
2010 April Issue Of Md News
28
AVAILABLE ONLINE. PASS IT ON. TWINCITIES.MDNEWS.COM TWIN CITIES | April 2010 | ■ A BUSINESS & PRACTICE MANAGEMENT MAGAZINE | ABOUT PHYSICIANS | FROM PHYSICIANS | FOR PHYSICIANS ■ Opens New Pediatric Cardiovascular Center Children’s Hospitals and Clinics of Minnesota REVIEW ONLY © 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
-
Upload
hsharrington -
Category
Documents
-
view
199 -
download
1
description
Transcript of 2010 April Issue Of Md News

AVAILABLE ONLINE. PASS IT ON.
T W I N C I T I E S . M D N E W S . C O M
TWIN CITIES | April 2010 |
! A BUSINESS & PRACTICE MANAGEMENT MAGAZINE | ABOUT PHYSICIANS | FROM PHYSICIANS | FOR PHYSICIANS !
Opens New Pediatric Cardiovascular Center
Children’s Hospitals and Clinics of MinnesotaREVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ +++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ +++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++++++
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

Twin Cities MD NEWS ! APRIL 2010 | 1""TWINCITIES.MDNEWS.COM
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ +++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ +++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++++++
Apr i l2010
TWIN CITIES
implanted fi ve pediatric patients with the device — two of which have now returned home and are enjoying a normal
implanted fi ve pediatric patients with the device — two
Medical DevicesCorporation, Inc. and Medical Director
Neurodiagnostic Center and Washoe
in Reno, NV, is a pediatric and adult
developed his love for those disciplines after reading books by Freud and other authors of psychoanalytical books as a ’s and medical degrees from the University of Rochester School of Medicine in Rochester, NY, pediatrics and child psychiatry at Massachusetts General Hospital in Boston, MA, and in child and adult neurology, as well as pediatrics at the Albert Einstein College of Medicine of
After completing a fellowship in pediatric neurology in Vancouver, British Columbia, Dr. Torch became the fi rst pediatric neurologist in Nevada when he accepted a position at the University of Nevada School of Medicine in Reno in 1979. He opened the Neurodevelopmental and Neurodiagnostic Center after spend-ing fi ve years at the university and later developed the Washoe Sleep Disorder Center. Today, both practices serve
“As someone trying to understand the mechanisms of the mind-brain relationship, Eye-Com has helped connect the original passions I had as a youngster,”
FEATURESCHILDREN’S HOSPITALS AND CLINICS OF MINNESOTA OPENS NEW PEDIATRIC CARDIOVASCULAR CENTER
6The new, state-of-the-art Pediatric Cardiovascular Center of Children’s
Hospitals and Clinics of Minnesota features cutting-edge technology and
revolutionized quality of care standards.EYES ON THE FUTURE
16William Torch, M.D., M.S., has developed eye-tracking technology — which uses micro-cameras to electronically monitor eye-lid and pupil
activity — that has evolved from a simple system constructed with parts
found at RadioShack to a sophisticated device with myriad applications
in medicine and other industries. REVOLUTIONARY MEDICAL DEVICES 20
In this issue of MD News, we take a look at three medical devices — the
iUniG2, HeartMate II and MASTERGRAFT Strip — that are transform-
ing the approach to treating certain medical conditionsDEPARTMENTSTHAT’S NEWS
4AUDIOLOGY
5Q&A
10THE SPINAL COLUMN
12PRACTICE MANAGEMENT
14CURRENT TOPICS
22ETHICS
24 ON THE COVERL-R: Charles M. Baker, MD, medical director of cardiology at Children’s, David Dassenko, MD, pediatric anesthesiologist and medical director of the cardiovascular center at Children’s, and David Overman, MD, FACS, FAAP, pediatric cardiothoracic surgeon at The Children’s Heart Clinic and Children’s Hospitals and Clinics of Minnesota all stand in the new Cardiovascular Center that recently opened at Children’s Hospitals and Clinics of Minnesota.
6
2016
COV
ER P
HO
TOCO
URT
ESY
OF
CHIL
DR
EN’S
HO
SPIT
ALS
AN
D C
LIN
ICS
OF
MIN
NES
OTA
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

2 | Twin Cities MD NEWS ! APRIL 2010 TWINCITIES.MDNEWS.COM
++++++++++++++++++++++++++++ ++++ ++++++++++++++++++++++++++++++
FROM THE PUBLISHER "
WW E L C O M E T O T H E
April edition of MD News. As the weather warms up
and summer is right around the corner, I just want to thank you for being a dedicated reader of our publication this year. If you have any article ideas or thoughts about MD News, I would love to hear about them. I am always available to answer questions and brainstorm ideas, as I want this magazine to be an intriguing and informative read for you.
I am excited to share with you the new Pediatric Cardiovascular Center that has just opened at Children’s Hospitals and Clinics of Minnesota in this month’s cover story. You will not want to miss reading how visions and years of planning have developed into a world-class center and how patients and physicians are seeing benefits already!
In this issue, we also take a look at various medical device advances that are beginning to reshape physicians’ abilities to help patients in the realm of orthope-dics, cardiology and spine surgery. The medical device feature introduces you to a new unicompartmental knee resurfacing device, an intracorporeal ventricular assist device for pediatric patients and a new ceramic scaffold to be used in spinal fusion procedures.
We also learn about a new technology that measures eye lid and pupil activity — the Eye Com 7. This revolutionary technology has the potential for a myriad of applications and is already being investigated for uses by the U.S. military and the U.S. Department of Transportation. You can read more about William Torch’s Eye-Com invention inside.
Also in this issue of MD News, you’ll find updates on the latest medical studies and research findings, pointers for managing your practice and a unique look at what is happening in the local medical field.
Thanks for reading,
Troy AndersonP U B L I S H E R
Publisher: Troy Anderson
Photographer: David Ginsberg
Contributing Writers: Adrienne Foley, Dr. Stefano Sinicroi____________________________________
Chief Executive Officer and
Executive Editor: David McDonald
President: Tony Young
Chief Operating Officer: Ann Farmer
Chief Financial Officer: Webster Andrews
Exec. Vice President
of Business Development: Jason Provonsha
Exec. Vice President
of Creative Services: J. Kevin Tugman
Vice President of
Marketing Development: Jason Skinner
Vice President, MIS: Eric Hibbs _____________________________________
Managing Editor: Hillary Myers
Founder: Robert J. Brennan
Market Development Managers: Jared Barnes, Betsy Skiles, Bill Staley
Senior Closing Administrator: Joanna Nash
Closing Administrator: Brian Shakley
Design Production Manager: Tanna Kempe
Editorial Manager: Shannon Wisbon
Production Coordinator: Kristen Gantler
Creative Services: David Andrews, Teneara Faw, Jessica Grogan, Travis Knight, Monika Bliss Morris, Katie Myles, Hope Shores, Michael Simmons
Controller: Grady Oakley
Financial Services: Julie Churay, Doug Condra, Lori Elliott
Manager of Human Resources: Carrie Hildreth_______________________________________MD News is published by Sunshine Media, Inc.735 Broad Street, Suite 708 Chattanooga, TN 37402 (423) 266-3234 | sunshinemedia.com
Although every precaution is taken to ensure accuracy of published materials, MD News cannot be held responsible for opinions expressed or facts supplied by its authors. Copyright 2010, Sunshine Media, Inc. All rights reserved. Reproduction in whole or in part without written permission is prohibited.
P O S T M A S T E R : Please send notices on Form 3579 to 735 Broad Street, Suite 708, Chattanooga, TN 37402
Advertise in MD NewsFor more information on advertising in the MD News Twin Cities edition, call Publisher, Troy Anderson at (612) 396-1455 or e-mail [email protected].
Contact Information Send press releases and all other information related to this local edition of MD News to [email protected] or via fax to (952) 679-4974.
Twin Cities
05-838
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

Twin Cities MD NEWS ! APRIL 2010 | 3""TWINCITIES.MDNEWS.COM
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

4 | Twin Cities MD NEWS ! APRIL 2010 TWINCITIES.MDNEWS.COM
+ + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + ++ + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + +
THAT’SNEWS """
Reductions in Daily Salt IntakeCould Prevent 100,000 Heart Attacks Each YearA RECENT STUDY published in the online edition of the New England Journal of Medicine revealed that 100,000 heart attacks and 92,000 deaths could be prevented each year if Americans would eliminate as little as 3 grams of salt from their daily diet.
Researchers from the University of California, San Francisco, Stanford University Medical Center and Columbia University Medical Center conducted the study by using the coronary heart disease (CHD) policy model to project possible benefits from salt reduction.
The CHD policy model found that reducing salt intake by 3 grams (1,200 mg of sodium) could result in 11% fewer new cases of heart disease, 13% fewer heart attacks, 8% fewer strokes and 4% fewer deaths. The projected health care savings for the United States would be $24 billion.
Because most Americans’ daily salt intake comes from processed foods, researchers are urging the food industry to reduce the amount of salt used to make these foods. !
Link Between Mild Chronic Obstructive Pulmonary Disease and Heart FunctionHEART FAILURE IN patients with severe chronic obstructive pulmonary disease (COPD) has been well documented; however, researchers at Columbia University Medical Center have recently found that mild COPD — even in patients presenting no symptoms — can cause diminished heart function.
Researchers evaluated 2,816 mostly healthy adults who had a median age of 61. Participants were part of the Multi-Ethnic Study of Atherosclerosis (MESA) lung study, an extension of the MESA. Through the use of magnetic resonance imaging and computed tomography scans, researchers found that even mild cases of COPD cause subclinical reductions in heart function. The link between mild COPD and diminished heart function was found to be strongest in smokers.
One in five Americans suffer from COPD, but many people are not aware that they have the disease. These new results demonstrate that COPD can affect the heart’s ability to pump blood effectively long before doctors once suspected — in some cases, even before COPD has been diagnosed.
PATIENTS SUFFERING FROM type 2 diabetes may have a harder time controlling their glucose levels if they suffer from untreated obstructive sleep apnea.
Sixty patients were included in a final analysis of results obtained from a study at the University of Chicago, where researchers found that people who suffer from severe obstructive sleep apnea have poor glucose control.
Researchers evaluated the patients’ medical histories as well as tested their sleep/wake cycles for five days through use of a wrist actigraphy and a self-reported sleep log. Each patient also underwent an overnight polysomnogram to check for obstructive sleep apnea. A blood sample was obtained for hemoglobin A1c measurement to assess the patients’ glucose control.
Researchers found that 38% of the study sample suffered from mild obstructive sleep apnea, 25% had moderate sleep apnea and 13% suffered from severe sleep apnea. Researchers also found that the more severe the sleep apnea, the less the patient was able to control his or her glucose level.
Findings indicate that reducing the severity of obstruc-tive sleep apnea may help improve glycemic control. Thus, researchers are recommending that type 2 diabetes patients be screened for obstructive sleep apnea for improved diabetes management. !
Obstructive Sleep Apnea May Lead to Poor Glucose Control
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

Twin Cities MD NEWS ! APRIL 2010 | 5""TWINCITIES.MDNEWS.COM
Help for Hearing Loss Patients
D ESIGNED TO HELP patients with mild to moderate hearing loss who were frustrated with current hearing aid options, the Lyric Hearing System is the first hearing aid that is 100% invisible. At Audiology Concepts in Edina, audiologist Paula Schwartz, Au.D., is proud to offer this unique,
technologically advanced hearing device to her patients.The Lyric hearing system’s technology and design allow the device to be inserted
deeply into the ear canal, providing many benefits for patients, including extended-wear time that allows the device to be worn 24 hours a day for up to four months.
“The Lyric device appeals to a group of people who might not otherwise treat their hearing loss,” says Dr. Schwartz. “For those people concerned with the stigma of wearing a hearing aid, Lyric allows them to treat their hearing loss without worrying about the cosmetic appearance of a hearing aid. Also, because the device can be worn 24 hours a day, there is added patient convenience. Patients do not have to worry about removing the device for certain activities or changing hearing aid batteries.”
How It WorksBiocompatible soft foam seals contour to the ear canal, and proprietary coating
technology protects the device from moisture and earwax, allowing it to be worn through all of the patient’s activities, including bathing, exercising and sleeping. There is no surgery involved in the insertion process and no anesthesia required.
The Lyric Hearing System promotes improved sound quality because the device lies within 4 millimeters of the eardrum. This deep canal placement of the Lyric Hearing System device allows for improved directionality and localization because the outer part of the ear is able to interact fully with incoming sounds. This interaction allows users to perceive the sound’s direction and location within their environment.
The Lyric Hearing system device also has a minimized occlusion effect. Because the device sits deeply within the bony portion of the eardrum, vibrations within the ear canal are reduced. Also, the Lyric Hearing System does not lie as close to the cartilaginous portion of the ear as traditional hearing aids. This unique design allows the device to stay in place, preventing sound waves from escaping through gaps between the cartilage and hearing aid, which can cause feedback.
A Health Care Approach to Hearing LossAt Audiology Concepts, physicians can refer their patients for full audiology services,
and unlike traditional chain hearing aid dispensers, Audiology Concepts takes a health care approach to hearing loss patients, involving the patient’s primary care physician in the care plan.
“We try to keep the patient’s hearing health managed within the context of his or her overall health,” says Dr. Schwartz. “By working with the patient’s primary care physician, we are keeping the patient’s best interest in mind.”
To refer a patient to Audiology Concepts, call (952) 831-4222. !
++++++++++++++++++ ++++ ++++++++++++++++++++
# AUDIOLOGY
When I refer patients to Audiology
Concepts, I am confident they will
get second-to-none professional
quality and service. The patient’s
well-being and satisfaction are
always given the highest priority. Dr. Schwartz’s
superior knowledge of
hearing instrument technology
results in optimal treatment plans and compliant
patients.— Kurt Brattain, M.D., family practice physician
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

6 | Twin Cities MD NEWS ! APRIL 2010 TWINCITIES.MDNEWS.COM
Cardiovascular Center rather than going through the hospital’s main admissions process.
“This new center will allow us to work together to accomplish our goals more effectively and efficiently,” says Charles M. Baker, M.D., Medical Director of Cardiology, Children’s Heart Clinic and Children’s Hospitals and Clinics of Minnesota. “The space gives us flexibility and provides us with extra capacity to improve patient care.”
Co-location of services also means greatly reducing postsurgical transportation time. “It’s been demonstrated statistically that transport is the most hazardous time of any patient’s hospitalization,” says David Dassenko, M.D., pediatric anesthesiologist and Medical Director of the Cardiovascular Center at Children’s Hospitals and Clinics of Minnesota.
At some hospitals, pediatric cardiac surgical patients have to be transported through a series of hallways and elevators after opera-tions, which adds to the risk of the procedure.
“In our old intensive care unit [ICU] we were lucky to have the cardiovascular ICU and operating rooms [OR] on the same floor, minimizing transport time. We feel it is vital to maintain that same close geographic relationship between our cardiac operating area and the cardiac ICU in our new unit,” he says. “At the new center, our patients can come from the operating room in our new unit and be in the ICU in about a minute’s time.”
Dr. Overman adds, “Co-location of these services minimizes disruption of a patient’s care because the care team is always the same; it also improves the family experience because they don’t have to move to different rooms. The patient arrives on the fourth floor
PHO
TOS
COU
RTES
Y O
F CH
ILD
REN
’S H
OSP
ITA
LS A
ND
CLI
NIC
S O
F M
INN
ESO
TA
AFTER YEARS OF planning, from initial dreams captured on scratch paper to detailed concepts imagined by a multidisciplinary team of cardiovascular experts, Children’s Hospitals and Clinics of Minnesota recently
opened the doors to its new pediatric Cardiovascular Center, the only dedicated center of its kind in the Upper Midwest.
“The field of pediatric cardiovascular diseases has been marked for the last 10 or 15 years by many advances in outcomes, the understanding of the disease and an understanding that the care is mandatorily multidisciplinary,” says David Overman, M.D., FACS, FAAP, pediatric cardiothoracic surgeon, Children’s Heart Clinic and Children’s Hospitals and Clinics of Minnesota.
“In addition, there are hybrid approaches that combine conven-tional surgical procedures and catheter-based interventions, which we’ve been doing for several years at Children’s, but in a physical environment that wasn’t as optimally structured,” says Dr. Overman.
The new Cardiovascular Center brings together the various factors of patient safety, family and patient experience and technological demands into a single location.
Co-Location of ServicesPart of what makes the center unique is its ability to house all
pediatric cardiac services — including inpatient care, diagnostics, outpatient and inpatient cardiac catheterization, surgical procedures, follow-up procedures and more — in one location, all on the hospital’s fourth floor. Most pediatric cardiac patients receiving either inpatient or outpatient treatment are admitted to and discharged from the
COVER FEATURE
Eric Carlson, now 6 years old, was diagnosed with hypoplastic left heart syndrome at Children’s Hospitals and Clinics of Minnesota when his mother was just 20 weeks pregnant. After having successful surgeries, he now spends afternoons with his friends.
Children’s Hospitals and Clinics of Minnesota Opens New Pediatric Cardiovascular CenterWORLD-CLASS CENTER IS FIRST OF ITS KIND IN THE UPPER MIDWESTBy Adrienne Foley
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

Twin Cities MD NEWS ! APRIL 2010 | 7""TWINCITIES.MDNEWS.COM
and leaves from the fourth floor. They don’t have to move about the hospital to receive their care.”
State-of-the-Art Technology, Including a Hybrid Operating Suite
The new Cardiovascular Center offers the highest level of technol-ogy available in the region and includes three procedural spaces: a standard cardiac OR, a cardiac hybrid operating room and a cardiac catheterization/electrophysiology lab.
The new ORs feature integration with the video system of the hospital’s information system and the radiology system, which allows physicians to request and view any previous diagnostic studies or patient-related dictation on demand.
In addition, co-location of the operating rooms and catheterization lab allows cardiologists and surgeons to immediately confer on patient cases.
“If a cardiologist wants a surgeon’s opinion, he can call into the OR, and we can display the real-time data into that room so a surgeon can weigh in on what the cardiologist is doing just two doors down,” says Dr. Dassenko. “Having all of the hospital information systems — charts, X-rays, moving pictures from caths and CT scans — able to be routed into that room for display at any time during surgery is very unique,” he adds.
Dr. Baker also adds that the new X-Ray equipment in the cath lab and hybrid operating room offers the latest diagnostic imaging to patients, which reduces radiation doses while maintaining optimal imaging quality.
Also unique is the hybrid operating suite, which combines a fully equipped surgical suite with a state-of-the-art cardiac catheterization laboratory in the same room. It is only one of a handful in a dedicated pediatric hospital in the U.S.
The hybrid approach encompasses the most advanced technology for catheterization and open-heart surgical procedures and allows the surgeon and cardiologist to collaborate on the safest and least invasive approach readily available to treat the patient.
At more than 800 square feet each, the new ORs are also larger in size. “The cost per foot to build operating rooms is incredibly expensive, so we feel blessed that our hospital was able to build them,” says Dr. Dassenko. “These are probably some of the largest ORs anywhere in the country because we factored into account any additional technology that may be developed five to 10 years from now that we’ll need space for.”
Family Considerations Factored Into New DesignTaking into consideration the needs of a patient’s family was also
an integral part in planning the new Cardiovascular Center.“We are fortunate that all of our new rooms face north so patients
and families have a view of the downtown Minneapolis skyline with lots of natural light,” says Dr. Dassenko. Compared to the old unit, patient rooms are double in size and include a defined parent space with sofa that turns into queen-sized bed, a bathroom for families, an entertainment system and Wi-Fi access.
Children’s Hospitals and Clinics of Minnesota also partnered with Best Buy recently to install the first in-hospital Geek Squad precinct,
which provides free technology support to patients and their families.“The Internet and social media are now more important than a
phone. We wanted to incorporate those means of communication so parents can stay connected to family, work and others while at the hospital,” says Dr. Dassenko. “They can also call on the Geek Squad if they need assistance with technology, because that’s their window to the world these days.”
Our People Make the DifferenceWhile the world-class facility is an important part of creating a
center of excellence, both Drs. Dassenko and Overman agree that it’s the people who set the Cardiovascular Center apart.
“Ultimately how your program performs is based on its people,” says Dr. Dassenko. “You have to have excellence in every area from surgery, anesthesia and cardiology to bedside nursing care. In creating our cornerstone program (a Center of Excellence), we’re ensuring our program remains among the best in the country because of the dedication of our staff and their expertise in cardiovascular care. If you look at our national comparative data, our clinical outcomes are outstanding, yet we will continuously strive to keep improving them.”
Staffing changes for the Cardiovascular Center include: + Consistent and experienced nursing care — Patients in the Cardiovascular Center will be admitted to and discharged from the same room, giving patients the continuum of nursing throughout their stay.
+ Dedicated cardiovascular intensive care unit physicians — Children’s Hospitals and Clinics of Minnesota is the only center in the region to provide on-site cardiac intensivists dedicated to caring for and monitoring patients 24/7.
Six-year-old Eric also enjoys riding his new bike.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

8 | Twin Cities MD NEWS ! APRIL 2010 TWINCITIES.MDNEWS.COM
BY THE NUMBERS
+ 12 pediatric cardiologists + 2 pediatric cardiovascular surgeons + 5 cardiac intensivists available 24/7 + nurse practitioner + surgical physician assistant + 19 patient beds + 3 procedural operating suites + 497 pediatric surgical cases in 2008 + 348 cardiac cath-based cases in 2008
+ A dedicated pain specialist — Traditionally, pain for cardiac patients is handled by critical care professionals, who serve all specialties of the hospital. Children’s Hospitals and Clinics of Minnesota will integrate pain service into its cardiac care with the addition of a pain specialist dedicated to pediatric cardiac patients (implementation in the near future).
Outstanding OutcomesWhile the Cardiovascular Center provides care for newborn
through adult patients with congenital heart disease, nearly half of patient volume is newborn.
Such was the case for Christina and Stephen Carlson of Chanhassen, whose son Eric, now 6, was diagnosed with hypoplastic left heart syndrome (HLHS) while Christina was just 20 weeks pregnant with him.
HLHS is the third most common serious congenital heart defect and is often fatal. According to Dr. Overman, national survival rates for surgical therapy historically have been somewhere between 50% to 65% through a three-stage surgical strategy.
“For the last three years in our center, survival for stage one pal-liation for HLHS has been 100%,” he says. Eric was no exception. He underwent the first and most serious surgery when he was 6 days old.
“Because he was diagnosed in utero, the doctors were ready to take care of him the minute he was born,” says Christina.
Compared to other programs in the nation who perform similar complex catheter-based or surgical cardiovascular interventions, Children’s Hospitals and Clinics of Minnesota has among the best outcomes.
“In fact, in 2008, amongst the most complex category of neonatal surgeries as defined by the Risk Adjustment in Congenital Heart Surgery system, we achieved the lowest mortality of any center in the Society of Thoracic Surgeon’s Congenital Heart Surgery Database,” says Dr. Overman. “The introduction of hybrid therapy for HLHS is
a promising advance, and we will have that capability on top of these outstanding surgical results going forward.”
In addition to technological advances, he attributes this success to a focused professional commitment on the part of the providers, nurses and ancillary staff to that patient population, the volume of patients seen and therefore the experience of all the caregivers involved.
“I think the fact that the care is delivered by experienced board-certified physicians is an advantage that we enjoy over a traditional academic model where bedside care may be rendered by a resident or fellow,” he says. “In this field, for better or for worse, the margin of error is narrow, and the price for a mistake is very high. Ours is a clinical discipline where experience and hands-on, multidisciplinary involvement by the most knowledgeable providers makes a difference.”
“The medical care we received was second to none. Their philoso-phy is that the physicians and parents are all on the same team. That team collaboration made a difference to us,” says Christina.
Communication With Family, Referring Physicians Is Key to Program’s Success
According to Dr. Overman, the one defining characteristic of the cardiovascular program and institution historically has been the tight circle of communication with families and referring physicians.
“Communication is something we take considerable pride in,” he says. “This practice has always been a standard bearer of that family and patient satisfaction metric, as measured by annual payor surveys. Simply put, I would say a referring physician can know that they will have frequent and meaningful contact with the physicians of the Cardiovascular Center about the progress of their patients from the time of admission, perioperatively and periodically until discharge.”
For a cardiac-related referral or consultation, please call Children’s Heart Clinic at 1-800-938-0301, or visit www.childrensmn.org. !
The new Pediatric Cardiovascular Center offers the highest level of technology available in the region and includes three procedural spaces: a standard operating room, a hybrid operating room and a cardiac catheterization lab.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

1 0 | Twin Cities MD NEWS ! APRIL 2010 TWINCITIES.MDNEWS.COM
M D N E W S R E C E N T LY sat down with Juan M . L a t o r r e ,
M.D., who is board certi-fied in physical medicine a nd reh a bi l i t a t ion a nd
spinal cord injury medicine, at St. David’s Rehabilitation
Hospita l in Aust in, T X, to discuss some of the challenges,
+ + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + ++ + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + ++ + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + ++ + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + ++ + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + +
Advances in Spinal Rehabilitation Therapy
new technologies and breakthroughs in rehabilitation.
P r ior t o j o i n i n g St . D a v id ’s Rehabilitation in Austin, Dr. Latorre ser ved as the spina l cord injur y program director at The Institute for Rehabilitation and Research Memorial Hermann Hospital in Houston. He has also served as The University of Texas Spinal Cord Injury Fellowship Director since 2004.
QWhat are some common misconceptions about treating patients with
spinal cord injuries?
Dr. Latorre: Many people believe there’s not much that can be done, when in fact these patients can regain a lot of lost independence. Spine injury patients face many challenges. Depending on the sever-ity of injury, other systems of the body are
+++++++++++++++++++++++++++++++++++++++++++++++++++ +++++++++++++++++++++++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++ ++++++++++++++++++++++++++++++ +++++++++++++++++++++++++++++++++++++++++++++++++++ +++++++++++++++++++++++++++++++++++++++++++++++++++
Q&A """
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

Twin Cities MD NEWS ! APRIL 2010 | 1 1""TWINCITIES.MDNEWS.COM
also affected, such as gastrointestinal and genitourinary. These patients lose some of the most basic functions. Rehabilitation focuses on retraining these systems to enhance a patient’s control through methods such as self-catheterization of the bladder or digital stimulation to gain control of the bowels. A patient’s quality of life is significantly affected by how these systems are managed. Many people tend to think patients with spinal cord injuries suffer and can’t be happy, although a great number of patients lead happy and fulfilling lives after completing comprehensive rehabilitation. My work can be challenging and difficult, but it is extremely gratifying. Seeing a patient’s achievements is extremely rewarding.
QWhat are some of the chal-lenges of treating spinal cord injuries?
Dr. Latorre: While patients with spinal cord injuries often focus on regaining the ability to walk, they also need to focus on regaining their independence, as they may have lost some of their most basic functions. Patience can be a challenge, as healing and recovery do not happen overnight. While people with spinal cord injuries may see neurological recovery after three to six months, it can be an obstacle to understand that there are both short- and long-term goals to focus on.
QHave there been any major advances recently in the field of rehabilitation for
patients with spinal cord injuries?
Dr. Latorre: A wide variety of spe-cialists care for patients with limited functions that we often take for granted, such as bladder and bowel function or even breathing. Current technology may allow some patients to come off a ventilator with diaphragmatic pacing. New power wheelchairs give patients better control and independence. Voice-operated switches and other assisted
technologies give patients other ways to control their environment and regain lost independence.As a specialist in rehabilitation for patients with spinal cord injuries, it’s really impor-tant to look at what has been done in the research arena. We need to ensure these results can transfer from the bench to the bedside to determine how we can reduce the effects of damage and inflammation, save nerve cells and
encourage correct neurological function. We do comprehensive rehabilitation and take a multidisciplinary approach to care. These patients are best served by undergoing rehabilitation where a l l phys ic ians , nurses and sta f f members are familiar with these kinds of injuries. !
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

1 2 | Twin Cities MD NEWS ! APRIL 2010 TWINCITIES.MDNEWS.COM
Total Disc Replacement FOR THE CERVICAL SPINEBy Dr. Stefano Sinicropi, Midwest Spine Institute
O THER JOINT REPLACEMENT procedures eventually followed including shoulder, elbow, ankle and other smaller joints of the hand. Large volumes of these procedures are performed at both hospital
and outpatient centers to correct painful arthritic conditions of the joints. Until recently however, arthroplasty of the spine (or artificial disc replacement), has not been a viable option in the United States.
The main challenge facing surgeons and engineers was the development of a suitable replacement for the intervertebral discs. Spinal disc replacements needed to have the ability to mimic a very complex range of movement and be safe to implant. Additionally, they had to be reliable and long lasting. Over the course of prior decades, dramatic improvements have been made in the development of the artificial disc. There are now several artificial disc replacements available for both the cervical and lumbar spine, and they are currently being offered to appropriate candidates in the United States.
Neck pain and arm pain can have a severe and sometimes even devastating effect on a patient’s quality of life. Symptoms may result from compression of the spinal nerves, spinal cord or from the disc itself. Typically, if standard conservative treat-ments are ineffective or the patient becomes unable to perform activities of daily living due to progression of pain or neurological symptoms, surgical intervention is indicated. Anterior cervical discectomy and fusion is currently considered definitive treatment for symptomatic cervical degenerative disc disease. Some disadvantages may include loss of flexibility, alteration of biomechanics, and the development of adjacent segment disc degeneration. Although the majority of patients will have good
to excellent results from cervical fusions, over time, symptomatic disc problems surrounding the fusion may occur.
Disc replacement in the cervical spine is a relatively new alternative treatment option for cervical disc disease and injury in certain patients and may possibly reduce the known shortcomings of fusion. Artificial disc replacement allows for motion preservation and near normal distribution of stress of the adjacent spine, possibly reducing damage to nearby discs and joints.
Recovery from cervical artificial disc replacement can be very rapid and bracing is generally not necessary. A typical patient may be released to most activities (including high-impact activi-ties) after the wound is healed. Imaging studies are generally performed postoperatively to ensure that the range of motion has been preserved and that there are no implant complications. Subsequently, X-rays are taken much less frequently because physicians are not waiting for “fusion” to occur.
The two cervical artificial discs that have been approved for use in the United States include the Prestige Cervical Disc System (Medtronic) and the ProDisc-C (Synthes Spine, Inc.). Both were
+++++++++++++++++++++++++++ ++++ +++++++++++++++++++++++++++++
THE SPINAL COLUMN "
HIP AND KNEE JOINT REPLACEMENT SURGERY OR ARTHROPLASTY HAS BECOME ROUTINE SINCE ITS INCEPTION IN THE EARLY 1960S WITH A HIGH DEGREE OF PATIENT SATISFACTION.
PHO
TOS
BY D
AVID
GIN
SBER
G
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

Twin Cities MD NEWS ! APRIL 2010 | 1 3""TWINCITIES.MDNEWS.COM
approved for usage in 2007. They are both indicated in the reconstruction of the disc from C3-C7 following single-level discectomy for intractable symptomatic cervical disc disease, radiculopathy and/or myelopathy. The Prestige disc features a metal on metal articulation while the Prodisc-C has a polyethylene spacer. The two implants have both demonstrated safety, durability and excellent clinical results in U.S. trials.
Medtronic’s Prestige Cervical Disc System has been studied rigorously. In a Level 1, multicenter prospective random-ized controlled 32-site study that involved 541 patients (2002-2004), a comparison was done between cervical disc replace-ment and anterior fusion (ACDF). Patients in the study had to be at least 18 years of age with documented cervical degenera-tive conditions/symptoms with associated neurologic involvement and had to fail at least six weeks of nonsurgical treatment. At the 12- and 24-month follow-up points, the disc replacement group reported more improvement in their neck pain and a greater ability to go about their daily activities than the fusion group. Sagittal (front and back) angular motion was maintained from 7.55º preoperatively to 7.59º at 12 and 24 months postoperatively. Patients undergoing disc replacement had
median return to work that was 16 days faster than the fusion group. There were no implant failures or migrations. Fewer patients in the replacement group required secondary surgical procedures. The most significant overall theme from this study was that the cervical fusion patients had excellent clinical results but the replacement patients did even better.
The ProDisc-C total disc replacement also underwent rigor-ous testing as part of FDA-regulated IDE clinical study. The prospective, randomized trial (13 centers) of 209 patients with symptomatic cervical disc disease at a single level from C3-C7 were randomized to receive either a total disc replacement or standard ACDF. Disc replacement patients demonstrated a significant improvement in pain and disability and required fewer re-operations than ACDF patients. Patients receiving disc replacement demonstrated a mean range of motion of 9.4° at the 24-month follow up, clearly demonstrating excellent motion-preservation.
With a continued increase in the number of artificial cervical disc replacements performed, indications have continued to expand. Many patients who have disc disease adjacent to a
previous fusion may become excellent candidates for cervical total disc replacement. The U.S. studies along with longer-term European experience demonstrate a role for cervical disc replacement in select patients. Currently, there are patients who travel overseas at significant expense seeking motion-preservation implants because multilevel total disc replacements occur in Europe but have not yet received FDA approval in the United States.
For FDA-approved single-level cervical artificial disc replace-ment, insurance acceptance has been slow. However, the success of disc replacement in selected cases and its cost-effectiveness may lead this procedure to eventually become an accepted standard of care for the treatment of symptomatic cervical disc disease.
For more information, please contact Midwest Spine Institute and Dr. Stefano Sinicropi at (651) 430-3800 or visit www.midwest-spineinstitute.com. !
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

1 4 | Twin Cities MD NEWS ! APRIL 2010 TWINCITIES.MDNEWS.COM
REDUCING TURNOVER AND
Increasing Employee Satisfaction
LOYAL , QUALIT Y EMPLOYEES are not only hard to come by; they’re difficult to replace. To en s u re you r pat ient s
are content, start with evaluating and maintaining the work satisfaction of your employees.
Staff turnover can hurt your practice more than you may think. Not only is it financially costly, but it also weighs on patient and employee satisfaction. According to an article published by the American Academy of Family
Physicians, a staff turnover rate of 20% or more within a five-year period is considered high.
To help reduce high staff turn over rates, physicians or office managers should ask themselves the following questions:
+ Have we created an attractive, positive work setting?
+ Are we hiring people who are well-qualified for the position, and are we training them sufficiently?
+ Do we have an effective line of com-munication set up for staff members?
+ Do we have a constructive, teamwork-style environment, where the staff support one another?
+ Does the staff feel that, as a whole, the practice values their opinions and suggestions?
A good way to evaluate the attitude of
+++++++++++++++++++++++++++++++ ++++ +++++++++++++++++++++++++++++++++
PRACTICE MANAGEMENT "
ALTHOUGH PATIENTS VISIT THEIR PHYSICIANS FOR MEDICAL ADVICE, IT CAN BE A PHYSICIAN’S STAFF THAT CAN MAKE OR BREAK A PATIENT EXPERIENCE.
See Page 18
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

Sunshine Media is proud to present Digital Editions, a state-of-the-art media solution that signifi cantly enhances the engagement, reach, and value of your presence in MD News magazine. These search-engine optimized, Flash-enabled Digital Editions take your message beyond the printed page, allowing your advertisement or feature article to be viewed 24/7 by anyone from anywhere in the world.
With Digital Editions, your target audience will enjoy the traditional “page fl ip” feel of a magazine, while deepening the reader experience and increasing your company or practice’s exposure exponentially via links to your website, e-mail address, and other valuable resources as featured within the publication.
To maximize the effectiveness of this new resource, each local Digital Edition will be prominently displayed on the home page of its website. The site also includes a Digital Editions archive so your message can be accessed indefi nitely by anyone in the world.
For more information on how you can appear within a Digital Edition of MD News magazine, or to view a sample of this state-of-the-art media solution, call your local MD News publisher or visit http://twincities.mdnews.com.
Digital Editions
readers take
action regarding a
product or service
90 percent of
the time, and over
76 percent visit
advertiser websites.
SOURCE: 2008 study by Texterity, Inc.
Contact Publisher:Troy Anderson
+++++++++++++++++++++++++++++++++
+++++++++++++++++++++++++++++++++
EXTENDING YOUR MESSAGE
W O R L D W I D E

1 6 | Twin Cities MD NEWS ! APRIL 2010 TWINCITIES.MDNEWS.COM
ONE SUCH FIGURE is William Torch, M.D., M.S., of Reno, NV, whose Eye-Com Biosenser, Communicator and Controller eye- and head-tracking technology — which uses micro-cameras to electronically monitor eyelid,
eye gaze and pupil activity — has evolved from a simple system constructed with parts found at RadioShack to a sophisticated device with myriad applications in medicine and other industries.
The Genesis and Evolution of the Eye-Com Biosensor
“I’m a researcher, and I have a passion for invention and fi nding solutions to problems,” says Dr. Torch, founder and Chairman of Eye-Com Corporation, Inc. and Medical Director of the Neurodevelopmental and Neurodiagnostic Center and Washoe Sleep Disorders Center, all located in Reno. “Several years ago, I was caring for a 28-year-old man named Glen who had developed a viral encephalomyelitis and was in a coma for a week and a half. He was maintained on a ventilator, and I thought he wouldn’t make it. One magical day, he opened his eyes, but he was unable to communicate aside from moving his eyes, blinking and crying. He and I developed a system of communication in which he blinked once for ‘yes’ and twice for ‘no,’ which inspired me to create a blink detector. I bought an infra-red emitter and matching detector at RadioShack and put together an electronic breadboard with the help of a friend. The system we devised contained a buzzer and an LED light, and when aimed at my eyes, I was able to create buzzing sounds and fl ashing lights through the system that represented the sounds of Morse code when I blinked. That device was the beginning of the Eye-Com Biosensor — Eye-Com 1.”
Dr. Torch founded Eye-Com Corporation in 1998, and the Eye-Com Biosensor is now in its ninth level of design , with each version seeking to solve problems created by its predecessors. With Eye-Com 3, Dr. Torch discovered that the blinks picked up by Eye-Com 2 could be transmitted as square waves to an electroencephalography machine. The use of a radio frequency transmitter attached to Eye-Com 4 allowed the wearer to transmit blink signals wirelessly through walls and doors to a remote site. Eye-Com 5 measured not only the frequency of blinks, but their duration, as well as the velocity of the eyelid’s up and down movement.
Eye-Com 6 took things a step further with its ability to measure the size of the pupil and its rate of constriction and dilation. The device also had the potential to find the center point of
the pupil and track it as it moved through all points of gaze. Dr. Torch demonstrated that the device could detect drowsiness and signs of inattention in children with attention defi cit disorder (ADD). Dr. Torch received several grants over the past decade the Centers for Disease Control and Prevention, the U.S. Army and the U.S. Departments of Transportation and Defense.
ApplicationsThe military has found several applications for Eye-Com 6,
including monitoring the eyes of helicopter pilots for fatigue, detect-ing signs of sleepiness induced by hypoxia in pilots fl ying at high altitudes and detecting signs of underwater fatigue, hypoxia and nitrogen narcosis when placed in the SCUBA masks of Navy SEALs.
A U.S. Department of Transportation (USDOT) study also dem-onstrated Eye-Com 6’s ability to monitor drivers of mass transport for signs of drowsiness using oculometrics. Most importantly, Eye-Com 6 was able to measure PERCLOS — the percentage of time one’s eyes are open or closed over a period of time — a new oculometric defi ned by the USDOT as the best biophysiological measure of drowsiness.
Eye-Com 7, the latest version of the technology, can be used not only for communicating with other people, but for controlling the cursor on a computer screen via eye-tracking algorithms. The device can even make a wheelchair travel where the wearer looks. Other current or potential applications for Eye-Com 7 identifi ed by Dr. Torch include:
+ tool for studying patients with epilepsy assistive communicator and controller tool for handicapped individuals
+ identifying ocular manifestations of ADD in children
+ identifying signs of post-traumatic stress disorder and traumatic brain injury
+ identifying the effects of medications, alcohol and illicit drugs
+ iris and security identifi cation
+ lie detector tool in forensic psychology
+ hands-free operation of medical, surgical and industrial tools
PIONEERING FIGURE
William Torch, M.D., M.S., founder and Chairman of Eye-Com Corporation, Inc. and Medical Director of the Neurodevelopmental and Neurodiagnostic Center and Washoe Sleep Disorder Center, all located in Reno, NV, is a pediatric and adult neurologist and child psychiatrist by training. The native New Yorker developed his love for those disciplines after reading books by Freud and other authors of psychoanalytical books as a teenager. He received his master’s and medical degrees from the University of Rochester School of Medicine in Rochester, NY, pediatrics and child psychiatry at Massachusetts General Hospital in Boston, MA, and in child and adult neurology, as well as pediatrics at the Albert Einstein College of Medicine of Yeshiva University, Bronx, NY.
After completing a fellowship in pediatric neurology in Vancouver, British Columbia, Dr. Torch became the fi rst pediatric neurologist in Nevada when he accepted a position at the University of Nevada School of Medicine in Reno in 1979. He opened the Neurodevelopmental and Neurodiagnostic Center after spend-ing fi ve years at the university and later developed the Washoe Sleep Disorder Center. Today, both practices serve pediatric and adult patients.
THE FUTURE OF MEDICINE IN THE NEW DECADE WILL BELONG TO THE MEN AND WOMEN WHO DRIVE TECHNOLOGY FORWARD THROUGH BIG IDEAS, METICULOUS RESEARCH AND TRIAL AND ERROR.
“As someone trying to understand the mechanisms of the mind-brain relationship, Eye-Com has helped connect the original passions I had as a youngster,” Dr. Torch says. “The most important thing to me is being able to improve the quality of life of my patients. Glen is still alive, and though he is triplegic, he now has full ability to communicate. He still ponders the meaning of his illness and wonders why he should be so affl icted. When I recently reminded him that he was the person who helped generate my thoughts about Eye-Com, he responded that those words and the thought behind those sentiments gave meaning to his life.”
For further information about the Eye-Com, please visit www.eyecomworld.com. !
FutureON THEEyes
TWINCITIES.MDNEWS.COM
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

Twin Cities MD NEWS ! APRIL 2010 | 1 7""TWINCITIES.MDNEWS.COM
ONE SUCH FIGURE is William Torch, M.D., M.S., of Reno, NV, whose Eye-Com Biosenser, Communicator and Controller eye- and head-tracking technology — which uses micro-cameras to electronically monitor eyelid,
eye gaze and pupil activity — has evolved from a simple system constructed with parts found at RadioShack to a sophisticated device with myriad applications in medicine and other industries.
The Genesis and Evolution of the Eye-Com Biosensor
“I’m a researcher, and I have a passion for invention and fi nding solutions to problems,” says Dr. Torch, founder and Chairman of Eye-Com Corporation, Inc. and Medical Director of the Neurodevelopmental and Neurodiagnostic Center and Washoe Sleep Disorders Center, all located in Reno. “Several years ago, I was caring for a 28-year-old man named Glen who had developed a viral encephalomyelitis and was in a coma for a week and a half. He was maintained on a ventilator, and I thought he wouldn’t make it. One magical day, he opened his eyes, but he was unable to communicate aside from moving his eyes, blinking and crying. He and I developed a system of communication in which he blinked once for ‘yes’ and twice for ‘no,’ which inspired me to create a blink detector. I bought an infra-red emitter and matching detector at RadioShack and put together an electronic breadboard with the help of a friend. The system we devised contained a buzzer and an LED light, and when aimed at my eyes, I was able to create buzzing sounds and fl ashing lights through the system that represented the sounds of Morse code when I blinked. That device was the beginning of the Eye-Com Biosensor — Eye-Com 1.”
Dr. Torch founded Eye-Com Corporation in 1998, and the Eye-Com Biosensor is now in its ninth level of design , with each version seeking to solve problems created by its predecessors. With Eye-Com 3, Dr. Torch discovered that the blinks picked up by Eye-Com 2 could be transmitted as square waves to an electroencephalography machine. The use of a radio frequency transmitter attached to Eye-Com 4 allowed the wearer to transmit blink signals wirelessly through walls and doors to a remote site. Eye-Com 5 measured not only the frequency of blinks, but their duration, as well as the velocity of the eyelid’s up and down movement.
Eye-Com 6 took things a step further with its ability to measure the size of the pupil and its rate of constriction and dilation. The device also had the potential to find the center point of
the pupil and track it as it moved through all points of gaze. Dr. Torch demonstrated that the device could detect drowsiness and signs of inattention in children with attention defi cit disorder (ADD). Dr. Torch received several grants over the past decade the Centers for Disease Control and Prevention, the U.S. Army and the U.S. Departments of Transportation and Defense.
ApplicationsThe military has found several applications for Eye-Com 6,
including monitoring the eyes of helicopter pilots for fatigue, detect-ing signs of sleepiness induced by hypoxia in pilots fl ying at high altitudes and detecting signs of underwater fatigue, hypoxia and nitrogen narcosis when placed in the SCUBA masks of Navy SEALs.
A U.S. Department of Transportation (USDOT) study also dem-onstrated Eye-Com 6’s ability to monitor drivers of mass transport for signs of drowsiness using oculometrics. Most importantly, Eye-Com 6 was able to measure PERCLOS — the percentage of time one’s eyes are open or closed over a period of time — a new oculometric defi ned by the USDOT as the best biophysiological measure of drowsiness.
Eye-Com 7, the latest version of the technology, can be used not only for communicating with other people, but for controlling the cursor on a computer screen via eye-tracking algorithms. The device can even make a wheelchair travel where the wearer looks. Other current or potential applications for Eye-Com 7 identifi ed by Dr. Torch include:
+ tool for studying patients with epilepsy assistive communicator and controller tool for handicapped individuals
+ identifying ocular manifestations of ADD in children
+ identifying signs of post-traumatic stress disorder and traumatic brain injury
+ identifying the effects of medications, alcohol and illicit drugs
+ iris and security identifi cation
+ lie detector tool in forensic psychology
+ hands-free operation of medical, surgical and industrial tools
PIONEERING FIGURE
William Torch, M.D., M.S., founder and Chairman of Eye-Com Corporation, Inc. and Medical Director of the Neurodevelopmental and Neurodiagnostic Center and Washoe Sleep Disorder Center, all located in Reno, NV, is a pediatric and adult neurologist and child psychiatrist by training. The native New Yorker developed his love for those disciplines after reading books by Freud and other authors of psychoanalytical books as a teenager. He received his master’s and medical degrees from the University of Rochester School of Medicine in Rochester, NY, pediatrics and child psychiatry at Massachusetts General Hospital in Boston, MA, and in child and adult neurology, as well as pediatrics at the Albert Einstein College of Medicine of Yeshiva University, Bronx, NY.
After completing a fellowship in pediatric neurology in Vancouver, British Columbia, Dr. Torch became the fi rst pediatric neurologist in Nevada when he accepted a position at the University of Nevada School of Medicine in Reno in 1979. He opened the Neurodevelopmental and Neurodiagnostic Center after spend-ing fi ve years at the university and later developed the Washoe Sleep Disorder Center. Today, both practices serve pediatric and adult patients.
THE FUTURE OF MEDICINE IN THE NEW DECADE WILL BELONG TO THE MEN AND WOMEN WHO DRIVE TECHNOLOGY FORWARD THROUGH BIG IDEAS, METICULOUS RESEARCH AND TRIAL AND ERROR.
“As someone trying to understand the mechanisms of the mind-brain relationship, Eye-Com has helped connect the original passions I had as a youngster,” Dr. Torch says. “The most important thing to me is being able to improve the quality of life of my patients. Glen is still alive, and though he is triplegic, he now has full ability to communicate. He still ponders the meaning of his illness and wonders why he should be so affl icted. When I recently reminded him that he was the person who helped generate my thoughts about Eye-Com, he responded that those words and the thought behind those sentiments gave meaning to his life.”
For further information about the Eye-Com, please visit www.eyecomworld.com. !
FutureON THEEyes
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

1 8 | Twin Cities MD NEWS ! APRIL 2010 TWINCITIES.MDNEWS.COM
your employees and how they view the practice is to ask. Conduct individualized interviews with staff members to gain insight and find ways you can improve the environment and increase their desire to stay with your practice. Explain that this is not an internal review of their performance as employees, but a review of the practice to make sure you are meeting their needs. This will take time, but it can be time well spent.
they’re not the only things that keep your staff from seeking another job. Work environment and verbal communication from you, the physician, goes a long way.
Here are some ways to help keep your staff happy and productive:
+ Speak to your employees. Physicians should address individual sta f f members by name when they see them. Instituting nametags can be beneficial to make this a reality. Be sure to make an effort to interact with your front office staff — even if it’s just a quick, “Hi, everyone.”
+ Know more than their names. Try to get to know your staff on a personal level. Circulating an office newsletter, whether it’s once a week or once a month, or having a bulletin board with fun staff information in the break room can help. Post and celebrate staff birthdays, anniversaries of employment and other exciting personal news, such as new babies or engagements, through these simple medias.
+ Implement and endorse open communication. Allowing your employees to speak their minds or contribute ideas is key to employee retention. Promote providing feedback — good or bad — with a suggestion box, and encourage staff to alert you if they have a problem. If an issue arises in your practice, let your staff know promptly.
Employees need to be acknowledged for a job well done, recognized for achievements and given the opportunity to perform new tasks or have more responsibility. Showing your employees that you care about their well-being and consider them valuable assets to your practice can promote staff satisfaction and retention. !
Continued from Page 14
+++++++++++++++++++++++++++++++ ++++ +++++++++++++++++++++++++++++++++
PRACTICE MANAGEMENT "
It’s More Than MoneyThough decent wages and benefits
are important elements of employment,
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

Twin Cities MD NEWS ! APRIL 2010 | 1 9""TWINCITIES.MDNEWS.COM
THE STRENGTH TO HEAL
©2007. Paid for by the United States Army. All rights reserved.
Learn the latest treatments and play an important role in the care of Soldiers andtheir Families. As a physician on the U.S. Army Reserve Health Care Team, you’llcontinue to practice in your community and serve when needed. You’ll work withthe most advanced technology and distinguish yourself while working withdedicated professionals. You’ll make a difference.
To learn more about the U.S. Army Reserve Health Care Team, call 866-660-3948or visit healthcare.goarmy.com/ .i761
and stand by those whostand up for me. REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
2 0 | Twin Cities MD NEWS ! APRIL 2010 TWINCITIES.MDNEWS.COM
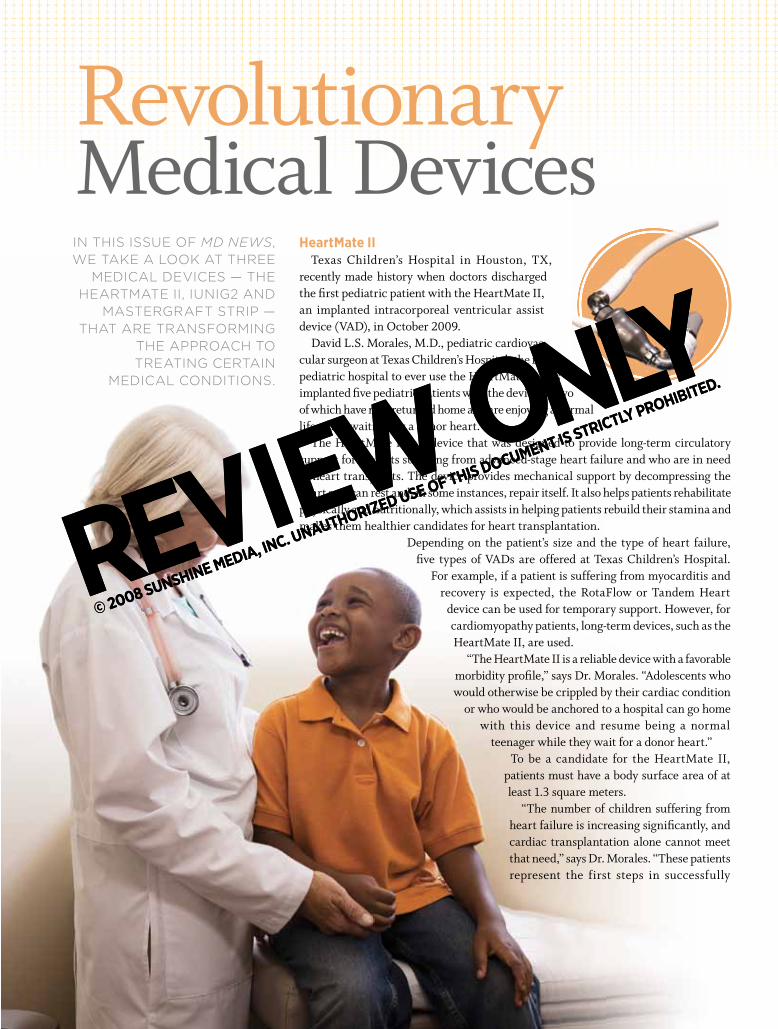
HeartMate IITexas Children’s Hospital in Houston, TX,
recently made history when doctors discharged the fi rst pediatric patient with the HeartMate II, an implanted intracorporeal ventricular assist device (VAD), in October 2009.
David L.S. Morales, M.D., pediatric cardiovas-cular surgeon at Texas Children’s Hospital, the fi rst pediatric hospital to ever use the HeartMate II, has implanted fi ve pediatric patients with the device — two of which have now returned home and are enjoying a normal life while waiting for a donor heart.
The HeartMate II is a device that was designed to provide long-term circulatory support for patients suffering from advanced-stage heart failure and who are in need of heart transplants. The device provides mechanical support by decompressing the heart so it can rest and, in some instances, repair itself. It also helps patients rehabilitate physically and nutritionally, which assists in helping patients rebuild their stamina and makes them healthier candidates for heart transplantation.
Depending on the patient’s size and the type of heart failure, fi ve types of VADs are offered at Texas Children’s Hospital.
For example, if a patient is suffering from myocarditis and recovery is expected, the RotaFlow or Tandem Heart
device can be used for temporary support. However, for cardiomyopathy patients, long-term devices, such as the HeartMate II, are used.
“The HeartMate II is a reliable device with a favorable morbidity profi le,” says Dr. Morales. “Adolescents who would otherwise be crippled by their cardiac condition
or who would be anchored to a hospital can go home with this device and resume being a normal
teenager while they wait for a donor heart.”To be a candidate for the HeartMate II,
patients must have a body surface area of at least 1.3 square meters.
“The number of children suffering from heart failure is increasing signifi cantly, and cardiac transplantation alone cannot meet that need,” says Dr. Morales. “These patients represent the first steps in successfully
IN THIS ISSUE OF MD NEWS, WE TAKE A LOOK AT THREE
MEDICAL DEVICES — THE HEARTMATE II, IUNIG2 AND
MASTERGRAFT STRIP — THAT ARE TRANSFORMING
THE APPROACH TO TREATING CERTAIN
MEDICAL CONDITIONS.
addressing the growing wave of children with heart failure in a fashion that improves their quality of life without chaining them to a hospital.”
iUniG2The iUniG2, manufactured by
ConforMIS, Inc., is a second-generation unicompartmental knee resurfacing device.
After considering surgeon feedback regarding the original iUni, ConforMIS has made several important changes to the product that will provide benefi ts for both surgeons and patients.
The iUniG2 features a patient-specific femoral component that improves the implant’s wear optimization. Using a patient’s CT scan, a coronal curve is created for the patient’s femur. The coronal curve is then matched to a contour poly (the insert for the metal plate), which also has a curve created specifi cally for the patient. This allows the two pieces to fi t together in a way that reduces the amount of contact stress on the implant when being used. Also, the interference fi t for the contour poly is tight, minimizing micromotion.
“Traditional implants only come in fi ve or six standard sizes and, considering how diverse our population is, it is not always easy to fi nd an implant that works for every patient,” says Jong Lee, Senior Vice President of Business Strategy at ConforMIS. “Now, patients are able to fi nd an implant that is personalized specifi cally for them, which is really changing the way people view orthopedic surgery.”
The iUniG2 also provides for a simpler surgical technique. Because the implant’s iJig pieces are designed specifi cally for each patient, surgeons are no longer required to cut through bone. This reduces the risk of blood clot formation after surgery. The iJig pieces are also disposable, preventing the hospital from having to sanitize and store the instruments.
Finally, ConforMIS is introducing something new with the iUniG2 — iView. iView is a sheet of images of the patient’s anatomy that is provided to the surgeon prior to surgery. These images show surgeons where osteocytes are located, where cuts should be made and what the implant should look like after it has been placed, allowing for easier planning prior to surgery.
MASTERGRAFT StripThe MASTERGRAFT Strip, produced by Medtronic,
Inc., is a new product that was given full market release in the United States in November 2009.
The MASTERGRAFT Strip is a highly fl exible ceramic scaffold that can be used in conjunction with a patient’s bone to fuse multiple levels of the posterolateral spine. The product features a geometric design that maximizes contact with the bone’s surface area and allows for continuous bone growth over gaps.
In clinical trials, the MASTERGRAFT Strip was used for a variety of bone grafting procedures with excellent intraoperative performance. Surgeons who evaluated the MASTERGRAFT Strip through the clinical trials were impressed with its ease of handling. The MASTERGRAFT Strip offers continuous latticework for longer grafting procedures, which are used when the spine has become unstable or has lost its natural shape. Surgeons were also impressed with the length of the MASTERGRAFT Strip because it eliminates the need for surgeons to use multiple units of synthetic product to complete the graft. !
implanted fi ve pediatric patients with the device — two
Revolutionary Medical Devices
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

Twin Cities MD NEWS ! APRIL 2010 | 2 1""TWINCITIES.MDNEWS.COM
HeartMate IITexas Children’s Hospital in Houston, TX,
recently made history when doctors discharged the fi rst pediatric patient with the HeartMate II, an implanted intracorporeal ventricular assist device (VAD), in October 2009.
David L.S. Morales, M.D., pediatric cardiovas-cular surgeon at Texas Children’s Hospital, the fi rst pediatric hospital to ever use the HeartMate II, has implanted fi ve pediatric patients with the device — two of which have now returned home and are enjoying a normal life while waiting for a donor heart.
The HeartMate II is a device that was designed to provide long-term circulatory support for patients suffering from advanced-stage heart failure and who are in need of heart transplants. The device provides mechanical support by decompressing the heart so it can rest and, in some instances, repair itself. It also helps patients rehabilitate physically and nutritionally, which assists in helping patients rebuild their stamina and makes them healthier candidates for heart transplantation.
Depending on the patient’s size and the type of heart failure, fi ve types of VADs are offered at Texas Children’s Hospital.
For example, if a patient is suffering from myocarditis and recovery is expected, the RotaFlow or Tandem Heart
device can be used for temporary support. However, for cardiomyopathy patients, long-term devices, such as the HeartMate II, are used.
“The HeartMate II is a reliable device with a favorable morbidity profi le,” says Dr. Morales. “Adolescents who would otherwise be crippled by their cardiac condition
or who would be anchored to a hospital can go home with this device and resume being a normal
teenager while they wait for a donor heart.”To be a candidate for the HeartMate II,
patients must have a body surface area of at least 1.3 square meters.
“The number of children suffering from heart failure is increasing signifi cantly, and cardiac transplantation alone cannot meet that need,” says Dr. Morales. “These patients represent the first steps in successfully
IN THIS ISSUE OF MD NEWS, WE TAKE A LOOK AT THREE
MEDICAL DEVICES — THE HEARTMATE II, IUNIG2 AND
MASTERGRAFT STRIP — THAT ARE TRANSFORMING
THE APPROACH TO TREATING CERTAIN
MEDICAL CONDITIONS.
addressing the growing wave of children with heart failure in a fashion that improves their quality of life without chaining them to a hospital.”
iUniG2The iUniG2, manufactured by
ConforMIS, Inc., is a second-generation unicompartmental knee resurfacing device.
After considering surgeon feedback regarding the original iUni, ConforMIS has made several important changes to the product that will provide benefi ts for both surgeons and patients.
The iUniG2 features a patient-specific femoral component that improves the implant’s wear optimization. Using a patient’s CT scan, a coronal curve is created for the patient’s femur. The coronal curve is then matched to a contour poly (the insert for the metal plate), which also has a curve created specifi cally for the patient. This allows the two pieces to fi t together in a way that reduces the amount of contact stress on the implant when being used. Also, the interference fi t for the contour poly is tight, minimizing micromotion.
“Traditional implants only come in fi ve or six standard sizes and, considering how diverse our population is, it is not always easy to fi nd an implant that works for every patient,” says Jong Lee, Senior Vice President of Business Strategy at ConforMIS. “Now, patients are able to fi nd an implant that is personalized specifi cally for them, which is really changing the way people view orthopedic surgery.”
The iUniG2 also provides for a simpler surgical technique. Because the implant’s iJig pieces are designed specifi cally for each patient, surgeons are no longer required to cut through bone. This reduces the risk of blood clot formation after surgery. The iJig pieces are also disposable, preventing the hospital from having to sanitize and store the instruments.
Finally, ConforMIS is introducing something new with the iUniG2 — iView. iView is a sheet of images of the patient’s anatomy that is provided to the surgeon prior to surgery. These images show surgeons where osteocytes are located, where cuts should be made and what the implant should look like after it has been placed, allowing for easier planning prior to surgery.
MASTERGRAFT StripThe MASTERGRAFT Strip, produced by Medtronic,
Inc., is a new product that was given full market release in the United States in November 2009.
The MASTERGRAFT Strip is a highly fl exible ceramic scaffold that can be used in conjunction with a patient’s bone to fuse multiple levels of the posterolateral spine. The product features a geometric design that maximizes contact with the bone’s surface area and allows for continuous bone growth over gaps.
In clinical trials, the MASTERGRAFT Strip was used for a variety of bone grafting procedures with excellent intraoperative performance. Surgeons who evaluated the MASTERGRAFT Strip through the clinical trials were impressed with its ease of handling. The MASTERGRAFT Strip offers continuous latticework for longer grafting procedures, which are used when the spine has become unstable or has lost its natural shape. Surgeons were also impressed with the length of the MASTERGRAFT Strip because it eliminates the need for surgeons to use multiple units of synthetic product to complete the graft. !
implanted fi ve pediatric patients with the device — two
Revolutionary Medical Devices
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

2 2 | Twin Cities MD NEWS ! APRIL 2010 TWINCITIES.MDNEWS.COM
Dangers of Media Overload
T HE AMOUNT OF time American children and teens spend watching television, playing video games or surfing the
Internet has increased dramatically during the past five years. In fact, a new survey finds that children spend almost
eight hours a day or 56 hours a week, consuming some type of media — more time than adults generally devote to a full-time job.
A report by the Program for the Study of Media Health at the Kaiser Family Foundation suggests the significant rise
in child media consumption is due in large part to the availability of mobile devices such as cell phones and iPods with Internet capabilities. In fact, in 2004, 39% of children had cell phones compared to 66% today. Social network-ing sites are also thought to play a role in
++++++++++++++++++++++++ ++++ ++++++++++++++++++++++++++
CURRENT TOPICS "
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

Twin Cities MD NEWS ! APRIL 2010 | 2 3""TWINCITIES.MDNEWS.COM
rampant media consumption, as these sites can be accessed in various ways, such as via a cell phone or computer.
What the Study FoundThe Kaiser Family Foundation survey
found that with the exception of going to a movie theater or reading, all forms of media usage have seen an increase in the last five years. Listening to music has increased by 47 minutes daily; watching television has gone up by 38 minutes; computer time has increased 27 minutes’ and time spent playing video games has gone up by 24 minutes a day. Total, the survey found that children spend about four and a half hours in front of the television, two and a half hours listening to music, an hour and a half on the computer and about an hour and a quarter playing video games.
The study also found: + Almost 50% of children and teens use media while doing homework.
+ Boys spend more time than girls play-ing video games, computer games or visiting video sites like YouTube.
+ Fewer children read magazines and newspapers, as this type of media can now be found online.
+ Girls spend more time visiting social networking sites, listening to music and reading than boys.
+ Media use increases dramatically beginning at age 11.
+ Teens spend about an hour and a half of their time texting every day.
Implications of a Media- Savvy Society
Though the effects of media consump-tion in children have been studied for quite some time, as children begin to spend more and more of their time with various forms of media the health effects must be investigated further.
Media consumption is thought to affect children in a variety of ways and can even manifest itself in the physical sense, as
inactivity due to media consumption can promote obesity. It may also have an impact on sleeping habits, attention and school performance. In addition, there are growing concerns that overindulgent media usage may also lead to:
+ Anxiety. Violent video games and scary television shows may lead chil-dren to become frightened that they will become a victim of violence or natural disaster.
+ Poor self esteem. Children may buy
into stereotypes seen on television and begin to doubt their self worth.
+ Unhealthy lifestyle choices. Children who obtain a lot of information from ads seen on television often make choices based on those ads. This can lead to poor food choices and risky behavior. !
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

2 4 | Twin Cities MD NEWS ! APRIL 2010 TWINCITIES.MDNEWS.COM
An Ethical Guide for Patient-Physician-Caregiver Relationships
I N JANUARY 2010, the American College of Physicians (ACP) pub-lished a new position paper on guidelines for ensuring good rela-
tions between physicians and their patients and caregivers.
The Journal of General Internal Medicine has published “Family Caregivers, Patients and Physicians: Ethical Guidance to Optimize Relationships.”
According to Joseph Stubbs, M.D., FACP, President of the ACP, the ethi-cal guidance outlined in the paper is intended to heighten physician awareness of the importance and complexity of the patient-physician-caregiver relationship. He states that it is essential for physicians to consider quality of life for both patients and caregivers.
A Vital RoleFamily caregivers play a crucial role
in optimizing the health and quality of life for the more than 30 million patients with acute or chronic illness. Routine functions provided by family caregivers may include assistance with daily activities, management of complex care regimens, health care system naviga-tion and communication with health care professionals.
Caregivers are more prone to injury and disease when they experience height-ened stress, whether physical, emotional and/or financial. Additional burdens may result when there is a geographical distance between the caregiver and patient, causing health care professionals to find themselves assuming the role of family caregiver.
Physicians must recognize the impor-tance of the caregiver role in facilitating a positive caregiving experience. Ethical cha l lenges a r ise when tr y ing to balance the primacy of the patient-phy-
sician relationship and the physician’s role in partnering with patients and family caregivers.
Ethical StandardsThe paper, which was endorsed by
10 other professional medical societies in addition to the ACP, defines caregiv-ers as relatives, partners, friends and neighbors of patients who assist with activities of daily living and complex health care needs.
T he col la b orat ive pap er pro -vides ethical recommendations for physicians, including:
+ Respect for a patient’s dignity, rights and values should guide all patient-physician-caregiver interactions.
+ To optimize appropriate patient autonomy and participation in decision-making, clinical encounters should be patient-centered.
+ To provide the patient’s desired level of privacy, the physician should routinely evaluate the patient’s preferences concerning the nature and degree of caregiver participation in the clinical visit.
+ Physician accessibility and effec-tive communication are essential for supporting the patient and family caregiver.
+ The physician should educate the patient, family caregiver and other family members, so they share an accurate understanding of the patient’s condition and prognosis.
+ To provide both the family caregiver and physician with a clear under-standing of the patient’s wishes, the
physician should facilitate discussion of the patient’s health care values and advance-care planning.
+ The physician should acknowledge the value of family caregivers as a source of continuity regarding the patient’s medical and psychological history and facilitate the emotional and intellectual transition to the end stage of serious chronic disease.
+ The physician should be watchful to detect distress in the family caregiver and provide appropriate referrals.
+ The palliative care plan should opti-mize quality of life for the caregiver as well as the patient.
+ When the caregiver is a health care professional, the physician should set appropriate boundaries, so the caregiver is not required to take a professional role in caring for the patient and the caregiver receives the appropriate support, referrals and services. !
ETHICS "+++++++++++++++ ++++ +++++++++++++++++
CityWest Prosthodontics, P.A. .............. 11Crutchfield Dermatology ........... Inside Front CoverHealthEast Care System ...........................9Hennepin County Medical Center ....................Inside Back Midwest Spine Institute .......................... 10National Dizzy & Balance Center ......... 14Neurosurgical Associates, Ltd ............. 22Physicians’ Diagnostics & Rehabilitation ................................... 23The Davis Group ..........................................3Twin Cities Spine Center ......................... 18U.S. Army ..................................................... 19
ADVERTISERS’ INDEX
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

Twin Cities MD NEWS ! APRIL 2010 | 2 5""TWINCITIES.MDNEWS.COM
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.
REVIEW ONLY
© 2008 SUNSHINE MEDIA, INC. UNAUTHORIZED USE OF THIS DOCUMENT IS STRICTLY PROHIBITED.

And I got there with Bethesda Hospital, member of HealthEast® Care System.When a 1,700-pound tree crushed Don Obernolte, he thought everything was over. But with the help of Bethesda, he’s reinvented his life. As one of the first and largest long-term acute care hospitals in the nation, Bethesda cares for chronically ill patients or victims of catastrophic accidents, with higher-than-national-average vent wean rates. So patients can recover, relearn and restart, creating a new normal for their lives.
For more information about Bethesda Hospital in St. Paul, Minnesota, visit bethesdahospital.org or call 651-232-2000.
!"#$"!%%&'()&*+&(,&-./0&12345677&&&" "89889!#&&&":"!:;;&<(







![MD Research News - mdfoundation.com.au 347 MD... · MD Research News Issue 347 Thursday 5 October, 2017 Drug treatment Asia Pac J Ophthalmol (Phila). 2017 Oct 3. [Epub ahead of print]](https://static.fdocuments.net/doc/165x107/5b75cadd7f8b9ade498dc84b/md-research-news-347-md-md-research-news-issue-347-thursday-5-october.jpg)










