2010 Summer - Kabuki Syndrome Network
11
The Kabuki Journal Summer 2010 Gidgets & Gadgets Page 10 Inside Medical Articles Page 11 SOS - Signals Help for Sensory Oral Feeding and Swallowing Problems! Pages 8 Promoting Positive Feeding Behaviors in Children with Kabuki Syndrome Pages 5 The Impact of Gastrointestinal Issues on Oral Feeding in Children with Kabuki Syndrome Pages 6 Understanding the Genetics of Kabuki Syndrome Pages 3 Open Door Forum Page 10 When my husband Daniel and I were expecting the birth of our daughter, we spent many evenings pouring over baby name books. We wanted to pick a meaningful name for her; one that would be beautiful, strong and positive. After much discussion, we finally selected “Mira Jordan Levinson”. In Hebrew, Mira Jordan means “light descending” and Mira has proven her name well, for she has not only brought light in her happy personality, resilience and inner and outer beauty, but she has also brought enlightenment in that we have learned so much from her. Mira was born on January 16, 2008 at 39 weeks gestation. While Mira’s apgar scores were normal, a physical exam identified a small head size and a sacral dimple. An ultrasound and x-rays of her brain and spine came back normal so we thought our worries were over. After her birth, Mira had trouble breastfeeding and low blood sugar, requiring formula feedings via dropper. After a few days, a doctor’s visit indicated improved blood sugar, but found two dislocated hips. Mira would need to wear a harness and undergo hip surgery and casting in the months ahead. This alone was tough to deal with, but more problems lay ahead. After a week home, Mira was still having feeding difficulties, so we took her to a lactation consultant. After an hour with the consultant, it seemed that Mira was finally making progress, but I noticed that her face was turning gray. We took her to the Children’s Hospital ER and made it just in time, because she stopped breathing in the admitting room. Out of nowhere came a crowd of doctors and nurses shouting orders at each other and placing monitors and tubes on our tiny baby as we stood by watching in shock and fear. After a few hours in the ER, Mira was admitted to the Pediatric Intensive Care Unit and sedated with breathing and feeding tubes. I’m still not sure why she needed all of those things. Looking back, I wish I wasn’t so exhausted and confused and knew the right questions to ask and the right ways to advocate for my daughter. Over the course of the next few weeks, we learned that Mira Had a host of medical problems. She had a staph infection, an Atrial Septal Defect (ASD) in her heart, an ectopic kidney and kidney reflux. A brain MRI identified two abnormal spots, but was inconclusive. A swallow study and upper GI determined aspiration risk and reflux. A Geneticist came and noticed attributes about Mira we never would have caught – the small size of her toenails, the low placement and lack of detail in her ears, etc. – and believed that this combination of medical issues and physical attributes indicated a genetic syndrome, but chromosomal testing came back normal. After three weeks in the hospital, we took our “little fighter” Mira home, along with a nasogastric tube attached to her face, a number of medicine prescriptions, and a follow-up plan with a handful of doctors. We went home feeling overwhelmed, but at least we had a plan to “solve” these problems and a good team of specialists to help us. It took time to realize that there isn’t always a solution to every problem. Often, there are more questions than answers. The next few months were exhausting as we worked to manage the schedule of feedings, medicines, doctor appointments, navigating the insurance maze, researching diagnoses, hiring help and brainstorming ways to make things better for all of us. After nine months, we still didn’t have an answer to the “syndrome” question, so we decided to take Mira to a new Geneticist to see if she had any insight on what might be tying all of Mira’s issues together. Right away, the new Genetic Counselor looked at Mira and identified Kabuki Syndrome. We had mixed feelings on the diagnosis. We were happy to finally have a name to identify what “it” was, but that meant we had to admit that “it” wasn’t just going to go away. However, having the diagnosis allowed us to be proactive about Mira’s care and to connect with other families affected with this syndrome, which has proven to be invaluable. This information has allowed us to provide Mira with Early Intervention, PT, OT, feeding and speech therapies which are so crucial at this early stage of her life and are already making an obvious impact on her growth and development. Mira is now two years old and while she still has challenges (still primarily tube fed, still wears a brace for her hips, still requires a lot of therapy) we Mira Levinson - Our Shining Star by Dana Levinson Continued...page 2 Daniel, Dana & Mira Mira
Transcript of 2010 Summer - Kabuki Syndrome Network

TheKabuki Journal
Summer 2010
Gidgets &GadgetsPage 10
Inside MedicalArticlesPage 11
SOS - Signals Help forSensory
Oral Feeding andSwallowing Problems!
Pages 8
Promoting PositiveFeeding Behaviors
in Children with KabukiSyndrome
Pages 5
The Impact ofGastrointestinal Issues onOral Feeding in Childrenwith Kabuki Syndrome
Pages 6
Understandingthe Genetics of
KabukiSyndrome
Pages 3
Open DoorForumPage 10
When my husband Daniel and I were expecting the birth of ourdaughter, we spent many evenings pouring over baby name books.We wanted to pick a meaningful name for her; one that would bebeautiful, strong and positive. After much discussion, we finally
selected “Mira Jordan Levinson”.In Hebrew, Mira Jordan means“light descending” and Mira hasproven her name well, for shehas not only brought light in herhappy personality, resilience andinner and outer beauty, but shehas also brought enlightenmentin that we have learned so muchfrom her. Mira was born on January 16,
2008 at 39 weeks gestation. While Mira’s apgar scores were normal,a physical exam identified a small head size and a sacral dimple. Anultrasound and x-rays of her brain and spine came back normal sowe thought our worries were over. After her birth, Mira had troublebreastfeeding and low blood sugar, requiring formula feedings viadropper. After a few days, a doctor’s visit indicated improved bloodsugar, but found two dislocated hips. Mira would need to wear aharness and undergo hip surgery and casting in the months ahead.This alone was tough to deal with, but more problems lay ahead. After a week home, Mira was still having feeding difficulties, sowe took her to a lactation consultant. After an hour with theconsultant, it seemed that Mira was finally making progress, but Inoticed that her face was turning gray. We took her to theChildren’s Hospital ER and made it just in time, because she stoppedbreathing in the admitting room. Out of nowhere came acrowd of doctors and nurses shouting orders at each other andplacing monitors and tubes on our tiny baby as we stood bywatching in shock and fear. After a few hours in the ER, Mira was admitted to thePediatric Intensive Care Unit and sedated with breathing andfeeding tubes. I’m still not sure why she needed all of thosethings. Looking back, I wish I wasn’t so exhausted and confusedand knew the right questions to ask and the right ways to advocatefor my daughter. Over the course of the next few weeks, we learned that MiraHad a host of medical problems. She had a staph infection, an Atrial
Septal Defect (ASD) in her heart, an ectopic kidney and kidneyreflux. A brain MRI identified two abnormal spots, but wasinconclusive. A swallow study and upper GI determined aspirationrisk and reflux. A Geneticist came and noticed attributes aboutMira we never would have caught – the small size of her toenails,the low placement and lack of detail in her ears, etc. – and believedthat this combination of medical issues and physical attributesindicated a genetic syndrome, but chromosomal testing came backnormal. After three weeks in the hospital, we took our “little fighter”Mira home, along with a nasogastric tube attached to her face, anumber of medicine prescriptions, and a follow-up plan with ahandful of doctors. We went home feeling overwhelmed, but at leastwe had a plan to “solve” these problems and a good team ofspecialists to help us. It took time to realize that there isn’t always asolution to every problem. Often, there are more questions thananswers. The next few months were exhausting as we worked to managethe schedule of feedings, medicines, doctor appointments, navigatingthe insurance maze, researching diagnoses, hiring help andbrainstorming ways to make things better for all of us. After nine months, we still didn’t have an answer to the“syndrome” question, so we decided to take Mira to a newGeneticist to see if she had anyinsight on what might be tyingall of Mira’s issues together.Right away, the new GeneticCounselor looked at Mira andidentified Kabuki Syndrome.We had mixed feelings on thediagnosis. We were happy tofinally have a name to identifywhat “it” was, but that meant wehad to admit that “it” wasn’t justgoing to go away.
However, having thediagnosis allowed us to be proactive about Mira’s care and toconnect with other families affected with this syndrome, which hasproven to be invaluable. This information has allowed us to provideMira with Early Intervention, PT, OT, feeding and speech therapieswhich are so crucial at this early stage of her life and are alreadymaking an obvious impact on her growth and development. Mira is now two years old and while she still has challenges(still primarily tube fed, still wears a brace forher hips, still requires a lot of therapy) we
Mira Levinson - Our Shining Starby Dana Levinson
Continued...page 2
Daniel, Dana & Mira
Mira

Mira....Continued from page 1
KSN FoundersDean & Margot Schmiedge8060 Struthers CrescentRegina, SaskatchewanS4Y 1J3CANADAPhone: 306-543-8715Email: [email protected]: www.kabukisyndrome.com
Newsletter EditorDana Levinson4020 West 39th StreetSt. Louis Park, MN 55416Phone: (952)285-1399Email: [email protected]
Newsletter PublisherSusan Tagliaferro85 West Valley Brook RoadCalifon, NJ 07830-3529Phone: 908-876-4999Email: [email protected]
Kabuki Syndrome of JapanToshinobu Ozeki255-8 HigashikitanoInuyama, Aichi 484-0868JAPANPhone: 81-568-67-7860Email: [email protected]:www003.upp.so-net.ne.jp/kabuki_j/
Assn. Syndrome de Kabuki (ASK)Catherine Mus14 rue Emile Zola59135 BellaingFRANCEEmail: [email protected]: http://asyndkabuki.neuf.fr/Supporting Aussie Kids withKabuki Syndrome (SAKKS)Peta Colton3 Harley Pl.Vista, South Australia 5091AUSTRALIAPhone: 08 82640209Email: [email protected]: http://www.sakks.org/
Netwerk Kabuki Syndroom(European KSN)Fam. VergouwenBeukenlaan 246241 Al BundeTHE NETHERLANDSPhone: 043-3650207Fax: +32 43 3650207Email: [email protected]
I would like to welcome and introduce you to the new team members of KSN. Lastyear I made an appeal for a new Editor for the Kabuki Journal and within a week Iwas contacted by Sue Tagliaferro and Dana Levinson. Sue lives in New Jerseywith her husband Joe and son Robert, and has taken the role of Publisher. Danalives in Minnesota with her husband Daniel and daughter Mira, and has taken therole of Editor. Together we make a great long distance team!
Susana Haywood, a Professional Translator with herown translating business has kindly volunteered manyhours translating articles for our Spanish-speakingfamilies. You can find her latest translation,“Audiological and Vestibular Findings” athttp://kabukisyndrome.com/spanish/span_files.html(#10). On March 6th Susana and her husbandwelcomed new twin additions to their family,Anthony and Valerie. KSN would like to extend ourcongratulations and appreciation once again for allyou do for us!
Bonnie Crane, a former Masters student at The University of Nevada, Las Vegashas completed her dissertation on a young boy with Kabuki Syndrome. Her studyis a welcome addition, in particular for medical personnel. “[...The patient’smedical history and pathophysiology are examined. In addition, a discussion ofcurrent advanced medical research and treatment in the area of genetics relating toKabuki Syndrome is explored. Ethical, social issues and disease prevention areincluded along with the financial impact this disorder can have on the family unit asa whole...]” I have ‘packaged’ it into a pdf file, complete with index for easierselection. You will find it at http://kabukisyndrome.com/files.html (#31). Thankyou Bonnie for sharing with us!!
Peta Colton, Director of Supporting Aussie Kids with Kabuki Syndrome (SAKKS),and I continue to work on developing a comprehensive Medical/Educationalpackage for parents and professionals...all neatly packaged in a pdf file with index.Currently, we send many articles to new families, but send them as separate
- 2 -
Anthony & Valerie
have all come a long way. When she was hospitalized and first diagnosed withKabuki Syndrome, Mira was too young to tell us who she was beyond all of themedical labels. We only had outside sources to tell us what to expect and theannoying company of our own worries to nag usabout what Mira’s future might hold. Now, thoughMira still doesn’t have a lot of words, she has somany ways of telling us who she is. She is happy,fun and loving. She has many interests and enjoysbeing around people. She is resilient and strong.
She is smart! She amazes us every day with thenew things she is learning and is so proud when shelearns a new skill. We delight in heraccomplishments and while she may be behind herpeers in her development, she continually makesprogress. Mira has enlightened us with many valuable lessons. We have learned that asmuch as we like to be in control, we can’t predict the future, so it’s best to prepare forall outcomes while in the moment. We have also gained confidence in ourselves asparents and advocates for Mira. We have learned to be grateful for all of thewonderful things we have – my husband who is a true teammate and incredible fatherto Mira, our incredibly supportive family and friends and the wonderful team oftherapists, doctors and caregivers who truly care about our child. Most importantly, we are so grateful for our precious daughter who brings us somuch joy. Mira has truly brought so much light into the world and we refuse tobelieve that her syndrome is a limiter to her happiness or her abilities. I’m not naive.I know that more problems will come as Mira grows older and we will have a steeplearning curve each time a problem arises. While she may not take thepath in life that we originally dreamed of or expected for her, that doesn’t meanshe cannot be truly happy in life or that she cannot achieve her own highestpotential whatever that may be. To quote our geneticist, “she is going to writeher own book” and we are so happy to be a part of her story!
Mira
(Maggie McMillin is a clinical researcher in Human Genetics,Bamshad Lab at the University of Washington)
Every cell in our body contains a full set of chromosomes andidentical genes. What then differentiates our cells? What makessome of our cells become muscle and others, say, skin? Thishappens because only a fraction amount of genes in each cell are'turned-on' or 'expressed'. That’s an interesting concept isn’t it?That our blood, hormones, bones, and heart all share the exact samebuilding blocks (genes), but only a select few are turned on in eachsystem!
Most of us don’t have an insatiable desire to understand genetics, butwe all have some basic curiosity as to what our bodies are made of.How does it all work? This is particularly true when things don’twork so perfectly.
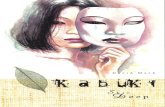
Let’s begin with the smallest most basic elements of the body –DNA. DNA is made up of four bases (adenine, cytosine, guanine,and thymine), each represented by the letter which they begin with.The bases pair with one another and are attached to sugar andphosphate molecules to make what looks like a ladder. See Figure 1
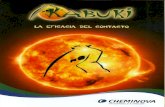
A gene is a length ofDNA ladders. Wehave approximately25,000 genes. TheDNA ladders make upa code, similar to ouralphabet. Actually,very similar to ouralphabet. They areread three letters at atime to produce aminoacids. Think of theamino acids like thewords of a sentence.They are read similarlyto the way we knowthat the letters c-o-l-asignifies a drink.These same letters putin a different order, c-o-a-l, now represents a combustible material.Since there are four different letters (A, C, G, and T), there are 64different combinations that can be used. However there are onlyapproximately 20 amino acids. That means that different codes canproduce the same amino acid. Some of them act as punctuation for
the sentence, signaling when a sentence begins and when it ends.See Figure 2
An example of an amino acid chain might be: CAT ATT GCA GATTGT
Use the DNA decoder wheel to find out what your amino acid chainwould look like. Start from the inside of the wheel and workoutwards to the second ring for your next letter and so on till you getto the outside ring to find the name of your amino acid.
You should have decoded: Histidine-Isoleucine-Alanine-AsparticAcid-Cysteine
Proteins are made up of many amino acids. Think of them as thesentences. It is these proteins that perform most of the criticalfunctions of each cell. Again, some proteins will form muscle, somewill work as enzymes to regulate hormonal and other chemicalprocesses, and yet others will regulate the genes themselves.
- 3 -
Understanding the Genetics of KabukiBy Margot Schmiedge
Edited by Maggie McMillin
Continued....page 4
Fig 2
Researchers at the University of Washington and Seattle Children’sHospital have identified a gene responsible for Kabuki Syndrome!Initial results have found that 70% of participating individuals hadthe change in this particular gene. The discovery opens the door forclinical testing to be developed. For those who do not have themutation, there could be other gene(s) involved and therefore testingcontinues. More than ever, we need families to participate in thestudies.
Please contact the Clinical Research Coordinator, Maggie Macmillinat:University of WashingtonDept of Pediatrics1959 NE Pacific St.Seattle, WA 98195Ph# 206-221-3849Pager# 206-469-1668Fax# 206-221-3795Email: [email protected]
Base pairs
Sugar phosphatebackbone
Adenine
CytosineGuanine
Thymine
Fig 1

- 4 -Understanding Genetics....Continued from page 3
Fig 3
Only about 1% of ourDNA is coded by genes,which in turn makeproteins. The rest isreferred to as non-codingDNA and is not yet wellunderstood. It isbelieved, among others,that they have aninfluence on our cells toknow when to switchcertain genes on and off.
Chromosomes are madeup of many genes. Humans have 22 pairs of chromosomes plus onepair that determines our sex. See Figure 3.
Let’s re-cap: DNA consists of four bases, and sugar and phosphatemolecules to form ladders. Genes consist of DNA ladders and it’sall tightly packaged into bundles called chromosomes.
DNA is read three bases (letters) at a time to produce amino acids(the words) and stops and starts (punctuation). Many amino acidsmake up proteins (the sentences) which are contained in genes(paragraphs or chapters). Proteins do the work in constructing ourbodies (which makes the story complete!)
So what happens in the case of disease or a syndrome? Sometimesone of the letters of the DNA is swapped for another. All of us carrysome of these errors. So why do we not all have a syndrome?Remember how the four DNA letters could be coded in 64 possiblecombinations (4x4x4x4) but will only produce about 20 differentamino acids? Some combinations can handle an error. For exampleif the letter T is swapped for an A in the codon GCT the resultingprotein would still be the same, since both the old codon (GCT) andnew codon (GCA) code for the same amino acid (see for yourselfwith the DNA decoder). Other error combinations may have veryserious effects. Swapping an A for a T in a gene for hemoglobinresults in the serious blood condition sickle cell anemia. Think ofit like this: it's OK if Jane the waitress doesn't show up because wecan move Mary into her position and Jack into Mary's position sincethey have all performed each other's tasks. However if Jessica theorthopedic surgeon doesn't show up, we can't very well have the ORnurse fill in for her! Other errors can occur as well, such as a bit ofthe DNA sequence is missed or a bit added, etc.
Karyotyping or blood chromosomal analysis is a study of ourchromosomes. Cells are stained and examined microscopically toexamine the size, shape and number of chromosomes in the sample.Think of it as a view of earth using a satellite. It will clearly show ifa continent or country has changed its shape.
Microarray analysis allows scientists to scan the chromosomes,looking more closely at the genes. Different types of microarraysare able to detect different things, for example if there are insertionsor deletions of genetic material or compare the expression of genes(remember, this means whether the gene is 'turned-on' or not) in ahealthy sample versus a diseased one. Think now of a morepowerful satellite image that gives you the ability to see cities.
Targeted gene sequencing allows scientists to look very closely atour DNA to detect small changes in the sequence, or ‘letters’ in theDNA. Think now of a satellite so powerful that is able to see singlehomes.
Most individuals with Kabuki will have normal chromosomal studytest results. The ‘error’ is in a letter – a home, not a continent. Eventhough the change is ‘small’, that is not to be misunderstood as beinga minor error – just a difficult one to see until recently. Increasedability to see smaller and smaller elements of our body and increasedunderstanding of what those elements do, make it possible to more
accurately diagnose conditions. But science is a continuous process- one discovery and level of understanding leads to another. Muchstill needs to be understood, which may even lead to prevention inthe future. These are exciting times in the genetic world!
More specifically in the case of Kabuki(Addition by Maggie McMillin)
A genome is an individual’s entire genetic code. The HumanGenome Project was the first time scientists had completely lookedat every base (letter) of the genome. There are about four billionbases in the entire genome. It is still very difficult and veryexpensive to sequence an entire genome.
Only about 1% of the genome contains genes. There are about20,000 genes in the genome. An exome is a newly made-up word todescribe targeted sequencing of all the genes. Remember that genesare the part of the genome that code for proteins, and proteins are thethings that perform functions in the body. If something does notfunction or develop properly, a gene is the first place to look to finda change that might cause the disease or dysfunction. So exomesequencing is a way to focus on looking at the most important part ofthe genome. And because there is much less sequencing thanlooking at the entire genome, the cost is much less.
Recently researchers studying Kabuki syndrome at the University ofWashington and Seattle Children’s Hospital used exome sequencingto identify the gene causing the syndrome. In the study, researcherssequenced the exomes (all the genes) of 10 individuals with KabukiSyndrome. Then they compared the information between all 10individuals to find a gene that contained a change that would bepredicted to cause dysfunction of the protein. They found a gene thathad changes, or mutations, in 9 out of the 10 individuals. Thenresearchers used targeted sequencing to look at the same gene inmore individuals with Kabuki and about 70% of individuals had achange in the gene.
The gene provides the instructions, (like a recipe) to make a type ofprotein called a histone methyltransferase. Histones are proteins thatthe DNA is tightly wound around, like a spool of thread. This helpsto package all the DNA so that it can fit inside the cell nucleus.When a cell needs to “read” the DNA to make a protein and performa function, it unwinds whatever little part needs to be read. Histonemethyltransferase is a type of protein, called an enzyme that helps tounwind the DNA from the histone.
There are two clues as to why this gene is a causative agent ofKabuki: 1) The individuals without Kabuki (control individuals) do not have the same types of changes in this particular gene. 2) The parents do not have the change (unless they also have Kabuki). So most of the time the change in an individual with Kabuki is a new, “sporadic” change. This is just something that happens by chance.
This means that researchers have identified a gene that explains alarge number of cases of Kabuki syndrome, and now a clinical testcan be developed. For individuals with Kabuki that do not havemutations, there is likely another gene that causes the syndrome.The researchers are still conducting the study to look for other genes.
It’s not yet known how the changes to the gene change the functionof protein or why it causes the features of Kabuki syndrome. It’salso not known if different changes within the gene can lead to moreor less severe clinical features. But now that the gene has beenidentified, scientists have the next step in moving forward to try toanswer these questions.
Copyrighted 2010

- 5 -
Due to advances in medical technology, more children aresurviving severe prematurity, rare genetic syndromes and complex
medical conditions. One of the firstmilestones that children must meet isthe ability to take in nourishmentsafely and efficiently. For feeding tobe safe and efficient, multiple physicalsystems must work together in aneffortless, coordinated fashion.Children born with multiplecomplications are at greater risk fororal functional/feeding problems for amultitude of reasons. Just as with thislarger population, children withKabuki Syndrome also have multipleissues that may interfere with safe,efficient and/or pleasurable eating in
the short run. These issues include structural issues such as cleftpalate, hypotonia, poor growth, dental or orthodontic issues, as wellas sensory and cognitive issues, just to name a few. Asoverwhelming as this list may appear, there are many children withKabuki Syndrome who eat safely, efficiently and happily. The keywords here are efficiently and happy. The development of apositive relationship with foods must occur to promote long termfunctional eating skills. The first step to treating feeding difficulties is early recognitionof elements that impact eating and their potential secondary impact.When evaluating any child for feeding difficulties, the physicaland/or structural issues that may interfere with safe and efficienteating must be identified and treated first. As reported by Dr's.Iida,Park and Iida in the 2008 Fall edition a medical journal, theincidence of cleft lip/palate in children with Kabuki Syndrome ishigher than average. Children with cleft lip/palatal issues tend tohave difficulty with efficiency of oral intake as they cannot buildup enough oral pressure to expel the formula from the nipple andmay require a non-traditional nipple or feeding method. This mayresult in lengthy feeding times or total inability to orally feed untiltheir palates/lips are repaired. Children with cleft lip and palateneed to be seen by a Speech-Language Pathologist or FeedingExpert as soon as possible to determine which type of nipple mayresult in the best quality and quantity of intake. Reflux should alsobe recognized and treated quickly and efficiently before childrencan associate the sight of food/bottle with emesis or pain. Children with Kabuki Syndrome also are at higher risk forissues with the cardiac system. Children with cardiac issues tend tohave limited stamina and fatigue easily. Bottle drinking takes quitea bit of stamina, strength and coordination and can be quitefatiguing for a child. Pair the cardiac issues with any structuralissues such as cleft lip/palate and you have a very inefficientsystem. Compounding the structural and cardiac factors is the issueof hypotonicity frequently seen in children with Kabuki Syndrome.Adequate muscle tone throughout the entire body is imperative forproper strength to expel formula via the nipple and for good trunksupport that is needed for spoon and finger feeding down the road. Children with Kabuki Syndrome have also been reported tohave sensory integration issues. Eating is a completely sensoryactivity; smelling, touching and tasting foods are all sensoryactivities and can be overwhelming to a child who has a system thatis unable to effectively process the input. It is important torecognize how significantly sensory issues can impact a child,especially one with low tone and potential structural issues that canalready interfere with eating. Sensory issues can be transitory andchange over time as a child matures and is exposed to more of theworld.
Developmental delays are common in Children with KabukiSyndrome. A good in-depth cognitive evaluation is imperative inorder to meet the children where they are most successful. Althougha child might be 18 months old chronologically, developmentally theymay have language and motor skills at a lower level. Requiringbehaviors at the 18 month level will only set them up for failure,where as presenting tasks at their current developmental level willresult in accomplishment and success. As brain development is so important for the first few years oflife, growth should be monitored closely and stagnant growth shouldbe treated quickly. Children with Kabuki Syndrome frequently havepoor growth trends. These children may need a supplemental feedingtube; either a Nasogastric tube or a surgically placed Gastrostomytube. If a supplemental feeding tube is necessary for longer than 3 to4 months, it may be better to have a G-tube or PEG placed. Lengthy use of nasogastric tubes can result in increased oralaversion as they need to be changed frequently, require tape to holdthem in place on the face and may impact swallow sensation. Topromote appropriate growth, formula can be given as a supplement towhat the child is able to eat orally and may not need to be a totalreplacement for oral intake. Although the thought of having a gastrostomy tube placed is veryscary, being able to support good growth while your child isobtaining the cognitive, motor, and sensory therapy milestones thatare necessary for positive and healthy eating habits is important. So, the bad news is that feeding problems in children withKabuki Syndrome seems inevitable and overwhelming. The goodnews is that almost any feeding problem can be overcome if it isapproached and handled in the right manner and at the right time.Promoting quality over quantity is imperative. Pushing an infant withcardiac and structural issues to take all calories orally by increasingfeeding times, using fast flow nipples or ignoring cues may result infeeding aversion. Sometimes the use of a supplemental feeding tubein the short term can be beneficial for the long run. Allowing a childto eat a small amount with good quality is always better than pushingthat child to eat a large amount unhappily or unsafely. Because children with hypotonia tend to meet motor milestonesat a slower rate, it is important to match our feeding expectations withthe child 's current motor and cognitive level, not necessarily theirchronological age. This may result in a slower transition from bottleor breast-to-spoon feeding and finger feeding, but improved quality oftransition. Pushing a child to transition to textures that they arephysically not ready for can result in poor quality of intake andfeeding aversion. Some children with sensory issues and low tonenever do well with purees and this texture may be better skipped. Exposure to solids usually occurs once a child has good headcontrol, good trunk support to support use of hands for reaching andpincher grasp for picking up small items. This time is really meantfor sensory and motor exploration and not really as a method ofgetting in many calories. This is a time to help your child develop apositive relationship with textures, smells and tastes even if thequantity of oral intake is low. Children who enjoy eating, even smallquantities, will go on to be oral eaters in the long run if we can helpthem become internally motivated to eat once the timing is right.Internal motivation comes from a sense of hunger and satiety. Helping children with feeding tubes recognize and react tohunger cues is an important first step in building this internal drive.Children on lengthy tube feedings or overnight drips may have adifficult time understanding the full/empty signs. Some childrenrequire continuous drips, but others can be transitioned to ageappropriate bolus feedings during the day. It may seem at times that your child is not moving forward in theprocess of learning to eat. Children without medical complicationsbegin to learn to eat at birth and are not fully competent eaters
by Polly Tarbel, Med. CCC-SLPDirector of the Encouragement Feeding Program at University of Virginia Children’s Hospital
Promoting Positive Feeding Behaviors in Children with Kabuki Syndrome
Continued...page 6
Polly Tarbel

- 6 -Promoting Positive Feeding....
The Impact of Gastrointestinal Issues on Oral Feedingin Children with Kabuki Syndrome
By Lori Scott, M.S., CCC-SLP, CLC
until at least 15 to 18 months. Children with complicationsneed to be given extra time to accomplish the same skills.Children demonstrate functional improvement in feeding onlyif it is comfortable, pleasant and internally motivating.
So the bottom line is; take it slow and steady, ensure that itis pleasurable at all times and recognize your child’s cognitive,sensory and motor strengths and weaknesses. Building a
positive and safe relationship with foods will result in a childwho is motivated to become an oral eater when the timing isright.
Please feel free to contact me with questions regarding thespecifics of how to build a positive relationship with foods [email protected].
Gastrointestinal (GI) issuessignificantly impact oral intakeby influencing a child’s relationshipwith food, their willingness to eatand their oral-motor skilldevelopment. The GI tract,comprised of a complex and intricateseries of organs, is designed totransport food through the digestivesystem absorb and distributenutrients necessary for growth andgenerate waste to be eliminated.Efficient (and painless)digestion
allows for a positive mealtime experience which in turn contributesto optimal nutrition and growth. When a child suffers from reflux,vomiting or discomfort during/after meals, he/she may begin to havea negative association with eating. Consequently, the child mayresist eating or become a very picky eater in an effort to avoid pain.Because there is a nigh incidence of gastrointestinal disorders inchildren with Kabuki Syndrome, it is important for parents andtherapists to understand the relationship between GI symptoms andfeeding, appetite and growth. This article outlines two major GIissues; gastroesophageal reflux disease and constipation, as well astheir impact on feeding in children with Kabuki Syndrome.
GASTROESOPHAGEAL REFLUX (GER) is defined as theeffortless movement of gastric contents into the esophagus. Themajority of infants and toddlers reflux or “spit up” occasionally andthis is a normal phase in the development of the GI system.Infrequent reflux typically has minimal effects on oral feeding andwill often be outgrown by 1-2 years of age. In contrast, chronicreflux or gastroesophageal refluxdisease (GERD) produces clinicalsymptoms that interfere with a child’s health, appetite and growth.GERD is prevalent in children with Kabuki Syndrome asapproximately 42% ofchildren have reflux, 23% have regurgitation and 63% gag/vomitwhile eating.
Causes: Gastroesophageal reflux occurs during transient relaxationsof the lower esophageal sphincter (LES) or with inadequateadaptation of the sphincter tone to changes in abdominal pressure.The LES is a band or muscle tissue responsible for closing andopening the lower end of the esophagus. When working properly,this muscle opens to allow food to pass through into the stomach andcloses again to keep stomach contents contained. If the LES opensspontaneously (called transient relaxations or TLESRs) the Stomachcontents may be transported back into the esophagus, mouth or beexpelled from the body.
Symptoms: GERD can present in a variety of ways and a child mayexhibit one or multiple symptoms. Common manifestations includevomiting (with poor growth), gagging/choking, respiratory issues(apnea, cyanosis, chronic cough, asthma, gurgly respirations),halitosis (bad breath), frequent swallowing, severe sleep
disturbances, frequent hiccups, dental carries, irritability, foodrefusal, back archingduring feeding, chronic ear infections/laryngitis/rhinosinusitis and/oran inability to consume large volumes per feeding. It is important toremember that not all children will vomit with reflux. Children mayhave more subtle symptoms (known as “silent reflux”) which canresult in esophageal inflammation and pain.
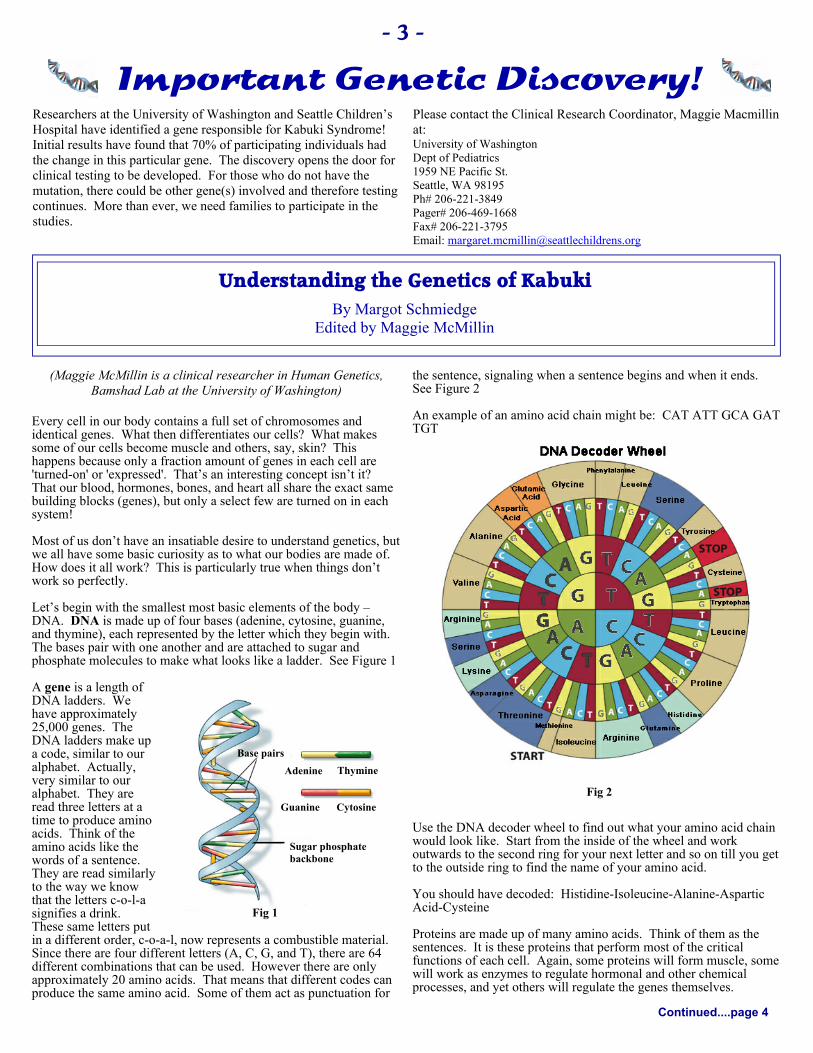
Assessment: Your child’s Pediatrician or Gastroenterologist mayrecommend a variety oftests to determine theseverity of his/her GER.
Upper GastrointestinalSeries (UGI) - Barium (achalky drink)is swallowed and x-raysshow the shape of theesophagus andstomach. This test can finda hiatal hernia, blockage andotherproblems that might mimicreflux.
Esophagogastroduodenoscopy (EGD) - After the patient is given asedative medication so they are asleep, a small flexible tube with avery tiny camera is inserted through the mouth and down into theesophagus and stomach. The lining of the esophagus, stomach andsmall intestine can be examined and biopsies (small pieces of thelining) can be painlessly obtained. The biopsies can later beexamined with a microscope, looking for inflammation and otherproblems.
PH Probe - A thinlight wire with an acidsensor at its tip isinserted through thenose into theesophagus. The probedetects and recordsthe amount ofstomach acid comingback up into theesophagus when thechild has symptomssuch as crying,arching or coughing.
Nuclear Milk Scan -A small amount of
radio active material is mixed into breast milk/formula andconsumed by the child. The scan beginswhile the child is swallowing and will Continued....page 7
Esophagogastroduodenoscopy(EGD or upper endoscopy)
Esophagus
Endoscope
Light Stomach
1 In hypopharynx (lower back of throat)
3 In esophagus just above lower esophageal sphincter
1
3
Naso-oropharynxEsophagusUpper arrow LPR
Stomach
Lower gastroesophageal refluxVocal folds
2 In esophagus just before upper esophageal sphincter
2
Lori Scott

- 7 -
continue for approximately one hour. The child will lay on theirback, on the table with the camera underneath them.
Treatment:Environmental/Behavioral Treatment Strategies:
Dietary - formula changes in infants (may be changed to soy,hydrolyzed or amino-acid formula), minimize foods high in fat(fat delays gastric emptying), avoid acidic/spicy foods, minimizecaffeine, tea, chocolate, spearmint/peppermint (may lower LESpressure).
Position - feed infants in an elevated side-lying position withno compression on the abdomen, staying upright 20 minutesafter meals, elevating the head of the bed.
Activity - no bouncing, swinging or compression of the stomachfor up to 20 minutes.
Frequency/Quantity of feedings - smaller, more frequent feedingsto avoid over distention of the stomach (total volume shouldremain the same).
Thickening formula with rice cereal - some physicians mayrecommend adding rice cereal to formula, but thickening is doneless frequently (especially by gastroenterologists) as this strategymay worsen GER symptoms if gastric emptying is slow.
Medications:
Antacids - neutralize gastric acid and reduce negative esophagealeffects of acid exposure (rarely used in infants/toddlers);examples include Tums, Mylanta, Maalox.
Histamine-2 Receptor Antagonists (H2Ras) - decrease acidproduction by inhibiting the receptivity of the cells that producehydrochloric acid in the stomach. Examples include; Ranitidine(Zantac), Cimetidine (Tagamet), Nizatidine (Axid), Famotidine(Pepcid).
Protein Pump Inhibitors (PPIs) - block the production of gastricacid completely by acting as a proton pump inhibitor. Examplesnclude; Omeprazole (Prilosec), Lansoprazole (Prevacid),Esomeprazole magnesium (Nexium), Zegerid (containsomeprazole and sodium bicarbonate {antacid}).
Prokinetic Drugs - increase upper GI motility (may improveperistalsis, increase LES resting pressure, reduce gastricemptying time). Examples include; Metoclopramide (Reglan).
Antibiotics - a low dose of Erythromycin is sometimes used toenhance stomach emptying. How effective are GERmedications? It depends on the child and the severity of reflux.Be aware that GERmedications are meant to decrease acid production and/orincrease GI motility (not necessarily eliminate vomiting).
Surgery: Nissen Fundoplication surgery is where the gastricfundus (upper part) of the stomach is wrapped 360° around theinferior portion of the esophagus, reinforcing the closing functionof the lower esophagealsphincter.
Impact on Feeding: Asmentioned previously,children withgastroesophageal refluxoften associate pain witheating and in turn altertheir eatingpatterns. Infants may
become averse to the bottle or have difficulty transitioning tosolid foods. Toddlers often become picky eaters and limit theirfood repertoire to certain textures, tastes and/or colors. In orderto maximize nutrition and weight gain, toddlers need to have atleast 30 foods in their diet (10 proteins, 10 starches and 10fruits/vegetables). If your toddler has a limited food repertoire, aformal feeding evaluation by a licensed Speech-LanguagePathologist or Occupational Therapist may be warranted.
CONSTIPATION is present in 47% of children with KabukiSyndrome. It is a gastrointestinal issue characterized byinfrequent bowel movements, hard stools or straining duringbowel movements.
Causes: Constipation can be caused by a variety offactors including (but not limited to) inadequate fluid intake,inadequate dietary fiber, cow’s milk protein allergy, abnormalmuscle tone and/or malnutrition.
Treatment: Fluids - increase fluid intake. Diet - decreaseconstipating foods (e.g., milk, cheese, yogurt, bananas,applesauce, etc.); increase fiber intake (high-fiber food listsavailable online). Medications - common medications forconstipation in the pediatric population includes Milk ofMagnesia, mineral oil, Lactulose and Miralax.
Impact on Feeding: When children are constipated, theyexperience a sensation of being bloated and full.Consequently, their appetite is affected and they often reducetheir oral intake. It is necessary to maintain a regular andpain-free bowel pattern in order to boost appetite andNutrition.
In summary, although parents are responsible for feedingtheir children, they do not have to shoulder the complicationsof a child’s GI and feeding problems alone. There arenumerous feeding clinics across the country andinternationally that focus on a multi-disciplinary approach tofeeding. By involving several specialists (GI’s, Dieticians,Speech-Pathologists, Occupational Therapists, etc.) in achild’s care, families can formulate a treatment plan thataddresses the medical, nutritional and emotional aspects of afeeding disorder.
For more information please contact me at:[email protected] or (615)322-1973.
The Impact of Gastrointestinal Issues....Continued from page 6
Fundoplication
While shopping in a food store, two nuns happenedto pass by the beer. The first nun said it would benice to enjoy a beer.
The second nun answered that, indeed, it would bevery nice to have one, but that she wouldn't feel
comfortable about buying it. The first nun replied that she couldhandle that without a problem. So, she picked up a six-pack andtook it to the cashier.
The cashier had a surprised look on his face, so the nun said, "We usebeer for washing our hair; a sort of shampoo, if you will."
Without blinking an eye, the cashier reached under the counter,pulled out a package of pretzel sticks and placed them in the bag withthe beer.
He then looked the nun straight in the eye, smiled, and said, "Thecurlers are on the house."

- 8 -
Every parent dreams of a momentwhen they will be joyfully holdingtheir child and that child issnuggled in their arms nursing orfeeding happily and eagerly.Feeding your child will be easy,fun and enjoyable. While allparents have moments when theirchild does not always like whatthey offer them at mealtime orthey spit up after a nursing orbottle feeding; these are rareexceptions and not interfering totheir family life. But, this is not sofor the parent of a child who hasfeeding and swallowingdifficulties. The emotions are veryhigh with the parent who cannotmeet their child’s nutritional needsdespite all the different formulas, nipples, cups and home-made foodthey have tried. Nothing is working and the question is why.
Why is my child vomiting after each meal? Why is my child able tostart to eat fine and then after a few minutes into mealtime he/shestops eating and starts crying? Why is my child able to chew on aplastic toy but not on food? These are the questions that manyfamilies with a child diagnosed with Kabuki Syndrome can relate toand face daily...feeding and swallowing skills are complex. Eightmuscles are required for us to chew and all of our four senses areused for eating; sight, sound, taste and small.
As a Pediatric Speech-Language Pathologist, I have specialized inthe area of evaluating and treating children with feeding andswallowing disorders for over 24 years. I have worked with only onechild, that I was aware of, that was diagnosed with KabukiSyndrome. Her family’s journey with her feeding difficulties is notunlike many other families who have children with low oral muscletone, gastric esophageal reflux and sensory oral sensitivities. Iworked with her and her family for almost a year before wediscovered her medical diagnosis. Despite the unknown, they stillneeded to know how to feed their daughter and how to help herprogress developmentally.
The focus of this article is to define the medical professionals whomay be players in the evaluation and treatment for a child who isdisplaying feeding and swallowing difficulties; the therapies andtests to consider and finally provide some helpful tools to use withyour child. This is not an exhausted list of the professionals orindividuals who assist in this area, however, it is important tounderstand that each of the professionals that you consult with are towork as a team.
The first player in the game is either your child’s Pediatrician orFamily Practice Physician who is the primary medical specialist foryour child’s overall health and well being. They are generally
driving the train with you to refer to specialists if needed and caringfor your child’s overall health and development. He/she could thenrefer your child to the following specialists: Gastroenterologist,Endocrinologist, Speech-Language Pathologist, OccupationalTherapist, Physical Therapist, Nutritionist and Dietician.
A Gastroenterologist is the physician who specializes in thediagnosis and treatment of disorders of the gastrointestinal tractincluding the esophagus, stomach, small intestine, large intestine,pancreas, liver and gall bladder. Individuals with Kabuki Syndromecan often experience chronic constipation, gastric reflux anddifficulties maintaining oral intake. The specialists are the ones whomanage the alternative feeding tubes; such as a nasogastric andgastric tube.
An Endocrinologist is the physician who specializes in the diagnosisand treatment of diseases of the endocrine system/; such as diabetesand growth disorders. Children with Kabuki Syndrome are at risk forhypoglycemia, growth hormone deficiency,hypothyroidism and/or adolescent obesity.
A Speech-Language Pathologist is a specialist who evaluates andtreats communication disorders and feeding/swallowingproblems. Speech-Language Pathologists can perform clinicalfeeding/swallowing assessments, as well as swallow studies with theradiologist, called either Oral Pharyngeal Motility Swallow studies,Barium Swallow studies or Video Fluoroscopic Swallow studies.The name of this objective swallow test can vary from area to area.
During a swallow study, a patient swallows a variety of liquids andfoods mixed with barium, as a radiologist takes video x-rays of themouth and throat. These images show how food passes from themouth through the throat and into the esophagus. They may alsoreveal aspiration - foreign matter entering the lungs - if bariumenters the windpipe.Aspiration puts patients at risk for lunginfections. (Answers.com, “References and Answers”, Dictionary ofMedical Professionals, http://www.answers.com.)
An Occupational Therapist is another specialist who can valuatefeeding and swallowing difficulties. They also are the experts onsensory integration, self-feeding skills and providingrecommendations for adaptive equipment and utensils. Dependingupon your area, either a Speech-Language Pathologist or anOccupational Therapist will be the specialist that your primaryphysician will refer your child to for a complete feeding andswallowing evaluation and treatment, if needed.
The Nutritionist and Dietician are the professionals trained to assistin evaluating and guiding the family regarding calorie intake,developing a well-balanced diet, assisting with tube feeding caloricintake and supporting the overall health of the child who isdisplaying feeding and swallowing difficulties.
SOS - Signals Help for Sensory Oral Feeding and Swallowing Problems!!
by Linda C. Lane, MS, CCC, SLPSpeech-Language Pathologist, Children’s Healthcare of Atlanta
Continued....page 9
Linda Lane

A Physical Therapist is the professional that can assist the muscletone and positioning issues, gross motor delays and toevaluate your child for a special adaptive seating system.
As a Parent you may find yourself the manager of this complexproblem. In some cases, you may be fortunate to have a person whoacts as a case manager, to assist you in this maze of medical andtherapeutic appointments. There are numerous therapeuticapproaches to assist children with feeding and swallowing disorders.Some involve oral motor exercises to promote improved oral muscletone and/or coordination. Other programs may be very structuredand systematic if the focus is reducing some of the sensorysensitivities (i.e., tactile defensiveness, gagging at the sight ofcertain foods, specific texture refusals) and coping behaviorssurrounding food.
For example, there is the Sensory Oral Sequential Feeding Programdeveloped by Dr. Kay Toomey and associated located in Coloradowhere they take a very systematic approach to assisting children thathave sensory oral feeding aversions and help them approach newfoods and/or undesirable foods in a safe and fun way.
It has been developed over the course of 17 years through theclinical work of Dr. Toomey, in conjunction with colleagues fromseveral different disciplines including: Pediatricians, OccupationalTherapists, Registered Dieticians and SpeechPathologists/Therapists.This program integrates sensory, motor, oral, behavioral/learning,medical and nutritional factors and approaches in order tocomprehensively evaluate and manage children with feeding/growthproblems. It is based on, and grounded philosophically in, the“normal” developmental steps, stages and skills of feeding found intypically developing children (Educations Resources, Inc., “PickyEaters Versus Problem Eaters”, The SOS Approach to Feeding,http://www.educationresourcesinc.com, 3/14/2010).
Another approach is the Applied Behavioral Analysis approach toeliminate negative food refusal/aversions that a child can develop tocope around foods that they associate with pain or discomfort.Generally, Behavioral Psychologists are on the feeding teams whenusing this applied behavior analysis approach. Each program has itsspecific purpose and therefore, whichever approach is used it isimportant that your child be evaluated by a skilled feeding andswallowing specialist, and that the therapeutic techniques and goalshave been individually developed for your child’s unique needs,strength and weaknesses.
There are several different types of nipples, bottles, cups, utensilsand oral motor stimulation devices on the market today and there arenew ones always being introduced everyday. It is the job of theFeeding and Swallowing Specialist to keep up with this as this istheir speciality. In my own practice I have found the following to behelpful with children that have some of the unique feedingdifficulties that are shared with Kabuki Syndrome: 1) When a childhas difficulties latching onto the nipple, an orthopedic nipple can behelpful since it gives more oral awareness for the baby to assist withlatching on; 2) If the child does not demonstrate a tongue grooveposture to anchor the nipple then a firm, cylinder-shaped nipple isuseful; 3) Several specialized nursing devices for children with cleftpalates are on the market such as the Haberman Feeder and thePigeon; 4) Using a flat plastic spoon such as the maroon spoon, canassist with beginning spoon feeding with a child that has difficultieswith lip closure and retraction movement; 5) Use of an Ark probe ora chewy tool can assist in promoting chewing and/or rotary jawmovement.
In closing, I hope that this article has been useful for families with achild who has been diagnosed with Kabuki Syndrome and feedingand/or swallowing difficulties. The information is intended to assistyou in your incredible journey with your child and to bring some ofthe joy back to mealtime. For further questions you may contact meat [email protected].
- 9 -SOS....Continued from page 8
R – rising O – over C – challenges K – is the key Y – to your success
Growing up, this person dreamed of becoming an actor & writer. He had a clear vision of his goals and hisabilities. In college, he studied drama & began writing screenplays, but left school early for New York. He auditionedfor almost every casting agent in town, but had little success. His first break came in 1974, when he played a lead in &received a writing credit for “The Lords of Flatbush.” With the money he had earned, he headed for Hollywood, butagain found few parts. He created a prizefighter in a script he had written. He knew it was good & determined to playthe lead part himself. Producers showed interest, but they wanted a known actor in the lead. This actor held out for hisdream, and his perseverance paid off. His movie received 8 Academy Award nominations and won the Oscar for BestPicture of 1976. Know who I’m talking about? Sylvester Stalone - Rocky.

Haberman Special Needs FeederOne-way valve for cleft lip and/or palate, adjustable flow rate, Straightshape, Variable flow rate (slow, medium, fast), firm feel, composition -silicone
Maroon SpoonShallow bowl promotes removal of food from spoon, can be usedfor dry stimulation as early as 3 months. Age range: small: 4+months, large: 6+ months.Available at: Ark Therapeutics Services and Super Duper, Inc.
Gidge
Gadg
et sts
Chewy TubeOral motor stimulation to practicing chewing and biting skills; also used as an aid to inhibit grinding or oral
sensory motor stimulation.Available at: Ark Therapeutic Services and Talk Tools Therapy
ARK ProbeStrengthens the jaw; flat biting surface with ruby texture. Helps to stimulate up./down jaw movement.Available at: Ark Therapeutic Services and Talk Tools Therapy
Z-VibeAdds vibration to ARK Probe; different textures available in tips.Available at: Ark Therapeutic Services and Talk Tools Therapy
- 10
Hi! My name is Robert Tagliaferro. I live with my mom and dad in Long Valley, New Jersey and I amgoing into 8th grade. About fifteen years ago I was born with Kabuki Syndrome. When I was small my parentstell me I did things slower than other kids., like I walked when I was two years old. I’m still a little behind the other kids,but it’s not so obvious because I stayed back in 1st grade. A lot of the kids my own age are bigger than me, but that’s OK My favorite band right now is The Beatles. I got Beatles Rockband for Wii for my birthday last year. I really enjoyplaying it. I also like to perform whenever I can. I go to a theater camp during thesummers and put on shows with the other kids. It’s a lot of fun. Another favoritething I like is listening to my music in my room and putting on shows. It’s how Irelax. Some days I need it more than others. Two years ago I got a puppy to raise for The Seeing Eye. Her name is Jadeand she is a Golden Retriever. We raised her for about a year before she wentback to The Seeing Eye to be trained to be a Guide Dog. But, much to mysurprise Jade did not pass, so we got to keep her! Now we are raising anotherone. She’s a golden retriever too and her name is Napa. She’s very different fromJade and not afraid of anything. I think she’s going to pass because she has moreenergy and is more curious than Jade. Right now we are busy working togetherto get ready for our annual 4H county fair. Things I do outside of school are karate and swimming on Saturdays becausethat’s when I see my buddies. They go to different schools and I don’t get to see them everyday. I also take pianolessons at the School of Rock. I also volunteer at our church as an altar server. I absolutely love doing it! Just last month, I went away for my first sleep away. I went to Maine with my Uncle Don and my cousins, Matt andSteve. I was a little nervous because it was so far and it was for two weeks. But the time flew by and I had a lot of fun. Anyway, I just want everyone to know that I’m facing a lot of challenges just like you, but I want you to know that if youtry hard and put your mind to it you can do anything.!! Your friend, Robert
Me with my mom and dad
Pigeon Bottle & NippleOne-way valve for cleft lip and/or palate: notch positionedup during feeding. Straight shape, Y-cut/fast flow rate, firmon top, soft on bottom, composition - plastic
The Kabuki Journal is the newsletter of the Kabuki Syndrome Network. The purpose of this news-letter is toprovide information and support to individuals with Kabuki syndrome and their families. KSN will not knowinglyprint inaccurate or libelous material. KSN does not promote or endorse any treatment or professional. Consult yourprivate physicians / professionals for information and advice regarding medical and therapeutic treatments.
1 Kabuki Syndrome and Cancer in Two Patients – Am J. Med Genet A. June:152A(6):1536-9 2010 Tumino M., LicciardelloM., Sorge G., Cutrupi M.C., DiBenedetto F., Amoroso L., Catania R., Pennisi M., D’Amico S., Di Cataldo A.“Both hepatoblastoma and neuroblastoma are occasionally associated with congenital syndromes such as Beckwith-WiedemannSyndrome and Trisomy 18. There have been no reports of hepatoblastoma in patients with Kabuki Syndrome, whereas onepatient with neuoblastoma and this syndrome has been reported. In this paper we present two patients with Kabuki Syndromeand a neoplasm: a child of 6 years with hepatoblastoma and an infant, of 6 months affected with neuorblastoma.”
2 A Japanese Patient with Kabuki Syndrome and Unilateral Perisylvian Cortical Dysplasia - Brain Dev.,May 3 [Epub ahead of print] 2010 Yoshioka S., Takano T., Matsuwake K., Sokada T., Takeuchi Y.“We report a case of Kabuki Syndrome with unilateral perisylvian cortical dysplasia. This two-year old boy was referred to ourhospital at 3 months of age for his growth retardation and muscle hypotonia. Because of his peculiar face, brachydactyly V andfingertip pad, we diagnosed him as having Kabuki Syndrome. His MRI revealed cortical dysplasia along the left sylvian fissure.However, neither epileptic seizures nor epileptiform discharges on electroencephalogram were observed. Cortical dysplasia is arelatively rare brain malformation among the central nervous system anomalies accompanying with this syndrome. We have to takeinto consideration the likely onset of epilepsy in this patient because it is one of the most frequent neurological consequences ofcortical dysplasia.”
3 Kabuki Syndrome - Ugeskr Laeger. 2010 May 3;172(18):1384-5. DANISH. Peterson R.B., Lindholm P., Bonde C.T.“A clinical case of the rare Kabuki Syndrome is described in a 2-year old boy. At the time of birth he was diagnosed with cleft palateand from the age of 6 months he presented with unusual facial features and slow psychomotoric development. At the age of 2, he hasno language and only minimal speech perception and is showing signs of growth retardation.”
4 Congenital Polymicrogyria Including the Perisylvian Region in Early Childhood - Congenit Anom (Kyoto), 2010 Mar;50(1):64-7, Takano T., Matsuwake K., Yoshioka S., Takeuchi Y.“Six pediatric cases including 4 infants with congenital polymicrogyria including the perisylvian region are presented herein. Theirclinical features were analyzed and compared with patients suffering from congenital bilateral perisylvian syndrome (CBPS). Twospecific abnormalities were diagnosed as accompanying disorders in two cases, namely Kabuki Syndrome and Peters’ anomaly. Inthe other 4 cases, the pathogenetic etiology was not elucidated...."
5 A Case of Kabuki Syndrome Admitted for Acute Diarrhea and Growth Retardation in a French Hospital in Tropical Area -Arch Pediatr. 2010 Feb. 4 May;17(5):588:93 FRENCH, Santiago J., Muszlak M., Goulois E., Ranaivoarivony V., Hebert J.C.,Lacombe D., Verloes A.“The authors report on a 6-month-old girl with Kabuki syndrome, admitted for acute diarrhoea and growth retardation at theMayotte hospital. From this case, they try to explain the way of understanding and management in front of dysmorphic features.”
6 Seizures and EEG Pattern in Kabuki Syndrome - Brain Dev. 2010 Jan.8 [Epub ahead of print], Lodi M., Chifari R., Parazzini C.,Viri M., Beccaria F., Lorenzetti M.E., Meloni M., Capovilla G., Romeo A.“...We analysed seizure characteristics and pattern EEG and clinical outcomes in eight KS patients. Results: All patients presentedwith focal seizures. A frontal epileptic status was present in two cases. ..”
7 Tapetoretinal Dystrophy and Unusual Facial Features in an 8-year-old boy - Ophthalmologe. 2010 Feb;107(2):182-5. GERMAN,Kramer S., Seitz B., Kasmann-Kellner B.“An 8-year-old boy showed multiple cardiovascular and urinogenital anomalies, neurological problems as well as endocrinologicalabnormalities even shortly after birth. The patient had ophthalmological peculiarities, such as eyelid cleft configuration, tapetoretinaldystrophy, retinal visual atrophy, early childhood converging strabismus with varying angle relationships, nystagmus, light sensitivityand substantial visual deficits. Finally a Kabuki syndrome could be confirmed by human genetic investigations (8q22-23 triplication).”
8 Hypoplastic Left Heart Syndrome in Patients with Kabuki Syndrome - Pediatr Cardiol. 2010 Jan;31(1):138-41. [Epub 2009,Dec.5]“The association of cardiac defects with Kabuki syndrome has been well described. The majority of these defects are isolated shuntlesions, conotruncal abnormalities, or various forms of arch obstruction. This report describes a series of three patients withhypoplastic left heart syndrome and Kabuki syndrome. The series illustrates the full spectrum of left-sided obstructive lesions andexpands the phenotype of cardiac defects associated with Kabuki syndrome.”
Medical Journal Articles