17 - ICD10 SpecialtyTips Podiatry - We Know the Business …€¦ · · 2017-05-24•...
5
ICD10 SPECIALTY TIPS PODIATRY | 1 of 5 SPECIALTY TIP #17 Podiatry The Basics As with Plastics, Podiatry often has an uphill battle as to whether a procedure will be paid by an insurance carrier. The procedures may have a justifiable medical necessity (as determined by the carriers) or a matter of comfort; it is the age old battle of need versus wants with added emphasis on supporting documentation to illustrate the medical necessity for treatment. According to CMS, the only covered podiatry services are those considered medically necessary and reasonable foot care. This means that any elective or nonmedically necessary services might not be covered as reasonable foot care. Some procedures may require precertification to determine whether or not the procedures would meet the criteria as determined by a carrier’s medical director review. Check with the carrier for procedures that may or may not be covered as each patient’s plan has its own guideline for coverage. Procedures For procedure coding, there are a few tips that would be helpful to the coders to make coding for your services more accurate. • Identify the specific location of surgery o Specify toes involved o Specify bones involved • Always state laterality. o This is especially relevant when treating different conditions and/or performing different procedures for contralateral sides. • Often it is difficult to determine if a surgery is for purely cosmetic reasons or could there be a medical condition that may support requesting reimbursement from an insurance carrier. o Example: One carrier considers foot cheilectomy medically necessary for symptomatic relief of either of the following conditions: • Painful bony spurs in the earlier stages of an arthritic joint; or • Painful hallux rigidus. For all other indications the carrier considers foot cheilectomy experimental and investigational because its effectiveness for indications other than the ones listed above has not been established. o The H&P or consult may be requested for the medical review, those documents are ideal to illustrate the need for treatment. A path report may also be needed support medical necessity in some instances. o Do not forget to include pertinent information and diagnoses in your surgical op report. Often, the supporting diagnosis (breast cancer with mastectomy, contracture from burn scarring, etc.) may be missing from the op reports and the H&P or consult are needed in order to obtain the information thus causing a delay in submitting the claim. • Provide adequate history to identify any former surgeries or conditions affecting treatment. o Often it is difficult to differentiate whether the current surgery is the initial procedure or is this surgery: A repeat surgery (76 modifier if same surgeon, 77 modifier by a different surgeon), A planned, staged procedure (58 modifier if within the postoperative global period), For a different condition (thereby starting the global “clock” for a different condition, 79 modifier), A correction of a defect (different diagnosis noting a complication). An unplanned return to the operating room for a related procedure (78 modifier). o For staged procedures, when was the last surgery? Is this within the global period of the previous surgery? o Otherwise, what condition has prompted the current surgery? • Your documentation should clearly explain WHY you did a procedure. o Do not just state that you performed a procedure without adequate medical necessity in the form of a codable definitive diagnosis or signs and/or symptoms. A noncodable “rule out” diagnosis might be useful in a denial situation or should there be a request for additional information from a carrier to illustrate your decision making process.
Transcript of 17 - ICD10 SpecialtyTips Podiatry - We Know the Business …€¦ · · 2017-05-24•...

ICD-‐10 SPECIALTY TIPS
PODIATRY | 1 of 5
SPECIALTY TIP #17 Podiatry The Basics As with Plastics, Podiatry often has an uphill battle as to whether a procedure will be paid by an insurance carrier. The procedures may have a justifiable medical necessity (as determined by the carriers) or a matter of comfort; it is the age old battle of need versus wants with added emphasis on supporting documentation to illustrate the medical necessity for treatment. According to CMS, the only covered podiatry services are those considered medically necessary and reasonable foot care. This means that any elective or non-‐medically necessary services might not be covered as reasonable foot care. Some procedures may require pre-‐certification to determine whether or not the procedures would meet the criteria as determined by a carrier’s medical director review. Check with the carrier for procedures that may or may not be covered as each patient’s plan has its own guideline for coverage. Procedures For procedure coding, there are a few tips that would be helpful to the coders to make coding for your services more accurate.
• Identify the specific location of surgery o Specify toes involved o Specify bones involved
• Always state laterality. o This is especially relevant when treating different conditions and/or performing different procedures for
contralateral sides. • Often it is difficult to determine if a surgery is for purely cosmetic reasons or could there be a medical condition that
may support requesting reimbursement from an insurance carrier. o Example:
§ One carrier considers foot cheilectomy medically necessary for symptomatic relief of either of the following conditions:
• Painful bony spurs in the earlier stages of an arthritic joint; or • Painful hallux rigidus.
§ For all other indications the carrier considers foot cheilectomy experimental and investigational because its effectiveness for indications other than the ones listed above has not been established.
o The H&P or consult may be requested for the medical review, those documents are ideal to illustrate the need for treatment. A path report may also be needed support medical necessity in some instances.
o Do not forget to include pertinent information and diagnoses in your surgical op report. Often, the supporting diagnosis (breast cancer with mastectomy, contracture from burn scarring, etc.) may be missing from the op reports and the H&P or consult are needed in order to obtain the information thus causing a delay in submitting the claim.
• Provide adequate history to identify any former surgeries or conditions affecting treatment. o Often it is difficult to differentiate whether the current surgery is the initial procedure or is this surgery:
§ A repeat surgery (-‐76 modifier if same surgeon, -‐77 modifier by a different surgeon), § A planned, staged procedure (-‐58 modifier if within the postoperative global period), § For a different condition (thereby starting the global “clock” for a different condition, -‐79 modifier), § A correction of a defect (different diagnosis noting a complication). § An unplanned return to the operating room for a related procedure (-‐78 modifier).
o For staged procedures, when was the last surgery? § Is this within the global period of the previous surgery?
o Otherwise, what condition has prompted the current surgery? • Your documentation should clearly explain WHY you did a procedure.
o Do not just state that you performed a procedure without adequate medical necessity in the form of a codable definitive diagnosis or signs and/or symptoms. A non-‐codable “rule out” diagnosis might be useful in a denial situation or should there be a request for additional information from a carrier to illustrate your decision making process.
ICD-‐10 SPECIALTY TIPS
PODIATRY | 2 of 5
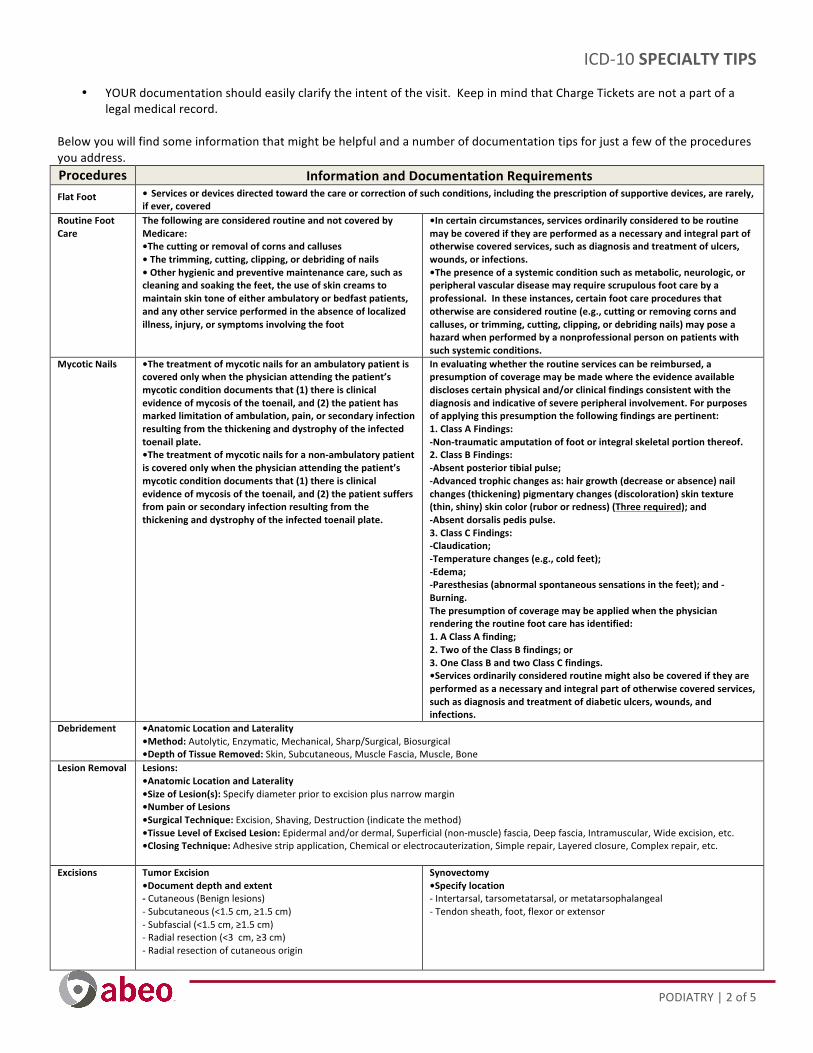
• YOUR documentation should easily clarify the intent of the visit. Keep in mind that Charge Tickets are not a part of a legal medical record.
Below you will find some information that might be helpful and a number of documentation tips for just a few of the procedures you address. Procedures Information and Documentation Requirements Flat Foot • Services or devices directed toward the care or correction of such conditions, including the prescription of supportive devices, are rarely,
if ever, covered Routine Foot Care
The following are considered routine and not covered by Medicare: •The cutting or removal of corns and calluses • The trimming, cutting, clipping, or debriding of nails • Other hygienic and preventive maintenance care, such as cleaning and soaking the feet, the use of skin creams to maintain skin tone of either ambulatory or bedfast patients, and any other service performed in the absence of localized illness, injury, or symptoms involving the foot
•In certain circumstances, services ordinarily considered to be routine may be covered if they are performed as a necessary and integral part of otherwise covered services, such as diagnosis and treatment of ulcers, wounds, or infections. •The presence of a systemic condition such as metabolic, neurologic, or peripheral vascular disease may require scrupulous foot care by a professional. In these instances, certain foot care procedures that otherwise are considered routine (e.g., cutting or removing corns and calluses, or trimming, cutting, clipping, or debriding nails) may pose a hazard when performed by a nonprofessional person on patients with such systemic conditions.
Mycotic Nails •The treatment of mycotic nails for an ambulatory patient is covered only when the physician attending the patient’s mycotic condition documents that (1) there is clinical evidence of mycosis of the toenail, and (2) the patient has marked limitation of ambulation, pain, or secondary infection resulting from the thickening and dystrophy of the infected toenail plate. •The treatment of mycotic nails for a non-‐ambulatory patient is covered only when the physician attending the patient’s mycotic condition documents that (1) there is clinical evidence of mycosis of the toenail, and (2) the patient suffers from pain or secondary infection resulting from the thickening and dystrophy of the infected toenail plate.
In evaluating whether the routine services can be reimbursed, a presumption of coverage may be made where the evidence available discloses certain physical and/or clinical findings consistent with the diagnosis and indicative of severe peripheral involvement. For purposes of applying this presumption the following findings are pertinent: 1. Class A Findings: -‐Non-‐traumatic amputation of foot or integral skeletal portion thereof. 2. Class B Findings: -‐Absent posterior tibial pulse; -‐Advanced trophic changes as: hair growth (decrease or absence) nail changes (thickening) pigmentary changes (discoloration) skin texture (thin, shiny) skin color (rubor or redness) (Three required); and -‐Absent dorsalis pedis pulse. 3. Class C Findings: -‐Claudication; -‐Temperature changes (e.g., cold feet); -‐Edema; -‐Paresthesias (abnormal spontaneous sensations in the feet); and -‐Burning. The presumption of coverage may be applied when the physician rendering the routine foot care has identified: 1. A Class A finding; 2. Two of the Class B findings; or 3. One Class B and two Class C findings. •Services ordinarily considered routine might also be covered if they are performed as a necessary and integral part of otherwise covered services, such as diagnosis and treatment of diabetic ulcers, wounds, and infections.
Debridement •Anatomic Location and Laterality •Method: Autolytic, Enzymatic, Mechanical, Sharp/Surgical, Biosurgical •Depth of Tissue Removed: Skin, Subcutaneous, Muscle Fascia, Muscle, Bone
Lesion Removal Lesions: •Anatomic Location and Laterality •Size of Lesion(s): Specify diameter prior to excision plus narrow margin •Number of Lesions •Surgical Technique: Excision, Shaving, Destruction (indicate the method) •Tissue Level of Excised Lesion: Epidermal and/or dermal, Superficial (non-‐muscle) fascia, Deep fascia, Intramuscular, Wide excision, etc. •Closing Technique: Adhesive strip application, Chemical or electrocauterization, Simple repair, Layered closure, Complex repair, etc.
Excisions Tumor Excision •Document depth and extent -‐ Cutaneous (Benign lesions) -‐ Subcutaneous (<1.5 cm, ≥1.5 cm) -‐ Subfascial (<1.5 cm, ≥1.5 cm) -‐ Radial resection (<3 cm, ≥3 cm) -‐ Radial resection of cutaneous origin
Synovectomy •Specify location -‐ Intertarsal, tarsometatarsal, or metatarsophalangeal -‐ Tendon sheath, foot, flexor or extensor

ICD-‐10 SPECIALTY TIPS
PODIATRY | 3 of 5
Bunionectomy
Document: •Approach •Additional procedures in detail
•Check that your documentation supports the procedures Examples of covered diagnoses for procedures from one carrier (CAUTION: These covered diagnoses may not be the same for other carriers):
28290
Correction, hallux valgus (bunion), with or without sesamoidectomy; simple exostectomy (e.g., Silver type procedure)
E10.51 -‐ E10.59 E11.51 -‐ E11.59 E13.51 -‐ E13.59
Diabetes with circulatory complications [with ulcer and/or infection stemming solely from bunion]
L89.890 -‐ L89.899 Pressure ulcer of other site [toes] [in diabetic members stemming solely from bunion]
L97.501 -‐ L97.529 Non-‐pressure ulcer of other part of foot [toes] [in diabetic members stemming solely from bunion]
M20.10 -‐ M20.12 Hallux valgus (acquired) M86.071 -‐ M86.079, M86.171 -‐ M86.179 M86.271 -‐ M86.279, M86.371 -‐ M86.379 M86.471 -‐ M86.479, M86.571 -‐ M86.579 M86.9
Osteomyelitis, periositis, and other infections involving bone [stemming solely from bunion]
28292 28294
28296
28297
28298
28299
Correction, hallux valgus (bunion), with or without sesamoidectomy; Keller, McBride or Mayo type procedure Correction, hallux valgus (bunion), with or without sesamoidectomy; with tendon transplants (e.g., Joplin type procedure) Correction, hallux valgus (bunion), with or without sesamoidectomy; with metatarsal osteotomy (e.g., Mitchell, Chevron or concentric type procedures) Correction, hallux valgus (bunion), with or without sesamoidectomy; Lapidus type procedure Correction, hallux valgus (bunion), with or without sesamoidectomy; by phalanx osteotomy Correction, hallux valgus (bunion), with or without sesamoidectomy; by double osteotomy
D21.20 -‐ D21.22 Benign neoplasm of connective and other soft tissue of lower limb, including hip
G57.60 -‐ G57.62 Lesion of plantar nerve [neuroma secondary to bunion]
M19.071 -‐ M19.079 Primary osteoarthritis ankle and foot
M19.171 -‐ M19.179 Post-‐traumatic osteoarthritis, ankle and foot M20.10 -‐ M20.12 Hallux valgus (acquired) M20.5x1 -‐ M20.5x9 Other deformities of toe(s) (acquired)
[overriding of great toe or crossover toe deformity]
M67.00 -‐ M67.02 Short Achilles tendon (acquired) M71.171 -‐ M71.179 Other infective bursitis, ankle and foot
[recurrent] M77.50 -‐ M77.52 Other enthesopathy of foot [recurrent
bursitis] M85.671 -‐ M85.679 Other cyst of bone, ankle and foot Q66.89 Other specified congenital deformities of feet
[overriding of great toe or crossover toe deformity]
Hammertoe Deformity
28285
28286
Correction, hammertoe (e.g., interphalangeal fusion, partial or total phalangectomy) Correction, cock-‐up fifth toe, with plastic skin closure (e.g., Ruiz-‐ Mora type procedure)
E64.3 Sequelae of rickets [hammertoe, claw toe, mallet toe]
G57.60 -‐ G57.62 Lesion of plantar nerve [interdigital neuroma] L97.501 -‐ L97.529 Non-‐pressure chronic ulcer of other part of
foot [of apices] M12.271 -‐ M12.279 Villonodular synovitis (pigmente), ankle and
foot [of MP joint] M20.40 -‐ M20.42 Other hammer toe(s) (acquired) M20.5x1 -‐ M20.62 Other and acquired anomalies of toes
[hammer toe, congenital] M24.571 -‐ M24.576 Contracture of joint, ankle and foot [MP joint] M24.671 -‐ M24.676 Ankylosis of joint, ankle and foot [ankylosis of
proximal interphalangeal joint] M65.871 -‐ M65.879 Other synovitis and tenosynovitis, ankle and
foot [of MP joint] M67.00 -‐ M67.02 Short Achilles tendon (acquired) M77.50 -‐ M77.52 Other enthesopathy of foot [adventitious
bursitis on the dorsal surface] M77.9 Enthesopathy, unspecified
[synovitis/capsulitis] Q66.7 Congenital pes cavus [claw toe, congenital] Q74.2 Other congenital malformations of lower
limb(s), including pelvic girdle [subluxation or dislocation MP joint]
S92.521x -‐ S92.529x Sprain of metatarsophalangeal joint of toe [lateral MP capsular tear]
S93.121x -‐ S92.129x Dislocation of metatarsophalangeal joint

ICD-‐10 SPECIALTY TIPS
PODIATRY | 4 of 5
Diagnosis Documentation tells a story enabling a coder to translate into numbers explaining what you did and why. The more detailed and complete the story, the less difficult it is to support and ask for reimbursement.
• Be sure to designate laterality (right, left, or bilateral). • Location, location, location... always be site specific and detail anatomical locations. • For musculoskeletal conditions and injuries, state whether the patient is:
o In the treatment phase (surgery, Emergency Department, evaluation and treatment by new physician, etc.), o In the healing phase (cast change or removal, medication adjustment, aftercare following treatment), o Or is this a late effect/sequela of an injury?
• When treating a sequela for an injury you need to gather information on the mechanism of the injury . o Details of the original injury (“closed fracture of the nasal bone with a dislocation of the septal cartilage of the
nose”) o When did the original injury occur? (Date) o What happened? (“driver in an MVA”, “slip and fall in home”, “hit by a baseball”, etc.)
• Is this a complication from a previous surgery? • Coding rules dictate that when coding for multiple conditions, the more severe or acute code is sequenced first with
chronic conditions as secondary. • Be sure to qualify the severity of the condition. Diagnostic sequencing depends on severity (acute over chronic, etc.). • State acute or chronic, old injury, any descriptive wording that help to illustrate the condition . • Document related, secondary or causal illness whenever appropriate. • Include comorbid and relevant conditions that impact decision making or complicate surgery. • If a patient is pregnant, always include trimester and number of weeks regardless of the setting.
o The only time pregnancy is considered incidental is when it is documented as such. Otherwise it is coded as “Pregnancy complicated by...”
• Social factors influencing diagnoses o Note tobacco use, abuse, dependence, past history, or exposure with type of tobacco product (cigarette,
chewing, etc.). • Document medical necessity in the op report as well as the H&P.
Some most often used diagnosis
Description ICD-‐10 ICD-‐10 Atherosclerosis of autologous vein bypass graft(s) of the left leg w/ulceration of other part of foot
I70.445
Atherosclerosis of autologous vein bypass graft(s) of the right leg w/ulceration of other part of foot
I70.435
Atherosclerosis of autologous vein bypass graft(s) of the right leg with ulceration of heel and midfoot
I70.434
Atherosclerosis of native arteries of left leg w/ulceration of other part of foot
I70.245
Atherosclerosis of native arteries of left leg with ulceration of heel and midfoot
I70.244
Atherosclerosis of native arteries of right leg w/ulceration of other part of foot
I70.235
Atherosclerosis of native arteries of right leg with ulceration of heel and midfoot
I70.234
Atherosclerosis of nonautologous biological bypass graft(s) of the left leg w/ulceration of other part of foot
I70.545
Atherosclerosis of nonautologous biological bypass graft(s) of the right leg w/ulceration of other part of foot
I70.535
Atherosclerosis of nonbiological bypass graft(s) of the left leg w/ulceration of other part of foot
I70.645
Atherosclerosis of nonbiological bypass graft(s) of the right leg w/ulceration of other part of foot
I70.635
Atherosclerosis of other type of bypass graft(s) of the left leg w/ulceration of other part of foot
I70.745
Atherosclerosis of other type of bypass graft(s) of the right leg w/ulceration of other part of foot
I70.735
Atherosclerosis of unspecified type of bypass graft(s) of the left leg w/ulceration of other part of foot
I70.345
Atherosclerosis of unspecified type of bypass graft(s) of the left leg with ulceration of heel and midfoot
I70.344
Atherosclerosis of unspecified type of bypass graft(s) of the right leg w/ulceration of other part of foot
I70.335
Atherosclerosis of unspecified type of bypass graft(s) of the right leg with ulceration of heel and midfoot
I70.334
Calcaneal spur, left foot M77.32 Calcaneal spur, right foot M77.31 Calcaneal spur, unspecified foot M77.30 Cellulitis of left toe L03.032 Cellulitis of right toe L03.031 Cellulitis of unspecified toe L03.039 Corns and callosities L84 Enthesopathy unspecified M77.9 Flat foot (acquired) M21.4 Flat foot (congenital) Q66.5 Foot drop M21.37 Hallux valgus (acquired) left foot M20.12 Hallux valgus (acquired) right foot M20.11 Hallux valgus (acquired) unspecified foot M20.10 In growing nail L60.0 Lesion of plantar nerve, left lower limb G57.62 Lesion of plantar nerve, right lower limb G57.61 Lesion of plantar nerve, unspecified lower limb G57.60

ICD-‐10 SPECIALTY TIPS
PODIATRY | 5 of 5
Non-‐pressure chronic ulcer of left heel and midfoot limited to breakdown of skin
L97.421
Non-‐pressure chronic ulcer of left heel and midfoot with fat layer exposed
L97.422
Non-‐pressure chronic ulcer of left heel and midfoot with necrosis of bone
L97.424
Non-‐pressure chronic ulcer of left heel and midfoot with necrosis of muscle
L97.423
Non-‐pressure chronic ulcer of left heel and midfoot with unspecified severity
L97.429
Non-‐pressure chronic ulcer of other part of left foot limited to breakdown of skin
L97.521
Non-‐pressure chronic ulcer of other part of left foot w/fat layer exposed
L97.522
Non-‐pressure chronic ulcer of other part of left foot w/necrosis of bone
L97.524
Non-‐pressure chronic ulcer of other part of left foot w/necrosis of muscle
L97.523
Non-‐pressure chronic ulcer of other part of left foot w/unspecified severity
L97.529
Non-‐pressure chronic ulcer of other part of right foot limited to breakdown of skin
L97.511
Non-‐pressure chronic ulcer of other part of right foot w/fat layer exposed
L97.512
Non-‐pressure chronic ulcer of other part of right foot w/necrosis of bone
L97.514
Non-‐pressure chronic ulcer of other part of right foot w/necrosis of muscle
L97.513
Non-‐pressure chronic ulcer of other part of right foot w/unspecified severity
L97.519
Non-‐pressure chronic ulcer of other part of unspecified foot limited to breakdown of skin
L97.501
Non-‐pressure chronic ulcer of other part of unspecified foot w/fat layer exposed
L97.502
Non-‐pressure chronic ulcer of other part of unspecified foot w/necrosis of bone
L97.504
Non-‐pressure chronic ulcer of other part of unspecified foot w/necrosis of muscle
L97.503
Non-‐pressure chronic ulcer of other part of unspecified foot w/unspecified severity
L97.509
Non-‐pressure chronic ulcer of right heel and midfoot limited to breakdown of skin
L97.411
Non-‐pressure chronic ulcer of right heel and midfoot with fat layer exposed
L97.412
Non-‐pressure chronic ulcer of right heel and midfoot with necrosis of bone
L97.414
Non-‐pressure chronic ulcer of right heel and midfoot with necrosis of muscle
L97.413
Non-‐pressure chronic ulcer of right heel and midfoot with unspecified severity
L97.419
Non-‐pressure chronic ulcer of unspecified heel and midfoot limited to breakdown of skin
L97.401
Non-‐pressure chronic ulcer of unspecified heel and midfoot with fat layer exposed
L97.402
Non-‐pressure chronic ulcer of unspecified heel and midfoot with necrosis of bone
L97.404
Non-‐pressure chronic ulcer of unspecified heel and midfoot with necrosis of muscle
L97.403
Non-‐pressure chronic ulcer of unspecified heel and midfoot with unspecified severity
L97.409
Other enthesopathy of left foot M77.52
Other enthesopathy of right foot M77.51 Other enthesopathy of unspecified foot M77.50 Other hammer toes (acquired) left foot M20.42 Other hammer toes (acquired) right foot M20.41 Other hammer toes (acquired) unspecified foot M20.40 Other specified diabetes mellitus with diabetic amyotrophy E13.44 Other specified diabetes mellitus with diabetic autonomic (poly)neuropathy
E13.43
Other specified diabetes mellitus with diabetic mononeuropathy E13.41 Other specified diabetes mellitus with diabetic neuropathic arthropathy
E13.610
Other specified diabetes mellitus with diabetic neuropathy, unspecified
E13.40
Other specified diabetes mellitus with diabetic polyneuropathy E13.42 Other specified diabetes mellitus with other diabetic neurological complication
E13.49
Other specified diabetes mellitus without complications E13.9 Other specified viral warts B07.8 Pain in left ankle and joints of left foot M25.572 Pain in left foot M79.672 Pain in left toe(s) M79.675 Pain in right ankle and joints of right foot M25.571 Pain in right foot M79.671 Pain in right toe(s) M79.674 Pain in unspecified ankle and joints of unspecified foot M25.579 Pain in unspecified foot M79.673 Pain in unspecified toe(s) M79.676 Peripheral vascular disease, unspecified I73.9 Peroneal tendinitis, left leg M76.72 Peroneal tendinitis, right leg M76.71 Peroneal tendinitis, unspecified leg M76.70 Plantar fascial fibromatosis M72.2 Plantar wart B07.0 Tinea unguium B35.1 Type 1 diabetes mellitus with diabetic autonomic (poly)neuropathy E10.43
Type 1 diabetes mellitus with diabetic mononeuropathy E10.41 Type 1 diabetes mellitus with diabetic neuropathic arthropathy E10.610 Type 1 diabetes mellitus with diabetic neuropathy, unspecified E10.40 Type 1 diabetes mellitus with diabetic polyneuropathy E10.42 Type 1 diabetes mellitus with other diabetic neurological complication
E10.49
Type 1 diabetes mellitus without complications E10.9 Type 2 diabetes mellitus with diabetic autonomic (poly)neuropathy E11.43
Type 2 diabetes mellitus with diabetic mononeuropathy E11.41 Type 2 diabetes mellitus with diabetic neuropathic arthropathy E11.610 Type 2 diabetes mellitus with diabetic neuropathy, unspecified E11.40 Type 2 diabetes mellitus with diabetic polyneuropathy E11.42 Type 2 diabetes mellitus with other diabetic neurological complication
E11.49
Type 2 diabetes mellitus without complications E11.9 Valgus (acquired), left ankle M21.072 Valgus (acquired), right ankle M21.071 Valgus (acquired), unspecified ankle M21.079 Valgus (congenital) Q66.6 Varus (congenital) Q66.3
The information provided is only intended to be a general summary and not intended to take place of either written law or regulations.