
2 Hour Surgical Complications
95
Complications: How to Treat and Avoid PART 2 – HOST FACTORS LOCAL BONE QUALITY / QUANTITY, LOADING, HYGIENE, GINGIVA
-
Upload
dr-paul-binon -
Category
Documents
-
view
220 -
download
5
description
PART 2 – HOST FACTORS LOCAL BONE QUALITY / QUANTITY, LOADING, HYGIENE, GINGIVITIS
Transcript of 2 Hour Surgical Complications

Complications: How to Treat and Avoid
PART 2 – HOST FACTORS LOCAL BONE QUALITY / QUANTITY, LOADING, HYGIENE,
GINGIVA

Surgical Complications
Host
Factors
Systemic
Factors
Local
Factors
Contributing
Etiology Non Host
Factors
Operator
Related
Biomaterial
Related
(Based on Etiology)

Surgical Complications:
Host Factors
• Systemic
• Age/health
• Previous periodontitis
• Smoking
• Genetics/Immunity
• Local
• Bone quality/quantity
• Excessive loading
• Poor plaque control
• Keratinized gingiva

Bone Quality/Quantity:
Anatomic Location
• Bränemark implants
• Higher failure in:
• Maxilla vs mandible
• Posterior vs anterior
Friberg et al., 1991, 1997, Henry et al., 1993 Zarb and Schmidt, 1990,Esposito et al., 1998 Adell et al., 1981, 1990, Albrektsson 1998 Becker et al., 1999, Moy et al 2006

Implants # Placed # Lost % Lost
Type I, II, III 3,192 113 4%
Type IV 1,009 160 16%
• J. Prost. Dent., 2003, Goodacre et. al.
7 Studies-Implant Loss: by Bone Quality

WHICH ONE WILL FAIL ?

SHORT MAXILLARY IMPLANTS IN
GRAFTED AND TYPE 4 BONE
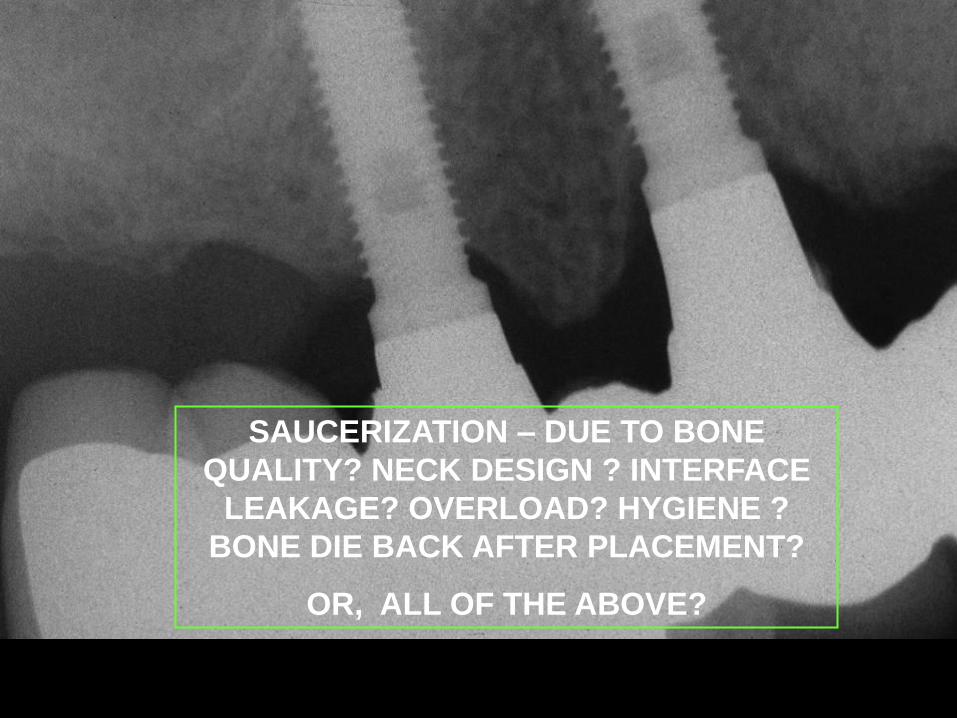
SAUCERIZATION – DUE TO BONE
QUALITY? NECK DESIGN ? INTERFACE
LEAKAGE? OVERLOAD? HYGIENE ?
BONE DIE BACK AFTER PLACEMENT?
OR, ALL OF THE ABOVE?

Bone Quality/Quantity:
Anatomic Location
• Higher early failure in very “dense”
bone due to:
• Iatrogenic overheating
• Diminished blood supply
Truhlar et al, 1994

Failure by Bone Quality
7.7%
5.6%
6.9%
17.1%
0
2
4
6
8
10
12
14
16
18F
ailu
re (
%)
Quality 1 Quality 2 Quality 3 Quality 4
Bone Quality

BONE QUANTITY AND IMPLANT
LENGTH ARE INTER-RELATED
WHICH WILL FAIL?

15 Years Restoration

Implants # Placed # Lost % Lost
Up to
10mm 2,754 272 10%
Greater
10mm 3,015 105 3%
• J. Prost. Dent., 2003, Goodacre et. al.
13 Studies-Implant Loss: by Implant Length

4.9% 6.7%
7.9%
21.8%
0
2
4
6
8
10
12
14
16
18
20F
ailu
re %
Volume A Volume B Volume C Volume D
Bone Quantity
Failure By Bone Quantity
L
O
T
S
M
I
N
I
M
A
L

0%
3.3%6.3%
32.9%
0%
5%
10%
15%
20%
25%F
ailu
re %
A1 B2 C3 D4
Bone Quantity
Failure by Bone Quality & Quantity

Short Implants: Advantages
• May avoid sinus grafting
• May avoid vertical bone augmentation
• May avoid inferior alveolar nerve transposition
• May reduce cost, time, morbidity and failure

“Short Implants: An Analysis of Longitudinal Studies”
Das Neves et al, JOMI, 2006
9.7%
7.5%
6.3%
5.4%
0
1
2
3
4
5
6
7
8
9
10
Failu
re (
%)
3.75 x 7 4.00 x 7 3.75 x 10 4.00 x 10
Implants
N =
66
N =
1,8
94
N =
1,7
83
N =
164
4.8%
95.2%
786 Failures
66.7
%
27.2
%
Poor Bone
Quality
Occlusal
Overload
• Medline search 1980-2004, for 7,8.5 or 10mm
• 33 studies, 16,344 Branemark and 3i implants
Attributed Etiology for Failure

Short Implants: (Medline Search 1980-2004)
Conclusions: • Short implants, a relative risk factor
• Prognosis may be improved with: 1. Better bone quality
2. Wider diameter implants
3. Rough surface implants
4. Good primary stability
5. Splinting
• Das Neves et al, JOMI, 2006
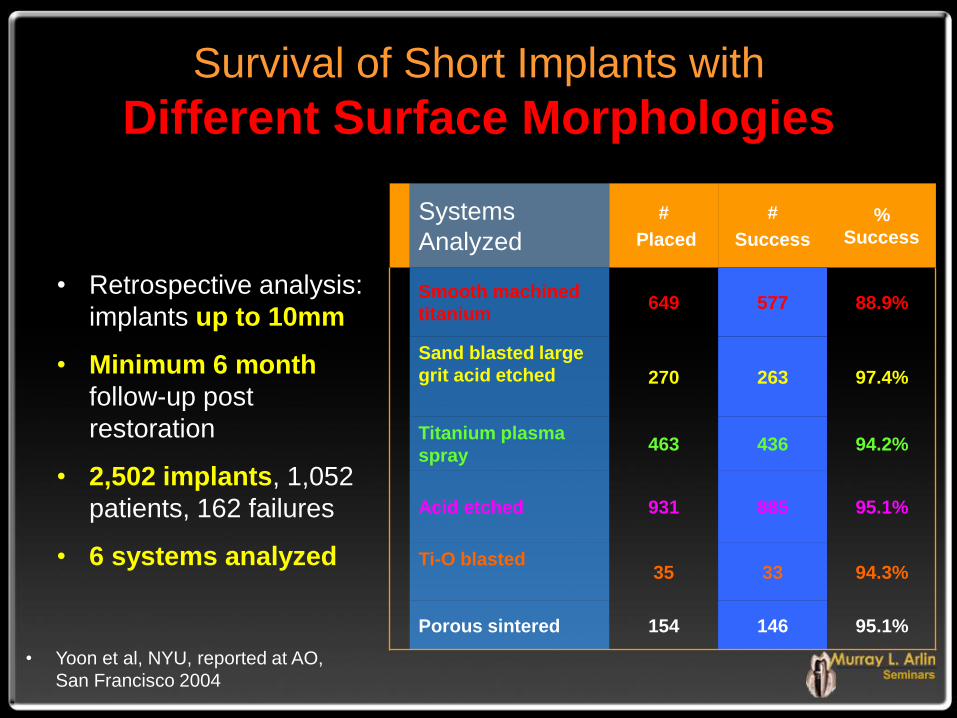
Survival of Short Implants with
Different Surface Morphologies
• Retrospective analysis:
implants up to 10mm
• Minimum 6 month
follow-up post
restoration
• 2,502 implants, 1,052
patients, 162 failures
• 6 systems analyzed
Systems
Analyzed
#
Placed
#
Success
%
Success
Smooth machined
titanium 649 577 88.9%
Sand blasted large
grit acid etched
270 263 97.4%
Titanium plasma
spray 463 436 94.2%
Acid etched 931 885 95.1%
Ti-O blasted
35 33 94.3%
Porous sintered 154 146 95.1%
• Yoon et al, NYU, reported at AO,
San Francisco 2004

Short Implants in the Severely Resorbed Maxilla: A 2 year Retrospective Clinical Study
• 85 patients, 96 short implants (6-8.5mm)
• Single and partially edentulous restorations
• One stage with delayed loading protocol
• Minimum 2 year follow up (average 37.6 months)
• 54 machined and 42 TiUnite implants
• Initial stability “optimized”
• Cumulative survival rate of 94.6%
• 92.6%-machined surface (4/54)
• 97.6%-TiUnite surface (1/42)
• Mean marginal bone resorption was 0.44 +- 0.52mm
• Renouard and Nisand, Clin Impl Dent and Related Res, 2005
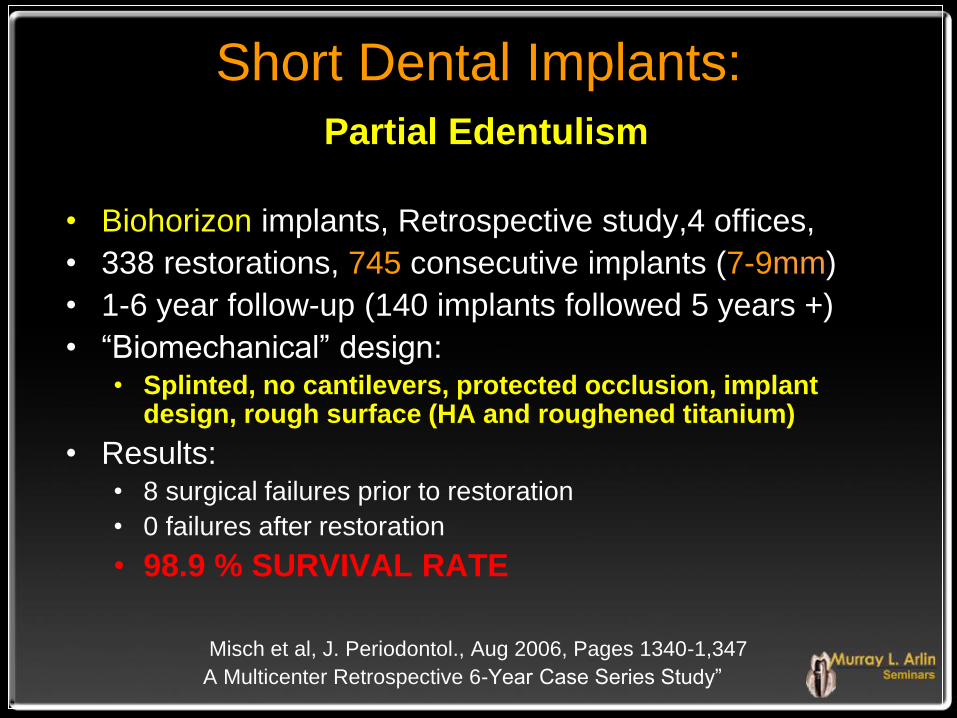
Short Dental Implants:
Partial Edentulism
• Biohorizon implants, Retrospective study,4 offices,
• 338 restorations, 745 consecutive implants (7-9mm)
• 1-6 year follow-up (140 implants followed 5 years +)
• “Biomechanical” design: • Splinted, no cantilevers, protected occlusion, implant
design, rough surface (HA and roughened titanium)
• Results: • 8 surgical failures prior to restoration
• 0 failures after restoration
• 98.9 % SURVIVAL RATE
Misch et al, J. Periodontol., Aug 2006, Pages 1340-1,347
A Multicenter Retrospective 6-Year Case Series Study”

Short (6mm) ITI Implants: Multicenter Trial of 1-7 Years
• 253 implants, 126 patients
• Maxilla: 86.7% survival rate (6 failures, N= 45)
• Mandible: 99.5% survival rate (1 failure, N=208)
• 91 solid screws (3 failures/maxilla)
• 94 hollow screws (4 failures )
• 68 hollow cylinders (0 failures)
• Ten Bruggenkate et al, Int J Oral Maxillofac Implants, 1998

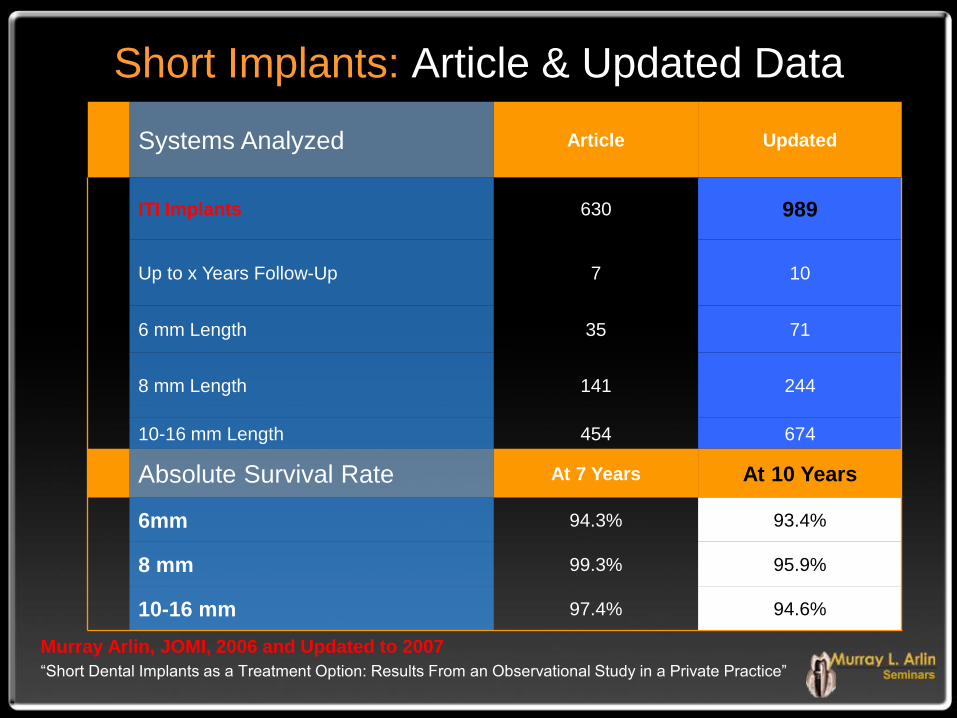
Short Implants: Article & Updated Data
Murray Arlin, JOMI, 2006 and Updated to 2007
“Short Dental Implants as a Treatment Option: Results From an Observational Study in a Private Practice”
Systems Analyzed Article Updated
ITI Implants 630 989
Up to x Years Follow-Up 7 10
6 mm Length 35 71
8 mm Length 141 244
10-16 mm Length 454 674
Absolute Survival Rate At 7 Years At 10 Years
6mm 94.3% 93.4%
8 mm 99.3% 95.9%
10-16 mm 97.4% 94.6%

POSTERIOR MAND RESTORED W/ 3 ITI
SHORT IMPLANTS

AT INSERTION

5 Years Restoration

5 Years Restoration

7 MM 7 MM
MINIMAL VOLUME

5 Years Restoration

Severely Resorbed Mandibles: Augmentation vs Short Implants
• “Major bone grafting of extremely resorbed
mandibles may not be justified”
• Compared to short implants, interposed iliac
crest grafts had greater:
• Surgical complications
• Prosthetic complications
• Pain and hospitalization
• Costs and time
• Cochrane Systematic Review,
Esposito et al, JOMI 2006

Short Implants: Guidelines • Can be predictable in good bone quality
• Avoid early transmucosal loading
• Avoid under-engineering (use 1:1 implant to
tooth)
• Avoid prosthetic overloading:
• Avoid cantilevers, balancing side contacts
• Provide protected occlusion, night guards
• Splint multiple implants together
• Check occlusion on an ongoing basis
Grafted Bone
High Success Rates
Similar to Native Bone
• van den Bergh et al, 1998, Raghoebar et al, 2001,
• Lorenzoni et al 2002, Simion et al 2002
• Zitzman et al, 2001, Cangini and Cornelini, 2002
• Buser et al, 2002, Radoni et al, 2005
• Fiorelini and Nevins, 2003, Fugazzotto, 2005

Grafted Bone: (Systematic Review-2003)
• 18 studies, 1,741 patients
• Most studies in private practice
• Survival rates similar to non grafted sites
• Insufficient data: re: membrane or graft type
• Further studies needed for:
• Distraction Osteogenesis, Ridge Splitting,
Ridge Expansion and Vertical Augmentation
• “Localized Ridge Augmentation/Preservation. A Systematic Review”
Annals of Periodontology, Dec 2003 Fiorellini and Nevins,
Grafted Bone
• Retrospective analysis: 607 implants
• All placed in regenerated bone:
• Dehiscence / Fenestration / Immediate extraction
• Augmentation: Buccolingual / Apico-occlusal
• 72 to 133 month follow-up
• Cumulative success:
• 97.2% maxilla
• 97.4% mandible
• Fugazzotto, JOMI, 2005
Grafted Bone
Higher failure in grafted bone: Poorer bone quantity &/or quality
Systemic factors e.g. osteoporosis
• Esposito et al, 1998, Albrektsson et al, 1986
• Blomqvist et al, 1998, Kapur et al, 1989
• Jenson et al, 1998, Lekholm et al, 1999
• Kan et al., 1999, Naert et al, 2002
• Wallace and Froum, 2003, Del Fabbro et al, 2004
• Tepper et al, 2006

Grafting / Area / Implant Length:
Meta-Analysis (Tepper et al)
• 22 prospective clinical trials
• 11,323 implants: 3,647 patients
• 83% of implants non grafted bone
• 5.3 years mean follow up
Results
Non Grafted Mand 98.7%
Non Grafted Ant MX 98.0%
Non Grafted Post MX 97.6%
Grafted Mandible 97.6%
Grafted Post Maxilla 93.8%
Grafted Ant Maxilla 91.0%
<8 mm Grafted Max 64.0%
Tepper et al, Meta-Analysis, COIR 2006

Meta-Analysis:
Grafting / Area / Implant Length
• Results- Non Grafted Bone: • Mandible-similar results
• Maxilla-more failures if <8mm
• Results-Grafted Bone: • Maxilla-more failures vs Mandible
• Maxilla-highest failures: <8mm implants
• Conclusion: Higher failure rate in grafted maxilla, especially if <8mm
• Tepper et al, Meta-Analysis, COIR 2006

Grafted Bone: (Systematic Review-2007)
• MAXILLARY SINUS (n=6,913)
87.7%-autogenous alone
94.88%-autogenous + combined
95.98%-non autogenous
85.64%-smooth implant surface
95.98%-rough implant surface
• ALVEOLAR RIDGE
95.5% Guided Bone Regeneration
90.4% Onlay Veneer Graft
94.7% Distraction Osteogenesis
83.8% Interpositional Inlay Graft
• Aghaloo and Moy, JOMI (Suppl), SSID, 2007
Grafted Bone: (Systematic Review-2007)
• “alveolar ridge augmentation procedures
may be more technique and operator-
experience-sensitive”
• “implant survival may be a function of
residual bone supporting the implant rather
than the grafted bone”
• Aghaloo and Moy, JOMI (Suppl), SSID, 2007

Grafting
fenestrations

3 mo later - bone
coverage

ANOTHER EXAMPLE

AT SECOND STAGE
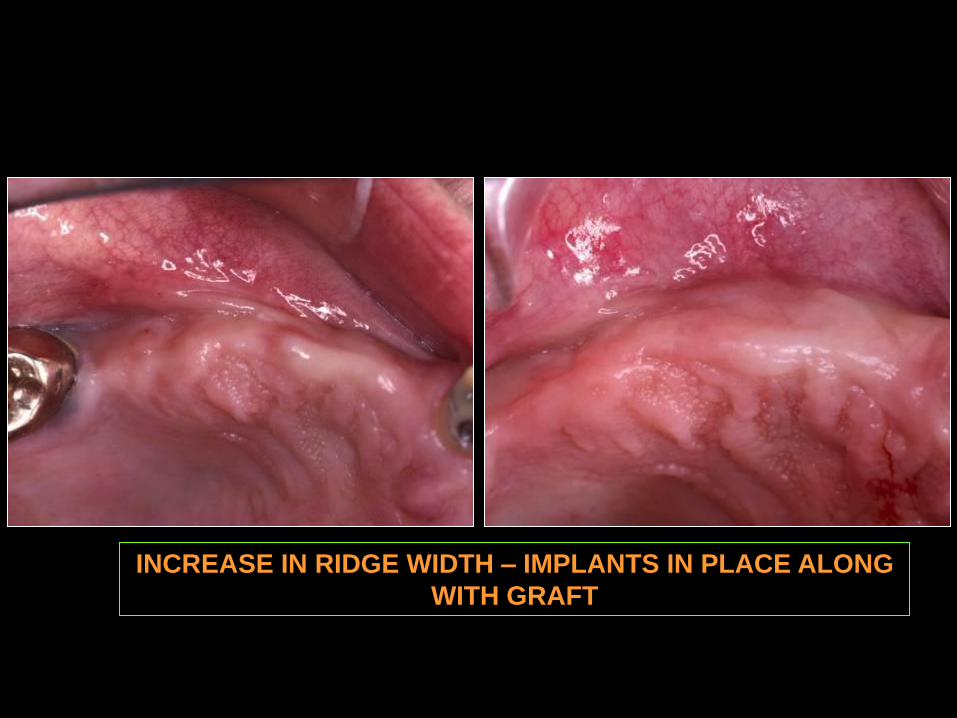
INCREASE IN RIDGE WIDTH – IMPLANTS IN PLACE ALONG
WITH GRAFT

RADIOGRAPH

COMPLETED BRIDGE

SINGLE

GRAFT with
GORE-TEX
MEMBRANE

RESTORATIVE RESULT

RADIOGRAPH

Surgical Protocol
8.7%
6.6%
5.8%
4.9%
3.7%
0
1
2
3
4
5
6
7
8
9
Cu
mu
lati
ve
Fa
ilu
re (
%)
Non-
Immediates-
Gore-Tex
All Protocols-
Gore-Tex
All
Immediates
All Protocols Immediates +
Gore-Tex
Surgical Protocol

Maxillary Sinus Augmentation:
A Systematic Review
• Articles searched up to April 2003
• Minimum of 1 year post loading
• 43 studies satisfied inclusion criteria
Annals of Periodontology
2003 Workshop on Contemporary Science in Clinical Periodontics,
Journal of Periodontology, V.8, #1,Dec. 2003, Pages 328-342,
Stephen Wallace & Stuart Froum

Lateral Window Sinus Elevation Literature Review on Survival Rates
Machined + Block 78.8%
Machined + Particulate 90.0%
Rough + Block 89.5%
Rough + Particulate 94.6%
All techniques 91.8%
Add Window Membrane + 7.3%
Annals of Periodontology Dec 2003, S. Wallace and S. Froum

Lateral Window Sinus Elevation: Literature Review Conclusions
Average survival rate 91.8%
Higher survival rate with:
• Rough surface implants
• Particulate vs block graft
• Membrane placed over window
Equivalent survival rate with:
• Type of membrane over the window
• Autogenous vs non autogenous
• Type of rough surface implant
Insufficient data with:
• Effects of smoking
• Residual crestal bone height
• Effect of healing duration
• Screw vs press fit design
• Use of PRP
Annals of Periodontology Dec 2003, S. Wallace and S. Froum

Grafted Bone: (Systematic Review-2007)
• MAXILLARY SINUS (n=6,913)
87.7%-autogenous alone
94.88%-autogenous +
combined
95.98%-non autogenous
85.64%-smooth implant surface
95.98%-rough implant surface
• ALVEOLAR RIDGE
95.5% Guided Bone Regeneration
90.4% Onlay Veneer Graft
94.7% Distraction Osteogenesis
83.8% Interpositional Inlay Graft
• Aghaloo and Moy, “Which Hard Tissue Augmentation Techniques Are the Most Successful
in Furnishing Bony Support for Implant Placement”, SSID, JOMI (Suppl) 2007

Sinus Grafts;
Efficacy of Graft Materials
• Bone substitutes may replace
autogenous bone for sinus lift
procedures!
• “The Efficacy of Various Bone Augmentation Procedures for Dental
Implants: A Cochrane Systematic Review of Randomized Clinical
Trials:, Esposito et al, JOMI 2006

BI AND 2 MOLARS REMOVED
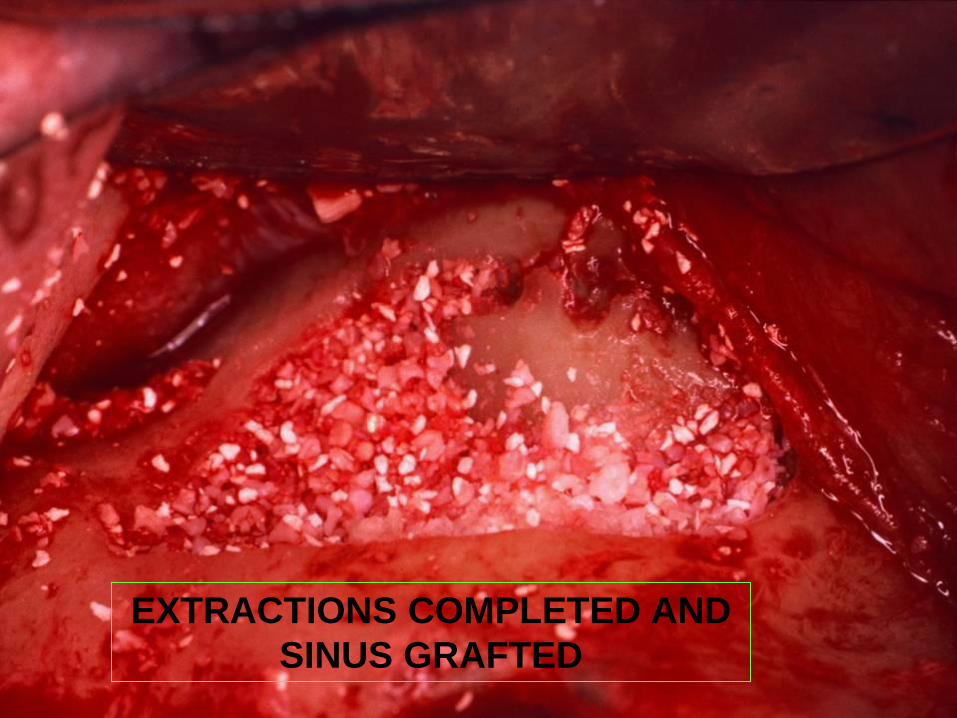
EXTRACTIONS COMPLETED AND
SINUS GRAFTED

IMPLANTS PLACED 5 TO 6
MONTHS

RADIOGRAPHIC RESULT

CLINICAL RESULT

INTERNAL
AUGMENTATION

Sinus Augmentation:
Internal / Osteotome
• Described by Summers in 1994
• over 95 % survival
• based on over 10 studies
• Average 3-4mm bone height gain
• With simultaneous implant placement, a
minimum of 4mm native bone suggested

TYPICAL CASE

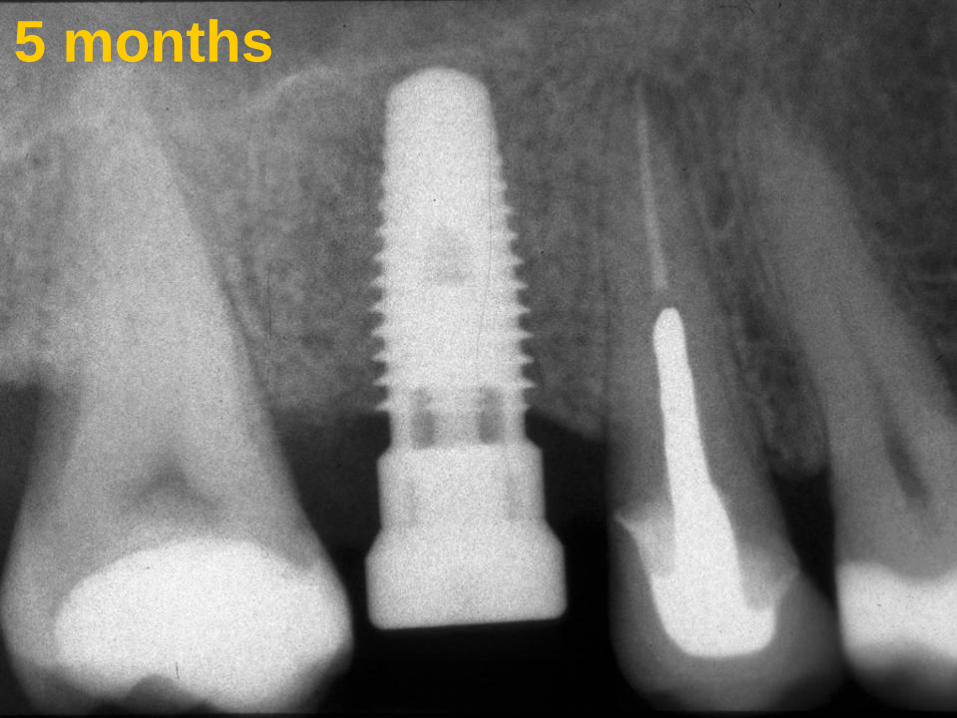
5 months
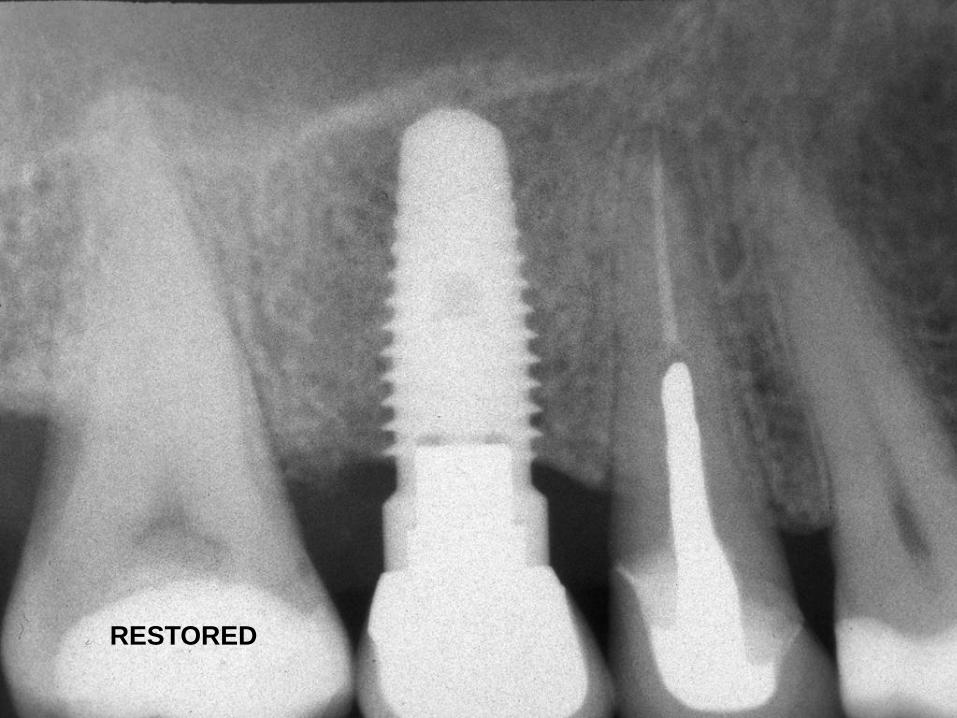
RESTORED
Osteotome Sinus Floor Elevation
Without Grafting Material
• 17 patients, 25 implants
• Mean residual bone = 5.4 mm
• Mean bone gain = 2.5mm
• 1/25 rotated at 35Ncm at 3 months
• 100% implants survived
• Nedir et al, Clin Oral Impl Res, 2006

Optimizing Success
in Low Density Bone
• Surgical technique
• Precise drilling
• Under-preparation
• Bone condensation
• Countersinking?
• Submerged ?
• Implant design
• Maximize length
• Maximize width
• Rough surface
• Threaded design?
• Tapered shape?
Osteotome Technique (Meta-Analysis)
• Medline search from 1953 to 2005
• From 165 articles only 5 met criteria
• Combined data of 349 implants
• 98% survival pre-restoration
• 99% survival after 56 months
• 12.1% considered “at risk”
• Shalabi et al, “A Meta-Analysis of Clinical Studies to Estimate
the 4.5-year Survival Rate of Implants Placed with the
Osteotome Technique”, JOMI, SSID (Suppl), 2007

Bone Quality/Quantity:
Implant Loss Radiation Therapy : 15 Studies
Implants # Placed # Lost % Lost
Maxilla 217 55 25%
Mandible 1,296 79 9%
• J. Prost. Dent., 2003, Goodacre et. al.
Surgical Complications:
Host Factors
• Systemic
• Age/health
• Previous periodontitis
• Smoking
• Genetics/Immunity
• Local
• Bone quality/quantity
• Excessive loading
• Poor plaque control
• Keratinized gingiva

Excessive Loading:
“Early” Complications
Macromovement induces fibrous tissue in:
• Orthopedic implants • Unthoff and Germain, 1973, Soballe et al., 1992
• Dental implants • Cameron et al., 1973, Schatzer et al., 1975
• Brunski et al., 1979, Akagawa et al., 1986

Excessive Loading:
“Early” Complications
• Osseointegration consistant if micromotion is
within a threshold limit of 50 um (possibly more)
• Osseointegration will not occur if early implant
micromotion exceeds 150 um (possibly less)
• Cameron et al., 1973, Pilliar et al., 1986 & 1995
• Maniatopoulos et al., 1986, Szmukler et al., 1998

Excessive Loading:
“Early” Complications
• Early and immediate loading can be successful with
limited micromotion and may actually increase the
quantity of bone in direct contact with implant surface
• Piatelli et al., 1993, 1997, 1998
• Salama et al., 1995, Chiapasco et al., 1997. 2001
• Tarnow et al., 1997, Schnitman et al.,1997
• Gatti et al., 2000, Romanos et al., 2001
• Rocci et al, 2002, Testori et al 2002

Excessive Loading:
“Late” Complications
• Etiological role controversial
• Difficult to study clinically
• Failure with experimental overload • Isidor F., 1996, Rangert et al., 1995
• Increased failures in poor quality bone • Many reports but indirect evidence
• Crestal bone loss and or failure? • Quirynen et al, 1992, Siegele & Soltesz JOMI 1989
• Borchers & Reichart 1983, Ekfeldt et al.,2001
• Rieger et al.,1989, Pilliar et al.,1991
• Kozlovsky et al (poster) COIR, 2006

TWO IMPLANTS SUPPORTING
4 UNITS IN MAXILLARY BONE!

10 Years Post Restoration
CRESTAL BONE LOSS

2006 EAO Consensus Conference:
“Influence of Forces on Peri-implant Bone”
• Results are conflicting
• Animal studies indicate occlusal load may
cause marginal bone loss and loss of
integration
• Clinical studies have stated, but have not
shown a causative relationship
Excessive Loading:
“Late” Complications
• Mechanical Complications • Screw loosening
• Screw fracture
• Prosthesis fracture
• Implant fracture
• Schwartz, M.S., 2000, Clin Oral Implant Res (Supp)
Surgical Complications:
Host Factors
• Systemic
• Age/health
• Previous periodontitis
• Smoking
• Genetics/Immunity
• Local
• Bone quality/quantity
• Excessive loading
• Poor plaque
control
• Keratinized gingiva

Role of Plaque:
Implant Complications
• Etiological role needs more study
• Cross contamination in partially edentulous?
• Early or late: complications? / failures?
• Gouvoussis et al., 1997

Partially Submerged Implants
• 206 implants
• Buried, partially exposed or fully exposed.
• Prematurely partially exposed, were
associated with greater bone loss
• Conclusion: “..fully expose ASAP”
•Tal, H., J. Periodontol 1999
•Tal et al., JOMI 2001
•Haim and Zvi, JOMI 2001
•Tal et al Implant Dent, 2002

Role of Plaque:
Implant Complications
• Pathogens associated with signs of “peri-implantitis” • Many association studies
• Listgarten and Lai, J Periodontol, 1999
• Susceptibility with Periodontitis • Ellegaard et al, Clin Oral Impl Res, 1997
• Brocard et al, JOMI, 2000, Hardt et al, COIR, 2002
• Karoussis et al, Clin Oral Impl Res, 2003 and 2004
• Rosenberg et al, JOMI, 2004
• Baelum and Ellegaard, J Periodontol, 2004
• Mengel and Flores-de-Jacoby, J Periodontol, 2005
• Paknejad, A., COIR 2006
• Correlation with increased biological complications • Zabaras et al, (Abst), COIR, 2006

Fixed Implant Reconstructions:
Biological and Prosthetic Complications
• Peri-implantitis:
• 1.81% good oral hygiene (n=55)
• 5.72% moderate oral hygiene (n=174)
• 13.44% poor oral hygiene (n=409)
• Marginal Bone Loss:
• 0.18mm with good oral hygiene
• 1.62mm with periimplantitis
• Other Risks: Bruxism / heavy smoking
• Zabaras et al, Abstract Clin Oral Impl Res, Aug. 2006

Role of Plaque:
Early or Late: Complications? / Failures?
• Limited # of studies correlating poor oral hygiene and
increased plaque, with increased biological complications
• “Clinical experience” correlates “early” & “late” increased
peri-implantitis, crestal bone loss & implant failure • Unpublished, Dr. Murray Arlin, Private Practice

Surgical Complications:
Host Factors
• Systemic
• Age/health
• Previous periodontitis
• Smoking
• Genetics/Immunity
• Local
• Bone quality/quantity
• Excessive loading
• Poor plaque control
• Keratinized
gingiva


Previous bridge illustrating healthy bone
without keratinized gingiva
Role of Keratinized Gingiva
• No correlation with implant failures • Esposito et al 1998, Cochran, Ann Perio 1996
• Plaque removal may be facilitated with
presence of keratinized gingiva
• Esposito et al, 1998, AAP 1996

Summary: Host Local Factors:
Bone Quality and Quantity:
• Higher failure rates with very poor quality and quantity bone • Short implants with rough surfaces may show relatively high
survival rates in good quality bone (e.g. in the mandible)
• Slightly higher failure rates with very dense quality
• Possibly higher failure rates with grafted bone
• Higher failure rates in grafted maxilla with short implants
• Success rate greater than 90% with sinus grafts
• Improved success rates with rough surfaced implants, particulate graft, and membrane covering lateral window
• Higher failure rates with irradiated maxillary bone

Summary: Host Local Factors:
Excessive Loading:
• Early Loading
• Macromovement induces fibrous encapsulation
• Osseointegration possible with limited micromovement
• Micromovement range is between <50 to < 150 microns
• Controlled loading may increase % of bone contact
• Late Loading
• Role in complications and failure needs further study

Summary: Host Local Factors:
Plaque/Keratinized Gingiva
• Poor plaque control:
• Etiological role needs additional study
• Some studies: increased complications
• Potentially more with “very” rough surfaces
• Empirically, causes biological complications
• Keratinized gingiva:
• Etiological role needs additional study
• No correlation with failure of “turned” titanium
• Possible risk factor with “very” rough surfaces
• Plaque removal and esthetics may be enhanced

Surgical Complications
Host
Factors
Systemic
Factors
Local
Factors
Contributing
Etiology Non Host
Factors
Operator
Related
Biomaterial
Related
(Based on Etiology)
PART 3 TO
FOLLOW


















