2. ventilatory modes
77
DR/ MAHMOUD EL NAGGAR Egyptian Board of Neonatology June 1, 2016 1 2. VENTILATORY MODES
-
Upload
mahmoud-elnaggar -
Category
Health & Medicine
-
view
511 -
download
0
Transcript of 2. ventilatory modes

DR/ MAHMOUD EL
NAGGAR
Egyptian Board of NeonatologyJune 1, 2016
1
2. VENTILATORY MODES

Definition of Mechanical
Ventilation
June 1, 2016
2
Mechanical ventilation is the
movement of gas in and out of
the lung by an external source
(an automatic mechanical device)
connected directly to the patient.

Purpose of MV
June 1, 2016
3
Facilitate alveolar ventilation and carbon dioxide removal.
Provide adequate tissue oxygenation
Reduce the work of breathing
Relieve respiratory distress and Reverse respiratory muscle fatigue
Permit lung healing
Avoid complications

Mechanism of action of MV
Patient
lung
Expiration
Patient
lung
Inspiration
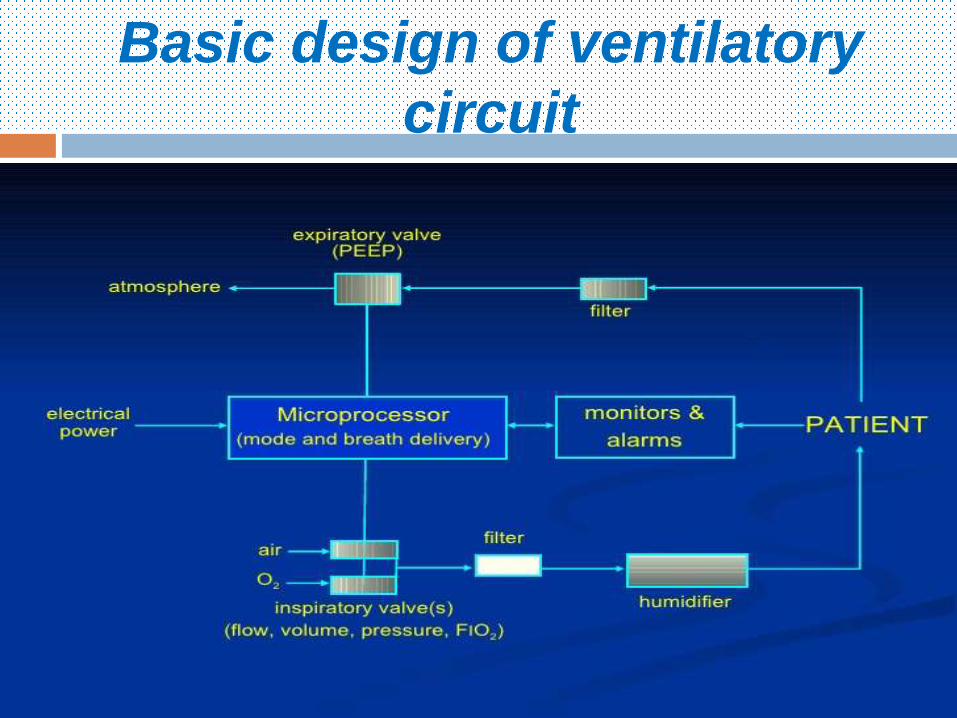
Expiratory valve
Leak
Continuous flowContinuous flow
spontaneo
us

Mechanism of action of MV5

Spontaneous Inspiration
Hera NICU 2016
Volume Change
Gas Flow
Pressure Difference

Mechanical Ventilation
Hera NICU 2016
Pressure Difference
Volume Change
Gas Flow Patient
lung
Inspiration
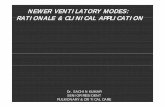
Basic design of ventilatory
circuit
Hera NICU 2016
Expiratory valve
Hera NICU 2016

Unique challenges during
neonatal ventilation
Children ≠ Small adult
Neonate ≠ Small child
10

Classification of Mechanical
ventilators
June 1, 2016
11
1- By power source:
a) Pneumatic
b) Electrical
2- By rate:
a) Conventional
b) High frequency
Classification of Mechanical
ventilators
June 1, 2016
12
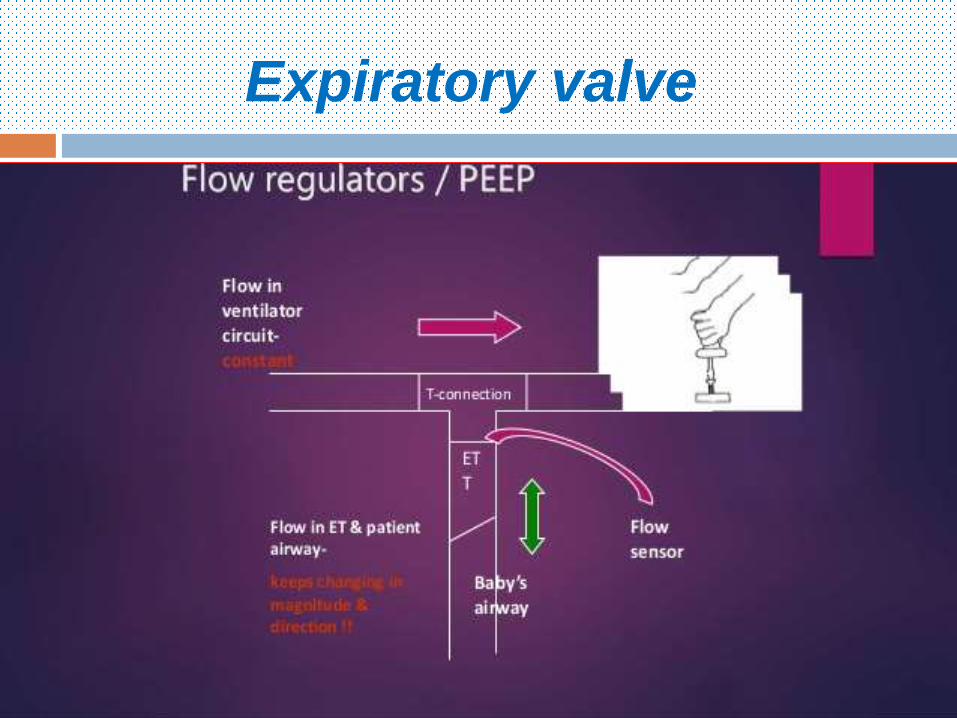
3- By pressure relationship to the patient:
a) Negative
b) Positive
4- By cycling mode at termination of inspiration:
a) Volume cycling
b) Pressure cycling
c) Flow cycling
d) Time cycling
e) Mixed cycling

Classification of Mechanical
ventilators
June 1, 2016
13
5- Loop control of ventilator output:
a) Opened loop
b) Closed loop

Negative-pressure ventilators (iron lungs)
Hera NICU 2016
•Non-invasive ventilation first used in Boston Children’s Hospital in 1928
•Used extensively during polio outbreaks in 1940s – 1950s

Polio outbreaks
June 1, 2016
15
Iron lung polio ward at Rancho Los Amigos Hospital in 1953

Negative pressure
ventilation16

Recent –Ve pressure
ventilator
Hera NICU 2016

1st Positive pressure
ventilation
June 1, 2016
18
• Invasive positive pressure ventilation first used at Massachusetts General Hospital in 1955
• Now the modern standard of mechanical ventilation

Volume control Vs Pressure
control
June 1, 2016
19

Volume control is good and
bad
Guaranteed tidal volume, even with variable
compliance and resistance
Less atelectasis compared to pressure
control
Can cause excessive airway pressure
The limited flow available may not meet the
patient desired inspiratory flow rate –
asynchrony
Leaks leads to volume lossHera NICU 2016

Pressure control is good and
bad
Limit excessive airway pressure
Improve gas distribution
Less tidal volume as pulmonary mechanic
change
Potentially excessive VT as compliance
improves
Hera NICU 2016
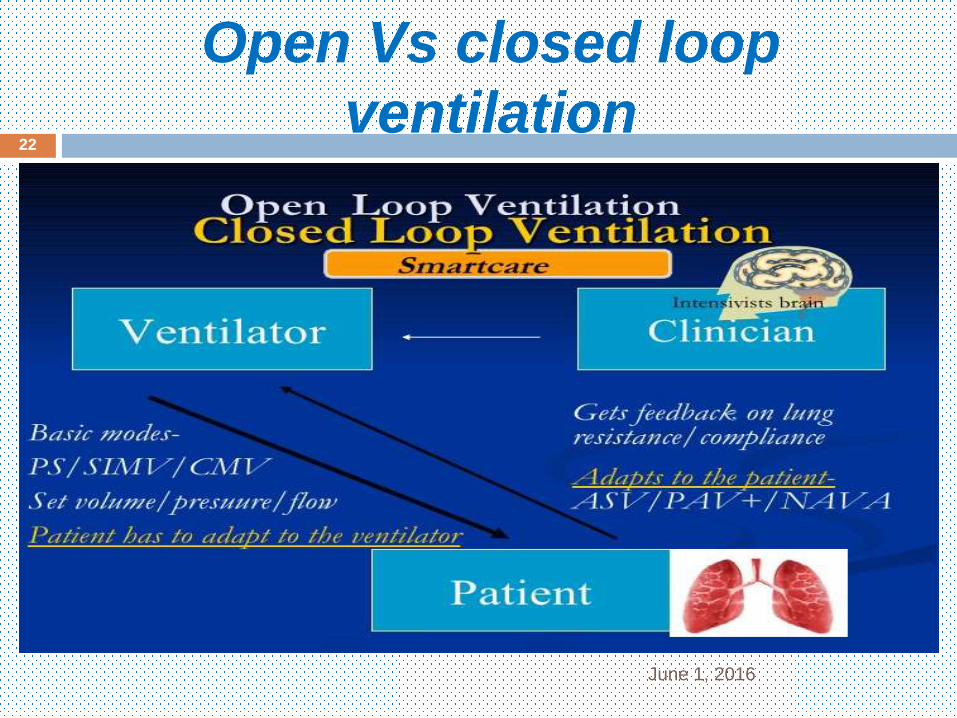
Open Vs closed loop
ventilation
June 1, 2016
22

June 1, 2016
23
1- Set tidal volume
With
2- Safer pressure limit
Target of
neonatal
ventilation

Conventional Neonatal
Ventilators
June 1, 2016
24
Pressure limited
Time cycled
Continuous flow
ventilators

In all pressure controlled
ventilation modes
June 1, 2016
25
Tidal Volume supplied depend on:
1- PIP- PEEP2- Lung mechanics3- Respiratory drive
of the patient

Why volume control not
suitable of newborn?
June 1, 2016
26
Use of small number of tidal volumes
Leak around un-cuffed ET
True tidal volume is influenced by ventilator
circuit compliance
Comprisable volume of the circuit including the
humidifier, can affect the tidal volume

Breath Types during mechanical
ventilation Mandatory (controlled)
Ventilator does the work
Ventilator controls start and stop
Spontaneous Patient takes on work
Patient controls start and stop
Assisted Patients triggers the breath
The ventilator delivers the breath as per control variable
Supported Patients triggers the breath
Ventilator delivers pressure support
Breath cycles at set flow
Hera NICU 2016

Hera NICU 2016

June 1, 2016
29

Ideal ventilator design
June 1, 2016
30
Achieve all the important goals of mechanical
ventilator
Provide a variety of modes that can ventilate
even the most challenging lung diseases.
Has monitoring capabilities to adequately
assess the ventilator and patient performance.
Has safety features and alarms that over lung
protective strategies.
Neonatal ventilator.

Ideal ventilator mode
June 1, 2016
31
The mode which deliver a breath that:
Synchronized with the patient spontaneous breathing
Maintain adequate and consistent tidal volume and minute ventilation at low airway pressure.
Response to rapid change of lung mechanic or patient demands.
Provide the lowest possible work of breathing.
A mode of ventilation is only as good as the operator who applies it.

Anatomy of Pressure waveform
Hera NICU 2016
Ti Te
Pre
ssu
re
Begin
inspiration
Cycle to expiration
Time
Flow determines rate
of rise and reaching
peak pressure
Pressure limited =
“PIP”
PEEP
∆pMAP

Which mode?
June 1, 2016
33
IMV
A/C SIPPV
SIMV
CPAPPS
SIMV&
PS
CM
VVG
BIPAP ASV
PC
V
VCV
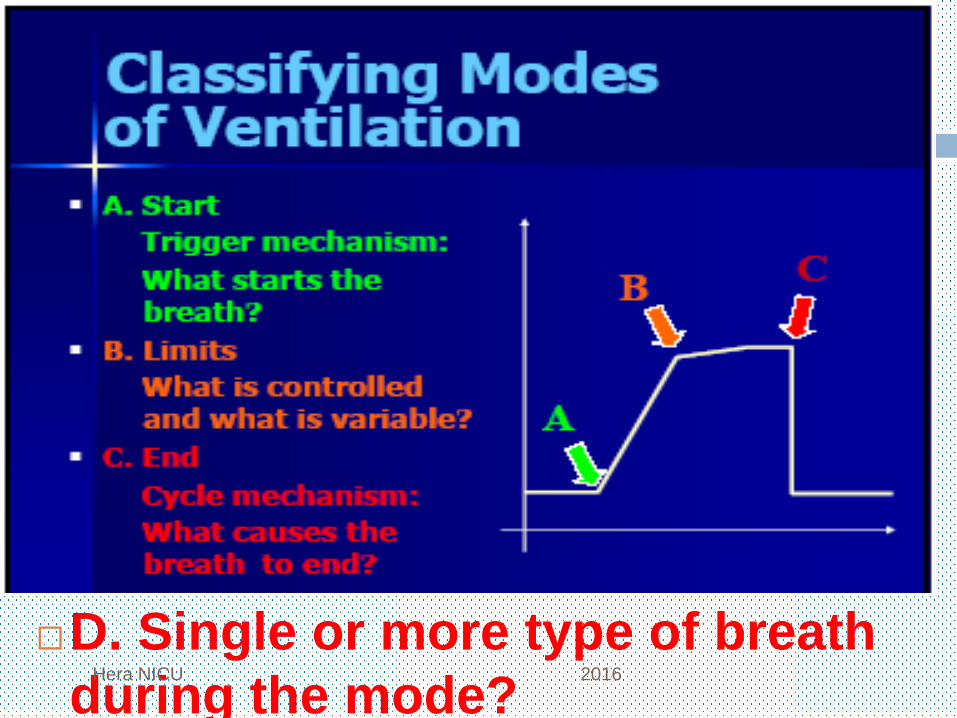
D. Single or more type of breath
during the mode?Hera NICU 2016

Classification of ventilatory
modes
June 1, 2016
35
Trigger:
1- Machine ( IMV)
2- Patient ( SIMV, SIPPV, PS)
Control:
1- Pressure
2- Volume
3- Dual-control

Classification of ventilatory
modes
June 1, 2016
36
Cycling:
1- Time
2- Flow
3- Volume
Types of breaths during ventilation:
1- Mandatory ( controlled)
2- Spontaneous
3- Assisted
4- Supported

Intermittent Mandatory
Ventilation
Controlled Mechanical
Ventilation
Hera NICU 2016
Trigger
Controll
ed
Cycling
Types of
breaths

2 Types of breaths of IMV
June 1, 2016
38

Hazards of desynchronization
June 1, 2016
39
Baby fighting with the ventilator
Inconsistent tidal volume delivery
Inefficient gas exchange
Increase the work of breathing
Abnormally high intra-thoracic and intra-pulmonary pressures leads to Barotrauma
Decreased venous return
Increase intra-cranial pressure leads to IVH
Sub-optimal training of respiratory muscle

So, synchrony is extremely important
and can be achieved by detecting infant’s
inspiratory effort and using it to trigger
positive pressure inflation (triggered-
ventilation).
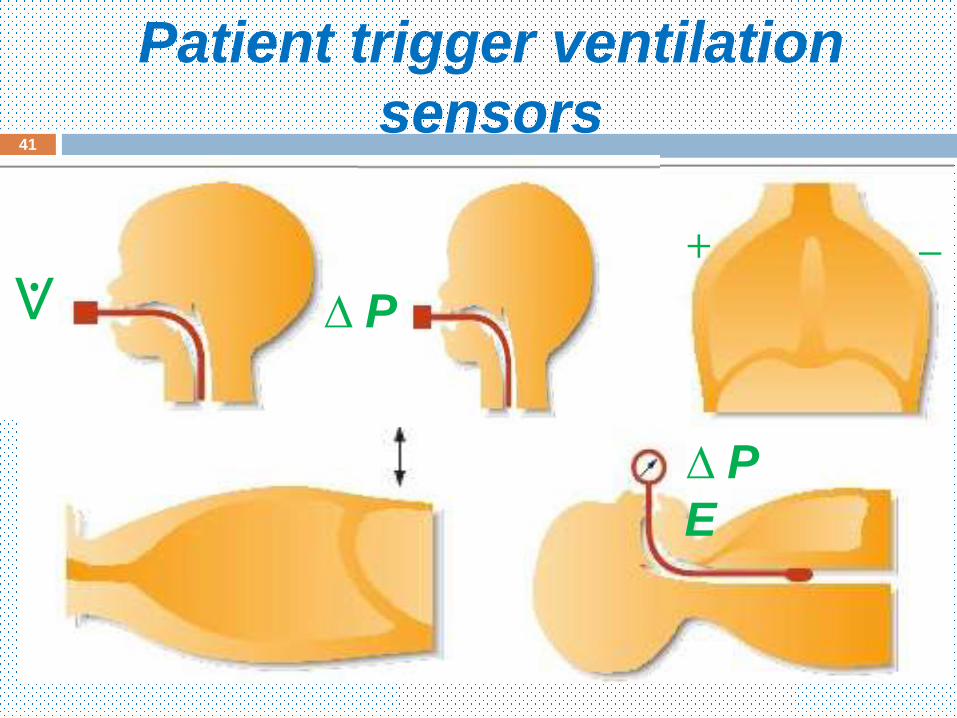
Patient trigger ventilation
sensors
June 1, 2016
41
+ −
∆ P⟇
∆ P
E

June 1, 2016
42
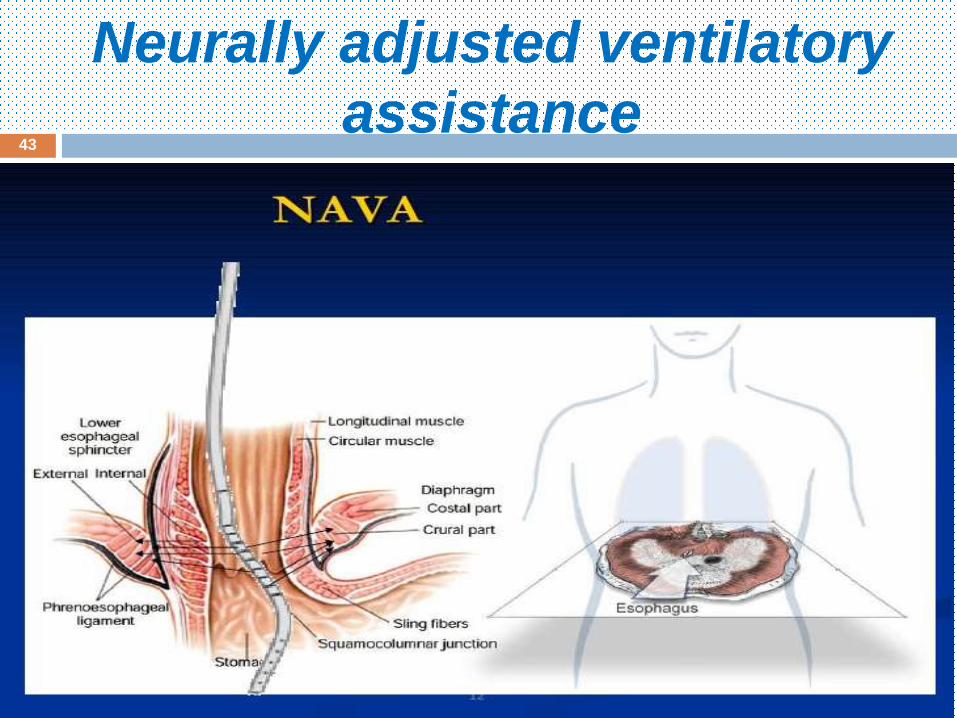
Neurally adjusted ventilatory
assistance
June 1, 2016
43

Steps in the process of activating
a ventilator breath(NAVA).

Trigger sensitivity
June 1, 2016
45
It determine how easy to the patient to trigger
the ventilator to deliver a breath.
Increase the sensitivity improve patient
ventilator synchronization.
High sensitivity my result in false or auto-
triggering.
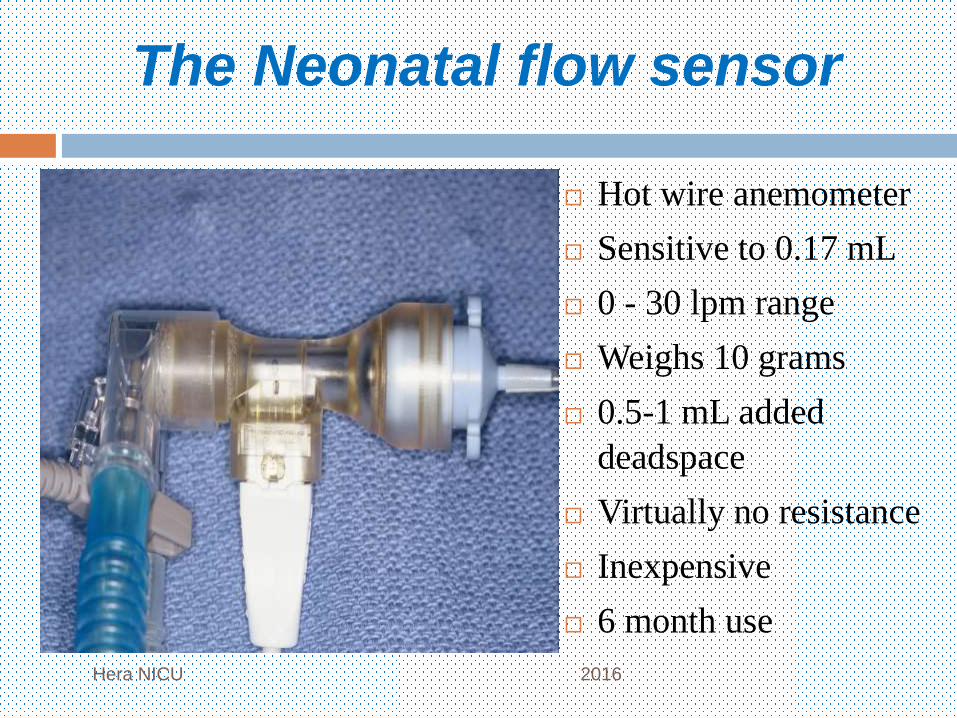
The Neonatal flow sensor
Hera NICU 2016
Hot wire anemometer
Sensitive to 0.17 mL
0 - 30 lpm range
Weighs 10 grams
0.5-1 mL added
deadspace
Virtually no resistance
Inexpensive
6 month use
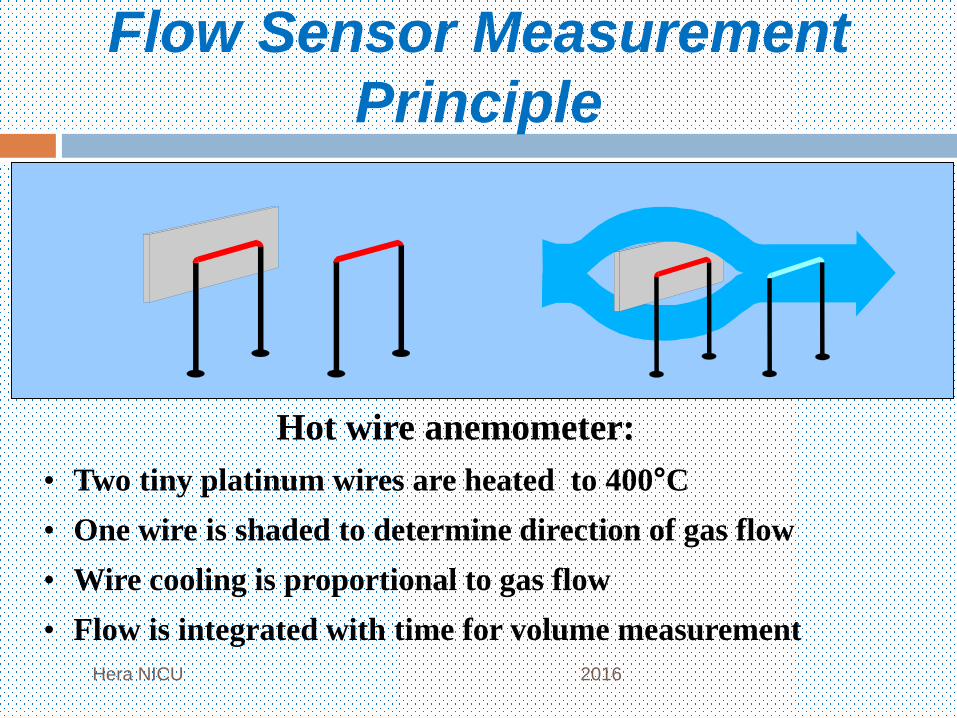
Flow Sensor Measurement
Principle
Hera NICU 2016
Hot wire anemometer:
• Two tiny platinum wires are heated to 400°C
• One wire is shaded to determine direction of gas flow
• Wire cooling is proportional to gas flow
• Flow is integrated with time for volume measurement
Limitations of the flow sensor
June 1, 2016
48
If ET leak, expiratory tidal volume may be
underestimated.
Imposing 1 ml of a dead space , which may
increase the WOB in very tiny preterm.
If less than the expected expiratory tidal
volume due to ET leak is registered as a
negative flow and trigger a ventilator breath,
auto-triggering.

Limitations of the flow sensor
June 1, 2016
49
Humidity; water will create significant
fluctuations of accuracy.
Secretions- surfactant; reading above or below
baseline in the presence of zero flow
Very delicate-breaks easily, wears-out due to
processing and age

Assist/Control
Synchronized Intermittent Positive Pressure
Ventilation
Hera NICU
2016
Trigger
Controll
ed
Cycling
Types of
breaths
Trigger window

June 1, 2016
51

2 Types of breaths on A/C
June 1, 2016
52

Synchronized Intermittent
Mandatory Ventilation
Hera NICU 2016
Trigger
Controll
ed
Cycling
Types of
breaths
Trigger windo
w

3 Types of breaths of SIMV
June 1, 2016
54

June 1, 2016
55

A/C Vs SIMV
June 1, 2016
56
More stable tidal volume
Less tachypnea
Smaller blood pressure fluctuation
Smaller tidal volume
Lower work of breathing
Faster weaning from mechanical ventilator
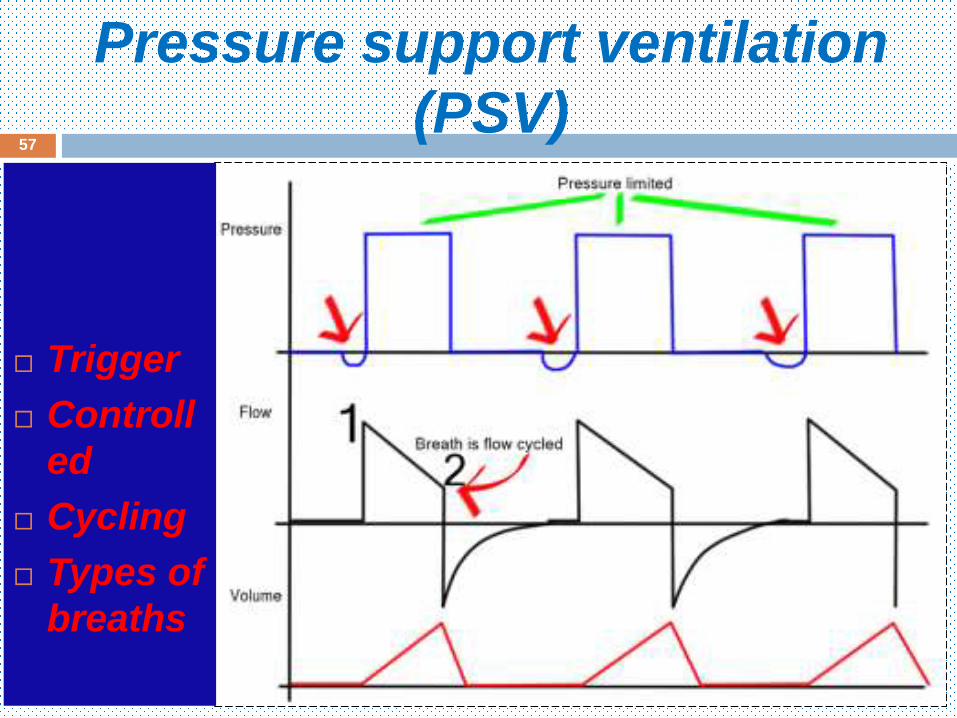
Pressure support ventilation
(PSV)
June 1, 2016
57
Trigger
Controll
ed
Cycling
Types of
breaths

Paw
V•
insp
exp
Patient or
vent ilator
initiated
inspiration PSV cycled
expiration
Peak flow
Drop to 15%
of peak flow
Pressure Support Ventilation
Set Pinsp
Hera NICU 2016

PSV Vs A/C
June 1, 2016
59
PSV, Allow the newborn more control over the
respiratory pattern, with synchronization at the
end of inspiration not only the beginning.
PSV, Decreasing asynchrony by minimize the
chance of active expiration against high
positive pressure.
PSV, Automatically adjust Ti according to
change in patient time constant breath by
breath.
PSV, Allow the infant to sigh as needed to
prevent atelectasis.

Synchronized intermittent
mandatory ventilation &
pressure support
June 1, 2016
60
Trigger
Controll
ed
Cycling
Types of
breaths

Proportional Assist Ventilation (PAV)&
Neurally adjusted ventilatory
assistance(NAVA)
June 1, 2016
61
New ventilatory modes designed to assist
spontaneous ventilation
The breath delivered is similar to PS but the
pressure support level is variable and is
proportional to patient spontaneous effort
a) The harder the patient work = the more
support by ventilator
b) The less the patient work = the less
support is provided
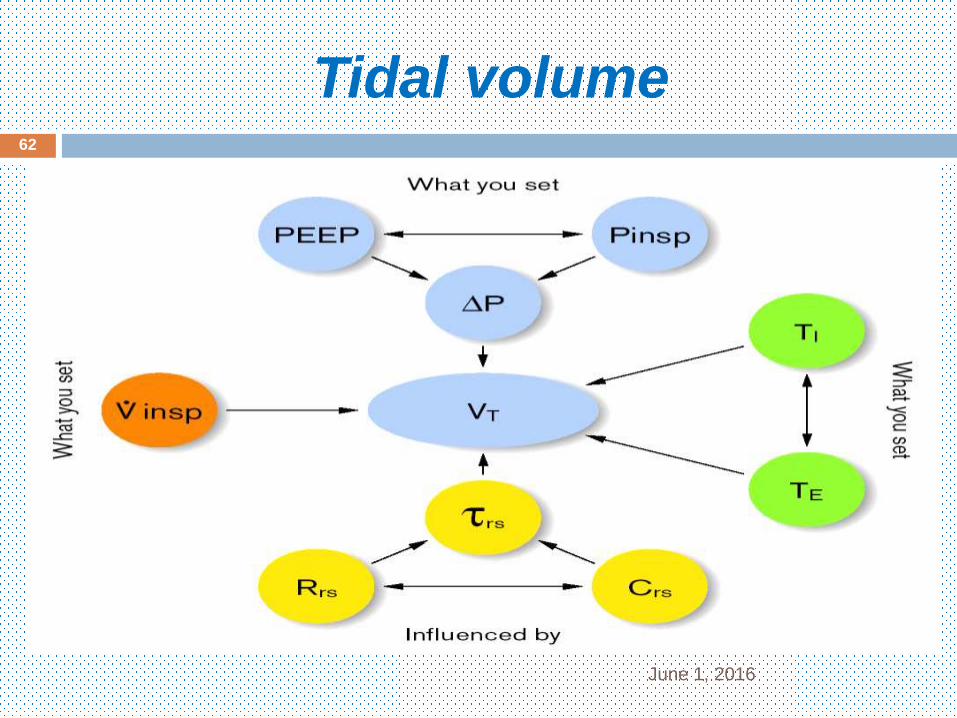
Tidal volume
June 1, 2016
62

Volume Guarantee
June 1, 2016
63
Working principle of Volume Guarantee. According to a set tidal volume, inspiratory pressure is automatically regulated by the ventilator.

Volume Guarantee (Dual-Control
Mode)
June 1, 2016
64
Several breaths may be needed to reach the target tidal volume after a sudden change.
Maximum
pressure

Principle of working of Volume
Guarantee
June 1, 2016
65
Test breath
Measure Vt
Inspiratory
pressure
Same
inspiratory
pressure
Inspiratory pressure
Compare to set VtMore
Equal
Less

Why volume targeted ventilation in
neonate?
Consistent VT Stable PaCO2 Stable CBF Less IVH
Hera NICU 2016

Open the lung and keep it
opened
June 1, 2016
67
The benefit of
Volume Targeted
Ventilation can not
be realized without
ensuring that the
tidal volume is
evenly distributed
throughout
an (open lung)
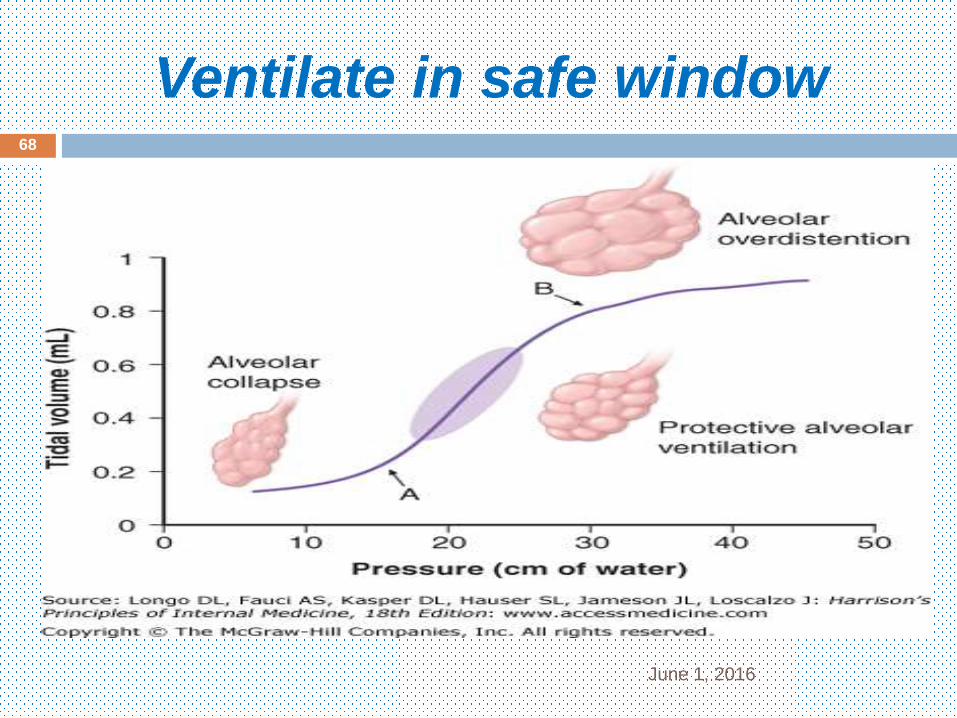
Ventilate in safe window
June 1, 2016
68
Volume guarantee why?
June 1, 2016
69
It is volu-trauma than baro-trauma
More stable tidal volume
Wean PIP if lung mechanics improved
Less hypo-capnea
Work better with A/C than SIMV
Bio-trauma decreased with TV 5ml/kg
Faster weaning from mechanical ventilator

Pressure Support + Volume
Guarantee
Concept of “Auto-weaning”
Hera NICU 2016
PIP
C lung
Vt
ExtubateTime

Patient control
Hera NICU 2016

Mandatory Minute Ventilation
MMV
June 1, 2016
72
Guarantee a minimum minute ventilation ( RR x TV)
If the patient maintain a MV above the set MV this mode will function like PS mode
If the patient MV falls below the set MV the mode will deliver mandatory breaths ( SIMV or IMV + VG), only the numbers of breaths that required to return patient MV to the set MV
Depends on the patient ventilatory drive
When the spontaneous breathing increased, fewer mandatory breaths will be provided
PC- MMV
June 1, 2016
73

Relationship between patient
effort and ventilator pressure
during various ventilation
modes.

Adaptive Support Ventilation
!!!???
June 1, 2016
75
Body weight
Sex
ASV delivers pressure-controlled breaths using an adaptive (optimal) scheme .
“Optimal” means minimizing the mechanical work of breathing
The machine selects a tidal volume and frequency that the patient’s brain would presumably select if the patient were not connected to a ventilator.
This pattern is assumed to encourage the patient to generate spontaneous breaths.

Different ventilatory modes
and their characteristics
Weaning byPIPInspiratory
time
Ventilator
respiration
rate
Assistance
of each
breath
Inspiratory
trigger
Ventilatory
mode
RR&
PIP
Fixe
d
Fixe
d
Fixe
dNoNoIMV
RR&
PIP
Fixe
d
Fixe
d
Fixe
dNoYesSIM
V
PIPFixe
d
Fixe
d
Variabl
eYesYesAC/
SIPP
V
PIPFixeVariablVariablYesYesPS

Thanks