1.sulfonamide final
46
SULFONAMIDES
-
Upload
vijay-prasad-sanghishetti -
Category
Technology
-
view
1.173 -
download
0
description
Transcript of 1.sulfonamide final

SULFONAMIDES

chemotherapy
A science of treating diseases with the help of drugs.
The term gradually came in to use in reference to treatment of infections, infestations, and cancers.

• Treatment of systemic/topical infection with
drugs that have selective toxicity for an invading
pathogens with out harming the host cells.
• Due to analogy between the pathogenic organism
and malignant cells the treatment of neoplastic
diseases with drugs is also called as Chemotherapy
»Contd.,

landmarks• 1877 – Louis Pasteur – “LIFE DESTROYS LIFE”-
Bacteria prevented growth of anthrax bacillus in urine
• 1891 – Paul Erlich (FATHER OF MODERN CHEMOTHERAPY- NOBEL 1909) - methylene blue inhibited growth of bacteria
• 1928 – Alexander Fleming: The fungus penicillium notatum could inhibit staphylococci in a culture plate
• 1938 – Domagk – Prontosil – a dye inhibited micro-organisms – sulfonamides- sulfanilamide
• 1941 – Penicillin – Fleming, Florey, Chain- Nobel

organisms• Bacteria• Fungi• Viruses• Spirochetes (Treponemes, Borrelia )• Actinomyces• Rickettsiae• Chlamydiae• Mycoplasma• Nocardia• Protozoa/parasites(ameba,giardia,trichomonas, toxoplasma)
worms (Helminths)• Prions

• Obtain MO (Antibiotics)
• Antimicorbials Syn in Lab,
• Semisenthetic antibiotics
»Contd.,

Mechanism of Action
• Antibiotic action can be split into 2 mechanisms:
Bacteriostatic
Bacteriocidal

STATIC - implications
• NO KILLING EFFECT – long period of treatment• Infection MAY NOT BE totally eradicated• ORGANISMS MAY REMAIN IN A DORMANT STAGE• MAY MULTIPLY LATER• RELAPSE• E.g. chloramphenicol for enteric fever
• COMBINATION – static drug may reduce the rate of growth – a cidal agent cannot work effectively.

CIDAL - IMPLICATIONS• KILLING EFFECT• Infection totally eradicated• Less chances of relapse• Example : ENTERIC FEVER (TYPHOID)• Chloramphenicol (static)• Cotrimoxazole, Ampi/amoxicillin, Ciprofloxacin, Ceftriaxone
(cidal)
• CIDAL drugs produce rapid effect – shortening of length of treatment – tuberculosis (streptomycin, INH, rifampicin, pyrazinamide)
010613 mmm

• Bacteriostatic Drugs arrest the growth and replication of bacteria and limits the spread of infection
• Bacteriostatic antibiotics hamper the growth of bacteria by interfering with bacterial:
Protein productionDNA replicationCellular metabolism
• Macrolids ,Broad spectrum antibiotics ,Sulfanamides• Trimethroprim, Clindamycin, Ethambutol

• Bacteriocidal kill or irrverisible damage the multiplying bacteria
• Microbe death is usually achieved by disruption of the bacterial cell membrane leading to lysis.
• Betalactum antibiotics• Cotrimoxazole, Aminoglycoside• Fluroquinolones, Vancomycin, Polymixins• Rifampicin, INH, Bacitracin

Spectrum of activity
• Spectrum = range of micro-organisms inhibited
• Narrow spectrum• Penicillin G (Benzyl penicillin) Mainly Gm +ve• Aminoglycosides, Metronidazole – Mainly Gm
–ve• Broad Spectrum Antibiotics: (BSA)• TETRACYCLINES, CHLORAMPHENICOL

Extended spectrum
• Broader than NARROW SPECTRUM• Narrower than BROAD SPECTRUM
• Extended spectrum penicillins• II and III generation cephalosporins• Co-trimoxazole• Sulfa drugs, trimethoprim• Quinolones• Macrolides

Mech
• Usually it take advantage of the biochemical
and physiological differences that exist betn
MO and human beings.

PROKARYOTIC EUKARYOTICSize 1-10µm 10-100m
Envelope by rigid cell wall Flexible plasma membrane
Sub cellular organs absent present
Ill- defined nucleus Well defined nucleus
Energy metabolism bounded to cell membrane
Located in mitochondria
Division -- fission mitosis
Ribosomes-70s– 30s & 50s 80s– 60s & 40s

Site and Mechanism of action of Antibiotics

Combination therapy
• To make broaden spectrum activity (Pulmonary, Aerobic, anaerobic)
• Increase antibacterial activity (Synergism)• To prevent resistance (TB, leprosy)• To reduce duration of therapy (MDT, leprosy)• Reduce adverse effects

Resistance
1. As result of mutation or by plasmid mediated1. Conjugation2. Transduction 3. Transformation
2. Producing an enzyme that inactivate antibiotic4. Betalactmase5. Chloramphenicol acetyltransferase 6. Acetyl transferase, phosphotrans, adenyltransferase (aminoglycosides)
3. Decreased bacterial permeability or active efflux of drug.4. An appearance of alternative pathway5. Decreased affinity for target : Penicillin binding proteins

Prevention of drug resistance
• Right drug• Right dose• Right period• Prefer rapidly acting selective spectrum• Combination of AMAs whenever prolong
therapy

Factors affecting choice of antimicrobial agents
Age: – Chloramphenicol – Gray baby syndrome– Half life amino glycosides is prolonged in elderly– Tetracyclines – CI in below 6 years it accumulates in developing bone
and teeth
Pregnancy:– All antibiotics produce risk to the fetus . Penicillins, Macrolids &
Cephalosproins
Impaired host defenses– Bactericidal drugs are must in immunocompromised patients

• Renal function:
• Liver function
CI in renal disease Dose reduction in renal failure
cephalothin Aminoglycosides
Cephaloridine Amphotericin B
Nalidixic acid Vancomycin
Nitrofurantoin Ethambutol
CI in liver disease Dose reduction in liver failure
Tetracycline Chloramphenicol
Pyrazinamide Isoniazid
Pefloxacin Rifampicin
Erythromycin Clindamycin

SULFONAMIDES
•Sulfonamide were the first antimicrobial agents effective against
pyogenic bacterial infections
•Anti metabolites
•Bacteriostatic agents
•GELMO 1908 – Synthesized
•Prontosil was first drug active in vivo
•In liver it converting to Sulfonamide
•These are synthetic agents(Antimicrobials)
•Originally, sulfonamides were synthesized in Germany as azodyes.

Gerhard Domagk (1895-1964)
German bacteriologist and pathologist who was awarded the 1939 Nobel Prize for Physiology or Medicine for his discovery (announced in 1932) of the antibacterial effects of Prontosil, the first of the sulfonamide drugs.

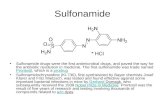
The process of discovery for sulfonamides
H2N
NH2
NN
SO2NH2
ProntosilProntosil Soluble
NaO3S SO3Na
CH3CONH N N
SO2NH2
NH2
H2N
NN
SO2NH2
[H]H2N
SO2NH2
Liver
inactive (in vitro) active(in vivo)

SULFONAMIDES• The antimicrobial containing a sulfonamido (sulfanilamide, SO4NH2)
group are called sulfonamides. H2N SO4-NH2
• Structurally related to p-aminobenzoic acid (PABA).SINCE THEN :
* 5000 SYNTHESISED. * 150 MARKETED.* 20 IN COMMON USE.
• This group is also present in other non-antibacterial compounds like -Sulphonureas -Benzothiazids -Furosemide -Acetazolamide

Mechanism of action
• Folic acid - synthesized from PABA, pteridine and glutamate.
• All sulfonamides are analogs of PABA.
• SA compete with this substrate for the bacterial
enzyme, dihydropteroate synthetase.
• All sulfa drugs are bacteriostatic.

Folic acid synthesis inhibitors
pterdine + para-amino benzoic acid
dihydropterate
dihydrofolate
tetrahydrofolate (folinic acid)
DNA/RNA
Trimethoprim
(Diaminopyrimidines)
Binding
Sulphamethoxazole
(Sulphonamides)
Structural analogues of PABA
Dihydropteroate synthetase
Dihydrofolate reductase


Antimicrobial effects
Both G+ & G- bacteria, nocardia, chlamydia trachomatis, some protozoa, some enteric bacteria (E coli, klebsiella, salmonella, shigella, & enterobacter)
Sulfonamides stimulate rickettsiae in their growth.

CLASSIFICATION
Orally absorbable agents• Short acting(6-9hrs.)- Sulfadiazine
SulfacytineSulfamethizole
Sulfisoxazole
• Intermidiate acting(10-12hrs.)- Sulfamethaxazole Sulfamoxole
• Long acting(7days)- Sulfadoxine sulfamethopyrazine
Orally non absorbable agentsSulfasalazineOlsalazine
Topical agents Silver sulfadiazine Sulfacetamide Mafenide

Pharmacokinetics• Absorbed rapidly from the gastrointestinal tract (except topically
used ).
Peak plasma levels are achieved in 2-6hrs.
• widely distributed and pass through BBB as well as placental barrier.
• Never administered SC & IM (Very painful)
• Metabolized as acetylated conjugates in liver. Acetylated metabolites are inactive and low soluble in acidic urine,
leads to ppt. of crystaluria and renal toxicity.
• Excreted through the glomerular filtration in urine.

COTRIMOXAZOLE
COMBINATION OF : Fixed dose combinationSULPHAMETHAXAZOLE : TRIMETHOPRIM.
5 : 1 400 mg. 800mg : 80 mg. 160mg
M. A. O. PABA F.A. SYNT. FOLIC ACID D. H. F. R. THFA
- SEQUENTIAL BLOCK. - Broad spectrum bactericidal combination. - Delays the development of bacterial resistance
SULPHA TRIMETHOPRIM

Clinical useOral sulfonamides• Cotrimoxazole UTIs –Actue uncomplicated • E.coli, Proteus• 5 -10 days cotrimaxozole DS BD
Prostatis- • concentrated in prostatic fluid• Acute prostatis – DS tablet BD- 3weeks• Chronic – 6-12 week

Respiratory tract infections- DS tablet BD• Frequent choice for acute sinusitis, bronchitis,
otitis media due to Pneumococcus and Haemophilus
Thyphoid- (Ciprofloxacin DOC)
• Alternative drug • DS tablet BD- 2week• 10-12 week course eradicate carrier state
Salmonella typhi

Bacterial diarrhoea and Dysentery (Ds tablet Bd 7 days)Gastroenteritis - Shigella & Yersinia entrocoliticaTraveler's diarrhoea - E.coliCholera - Vibrio cholerae
Nocardiosis (Sulfadiazine)Pulmonary lesions or Brain abscess -DOC

STD DS tablet BD for 7-10days– Chancoroid- Haemophilus ducreyi(Chancoroiod – highly infectious nonsyphilitic venereal ulcer)– Lymphomagranuloma – Chalamydia – Gonorrhoea- Neisseria gonorrhoea
Pneumonia• Prophylactic DS tablet OD • Curative – DS 4 times a day for 2-3 week
Sulfadiazine + Pyrimethamine • 1st line Acute Toxoplasmosis• Folinic acid 10mg each day to minimize bone marrow
suppression

• IV cotrimoxazole - 80mg Trimetho + 500mg Sulfamethoxazole in 5ml diluted in 125ml of 5% dextrose infusion over period 60-90min
• Preferred for moderate to severe– Pneumocytis carinii-pneumonia– Shigellosus– Thyoid fever– Nocardiosis– Gram –ve bacterial sepsis

Sulfadoxine + Pyrimethamine combination
• Sequential block in protozoal folic acid synthesis
• Clinical curative for choloro qunine resistance P.
Falciparum (1500mg sulfadoxine+ 75mg Pyri)
sulfadoxine 500mg + Pyrimethamine 25mg (1:20)
• Pyrimethamine + sulfadoxine in toxoplasmosis

Oral non absorbable
• Sulfaslazine Poorly absorbed by GIT
Bacterial flora5 Aminosalicyclic acid + sulfapyridine
Anti inflammatory activityUlcerative colitis
Anti bacterial agentCarrier moiety for 5AMA to reach bowelRheumatoid arthritis

Topical agents
Sodium sulfacetamide- 10%, 20%, 30%• Ophthalmic solution or ointment – conjunctivitis
Mafenide acetate Prevent bacterial colonization and infection of
burn wounds,Silver sulfadiazine For prevention of infection of burn wounds

Adverse effects
Crystalluria and renal toxicity- Adequate intake of water By making urine alkaline
Blood Hemolytic and aplastic anemia (G6PD def.)
Thrombocytopenia
Hypersensitivity Photosensitivity Exfoliative dermatitis
Eosinophelia

• Kernicterus in neonates-– Sulfonamides displace bilirubin from protein binding – Free bilirubin gets diposited in basal anglia,
subthalamic nuclei - toxic encephalopathy – Avoided in neonates & pregnancy (last trimi)
• GI - Nausea, vomiting, diarrhea, pancreatitis

• R- Rash• A- Acetylation• S- Systemic lupus erythromatus • H- Heamolysis in G6PD • A- Aplastic, Megaloblastic anemia• B- Bilirubin displace • C- Crystalluria

Resistance to Sulfonamides
①Over-production of PABA②Produce dihydropteroate synthase with
low sulfonamide affinity③Loss permeability to the sulfonamide ④Use exogenous sources of folate;

CONTRAINDICATIONS
• Pregnancy (full term)• Newborn and infant (<2months)• Patients on Methenamine, Tolbutamide, oral
anticoagulants.

THANK Q