Skull. Mandible Skull Mandible clavicle Skull Mandible clavicle humerus.
Upload
david-exposito-gonzalezCategory
view
219download
0
8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 1/13
ORIGINAL PAPER
Correlations between the abnormal development of the skull
base and facial skeleton growth in anterior synostotic
plagiocephaly: the predictive value of a classification
based on CT scan examination
Sandro Pelo & Giampiero Tamburrini & Tito Matteo Marianetti &
Gianmarco Saponaro & Alessandro Moro & Giulio Gasparini & Concezio Di Rocco
Received: 30 April 2011 /Accepted: 14 June 2011 /Published online: 1 July 2011# Springer-Verlag 2011
Abstract
Background Anterior cranial plagiocephaly, depending on
the early hemicoronal suture fusion, is the most relevant
form of plagiocephaly in terms of clinical implications. Its
estimated incidence ranges between 0.4 and 1 per 1,000
live births. In the present report, we aim at validating the
classification of Di Rocco and Velardi, proposing a scheme
based on basicranium analysis using CT scans and its
predictive value by evaluating the developmental character-
istics of a population of adult subjects affected by anterior
plagiocephaly who had underwent the surgical correction in
the first months of life.
Materials and methods The group of patients here consid-ered was retrieved from among all patients operated upon
for craniostenosis in the pediatric neurosurgery unit of
Policlinico Gemelli in Rome between January 1, 1980 and
December 31, 1989. The study group consisted of 13
patients, seven females and six males, affected by anterior
synostotic plagiocephaly ranging in age between 20 and32 years (mean 25.54 years). We also formed a group of
unaffected patients in order to control for normal variability
in the population. The subjects of the study group were
evaluated using CT scan exams and cephalometric analyses
were performed using three-dimensional reconstruction.
Discussion and conclusion In this study, we were able to
associate a facial phenotype to confirm the predictive value
of the classification proposed. It is highly probable that the
different outcomes depend on the different degrees of
involvement in the synostotic process by the various skull
base sutures which were essentially unaffected by the
surgical procedures.
Keywords Anterior synostotic plagiocephaly.
Craniostenoses . Craniofacial malformations . Unicoronal
synostosis . Skull base . Coronal suture . Nasal deformities .
Facial asymmetries
Introduction
The term “ plagiocephaly”, from the Greek word πλαγιος
(oblique, twisted), introduced by Virchow in 1851, has been
commonly utilized to define those developmental cranial
deformations, either congenital or acquired, resulting in an
asymmetry and scoliotic appearance of the craniofacial
skeleton [1, 2].
Plagiocephaly is characterized by a complex phenotype
which may vary in the different subjects considerably.
Indeed, it depends on the variable combination of anatom-
ical and functional abnormalities. Among the former, the
early fusion of some cranial suture leads to a focally
impaired growth of the bones of the vault and the skull
S. Pelo (*) : T. M. Marianetti : G. Saponaro : G. GaspariniMaxillo Facial Surgery, Complesso Integrato Columbus,Catholic University Medical School,Via Giuseppe Moscati 31-33,00168 Rome, Italye-mail: [email protected]
G. Gasparinie-mail: [email protected]
G. Tamburrini : C. Di RoccoPediatric Neurosurgery, Policlinico Universitario “A. Gemelli”,Catholic University Medical School,Largo Agostino Gemelli 8,Rome, Italy
A. MoroMaxillo Facial Unit, Ospedale S. Giovanni Battista,Foligno, Perugia, Italy
Childs Nerv Syst (2011) 27:1431 – 1443
DOI 10.1007/s00381-011-1514-x

8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 2/13
base, to malalignment of the cranial and facial bones and to
imbalanced volumetric development of the intracranial
spaces. Ocular, masticatory and cervical muscle functional
abnormalities, varying from mild to severe, also contribute
to the clinical picture. Anterior cranial plagiocephaly,
depending on the early hemicoronal suture fusion, is the
most relevant form of plagiocephaly in terms of clinical
implications. Its estimated incidence ranges between 0.4and 1 per 1,000 live births [3].
The varying severity of the phenotype depends on the
different involvement at the diagnosis, and subsequently,
during the cranial growth of the fronto-zygomatic, the
fronto-sphenoid, spheno-ethmoidal and sphenozygomatic
sutures [3 – 6]. Consequently, the malformation is fully
expressed at the end of the craniofacial growth [7 – 9]
(Fig. 1). Until now, the interception of the disease is based
on the correction in early life of the anterior skull base and
orbital anomalies, while the facial skeleton is usually
approached after 6 – 7 years of age. The posterior skull base
anomaly and the asymmetry of the cervico-cranial junctionare rarely offered a surgical treatment, although physiother-
apy is nearly always suggested.
In the late seventies and early eighties, the advent of CT
scan examination allowed to differentiate different grades of
severity of the disease based on the skull base abnormalities
characterizing the condition in the single subject but did not
result in specific and different surgical approach. Essential-
ly, a unique surgical modality (which implies the unilateral,
or more rarely bilateral, removal and remodelling and
replacement of the frontal bone flap, opening of the orbit
roof, anterior replacement of the superior orbital ridge) was
offered to all the affected infants. The search for criteria to
predict the late outcomes was stimulated.
In 1988, Di Rocco and Velardi [10] proposed a classifica-tion scheme based on basicranium analysis using CT
scans. This classification divides the patients into three
groups. Patients in group I show frontal bone flattening
ipsilaterally to the affected suture, as well as elevation of
the orbital roof without nasal pyramid deviation. In these
children, axial CT scan views show normopositioned vomer
and rocca petrosa.
Patients in group II associate the frontal and orbital
abnormalities with a contralateral deviation of the nasal
pyramid and a variable grade of anterior displacement of the
external ear on the synostotic side. This group is further
divided in two subgroups: IIA and IIB, according to theseverity of rocca petrosa anterior displacement and the
presenceof vomer bone deviation. Group IIA includes patients
with normal positioning of the vomer with a mild or absent
anterior displacement of the rocca petrosa on the affected side.
Group II B includes patients with a moderate grade of vomer
deviation and severe displacement of the rocca petrosa, which
results in reduced size of the middle cranial fossa.
Finally, group III includes patients with a severe nasal
deviation associated with homolateral deviation of the vomer
and anterior displacement of the rocca petrosa besides the
frontal bone flattening and orbital bone anomalies. This
classification is based on the degree of sutural synostosis
extension, which makes it ideal for our research.
It was assumed by the authors that group I only
represented the result of the mere early fusion of the
hemicoronal suture, whereas the other two groups, identified
on the grounds of the skull base anomalies as shown by the
CT scan examination, harboured progressively extended
sutural synostosis of the skull base sutures and corresponded
to different degrees of severity of clinical phenotypes. In the
present report we aim at validating the just mentioned
classification hypothesis and its predictive value by evaluating
the developmental characteristics of a population of adult
subjects affected by anterior plagiocephaly who had under-
went the surgical correction in the first months of life.
Materials and methods
The group of patients here considered was retrieved from
among all patients operated upon for craniostenosis in the
pediatric neurosurgery unit of Policlinico Gemelli in Rome
between January 1, 1980 and December 31, 1989. During
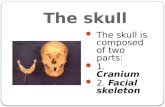
Fig. 1 Typical findings in severe anterior synostotic plagiocephaly: 1
the retrusion of the front on the affected side, 2 retrusion of the roof of the orbit on the affected side, 3 the contralateral frontal bossing, 4 thehypertelorism, 5 the deviation of the nasal pyramid controlaterallyfrom the synostosis, 6 the retrusion of the malar prominence on theaffected side, 7 the mandibular deviation toward the unaffected side
1432 Childs Nerv Syst (2011) 27:1431 – 1443

8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 3/13
this period of time, 239 patients were treated for syndromic
and non-syndromic craniostenoses. The original group
consisted of 122 patients with scaphocephaly, 40 patients
with trigonocephaly, 40 patients with anterior synostotic
plagiocephaly, nine patients with posterior synostotic
plagio cephaly, two patien ts wit h brachicep haly and
patients with complex craniosynostoses, namely: 15 cases of
Crouzon’s syndrome, 12 cases of Apert ’s syndrome and a caseof Saethre – Chotzen syndrome.
Inclusion criteria for this study included the following:
patients affected by anterior synostotic plagiocephaly who
had undergone frontal bone advancement osteotomy as
neonates and had not undergone any other corrective
surgical procedures and who had reached the end of
craniofacial growth. The study group consisted of 13
patients, seven females and six males, affected by anterior
synostotic plagiocephaly ranging in age between 20 and
32 years (mean 25.54 years). We also formed a group of
unaffected patients in order to in order to control for normal
variability in the population.As control, we considered 15 subjects of similar ages
(20 – 32 years) who were not affected by craniofacial or
dentoskeletal malformation that were clinically detectable and
did not experience any facial correction procedures who had
undergone a CT scan of the cranium, facial skeleton and
mandible, following craniofacial traumatic injuries. The 13
subjects of the study group were evaluated between July and
September 2009 in the Radiology Unit of Complesso
Integrato Columbus using a TC Phillips Brilliance 190P
64-slice ® with spiral scansion and multiplanar acquisition.
Two-dimensional images were processed with Mimics
v10.01® (Fig. 2), a software package developed by
Materialise Inc. that allows the user to perform three-dimensional reconstructions from two-dimensional images.
Cephalometric analyses were performed using three-
dimensional reconstruction. As it was not possible to use
standard cephalometric plans in these patients affected by
anterior synostotic plagiocephaly, with the sole exception of
grade I, due to facial asymmetry the most preserved
structure was the complex of sella turcica, which demon-
strated less marked interindividual variability between
affected and unaffected people, were utilized cephalometric
plans passing at this level. Three-dimensional models from
patients’ CT scans were elaborated using Materialise
Mimics 10.0 ® software, and the programme was also usedto create a system of three orthogonal planes to be utilized
as references for metrical evaluations of the dysmorphosis.
The axial reference plan was built using the tips of
anterior clinoid processes and the middle point on the line
connecting the tips of the two posterior clinoid processes as
Fig. 2 Interface of materialise mimics ® software that allows to elaborate three-dimensional reconstruction of soft and hard tissue and permitscephalometric assessments and surgical simulation
Childs Nerv Syst (2011) 27:1431 – 1443 1433

8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 4/13
reference points. For the sagittal plane, we used the middle
point on the line connecting the tips of the two posterior
clinoid processes and the middle point on the line linking
the tips of the two anterior clinoid processes. We drew a
line between these two points to define a plane passing
through this line and orthogonal to the axial plane.
The frontal plane is traced using the two middle points
of the two lines linking the tip of the anterior clinoid processes and the homolateral posterior clinoid processes
orthogonal to the sagittal and axial planes (Fig. 3).
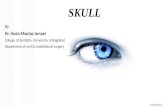
To perform the cephalometric analysis, we chose 22
points (18 paired and 4 unpaired) on which to evaluate the
facial skeleton, the mandible and the basicranium (Fig. 4).
To evaluate the orbit we used:
– Lower orbital point (the lower part of the orbital frame)
– Upper orbital point (upper orbital incision)
– FZ (most medial point of the fronto-zygomatic suture
on the orbital frame)
– Lacrimal point (bottom of the lacrimal sac)
– NOE (point on the emergence of the optic nerve on the
neuro-orbital plane)
For the nose, we chose a non-paired point:
Nasion (intersection of the internasal suture and the
frontonasal suture)
For malar prominences, we chose three-paired points:
– Infraorbital foramen
– Temporal intersection of the zygomatic arch
– Zygion (most prominent point of the zygomatic arch on
its lower side)
For upper maxilla:
– Anterior nasal spine apex
– Posterior nasal spine apex
– Tip of the 1.3 and 2.3 dental elements
– Mesial tips of the 1.6 and 2.6. dental elements
For lower maxilla:
– Menton (most anterior point of the mental process)
– Condylion (tip of the mandibular condyles)
– Coronoid (tips of coronoid processes)
– Gnathion (tip of mandibular angulus)
To evaluate the basicranium:
– The most anterior point on the curve of the small
sphenoidal wings
–
The line traced on the main axis of the rocca petrosa and the angle between this line and the middle plane.
– The internal acoustic meatus
To evaluate the posterior section of the basicranium:
– The most anterior point of the occipital condyles
– The two porions (antero-superior point of the external
meatus)
– Mastoid process tips
All selected points were localized in three-dimensional
space by using the reference planes described previously.
We also measured the distance between the gnathion and
menton for improved evaluation of the mandibular body.We used a minus sign (−) to describe the position of the
points in relation to frontal and axial planes when the points
were behind the frontal plane or under the axial plane.
Results
These data illustrated the differential development of the
various skeletal segments (Tables 1 and 2).
Fig. 4 View of some of the cranial points used for the cephalometricassessments
Fig. 3 View of the reference plan system developed specifically for the purpose of the study
1434 Childs Nerv Syst (2011) 27:1431 – 1443

8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 5/13
The orbital position was evaluated using the following points: upper orbital point, lower orbital point, FZ point,
lacrimal point and NOE. The position and shape of the orbit
were different in the various grades.
In grade I, metrical parameters were similar to those
found in unaffected patients. These patients did not show
significant differences between affected and unaffected
sides, with the sole exception of a moderate retrusion of
the upper orbital point on the synostotic side, which
corresponds to a light asymmetry, characterized by a light
retrusion of the upper orbital rim.
In grade IIA, parameters of the orbital points showed a
more evident retrusion compared to unaffected patients and
more evident asymmetry. Upper orbital points (upper orbital
point and FZ) appeared to be more retruded on the
synostotic side. These parameters were compatible with a
moderate retrusion (mean value of 5 mm) that only involves
the upper part of the orbit, with minimal alteration of the
lower orbital frame. The lacrimal point and the lower
orbital point, in fact, did not show evident alterations
between sides or compared to unaffected patients. Upper
orbital points on the non-synostotic side showed a greater
projection compared to those of unaffected patients,resulting in moderate compensatory growth on the unaf-
fected side. Orbital points of the upper section demonstrat-
ed asymmetry when compared to those on the unaffected
side when evaluated from both the frontal and axial planes.
The orbital points of the lower section exhibited no
alteration. Variability in the position from the axial plane
was not significant from any point, apart from the FZ point,
which was positioned higher on the synostotic side
compared to the contralateral side. Assessments in grade
IIA patients are compatible with moderate asymmetric
patterns that involve both sides of the face, resulting in
only partial expression of the pathology.
In grade IIB, all orbital points on the synostotic side
showed a minor projection from the frontal plane as compared
to contralateral points, with a mean difference of approxi-
mately 8 mm for those points situated on the upper section.
Points on the contralateral side displayed greater projections
in unaffected people than in grade IIA patients, suggesting
compensatory growth. The lower orbital point was also
involved in this grade, although with minimal severity,
whereas the lacrimal point showed no alterations. Grade IIB
Table 1 The differential development of the various skeletal segments of unaffected individuals (assessments are expressed in mm)
Points Front Sn Front Dx Front Sagitt Sn Sagitt Dx Sagitt Axial Sn Axial Dx Axial
Unaffected individuals
Lower Orbital Point 45.5 44.95 35.10 35.10 −22.45 −22.40
Upper Orbital Point 55.08 57.98 24.97 25.12 14.70 15.0
FZ 47.56 48.01 48.77 49.01 1.25 1.60
NOE 16.10 15.97 15.69 15.49 −
8.35 −
7.98
Infraorbital Foramen 46.00 45.00 23.80 24.0 −36.40 −35.98
Ins temp zyg −8.26 −8.13 56.66 55.96 −16.36 −16.28
Zygion 35.34 34.89 52.46 52.66 −28.59 −29.04
Canine 41.4 40.78 18.50 18.70 −78.31 −78.29
Condylion 21.03 20.83 44.38 44.42 −22.22 −22.40
Coronoid 15.97 16.20 44.39 44.39 −34.96 −35.13
Gnation −18.31 −17.91 44.50 44.49 −72.44 −72.35
Small Sphenoid Wing 18.37 17.98 35.68 34.98 10.00 9.87
Ang RP p med 57.35° SN
57.68° DX
Internal acoustic meatus −29.64 −30.04 23.80 24.10 −11.98 −12.22
Occipital Condyle −28.50 −28.68 9.36 9.46 −38.88 −38.75
Porion −28.11 −27.91 52.49 52.50 −17.89 −18.01
Mastoid Proc −43.47 −43.50 50.34 49.34 −38.98 −39.20
Lacrimal 50.04 51.24 10.61 10.58 −18.30 −18.45
Molar 31.06 31.16 21.46 21.55 −70.23 −69.87
Points unpaired
Nasion 70.00 0.6 7.02
Ant Nasal Spine 62.03 0.23 −50.30
Post Nasal Spine 11.03 0.1 −43.98
Menton 44.57 0.3 −111.02
Childs Nerv Syst (2011) 27:1431 – 1443 1435

8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 6/13
Table 2 The differential development of the various skeletal segments of grades I, IIA and B and III (assessments are expressed in mm)
Points Front I Front C Front Sagitt I Sagitt C Sagitt Axial I Axial C Axial
Grade I
Lower Orbital Point 47.99 50.31 32.51 33.53 −22.81 −22.00
Upper Orbital Point 57.21 55.68 28.14 23.75 13.83 14.1
FZ 43.5 46.25 47.35 49.04 1.29 0.81
NOE 15.51 15.8 14.52 16.69 −
6.9 −
5.84
Infraorbital Foramen 47.41 46.47 23.8 25.26 −32.06 −30.3
Ins temp zyg −11.25 −11.45 56.67 56.75 −13.02 −12.86
Zygion 33.88 35.25 54.87 53.56 −29.42 −29.24
Canine 50.17 50.02 15.24 18.29 −74.01 −74.81
Condylion −16.09 −13.34 45.27 43.98 −18.92 −24.05
Coronoid 17.27 16.96 43.84 45.43 −30.77 −28.76
Gnation −17.11 −17.4 45.14 43.69 −69.44 −68.44
Small Sphenoid Wing 21.17 22.76 35.67 36.87 6.69 9.87
Ang RP p med 59.25° I
59.06°C
Internal acoustic meatus −27.69 −26.53 23.80 25.40 −13.23 −12.5
Occipital Condyle −27.84 −29.99 5.95 10.74 −38.86 −38.91
Porion −24.65 −24.2 51.09 52.69 −16.00 −15.8
Mastoid Proc −41.90 −39.58 47.75 50.22 −36.95 −36.02
Lacrimal 48.82 40.3 19.17 10.19 −17.94 −17.09
Molar 30.74 30.02 19.74 20.22 −66.51 −65.70
Points unpaired
Nasion 63.80 0.51 I 5.72
Ant Nasal Spine 62.64 1.01 C 49.13
Post Nasal Spine 12.03 0.4 I 41.97
Menton 45.67 1.33 C 108.52
Grade IIA
Lower Orbital Point 46.13 45.82 42.4 39.34 −28.02 −30.96
Upper Orbital Point 51.26 64.82 28.8 21.34 3.59 2.69
FZ 43.57 45.09 52.4 49.64 −2.58 −9.47
NOE 16.1 14.83 19.16 18.87 −7.52 −8.04
Infraorbital Foramen 47.12 48.15 24.53 29.6 −39.03 −39.99
Ins temp zyg −14.79 −12.8 56.61 58.61 −16.18 −17.01
Zygion 31.75 34.29 53.54 57.04 −40.47 −37.38
Canine 51.76 49.88 15.00 18.87 −82.64 −81.68
Condylion −16.00 −18.87 51.13 47.32 −20.72 −19.72
Coronoid 14.30 12.90 45.58 44.85 −36.18 −32.92
Gnation −21.37 −22.04 50.4 46.59 −83.45 −82.25
Small Sphenoid Wing 18.02 16.96 38.26 41.1 11.78 7.72Ang RP p med 60.03° I
52.61°C
Internal acoustic meatus −24.21 −31.32 31.15 23.22 −11.09 −10.41
Occipital Condyle −31.01 −32.62 11.71 9.87 −36.88 −35.93
Porion −20.86 −22.48 56.69 52.83 −14.87 −16.87
Mastoid Proc −40.7 −51.62 54.65 51.09 −44.7 −41.16
Lacrimal 53.77 53.79 10.11 8.87 −18.7 −19.69
Molar 23.20 21.46 24.39 23.81 −71.32 −71.32
1436 Childs Nerv Syst (2011) 27:1431 – 1443

8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 7/13
Table 2 (continued)
Points Front I Front C Front Sagitt I Sagitt C Sagitt Axial I Axial C Axial
Points unpaired
Nasion 65.84 4.35 I −1
Ant Nasal Spine 65.25 0.87 C −54.99
Post Nasal Spine 11.31 0.58 I −45.94
Menton 49.15 1.59 C −
113.91
Grade IIB
Lower Orbital Point 46.83 48.14 47.9 39.17 −28.89 −28.24
Upper Orbital Point 58.07 67.14 33.38 19.16 2.29 3.27
FZ 41.03 49.15 55.75 47.32 −2.48 −5.09
NOE 20.45 17.54 18.58 18.43 −10.06 −8.86
Infraorbital Foramen 49.15 51.18 24.82 30.92 −38.41 −26.93
Ins temp zyg −14.35 −4.78 57.19 61.83 −18.04 −12.57
Zygion 37.7 37.41 51.95 57.04 −37.38 −34.74
Canine 52.63 49.76 17.99 14.08 −82.33 −81.37
Condylion −8.7 −16.82 47.46 47.03 −21.52 −18.9
Coronoid 21.46 20.3 46.74 45.14 −
37.21 −
32.55
Gnation −10.87 −17.68 50.22 46.79 −86.50 −83.99
Small Sphenoid Wing 24.79 21.89 38.90 38.17 5.07 5.16
Ang RP p med 64.93° I
54.76°C
Internal acoustic meatus −29.69 −49.90 26.7 22.2 −11.65 −11.54
Occipital Condyle −27.55 −30.59 13.06 7.11 −38.85 −38.19
Porion −16.67 −28.85 58.78 52.83 −18.37 −15.17
Mastoid Proc −35.09 −45.96 57.04 49.21 −43.25 −39.56
Lacrimal 54.34 54.08 18.14 7.84 −22.0 19.93
Molar 26.68 23.68 25.84 25.84 −74.39 −73.95
Points unpaired
Nasion 68.59 6.24 I −1.46
Ant Nasal Spine 68.14 2.47 C −53.22
Post Nasal Spine 14.64 0.43 I −49.18
Menton 51.62 1.71 C −115.83
Grade III
Lower Orbital Point 47.42 53.58 40.68 47.9 −17.99 −28.89
Upper Orbital Point 51.78 57.76 26.92 33.38 12.78 8.23
FZ 41.91 48.8 46.94 55.75 6.76 −2.48
NOE 19.31 20.77 15.27 18.58 −5.00 − 4.39
Infraorbital Foramen 51.67 55.42 26.04 30.92 −38.41 −26.8
Ins temp zyg −8.03 −2.66 61.83 53.38 −15.78 −18.04
Zygion 25.37 33.00 54.47 57.04 −25.68 −37.38
Canine 62.10 57.74 12.42 14.42 −68.87 −65.50
Condylion −4.79 −11.19 41.53 48.46 −22.11 −16.67
Coronoid 28.42 19.15 41.28 45.33 −28.79 −26.43
Gnation −5.51 −10.92 42.81 44.45 −76.00 −72.1
Small Sphenoid Wing 20.28 53.58 30.50 47.9 −11.9 −28.89
Ang RP p med 73.42° I
52.76°C
Childs Nerv Syst (2011) 27:1431 – 1443 1437

8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 8/13
patients are characterized by an augmented distance of the
points from the middle plane on the affected side of both the
upper section and the lower section, with a mean value of
7 mm, which is bigger than in grade IIA. Similar to grade IIA,there were no significant signs of asymmetry from the axial
plane, with the sole exception of the FZ point, which is
situated in a higher position on the synostotic side.
In grade III, all orbitary points were retruded compared
to the non-synostotic side, with a mean value of 7 mm. This
retrusion involved all orbital points, including the lacrimal
point, which showed no alterations in the other grades.
Points on the non-synostotic side displayed greater projec-
tion than in unaffected patients. We found a larger distance
from the middle plane for points on the synostotic side,
with a mean value of 7 mm, similar to grade IIB. All points
were positioned higher from the axial plan on the synostotic
side, with the exception of the lower orbital point, whose
position was lower than that on the non-synostotic side.
These assessments are significant for an orbit of
increased dimension whose upper section is positioned
upwards from the axial plan, configuring the so-called
“Harlequin’s phenomenon”. Hypertelorism was present in
three patients and did not appear to be linked with grades.
Nose position was analysed through the position of the
nasion and the anterior nasal spine.
In grade I, the nasion showed a light displacement toward
the affected side. This displacement was minimal and was
present in the group of unaffected patients, potentially
representing anatomical variability. The nasal anterior spine
was also slightly deviated contralaterally from the synostosis,
and its entity was bigger than in unaffected individuals. These
parameters describe a slight deviation of the nasal pyramid,
with a minimally oblique axis top-down from the synostotic
side toward the non-synostotic side that is superimposable to
the normal anatomic variability.
In grade IIA, the nasion showed a larger deviation
toward the non-synostotic side than in grade I; the anterior
nasal spine was also minimally deviated toward the non-
synostotic side. The reciprocal position of the two points is
suggestive of a nasal pyramid deviation with the same
direction of grade I, but the deviation is of a bigger entitythan grade I, and it is not superimposable on unaffected
individuals. In grade IIB, the displacement of the nasion
from the sagittal middle plane was greater than in grade
IIA, whereas anterior nasal spine deviation was superim-
posable with regard to entity and direction.
In grade III, nasion displacement was superimposable for
entity and direction to grade IIB, whereas anterior nasal
spine deviation was bigger than grade IIB. This pattern was
suggestive of a more severe nasal deviation but with the
same direction of the other grades. Malar prominences were
evaluated through three-paired points: infraorbital foramen,
zygion and temporal insertion of the zygomatic arch.
In grade I, the coordinates of the three points did not differ
significantly on the two sides; coordinates were symmetrical
and superimposable in unaffected individuals expressing a
pattern of normoprotrusion and malar symmetry. In grade IIA,
there was an evident retrusion of the malar – zygomatic
complex on the affected side, with a reduction of all projection
assessments. On non-synostotic side projections, assessments
were superimposable to those of unaffected patients. We
therefore conclude that no compensatory growth was present
in this grade. All malar points on the synostotic side were
closer to the sagittal middle plane than on the contralateral
side, whereas no difference was assessed in the distance from
the axial plane with the exception of the zygion, which was
higher on the affected side.
In grade IIB, there was an evident retrusion of the
middle third of the face on the synostotic side; all points
were, in fact, closer to the frontal plane compared to those
on the contralateral side. In this grade, all points on the non-
synostotic side had a moderately increased projection from
the frontal plane, supposedly for compensatory growth. All
points were closer to the sagittal plane on the synostotic
Table 2 (continued)
Points Front I Front C Front Sagitt I Sagitt C Sagitt Axial I Axial C Axial
Internal acoustic meatus −17.50 −22.36 26.70 21.7 −11.65 −15.98
Occipital Condyle −20.53 −20.23 8.49 12.44 −38.85 −40.75
Porion −15.45 26.67 57.72 57.75 −18.37 −17.72
Mastoid Proc −28.46 −35.09 51.64 50.84 −43.25 −42.12
Lacrimal 56.52 54.34 10.76 6.3 −
22.0 −
4.1
Molar 34.65 31.50 22.30 25.26 −74.39 −55.66
Points unpaired
Nasion 67.52 6.67 I −1.46
Ant Nasal Spine 74.55 3.14 C −53.22
Post Nasal Spine 20.94 0.5 I −49.18
Menton 61.24 4.3 C −115.83
1438 Childs Nerv Syst (2011) 27:1431 – 1443

8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 9/13

8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 10/13
tilted toward the synostotic side. These changes were similar
to those found in previous grades, but they were larger. There
were also imbalances in the positions of the points matched
against the axial plane. The tips of the canines and the mesial
cuspeds of the molars were, in fact, lower on the synostotic
side. This framework has significant tilting of the maxilla,which is tilted in the frontal plane, higher on the synostotic
side and lower on the non-synostotic side.
The mandible has been studied by means of three-paired
items (condylion, apex of coronoid and gnathion) and a
non-matched point (the menton). To evaluate the mandib-
ular body, we compared the distance between the gonion
and menton on the two sides.
In grade I, we did not note significant asymmetries on
the two sides; only the condylion was slightly forward with
a slight drop in the affected side. All other values were
symmetrical and similar in the two hemifaces with values
similar to healthy subjects. The menton was moved to theside contralateral to the lesion; this shift was probably due
to the, albeit limited, condylion/glenoid fossa anterioriza-
tion. The distances between the gnathion and menton were
the same in the two hemimandibles and superimposable to
healthy subject findings. The mandibular deviation was
likely due to displacement of the glenoid fossa when we
consider the condylion as an indirect index of its position.
In the grade IIA samples, paired points showed a greater
distance from the frontal plane on the synostotic side than on
the contralateral side. They were also more distant from the
sagittal plane, and they were further down from the axial plane
on the synostotic side. The distance between the menton and
gonion was less on the hemimandibula of synostotic side, andit was equal to that of healthy subjects on the non-synostotic
side. The jaw was moved to the front and down on the
synostotic side, with a slight deviation from the middle plane
of the menton to the side contralateral to the lesion. The
deviation was less than expected because this anteriorization
of the glenoid fossa is compensated for by hemimandibular
hypoplasia on the affected side.
Patients in grade IIB had similar values to the grade IIA,
but greater anteriorization and lowering of the points of the
synostotic side were detectable. The deviation of the
menton and the distance between the menton and gonion
on the affected side were similar in magnitude to thoseobserved in grade IIA, and the distance between the menton
and gonion in the unaffected side showed compensatory
growth and was increased compared to normal individuals.
This condition was significant for the presence of compen-
sation implemented by hemimandibular hypoplasia on the
synostotic side and elongation on the non-synostotic side
compensating for glenoid fossa anteriorization.
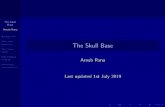
Fig. 6 Picture, soft tissue three-dimensional reconstructionand facial skeleton three-dimensional reconstructionof a patient with grade I
Fig. 7 Picture, soft tissue three-dimensional reconstructionand facial skeleton three-
dimensional reconstructionof a patient with grade IIA
1440 Childs Nerv Syst (2011) 27:1431 – 1443

8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 11/13

8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 12/13

8/12/2019 2011-Correlations between the abnormal development of the skull-Sandro Pelo.pdf
http://slidepdf.com/reader/full/2011-correlations-between-the-abnormal-development-of-the-skull-sandro-pelopdf 13/13
5. Stricker M., Van der Meulen JC, Raphael B (1990) CraniofacialMalformations. Curchill Livingstone Ed. London. pp 234 – 242
6. Marianetti TM, Gasparini G, Moro A, Alimonti V, Cervelli D,Boniello R, Di Rocco C, Saponaro G, Pelo S (2011) Nasal andethmoidal alterations in anterior synostotic plagiocephaly. JCraniofac Surg 22(2):509 – 513
7. Sakurai A, Hirabayashi S, Sugawara Y, Harii K (1998) Skeletalanalysis of craniofacial asymmetries in plagiocephaly (unilateralcoronal synostosis). Scand J Plast Reconstr Surg Hand Surg 32
(1):81 – 898. Richtsmeier JT, Grausz HM, Morris GR, Marsh JL, Vannier MW
(1991) Growth of the cranial base in craniosynostosis. Cleft PalateCraniofac J 28(1):55 – 67
9. Besson A, Pellerin P, Doual A (2002) Study of asymmetries of the cranial vault in plagiocephaly. J Craniofac Surg 13(5):664 – 669
10. Di Rocco C, Velardi F (1988) Nosographic identification andclassification of plagiocephaly. Childs Nerv Syst 4(1):9 – 15
11. Bentley RP, Sgouros S, Natarajan K, Dover MS, Hockley AD(2002) Changes in orbital volume during childhood in cases of craniosynostosis. J Neurosurg 96(4):747 – 754
12. Captier G (2006) Involvement of the basilar coronal ring in
unilateral coronal synostosis. Plast Reconstr Surg 118(1):27313. Fearon JA, Ruotolo RA, Kolar JC (2009) Single sutural craniosy-
nostoses: surgical outcomes and long-term growth. Plast Reconstr Surg 123(2):635 – 642
Childs Nerv Syst (2011) 27:1431 – 1443 1443