
2 VISION Conquer the Complexrobseide.com/images/previews/Alpine.pdfStroke / cerebrovascular accident...
2
Abbott Vascular 3200 Lakeside Dr., Santa Clara, CA 95054 USA, Tel: 1.800.227.9902 Caution: This product is intended for use by or under the direction of a physician. Prior to use, reference the Instructions for Use at www.abbottvascular.com/ifu for more detailed information on Indications, Contraindications, Warnings, Precautions and Adverse Events. Tests performed by and data on file at Abbott Vascular. Illustrations are artist’s representations only and should not be considered as engineering drawings or photographs and are not drawn to scale. Photos taken by and on file at Abbott Vascular. XIENCE V, XIENCE nano, XIENCE PRIME, XIENCE Xpedition, XIENCE Alpine, MULTI-LINK VISION, and MULTI-LINK MINI VISION are trademarks of the Abbott Group of Companies. Endeavor and Endeavor Resolute are trademarks of Medtronic. Taxus is a trademark of Boston Scientific Corporation or its affiliates. Cypher is a trademark of Cordis, a Johnson & Johnson Company. www.AbbottVascular.com ©2014 Abbott. All rights reserved. LT2940503 Rev. A 10/14 Conquer the Complex INDICATIONS The XIENCE Family of Everolimus Eluting Coronary Stent Systems are indicated for improving coronary luminal diameter in patients with symptomatic heart disease due to de novo native coronary artery lesions for XIENCE V (length ≤ 28 mm), XIENCE PRIME, XIENCE Xpedition and XIENCE Alpine (lengths ≤ 32 mm) with reference vessel diameters of ≥2.25 mm to ≤ 4.25 mm. Additionally, the entire XIENCE Family is indicated for treating de novo chronic total coronary occlusions. The only CTO Indicated stent RX Ordering Information mm 8 12 15 18 23 28 33 38 2.25 1125225-08 1125225-12 1125225-15 1125225-18 1125225-23 1125225-28 2.5 1125250-08 1125250-12 1125250-15 1125250-18 1125250-23 1125250-28 1125250-33 1125250-38 2.75 1125275-08 1125275-12 1125275-15 1125275-18 1125275-23 1125275-28 1125275-33 1125275-38 3.0 1125300-08 1125300-12 1125300-15 1125300-18 1125300-23 1125300-28 1125300-33 1125300-38 3.25 1125325-08 1125325-12 1125325-15 1125325-18 1125325-23 1125325-28 1125325-33 1125325-38 3.5 1125350-08 1125350-12 1125350-15 1125350-18 1125350-23 1125350-28 1125350-33 1125350-38 4 1125400-08 1125400-12 1125400-15 1125400-18 1125400-23 1125400-28 1125400-33 1125400-38 The XIENCE V ® , XIENCE nano ® , XIENCE PRIME ® , XIENCE PRIME ® LL, XIENCE Xpedition ® , XIENCE Xpedition ® SV and XIENCE Xpedition ® LL , XIENCE Alpine TM (XIENCE Family) of Everolimus Eluting Coronary Stents on the MULTI-LINK VISION ® or MULTI-LINK MINI VISION ® Delivery Systems INDICATIONS The XIENCE Family of Everolimus Eluting Coronary Stent Systems are indicated for improving coronary luminal diameter in patients with symptomatic heart disease due to de novo native coronary artery lesions for XIENCE V (length ≤ 28 mm), XIENCE PRIME, XIENCE Xpedition and XIENCE Alpine (lengths ≤ 32 mm) with reference vessel diameters of ≥2.25 mm to ≤ 4.25 mm. Additionally, the entire XIENCE Family is indicated for treating de novo chronic total coronary occlusions. CONTRAINDICATIONS The XIENCE Family of stents is contraindicated for use in patients: • Who cannot receive antiplatelet and/or anti-coagulant therapy • With lesions that prevent complete angioplasty balloon inflation or proper placement of the stent or stent delivery system • With hypersensitivity or contraindication to everolimus or structurally-related compounds, cobalt, chromium, nickel, tungsten, acrylic, and/or fluoropolymers. WARNINGS • Ensure that the inner package sterile barrier has not been opened or damaged prior to use. • Judicious patient selection is necessary because the use of this device carries the associated risk of stent thrombosis, vascular complications, and/or bleeding events. • This product should not be used in patients who are not likely to comply with the recommended antiplatelet therapy. PRECAUTIONS • Stent implantation should only be performed by physicians who have received appropriate training. • Stent placement should be performed at hospitals where emergency coronary artery bypass graft surgery is accessible. • Subsequent restenosis may require repeat dilatation of the arterial segment containing the stent. Long-term outcomes following repeat dilatation of the stent are presently unknown. • Risks and benefits should be considered in patients with severe contrast agent allergies. • Care should be taken to control the guiding catheter tip during stent delivery, deployment and balloon withdrawal. Before withdrawing the stent delivery system, visually confirm complete balloon deflation by fluoroscopy to avoid guiding catheter movement into the vessel and subsequent arterial damage. • Stent thrombosis is a low-frequency event that is frequently associated with myocardial infarction (MI) or death. • When DES are used outside the specified Indications for Use, patient outcomes may differ from the results observed in the SPIRIT family of trials. • Compared to use within the specified Indications for Use, the use of DES in patients and lesions outside of the labeled indications may have an increased risk of adverse events, including stent thrombosis, stent embolization, MI, or death. • Orally administered everolimus combined with cyclosporine is associated with increased serum cholesterol and triglycerides levels. • A patient’s exposure to drug and polymer is proportional to the number and total length of implanted stents. See Instructions for Use for current data on multiple stent implantation. • Safety and effectiveness of the XIENCE Family of stents have not been established for subject populations with the following clinical settings: • Patients with prior target lesion or in-stent restenosis related brachytherapy, patients in whom mechanical atherectomy devices or laser angioplasty catheters are used in conjunction with XIENCE Family stents, women who are pregnant or lactating, men intending to father children, pediatric patients, unresolved vessel thrombus at the lesion site, coronary artery reference vessel diameters < 2.25 mm or > 4.25 mm or lesion length > 32 mm, lesions located in saphenous vein grafts, unprotected left main coronary artery, ostial lesions, lesions located at a bifurcation or previously stented lesions, diffuse disease or poor flow (TIMI < 1) distal to the identified lesions, excessive tortuosity proximal to or within the lesion, recent acute myocardial infarction (AMI) or evidence of thrombus in target vessel multivessel disease, and in-stent restenosis • Everolimus has been shown to reduce the clearance of some prescription medications when administered orally along with cyclosporine (CsA). Formal drug interaction studies have not been performed with the XIENCE Family of stents because of limited systemic exposure to everolimus eluted from the stent. • Everolimus is an immunosuppressive agent. Consideration should be given to patients taking other immunosuppressive agents or who are at risk for immune suppression. • Oral everolimus use in renal transplant patients and advanced renal cell carcinoma patients was associated with increased serum cholesterol and triglycerides, which in some cases required treatment. • Nonclinical testing has demonstrated that the XIENCE Family of stents, in single and in overlapped configurations are MR conditional up to 68 mm in length for XIENCE V and XIENCE nano only and up to 71 mm in length for all other XIENCE Family stents. It can be scanned safely under the conditions in the Instructions for Use. • The XIENCE Family of stents should be handled, placed, implanted, and removed according to the Instructions for Use. POTENTIAL ADVERSE EVENTS Adverse events (in alphabetical order) which may be associated with percutaneous coronary and treatment procedure including coronary stent use in native coronary arteries include, but are not limited to: • Abrupt closure, Access site pain, hematoma, or hemorrhage, Acute myocardial infarction, Allergic reaction or hypersensitivity to contrast agent or cobalt, chromium, nickel, tungsten, acrylic and fluoropolymers; and drug reactions to antiplatelet drugs or contrast agent, Aneurysm, Arterial perforation and injury to the coronary artery, Arterial rupture, Arteriovenous fistula, Arrhythmias, atrial and ventricular, Bleeding complications, which may require transfusion, Cardiac tamponade, Coronary artery spasm, Coronary or stent embolism, Coronary or stent thrombosis, Death, Dissection of the coronary artery, Distal emboli (air, tissue or thrombotic), Emergent or non-emergent coronary surgery, Fever, Hypotension and / or hypertension, Infection and pain at insertion site, Injury to the coronary artery, Ischemia (myocardial), Myocardial infarction (MI), Nausea and vomiting, Palpitations, Peripheral ischemia (due to vascular injury), Pseudoaneurysm, Renal Failure, Restenosis of the stented segment of the artery, Shock/pulmonary edema, Stroke / cerebrovascular accident (CVA), Total occlusion of coronary artery, Unstable or stable angina pectoris, Vascular complications including at the entry site which may require vessel repair, Vessel dissection Adverse events associated with daily oral administration of everolimus to organ transplant patients include but are not limited to: • Abdominal pain (including upper abdominal pain); Anemia; Angioedema; Anorexia; Asthenia; Constipation; Cough; Delayed wound healing/fluid accumulation; Diarrhea; Dyslipidemia (including hyperlipidemia and hypercholesterolemia); Dyspnea; Dysgeusia; Dyspepsia; Dysuria; Dry skin; Edema (peripheral); Epistaxis; Fatigue; Headache; Hematuria; Hyperglycemia (may include new onset of diabetes); Hyperlipidemia; Hyperkalemia; Hypertension; Hypokalemia; Hypomagnesemia; Hypophosphatemia; Increased serum creatinine; Infections and serious infections: bacterial, viral, fungal, and protozoal infections (may include herpes virus infection, polyoma virus infection which may be associated with BK virus associated nephropathy, and/or other opportunistic infections); Insomnia; Interaction with strong inhibitors and inducers of CY3PA4 or PgP; Leukopenia; Lymphoma and other malignancies (including skin cancer); Male infertility (azospermia and/or oligospermia); Mucosal inflammation (including oral ulceration and oral mucositis); Nausea; Neutropenia; Non-infectious pneumonitis; Pain: extremity, incision site and procedural, back, chest, and musculoskeletal; Proteinuria; Pruritus; Pyrexia; Rash; Stomatitis; Thrombocytopenia; Thrombotic microangiopathy (TMA)/Thrombotic thrombocytopenic purpura (TTP)/ Hemolytic uremic syndrome (HUS); Tremor; Urinary tract infection; Upper respiratory tract infection; Vomiting • Live vaccines should be avoided and close contact with those that have had live vaccines should be avoided. Fetal harm can occur when administered to a pregnant woman. There may be other potential adverse events that are unforeseen at this time. XIENCE Safety Results from the Unique Design of the Proven MULTI-LINK Implant 11 The BMS comparator is a composite of several bare metal stents as a representation of the BMS category. 12 Source: Palmerini, et al. The Lancet. 379:9824, 14-20 April 2012, pp. 1393-1402. 13 “Meta-analyses should be regarded as hypothesis-generating and the findings of Palmerini and colleagues suggest that a randomized trial of CoCr EES and BMS is desirable.” Ormiston, The Lancet, April 2012. The XIENCE system’s clinical outcomes result from its components, including: a thin-strut, flexible ring and link design, with favorable strut apposition, no metal-to-metal touch points, and low strain upon expansion; the novel Everolimus compound; and the multi-layer coating and primer technologies, using a fluorinated polymer class known for cardiovascular implants, and known for having excellent mechanical properties. 14 An odds ratio is a method of comparing the odds of an event between two groups. 15 Source: Dr. Valgimigli, Effects of Cobalt-chromium everolimus eluting or bare metal stent on fatal and non-fatal cardiovascular events. A patient-level meta analysis. EuroPCR 2014. 16 44% STEMI, 19% diabetes, mean age of 67. The XIENCE system’s clinical outcomes result from its components, including: a thin-strut, flexible ring and link design, with favorable strut apposition, no metal-to-metal touch points, and low strain upon expansion; the novel Everolimus compound; and the multi-layer coating and primer technologies, using a fluorinated polymer class known for cardiovascular implants, and known for having excellent mechanical properties. P=0.013 Cumulative Hazard 0.00 0.02 0.04 0 200 400 600 800 Days BMS 11 XIENCE 4.0% 2.7% Cumulative Hazard P=0.003 0.00 0.01 0.02 0.03 0 200 400 600 800 Days BMS 11 XIENCE 0.8% 0.08% XIENCE results in 33% risk reduction XIENCE results in 89% risk reduction Primary Endpoint: Cardiac Death at 2 Years Fatal Myocardial Infarction at 2 Years XIENCE Demonstrates Significant Reductions in Cardiac Death and Fatal MI in Meta-Analysis 15 98% All-Comer or Complex Patients - Independent patient-level meta- analysis comparing XIENCE vs. BMS 11 in a complex 16 patient population - N=4,896 patients, from 5 randomized clinical trials and follow-up through 2 years - Presented by Dr. Marco Valgimigli at EuroPCR 2014 Stent Design - Proven CoCr MULTI-LINK design - Flexible stent & delivery system for conformability, less injury 2 - Low metal to artery ratio reduces injury, inflammation 9 - Thin well-apposed struts for rapid re-endothelialization, healing, and reduced thrombogenicity 3,4 - Reliable coating integrity because of no touch points and low strain stent design Coating Technology - Fluorinated polymer 5,8 - Coating durability, flexibility and elasticity for stent use 7,8 - Known biocompatible for cardiovascular implants 5,6,7 - Attracts albumin to surface for thromboresistance 10 - Minimal inflammation 5 - Faster endothelialization 5 - Multi-layer application over a primer to minimize coating defects Drug - Everolimus - Patented for restenosis reduction - Elution rate matched to restenosis cascade by optimal coating thickness - Cytostatic - Low drug dose - Broad therapeutic range 2 Colombo et al.; J Amer Coll Cardiol 2002;40(6): 1021-1033. 3 Kolandaivelu et al.; Circulation 2011; 123; 1400-1409. 4 Kastrati et al.; Circulation 2001; 103; 2816-2821. 5 Paton et al.; U.S. Patent 5,356,668. 6 Lilenfeld et al.; U.S. Patent 4,564,013. 7 Tu et al.; U.S. Patent 4,816,339. 8 Lo et al.; U.S. Patent 3,178,399. 9 Data on file at Abbott Vascular. 10 Panchalingam V, et al. ASAIO J 1993;39:M305-M309. 69% All-Comer or Complex Patients Definite Stent Thrombosis Rate 49 RCTs, 50,344 Patients XIENCE Demonstrates Significantly Lower Stent Thrombosis Rates than BMS 11 and Other DES in Large-Scale Meta Analysis 12,13 30 Day 2 Year Odds Ratio 14 (95%) Cl XIENCE vs. BMS 11 XIENCE vs. Taxus ® XIENCE vs. Cypher ® XIENCE vs. Endeavor ® XIENCE vs. Endeavor ® Resolute TM 0.21 (0.11-0.42) 0.27 (0.14-0.51) 0.40 (0.21-0.79) 0.22 (0.09-0.54) 0.07 (0.00-0.46) 0.35 (0.17-0.69) 0.34 (0.19-0.62) XIENCE vs. BMS 11 XIENCE vs. Taxus ® 1 Year 0.23 (0.13-0.41) 0.28 (0.16-0.48) 0.41 (0.24-0.70) 0.21 (0.10-0.44) 0.14 (0.03-0.47) XIENCE vs. BMS 11 XIENCE vs. Taxus ® XIENCE vs. Cypher ® XIENCE vs. Endeavor ® XIENCE vs. Endeavor ® Resolute TM 0.01 0.1 1 10 Favors XIENCE Favors Other -Network meta-analysis comparing the safety and efficacy between DES and BMS 11 -Analyzed data across only RCTs -Note that as with any meta-analysis, the underlying studies may have differences in design, enrollment criteria and endpoints; and these results would share the same limitations as the original underlying studies.
Transcript of 2 VISION Conquer the Complexrobseide.com/images/previews/Alpine.pdfStroke / cerebrovascular accident...

Abbott Vascular3200 Lakeside Dr., Santa Clara, CA 95054 USA, Tel: 1.800.227.9902
Caution: This product is intended for use by or under the direction of a physician. Prior to use, reference the Instructions for Use at www.abbottvascular.com/ifu for more detailed information on Indications, Contraindications, Warnings, Precautions and Adverse Events.
Tests performed by and data on fi le at Abbott Vascular. Illustrations are artist’s representations only and should not be considered as engineering drawings or photographs and are not drawn to scale. Photos taken by and on fi le at Abbott Vascular.
XIENCE V, XIENCE nano, XIENCE PRIME, XIENCE Xpedition, XIENCE Alpine, MULTI-LINK VISION, and MULTI-LINK MINI VISION are trademarks of the Abbott Group of Companies. Endeavor and Endeavor Resolute are trademarks of Medtronic. Taxus is a trademark of Boston Scientifi c Corporation or its affi liates. Cypher is a trademark of Cordis, a Johnson & Johnson Company.
www.AbbottVascular.com ©2014 Abbott. All rights reserved. LT2940503 Rev. A 10/14
Conquer the Complex
INDICATIONS The XIENCE Family of Everolimus Eluting Coronary Stent Systems are indicated for improving coronary luminal diameter in patients with symptomatic heart disease due to de novo native coronary artery lesions for XIENCE V (length ≤ 28 mm), XIENCE PRIME, XIENCE Xpedition and XIENCE Alpine (lengths ≤ 32 mm) with reference vessel diameters of ≥2.25 mm to ≤ 4.25 mm. Additionally, the entire XIENCE Family is indicated for treating de novo chronic total coronary occlusions.
Conquer the Complex
The only
CTO Indicated
stent
RX Ordering Information mm 8 12 15 18 23 28 33 382.25 1125225-08 1125225-12 1125225-15 1125225-18 1125225-23 1125225-28
2.5 1125250-08 1125250-12 1125250-15 1125250-18 1125250-23 1125250-28 1125250-33 1125250-38
2.75 1125275-08 1125275-12 1125275-15 1125275-18 1125275-23 1125275-28 1125275-33 1125275-38
3.0 1125300-08 1125300-12 1125300-15 1125300-18 1125300-23 1125300-28 1125300-33 1125300-38
3.25 1125325-08 1125325-12 1125325-15 1125325-18 1125325-23 1125325-28 1125325-33 1125325-38
3.5 1125350-08 1125350-12 1125350-15 1125350-18 1125350-23 1125350-28 1125350-33 1125350-38
4 1125400-08 1125400-12 1125400-15 1125400-18 1125400-23 1125400-28 1125400-33 1125400-38
The XIENCE V®, XIENCE nano®, XIENCE PRIME®, XIENCE PRIME® LL, XIENCE Xpedition®, XIENCE Xpedition® SV and XIENCE Xpedition® LL , XIENCE AlpineTM (XIENCE Family) of Everolimus Eluting Coronary Stents on the MULTI-LINK VISION® or MULTI-LINK MINI VISION® Delivery Systems
INDICATIONSThe XIENCE Family of Everolimus Eluting Coronary Stent Systems are indicated for improving coronary luminal diameter in patients with symptomatic heart disease due to de novo native coronary artery lesions for XIENCE V (length ≤ 28 mm), XIENCE PRIME, XIENCE Xpedition and XIENCE Alpine (lengths ≤ 32 mm) with reference vessel diameters of ≥2.25 mm to ≤ 4.25 mm. Additionally, the entire XIENCE Family is indicated for treating de novo chronic total coronary occlusions.
CONTRAINDICATIONSThe XIENCE Family of stents is contraindicated for use in patients:• Who cannot receive antiplatelet and/or anti-coagulant therapy • With lesions that prevent complete angioplasty balloon infl ation
or proper placement of the stent or stent delivery system• With hypersensitivity or contraindication to everolimus or
structurally-related compounds, cobalt, chromium, nickel, tungsten, acrylic, and/or fl uoropolymers.
WARNINGS• Ensure that the inner package sterile barrier has not been
opened or damaged prior to use. • Judicious patient selection is necessary because the use of
this device carries the associated risk of stent thrombosis, vascular complications, and/or bleeding events.
• This product should not be used in patients who are not likely to comply with the recommended antiplatelet therapy.
PRECAUTIONS• Stent implantation should only be performed by physicians
who have received appropriate training.• Stent placement should be performed at hospitals where
emergency coronary artery bypass graft surgery is accessible.• Subsequent restenosis may require repeat dilatation of the
arterial segment containing the stent. Long-term outcomes following repeat dilatation of the stent are presently unknown.
• Risks and benefi ts should be considered in patients with severe contrast agent allergies.
• Care should be taken to control the guiding catheter tip during stent delivery, deployment and balloon withdrawal. Before withdrawing the stent delivery system, visually confi rm complete balloon defl ation by fl uoroscopy to avoid guiding catheter movement into the vessel and subsequent arterial damage.
• Stent thrombosis is a low-frequency event that is frequently associated with myocardial infarction (MI) or death.
• When DES are used outside the specifi ed Indications for Use, patient outcomes may differ from the results observed in the SPIRIT family of trials.
• Compared to use within the specifi ed Indications for Use, the use of DES in patients and lesions outside of the labeled indications may have an increased risk of adverse events, including stent thrombosis, stent embolization, MI, or death.
• Orally administered everolimus combined with cyclosporine is associated with increased serum cholesterol and triglycerides levels.
• A patient’s exposure to drug and polymer is proportional to the number and total length of implanted stents. See Instructions for Use for current data on multiple stent implantation.
• Safety and effectiveness of the XIENCE Family of stents have not been established for subject populations with the following clinical settings:• Patients with prior target lesion or in-stent restenosis
related brachytherapy, patients in whom mechanical atherectomy devices or laser angioplasty catheters are used in conjunction with XIENCE Family stents, women who are pregnant or lactating, men intending to father children, pediatric patients, unresolved vessel thrombus at the lesion site, coronary artery reference vessel diameters < 2.25 mm or > 4.25 mm or lesion length > 32 mm, lesions located in saphenous vein grafts, unprotected left main coronary artery, ostial lesions, lesions located at a bifurcation or previously stented lesions, diffuse disease or poor fl ow (TIMI < 1) distal to the identifi ed lesions, excessive tortuosity proximal to or within the lesion, recent acute myocardial infarction (AMI) or evidence of thrombus in target vessel multivessel disease, and in-stent restenosis
• Everolimus has been shown to reduce the clearance of some prescription medications when administered orally along with cyclosporine (CsA). Formal drug interaction studies have not been performed with the XIENCE Family of stents because of limited systemic exposure to everolimus eluted from the stent.
• Everolimus is an immunosuppressive agent. Consideration should be given to patients taking other immunosuppressive agents or who are at risk for immune suppression.
• Oral everolimus use in renal transplant patients and advanced renal cell carcinoma patients was associated with increased serum cholesterol and triglycerides, which in some cases required treatment.
• Nonclinical testing has demonstrated that the XIENCE Family of stents, in single and in overlapped confi gurations are MR conditional up to 68 mm in length for XIENCE V and XIENCE nano only and up to 71 mm in length for all other XIENCE Family stents. It can be scanned safely under the conditions in the Instructions for Use.
• The XIENCE Family of stents should be handled, placed, implanted, and removed according to the Instructions for Use.
POTENTIAL ADVERSE EVENTSAdverse events (in alphabetical order) which may be associated with percutaneous coronary and treatment procedure including coronary stent use in native coronary arteries include, but are not limited to:• Abrupt closure, Access site pain, hematoma, or hemorrhage,
Acute myocardial infarction, Allergic reaction or hypersensitivity
to contrast agent or cobalt, chromium, nickel, tungsten, acrylic and fl uoropolymers; and drug reactions to antiplatelet drugs or contrast agent, Aneurysm, Arterial perforation and injury to the coronary artery, Arterial rupture, Arteriovenous fi stula, Arrhythmias, atrial and ventricular, Bleeding complications, which may require transfusion, Cardiac tamponade, Coronary artery spasm, Coronary or stent embolism, Coronary or stent thrombosis, Death, Dissection of the coronary artery, Distal emboli (air, tissue or thrombotic), Emergent or non-emergent coronary surgery, Fever, Hypotension and / or hypertension, Infection and pain at insertion site, Injury to the coronary artery, Ischemia (myocardial), Myocardial infarction (MI), Nausea and vomiting, Palpitations, Peripheral ischemia (due to vascular injury), Pseudoaneurysm, Renal Failure, Restenosis of the stented segment of the artery, Shock/pulmonary edema, Stroke / cerebrovascular accident (CVA), Total occlusion of coronary artery, Unstable or stable angina pectoris, Vascular complications including at the entry site which may require vessel repair, Vessel dissection
Adverse events associated with daily oral administration of everolimus to organ transplant patients include but are not limited to:• Abdominal pain (including upper abdominal pain);
Anemia; Angioedema; Anorexia; Asthenia; Constipation; Cough; Delayed wound healing/fl uid accumulation; Diarrhea; Dyslipidemia (including hyperlipidemia and hypercholesterolemia); Dyspnea; Dysgeusia; Dyspepsia; Dysuria; Dry skin; Edema (peripheral); Epistaxis; Fatigue; Headache; Hematuria; Hyperglycemia (may include new onset of diabetes); Hyperlipidemia; Hyperkalemia; Hypertension; Hypokalemia; Hypomagnesemia; Hypophosphatemia; Increased serum creatinine; Infections and serious infections: bacterial, viral, fungal, and protozoal infections (may include herpes virus infection, polyoma virus infection which may be associated with BK virus associated nephropathy, and/or other opportunistic infections); Insomnia; Interaction with strong inhibitors and inducers of CY3PA4 or PgP; Leukopenia; Lymphoma and other malignancies (including skin cancer); Male infertility (azospermia and/or oligospermia); Mucosal infl ammation (including oral ulceration and oral mucositis); Nausea; Neutropenia; Non-infectious pneumonitis; Pain: extremity, incision site and procedural, back, chest, and musculoskeletal; Proteinuria; Pruritus; Pyrexia; Rash; Stomatitis; Thrombocytopenia; Thrombotic microangiopathy (TMA)/Thrombotic thrombocytopenic purpura (TTP)/ Hemolytic uremic syndrome (HUS); Tremor; Urinary tract infection; Upper respiratory tract infection; Vomiting
• Live vaccines should be avoided and close contact with those that have had live vaccines should be avoided. Fetal harm can occur when administered to a pregnant woman. There may be other potential adverse events that are unforeseen at this time.
XIENCE Safety Results from the Unique Design of the Proven MULTI-LINK Implant
11 The BMS comparator is a composite of several bare metal stents as a representation of the BMS category. 12 Source: Palmerini, et al. The Lancet. 379:9824, 14-20 April 2012, pp. 1393-1402.13 “Meta-analyses should be regarded as hypothesis-generating and the fi ndings of Palmerini and colleagues suggest that a randomized trial of CoCr EES and BMS is desirable.”
Ormiston, The Lancet, April 2012. The XIENCE system’s clinical outcomes result from its components, including: a thin-strut, fl exible ring and link design, with favorable strut apposition, no metal-to-metal touch points, and low strain upon expansion; the novel Everolimus compound; and the multi-layer coating and primer technologies, using a fl uorinated polymer class known for cardiovascular implants, and known for having excellent mechanical properties.
14 An odds ratio is a method of comparing the odds of an event between two groups. 15 Source: Dr. Valgimigli, Effects of Cobalt-chromium everolimus eluting or bare metal stent on fatal and non-fatal cardiovascular events. A patient-level meta analysis. EuroPCR 2014. 16 44% STEMI, 19% diabetes, mean age of 67. The XIENCE system’s clinical outcomes result from its components, including: a thin-strut, fl exible ring and link design, with favorable strut
apposition, no metal-to-metal touch points, and low strain upon expansion; the novel Everolimus compound; and the multi-layer coating and primer technologies, using a fl uorinated polymer class known for cardiovascular implants, and known for having excellent mechanical properties.
P=0.013
Cum
ulat
ive H
azar
d
Cum
ulat
ive H
azar
d
P=0.003
0.00
0.0
2
0
.04
0.00
0
.01
0.
02
0.
03
0 200 400 600 800 Days
0 200 400 600 800 Days
BMS11
XIENCE
BMS11
XIENCE4.0%
2.7%
0.8%
0.08%
P=0.013
Cum
ulat
ive H
azar
d
Cum
ulat
ive H
azar
d
P=0.003
0.00
0.0
2
0
.04
0.00
0
.01
0.
02
0.
03
0 200 400 600 800 Days
0 200 400 600 800 Days
BMS11
XIENCE
BMS11
XIENCE4.0%
2.7%
0.8%
0.08%
XIENCE results in 33% risk reduction XIENCE results in 89% risk reduction
Primary Endpoint: Cardiac Death at 2 Years Fatal Myocardial Infarction at 2 Years
XIENCE Demonstrates Signifi cant Reductions in Cardiac Death and Fatal MI in Meta-Analysis15
98% All-Comer or Complex Patients
- Independent patient-level meta-analysis comparing XIENCE vs. BMS11 in a complex16 patient population
- N=4,896 patients, from 5 randomized clinical trials and follow-up through 2 years
- Presented by Dr. Marco Valgimigli at EuroPCR 2014
Stent Design- Proven CoCr MULTI-LINK design- Flexible stent & delivery system for
conformability, less injury2
- Low metal to artery ratio reduces injury, infl ammation9
- Thin well-apposed struts for rapid re-endothelialization, healing, and reduced thrombogenicity3,4
- Reliable coating integrity because of no touch points and low strain stent design
Coating Technology- Fluorinated polymer5,8
- Coating durability, fl exibility and elasticity for stent use7,8
- Known biocompatible for cardiovascular implants5,6,7
- Attracts albumin to surface for thromboresistance10
- Minimal infl ammation5
- Faster endothelialization5
- Multi-layer application over a primer to minimize coating defects
Drug- Everolimus- Patented for restenosis
reduction- Elution rate matched to
restenosis cascade by optimal coating thickness
- Cytostatic- Low drug dose- Broad therapeutic range
2 Colombo et al.; J Amer Coll Cardiol 2002;40(6): 1021-1033. 3 Kolandaivelu et al.; Circulation 2011; 123; 1400-1409.
4 Kastrati et al.; Circulation 2001; 103; 2816-2821.
5 Paton et al.; U.S. Patent 5,356,668. 6 Lilenfeld et al.; U.S. Patent 4,564,013.
7 Tu et al.; U.S. Patent 4,816,339.
8 Lo et al.; U.S. Patent 3,178,399. 9 Data on fi le at Abbott Vascular.
10 Panchalingam V, et al. ASAIO J 1993;39:M305-M309.
69% All-Comer or Complex Patients
Defi nite Stent Thrombosis Rate
49 RCTs, 50,344 Patients
XIENCE Demonstrates Signifi cantly Lower Stent Thrombosis Rates than BMS11 and Other DES in Large-Scale Meta Analysis12,13
30 Day
2 Year
Odds Ratio14 (95%) Cl
XIENCE vs. BMS11
XIENCE vs. Taxus®
XIENCE vs. Cypher®
XIENCE vs. Endeavor®
XIENCE vs. Endeavor® ResoluteTM
0.21 (0.11-0.42)0.27 (0.14-0.51)0.40 (0.21-0.79)0.22 (0.09-0.54)0.07 (0.00-0.46)
0.35 (0.17-0.69)0.34 (0.19-0.62)
XIENCE vs. BMS11
XIENCE vs. Taxus®
1 Year
0.23 (0.13-0.41)0.28 (0.16-0.48)0.41 (0.24-0.70)0.21 (0.10-0.44)0.14 (0.03-0.47)
XIENCE vs. BMS11
XIENCE vs. Taxus®
XIENCE vs. Cypher®
XIENCE vs. Endeavor®
XIENCE vs. Endeavor® ResoluteTM
0.01 0.1 1 10
Favors XIENCE Favors Other
- Network meta-analysis comparing the safety and effi cacy between DES and BMS11 -Analyzed data across only RCTs -Note that as with any meta-analysis, the underlying studies may have differences in design, enrollment criteria and endpoints; and these results would share the same limitations as the original underlying studies.
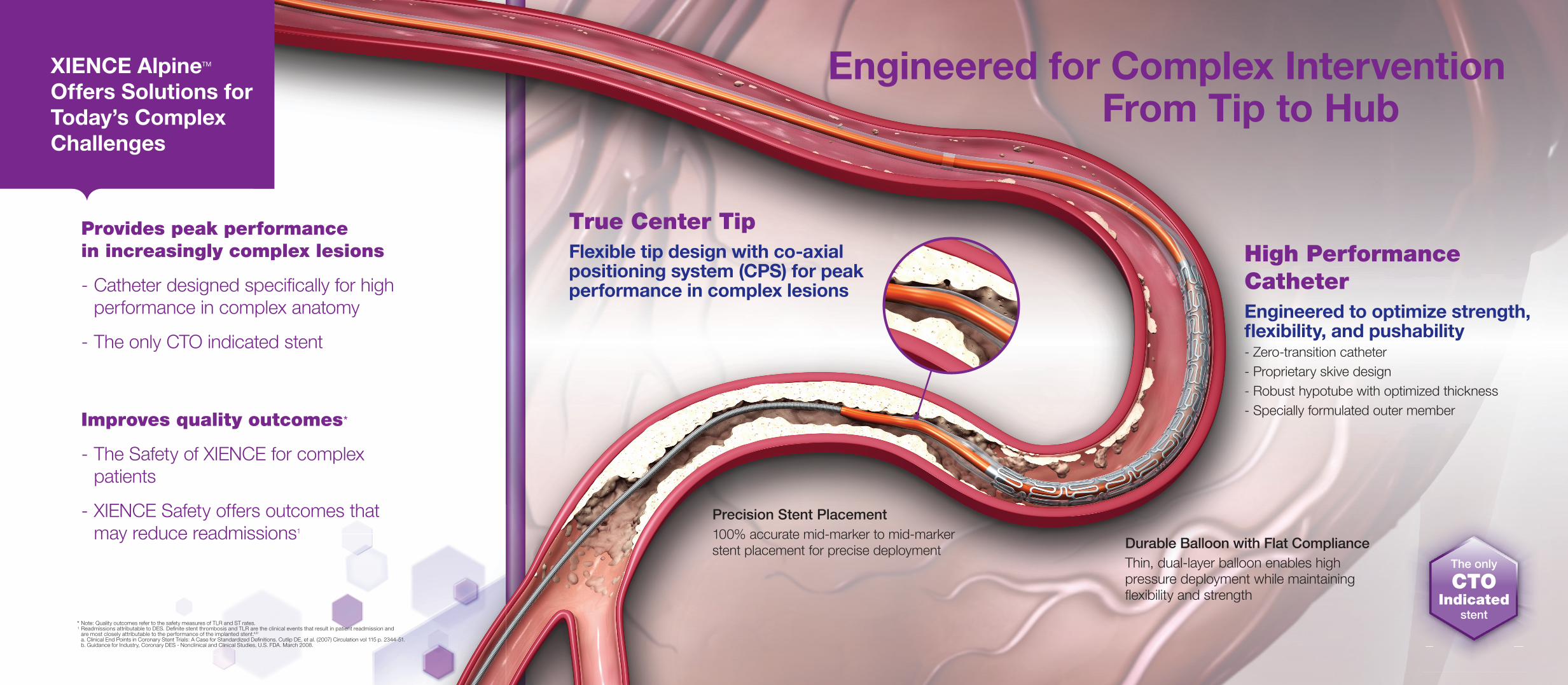
XIENCE AlpineTM Offers Solutions for Today’s Complex Challenges
Provides peak performance in increasingly complex lesions
- Catheter designed specifi cally for high performance in complex anatomy
- The only CTO indicated stent
Engineered for Complex Intervention From Tip to Hub
True Center TipFlexible tip design with co-axial positioning system (CPS) for peak performance in complex lesions
Durable Balloon with Flat ComplianceThin, dual-layer balloon enables high pressure deployment while maintaining fl exibility and strength
Precision Stent Placement100% accurate mid-marker to mid-marker stent placement for precise deployment
High Performance CatheterEngineered to optimize strength, fl exibility, and pushability- Zero-transition catheter- Proprietary skive design- Robust hypotube with optimized thickness- Specially formulated outer member
The only
CTO Indicated
stent
Improves quality outcomes*
- The Safety of XIENCE for complex patients
- XIENCE Safety offers outcomes that may reduce readmissions1
* Note: Quality outcomes refer to the safety measures of TLR and ST rates. 1 Readmissions attributable to DES. Defi nite stent thrombosis and TLR are the clinical events that result in patient readmission and
are most closely attributable to the performance of the implanted stent.a,b a. Clinical End Points in Coronary Stent Trials: A Case for Standardized Defi nitions. Cutlip DE, et al. (2007) Circulation vol 115 p. 2344-51. b. Guidance for Industry, Coronary DES - Nonclinical and Clinical Studies, U.S. FDA. March 2008.






