18th Expert Committee on the Selection and Use of Essential
24
1 18th Expert Committee on the Selection and Use of Essential Medicines Reviewer No. 1 checklist for: Review of medicines for the treatment of common tumours in Children In the WHO Essential Medicines List (1) Have all important studies that you are aware of been included? Yes No X (2) Is there adequate evidence of efficacy for the proposed use? Yes No X (3) Is there evidence of efficacy in diverse settings and/or populations? Yes X No (4) Are there adverse effects of concern? Yes X No (5) Are there special requirements or training needed for safe/effective use? Yes X No (6) Is this product needed to meet the majority health needs of the population? Yes No X (7) Is the proposed dosage form registered by a stringent regulatory authority? Yes X No
Transcript of 18th Expert Committee on the Selection and Use of Essential

1
18th Expert Committee on the Selection and Use of Essential
Medicines
Reviewer No. 1 checklist for:
Review of medicines for the treatment of common tumours in Children
In the WHO Essential Medicines List
(1) Have all important studies that you are aware of been included? Yes No X (2) Is there adequate evidence of efficacy for the proposed use? Yes No X (3) Is there evidence of efficacy in diverse settings and/or populations? Yes X No (4) Are there adverse effects of concern? Yes X No (5) Are there special requirements or training needed for safe/effective use? Yes X No (6) Is this product needed to meet the majority health needs of the population? Yes No X (7) Is the proposed dosage form registered by a stringent regulatory authority? Yes X No
2
(8) What action do you propose for the Committee to take? To rename the subsections 8.2 and 8.3.
To delete cytotoxic agents not mentioned for prevalent childhood cancer (subsection 8.2). To add mesna as an adjuvant medicine (subsection 8.2).
To discuss retaining two anthracycline agents, two alkylating agents, and two Vinca alkaloids or choosing one of them (subsection 8.2). To delete dexamethasone oral formulation (subsection 8.3) To delete the observation “Specific use for management of bone pain.” regarding ibuprofen for palliative care (subsection 8.4). To add fluoxetine and ondansetron for palliative care (subsection 8.4). To add oral midazolam formulations for palliative care (subsection 8.4).
(9) Additional comment, if any. General Comments
Antineoplastic agents are used for different purposes: curative (for eradicating the disease and preventing the recurrence), palliative (for relieving tumour symptoms), adjuvant (for preventing tumour recurrence after proved exclusion of residual disease), and neo‐adjuvant (for administrating before a local definitive treatment is done). These agents are prescribed in monotherapy or in combination. Antineoplastic medicines in combination are more effective, since they act in different phases of the cell cycle, by different and synergistic mechanisms of action. The combination therapy has additional benefits relating to not sharing common mechanisms of resistance and similar profiles of major toxicities. So, it is convenient to include at least one representative of each antineoplastic class, according to his benefit in children cancer treatment.
To say the least, the therapeutic response depends on the tumour histological type and localization, as well as the disease stage and other concomitant cancer strategies, such as surgery and radiotherapy. These multiple variables influence the choice of antineoplastic agents. The efficacy is usually evidenced by clinical protocols rather than by randomised clinical trials or meta‐analyses. The great variability retrains pooled‐data.
Actually the literature search finds mainly book chapters, descriptive reviews, cohort studies (follow‐up studies), non‐randomised trials, and guidelines, as showed in the review offered to be analysed. The strong evidence of efficacy and safety – provided by systematic reviews, meta‐analyses and randomised controlled studies (RCTs) – is scarce in cancer pharmacology for children, especially the face‐to‐face comparisons. Even the RCTs have methodological limitations.
Additionally the difficulty of choice increases because cancer is a complex disease, with variable development, severe and multiple clinical manifestations and sequelae which compromise survival, morbidity and quality of life.

3
Therefore, the decision of which medicines should be included for treatment of cancer diseases in children needs to follow a different and unusual rationality, somehow changing the criteria. The efficacy usually comes from clinical protocols (in general including medicine combinations to minimize the emergence of resistance) based on the institutional and professional experience. The inclusion also considers the ability to act in different phases of the cell cycle (subclasses with different mechanisms of action), and the degree of tumour cell resistance to certain medicines (justifying more than one representative of the same pharmacological subclass). Clinically the medicine choice is made regarding patient’s age, intensity and stage of the disease, potential treatment toxicity, and risk of relapses. Taking into account that all antineoplastic agents induce harmful, and even severe, side effects, the safety criterion has to counterbalance these risks with the rapid, and even fatal, cancer disease development. The convenience of treatment is an important issue to consider, especially in children (dosage, concentration, pharmaceutical formulation, routes of administration). The favourable comparative cost should be also considered, allowing the developing countries can afford it. Considering the essential concept that guides the List, it is worth choosing medicines used for treatment of the most common cancer diseases in children. The most common paediatric malignancies have a general incidence in the following order: leukaemias (30%), brain and other nervous system cancers (22.3%), neuroblastoma (7.3%), Wilms tumour (5.6%), non‐Hodgkin lymphoma (4.5%), rhabdomyosarcoma (3.1%), retinoblastoma (2.8%), osteosarcoma (2.4%), and Ewing sarcoma (1.4%). 1 The offered review only analyses acute lymphoblastic leukaemia (ALL), Burkitt lymphoma (BL) and Wilms Tumour (WT).
Aim of the comments: To review, through a clinical pharmacologic perspective, antineoplastic and adjuvant medicines (for correction of some antineoplastic side effects), and medicines used in palliative care during cancer treatment to rationally decided their inclusion in the WHO EMLc. Literature search: A PubMed search – performed in February 2011, using as key words the names of the common cancer diseases in children and the names of recommended antineoplastic agents, with the activated limits “Humans, Meta‐Analysis or Randomized Controlled Trial, All Children: 0‐18 years, published in the last 3 years” – found few studies regarding leukaemias (e.g. acute lymphoblastic leukaemia – ALL), non‐Hodgkinʹs lymphoma (e.g. Burkitt´s lymphoma – BL), Wilms Tumour, Ewingʹs sarcoma, rhabdomyosarcoma, and brain tumours treatment. For instance: For ALL – 7 meta‐analyses; 52 RCTs For BL – no items found (meta‐analysis); 2 RCTs For WT – 2 meta‐analyses; 7 RCTs

4
The 3‐year search period was chosen to partially cover the published information after the former committee had decided the inclusion of cancer medicines in the current EMLc. An additional search in the Cochrane Library found recent reviews about antineoplastic treatment for LLA (n=5), BL (n=5), WT (n=8), and Rhabdomyosarcoma (n=1), as well as about cytoprotective medicines (corrective effect) and medicines for palliative care. ANTINEOPLASTIC MEDICINES Cytotoxic medicines (Subsection 8.2) and Hormones and antihormones (Subsection 8.3) First of all, two suggestions: 1. Since the EMLc 8.2 subsection contains allopurinol and calcium folinate (corrective medicines instead of cytotoxic medicines) I suggest substituting its title for: 8.2 Cytotoxic medicines and adjuvant medicines (or cytoprotective medicines)
2. Since the EMLc 8.3 subsection only contains corticosteroids, antihormones are absent. So, there is no reason for the current title. I suggest its change for: 8.3 Hormones Preliminary notes:
1. The underlined medicines in the text are those already included in the 2nd EMLc (2010).
2. The reported information collected in cited RCTs and systematic reviews is only the one which concerns the members with the choice of antineoplastic medicines.
Leukaemias For childhood Acute Lymphoblastic Leukaemia or Acute lymphocytic leukaemia, clofarabine with etoposide and cyclophosphamide, 2 mitoxantrone or idarubicin,3 vincristine (VCR) plus steroid pulses (prednisone/prednisolone),4 6‐mercaptopurine (6‐MP) and methotrexate (MTX),5 and anthracyclines6 were studied. A combination of daily 6‐MP, weekly MTX and VCR/DEX (dexamethasone) pulse for maintenance treatment in standard risk or high risk 201 ALL patients evidenced no differences in the event‐free survival or overall survival in comparison to the therapy stated by ALL‐96 protocol. However the first regimen induced more liver toxicity.7 In the previous review, the 17 mentioned medicines used for ALL were: asparaginase, busulphan, cyclophosphamide, cyclosporine, cytarabine (ARA‐C), daunorubicin or doxorubicin (DOX), dexamethasone (DEX), etoposide, hydrocortisone, imatinib, leucovorin, mercaptopurine (6‐MP), methotrexate (MTX), methylprednisolone, prednisone, and vincristine (VCR). The review said that “intensive use of asparaginase either IM or IV, is especially recommended in CNS prophylaxis, but at present there appears to be no reasonable alternative to the availability of all three forms of asparaginase”. The current list already includes 13 of these medicines. The exceptions are busulphan, imatinib, methylprednisolone, and prednisone.

5
Attention: Looking at the classification of antineoplastic medicines (Table 1), one can realize that there is more than one representative in the same subclass. So, it is interesting to discuss efficacy and safety among representatives. 1. A RCT8 compared two purine analogs – oral 6‐mercaptopurine (6‐MP) versus oral 6‐thioguanine (6‐TG) – in the treatment of standard‐risk ALL. The estimated 7‐year event‐free survival for subjects randomized to TG was 84.1% (+/‐ 1.8%) and to MP was 79.0% (+/‐ 2.1%); P = 0.004 log rank), although overall survival was 91.9% (+/‐ 1.4%) and 91.2% (+/‐ 1.5%), respectively (P = 0.6 log rank). However, 6‐TG was associated with hepatic veno‐occlusive disease or disproportionate thrombocytopenia. The toxicities of TG preclude its protracted use as given in this study. In conclusion, 6‐MP has similar overall survival and lesser serious toxicity than 6‐TG in ALL treatment. 2. Anthracycline antibiotics include daunorubicin, doxorubicin, idarubicin, valrubicin, epirubicin. For ALL patients’ treatment, daunorubicin or doxorubicin or idarubicin were used. One issue to discuss is related to their cardiotoxicity. Anthracycline treatment versus non‐anthracycline treatment A systematic Cochrane review9 identified RCTs for 5 types of tumour: acute lymphoblastic leukaemia (ALL) (n=3; 912 children), Wilmsʹ tumour (n=1; 316 children), rhabdomyosarcoma/ undifferentiated sarcoma (n=1; 413 children), Ewingʹs sarcoma (n=1; 94 children), and non‐Hodgkin lymphoma (n=1; 284 children). The comparison of anthracycline treatment versus non‐anthracycline treatment showed no evidence of a significant difference in antitumour efficacy between the treatment groups for the management of ALL, rhabdomyosarcoma/undifferentiated sarcoma and non‐Hodgkin lymphoma patients. For both Wilms´ tumour and Ewingʹs sarcoma a significant difference in survival in favour of treatment with anthracyclines was identified. The hazard ratios for overall and event‐free survival in Wilmsʹ tumour were 1.85 (95% CI: 1.09 to 3.15) and 2.21 (95% CI: 1.44 to 3.40), respectively. For patients with Ewingʹs sarcoma only descriptive results were available (P = 0.02 for overall survival and P = 0.01 for event‐free survival). Clinical cardiotoxicity was evaluated in 3 RCTs. No significant difference between both treatment groups was identified, but in all individual studies there was a suggestion of a lower rate of clinical cardiotoxicity in patients who did not receive anthracyclines. Epirubicin versus doxorubicin regarding cardiotoxicity Regarding cardiotoxicity another Cochrane systematic review10 evaluated five RCTs of varying quality addressing epirubicin versus doxorubicin (1036 patients) with the same dose. The meta‐analysis showed no evidence for a significant difference in the occurrence of clinical heart failure between the treatment groups (RR = 0.36; 95% CI: 0.12 to 1.11). However, there is some suggestion of a lower rate of clinical heart failure in patients treated with epirubicin. For both epirubicin versus doxorubicin and liposomal‐encapsulated doxorubicin versus conventional doxorubicin no conclusions can be made about the effects of treatment in children treated with anthracyclines and also not in patients diagnosed with leukaemia.

6
In conclusion, anthracycline derivatives probably have similar efficacy and safety in childhood common malignancies. The Committee may choose either doxorubicin or daunorubicin, the most frequent representatives used. 3. Regarding corticosteroid choice in ALL and lymphomas, the previous review mentioned dexamethasone as “a more potent agent than prednisone, especially in relation to control of subclinical disease in the CNS, but it is associated with more morbidity from infection, greater neurocognitive pathology and increased bony sequelae (demineralization and osteonecrosis) in ALL patients”.11 Actually, corticosteroid agents have different relative anti‐inflammatory potencies, well‐balanced by equivalent doses,12 and the term potency does not mean exactly efficacy. Other studies use prednisone rather than prednisolone, already included in the EMLc. By injection, dexamethasone (long‐action) and hydrocortisone (short‐action) could be rationally employed. For oral use, it seems better to choose prednisolone due to its both pharmaceutical forms – tablet and oral liquid – useful in children at different ages. For diminishing HPA axis suppression, the intermediate‐acting steroid preparations (e.g. prednisone or prednisolone) given early in the morning, as a single dose, should be preferred for patients who need long‐term (beyond one week) oral therapies. Then, dexamethasone oral preparation could be deleted from the subsection 8.3 of WHO EMLc. In conclusion, it seems reasonable to maintain oral prednisolone and injectable dexamethasone and hydrocortisone in the 8.3 subsection. Concerning treatment for childhood acute myeloid leukaemia (AML), a multicentre study13 randomised 230 patients to receive high‐dose or low‐dose cytarabine with daunorubicin and etoposide (ADE) for induction 1. Induction 2 consisted of ADE with or without gemtuzumab ozogamicin (GO anti‐CD33 monoclonal antibody). Complete remission was achieved in 80% (173 of 216 patients) after induction 1 and 94% (203 of 216) after induction 2. High‐dose versus low‐dose cytarabine did not show significantly difference in efficacy (P=0.17), and high‐dose was associated with higher infection. For the authors the use of targeted chemotherapy can improve outcome in patients with childhood AML. Because cladribine can increase cytarabine triphosphate levels, cladribine‐cytarabine combination was administered before standard chemotherapy to 96 children with acute myeloid leukemia (AML) or myelodysplastic syndrome. Patients received the combination in intermittent way (arm A) or through continuous infusion (arm B). Although there were trends toward better complete remission rates and overall survival for patients treated in arm B, the reduced efficacy of arm A may have been partially compensated by more intense timing of therapy for that group. 14
Brain and other nervous system cancers The studies mentioned cyclophosphamide and carboplatin,15 and topotecan16 for recurrent or resistant paediatric brain tumours. A review17 considered cyclophosphamide, cisplatin, doxorubicin, and teniposide as a standard treatment and carboplatin plus etoposide or cyclophosphamide, doxorubicin, and vincristine as

7
two alternative regimens for neuroblastoma treatment. Cisplatin plus etoposide and melphalan plus cyclophosphamide were considered for standard risk and recurrent medulloblastomas, respectively. For high‐risk neuroblastoma the current standard treatment includes initial induction chemotherapy, performed as a rapid regimen (cisplatin, vincristine, carboplatin, etoposide, and cyclophosphamide, known as COJEC) or standard treatment (vincristine, cisplatin, etoposide, and cyclophosphamide, ie, OPEC), alternated with vincristine, carboplatin, etoposide, and cyclophosphamide (ie, OJEC). In 262 patients (median age 2.95 years) with high‐risk neuroblastoma, randomly assigned to rapid or standard regimen, there was not significant difference in overall survival. However, an increasing difference in event‐free survival after 3 years suggests that the efficacy of the rapid regimen is better than the standard regimen.18 In an observational study,19 21 children less than 3 years old with non‐metastatic medulloblastoma received induction chemotherapy consisting of vincristine, cisplatin, cyclophosphamide and etoposide. Following induction, all patients underwent myeloablative chemotherapy using carboplatin, thiotepa and etoposide. Irradiation was used only at relapse. This strategy of brief intensive chemotherapy eliminated the need for craniospinal irradiation in 52% of the patients, and may preserve intellectual functioning. The excellent survival rates are somewhat dampened by high toxic mortality.
Lymphomas For childhood Non‐Hodgkin Lymphoma, LSA2‐L2 protocol (cyclophosphamide, vincristine, methotrexate, carmustine, hydroxyurea, daunorubicin, prednisone, cytarabine, thioguanine, and asparaginase) was compared with COMP (cyclophosphamide, vincristine, methotrexate, prednisone), identifying that these chemotherapy regimens exert different effects in different NHL subtypes. COMP regimen is an effective combination for non‐lymphoblastic lymphoma, including Burkitt’s lymphoma (BL). Lymphoblastic lymphoma – the regimen includes corticosteroids, vincristine (VCR), anthracyclines, L‐asparaginase (L‐Asp), cyclophosphamide (CP), methotrexate (MTX), cytarabine, 6‐mercaptopurine (6‐MP), and 6‐thioguanine. B‐NHL ‐ corticosteroids, VCR, CP or ifosfamide, MTX, cytarabine, doxorubicin, etoposide, and triple drug (MTX/cytarabine/corticosteroid) ALCL ‐ for high‐risk anaplastic large‐cell lymphoma vinblastine was used as induction and maintenance treatment. 20 For Burkittʹs lymphoma cyclophosphamide as monotherapy was used in children.21 The previous review considered cyclophosphamide, cytarabine, doxorubicin, etoposide, hydrocortisone, methotrexate, prednisone, and vincristine as essential medicines for this lymphoma. In a study22 performed in Malawi, Cameroon, and Ghana, Burkittʹs lymphoma was treated with cyclophosphamide, vincristine, prednisone and methotrexate, all of which are inexpensive. High dose intense combinations are not always appropriate if the supportive care resources are not present. A Cochrane systematic review23 of ten studies of insufficient quality does not currently provide any strong evidence on the relative effectiveness of interventions

8
to treat Burkittʹs lymphoma. The studies were small, underpowered and prone to both systematic and random error. A cohort study (n= 132 children and adolescents) 24 recommends two courses of COPAD (cyclophosphamide, vincristine, prednisolone and doxorubicin) for all children with localized resected Burkitt´s lymphoma. Two of 264 (0.9%) courses were associated with grade IV toxicity (one stomatitis and one infection). With a median follow up of 50.5 months, the 4 year event‐free survival is 98.3% and overall survival is 99.2%.
Wilms Tumour or nephroblastoma Vincristine, dactinomycin, doxorubicin and cyclophosphamide were mentioned for the management of Wilms tumour. 25 More recently ifosfamide, carboplatin and etoposide (ICE) constitute a second line therapy for poor‐risk relapsed patients. In a descriptive study26 performed in 11 children the authors considered that the optimal approach for post‐ICE consolidation therapy has yet to be determined. In low income countries, vincristine and actinomycin D are the commonly used medicines. In the previous review dactinomycin, carboplatin, cyclophosphamide, doxorubicin, etoposide, ifosfamide, and vincristine are considered essential medicines for WT management. In the already cited Cochrane review9 only one RCT (n=316 children) showed a significant difference in survival in favour of treatment with anthracyclines for WT. The hazard ratios for overall and event‐free survival in WT were 1.85 (95% CI: 1.09 to 3.15) and 2.21 (95% CI: 1.44 to 3.40), respectively. Soft‐tissues sarcomas Rhabdomyosarcoma (RMS) is the most common soft tissue sarcoma of childhood. For the treatment of children with RMS the recommended regimens included irinotecan with vincristine,27 and vincristine, actinomycin D and cyclophosphamide (standard VAC).28 An alternative regimen included vincristine, topotecan, and cyclophosphamide.29 A combination of etoposide, vincristine, dactinomycin, ifosfamide, and doxorubicin (EVAIA) was evaluated for high‐risk patients. Intensified chemotherapy with EVAIA did not improve outcome of localized high‐risk rhabdomyosarcoma.30 A Cochrane review31 intended to evaluate the effectiveness of high‐dose chemotherapy (HDC) versus standard‐dose chemotherapy in improving event‐free survival (EFS) and overall survival (OS) in children and young adults with metastatic rhabdomyosarcoma. No RCTs could be identified. All studies have severe methodological limitations, in particular selection bias could not be excluded. A clinically important excess of adverse risk patients in the HDC arms may explain the non‐beneficial effect of HDC.
Bone tumours For osteosarcoma the combination of gemcitabine and irinotecan32 was recommended, as well as a multimodal therapy including epirubicin, cisplatin, and ifosfamide.33 Conventional treatment regimens for metastatic and recurrent localized Ewing sarcoma vary but in general consist of a combination of the following

9
chemotherapeutic agents: vincristine, dactinomycin, cyclophosphamide, doxorubicin, ifosfamide, and etoposide. In North America, the 5‐drug regimen of vincristine, doxorubicin, and cyclophosphamide (VDC) alternating with ifosfamide and etoposide (IE) is considered standard.34 The European Intergroup Cooperative Ewingʹs Sarcoma Study investigated whether cyclophosphamide has a similar efficacy as ifosfamide in standard‐risk (SR) patients and whether the addition of etoposide improves survival in high‐risk (HR) patients. SR patients were randomly assigned to receive vincristine, dactinomycin, ifosfamide, and doxorubicin (VAIA) induction therapy or vincristine, dactinomycin, cyclophosphamide, and doxorubicin (VACA; cyclophosphamide replacing ifosfamide). HR patients were randomly assigned to receive either VAIA or VAIA plus etoposide (EVAIA). Cyclophosphamide seemed to have a similar effect on EFS and OS as ifosfamide in SR patients but was associated with increased toxicity. In HR patients, the addition of etoposide seemed to be beneficial.35 A regimen including vincristine, cyclophosphamide, doxorubicin (VDC), and dactinomycin alternating with ifosfamide and etoposide (intensified regimen) was compared to VDC (standard regimen) in patients with nonmetastatic Ewing sarcoma family of tumors (ESFT) of bone. There was no difference in outcome between patients with soft tissue and bone primary sites.36 Attention: Cyclophosphamide vs. ifosfamide For bone and soft tissue sarcomas management cyclophosphamide (standard therapy) and ifosfamide (second line therapy) were considered in children and adolescents. Despite an improved survival with both alkylating agents, there is still controversy regarding their comparative anti‐tumour efficacy and possible adverse effects. A systematic Cochrane review37 intended to compare the possible effectiveness of cyclophosphamide with that of ifosfamide for paediatric and young adult patients with sarcoma. No studies (RCTs or controlled clinical trials) meeting the inclusion criteria of the review were identified. The authors concluded that no definitive conclusions can be reached about the effects of cyclophosphamide and ifosfamide in these patients. Based on the currently available evidence it is not possible to give recommendations for clinical practice. More high quality research is needed. However, ifosfamide is associated with higher incidence of haemorrhagic cystitis and haematuria (see adjuvant medicines – mesna). In conclusion, the Committee should discuss the inclusion of only one or both alkylating agents, balancing the lack of evidence, the higher nephrotoxicity of ifosfamide, and the clinical use of ifosfamide. Adjuvant medicines or cytoprotective agents Some medicines in subsection 8.2 are adjuvant medicines: they are not antineoplastic medicines; their role is to control side effects of antineoplastic agents. I suggest adding this word in the subsection 8.2 title. The current EMLc already includes allopurinol and calcium folinate. The role of allopurinol is to correct hiperuricemia which may occur during 6‐MP. Calcium folinate acts as rescue therapy in high‐dose MTX regimen.

10
I suggest discussing the inclusion of other adjuvant medicines, such as:
Urate Oxidase – a Cochrane review38 of 5 studies (336 patients in the treatment groups and 458 patients in the control groups) evaluated the effectiveness and safety of urate oxidase in the prevention and treatment of tumour lysis syndrome (TLS) in children with malignancies. Preliminary reports suggest that urate oxidase is highly effective in reducing serum uric acid. One RCT and three CCTs compared urate oxidase and allopurinol. The RCT showed no significant difference in mortality or renal failure between the treatment and the control groups. One CCT reported significantly lower mortality due to TLS and lower incidence of renal failure in the treatment group. Another CCT found significantly lower uric acid in the treatment group at 72 hours and 168 hours. All included trials are highly susceptible to biases. So, it is still unclear the real benefit of reducing uric acid and preventing renal failure or mortality from TLS with this agent.
Mesna (2‐Mercapto Ethane Sulfonate sodium [NA]) ‐ to correct high‐dose cyclophosphamide or ifosfamide‐induced haemorrhagic cystitis or haematuria. Mesna is always given with ifosfamide, 39 and normally only given with higher doses of cyclophosphamide. Nephrotoxicity correlates with the total dose of the antineoplastic agents and increases in frequency in children less than 5 years of age. Mesna is used as an intravenous injection or infusion (injection 100 mg/ml). In my opinion, this medicine should be included. Dexrazoxane – anthracycline cardiotoxicity is a concern in patients receiving anticancer chemotherapy. Dexrazoxane is an iron chelator which protects against cardiac toxicity. A RCT40 randomised 100 children to receive doxorubicin (66 analysed) and 105 to doxorubicin plus dexrazoxane (68 analysed) for high‐risk ALL treatment. Five years after the completion of doxorubicin chemotherapy, mean left ventricular fractional shortening and end‐systolic dimension Z scores were significantly worse than normal for children who received doxorubicin alone but not for those who also received dexrazoxane. The protective effect of dexrazoxane in comparison to doxorubicin alone was only statistically significant concerning left ventricular wall thickness at 5 years follow‐up. With a median follow‐up for recurrence and death of 8.7 years (range 1.3‐12.1), event‐free survival was 77% (95% CI: 67‐84) for children in the doxorubicin‐alone group, and 76% (67‐84) for children in the doxorubicin plus dexrazoxane group (P=0∙99). I suggest not including this medicine due to the modest benefit in only one surrogate outcome.
Glutamic acid – can protect against vincristine‐induced neurotoxicity. In a pilot study,41 the onset of neurotoxicity was significantly earlier in placebo group than in glutamic acid group regarding tendon Achilles reflex, patellar reflex, parestesias, and increased frequency of constipation. Glutamic acid was well tolerated with no gastrointestinal side effects in patients. This study suggested that the coadministration of oral glutamic acid with repetitive intravenous bolus injections of vincristine resulted in a reduction of its neurotoxicity. This is the only weak evidence found in this search. At this time I do not recommend its inclusion in the EMLc.
11
Granulocyte colony‐stimulating factors (G‐CSF) or granulocyte macrophage colony‐stimulating factors (GM‐CSF) – a Cochrane meta‐analysis42 evaluated the clinical benefit of the colony‐stimulating factors (CSF) in addition to myelosuppressive chemotherapy in 333 children with ALL in an effort to prevent the development of febrile neutropenia. Children with ALL treated with CSF benefit from shorter hospitalisation and fewer infections. However, there was not evidence of shortened duration of neutropenia or fewer treatment delays. There was also no useful information about survival. The role of CSF in the context of febrile neutropenia episodes is still uncertain. Although current data show statistical benefit with CSF use, substantial heterogeneity between included trials does not allow this inclusion. In conclusion, at this moment only the addition of mesna can be proposed. Section 8.4 Medicines used in palliative care
At terminal stages of cancer diseases or in cases of intolerance to the cancer therapies, patients can no longer be managed with cytotoxic therapy. At that moment alternative palliative treatment (section 8.4) should be considered. This strategy should be interprofessional. It includes medicines, supportive care, social interventions, and adequate service conditions. The aim is to get better quality of life in cancer patients. Palliative care intends to alleviate pain and other symptoms which affect childhood mortality, morbidity, and quality of life. Therefore an appropriate palliative care can be provided for controlling the most common clinical consequences of cancer diseases, such as fatigue and weakness, pain, breathlessness, anorexia and weight loss, nausea and vomiting, constipation, depression, excess respiratory tract secretions and anxiety. Even in the beginning of the disease, palliative medicines are adjuvants to other treatments which intend to prolong life. They also control clinical manifestations induced by cancer medicines.43 Systematic evidence for the safety and efficacy of these medicines in paediatric populations is often lacking. In the absence of randomized controlled trials in paediatric populations, recommendations have been based on current best available evidence which may be extrapolated from adult studies or, in some instances, based on expert opinion.44 Palliative medicines included in the EMLc (2010) are: amitriptyline, cyclizine, dexamethasone, diazepam, docusate sodium, hyoscine hydrobromide, ibuprofen, midazolam, morphine, and senna.
12
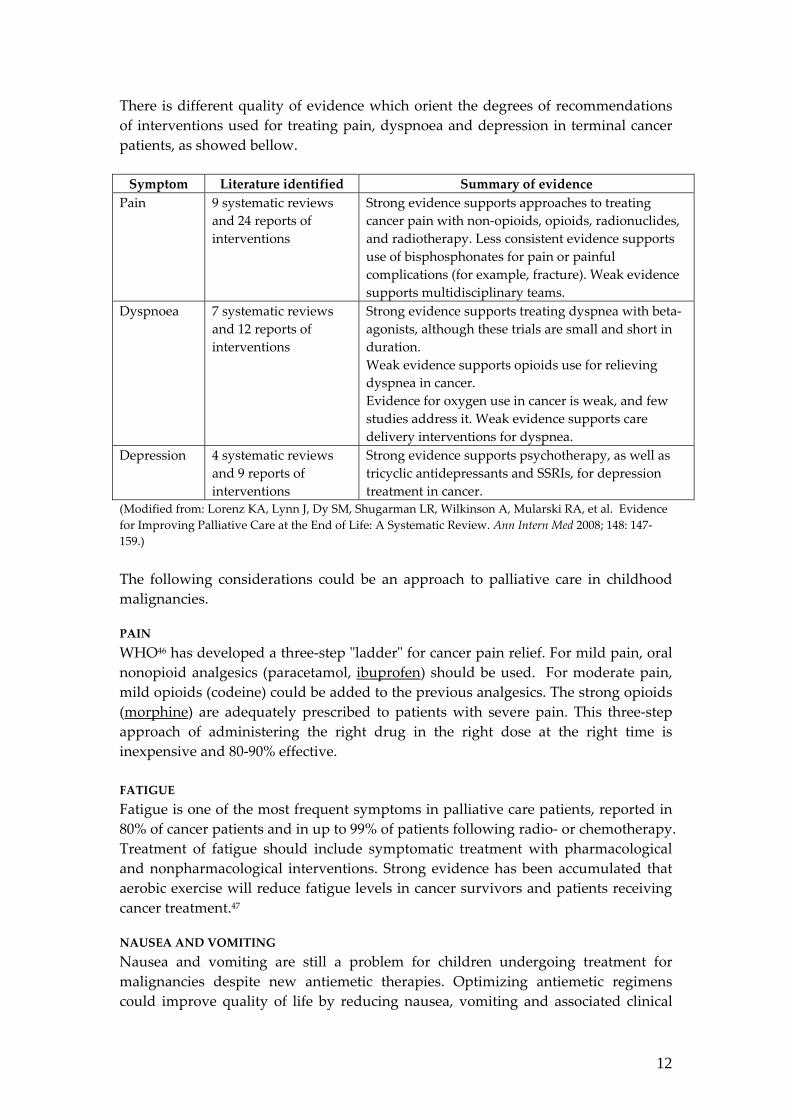
There is different quality of evidence which orient the degrees of recommendations of interventions used for treating pain, dyspnoea and depression in terminal cancer patients, as showed bellow. Symptom Literature identified Summary of evidence
Pain 9 systematic reviews and 24 reports of interventions
Strong evidence supports approaches to treating cancer pain with non‐opioids, opioids, radionuclides, and radiotherapy. Less consistent evidence supports use of bisphosphonates for pain or painful complications (for example, fracture). Weak evidence supports multidisciplinary teams.
Dyspnoea
7 systematic reviews and 12 reports of interventions
Strong evidence supports treating dyspnea with beta‐agonists, although these trials are small and short in duration. Weak evidence supports opioids use for relieving dyspnea in cancer. Evidence for oxygen use in cancer is weak, and few studies address it. Weak evidence supports care delivery interventions for dyspnea.
Depression
4 systematic reviews and 9 reports of interventions
Strong evidence supports psychotherapy, as well as tricyclic antidepressants and SSRIs, for depression treatment in cancer.
(Modified from: Lorenz KA, Lynn J, Dy SM, Shugarman LR, Wilkinson A, Mularski RA, et al. Evidence for Improving Palliative Care at the End of Life: A Systematic Review. Ann Intern Med 2008; 148: 147‐159.) The following considerations could be an approach to palliative care in childhood malignancies.
PAIN WHO46 has developed a three‐step ʺladderʺ for cancer pain relief. For mild pain, oral nonopioid analgesics (paracetamol, ibuprofen) should be used. For moderate pain, mild opioids (codeine) could be added to the previous analgesics. The strong opioids (morphine) are adequately prescribed to patients with severe pain. This three‐step approach of administering the right drug in the right dose at the right time is inexpensive and 80‐90% effective. FATIGUE Fatigue is one of the most frequent symptoms in palliative care patients, reported in 80% of cancer patients and in up to 99% of patients following radio‐ or chemotherapy. Treatment of fatigue should include symptomatic treatment with pharmacological and nonpharmacological interventions. Strong evidence has been accumulated that aerobic exercise will reduce fatigue levels in cancer survivors and patients receiving cancer treatment.47
NAUSEA AND VOMITING Nausea and vomiting are still a problem for children undergoing treatment for malignancies despite new antiemetic therapies. Optimizing antiemetic regimens could improve quality of life by reducing nausea, vomiting and associated clinical

13
problems. A Cochrane review48 included 28 RCTs which compared a pharmacological antiemetic, cannabinoid or benzodiazepine with placebo or any alternative active intervention in children and young people (< 18 years) with a diagnosis of cancer who were to receive chemotherapy. The authors concluded that the overall knowledge of the most effective antiemetics to prevent chemotherapy‐induced nausea and vomiting in childhood is incomplete. This review suggested that 5‐HT3 antagonists with dexamethasone added are effective in patients who are to receive highly emetogenic chemotherapy although the risk‐benefit profile of additional steroid remains uncertain.
In a double‐blind, randomized, placebo‐controlled, factorial trial49 performed in children with ALL undergoing combined bone marrow aspirations and lumbar punctures during maintenance therapy the addition of an opioid analgesic (fentanyl) and an anti‐emetic (ondansetron) diminishes the risk of nausea and vomiting, respectively. In EMLc dexamethasone is included, but the list misses a 5‐HT3 antagonist. Transdermal patches of hyoscine hydrobromide, indicated for excessive respiratory secretions, is also used for the prevention of postoperative nausea and vomiting.50 Motion sickness is controlled by both hyoscine hydrobromide or cyclizine.51
DEPRESSION A systematic review45 identified 11 controlled trials of antidepressants and 1 trial of pain and depression treatment in cancer. Tricyclic antidepressants (amytriptiline) and selective serotonin reuptake inhibitors (SSRI) were uniformly effective, given for sufficient treatment duration (that is, 6 weeks). This review also found strong, consistent efficacy from RCTs of various psychosocial interventions (that is, education, cognitive and noncognitive behavioral therapy, informational interventions, and individual and group support). Amytriptiline also works for chronic and neuropathic pain. On the other hand, SSRI demonstrate lesser frequency of side effects. Among SSRI agents, fluoxetine was the only one whose benefits balanced risks, according to a meta‐analysis of 27 RCTs in children. For children with age less than 12 years and depression, only fluoxetine was superior to placebo.52 In a Cochrane review of ten studies fluoxetine was the only SSRI which consistently evidenced from three trials that it was effective in reducing depression symptoms in both children and adolescents. However there was also evidence of an increased risk of suicidal ideation and behaviour in patients receiving SSRIs (RR= 1.80; 95% CI: 1.19 to 2.72).53 AGITATION/ANXIETY Fear and anxiety go along with painful procedures in children with cancer. In a double‐blind, randomized, placebo‐controlled, factorial trial49 performed in children with ALL undergoing combined bone marrow aspirations and lumbar punctures during maintenance therapy a combination of a sedative (midazolam) and an anesthetic (propofol) showed a measurable benefit in children who undergo procedures that are painful. Diazepam can be used, as well. Midazolam (short‐action) and diazepam (long‐action) have similar efficacy and different duration of effects. For intramuscular administration, midazolam is the first choice. Low‐dose oral midazolam was effective in reducing fear and distress in pediatric oncology

14
patients, especially in younger children, undergoing subcutaneous port needle insertion. The rapid beginning of action and short duration of effect is an advantage of oral midazolam over oral diazepam.
CONSTIPATION Constipation is a major source of distress for patients with cancer, significantly affecting quality of life. It can be secondary to disease sequelae, side effects of treatment, or preexisting conditions. A Cochrane review55 did not find adequate studies which evidenced the effect of stimulant laxative treatment in children with chronic constipation. Another comprehensive literature search identified 7 qualifying studies (n= 594 children) which randomly compared polyethylene glycol (PEG) versus either placebo or active comparator for chronic constipation. Five were comparisons of PEG with lactulose, one with milk of magnesia and one with placebo. PEG was significantly more effective than placebo and either equivalent to (two studies) or superior to (four studies) active comparator. Differences in study design precluded meaningful meta‐analysis. Lack of high quality studies has meant that the management of childhood constipation has tended to rely on anecdote and empirical treatment choice. 56 A recent Cochrane meta‐analysis (10 RCTs)57 compared lactulose with polyethylene glycol (PEG) for treatment for chronic constipation. PEG was better than lactulose in outcomes of stool frequency per week, form of stool, relief of abdominal pain and the need for additional products. On subgroup analysis, this was seen in both adults and children, except for relief of abdominal pain. PEG has been used frequently in the oncology population, although no published meta‐analyses, systematic reviews, or RCTs were found to support its use in that population. Stimulant (senna) or osmotic laxatives (docusate) also are likely to be effective in improving bowel function in patients with cancer who have persistent constipation. Although a guideline recommends the use of senna and docusate, a systematic review of the literature did not identify any trial to recommend the use of a specific stimulant laxative with or without the addition of a stool softener in the management of constipation in any population.58 One RCT performed in patients with terminal cancer (n = 91) comparing senna to lactulose found no significant difference in efficacy or tolerability.59
SEIZURE Seizures can present at any time before or after diagnosis of a brain tumor. The risk of seizures varies by tumor type and its location in the brain. A Cochrane review60 estimated the effectiveness of seizure prophylaxis in people with brain tumors. There was no difference between the treatment interventions and the control groups in preventing a first seizure in participants with brain tumors. The risk of an adverse event was higher for those on antiepileptic medicines, such as phenytoin, phenobarbital, and divalproex sodium, than for participants not on antiepileptic drugs (NNH 3; RR 6.10, 95% CI 1.10 to 34.63; P = 0.046). So, there is no reason to include an antiepileptic medicine in the EMLC. The following tables intend to summarize the evidenced information and the opinion of this reviewer:

15
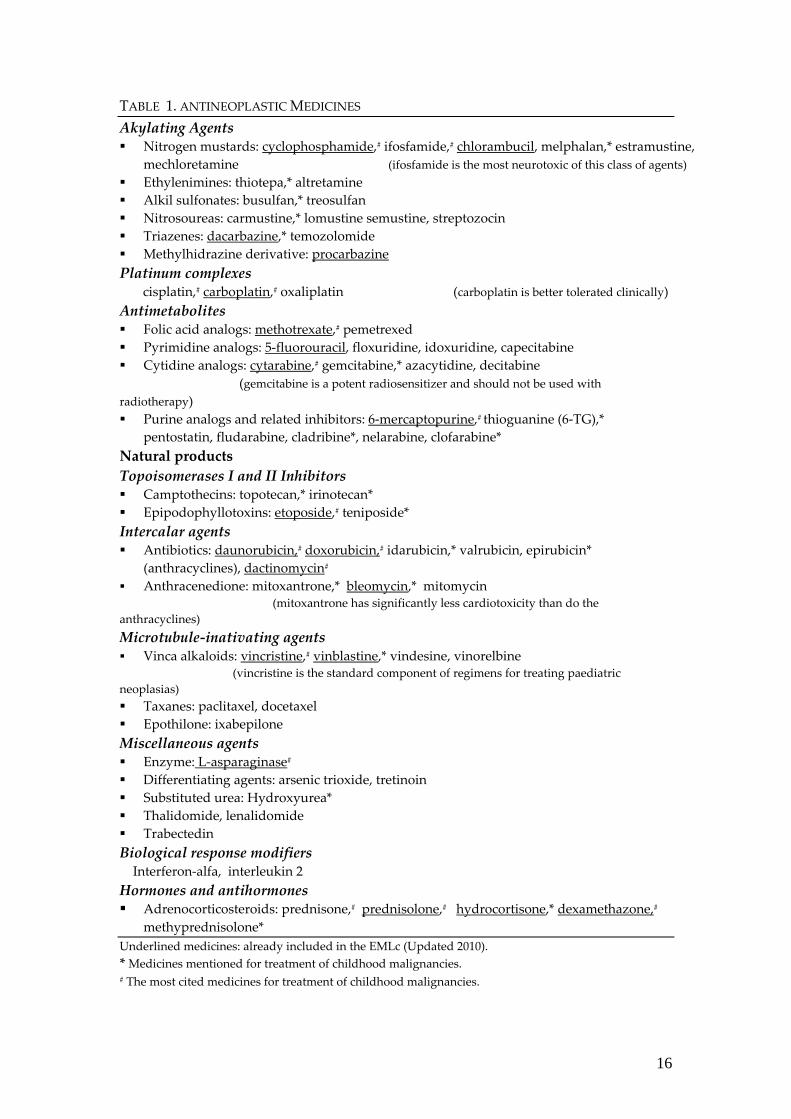
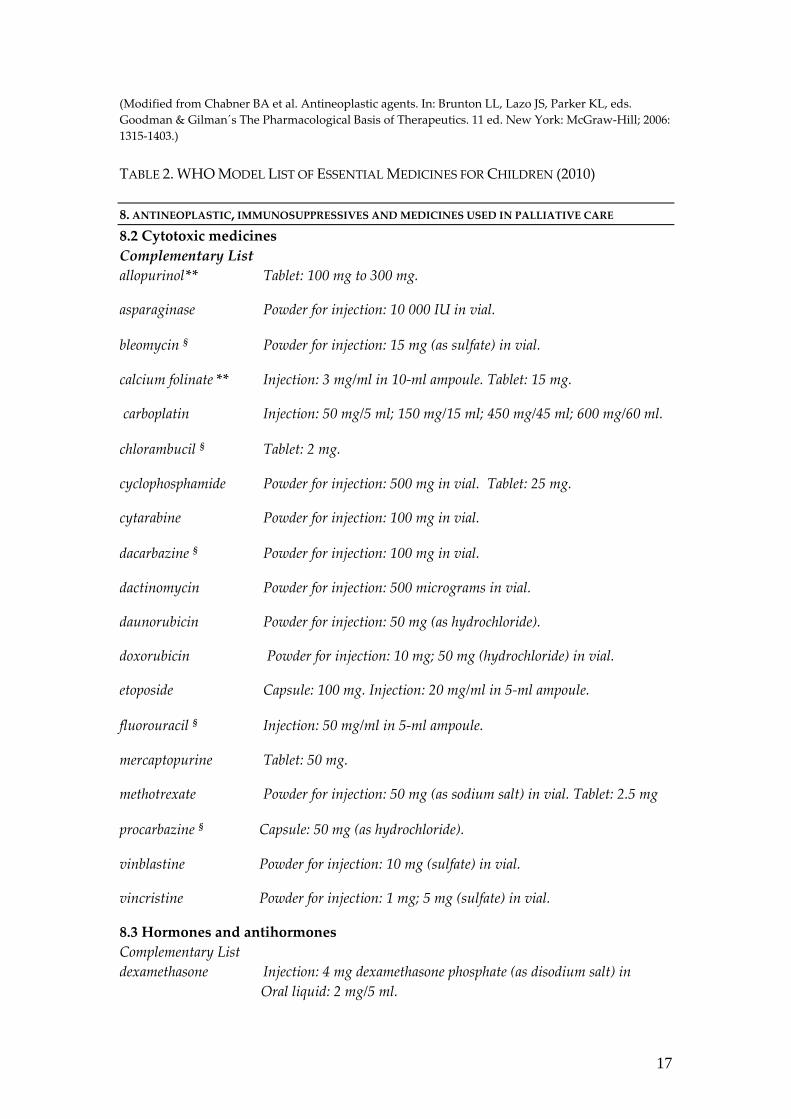
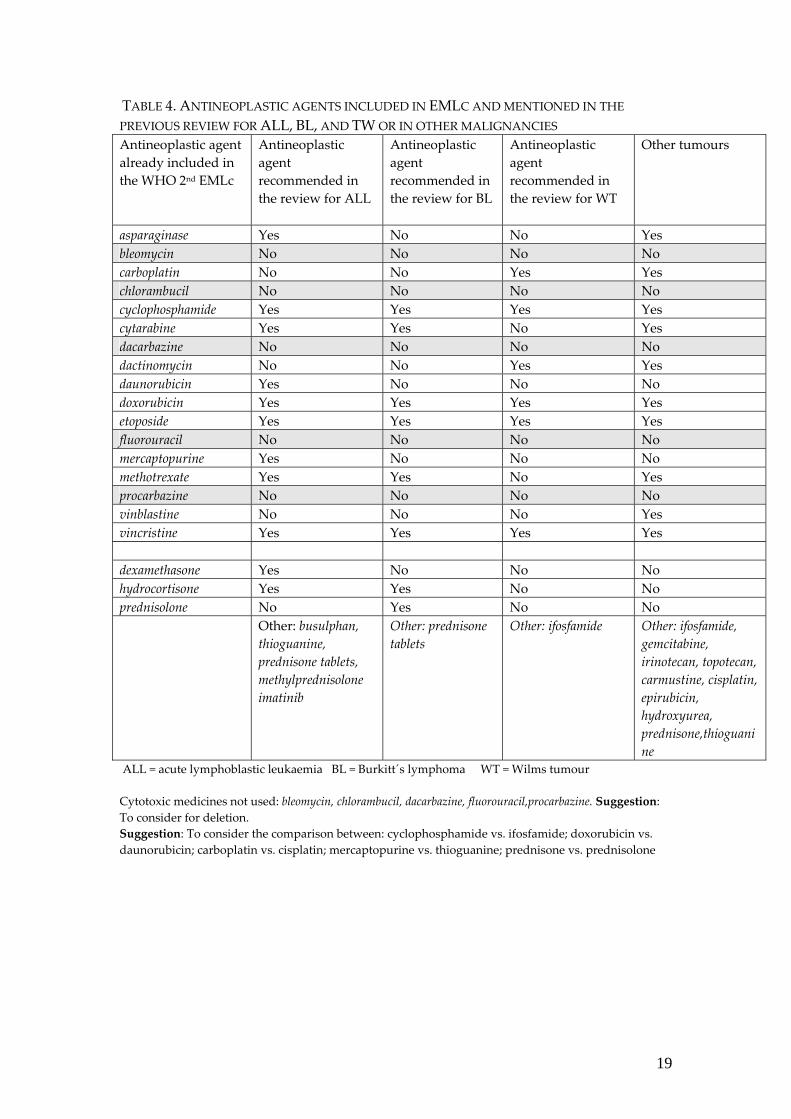
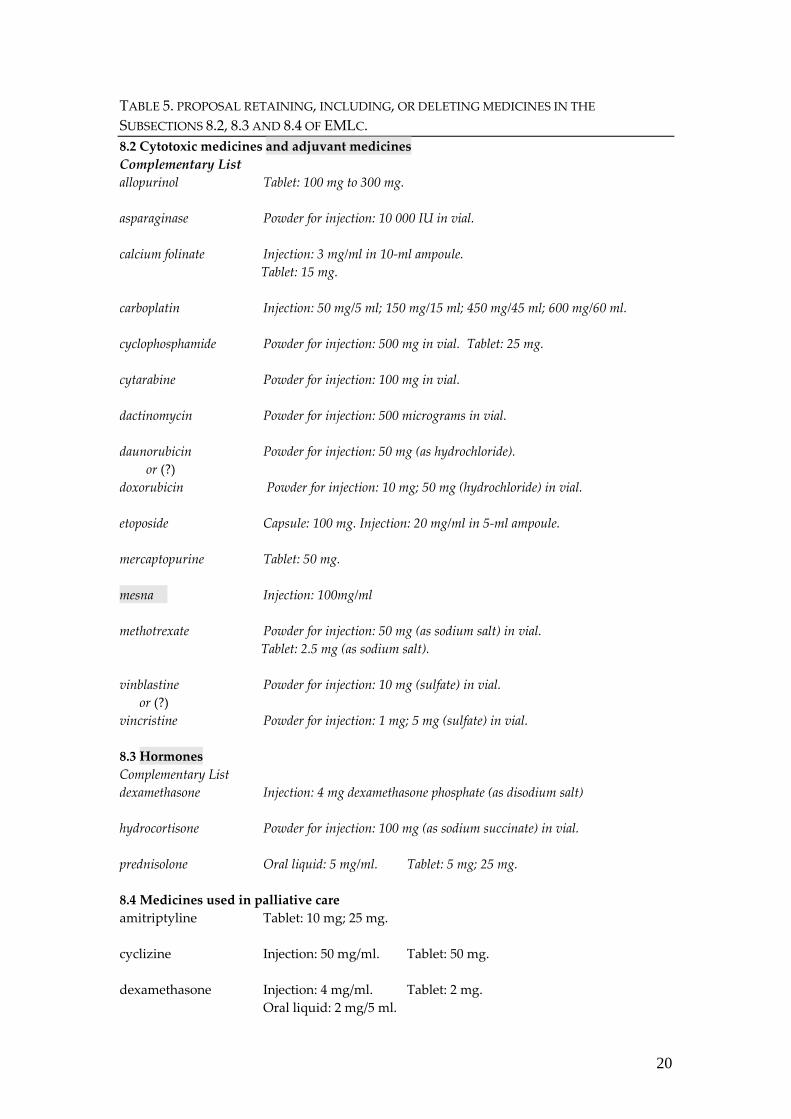
1. Table 1. Antineoplastic representatives in each pharmacological subclass; 33 cytotoxic medicines mentioned in the previous review; 13 cytotoxic medicines included in the EMLc. 2. Table 2. Subsections 8.2 and 8.3 in the EMLc (Updated 2010) 3. Table 3. List of recommended medicines by the Review of medicines for the treatment of common tumours in children. 4. Table 4. Antineoplastic medicines shared by the three childhood malignancies considered in the Review of medicines for the treatment of common tumours in children and in other cancer diseases found in the literature search (to see the prevalence of the current use). 5. Table 5. Proposal for retaining, including, deleting or modifying medicines in the Subsections 8.2, 8.3, and 8.4 of the EMLc.
16
TABLE 1. ANTINEOPLASTIC MEDICINES Akylating Agents Nitrogen mustards: cyclophosphamide,# ifosfamide,# chlorambucil, melphalan,* estramustine,
mechloretamine (ifosfamide is the most neurotoxic of this class of agents) Ethylenimines: thiotepa,* altretamine Alkil sulfonates: busulfan,* treosulfan Nitrosoureas: carmustine,* lomustine semustine, streptozocin Triazenes: dacarbazine,* temozolomide Methylhidrazine derivative: procarbazine Platinum complexes cisplatin,# carboplatin,# oxaliplatin (carboplatin is better tolerated clinically) Antimetabolites Folic acid analogs: methotrexate,# pemetrexed Pyrimidine analogs: 5‐fluorouracil, floxuridine, idoxuridine, capecitabine Cytidine analogs: cytarabine,# gemcitabine,* azacytidine, decitabine (gemcitabine is a potent radiosensitizer and should not be used with radiotherapy) Purine analogs and related inhibitors: 6‐mercaptopurine,# thioguanine (6‐TG),*
pentostatin, fludarabine, cladribine*, nelarabine, clofarabine* Natural products Topoisomerases I and II Inhibitors Camptothecins: topotecan,* irinotecan* Epipodophyllotoxins: etoposide,# teniposide* Intercalar agents Antibiotics: daunorubicin,# doxorubicin,# idarubicin,* valrubicin, epirubicin*
(anthracyclines), dactinomycin# Anthracenedione: mitoxantrone,* bleomycin,* mitomycin (mitoxantrone has significantly less cardiotoxicity than do the anthracyclines) Microtubule‐inativating agents Vinca alkaloids: vincristine,# vinblastine,* vindesine, vinorelbine (vincristine is the standard component of regimens for treating paediatric neoplasias) Taxanes: paclitaxel, docetaxel Epothilone: ixabepilone Miscellaneous agents Enzyme: L‐asparaginase# Differentiating agents: arsenic trioxide, tretinoin Substituted urea: Hydroxyurea* Thalidomide, lenalidomide Trabectedin Biological response modifiers Interferon‐alfa, interleukin 2 Hormones and antihormones Adrenocorticosteroids: prednisone,# prednisolone,# hydrocortisone,* dexamethazone,#
methyprednisolone* Underlined medicines: already included in the EMLc (Updated 2010). * Medicines mentioned for treatment of childhood malignancies. # The most cited medicines for treatment of childhood malignancies.
17
(Modified from Chabner BA et al. Antineoplastic agents. In: Brunton LL, Lazo JS, Parker KL, eds. Goodman & Gilman´s The Pharmacological Basis of Therapeutics. 11 ed. New York: McGraw‐Hill; 2006: 1315‐1403.) TABLE 2. WHO MODEL LIST OF ESSENTIAL MEDICINES FOR CHILDREN (2010) 8. ANTINEOPLASTIC, IMMUNOSUPPRESSIVES AND MEDICINES USED IN PALLIATIVE CARE 8.2 Cytotoxic medicines Complementary List allopurinol** Tablet: 100 mg to 300 mg.
asparaginase Powder for injection: 10 000 IU in vial.
bleomycin § Powder for injection: 15 mg (as sulfate) in vial.
calcium folinate ** Injection: 3 mg/ml in 10‐ml ampoule. Tablet: 15 mg.
carboplatin Injection: 50 mg/5 ml; 150 mg/15 ml; 450 mg/45 ml; 600 mg/60 ml.
chlorambucil § Tablet: 2 mg.
cyclophosphamide Powder for injection: 500 mg in vial. Tablet: 25 mg.
cytarabine Powder for injection: 100 mg in vial.
dacarbazine § Powder for injection: 100 mg in vial.
dactinomycin Powder for injection: 500 micrograms in vial.
daunorubicin Powder for injection: 50 mg (as hydrochloride).
doxorubicin Powder for injection: 10 mg; 50 mg (hydrochloride) in vial.
etoposide Capsule: 100 mg. Injection: 20 mg/ml in 5‐ml ampoule.
fluorouracil § Injection: 50 mg/ml in 5‐ml ampoule.
mercaptopurine Tablet: 50 mg.
methotrexate Powder for injection: 50 mg (as sodium salt) in vial. Tablet: 2.5 mg
procarbazine § Capsule: 50 mg (as hydrochloride).
vinblastine Powder for injection: 10 mg (sulfate) in vial.
vincristine Powder for injection: 1 mg; 5 mg (sulfate) in vial.
8.3 Hormones and antihormones Complementary List dexamethasone Injection: 4 mg dexamethasone phosphate (as disodium salt) in
Oral liquid: 2 mg/5 ml.

18
hydrocortisone Powder for injection: 100 mg (as sodium succinate) in vial.
Prednisolone Oral liquid: 5 mg/ml. Tablet: 5 mg; 25 mg. § Medicines (n=5) not mentioned in the collected references. ** No cytotoxic medicines. TABLE 3: LIST OF RECOMMENDED DRUGS BY THE REVIEW OF MEDICINES FOR THE TREATMENT OF COMMON TUMOURS IN CHILDREN. L. Asparaginase (E. coli) 10,000 IU vial. L. Asparaginase (PEG product) 3,750 IU/5ml vial. L. Asparaginase (Erwinia product) 10,000 IU vial. Busulphan 2mg tablets and 10ml vials (6mg/ml) Cyclophosphamide 1 and 2g vials. Cyclosporine 10, 25, 50 and 100mg capsules, oral solution 100mg/ml, injection 50mg/ml Cytosine arabinoside 100mg and 1g vials. Daunorubicin 20mg vial. Dexamethasone 0.5, 0.75, 2 and 4 mg tablets; multi‐dose(5ml‐4mg/ml)
and single dose (1ml‐10mg/ml) vials. Doxorubicin 10 and 50 mg vials. Etoposide 50mg capsules; 5, 25 and 50 mg multi‐dose vials Hydrocortisone 100mg. vial. Imatinib 100 and 400mg tablets. Leucovorin 5mg tablet, and 5 and 50ml. vials (10mg/ml) Mercaptopurine 50 mg tablet Methotrexate 2.5 and 10mg tablets;
1ml (10mg/ml) and 2, 10, 40, 100ml (25mg/ml) vials. Methylprednisolone 5ml (40 mg/ml) multidose and 1ml (40 and 80mg/ml)
single dose vials. Prednisone 1, 5 and 50 mg tablets. Thioguanine 40mg tablet. Vincristine 1, 2 and 5 ml vials (1mg/ml)
19
TABLE 4. ANTINEOPLASTIC AGENTS INCLUDED IN EMLC AND MENTIONED IN THE PREVIOUS REVIEW FOR ALL, BL, AND TW OR IN OTHER MALIGNANCIES Antineoplastic agent already included in the WHO 2nd EMLc
Antineoplastic agent recommended in the review for ALL
Antineoplastic agent recommended in the review for BL
Antineoplastic agent recommended in the review for WT
Other tumours
asparaginase Yes No No Yes bleomycin No No No No carboplatin No No Yes Yes chlorambucil No No No No cyclophosphamide Yes Yes Yes Yes cytarabine Yes Yes No Yes dacarbazine No No No No dactinomycin No No Yes Yes daunorubicin Yes No No No doxorubicin Yes Yes Yes Yes etoposide Yes Yes Yes Yes fluorouracil No No No No mercaptopurine Yes No No No methotrexate Yes Yes No Yes procarbazine No No No No vinblastine No No No Yes vincristine Yes Yes Yes Yes dexamethasone Yes No No No hydrocortisone Yes Yes No No prednisolone No Yes No No Other: busulphan,
thioguanine, prednisone tablets, methylprednisolone imatinib
Other: prednisone tablets
Other: ifosfamide Other: ifosfamide, gemcitabine, irinotecan, topotecan, carmustine, cisplatin, epirubicin, hydroxyurea, prednisone,thioguanine
ALL = acute lymphoblastic leukaemia BL = Burkitt´s lymphoma WT = Wilms tumour Cytotoxic medicines not used: bleomycin, chlorambucil, dacarbazine, fluorouracil,procarbazine. Suggestion: To consider for deletion. Suggestion: To consider the comparison between: cyclophosphamide vs. ifosfamide; doxorubicin vs. daunorubicin; carboplatin vs. cisplatin; mercaptopurine vs. thioguanine; prednisone vs. prednisolone
20
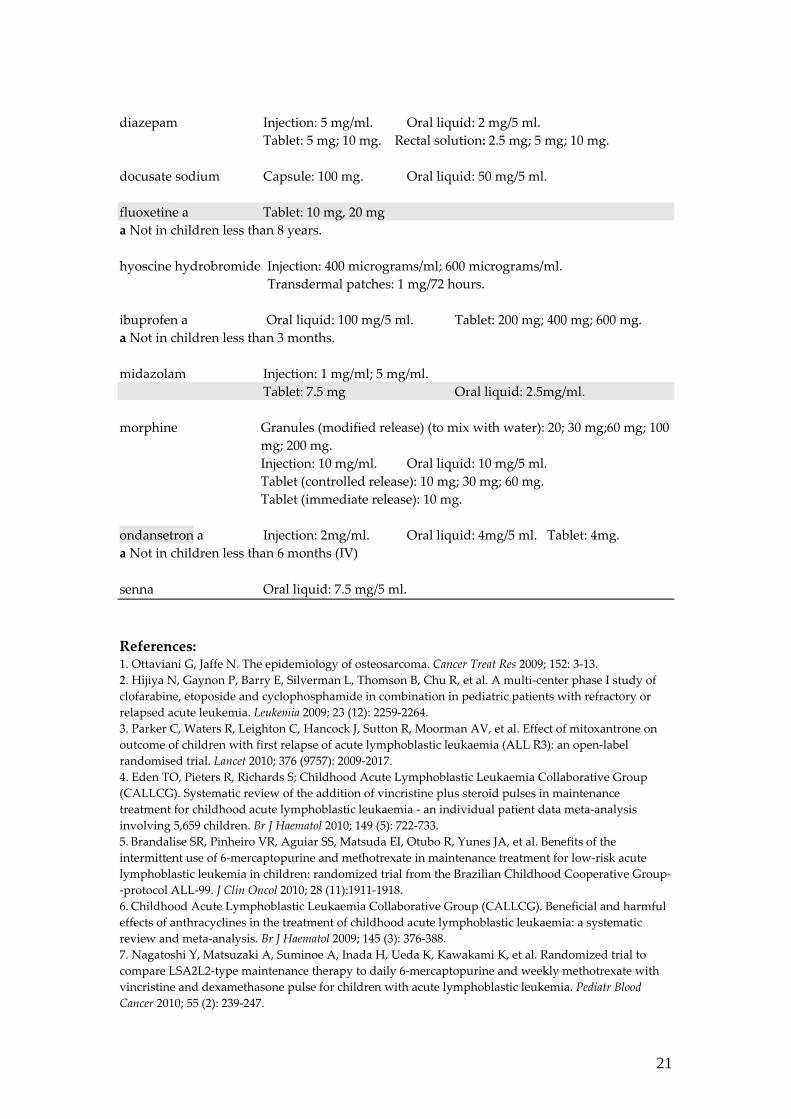
TABLE 5. PROPOSAL RETAINING, INCLUDING, OR DELETING MEDICINES IN THE SUBSECTIONS 8.2, 8.3 AND 8.4 OF EMLC. 8.2 Cytotoxic medicines and adjuvant medicines Complementary List allopurinol Tablet: 100 mg to 300 mg. asparaginase Powder for injection: 10 000 IU in vial. calcium folinate Injection: 3 mg/ml in 10‐ml ampoule.
Tablet: 15 mg. carboplatin Injection: 50 mg/5 ml; 150 mg/15 ml; 450 mg/45 ml; 600 mg/60 ml. cyclophosphamide Powder for injection: 500 mg in vial. Tablet: 25 mg. cytarabine Powder for injection: 100 mg in vial. dactinomycin Powder for injection: 500 micrograms in vial. daunorubicin Powder for injection: 50 mg (as hydrochloride). or (?) doxorubicin Powder for injection: 10 mg; 50 mg (hydrochloride) in vial. etoposide Capsule: 100 mg. Injection: 20 mg/ml in 5‐ml ampoule. mercaptopurine Tablet: 50 mg. mesna Injection: 100mg/ml methotrexate Powder for injection: 50 mg (as sodium salt) in vial.
Tablet: 2.5 mg (as sodium salt). vinblastine Powder for injection: 10 mg (sulfate) in vial. or (?) vincristine Powder for injection: 1 mg; 5 mg (sulfate) in vial. 8.3 Hormones Complementary List dexamethasone Injection: 4 mg dexamethasone phosphate (as disodium salt) hydrocortisone Powder for injection: 100 mg (as sodium succinate) in vial. prednisolone Oral liquid: 5 mg/ml. Tablet: 5 mg; 25 mg. 8.4 Medicines used in palliative care amitriptyline Tablet: 10 mg; 25 mg. cyclizine Injection: 50 mg/ml. Tablet: 50 mg. dexamethasone Injection: 4 mg/ml. Tablet: 2 mg.
Oral liquid: 2 mg/5 ml.
21
diazepam Injection: 5 mg/ml. Oral liquid: 2 mg/5 ml. Tablet: 5 mg; 10 mg. Rectal solution: 2.5 mg; 5 mg; 10 mg. docusate sodium Capsule: 100 mg. Oral liquid: 50 mg/5 ml. fluoxetine a Tablet: 10 mg, 20 mg a Not in children less than 8 years. hyoscine hydrobromide Injection: 400 micrograms/ml; 600 micrograms/ml.
Transdermal patches: 1 mg/72 hours. ibuprofen a Oral liquid: 100 mg/5 ml. Tablet: 200 mg; 400 mg; 600 mg. a Not in children less than 3 months. midazolam Injection: 1 mg/ml; 5 mg/ml. Tablet: 7.5 mg Oral liquid: 2.5mg/ml. morphine Granules (modified release) (to mix with water): 20; 30 mg;60 mg; 100
mg; 200 mg. Injection: 10 mg/ml. Oral liquid: 10 mg/5 ml. Tablet (controlled release): 10 mg; 30 mg; 60 mg. Tablet (immediate release): 10 mg.
ondansetron a Injection: 2mg/ml. Oral liquid: 4mg/5 ml. Tablet: 4mg. a Not in children less than 6 months (IV) senna Oral liquid: 7.5 mg/5 ml. References: 1. Ottaviani G, Jaffe N. The epidemiology of osteosarcoma. Cancer Treat Res 2009; 152: 3‐13. 2. Hijiya N, Gaynon P, Barry E, Silverman L, Thomson B, Chu R, et al. A multi‐center phase I study of clofarabine, etoposide and cyclophosphamide in combination in pediatric patients with refractory or relapsed acute leukemia. Leukemia 2009; 23 (12): 2259‐2264. 3. Parker C, Waters R, Leighton C, Hancock J, Sutton R, Moorman AV, et al. Effect of mitoxantrone on outcome of children with first relapse of acute lymphoblastic leukaemia (ALL R3): an open‐label randomised trial. Lancet 2010; 376 (9757): 2009‐2017. 4. Eden TO, Pieters R, Richards S; Childhood Acute Lymphoblastic Leukaemia Collaborative Group (CALLCG). Systematic review of the addition of vincristine plus steroid pulses in maintenance treatment for childhood acute lymphoblastic leukaemia ‐ an individual patient data meta‐analysis involving 5,659 children. Br J Haematol 2010; 149 (5): 722‐733. 5. Brandalise SR, Pinheiro VR, Aguiar SS, Matsuda EI, Otubo R, Yunes JA, et al. Benefits of the intermittent use of 6‐mercaptopurine and methotrexate in maintenance treatment for low‐risk acute lymphoblastic leukemia in children: randomized trial from the Brazilian Childhood Cooperative Group‐‐protocol ALL‐99. J Clin Oncol 2010; 28 (11):1911‐1918. 6. Childhood Acute Lymphoblastic Leukaemia Collaborative Group (CALLCG). Beneficial and harmful effects of anthracyclines in the treatment of childhood acute lymphoblastic leukaemia: a systematic review and meta‐analysis. Br J Haematol 2009; 145 (3): 376‐388. 7. Nagatoshi Y, Matsuzaki A, Suminoe A, Inada H, Ueda K, Kawakami K, et al. Randomized trial to compare LSA2L2‐type maintenance therapy to daily 6‐mercaptopurine and weekly methotrexate with vincristine and dexamethasone pulse for children with acute lymphoblastic leukemia. Pediatr Blood Cancer 2010; 55 (2): 239‐247.

22
8. Stork LC, Matloub Y, Broxson E, La M, Yanofsky R, Sather H, Hutchinson R, Heerema NA, Sorrell AD, Masterson M, Bleyer A, Gaynon PS. Oral 6‐mercaptopurine versus oral 6‐thioguanine and veno‐occlusive disease in children with standard‐risk acute lymphoblastic leukemia: report of the Childrenʹs Oncology Group CCG‐1952 clinical trial. Blood 2010; 115(14):2740‐2748. 9. van Dalen EC, Raphaël MF, Caron HN, Kremer LCM. Treatment including anthracyclines versus treatment not including anthracyclines for childhood cancer. Cochrane Database of Systematic Reviews. In: The Cochrane Library, Issue 12, 2010. Art. No. CD006647. 10. van Dalen EC, Michiels EMC, Caron HN, Kremer LCM. Different anthracycline derivates for reducing cardiotoxicity in cancer patients. Cochrane Database of Systematic Reviews. In:The Cochrane Library, Issue 12, 2010. Art. No. CD005006. 11. Bostrom BC, Sensel MR, Sather HN, et al. Dexamethasone versus prednisone and daily oral versus weekly intravenous mercaptopurine for patients with standard‐risk acute lymphoblastic leukaemia: a report from the Children’s Cancer Group. Blood 2003; 101: 3809‐3817. 12. Schimmer BP, Parker KL. Adrenocorticotropic hormone; adrenocortical steroids and their synthetic analogs; inhibitors of the synthesis and actions of adrenocortical hormones. In: Hardman JG, Limbird LE, Gilman AG, eds. Goodman & Gilmanʹs the pharmacological basis of therapeutics. 11 ed. New York: McGraw‐Hill; 2006:1587‐1612. 13. Rubnitz JE, Inaba H, Dahl G, Ribeiro RC, Bowman WP, Taub J, et al. Minimal residual disease‐directed therapy for childhood acute myeloid leukaemia: results of the AML02 multicentre trial. Lancet Oncol 2010; 11(6): 543‐552. 14. Rubnitz JE, Crews KR, Pounds S, Yang S, Campana D, Gandhi VV, et al. Combination of cladribine and cytarabine is effective for childhood acute myeloid leukemia: results of the St Jude AML97 trial. Leukemia 2009; 23(8):1410‐1416. 15. Foreman NK, Schissel D, Le T, Strain J, Fleitz J, Quinones R, Giller R. A study of sequential high dose cyclophosphamide and high dose carboplatin with peripheral stem‐cell rescue in resistant or recurrent pediatric brain tumors. J Neurooncol 2005; 71(2):181‐187. 16. Minturn JE, Janss AJ, Fisher PG, Allen JC, Patti R, Phillips PC, Belasco JB. A phase II study of metronomic oral topotecan for recurrent childhood brain tumors. Pediatr Blood Cancer 2011; 56 (1): 39‐44. 17. Schor NF. New approaches to pharmacotherapy of tumors of the nervous system during childhood and adolescence. Pharmacol Ther 2009l; 122 (1): 44–55. 18. Pearson AD, Pinkerton CR, Lewis IJ, Imeson J, Ellershaw C, Machin D; European Neuroblastoma Study Group; Childrenʹs Cancer and Leukaemia Group (CCLG formerly United Kingdom Childrenʹs Cancer Study Group). High‐dose rapid and standard induction chemotherapy for patients aged over 1 year with stage 4 neuroblastoma: a randomised trial. Lancet Oncol 2008; 9 (3):247‐256. 19. Dhall G, Grodman H, Ji L, Sands S, Gardner S, Dunkel IJ, McCowage GB, et al. Outcome of children less than three years old at diagnosis with non‐metastatic medulloblastoma treated with chemotherapy on the ʺHead Startʺ I and II protocols. Pediatr Blood Cancer 2008; 50(6): 1169‐1175. 20. Le Deley MC, Rosolen A, Williams DM, Horibe K, Wrobel G, Attarbaschi A, et al. Vinblastine in children and adolescents with high‐risk anaplastic large‐cell lymphoma: results of the randomized ALCL99‐vinblastine trial. J Clin Oncol 2010; 28 (25): 3987‐3993. 21. Traoré F, Coze C, Atteby JJ, André N, Moreira C, Doumbe P, Ravelomanana N, Ye D, Patte C, Raquin MA, Raphael M, Lemerle J. Cyclophosphamide monotherapy in children with Burkitt lymphoma: a study from the French‐African Pediatric Oncology Group (GFAOP). Pediatr Blood Cancer 2011; 56(1): 70‐76. 22. Hesseling PB, Molyneux E, Tchintseme F, Welbeck J, McCormick P, Pritchard‐Jones K, et al. Treating Burkittʹs lymphoma in Malawi, Cameroon, and Ghana. Lancet Oncol 2008; 9: 512‐513. 23. Okebe JU, Lasserson TJ, Meremikwu MM, Richards S. Therapeutic interventions for Burkittʹs lymphoma in children. Cochrane Database of Systematic Reviews. In: The Cochrane Library,Issue 12, 2010. Art. No. CD005198. 24. Gerrard M, Cairo MS, Weston C, Auperin A, Pinkerton R, Lambilliote A, et al.; FAB LMB96 International Study Committee. Excellent survival following two courses of COPAD chemotherapy in children and adolescents with resected localized B‐cell non‐Hodgkinʹs lymphoma: results of the FAB/LMB 96 international study. Br J Haematol 2008; 141 (6): 840‐847. 25. Wu HY, Snyder HM 3rd, DʹAngio GJ. Wilmsʹ tumor management. Curr Opin Urol 2005; 15 (4): 273‐276.
23
26. Abu‐Ghosh AM, Krailo MD, Goldman SC, Slack RS, Davenport V, Morris E, et al. Ifosfamide, carboplatin and etoposide in children with poor‐risk relapsed Wilmsʹ tumor: a Childrenʹs Cancer Group report. Ann Oncol 2002; 13:460‐469. 27. Mascarenhas L, Lyden ER, Breitfeld PP, Walterhouse DO, Donaldson SS, Paidas CN, et al. Randomized phase II window trial of two schedules of irinotecan with vincristine in patients with first relapse or progression of rhabdomyosarcoma: a report from the Childrenʹs Oncology Group. J Clin Oncol 2010; 28 (30): 4658‐4663. 28. McDowell HP, Foot AB, Ellershaw C, Machin D, Giraud C, Bergeron C. Outcomes in paediatric metastatic rhabdomyosarcoma: results of The International Society of Paediatric Oncology (SIOP) study MMT‐98. Eur J Cancer 2010; 46(9):1588‐1595. 29. Arndt CA, Stoner JA, Hawkins DS, Rodeberg DA, Hayes‐Jordan AA, Paidas CN, et al. Vincristine, actinomycin, and cyclophosphamide compared with vincristine, actinomycin, and cyclophosphamide alternating with vincristine, topotecan, and cyclophosphamide for intermediate‐risk rhabdomyosarcoma: childrenʹs oncology group study D9803. J Clin Oncol 2009; 27(31): 5182‐5188. 30. Dantonello TM, Int‐Veen C, Harms D, Leuschner I, Schmidt BF, Herbst M, et al. Cooperative trial CWS‐91 for localized soft tissue sarcoma in children, adolescents, and young adults. J Clin Oncol 2009; 27(9):1446‐1455. 31. Admiraal R, van der Paardt M, Kobes J, Kremer LCM, Bisogno G, Merks JHM. High‐dose chemotherapy for children and young adults with stage IV rhabdomyosarcoma. Cochrane Database of Systematic Reviews. In: The Cochrane Library, Issue 12, 2010. Art. No. CD006669. 32. Zak D, Styler MJ, Rosenbluth JZ, Brodsky I.Combination of gemcitabine and irinotecan for recurrent metastatic osteogenic sarcoma. Clin Adv Hematol Oncol 2005; 3(4): 297‐299. 33. Ayan I, Kebudi R, Ozger H. Childhood osteosarcoma: multimodal therapy in a single‐institution Turkish series. Cancer Treat Res 2009; 152: 319‐338. 34. Huang M, Lucas K. Current Therapeutic Approaches in Metastatic and Recurrent Ewing Sarcoma. Sarcoma 2011; 2011: 863210. 35. Paulussen M, Craft AW, Lewis I, Hackshaw A, Douglas C, Dunst J, et al.; European Intergroup Cooperative Ewingʹs Sarcoma Study‐92. Results of the EICESS‐92 Study: two randomized trials of Ewingʹs sarcoma treatment‐‐cyclophosphamide compared with ifosfamide in standard‐risk patients and assessment of benefit of etoposide added to standard treatment in high‐risk patients. J Clin Oncol 2008; 26(27): 4385‐4393. 36. Granowetter L, Womer R, Devidas M, Krailo M, Wang C, Bernstein M, et al. Dose‐intensified compared with standard chemotherapy for nonmetastatic Ewing sarcoma family of tumors: a Childrenʹs Oncology Group Study. J Clin Oncol 2009; 27(15): 2536‐2541. 37. Mulder RL, Paulides M, Langer T, Kremer LC, van Dalen EC. Cyclophosphamide versus ifosfamide for paediatric and young adult bone and soft tissue sarcoma patients. Cochrane Database Syst Rev 2010 Feb 17; (2):CD006300. 38. Cheuk Daniel KL, Chiang Alan KS, Chan Godfrey CF, Ha Shau Yin. Urate oxidase for the prevention and treatment of tumor lysis syndrome in children with cancer. Cochrane Database of Systematic Reviews. In: The Cochrane Library, Issue 12, 2010. Art. No. CD006945. 39. Anderson P. Continuously improving ifosfamide/mesna: a winning combination. Pediatr Blood Cancer 2010; 55 (4): 599‐600. 40. Lipshultz SE, Scully RE, Lipsitz SR, Sallan SE, Silverman LB, Miller TL, et al. Assessment of dexrazoxane as a cardioprotectant in doxorubicin‐treated children with high‐risk acute lymphoblastic leukaemia: long‐term follow‐up of a prospective, randomised, multicentre trial. Lancet Oncol 2010; 11(10): 950‐961. 41. Mokhtar GM, Shaaban SY, Elbarbary NS, Fayed WA. A trial to assess the efficacy of glutamic acid in prevention of vincristine‐induced neurotoxicity in pediatric malignancies: a pilot study. J Pediatr Hematol Oncol 2010; 32 (8): 594‐600. 42. Sasse EC, Sasse AD, Brandalise SR, Clark OAC, Richards S. Colony‐stimulating factors for prevention of myelosuppressive therapy‐induced febrile neutropenia in children with acute lymphoblastic leukaemia. Cochrane Database of Systematic Reviews. In: The Cochrane Library, Issue 12, 2010. Art. No. CD004139. 43. Wannmacher L. Palliative Medicine: medicines and care. In: Farmacoterapia baseada em evidências. Temas Selecionados. V. 5, N. 1. Brasília: OPAS; December 2007. [www.opas.org.br/medicamentos/temas] 44. World Health Organization. WHO Model Formulary for Children 2010. Based on the second model list of essential medicines for children 2009. Geneva: WHO; 2010.

24
45. Lorenz KA, Lynn J, Dy SM, Shugarman LR, Wilkinson A, Mularski RA, et al. Evidence for Improving Palliative Care at the End of Life: A Systematic Review. Ann Intern Med 2008; 148: 147‐159. 46. WHOʹs pain ladder. Available in: http://www.who.int/cancer/palliative/painladder/en/index.html [Acessed in: 11.02.2011] 47. Radbruch L, Strasser F, Elsner F, Gonçalves JF, Løge J, Kaasa S, et al.; Research Steering Committee of the European Association for Palliative Care (EAPC). Fatigue in palliative care patients ‐‐ an EAPC approach. Palliat Med 2008; 22(1):13‐32. 48. Phillips RS, Gopaul S, Gibson F, Houghton E, Craig JV, Light K, Pizer B. Antiemetic medication for prevention and treatment of chemotherapy induced nausea and vomiting in childhood. Cochrane Database of Systematic Reviews. In: The Cochrane Library, Issue 12, 2010. Art. No. CD007786. 49. Nagel K, Willan AR, Lappan J, Korz L, Buckley N, Barr RD. Pediatric oncology sedation trial (POST): A double‐blind randomized study. Pediatr Blood Cancer 2008; 51(5): 634‐638. 50. Gan TJ, Sinha AC, Kovac AL, Jones RK, Cohen SA, Battikha JP, et al. for the TDS Study Group. A randomized, double‐blind, multicenter trial comparing transdermal scopolamine plus ondansetron to ondansetron alone for the prevention of postoperative nausea and vomiting in the outpatient setting. Anesth Analg 2009; 108: 1498‐1504. 51. Spinks A, Wasiak J, Villanueva E, Bernath V. Scopolamine (hyoscine) for preventing and treating motion sickness. Cochrane Database of Systematic Reviews. In: The Cochrane Library, Issue 3, Art. No. CD002851. 52. Bridge JA, Iyengar S, Salary CB, Barbe RP, Birmaher B, Pincus HA, Ren L, Brent DA. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta‐analysis of randomized controlled trials. JAMA 2007; 297: 1683‐1696. 53. Hetrick SE, Merry SN, McKenzie J, Sindahl P, Proctor M. Selective serotonin reuptake inhibitors (SSRIs) for depressive disorders in children and adolescents. Cochrane Database of Systematic Reviews. In: The Cochrane Library, Issue 12, 2010. Art. No. CD004851. 54. Hedén L, von Essen L, Frykholm P, Ljungman G. Low‐dose oral midazolam reduces fear and distress during needle procedures in children with cancer. Pediatr Blood Cancer 2009; 53(7):1200‐1204. 55. Price KJ, Elliott TM. Stimulant laxatives for constipation and soiling in children. Cochrane Database of Systematic Reviews. In: The Cochrane Library, Issue 12, 2010. Art. No. CD002040. 56. Candy D, Belsey J. Macrogol (polyethylene glycol) laxatives in children with functional constipation and faecal impaction: a systematic review. Arch Dis Child 2009; 94 (2): 156‐160. 57. Lee‐Robichaud H, Thomas K, Morgan J, Nelson RL. Lactulose versus Polyethylene Glycol for Chronic Constipation. Cochrane Database Syst Rev 2010 Jul 7; (7):CD007570. 58. Myra Woolery M, Bisanz A, Lyons HL, Gaido L, Yenulevich M, Fulton S, McMillan SC. Putting Evidence Into Practice: Evidence‐Based Interventions for the Prevention and Management of Constipation in Patients With Cancer. Clinical Journal of Oncology Nursing 2008; 12 (2): 317‐333.57. 59. Agra Y, Sacristan A, Gonzalez M, Ferrari M, Portugues A, Calvo MJ. Efficacy of senna versus lactulose in terminal cancer patients treated with opioids. Journal of Pain and Symptom Management 1998; 15 (1): 1–7. 60. Tremont‐Lukats IW, Ratilal BO, Armstrong T, Gilbert MR. Antiepileptic drugs for preventing seizures in people with brain tumors. Cochrane Database of Systematic Reviews. In: The Cochrane Library, Issue 12, 2010. Art. No. CD004424.