1954 Congenital Tracheo-esophageal Fistula Without Atresia of the Esophagus by George Wiwarsi War.e,

of 7
Transcript of 1954 Congenital Tracheo-esophageal Fistula Without Atresia of the Esophagus by George Wiwarsi War.e,
-
8/8/2019 1954 Congenital Tracheo-esophageal Fistula Without Atresia of the Esophagus by George Wiwarsi War.e,
1/7
1954;14;254-258PediatricsGEORGE WILLIAM WARE and LOUIS L. CROSS
THE ESOPHAGUSCONGENITAL TRACHEO-ESOPHAGEAL FISTULA WITHOUT ATRESIA OF
http://www.pediatrics.orgthe World Wide Web at:
The online version of this article, along with updated information and services, is located on
Online ISSN: 1098-4275.Copyright 1954 by the American Academy of Pediatrics. All rights reserved. Print ISSN: 0031-4005.
American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007.has been published continuously since 1948. PEDIATRICS is owned, published, and trademarked by thePEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly publication, it
. Provided by Viet Nam:AAP Sponsored on November 19, 2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/ -
8/8/2019 1954 Congenital Tracheo-esophageal Fistula Without Atresia of the Esophagus by George Wiwarsi War.e,
2/7
CONGEN ITAL TRACHEO -ESO PHAGEAL F ISTULA W ITHOUTATRES IA O F THE ESOPHAGUS
B y GEORGE W iwA rsi W AR .E , M .D ., AN D L ou is L . C no ss, M .D .W a sh in g to n , D .C .
25 4
TRACHEO -ESOPHAGEAL F Isi-u i. AC ONGEN I TA L tracheo-esoph ag eal fistu law itho u t atres ia o f the eso phag us is a
ra re an om a ly . In d is cu ssing th is su b ject,G ross s tate s : W e h av e encoun te red fou ro f th ese ab norm a litie s du rin g th e tim e tha tw e have seen 25 9 bab ie s w ith esoph ag ea la tre sia . H a ig h t, w ith ex pe rience in 6 3 caseso f e sop hageal a tres ia, trea ted tw o cases o ftracheo-e sop hageal fis tu la w ith ou t a tre sia .A t the C h ild ren s H osp ital in C h icag o , o n lyone case w as seen , w h ile 43 cases o f a tre siao f the eso phagu s w ith tracheo-e soph agealf is tu la w ere trea ted .h l W e have rev iew edth e E ng lish lite ratu re an d fo und 26 caseso f th is en tity . To th is g roup , w e w ish to addan o the r case w hich w as treated su ccessfu llyb y su rge ry .
W e have co nside red adu lts rep o rted w ithth e an om a ly as p ossib le case s.2 5 , 26, 2 7 Pa -tien ts desc ribed b y G engenb ach ( C ase 7)and S toeck le in a re a lso p laced in th is pos -s ib le ca tegory . A spon taneous cu re o f acong en ita l trach eo -e so phagea l f is tu la hasb een repo rted , bu t has b een co nsid ereddoub tfu l by us .31 N o poss ib le o r d oub tfu lcase w as used in com piling the s ta tis tic s .
CA SE R EPO RT
F . P . A w hite m a le , w as born a t P ro v iden ceH osp ital on Ju ly 20 , 19 53 . H is b ir th w e igh tw as eig h t p ounds, 1 2 ounces . H e w as the firs tliv ing ch ild o f fou r p regn an cie s . N o th in g ab -norm a l w as no ted a t b ir th .
T he firs t feed in g w as a ttend ed by cough ingan d vom iting . T he n urse la te r reco rded ab-dom ina l d isten tion , dy spn ea w ith ra spy resp ira -tions. The re w as no cyano sis .
O n th e second d ay o f life a d iagno sis o fa te lecta sis o f the le f t low er lobe w as m ade . T heabdom en w as d istend ed , bu t such d isten tion re-
F rom the D ep artm en ts o f T ho rac ic S urg ery andPed ia tric s, P rov ince H osp ital, W ash ing ton , D .C .
spon ded to asp ira tion o f stom ach . P assag e ofL ev ine tub e w as co nside red to ru le ou t th ed iag nosis o f e soph ageal a tres ia w ith trach eo-e sop hagea l f is tu la . P a tien t passed a m econ iumstoo l. T he fo llow ing day , a chest film show edno pu lm on ary p ath o log y bu t tho rac ic h em ive r-teb rae w ere no ted . A n abdom ina l film sh ow edco nsid erab le gas in the stom ach . Th is sam eeven ing , fo llow ing feed ing , rhon ch i w ere n o tedin the chest w ith d im in ished brea th sounds ov erthe rig h t lu ng . Th ere w as d ysp nea and ab -dom ina l d isten tio n . P atien t w as p laced in o xy-g en . F or th e n ex t seve ra l days p atien ts con d i-tio n w as p oor. C ough an d vom iting usua l lyo ccu rred w ith feed ings .
R ad io log ic stud ies o f Ju ly 28 th rev ealedp neum onic conso lida tion occupy ing the rig h tu ppe r lob e w ith heavy congestive chan ges inth e rem a ind er o f the rig h t lung and le f t u pp erlo be . A barium en em a w as nega tive .
A lip iod o l s tudy ru led ou t ca rd iosp asm orh ia ta l he rn ia . A defin ite sea rch w as m ade of atracheo-esoph ag ea l fistu la . D uring exam ina tio nlip io do l w as seen in the trachea , bu t w asth oug h t to b e asp ira ted .#{1 76 }
The pa tien t w as p laced on an tib io tic s andp am en tera l f lu ids . A s h is co nd itio n im proved ,v a riou s fo rm ulae w ere tried w ith va ry ing sue -cess. T he pa tien t w ou ld have no d ifficu lty oned ay , on ly to v om it the m ajo rity o f feed in gs onthe nex t day .
D uring th e firs t w eek of A ugu st an o the rlip io do l sw a llow w as p erfo rm ed . A t th is ex am i-na tion , a qu estio nab le fis tu la w as seen b etw eenthe trachea and esoph agus. Th e pos sib ility o fa sp iratio n cou ld no t be ru led ou t.
F o r the nex t seve ral w eeks g as tric g av ag ew as perfo rm ed . T here w as som e w eigh t ga in .How ever , th e in fan t w as foun d cy ano tic andsevere ly dyspne ic in h is c rib on severa l occa-sions fo llow in g feed in g . F o llow ing one o f th eseep isod es pn eum on ia o f the righ t upp er lo bed ev e loped . T he in fan t w as critic ally ill du ringth is ep iso de .
#{176}R aym ond I. T erra franca , M .D . p erfo rm ed a llco n trast stud ies .
. Provided by Viet Nam:AAP Sponsored on November 19, 2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/ -
8/8/2019 1954 Congenital Tracheo-esophageal Fistula Without Atresia of the Esophagus by George Wiwarsi War.e,
3/7
TRACHEO- ESOPHAGEAL F I S TULA WI THOUT ATRES I A 25 5On September 4, a contrast study w ith
lipiodo l w as repeated and a de finite diagnosiso f t ra ch e o- e so pha g ea l f istula made.
Patient w ent to surgery on the fo llow ing day ,ag e six w eeks, w eight seven pounds and tw oounces. Dr. John Leahy gav e the anesthesia. Arig ht thoraco tomy w as performed under endo -tracheal anesthes ia. The pleural cav ity w asentered through the fo urth intercostal space .
The esophagus w as identif ied and dissec tedcephalad from the lev e l o f the carina. Af is tula w as fo und be low the subc lav ian v e inat the leve l o f the third rib po steriorly . Theesophageal portion w as s lightly low er thanhetracheal opening . The tracheal opening wasc lo sed w ith five interrupted s ilk sutures (5 -0 ).The esophagus w as c losed in tw o lay ers. Themucosa w as c lo sed w ith tw o sutures and thenfour sutures in the musculature. A ro utine chestclo sure was performed.
A t the end of the procedure cerv ical em -physema w as no ted. Ten cc . o f air w as as-pirated w ith nearly complete disappearance o fthe emphy sema. This occurrence w as attributedto the high lev e l o f dissec tion.
On the first post-operative day , there wasate lec tasis o f the right upper and m iddle lobesw hich cleared by coughing and tracheal aspira-t iOIl. There w ere audible rhonchi over bo thlung fie lds w ith normal breath sounds and clearx -ray fo r several day s.
W ater by mouth w as started on the thirdpos t-operative day and formula on the fourth.Improvement w as progressive . Patient w as dis -charged at 10 w eeks of ag e, w e ighing e ightpounds and tw o ounces.
Etio lo gy o f Tra cheo-Esop ha gea l Fis-tula .6 , 15 , 16 , 3 0 There are three theoriespropounded to explain the occurrence oftracheo -esophageal fistula. Ke ith and Spicermaintain that there is an incomplete unionof the lateral tracheo-esophag eal groov es.Such g rooves in the embryo normally forma septum w hich separates the trachea andesophagus.
Pressure ex erted by the anlage of theheart o r by an abnormal vascular system hasalso been propo sed as a cause. A n abnormalblo od vesse l has been recorded in threecases o f proved esophageal f istula6 andin one possible case of congenital f istula.2
The final theory states cellular pro lifera-tion from the embryonic esophagus is de-fic ient; hence , a comple te separation o ftrachea and esophagus do es no t o ccur.
Signs a nd Sympto ms of Tracheo-Esopha-gea l Fistula .6 1O I i , 1 2 These figures arecompiled from 2 7 patients, 11 o f w hom w ereno ted to be males, and nine stated to befemales. (Sex not stated for 7 .) The lesionis more diff icult to diagnose than is atres iaof the esophagus, since symptom s may beunre lated to sw allow ing and there may beasymptomatic periods.
He lmsw orth has po inted out an exce llentdiagno stic triad.1. P aroxysms o f C o ughing w ith Feed ings.Liquids cause the most diff iculty . Suchcoughing is o ften attended by cyanosis . Thedirec tion of the fistula w ill play a part inthis particular instance. If the low er open-ing of the fistula is esophageal, sw allow ingmay be unattended by difficulty . Regurg i-tation of food, how ever, precipitates thetrouble. Hence , coughing and cyano sis mayoccur only after feeding .
Characteristically , symptom s disappearw hen the infant is fed by gavag e. In re -po rted cases the long periods o f g avag e havebeen interes ting . Some infants have beenfed as long as a year by this method.2. Abno rma l D rstentio n of the Abd omen.This is due to div ersion of tracheal air intothe esophagus, which is then sw allow ed intothe s tomach. Rapid direc t inflation of thestomach during coughing is pathognomico f a fistula betw een the tracheo-bronchialtree and upper alim entary t ra c t .h l
In s ix out of nineteen cases w here a com-ple te pro toco l is available , abdominal dis -tention w as a prom inent feature . In our casedistention w as such that intestinal obs truc-lion due to a congenital abnormality w asconsidered. In this patient it w as no ted thata catheter placed into the stomach re lievedthe distention, w hile a rec tal tube did no t.3. P ersistent P neumo nitL Pulmonary pa-tho logy is alw ays present regardle s s o fh eseverity o f g astro-intestinal symptom s. Thepulmonary problem may be the main rea-
. Provided by Viet Nam:AAP Sponsored on November 19, 2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/ -
8/8/2019 1954 Congenital Tracheo-esophageal Fistula Without Atresia of the Esophagus by George Wiwarsi War.e,
4/7
S
11111111111
Ferguson
FlussHa i g h tHelmsworthHo l i n g e rI mp e r a t o r iKnoxLeigh
R o b bAu t h o r sAv e r a g e
256 GEORGE WILLIAM WARE AND LOUIS L. CROSSson for seeking medical adv ice . The rightupper lobe is most frequently invo lved.Coarse rhonchi, w hich may be bilateral, areusually present. Chronic cough comple testhe respiratory picture .
General symptom s inc lude poor w eightgain, dehydration, and apathy .
R adiologic A spects.10 21 Pneumonitis w illbe v isible on routine chest f ilm and, as men-tioned, usually invo lv es the right upperlobe.
Lipiodo l is the usual medium for con-trast studies o f the esophagus . The examina-tion should be done in the prone or anterioroblique position so that the o il w ill f lowanteriorly to the trachea. Careful observa-tion is necessary during fluoroscopy .
If the s tudies w ith iodized o il are no tsucces sful, Le igh and his assoc iates recom-mend a tracheogram . The lipiodo l is in-jec ted by laryngo scopic guidance . Films areimmediately taken in the anterior-posterior,posterio -anterior, and bo th lateral pro jec -lions. Such studies may succeed since thetracheal opening is le ss liable to co llapseand clo se the fistula.
I n t h is ser ie s, con t r a s t s t u d ie s h a ve b eendone on 18 patients . In 11 the fistula w asseen on at least one exam ination.
It should be emphasized that one ex -am ination w ith contras t medium is no t
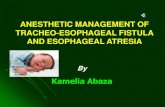
CHART IASSOCIATED ANOMALIES IN CONGEN ITA L TRACHEO-
ESOPHAGEA L FIsTu
Aberrant A rteryP h a r y n gea l D ive r t ic u lu mP a t en t D u ct u s A r te r io su sAnomalous Ribs and/or V ertebraeInterventricular Septal D efectJ e j u n a l D ive r t ic u lu mOrigin of RUL from TracheaM eck el s D iver t icu lu mE sop h a gea l S te n os isMongo l i smCongenital H eart D iseaseLeft-S ided Fused Kidney sMairotation of CecumGastric A berrant PancreasD ouble Tracheo -Esophageal Fis tula
enough. Failure to demonstrate the tract oneven repeated exam inations does not e lim i-nate the diagnos is .
Endoscopy. Such a surg ical maneuvermay prove a valuable aid. Esophag oscopyis usually performed first. If the fistula isseen , bronchosco py w ith the poss ibility o flaryngeal edema w ill no t be necessary .
Leigh and assoc iates hav e recommendedinjec ting methylene blue into the esophagusand then searching for the characteris ticstain in the trachea.
Eight patients have receiv ed endoscopy;the fistulous opening has been identif ied bybroncho scopy on three o ccasions andbroncho scopy plus esophagoscopy on tw ooccasions. I t is ev ident that lack o f v isuali-zatio n w ith endoscopy does no t rule out thediagnosis.
A ssociated A nom alies. These have beenlisted in Chart I. This group has beengathered from the proto co ls o f 1 9 patients.
Treatm ent. Surgery is the o nly cure forthe condition. The one case repo rted as aspontaneous cure is considered a doubtfulcase . Holinger used sodium hydroxide tocauterize the opening of the tract. The fis-tula recurred and surgery w as required forpermanent cure .
The first case treated surg ically w as re -ported by Imperatori in 1939 . The patientw as the son of a doctor and was operated at
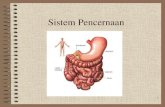
CHART IIAG E AT TIME OF SURGERY IN CONGEN ITA L TRAdHEO-
ESOPhAGEAL FISTULA
a. 4 daysb. 5 w eeksc. 5 w eeks
8 months4 ye a r s6 months6 years7 years3 months
a. 7 w eeksb. 1 w eek
11 years6 weeks
3 months
. Provided by Viet Nam:AAP Sponsored on November 19, 2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/ -
8/8/2019 1954 Congenital Tracheo-esophageal Fistula Without Atresia of the Esophagus by George Wiwarsi War.e,
5/7
TRACHEO- ES OP HAGEAL F I S TULA WI THOUT ATRES I A 2 5 7the ag e of seven y ears. H is prev ious historyand tribulations form fasc inating reading .
Thirteen patients have now been oper-ated.6 10, 1 1, 12, 14 , 17, 21, 29Three patientsdid no t surv iv e surg ery .6 21 The age of thepatients at time of surgery is shown in ChartI I .
Post-operative complications inc luded re-currence or pers istence of the fistula/4 17 in-fec tion o f thigh and back,2 and tensionpneumothorax .2 One of the persistent o rrecurrent fistulae c losed spontaneously , butthe second required another operation.14
SUMMARYCongenital tracheo -esophageal f istula
w ithout atres ia o f the esophagus is a rareanomaly . Tw enty-six patients are repo rtedin the literature . The autho rs report an ad-ditional case . The etio logy is still o bscure ,but may be due to the dev elopment of aber-rant blood vesse ls .
Patients present a triad of signs andsymptom s, coughing and cyanosis w ith feed-ing s, abnormal dis tention o f gastro -intesti-nal trac t and persistent pneumonitis .
Radiographic investigation is mo st im-po rtant. Lipiodo l study o f the esophagus inthe oblique or prone position is the mostrew arding diagnostic test.
Surg ery is the only method o f cure .B I B L I O G RAPHY
1. Barkely , H . T., Quoted by Haight: J. Tho-racic Surg ., 17 :600-612, Oct. 1948 .
2. Berman, J. K ., Test, P. S ., M cA rt, B . A .:Congenital esophagobronchial f istula inan adult. J. Thoracic Surg ., 24:4 93 -500 ,N ov . 1952.
3 . B row n, R. K ., B row n, E. C. : Cong eni-tal e sophageal anomalies . Surg . Gynec.Obst., 91 :5 45-550 , N ov . 1951 .
4. Cautley , E. : M alformation o f e so phagus .Brit. J. Child. D is., 1 4:1-10 , Jan. 1917 .
5 . Cardullo , H . M ., B erens, D . L. : Tracheo -e sophageal fistula unassoc iated w ithatresia or s teno sis , N ew Eng land J.M ed., 243:853-856 , N ov . 1950 .
6. Ferguson, C. F. : Congenital tracheo -e so -phageal fis tula no t assoc iated w ith eso -phageal atre sia. Laryng oscope , 61 :7 18 -766 , A ug . 195 1 .
7. Fluss, Z., Poppen, K .J. : Embryogenesiso f tracheo -e sophageal fistula and eso -phageal atre sia. A rch. Path., 5 2 :168 -181 ,Aug . 1951 .
8 . Gengenbach, F.P. , D obos, E. I. Congeni-tal tracheo-esophag eal fis tula. J. Pediat.,.19 :6 44-655 , N ov . 1 941 .
9 . Gross , R. E. : A tresia of the Esophagus, inThe Surgery of Infancy and Child-hood. Philade lphia, W . B . Saunders,1 953 , p. 7 5 .
10 . Haight, C . : Congenital tracheo-esophag ealfistula w ithout esophag eal atresia. J.Thorac ic Surg ., 1 7:600-612 , Oct. 1948 .
11 . Helm sw orth, J. A ., Pry les, C. V .Congeni-tal tracheo -e sophageal fis tula w itho ute sophageal atre sia. J. Pediat., 38 :610 -6 17 , May , 1 951 .
12 . Holinger, P.H ., Johnston, K. C ., Po tts,w . J. : Congenital anomalies of theesophagus. A nn. O to l. Rhin. & Laryng .,60 :707 -731 , S ept. 1951 .
13 . Holt, J. F., Haight, C., Hodges, F. J.:Congenital atresia of esophagus andtracheo-esophag eal f istula. Radio lo gy ,47 :457 -470 , N ov . 1946 .
14 . Imperatori, C. J. Congenital Tracheo-eso-phageal fistula w ithout atre s ia o f e so pha-gus. A rch. Oto laryng ., 30 :352 -360 , S ept.1 939 .
15 . Ingalls , T. H., Prindle , R. A . : Esophagealatres ia w ith tracheo -e so phageal fistula.N ew Eng land J. Med., 2 40:9 87-995 ,June 1949 .
16 . Keith, A ., Spicer, J. E.Three cases ofmalfo rmation o f tracheo-esophag eal sep-tum . J. A nat. & Phys io l., 41 :5 2 -55 , Oct.1906 .
17 . Knox , G. : Congenital tracheo-esophag ealfis tula w itho ut e sophageal atre sia. Sur-gery , 30 :101 6 -102 0 , D ec . 19 51 .
18 . Lamb, D . S . : A fatal case o f co ngenitaltracheo -e sophageal fis tula. Philade lphiaMed. Times, 3 :705 -707 , A ug . 1873 .
19 . Lev en, N . L., Lannin, B . G . : Congeni-tal atre s ia and congenital tracheo -eso -phageal fis tula. Journal-Lance t, 65 : 179 -1 81 , M ay 1945 .
20 . Leven, N . L., V arco , R. L., Lannin, B . C .,Torgen, L. A . : Surg ical management o fcongenital atresia o f esophagus andtracheo -e sophageal f is tula. A nn. S urg .,1 3 6 : 7 0 1 - 7 1 9 , Oc t . 1 9 5 2 .
2 1 . Le igh, T. F., A bbott, 0 . A ., Hopkins , W .A . : Roentg enolog ic considerations intracheo-esophageal f istula w ithout eso-phageal atresia. Radio logy , 5 7:871-877 ,D ec. 1951 .
. Provided by Viet Nam:AAP Sponsored on November 19, 2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/ -
8/8/2019 1954 Congenital Tracheo-esophageal Fistula Without Atresia of the Esophagus by George Wiwarsi War.e,
6/7
25 8 GEORGE WI LLI AM WARE AND LOUI S L. CROS S
90 0 17 th Stree t N.W .
22 . L ohnes , H . R . : R are fo rm of con gen ita ltracheo-esoph ag ea l fis tu la . B u ll. B uffa loG en . H osp ., 1 :109 -1 12 , O c t. 1 92 3 .
23 . M acK enz ie , M . : M alfo rm ations of th eesoph ag us. A rch . L aryng ., 1 :3 01-3 15 ,D ec. 18 80 .
24 . M acK enz ie , M . A M anua l o f D iseases o fth e T hroa t an d N ose. N ew Y ork , W m .W ood and C o ., 188 4 , p . 1 49 .
25 . M cK inn ey , R . : T rach eo -esop hagea l fis tu la ,p ro bab ly congen ita l. A nn . O to l. R h in . &Laryn g ., 4 2 :1234 -1236 , D ec . 1933 .
26 . M orton , D . R ., O sbourne , J . F ., K la ssen ,K . P . : An appa ren tly con gen ita l b ro ncho-e so phagea l f is tu la pe rsis ten t to adu ltlife. J. Thorac ic Surg ., 1 9 :81 1-816 , M ay1950 .
27 . N egu s, V . E . : E sop hag us from a midd le -aged m an sh ow ing co ngen ita l open in gin to trachea. J. Lary n g . & O to l., 4 4 :18 4 ,M ay 1929 .
28 . Po tts , W . J. : A tres ia o f esoph ag us. P os t-g rad ua te M ed ., 10 :304 -3 10 , O c t. 1 951 .
29 . R obb , D . : C ongen ita l tracheo-e sop hagealfistula w itho u t atre sia. A ustralian andN ew Zealand J. Surg . , 22 : 120-12 2 , N ov .1952 .
30 . R osen th a l, H . H . : C ong en ital atre sia o fe sop hagus w ith tracheo-eso ph ag ea l fis-tu la . A rch . P a th ., 12 :756 -7 72 , M arch1 931 .
3 1 . R uck s, W . L . : T racheo-e soph ageal fis tu la .M em phis M ed . J. , 7 :2 09-21 1 , N ov .1 9 3 0 .
32 . S haw , R . : Q uo ted by H aigh t. J . T ho rac icSurg . , 17 :6 00-61 2 , O c t. 1 948 .
33 . S toeck le in , C .J. , N ettrour, W . S . : A cu te
tracheo-eso phagea l fistu la . P en nsy lv an iaM J ., 4 6 :89 8-9 01 , S ep t. 19 43 .
SPAN ISH AB STR AC TFIstu la T r a q u eo E so f g ica C on g#{233}n it a
s in A t r e s ia d e E s#{243 }f agoL a fIs tu la con g#{233 }n ita traqueo-e so f#{2 25}g ica s in
atresia de es# {243 }fago es una anom alIa rara. L arev is io n de la lite ra tu ra al re spec to reve l#{243 } lafecha so lo 26 caso s, a lo s que lo s au to re s ag re -gan uno m #{225} s,u e se tra t#{243}u ir#{241}rg icam en te contodo #{233}x ito .
L a e tio lo g Ia de Ia fIstu la no se ha ex p licadoann sa tisfacto riam ente ; pu ede deberse aa pre-sion que erjecen vasos sanguIn eo s aberran tesduran te e l d esa rro llo em brio l#{2 43}g ico .
D esde e l pu n to de v ista c lm nico H elm sw o rthha sef la la do una tria da d iagn #{243} stic a: pa rox ism osde tos a l alim en ta rse a l n ifio ; d is ten sion an orm alde l tu bo gas tro -in testina l deb id o a l p aso de la ire traq uea l hac ia e l es#{2 43}fag o y neum onitispers isten te q ue por lo com #{241}n se loc aliza en e ll#{24 3}bu lo up er io r d erecho . L os es tud ios rad io l#{243}g i-co s p ara ac la ra r Ia anom alla deben inc lu irsiempre Ia ing estion de lip io do l, co locando a lnino en p osic i#{2 43}n decib ita dorsa l u ob licua ; enes ta fo rm a e l d iagn# {243 }s tico se ob tiene en m #{225}sel50% de los caso s. L a eso fago scop la y /# {2 43}a bro n-cosco pla ayu dan frecu en tem ente a rev elar IafIstula.
E l in ico tratam ien to es el qu iru rg ico ; searea lizado con #{233 }x iton 10 de lo s 1 3 casos tra -tados .
. Provided by Viet Nam:AAP Sponsored on November 19, 2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/ -
8/8/2019 1954 Congenital Tracheo-esophageal Fistula Without Atresia of the Esophagus by George Wiwarsi War.e,
7/7
1954;14;254-258PediatricsGEORGE WILLIAM WARE and LOUIS L. CROSS
THE ESOPHAGUSCONGENITAL TRACHEO-ESOPHAGEAL FISTULA WITHOUT ATRESIA OF
& ServicesUpdated Information
http://www.pediatrics.orgincluding high-resolution figures, can be found at:
Citationshttp://www.pediatrics.org#otherarticles
This article has been cited by 3 HighWire-hosted articles:
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtmlits entirety can be found online at:Information about reproducing this article in parts (figures, tables) or in
Reprintshttp://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be found online:
. Provided by Viet Nam:AAP Sponsored on November 19, 2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/#otherarticleshttp://www.pediatrics.org/#otherarticleshttp://www.pediatrics.org/#otherarticleshttp://www.pediatrics.org/misc/Permissions.shtmlhttp://www.pediatrics.org/misc/Permissions.shtmlhttp://www.pediatrics.org/misc/Permissions.shtmlhttp://www.pediatrics.org/misc/reprints.shtmlhttp://www.pediatrics.org/misc/reprints.shtmlhttp://www.pediatrics.org/misc/reprints.shtmlhttp://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/misc/reprints.shtmlhttp://www.pediatrics.org/misc/Permissions.shtmlhttp://www.pediatrics.org/#otherarticleshttp://www.pediatrics.org/