
“Social housing practices and financing schemes in Europe ...
Upload
alex-hakuzimanaCategory
view
45download
4
Mapping of HealthFinancing Schemes
in Rwanda
Alex HakuzimanaMPH/HSMP
Health Pol icy
July 2, 2014
Antwerpen, Belgium
1

Introduction
Growing evidence on low access to health care and catastrophic payments.
Every year,
• 1,300 million people with no access to affordable health services
• 150 million people suffer financial catastrophe
• 100 million pushed into poverty because of out-of-pocket payments at the entry point seeking healthservices.
2Xu K, Evans DB, Carrin G, Aguilar-Rivera AM, Musgrove P, Evans T. Protecting households from catastrophic health spending. Health Aff
(Millwood ) 2007 Jul;26(4):972-83

3
Path towards Universal Health Coverage (UHC)
WHO. The World Health Report 2010. Health systems financing: the path to universal coverage.
Ensure all people have
access to needed
services
Without risk of financial catastrophe
Well-functioning Health Financing
System

4
Where do we stand now?
Feasible in high income countries
Major reforms: BRICS, LICs e.g. Rwanda, Ghana, Georgia
No “one-fits-all”
Lessons & experiences e. g. Rwanda
“Know before you go”
Study on
UHC

Multicountry descriptive study on UHC
5
Mapping health care financing fragmentation
12 countries
Two CoPs: PBF & FAHSSame challenge: fragmentation
Hypothesis: many actors, different objectives

0
50
100
150
200
250
300
1990 1995 2000 2005 2010 2015MDG Target
Probability of child dying by age 5 per
1,000 live births
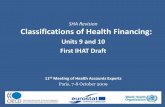
Child Mortality in Rwanda, 1990 – 2011
Rwanda
Sub-Saharan Africa
World
87 8273
6353 51
156
275
183
108
6054
178170
154
133
112109
29
5259
Farmer PE, Nutt CT, Wagner CM, Sekabaraga C, Nuthulaganti T, et al. (2013). “Reduced Premature Mortality in Rwanda: Lessons
from Success.” British Medical Journal 346(f65)
Rwanda, one of top performers to reach MDGs
6

7
Outcomes
. Whole architecture
. Process

Goal
Contribute to the Rwanda UHC path by
providing a comprehensive
overview on existing health care financing
schemes
Specific
List, describe, & analyse schemes
Compare with findings of multi-
country descriptive study on UHC
Recommendations on Rwanda & mapping
8
Objectives

Universal health Coverage: 3 dimensions
Population coverage
Fin
anci
al c
ove
rage
9

Hypothetical country: Health financing architecture
EPI
Pregnant women, under five children, poor, employees + affiliates to
schemes
Co-payment,
reimbursement
by a scheme
according to
user’s income,
salary, supply,
trainings, etc.
Primary care,
exempted services,
emergency and
referral services
SHICBHI
Private
10
Public input financing

Health Care Financing Scheme
• Building blocks or subsystems of a health financing system
• Financing arrangement through which people can getaccess to health care
• Features: coverage, resource collection, pooling andpurchasing
• Patterns: legal basis, institutional agent, source of fundsand time-bound
11

12
Document review: secondary data
Sources: policy documents, reports, websites,
databases, expert opinions, key informants, own
experience
Description and analysis of interaction/canvas:
conceptual framework.
Comparison with multi-country study: UHC
dimensions
Methods

13
Conceptual Framework
Kutzin J. A descriptive framework for country-level analysis of health care financing arrangements. Health Policy
2001 Jun;56(3):171-204
Funding flows
Benefit flows

14
General Government
Budget
Exemption Schemes (5)
Health Insurance
Schemes (4)
Performance-Based Financing
(PBF)
Through all other
schemes
- EPI- HIV/AIDS- TB- Malaria- MCH
- MedicalScheme
- MilitaryMedicalInsurance
- Community-Based HealthInsurance
- Private sector
Facility andcommunity-level
Actually, 11 schemes in Rwanda

Many health care financing schemes
2132
20
20
18
28
30
24
19
23
27
28
Source: Multi-country study report
Average= 23.8
15

16
C B H I - M u t u e l l e s d e s a n t e
Benefit package & coverage
Primary care package and referral care countrywide
Target population
Informal sector & rural
Financing
Premium contributions, subsidies (government & Global Fund) on a
fee-for-service schedule
Management & implementation:
Central entity, three-level pooling system

17
Financial protection
Mandatory health
insurance: 11% OOP in
2009/10
. Costly Co-payment and
referrals
. Spending gradient between schemes
Resource collection,
pooling and purchasing
.Reduction of transaction
costs
. Efficiency
. High external dependence
. Low contribution collection.
. Weak active purchasing
Provision of services
. Geographical access: good
. Benefit package
. More beneficial for
better-off
. Unmet need FP, chronic conditions,
referral abroad
Institutional arrangements
. Legal frameworks
. Aid Policy
. SWAp
. Merging
. Synergy
. High administrative
costs
. Still parallel systems
. Law enforcement

18
Financial protection, collection, pooling &
purchasing
Mandatory health insurance
and decline of OOP: 11%
No mandatory insurance
High OOP:
e.g. 65% Burundi
Population coverage
Universal insurance coverage
. No institutionalized
scheme
. Non operational pro-poor targeting
programs
Benefit package
Minimum essential
package & referral care
MDG & DCP-specific services
Rwanda
12 countries
Women and
< five children
High donor funding, mixed provider payment methods
Better-off, chronic care, NCD, referral abroad

19
Conclusion
Rwanda UHC cube not yet filled
Decline OOP but
expensive referral care
High external funding
Universal insurance
coverage with CLLC & NCD
Ownership & alignment
Research tools to be adapted to
context
Lessons for multi-country study participating
countries

20
Insufficient info for some schemes
Some data out of date
OOP excluded
Only national scale schemes included

21
Health Financing Strategy
Discuss on choices on UHC
Sustainability strategy
Improve pooling (CBHI to RSSB)
Review provider payment methods

22
Thank you for your attention















![[No. 37] STL Global Weekly Report Updated 150217](https://static.fdocuments.net/doc/165x107/568cab7e1a28ab186da5c8ef/no-37-stl-global-weekly-report-updated-150217.jpg)
