 hours between duty periods
In-house call no more than 1 day in 3

8
Duty Hour Requirements Update
Duty Hour requirements for PGY3 and above residents:
80 hours/week (DHE allowed)
1 day off in 7
Maximum duty period 24+4 hours
< 8 hours between duty periods allowed
In-house call no more than 1 day in 3
Duty Hour Requirements Update
• New specialty-specific requirements/FAQs added February 2012:VI.D.1 Supervision (FAQ)
VI.E. Clinical Workload (PRs and FAQs)
VI.F. Teamwork (FAQ)

9
VI.D.1 Supervision (FAQ)
Q. Are there any situations in which residents may be supervised by non-neurosurgical licensed independent practitioners?
A. In certain learning environments such as the neuro-intensive care unit (ICU), a properly credentialed and privileged critical care physician may supervise a resident. In the operating room environment, a properly credentialed and privileged anesthesiologist may supervise certain procedures, such as central line placement, arterial line
placement, and endotracheal intubations.
VI.E. Clinical Workload (PRs)
Neurological surgery residents practice across a diversity of care settings with varying degrees of primary patient responsibility. These situations vary from first call cross-coverage on the floors to possible interaction with a primary intensivist, pediatric, or hospitalist service.
Peri-operative inpatient care must be further balanced with resident participation in the operating room. Program directors must consider the following when assigning patient loads:
adequate coverage and provision of patient care;
sufficient inpatient clinical responsibility to allow resident progression along clinical care milestones; and,
meaningful insulation of operative experiences from inpatient care to allow technical progress and facilitate resident development of organizational and triage skills.

10
VI.E. Clinical Workload (FAQs)
Q. What is an appropriate patient load for residents?
A. The program director must make an assessment of the learning environment with input from faculty members and residents. Minimum patient loads should usually be five on the general inpatient unit and four while on clinical neurological surgery services. However, there may be situations in which lower patient loads may be acceptable. Programs will need to justify lower patient loads with evidence such as severity of illness indicators or other factors.
VI.E. Clinical Workload (FAQs)
Q. What would an appropriate patient load be for a chief resident, or a resident in the final transition-to-practice year?
A. The program director must make an assessment of the learning environment with input from faculty members and residents. Residents in the final year of education generally take on more patient care responsibilities than earlier in residency education. Minimum patient loads should usually be 10 on the general inpatient unit, and three in the intensive care unit.

11
VI.F. Teamwork (FAQ)
Q. Who should be included in the interprofessional teams?
A. Advanced practice providers, audiologists, certified registered nurse anesthetists (CRNAs), child-life specialists, nurses, nutritionists, operating room technicians, pharmacists, physical and occupational therapists, physician assistants, psychologists, radiology technicians, respiratory therapists, social workers, and speech and language pathologists are examples of professional personnel who may be part of the interprofessional teams.
Q. Must every interprofessional team include representation from every professional listed above? A. No. The Review Committee recognizes that the needs of specific patients change with their health statuses and circumstances. The Review Committee’s intent is to ensure that the program has access to these professional and paraprofessional personnel, and that interprofessional teams be constituted as appropriate and as needed, not to mandate that all be included in every case/care environment.
Q. What roles must residents have in the interprofessional health care team?
A. As members of the interprofessional health care team, residents must have key roles in diagnostic work-up, operative procedures, treatment decisions, measurement of treatment outcomes, and the communication and coordination of these activities with program faculty members and referring sources.
Major Program Requirement Revision
• Public comment period closes June 21, 2012
http://www.acgme-nas.org/neurological-surgery.html

12
Major Changes
• Program length 84 months (7 years)• Must have ACGME-accredited programs
(anesthesiology neurology and diagnostic radiology): Sponsoring Institution
• Should have ACGME-accredited programs (internal medicine, pediatrics, surgery): primary clinical site or participating site
• Site directors must be ABNS certified• One FTE program coordinator with support from
sponsoring institution
Major Changes
• Resources must include neuroangiography suite with extracranial and intracranial interventional capabilities
• ICU specifically for care of neurological surgery patients (desirable → should)
• Patient care outcomes: defined case categories• Medical knowledge outcomes for treating
specified NS conditions

13
Major Changes
• PGY-1 must include 6 months general patient care (critical care, neurology,
surgery, trauma or other related rotations) Maximum 6 months neurosurgery
• First 36 months must include at least 3 months basic clinical neuroscience and at least 6 months neurocritical care education
• Following PGY1, additional 54 months clinical neurological surgery education includes 21 months at primary clinical site includes 12 months as chief resident (PCS or PS)
• Remaining 18 months used for elective clinical education and/or research
Major Changes
• Resident Experiences must include: participating in surgical, endovascular, interventional,
and radiological procedures recording procedures in ACGME case log system as
assistant resident surgeon, senior resident surgeon, or lead resident surgeon
clinical experience in neuroradiology, including endovascular surgical neuroradiology, and neuropathology designed specifically for neurological surgery residents
• Case log operative data must be reviewed with each resident at least semiannually
• 80% program graduates in past 7 years must take ABNS oral exam
• 80% first-time oral exam takers must pass

14
Case Log System
• Case Log Interface and Reports
• Defined Case Categories/Minimum Numbers
• Resident Roles
• Remapping and Timeline
• Announcements and Resources
Case Log Interface

15
Case Log Features
Case Log Features

16
Case Log Reports
Case Log Reports
• Unique purposes• Filtering reports: Resident (all or specific name) Procedure Resident Year (1-7) Patient Type (all/adult/pediatric) Area Description (current CPT code mapping areas) Resident Year (1-7) Resident Status (all/active/inactive…always use “active”) Credit (all/primary/secondary) Date Range Institution (all or by participating site) Resident Role (all/other/senior clinical year)) Attending (all or by name) RRC Procedure List (all or by specific type within an area)

17
Case Log Reports: Resident Activity
Use this report to answer:• Are residents logging data?• How much data are they logging and with what frequency?• How can I quickly and easily see what residents are doing?
Case Log Reports: Resident Operative
Use this report to answer:• What is the overall experience for (as filtered)?

18
Case Log Reports: Resident Full Detail
Use these reports to answer:• How do I view data on a case-by-case basis?• What are the specifics of each case?• Which codes were claimed for credit?• What are the details of the “unassigned” cases?
Case Log Remapping
• Defined Case Categories and Minimum Numbers Adult Cranial (205)
Adult Spinal (90)
Pediatric (30)
Adult and Pediatric Epilepsy (10)
Critical Care (90)
Total All Defined Case Categories = 425
• See handouts for case category and CPT code mapping details

19
Case Log Resident Roles
Resident must scrub-in (scrub hands, use sterile gloves, with or without gown)
• Assistant Resident SurgeonIncludes positioning, sterile preparation, monitoring devices, microscope preparation, participation in the initial (‘opening’) or final (‘closing’) portions of the case; and/or assisting the resident or staff surgeon(s)
Case Log Resident Roles
Resident must scrub-in (scrub hands, use sterile gloves, with or without gown)
• Senior Resident SurgeonMay include aspects of all of the activities of assistant resident surgeon as well as participation in the surgical procedure between opening and closing

20
Case Log Resident Roles
Resident must scrub-in (scrub hands, use sterile gloves, with or without gown)
• Lead Resident SurgeonMay include aspects of all of the activities of assistant resident surgeon and senior resident surgeon as well as participation in the critical portion of the case
Rules for Claiming a Role
• A resident may claim only one role per case
• There can be only one lead resident surgeon per case
• All cases must be under the direct supervision of attending staff members

21
Timeline for Case Log Revision
• Remapping is underway now
• After all graduating neurosurgery resident cases have been archived, all cases for current residents will be automatically updated to the new category mappings (late September); all current roles updated to senior resident surgeon
• Unarchived cases may be edited at any time
• Opportunity to archive case logs for graduates now open
• Programs may wait until the end of June to begin archiving data
• Residents graduating in 2013 and beyond are expected to demonstrate compliance with defined case category minimum numbers
Announcements
• New information for duty hour exception requests available now on RRC website
• See handout for details

22
Accreditation Council for Graduate Medical Education
Neurosurgery Program Coordinator Workshop
Session 2: Next Accreditation System
Overview
• Background and Rationale
• Program Requirements
• Milestones
• Timeline

23
Background and Rationale
ACGME Mission
We improve healthcare by assessing and
advancing the quality of resident physicians’ education through
accreditation

24
Goals of Accreditation
Ensure:
• the safety and quality of care of the patients under the care of residents today
• the safety and quality of care of the patients under the care of our graduates in their future practice
• the provision of a humanistic educational environment where residents are taught to manifest professionalism and effacement of self interest to meet the needs of their patients
Goals of the Next Accreditation System (NAS)
• Begin the realization of the promise of Outcomes
• Free good programs to innovate
• Assist poor programs to improve
• Reduce the burden of accreditation
• Provide accountability for outcomes (in tandem with ABMS) to the Public

25
Next Accreditation System Basics
• Continuous Accreditation Model – annually updated Based on annual data submitted, other data requested, and
program trends
• Scheduled Site Visits replaced by 10 year Self-Study Visit
• Standards revised every 10 years Standards Organized by
• Core Processes
• Detailed Processes
• Outcomes
Conceptual ChangeThe Current Accreditation System
Rules
Corresponding Questions
“Correct or Incorrect” Answer
Citations and Accreditation Decision
Repeated cycles of:

26
Conceptual Change
“Continuous”
Observations
Assure that the Program Number of Potential Fixed the Problem Related “Rules” Problems
Promote
Innovation
Diagnose
the Problem
(if there is one)!
The Next Accreditation System
Next Accreditation System
Continuous Accreditation
No Cycle Lengths
No PIF!!!!!

27
NAS and Program Requirements
STANDARDS
Core ProcessDetailed Process
Outcomes
InitialAccreditation
New Programs
Core ProcessDetailed ProcessOutcomes
Accreditation with Warning
New Programs,Accredited Programs with Major Concerns
Probationary Accreditation
Core ProcessDetailed ProcessOutcomes
Maintenance ofAccreditation
Accredited Programs without Major Concerns
Maintenance of Accreditation with
Commendation
Core ProcessDetailed ProcessOutcomes
Program Requirements

28
Program Requirements
• Definition of Categories Core Requirements: Statements that define structure, resource,
or process elements essential to every graduate medical educational program.
Detail Requirements: Statements that describe a specific structure, resource, or process for achieving compliance with a Core Requirement. Programs in substantial compliance with the Outcome Requirements may utilize alternative or innovative approaches to meet Core Requirements.
Outcome Requirements: Statements that specify expected measurable or observable attributes (knowledge, abilities, skills, or attitudes) of residents or fellows at key stages of their graduate medical education.
Program Requirement Categories
• Examples for CPRs Core Requirement:
Qualifications of the program director must include:
II.A.3.b) current certification in the specialty by the American Board of
Colon and Rectal Surgery (ABCRS), or specialty qualifications that are acceptable to the Review Committee; and, (Core)
Detail Requirement:The program director must:II.A.4.l) comply with the sponsoring institution’s written policies and
procedures, including those specified in the Institutional Requirements, for selection, evaluation and promotion of residents, disciplinary action, and supervision of residents; (Detail)
Outcome Requirement:Residents are expected to:
IV.A.5.f).(1) work effectively in various health care delivery settings and systems relevant to their clinical specialty; (Outcome)

29
Program Requirement Categories
• Specialty-specific Examples Core Requirement:
IV.A.3.a) Didactic sessions must include teaching conferences, rounds, and other educational activities in which both the neurological surgery faculty members and residents participate. (Core)
Detail Requirement:IV.A.3.a).(1) A majority of staff faculty members and residents must attend these sessions. (Detail)
IV.A.3.a).(2) A conference attendance record for both residents and
faculty members must be maintained. (Detail)
Outcome Requirement:Residents must demonstrate competence in:IV.A.5.a).(2).(a).(vii) assessing post-operative recovery, recognizing and treating complications, communicating with referring physicians, and developing the physician patient relationship; (Outcome)
View PR Category Assignment
http://www.acgme-nas.org/neurological-surgery.html
The Next Accreditation System Website

30
Milestones
Brief History of Competencies/Milestones
• ACGME Outcome Project initiated
• MedPac, IOM, and Macy Foundation call for GME reform
• Original Healthcare Reform bill includes “New Physician Competencies” and government regulation of GME
• Increasing calls to link GME funding with patient outcomes
• 2011 Macy Report: Ensuring an Effective Physician Workforce
• IOM new initiative: Governance and Financing of Graduate Medical Education
31
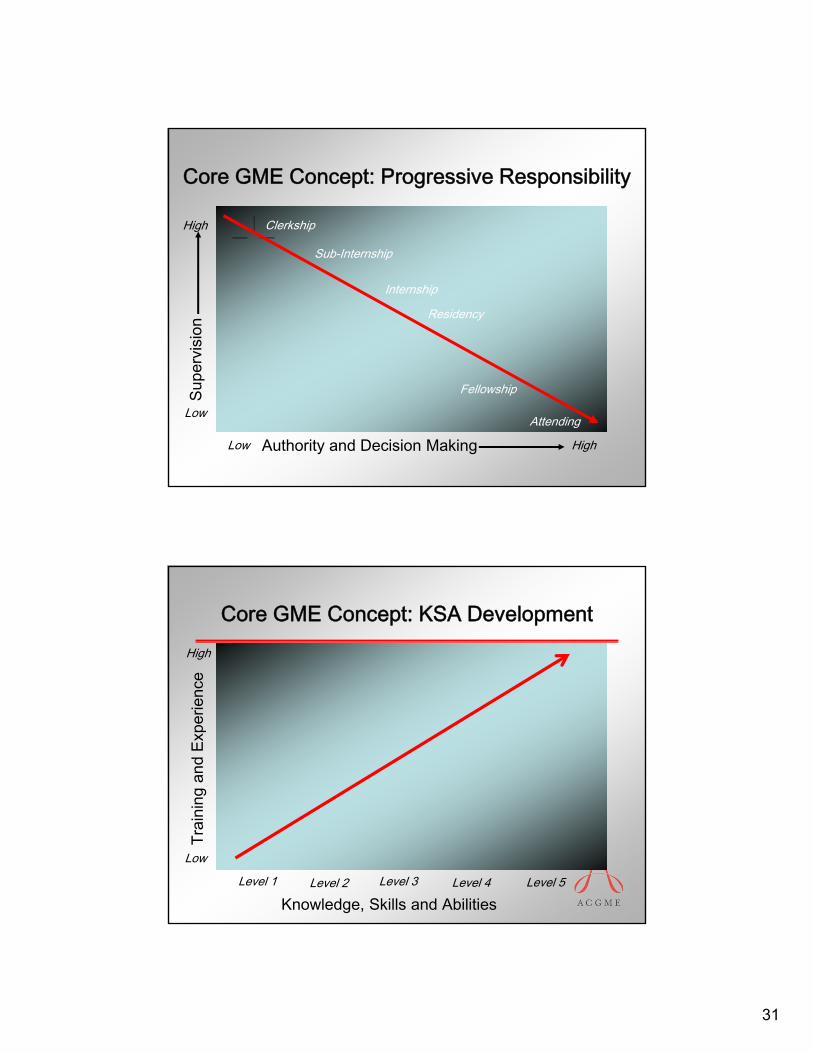
Core GME Concept: Progressive Responsibility
Authority and Decision MakingLow High
Supe
rvis
ion
Low
High
Internship
Residency
Fellowship
Sub-Internship
Attending
Clerkship
Core GME Concept: KSA Development
Knowledge, Skills and AbilitiesLevel 1
Trai
ning
and
Exp
erie
nce
Low
High
Level 2 Level 3 Level 4 Level 5

32
Milestone Goals
• Specialty-specific targets for medical school graduation level identified
• Begins using existing tools and observations of the faculty
• Tracks resident outcomes throughout training
• ABMS Board has the opportunity to track the identified individual
• ACGME Review Committee tracks unidentified individuals’ trajectories
• Provides data supporting ACGME and ABMS goals for public accountability for GME
NS PC/MK Milestone Domains
• Critical Care
• Extra-parenchymal Tumor
• Hemorrhagic Stroke
• Intrinsic Brain Tumor
• Occlusive CVD and Ischemic Stroke
• Pain
• Pediatric Neurosurgery
• Peripheral Nerve
• Spinal Spondylosis
• Spinal Tumor
• Spinal Trauma
• Surgical Treatment ofEpilepsy
• Surgical Treatment ofMovement Disorders
• Traumatic Brain Injury
33
Milestone Advisory Group
• Dan Barrow - ABNS Chair
• Hunt Batjer - RRC Chair
• Kim Burchiel - SNS Sec., RRC Vice-Chair
• Ralph Dacey - SNS Pres-Elect, RRC
• Arthur Day - SNS President
• Allan Friedman – SNS Past President
• Fred Meyer - ABNS Secretary
Sample NS Draft Milestones
• Medical Knowledge – Intrinsic Brain Tumor
• Patient Care – Intrinsic Brain Tumor

34
Next Accreditation System Timeline
• Seven specialties/RRC’s begin training 7/2012 (phase 1) Pediatrics
Internal Medicine
Diagnostic Radiology
Emergency Medicine
Orthopedic Surgery
Neurological Surgery
Urological Surgery
• Phase 1specialties/RRC’s “go live” 7/2013
• Remaining specialties/RRC’s begin training 7/2013 (phase 2)
• Phase 2 specialties/RRC’s using the Next Accreditation System 7/2014
NAS Timeline for NS
• Milestone final drafts - 12/31/2012
• Self study dates determined – notify all programs (done) self study visits begin 7/2014
programs with adverse accreditation or short cycles scheduled for traditional site visit no later than 1/2013
• Comment period for PR revision/categories closes 6/21/12ACGME Board approval fall 2012

35
NAS Timeline for NS• Training phase begins 7/2012RRC reviews all data for all programs at spring 2013
meeting (includes 2012 surveys, annual ADS update info, case log reports, milestone reports): will not ‘count’
RRC determines benchmarks for follow-up actions (e.g., progress report, focused site visit, etc.)
Traditional program reviews and non-accreditation requests reviewed as usual (January and June 2013 RRC meetings
Programs establish process for use of milestone reporting tools
• Enter NAS 7/2013
Resources• Neurological Surgery FAQs
http://acgme.org/acWebsite/downloads/RRC_FAQ/160_Neurological_Surgery_FAQs.pdf
• Duty Hour Common FAQshttp://acgme.org/acWebsite/dutyHours/dh-faqs2011.pdf
• Duty Hour Glossary of Termshttp://acgme.org/acWebsite/dutyHours/dh-GlossaryofTerms2011.pdf
• Resident Survey Key Terms and Content Areashttp://acgme.org/acWebsite/Resident_Survey/ResidentSurvekyKeyTermsContentAreas.pdf
• Neurosurgery newslettershttp://acgme.org/acWebsite/RRC_160_News/160n_Index.asp
• NAS Website http://www.acgme-nas.org/
• ACGME weekly e-communication


















