
17/10/16 · terapie per l’epa*te C nei ... Life Expectancy in Patients With Chronic HCV Infection...
30
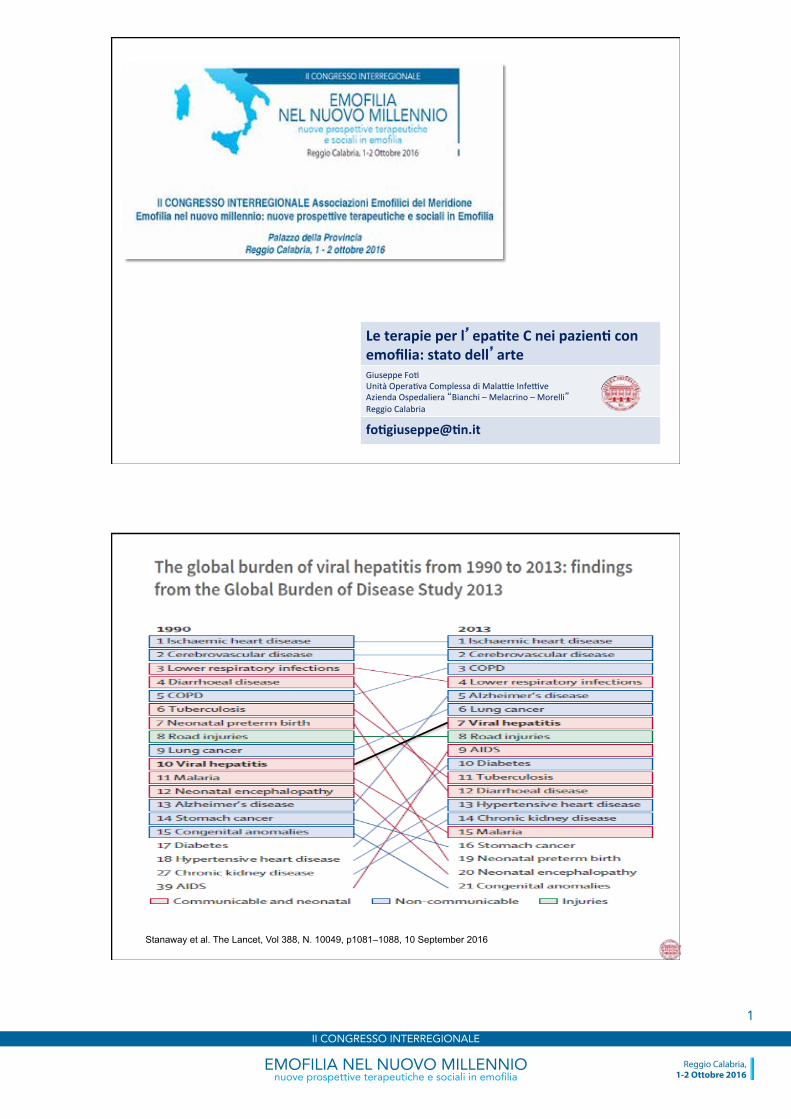
Le terapie per l’ epa*te C nei pazien* con emofilia: stato dell’ arte Giuseppe Fo/ Unità Opera/va Complessa di Mala=e Infe=ve Azienda Ospedaliera “Bianchi – Melacrino – Morelli” Reggio Calabria fo*giuseppe@*n.it Stanaway et al. The Lancet, Vol 388, N. 10049, p1081–1088, 10 September 2016 EMOFILIA NEL NUOVO MILLENNIO nuove prospettive terapeutiche e sociali in emofilia Reggio Calabria, 1-2 Ottobre 2016 II CONGRESSO INTERREGIONALE 1
Transcript of 17/10/16 · terapie per l’epa*te C nei ... Life Expectancy in Patients With Chronic HCV Infection...
17/10/16
1
Le terapie per l’epa*te C nei pazien* con emofilia: stato dell’arte Giuseppe Fo/ Unità Opera/va Complessa di Mala=e Infe=ve Azienda Ospedaliera “Bianchi – Melacrino – Morelli” Reggio Calabria
fo*giuseppe@*n.it
Stanaway et al. The Lancet, Vol 388, N. 10049, p1081–1088, 10 September 2016
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
1
17/10/16
2
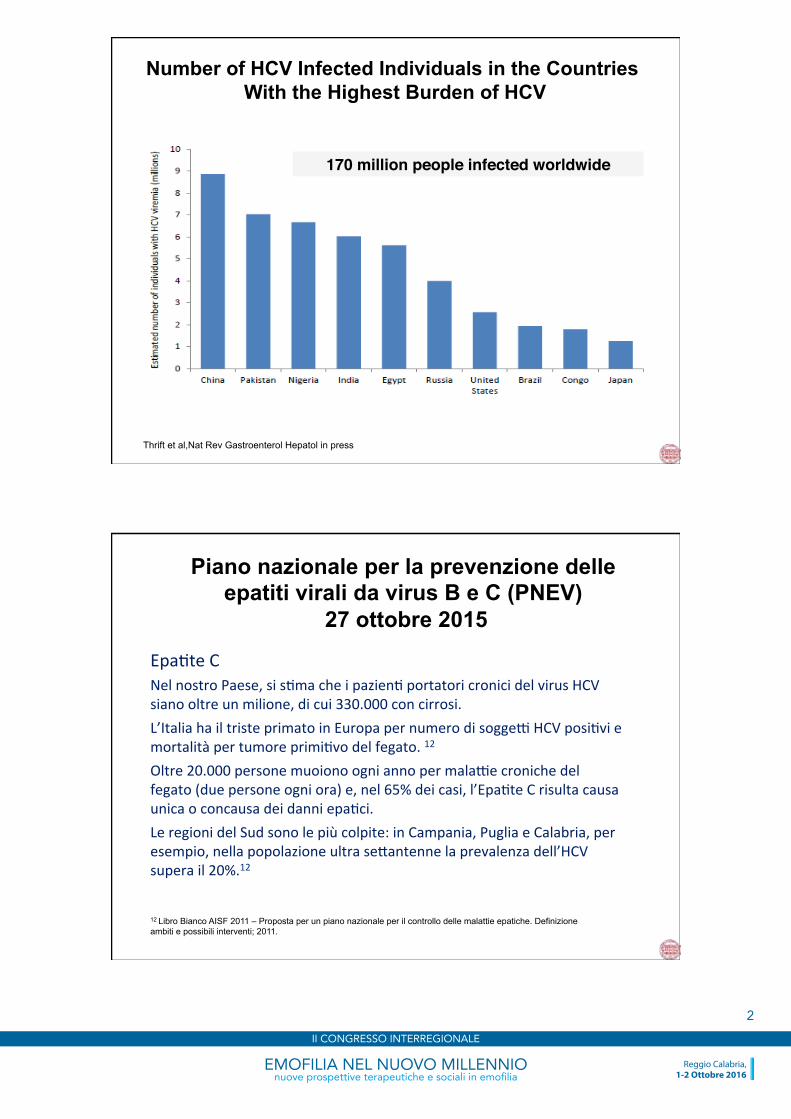
Number of HCV Infected Individuals in the Countries With the Highest Burden of HCV
Thrift et al,Nat Rev Gastroenterol Hepatol in press
170 million people infected worldwide
Piano nazionale per la prevenzione delle epatiti virali da virus B e C (PNEV)
27 ottobre 2015
Epa/te C Nel nostro Paese, si s/ma che i pazien/ portatori cronici del virus HCV siano oltre un milione, di cui 330.000 con cirrosi. L’Italia ha il triste primato in Europa per numero di sogge= HCV posi/vi e mortalità per tumore primi/vo del fegato. 12 Oltre 20.000 persone muoiono ogni anno per mala=e croniche del fegato (due persone ogni ora) e, nel 65% dei casi, l’Epa/te C risulta causa unica o concausa dei danni epa/ci. Le regioni del Sud sono le più colpite: in Campania, Puglia e Calabria, per esempio, nella popolazione ultra se[antenne la prevalenza dell’HCV supera il 20%.12
12 Libro Bianco AISF 2011 – Proposta per un piano nazionale per il controllo delle malattie epatiche. Definizione ambiti e possibili interventi; 2011.
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
2
17/10/16
3
• The goal of therapy is to cure HCV infec/on to prevent hepa/c cirrhosis, decompensa/on of cirrhosis, HCC, severe extrahepa/c manifesta/ons and death (A1).
• The endpoint of therapy is undetectable HCV RNA in blood by a sensi/ve assay (lower limit of detec/on ≤15 IU/ml) 12 weeks (SVR12) and/or 24 weeks (SVR24) ader the end of treatment (A1).
HCV - Therapy
SVR Susteined
Virological
Response
EASL Recommenda/ons on Treatment of Hepa//s C 2016
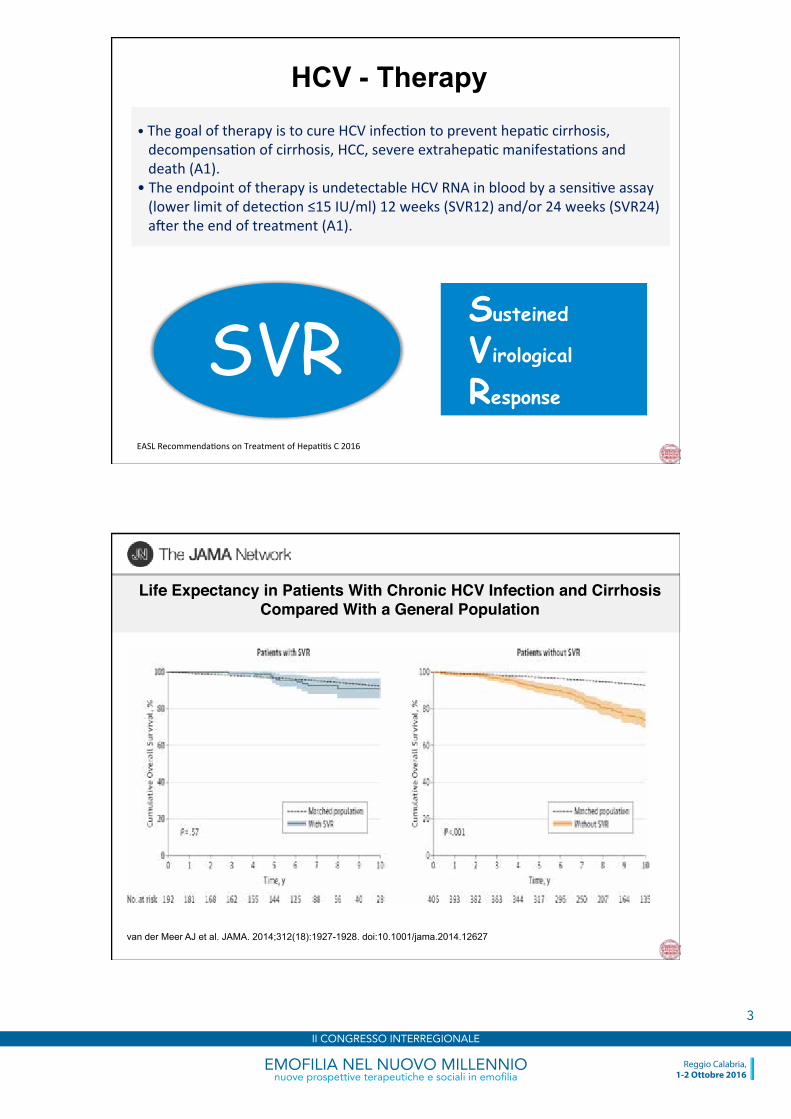
Life Expectancy in Patients With Chronic HCV Infection and Cirrhosis Compared With a General Population
van der Meer AJ et al. JAMA. 2014;312(18):1927-1928. doi:10.1001/jama.2014.12627
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
3
17/10/16
4
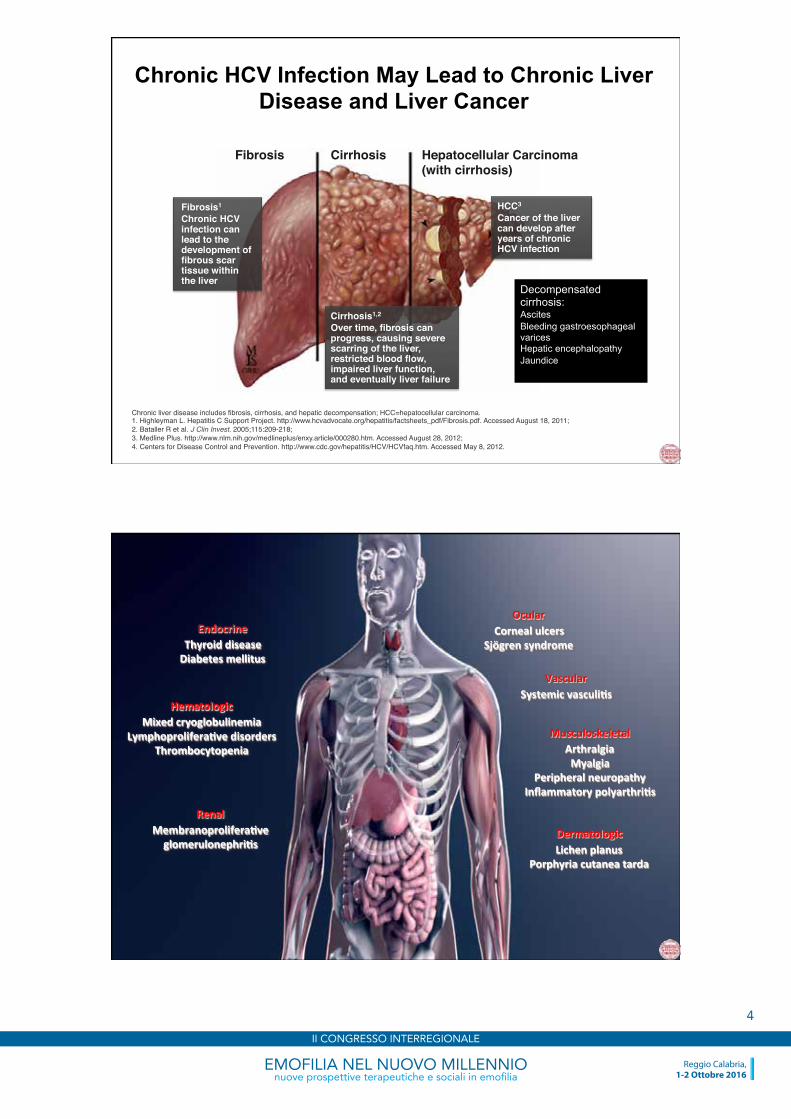
Chronic HCV Infection May Lead to Chronic Liver Disease and Liver Cancer
Fibrosis1
Chronic HCV infection can lead to the development of fibrous scar tissue within the liver
Fibrosis Cirrhosis Hepatocellular Carcinoma (with cirrhosis)
Cirrhosis1,2
Over time, fibrosis can progress, causing severe scarring of the liver, restricted blood flow, impaired liver function, and eventually liver failure
HCC3
Cancer of the liver can develop after years of chronic HCV infection
Chronic liver disease includes fibrosis, cirrhosis, and hepatic decompensation; HCC=hepatocellular carcinoma.1. Highleyman L. Hepatitis C Support Project. http://www.hcvadvocate.org/hepatitis/factsheets_pdf/Fibrosis.pdf. Accessed August 18, 2011; 2. Bataller R et al. J Clin Invest. 2005;115:209-218; 3. Medline Plus. http://www.nlm.nih.gov/medlineplus/enxy.article/000280.htm. Accessed August 28, 2012; 4. Centers for Disease Control and Prevention. http://www.cdc.gov/hepatitis/HCV/HCVfaq.htm. Accessed May 8, 2012.
Decompensated cirrhosis: Ascites Bleeding gastroesophageal varices Hepatic encephalopathy Jaundice
7
Endocrine Thyroid disease Diabetes mellitus
Hematologic Mixed cryoglobulinemia
Lymphoprolifera*ve disorders Thrombocytopenia
Renal Membranoprolifera*ve glomerulonephri*s
Ocular Corneal ulcers
Sjögren syndrome
Vascular Systemic vasculi*s
Dermatologic Lichen planus
Porphyria cutanea tarda
Musculoskeletal Arthralgia Myalgia
Peripheral neuropathy Inflammatory polyarthri*s
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
4
17/10/16
5
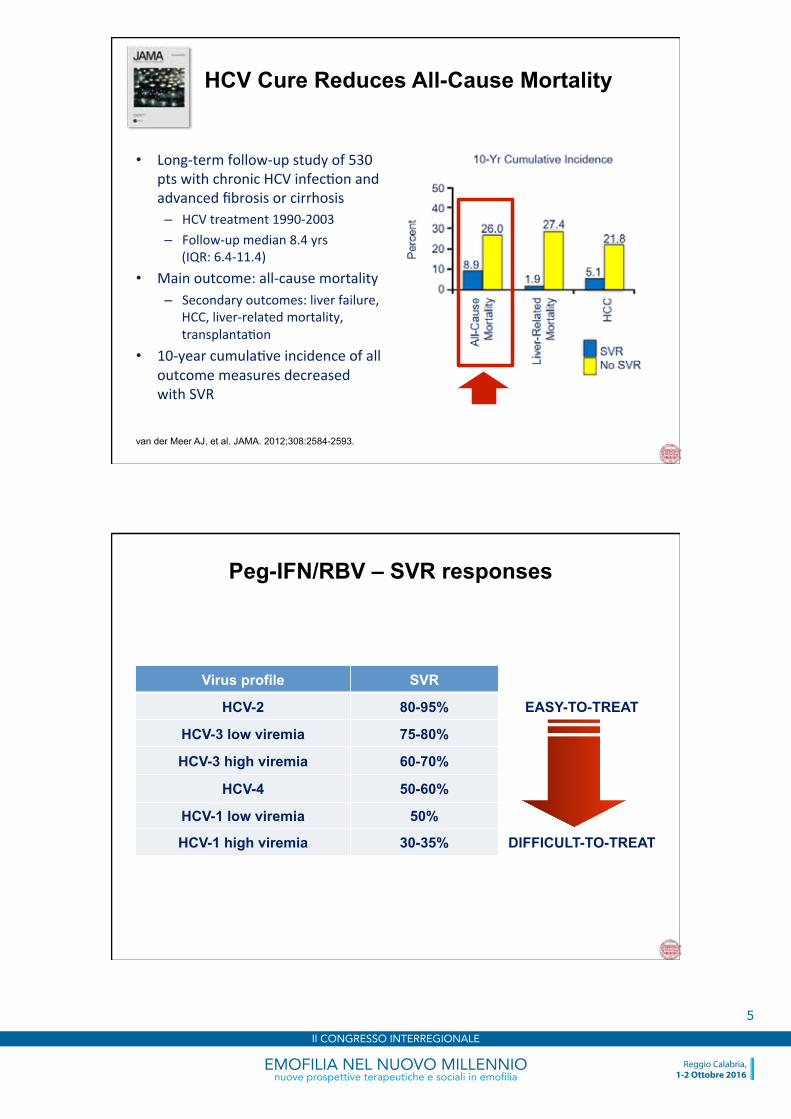
HCV Cure Reduces All-Cause Mortality
• Long-‐term follow-‐up study of 530 pts with chronic HCV infec/on and advanced fibrosis or cirrhosis – HCV treatment 1990-‐2003 – Follow-‐up median 8.4 yrs
(IQR: 6.4-‐11.4) • Main outcome: all-‐cause mortality
– Secondary outcomes: liver failure, HCC, liver-‐related mortality, transplanta/on
• 10-‐year cumula/ve incidence of all outcome measures decreased with SVR
van der Meer AJ, et al. JAMA. 2012;308:2584-2593.
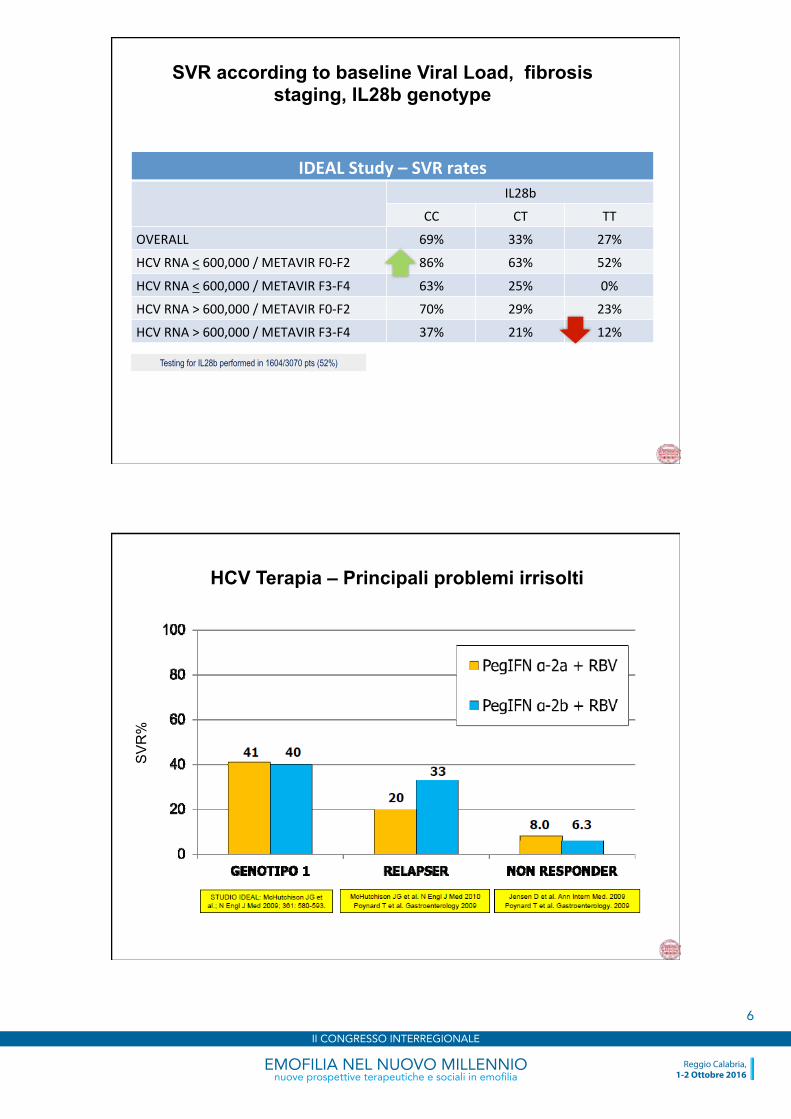
Virus profile SVR
HCV-2 80-95% EASY-TO-TREAT
HCV-3 low viremia 75-80%
HCV-3 high viremia 60-70%
HCV-4 50-60%
HCV-1 low viremia 50%
HCV-1 high viremia 30-35% DIFFICULT-TO-TREAT
Peg-IFN/RBV – SVR responses
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
5
17/10/16
6
SVR according to baseline Viral Load, fibrosis staging, IL28b genotype
IDEAL Study – SVR rates IL28b
CC CT TT
OVERALL 69% 33% 27%
HCV RNA < 600,000 / METAVIR F0-‐F2 86% 63% 52%
HCV RNA < 600,000 / METAVIR F3-‐F4 63% 25% 0%
HCV RNA > 600,000 / METAVIR F0-‐F2 70% 29% 23%
HCV RNA > 600,000 / METAVIR F3-‐F4 37% 21% 12%
Testing for IL28b performed in 1604/3070 pts (52%)
HCV Terapia – Principali problemi irrisolti
SV
R%
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
6
17/10/16
7
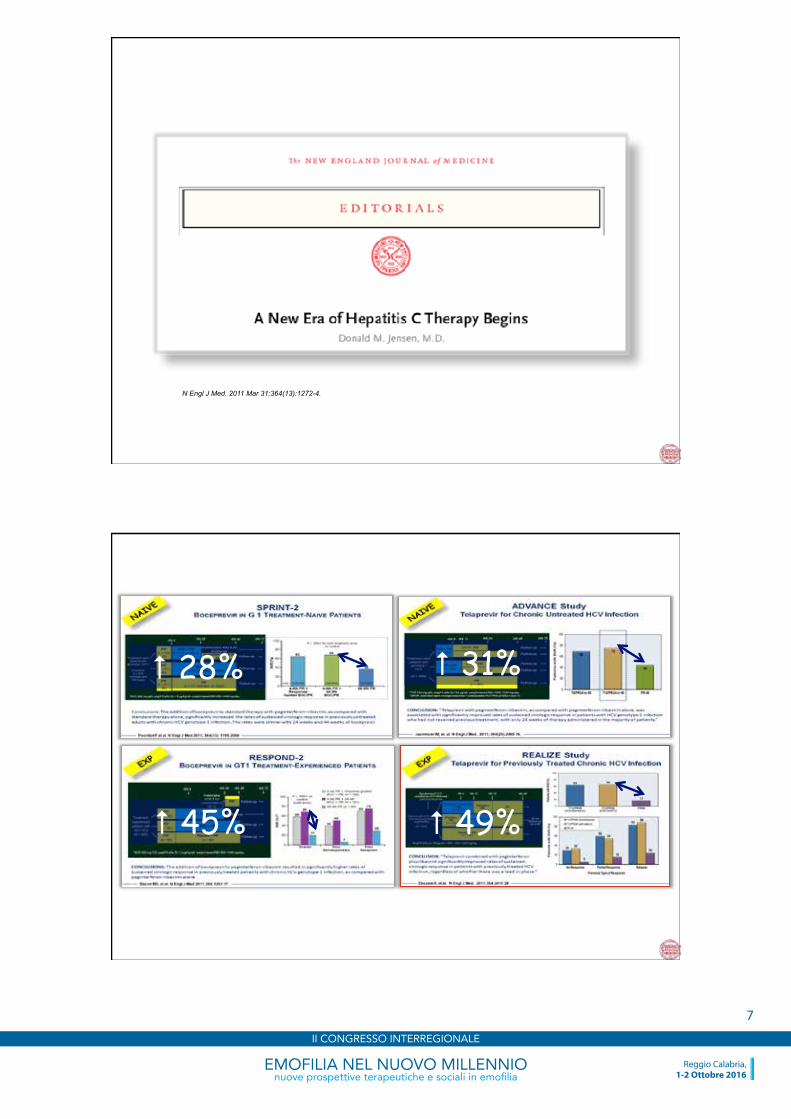
N Engl J Med. 2011 Mar 31;364(13):1272-4.
# 28%
# 49%
# 31%
# 45%
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
7
17/10/16
8
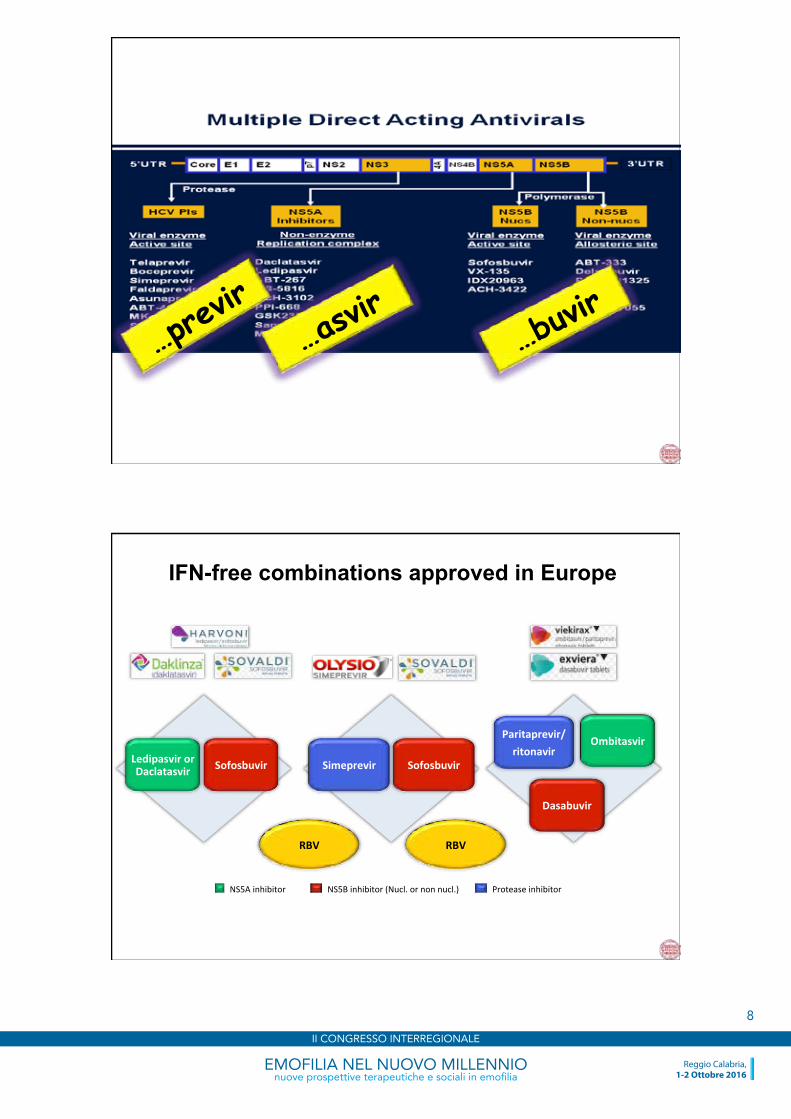
…previr
…asvir
…buvir
IFN-free combinations approved in Europe
RBV RBV
NS5A inhibitor NS5B inhibitor (Nucl. or non nucl.) Protease inhibitor
Ledipasvir or Daclatasvir Sofosbuvir Simeprevir Sofosbuvir
Paritaprevir/ ritonavir
Ombitasvir
Dasabuvir
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
8

17/10/16
9
NS5A inhibitor
NS5B inhibitor (Nucl. or Non Nucl.)
Protease inhibitor
…. near future ….
Elbasvir NS5A inh
MK 3682 Polym.inh
Grazoprevir Protease inh
Daclatasvir NS5A inh
Asunaprevir Protease inh
Beclabuvir Polym.inh
Sofosbuvir Polym inh
GS 5816 Velpatasvir NS5A inh
ABT-‐530 NS5A inh
ABT-‐493 Protease inh
MK 8408 NS5A inh
GS-‐9857 Protease inh
EMA Approved IFN-free Regimens for HCV Treatment
Ombitasvir/Paritaprevir/Ritonavir + Dasabuvir (± RBV)
Sofosbuvir + Simeprevir (± RBV)
Sofosbuvir + Daclatasvir (± RBV)
Ombitasvir/Paritaprevir/Ritonavir (± RBV)
Sofosbuvir + Velpatasvir (± RBV)
Grazoprevir + Elbasvir (± RBV)
Sofosbuvir + RBV
Sofosbuvir/Ledipasvir (± RBV)
GT
1
1, 4
All
4
1, 4
2, 3
1, 4, 5, 6
All coming soon
coming soon
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
9
17/10/16
10
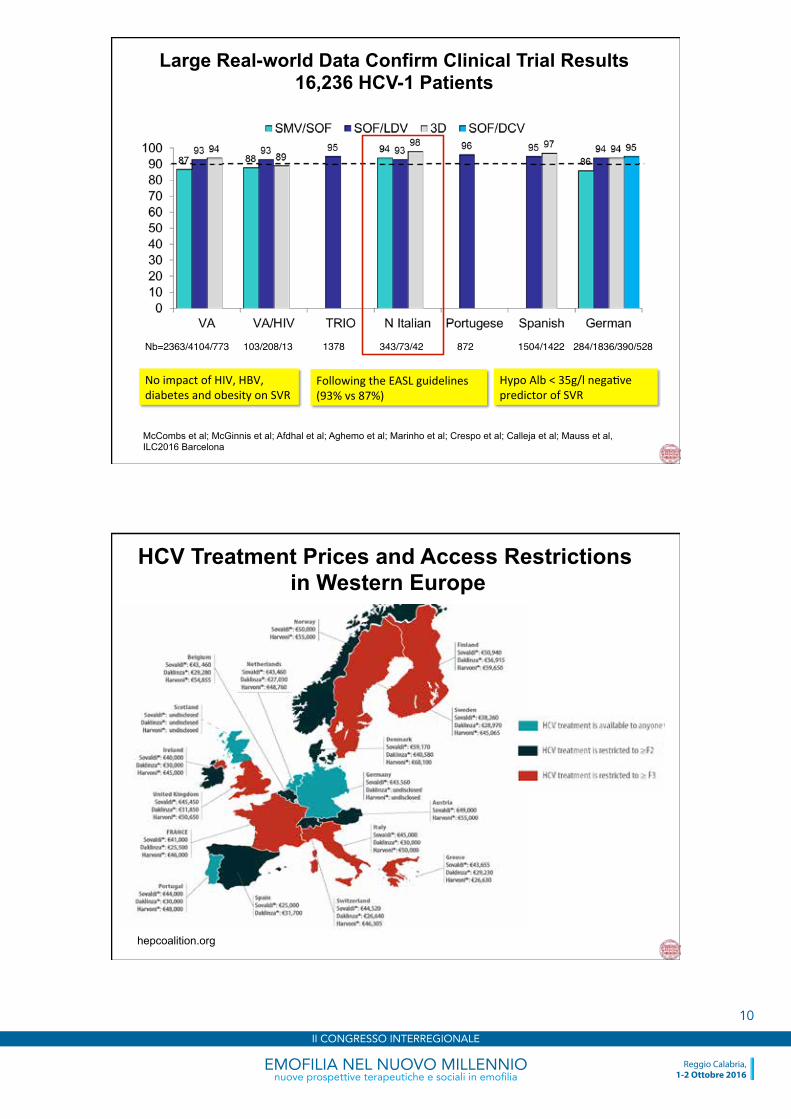
Large Real-world Data Confirm Clinical Trial Results 16,236 HCV-1 Patients
McCombs et al; McGinnis et al; Afdhal et al; Aghemo et al; Marinho et al; Crespo et al; Calleja et al; Mauss et al, ILC2016 Barcelona
No impact of HIV, HBV, diabetes and obesity on SVR
Following the EASL guidelines (93% vs 87%)
Hypo Alb < 35g/l nega/ve predictor of SVR
Nb=2363/4104/773 103/208/13 1378 872343/73/42 1504/1422 284/1836/390/528
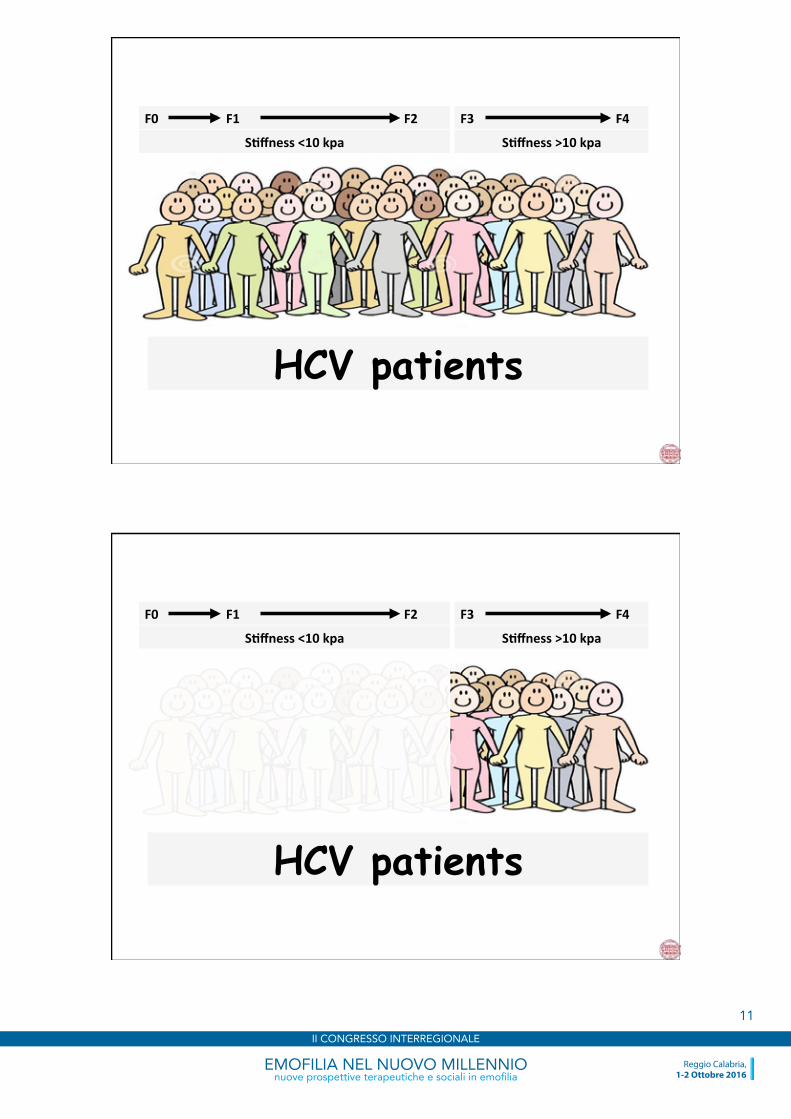
hepcoalition.org
HCV Treatment Prices and Access Restrictions in Western Europe
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
10
17/10/16
11
HCV patients
F0 F1 F2
S*ffness <10 kpa
F3 F4
S*ffness >10 kpa
HCV patients
F0 F1 F2
S*ffness <10 kpa
F3 F4
S*ffness >10 kpa
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
11
17/10/16
12
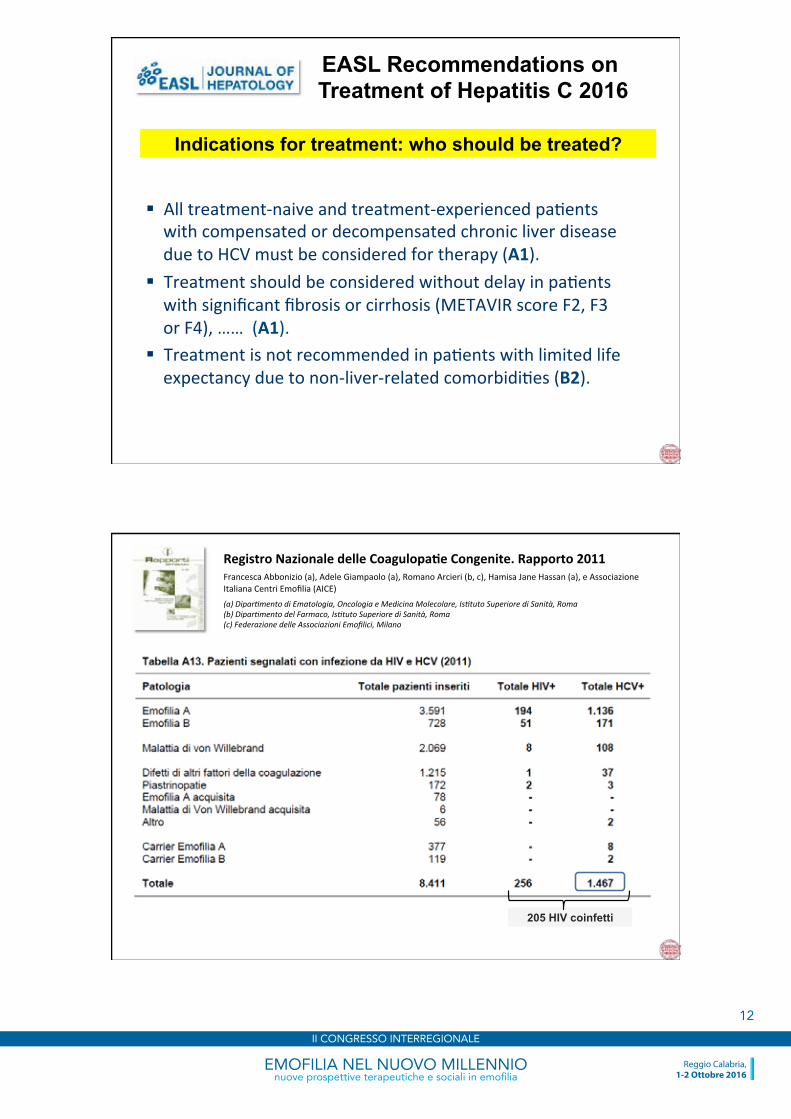
EASL Recommendations on Treatment of Hepatitis C 2016
§ All treatment-‐naive and treatment-‐experienced pa/ents with compensated or decompensated chronic liver disease due to HCV must be considered for therapy (A1).
§ Treatment should be considered without delay in pa/ents with significant fibrosis or cirrhosis (METAVIR score F2, F3 or F4), …… (A1).
§ Treatment is not recommended in pa/ents with limited life expectancy due to non-‐liver-‐related comorbidi/es (B2).
Indications for treatment: who should be treated?
Registro Nazionale delle Coagulopa*e Congenite. Rapporto 2011 Francesca Abbonizio (a), Adele Giampaolo (a), Romano Arcieri (b, c), Hamisa Jane Hassan (a), e Associazione Italiana Centri Emofilia (AICE)
(a) Dipar8mento di Ematologia, Oncologia e Medicina Molecolare, Is8tuto Superiore di Sanità, Roma (b) Dipar8mento del Farmaco, Is8tuto Superiore di Sanità, Roma (c) Federazione delle Associazioni Emofilici, Milano
205 HIV coinfetti
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
12
17/10/16
13
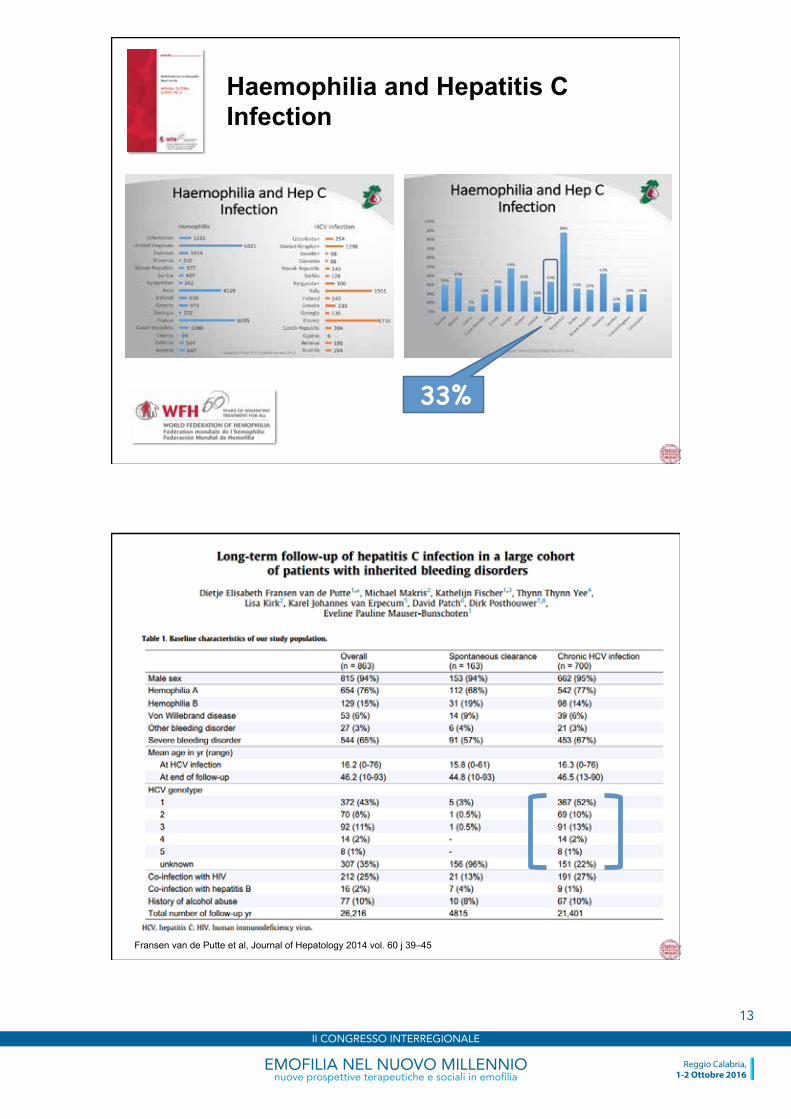
Haemophilia and Hepatitis C Infection
33%
Fransen van de Putte et al, Journal of Hepatology 2014 vol. 60 j 39–45
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
13
17/10/16
14
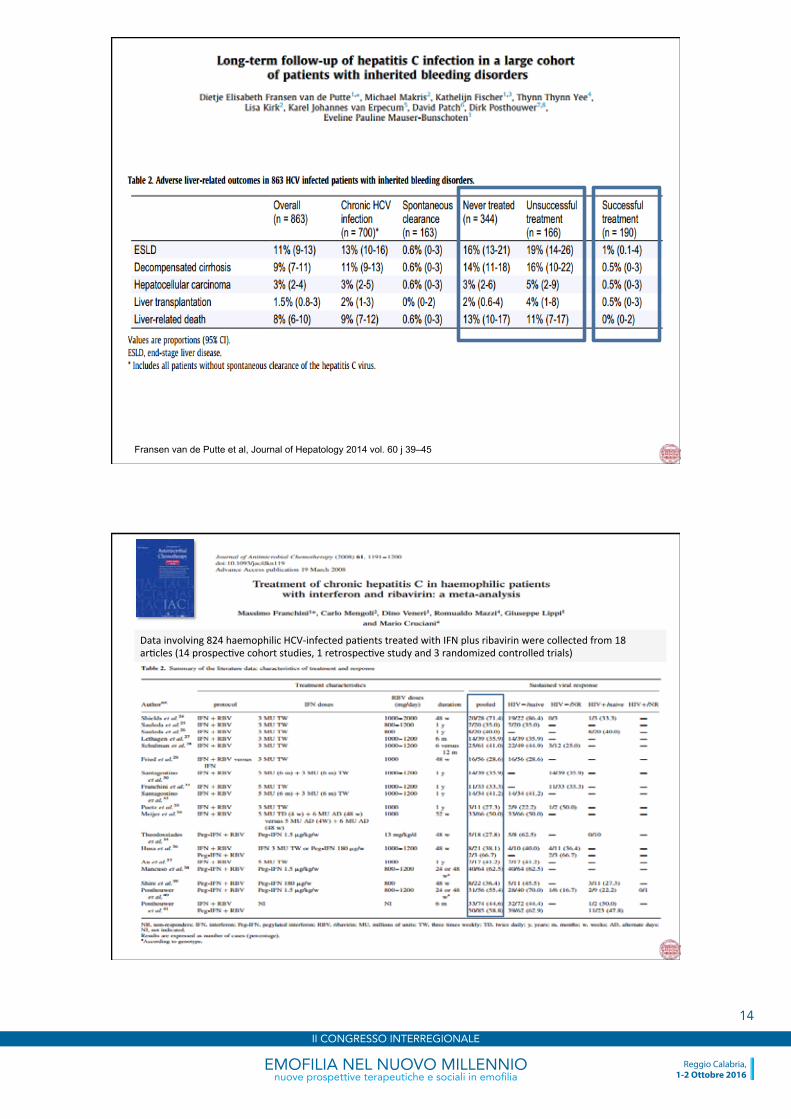
Fransen van de Putte et al, Journal of Hepatology 2014 vol. 60 j 39–45
Data involving 824 haemophilic HCV-‐infected pa/ents treated with IFN plus ribavirin were collected from 18 ar/cles (14 prospec/ve cohort studies, 1 retrospec/ve study and 3 randomized controlled trials)
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
14

17/10/16
15
Data involving 824 haemophilic HCV-‐infected pa/ents treated with IFN plus ribavirin were collected from 18 ar/cles (14 prospec/ve cohort studies, 1 retrospec/ve study and 3 randomized controlled trials)
These results were comparable to those observed in the general popula/on of HCV treated pa/ents. As observed in non-‐haemophilic pa/ents, genotype 1 (OR, 0.15; 95% CI, 0.09 – 0.25) and HIV-‐1 co-‐infec/on (OR, 0.25; 95% CI, 0.08 – 0.81) were strong predictors of worse response to IFN therapy. In conclusion, this meta-‐analysis documents that chronic hepa//s C in haemophiliacs has a behaviour similar to that in non-‐haemophilic pa/ents both in terms of response to ribavirin plus IFN therapy and in terms of nega/ve predictors of IFN therapy efficacy. The heterogeneity of treatment effect was explained by HCV genotype, HIV infec/on status and, to a lesser extent, to the type of IFN used.
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
15

17/10/16
16
Walsh C et al. Presented at AASLD: The Liver Meeting®, November 13–17, 2015, San Francisco, CA
120 patients
Walsh C et al. Presented at AASLD: The Liver Meeting®, November 13–17, 2015, San Francisco, CA
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
16
17/10/16
17
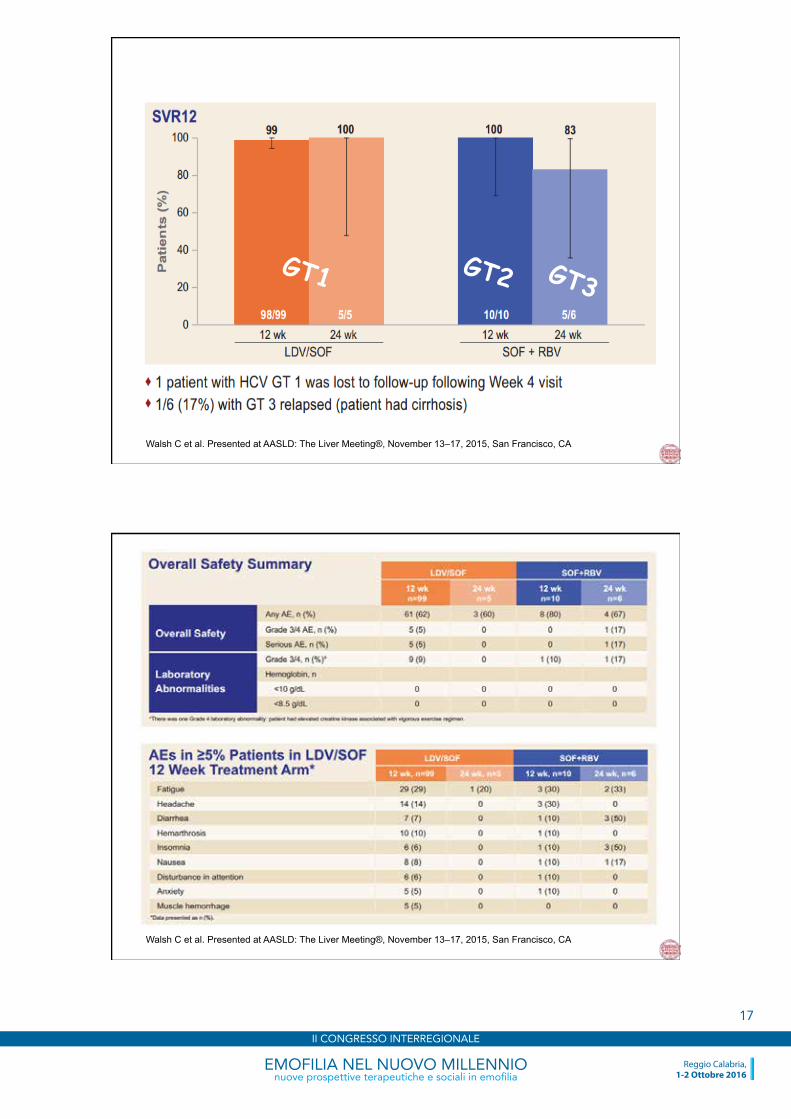
Walsh C et al. Presented at AASLD: The Liver Meeting®, November 13–17, 2015, San Francisco, CA
GT1 GT2 GT3
Walsh C et al. Presented at AASLD: The Liver Meeting®, November 13–17, 2015, San Francisco, CA
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
17
17/10/16
18
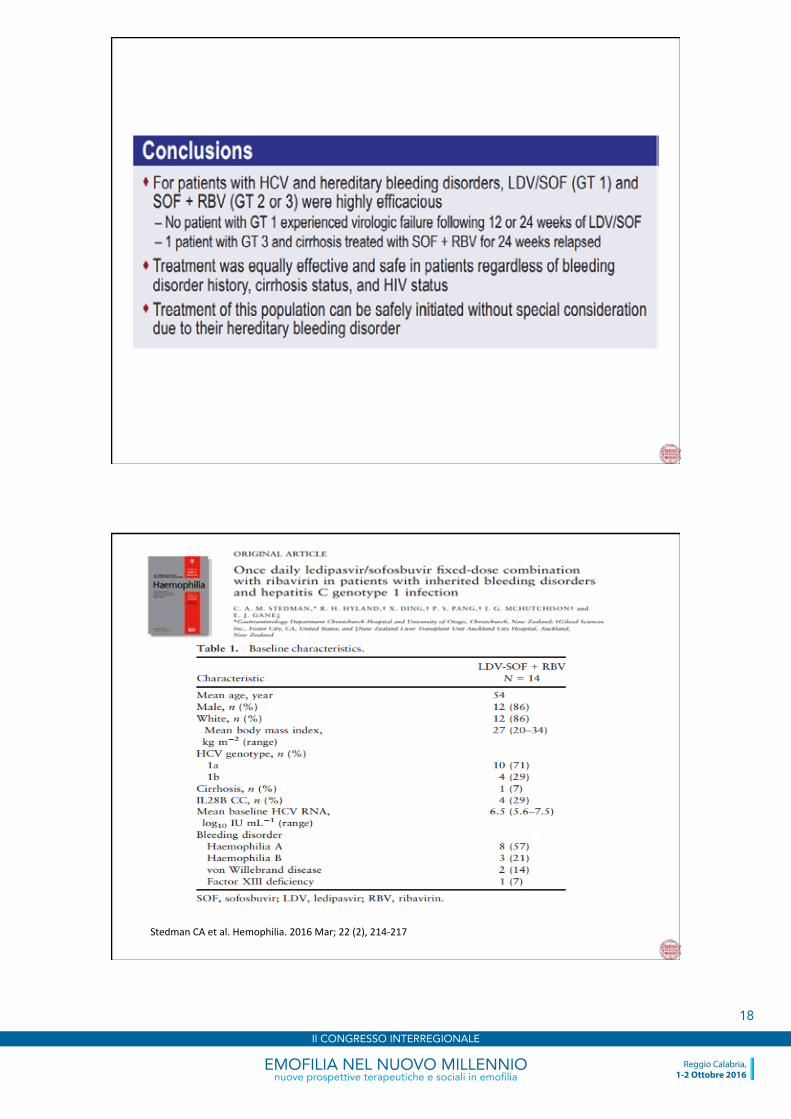
Stedman CA et al. Hemophilia. 2016 Mar; 22 (2), 214-‐217
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
18
17/10/16
19
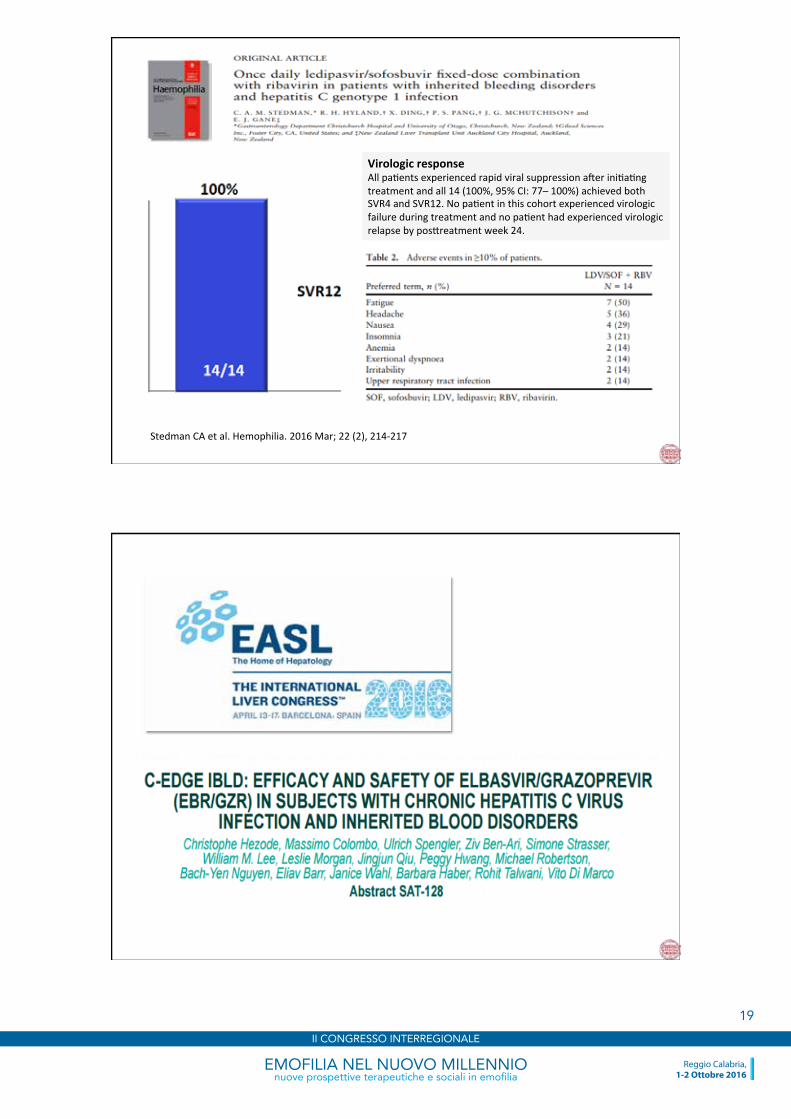
Stedman CA et al. Hemophilia. 2016 Mar; 22 (2), 214-‐217
Virologic response All pa/ents experienced rapid viral suppression ader ini/a/ng treatment and all 14 (100%, 95% CI: 77– 100%) achieved both SVR4 and SVR12. No pa/ent in this cohort experienced virologic failure during treatment and no pa/ent had experienced virologic relapse by pos[reatment week 24.
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
19
17/10/16
20
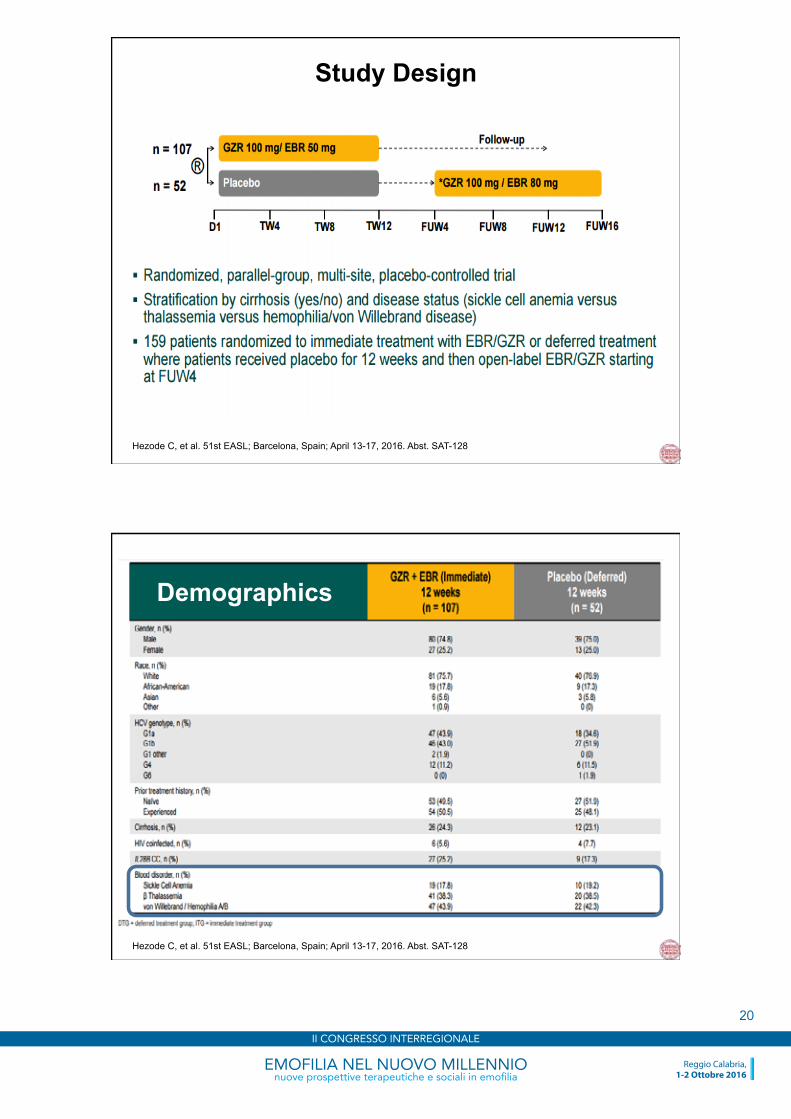
Study Design
Hezode C, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. SAT-128
Hezode C, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. SAT-128
Demographics
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
20
17/10/16
21
Hezode C, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. SAT-128
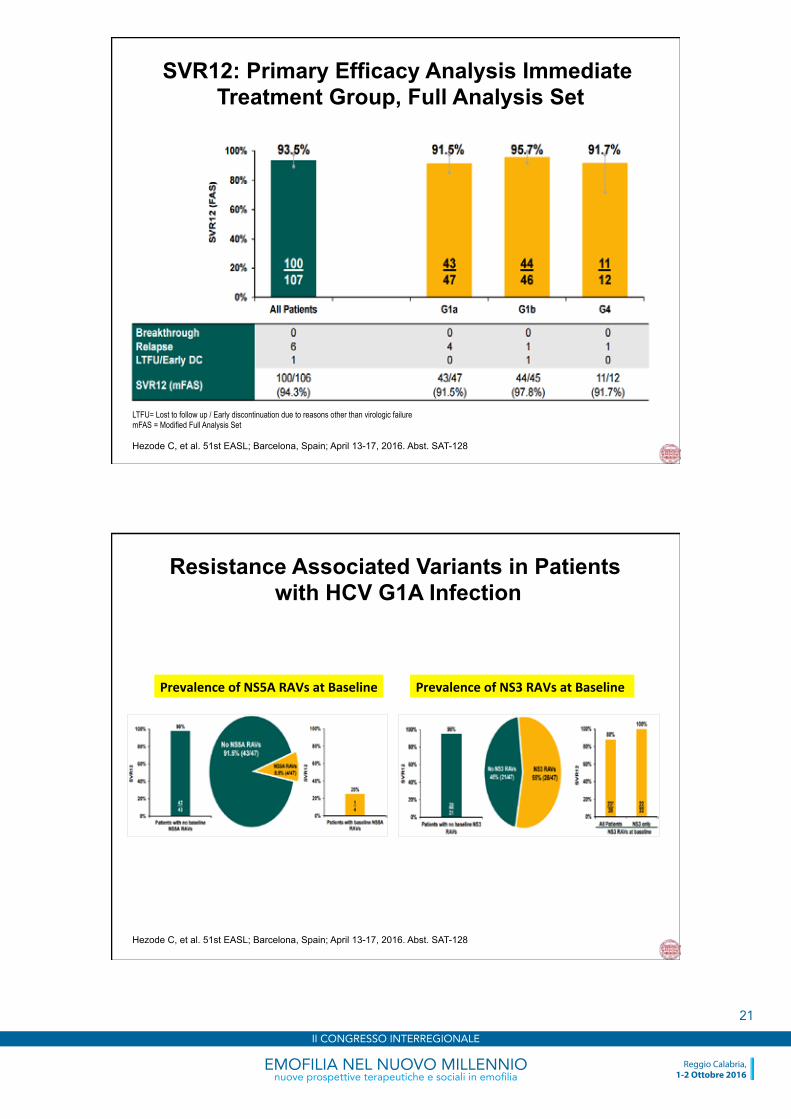
SVR12: Primary Efficacy Analysis Immediate Treatment Group, Full Analysis Set
LTFU= Lost to follow up / Early discontinuation due to reasons other than virologic failure mFAS = Modified Full Analysis Set
Hezode C, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. SAT-128
Resistance Associated Variants in Patients with HCV G1A Infection
Prevalence of NS3 RAVs at Baseline Prevalence of NS5A RAVs at Baseline
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
21
17/10/16
22
Hezode C, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. SAT-128
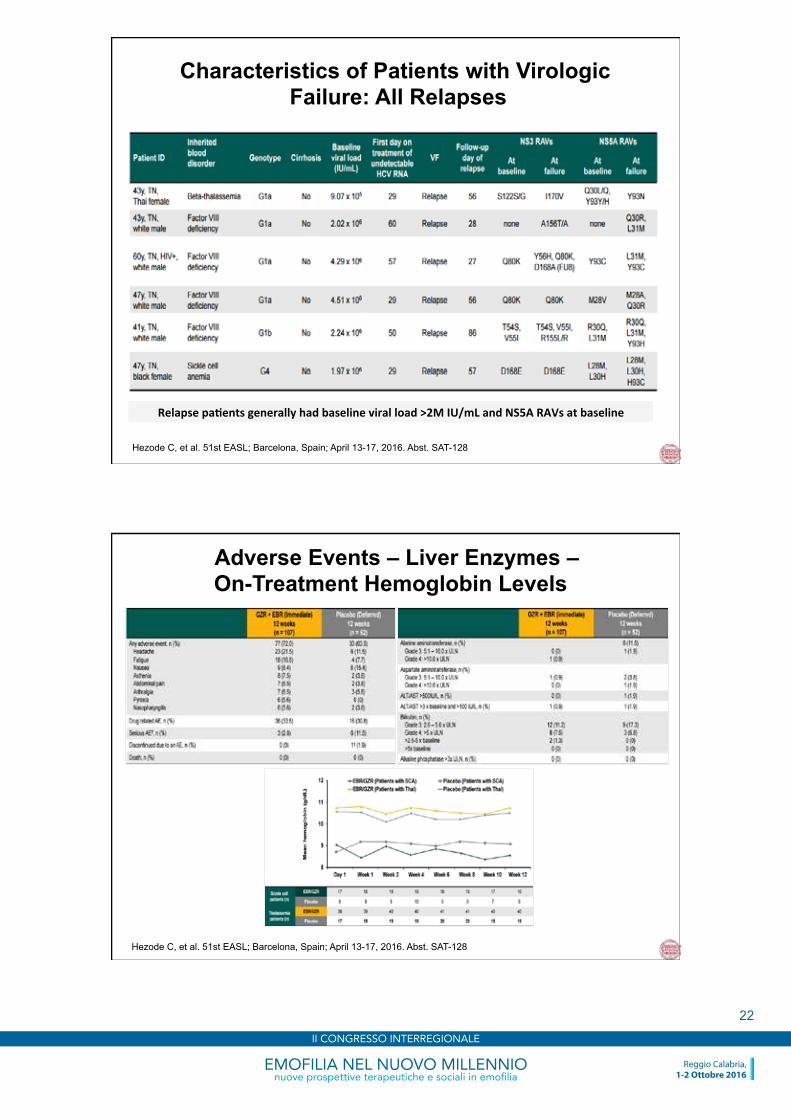
Characteristics of Patients with Virologic Failure: All Relapses
Relapse pa*ents generally had baseline viral load >2M IU/mL and NS5A RAVs at baseline
Hezode C, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. SAT-128
Adverse Events – Liver Enzymes – On-Treatment Hemoglobin Levels
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
22
17/10/16
23
Hezode C, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. SAT-128
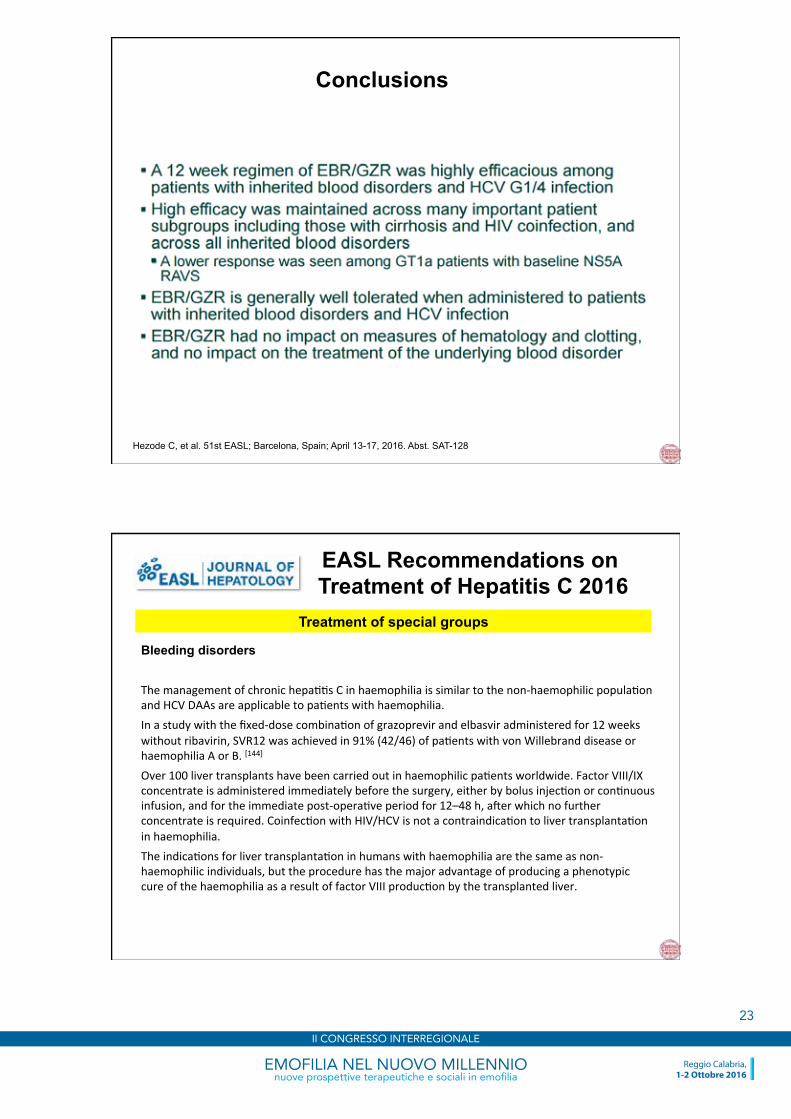
Conclusions
EASL Recommendations on Treatment of Hepatitis C 2016
Treatment of special groups
Bleeding disorders The management of chronic hepa//s C in haemophilia is similar to the non-‐haemophilic popula/on and HCV DAAs are applicable to pa/ents with haemophilia. In a study with the fixed-‐dose combina/on of grazoprevir and elbasvir administered for 12 weeks without ribavirin, SVR12 was achieved in 91% (42/46) of pa/ents with von Willebrand disease or haemophilia A or B. [144]
Over 100 liver transplants have been carried out in haemophilic pa/ents worldwide. Factor VIII/IX concentrate is administered immediately before the surgery, either by bolus injec/on or con/nuous infusion, and for the immediate post-‐opera/ve period for 12–48 h, ader which no further concentrate is required. Coinfec/on with HIV/HCV is not a contraindica/on to liver transplanta/on in haemophilia. The indica/ons for liver transplanta/on in humans with haemophilia are the same as non-‐haemophilic individuals, but the procedure has the major advantage of producing a phenotypic cure of the haemophilia as a result of factor VIII produc/on by the transplanted liver.
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
23
17/10/16
24
EASL Recommendations on Treatment of Hepatitis C 2016
Treatment of special groups
Bleeding disorders The management of chronic hepa//s C in haemophilia is similar to the non-‐haemophilic popula/on and HCV DAAs are applicable to pa/ents with haemophilia. In a study with the fixed-‐dose combina/on of grazoprevir and elbasvir administered for 12 weeks without ribavirin, SVR12 was achieved in 91% (42/46) of pa/ents with von Willebrand disease or haemophilia A or B. [144]
Over 100 liver transplants have been carried out in haemophilic pa/ents worldwide. Factor VIII/IX concentrate is administered immediately before the surgery, either by bolus injec/on or con/nuous infusion, and for the immediate post-‐opera/ve period for 12–48 h, ader which no further concentrate is required. Coinfec/on with HIV/HCV is not a contraindica/on to liver transplanta/on in haemophilia. The indica/ons for liver transplanta/on in humans with haemophilia are the same as non-‐haemophilic individuals, but the procedure has the major advantage of producing a phenotypic cure of the haemophilia as a result of factor VIII produc/on by the transplanted liver.
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
24

17/10/16
25
Anticoagulant, Anti-platelet and Fibrinolytic
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
25
17/10/16
26
Riunione Annuale Neo Gr.E.Ca.S Reggio Calabria Hotel Excelsior 16-‐17 Dicembre 2016
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
26
17/10/16
27
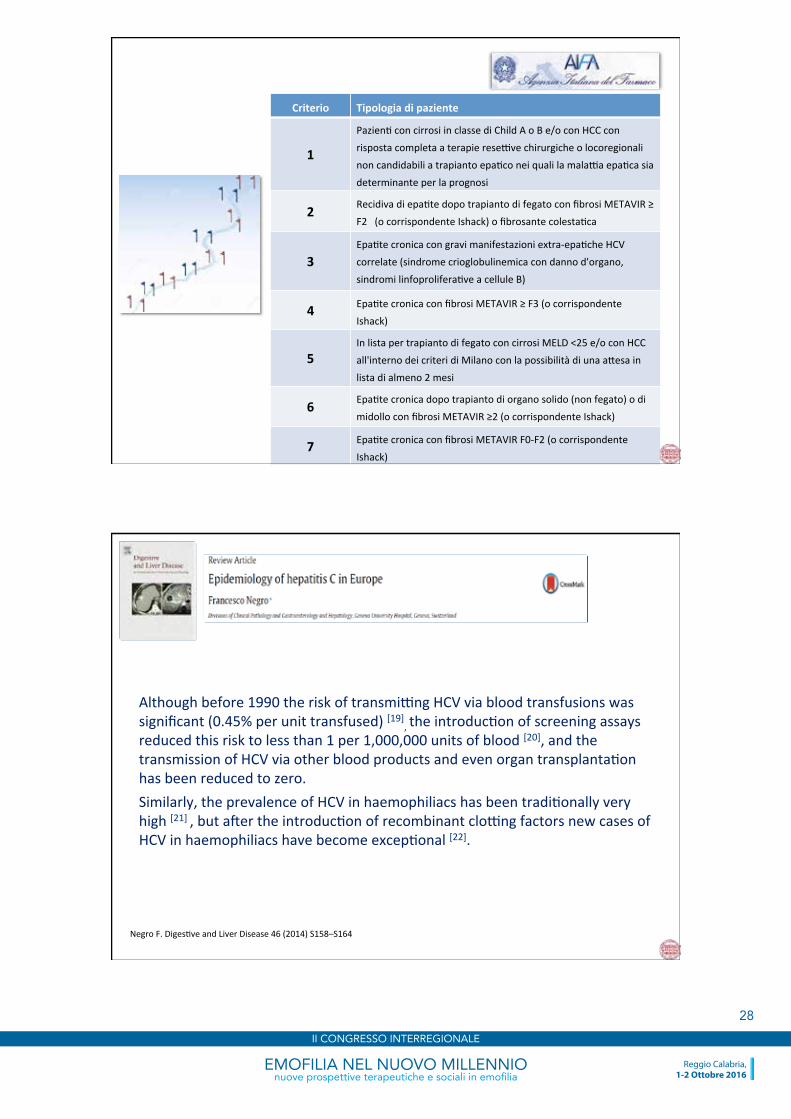
The WHO Viral Hepatitis Elimination Goals
By 2030: 90% chronic HCV diagnosed 80% treated 65% mortality reduc/on Treatment-‐as-‐preven*on: People who inject drugs (PWID) HIV + men who have sex with men (MSM)
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
27
17/10/16
28
Criterio Tipologia di paziente
1
Pazien/ con cirrosi in classe di Child A o B e/o con HCC con risposta completa a terapie rese=ve chirurgiche o locoregionali non candidabili a trapianto epa/co nei quali la mala=a epa/ca sia determinante per la prognosi
2 Recidiva di epa/te dopo trapianto di fegato con fibrosi METAVIR ≥ F2 (o corrispondente Ishack) o fibrosante colesta/ca
3 Epa/te cronica con gravi manifestazioni extra-‐epa/che HCV correlate (sindrome crioglobulinemica con danno d'organo, sindromi linfoprolifera/ve a cellule B)
4 Epa/te cronica con fibrosi METAVIR ≥ F3 (o corrispondente Ishack)
5 In lista per trapianto di fegato con cirrosi MELD <25 e/o con HCC all'interno dei criteri di Milano con la possibilità di una a[esa in lista di almeno 2 mesi
6 Epa/te cronica dopo trapianto di organo solido (non fegato) o di midollo con fibrosi METAVIR ≥2 (o corrispondente Ishack)
7 Epa/te cronica con fibrosi METAVIR F0-‐F2 (o corrispondente Ishack)
Negro F. Diges/ve and Liver Disease 46 (2014) S158–S164
Although before 1990 the risk of transmi=ng HCV via blood transfusions was significant (0.45% per unit transfused) [19], the introduc/on of screening assays reduced this risk to less than 1 per 1,000,000 units of blood [20], and the transmission of HCV via other blood products and even organ transplanta/on has been reduced to zero. Similarly, the prevalence of HCV in haemophiliacs has been tradi/onally very high [21] , but ader the introduc/on of recombinant clo=ng factors new cases of HCV in haemophiliacs have become excep/onal [22].
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
28
17/10/16
29
EASL Recommendations on Treatment of Hepatitis C 2016
Treatment of special groups
Haemoglobinopathies The most frequent haemoglobinopathy associated with chronic hepa//s C is thalassemia major, which requires frequent blood transfusions and is prevalent in countries where blood supply screening may be, or has been, subop/mal. Chronic HCV infec/on is also frequent in individuals with sickle cell anaemia or thalassemia, with a more rapid course of liver disease because of the concurrent iron overload [143]. Treatment has oden been withheld in these pa/ents because both pegylated IFN-‐a and ribavirin can cause anaemia. Few trials with an/viral therapy have been published in this popula/on, but there is no reason to consider that HCV DAAs are specifically contraindicated. For instance, in the C-‐EDGE IBLD study, the fixed-‐dose combina/on of grazoprevir and elbasvir was administered for 12 weeks without ribavirin in pa/ents with haemoglobinopathies infected with genotypes 1a, 1b or 4. Approximately one pa/ent out of four had cirrhosis. Pa/ents with a haemoglobin level <7 g/dL were excluded. SVR12 was achieved in 95% (18/19) of pa/ents with sickle cell anaemia and in 98% (40/41) of pa/ents with b-‐thalassemia [144]. On treatment, haemoglobin levels were maintained. Thus, IFN-‐free, ideally ribavirin-‐free drug regimens should be used in these pa/ents because they have the great advantage of not aggrava/ng the anaemia. Sofosbuvir-‐based studies in this group are in progress.
EASL Recommendations on Treatment of Hepatitis C 2016
Treatment of special groups
Haemoglobinopathies The most frequent haemoglobinopathy associated with chronic hepa//s C is thalassemia major, which requires frequent blood transfusions and is prevalent in countries where blood supply screening may be, or has been, subop/mal. Chronic HCV infec/on is also frequent in individuals with sickle cell anaemia or thalassemia, with a more rapid course of liver disease because of the concurrent iron overload [143]. Treatment has oden been withheld in these pa/ents because both pegylated IFN-‐a and ribavirin can cause anaemia. Few trials with an/viral therapy have been published in this popula/on, but there is no reason to consider that HCV DAAs are specifically contraindicated. For instance, in the C-‐EDGE IBLD study, the fixed-‐dose combina/on of grazoprevir and elbasvir was administered for 12 weeks without ribavirin in pa/ents with haemoglobinopathies infected with genotypes 1a, 1b or 4. Approximately one pa/ent out of four had cirrhosis. Pa/ents with a haemoglobin level <7 g/dL were excluded. SVR12 was achieved in 95% (18/19) of pa/ents with sickle cell anaemia and in 98% (40/41) of pa/ents with b-‐thalassemia [144]. On treatment, haemoglobin levels were maintained. Thus, IFN-‐free, ideally ribavirin-‐free drug regimens should be used in these pa/ents because they have the great advantage of not aggrava/ng the anaemia. Sofosbuvir-‐based studies in this group are in progress.
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
29

17/10/16
30
Walsh C et al. Presented at AASLD: The Liver Meeting®, November 13–17, 2015, San Francisco, CA
EMOFILIA NEL NUOVO MILLENNIOnuove prospettive terapeutiche e sociali in emofilia
Reggio Calabria,1-2 Ottobre 2016
II CONGRESSO INTERREGIONALE
30




![Grazoprevir/Elbasvir for the treatment of Hepatitis C...replication. Elbasvir is an NS5A inhibitor, preventing HCV viral RNA replication and virion assembly. [2] The regimen is included](https://static.fdocuments.net/doc/165x107/5e5eb3646cbcfe3c9334a7a7/grazoprevirelbasvir-for-the-treatment-of-hepatitis-c-replication-elbasvir.jpg)













