2. Hydrocephalus
51
Hydrocephalus Dr.Arie Ibrahim SpBS Dr.Arie Ibrahim SpBS SMF/LAB Bedah Saraf SMF/LAB Bedah Saraf RSU A Wahab Sjahranie/PSKU RSU A Wahab Sjahranie/PSKU UNMUL UNMUL Samarinda Samarinda
-
Upload
bocahbritpop -
Category
Documents
-
view
70 -
download
2
description
tes
Transcript of 2. Hydrocephalus

Hydrocephalus
Dr.Arie Ibrahim SpBSDr.Arie Ibrahim SpBSSMF/LAB Bedah SarafSMF/LAB Bedah Saraf
RSU A Wahab Sjahranie/PSKU RSU A Wahab Sjahranie/PSKU UNMULUNMUL
SamarindaSamarinda

DefinisiDefinisi
•Hydrocephalus Hydrocephalus : penumpukan : penumpukan cairan di dalam rongga cairan di dalam rongga ventrikelventrikel atau rongga atau rongga subarakhnoid.subarakhnoid.
•Bisa didapatkan pada bayi dan Bisa didapatkan pada bayi dan anak-anak ataupun pada orang anak-anak ataupun pada orang dewasa.dewasa.


IncidenceIncidence•Occurs in 3-4 of every 1000 births.Occurs in 3-4 of every 1000 births.
•Cause may be congenital or acquired.Cause may be congenital or acquired.
•Congenital Congenital - may be due to - may be due to maldevelopment or intrauterine maldevelopment or intrauterine infection ( toxoplasmosis etc)infection ( toxoplasmosis etc)
•Acquired Acquired - may be due to infection, - may be due to infection, neoplasm or hemorrhage.neoplasm or hemorrhage.

PathophysiologyPathophysiology
•CSF is formed by two mechanisms:CSF is formed by two mechanisms:– Secretion by the choroid plexusSecretion by the choroid plexus,,– Lymphatic-like drainage by the Lymphatic-like drainage by the
extracellular fluid in brain.extracellular fluid in brain.
CSF circulates thru ventricular system CSF circulates thru ventricular system and is absorbed within subarachnoid and is absorbed within subarachnoid spaces by unknown mechanism.spaces by unknown mechanism.


Mechanisms of Fluid Mechanisms of Fluid ImbalanceImbalance•Hydrocephalus results from:Hydrocephalus results from:
1. 1. Impaired absorption of CSFImpaired absorption of CSF
within the subarachnoid space within the subarachnoid space (communicating hydrocephalus), or(communicating hydrocephalus), or
2. 2. Obstruction to the flow of CSFObstruction to the flow of CSF through the ventricular system (non-through the ventricular system (non-communicating hydrocephalus)communicating hydrocephalus)
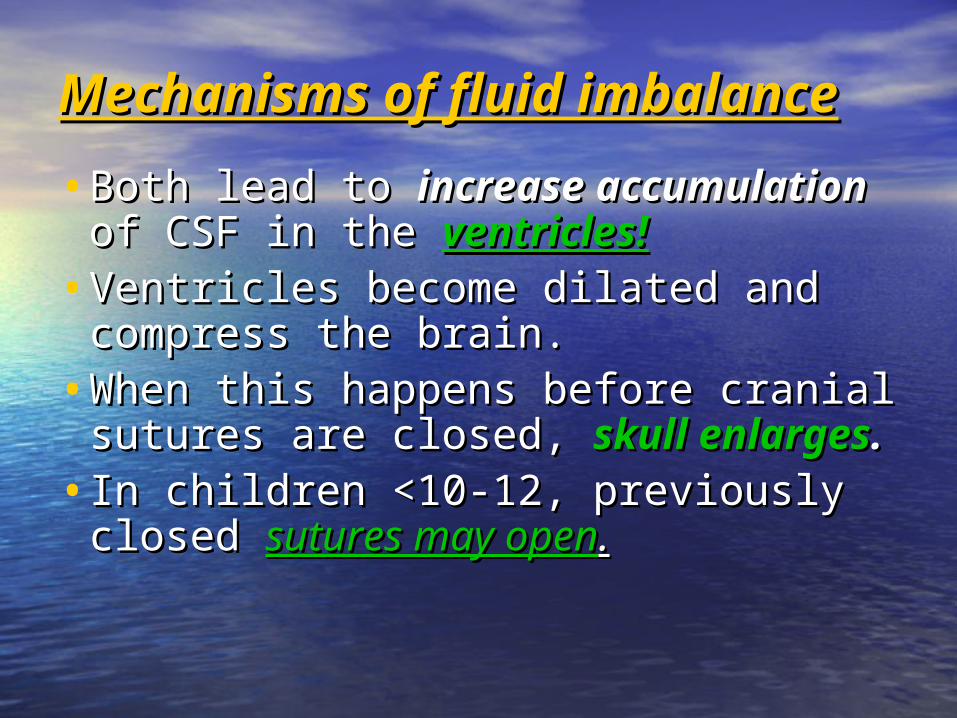
Mechanisms of fluid Mechanisms of fluid imbalanceimbalance•Both lead to Both lead to increase accumulationincrease accumulation
of CSF in the of CSF in the ventricles!ventricles!•Ventricles become dilated and Ventricles become dilated and
compress the brain.compress the brain.•When this happens before cranial When this happens before cranial
sutures are closed, sutures are closed, skull enlargesskull enlarges.. • In children <10-12, previously closed In children <10-12, previously closed
sutures may opensutures may open..

HydrocephalusHydrocephalus
• Most cases of Most cases of non-communicatingnon-communicating
(obstructive) hydrocephalus are a result (obstructive) hydrocephalus are a result
of developmental malformationsof developmental malformations
• Other causes: neoplasms, Other causes: neoplasms, intrauterine intrauterine
infectionsinfections, , trauma.trauma.
• Developmental defects account for most Developmental defects account for most
causes of hydrocephalus from birth to 2 causes of hydrocephalus from birth to 2
years of age. years of age.

Common DefectsCommon Defects
•Arnold-Chiari MalformationArnold-Chiari Malformation (ACM) (ACM)– Type 2 malformation of brain seen most Type 2 malformation of brain seen most
exclusively with exclusively with myelomeningocelemyelomeningocele, is , is characterized by herniation of a small characterized by herniation of a small cerebellum, medulla, pons, and fourth cerebellum, medulla, pons, and fourth ventricle into the cervical spinal canal ventricle into the cervical spinal canal through an enlarged foramen magnum. through an enlarged foramen magnum.



Clinical manifestationsClinical manifestations
•Clinical picture depends on Clinical picture depends on
acuity of acuity of onsetonset and and
presence of preexisting presence of preexisting
structural lesionsstructural lesions..

InfancyInfancy
• Head grows at alarming rate with Head grows at alarming rate with hydrocephalus.hydrocephalus.– First signsFirst signs bulgingbulging of fontanels without of fontanels without
head enlargement.head enlargement.
– Tense, bulging, non-pulsatile anterior Tense, bulging, non-pulsatile anterior fontanelfontanel
– Dilated scalp veinsDilated scalp veins, esp. when crying, esp. when crying
– Thin skull bones with separated sutures Thin skull bones with separated sutures ((cracked pot sounds on percussioncracked pot sounds on percussion))

InfancyInfancy• Protruding forehead or Protruding forehead or bossing.bossing.
• Depressed eyes or Depressed eyes or setting-sun eyessetting-sun eyes ( (eyes eyes rotating or downward with sclera visible rotating or downward with sclera visible above pupil)above pupil)
• Pupils sluggish with unequal response to lightPupils sluggish with unequal response to light
• Irritability, lethargy, feeds poorly, changes in Irritability, lethargy, feeds poorly, changes in LOC, arching of back (opisthotonos), lower LOC, arching of back (opisthotonos), lower extremity spasticity.extremity spasticity.
• May cry when picked up or rocked; quiets May cry when picked up or rocked; quiets when allowed to lay still.when allowed to lay still.



InfancyInfancy•Swallowing difficulties, stridor, Swallowing difficulties, stridor,
apnea, aspiration, respiratory apnea, aspiration, respiratory difficulties and arm weakness may difficulties and arm weakness may indicate indicate brain stem brain stem compressioncompression..
• If hydrocephalus progresses, If hydrocephalus progresses, difficulty sucking and feeding, and a difficulty sucking and feeding, and a high-pitched shrill cry results. high-pitched shrill cry results. ((lower brain stem dysfunction)lower brain stem dysfunction)


InfancyInfancy
•Emesis, somnolence, seizures, Emesis, somnolence, seizures,
and cardiopulmonary distress and cardiopulmonary distress
ensues and hydrocephalus ensues and hydrocephalus
progresses.progresses.
•Severely affected infants may not Severely affected infants may not
survive neonatal period.survive neonatal period.

ChildhoodChildhood
•Signs and symptoms caused by Signs and symptoms caused by
increased ICP.increased ICP.
•Manifestations caused by posterior Manifestations caused by posterior
neoplasms and aqueduct stenosis, neoplasms and aqueduct stenosis,
manifestations associated with manifestations associated with
space-occupying lesions.space-occupying lesions.

ChildhoodChildhood•Headache on awakening with Headache on awakening with
improvement following emesis or sitting improvement following emesis or sitting up.up.
•Papilledema (swelling of optic disc DT Papilledema (swelling of optic disc DT obstruction), strabismus, and obstruction), strabismus, and extrapyramidal tract signs such as ataxiaextrapyramidal tract signs such as ataxia
• Irritability, lethargy, apathy, confusion, Irritability, lethargy, apathy, confusion, and often incoherent and often incoherent


ChildhoodChildhood
•Dandy-Walker syndrome-Dandy-Walker syndrome- congenital defect-late onset.congenital defect-late onset.– Obstruction of foramen of Lushka Obstruction of foramen of Lushka
and Magendieand Magendie
– Bulging occiput, nystagmus, ataxia, Bulging occiput, nystagmus, ataxia, cranial nerve palsiescranial nerve palsies
– Female predominance (3:1)Female predominance (3:1)
– Absence or occlusion of ventriclesAbsence or occlusion of ventricles

Diagnostic Diagnostic EvaluationEvaluation
• Antenatal- fetal Antenatal- fetal ultrasoundultrasound as early as as early as
14 weeks14 weeks
• Infancy- based on head circumference Infancy- based on head circumference
crosses one or more grid lines on the crosses one or more grid lines on the
infant growth chart within a 4 week infant growth chart within a 4 week
period and there are progressive neuro period and there are progressive neuro
signs.signs.
• CT CT and and MRIMRI to localize site of to localize site of
obstruction; reveal large ventriclesobstruction; reveal large ventricles



Therapeutic Therapeutic managementmanagement
GoalsGoals
•Relieve hydrocephalyRelieve hydrocephaly
•Treat complicationsTreat complications
•Manage problem resulting from Manage problem resulting from effects of disorder on effects of disorder on psychomotor developmentpsychomotor development
•USUALLY USUALLY SURGICAL SURGICAL

Surgical TreatmentSurgical TreatmentTherapy of choice!Therapy of choice!
1.1. Direct removal of source of obstruction Direct removal of source of obstruction
(neoplasm, cyst, or hematoma)(neoplasm, cyst, or hematoma)
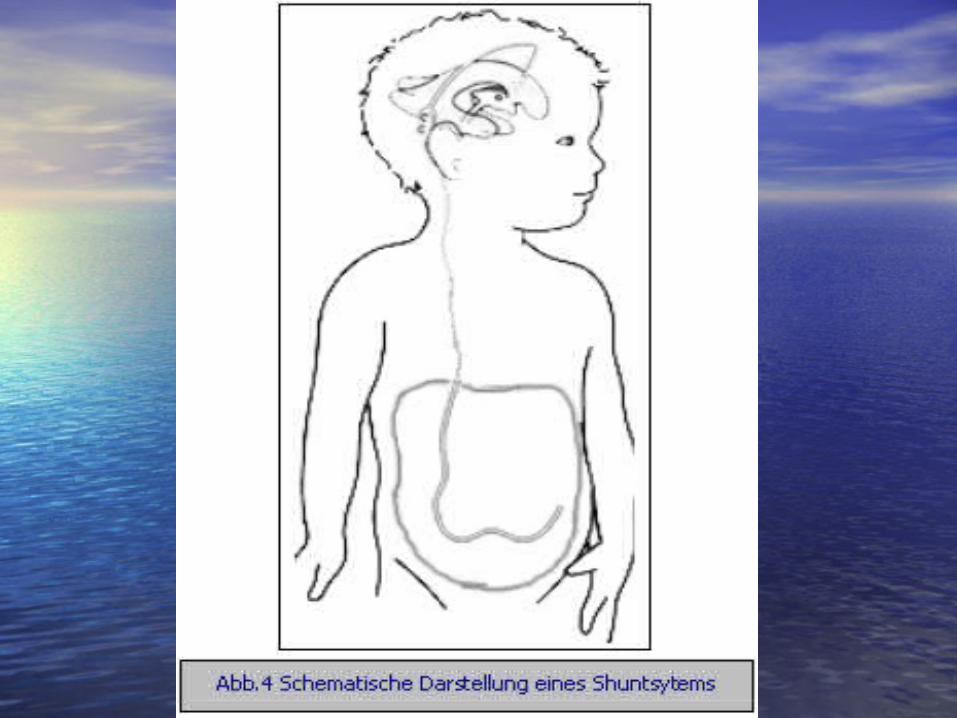
2.2. Most require shunt procedure to drain Most require shunt procedure to drain
CSF from ventricles to extracranial area; CSF from ventricles to extracranial area;
usually peritoneum (usually peritoneum (VP shuntVP shunt), or right ), or right
atrium (atrium (VA shuntVA shunt) for absorption. ) for absorption.
3.3. NeuroendoscopicNeuroendoscopic procedure . procedure .


VP shunt VP shunt (ventriculoperitoneal (ventriculoperitoneal ))
•Used in Used in neonatesneonates and and young young
infantsinfants
•Greater allowance for excess Greater allowance for excess
tubing; which minimizes number tubing; which minimizes number
of revisions needed as child growsof revisions needed as child grows

VA shunt VA shunt ( Ventriculoatrial )( Ventriculoatrial )
•Reserved for Reserved for older childrenolder children who have attained most of who have attained most of somatic growth, or children somatic growth, or children with abdominal pathology.with abdominal pathology.
•ContraindicatedContraindicated in children in children with cardiopulmonary disease with cardiopulmonary disease or with elevated CSF protein.or with elevated CSF protein.











Major ComplicationsMajor Complications
•Shunt Shunt infectioninfection is most serious is most serious complication!complication!
•Period of greatest risk is 1 to 2 Period of greatest risk is 1 to 2 months following placement.months following placement.
•staphylococcus and staphylococcus and streptococcusstreptococcus, most common , most common organismsorganisms

ComplicationsComplications
•Mechanical difficultiesMechanical difficulties
kinking, plugging, migration of tubing.kinking, plugging, migration of tubing.
•MalfunctionMalfunction is most often by is most often by
mechanical obstruction!mechanical obstruction!
•Look for signs of increased ICP; fever, Look for signs of increased ICP; fever,
inflammation and abdominal pain.inflammation and abdominal pain.

Post-op carePost-op careIn addition to routine post-op care:In addition to routine post-op care:
• 1. Place on unoperated side to prevent 1. Place on unoperated side to prevent pressure on shunt valvepressure on shunt valve
• 2. Keep 2. Keep HOB flatHOB flat; rapid decrease in IC ; rapid decrease in IC fluid may cause subdural hematoma fluid may cause subdural hematoma due to small vein rupture in cerebral due to small vein rupture in cerebral cortex.cortex.
• 3. 3. Do not pump shuntDo not pump shunt withoutwithout specific direction from doctor (too many specific direction from doctor (too many different pump devices)different pump devices)

Post-op carePost-op care• 4. Observe for signs of 4. Observe for signs of Increased ICPIncreased ICP! !
May indicate obstruction of shunt!May indicate obstruction of shunt!– Assess Assess pupil sizepupil size; as pressure on ; as pressure on
oculomotor nerve may cause dilation oculomotor nerve may cause dilation on same side as pressure.on same side as pressure.
– Blood pressureBlood pressure may be variable due may be variable due to hypoxia to brainstemto hypoxia to brainstem
– Abdominal distention-Abdominal distention- due to CSF due to CSF peritonitis or post-op ileus due to peritonitis or post-op ileus due to catheter placement.catheter placement.

•5. Monitor I and O- may be on fluid 5. Monitor I and O- may be on fluid restriction or NPO for 24 hours to restriction or NPO for 24 hours to prevent fluid overload.prevent fluid overload.
•6. Monitor VS- 6. Monitor VS- increased tempincreased temp may indicate infection.may indicate infection.
•7. Give good skin care to prevent 7. Give good skin care to prevent tissue damage, etc.tissue damage, etc.
Post-op carePost-op care

Family supportFamily support
•FearFear
•Communication of Communication of
proceduresprocedures
•Prepare for discharge.Prepare for discharge.