15 Hepatic Failure
60
Fulminant Hepatic Failure Fulminant Hepatic Failure in Children in Children John F. Sommerauer MD, FRCPC Children¶s Mercy Hospital University of Missouri-Kansas City Sue Sreedhar MD Medical College of Virginia Virginia Commonwealth University
-
Upload
kumar-gaurav-gupta -
Category
Documents
-
view
230 -
download
0
Transcript of 15 Hepatic Failure
8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 1/60
Fulminant Hepatic FailureFulminant Hepatic Failure
in Childrenin ChildrenJohn F. Sommerauer MD, FRCPC
Children¶s Mercy Hospital
University of Missouri-Kansas City
Sue Sreedhar MDMedical College of Virginia
Virginia Commonwealth University

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 2/60
Hepatic RegenerationHepatic Regeneration
Regenerating power of the liver is
well known
Perpetually regenerating liver in
Greek mythology - Prometheus

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 3/60
Liver FunctionsLiver Functions
Protein synthesis
Excretion of
metabolic wastesOxidative
phosphorylation
Breakdown of glycogen
Fatty acid oxidation
Synthesis of
cholesterol & bile
acidsEnzymes
NADPH
Cytochrome P-450 Cytochrome
reductase systems

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 4/60
Necessities for NormalL
iver FunctionNecessities for NormalL
iver Function
Adequate blood flow
20 ± 40% of cardiac output with only ~25% of
blood entering through the Hepatic Artery
Majority of blood flow comes from the portal
venous system
Oxygen Hepatocyte damage from hypoxia/hypotension
Low-pressure biliary system

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 5/60
Fulminant Hepatic Failure: BackgroundFulminant Hepatic Failure: Background
Fulminant hepatic failure in
children is a relatively rare clinical
syndrome - 2,000 patients/ yr. in theUSA (total ± adult and children)
Mortality rate is high- 60 to 80%
Challenge for the health care team

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 6/60
FHF: DefinitionsFHF: Definitions
FHFFHF - acute liver failure & encephalopathy within 8
weeks of signs and symptoms & without history or
physical evidence of chronic liver disease
Subfulminant HFSubfulminant HF- acute liver failure & encephalopathy
8 and 24 weeks after the onset of signs & symptoms
A Classification based on the time interval from the
onset of jaundice to the development of encephalopathy
Hyperacute LFHyperacute LF - within 7days
Acute LFAcute LF - within 8 to 28 days
Subacute LFSubacute LF - between 5 to 28 weeks

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 7/60
FHF: EtiologyFHF: Etiology -- InfectionsInfections
ViralViral
Hepatitis A, B,
C,, E, non-A,non-B, non-C
CMV
Herpes simplex Enterovirus
EBV
Parvovirus
HHV 6
Varicella ± zoster
Adenovirus
Leptospirosis

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 8/60
FHF: EtiologyFHF: Etiology ± ±Drugs and ToxinsDrugs and Toxins
ToxicityToxicity
Acetaminophen
Carbontetrachloride
Iron
Vitamin A
Mushrooms
Amanitaphalloides
Idiosyncratic reactionIdiosyncratic reaction
Phenytoin
Valproic acid INH
Halothane

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 9/60
FHF: EtiologyFHF: Etiology ± ± Metabolic DiseaseMetabolic Disease
Tyrosinemia
Galactosemia
Alpha-1 antitrypsindeficiency
Fatty acid oxidationdefects
Wilson¶s diseaseNeonatal iron storage
disease
Niemann-Pick disease
Hereditary fructose
intoleranceCF
Reye¶s syndrome
Mitochondrial electron
transport chain defectsFatty liver of pregnancy

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 10/60

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 11/60

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 12/60
FHF: Mechanisms of hepatic injuryFHF: Mechanisms of hepatic injury
Direct hepatocellular injury
Herpes virus family - HAV, HBV, HCV
Toxic or reactive metabolites - acetaminophen
Toxic metabolites of compounds - metabolic diseases
Immune mediated hepatocellular injury
Viral infections
Drug hepatotoxicity (dihydralazine, halothane)
Ischemic hepatocellular injury - shock states,
SIRS

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 13/60
FHF: Clinical FeaturesFHF: Clinical Features
FHF syndrome occurs from either acute
necrosis of a large mass of hepatocytes or the
sudden loss of hepatocellular function
Synthetic, excretory & metabolic functions are
impaired
Bacterial translocation, endotoxemia, activation
of macrophages, cytokine release, initiation of inflammatory cascade, circulatory compromise,
tissue hypoxia & end organ injury (SIRS)

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 14/60
Signs & SymptomsSigns & Symptoms
N/V, fatigue, anorexia, jaundice, ascites
Altered behavior (encephalopathy)
Euphoria, belligerence, foul language
Altered sleep, confusion, slurred speech,
disorientation, hyperventilation, lethargy,
hyperreflexia, unarousable, posturing
Increased bruisibility

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 15/60
Circulatory changesCirculatory changes
Hyperdynamic circulation
High cardiac output, low SVR
Pulmonary arteriovenous shunting
resulting in hypoxemia
Elevated portal pressure
Sodium and fluid retention
Marked renal vasoconstriction, ATN
8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 16/60
FHF: Clinical FeaturesFHF: Clinical Features
Hepatic injury ± elevated transaminases (ALT,AST)
Hepatic dysfunction
hypoglycemia
low cholesterol
coagulopathy (PT> 20 sec.) not correctable with
parenteral vitamin K
progressively rising bilirubin
hyperammonemia and encephalopathy
Absence of chronic liver disease - malnutrition, portal
hypertension, rickets, spider angioma, clubbing

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 17/60
FHF: Common ComplicationsFHF: Common Complications
Encephalopathy
Cerebral edema
Increased intracranial
pressure*
Hemorrhage, DIC,
Coagulopathy*
Cardiac & circulatory
instability
Pulmonary failure
Renal failure, MOSF,
MODS*
Hypoglycemia
(profound)
Acid-base
derangements
Sepsis*
* Most common causes of death

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 18/60
FHF: Hepatic encephalopathyFHF: Hepatic encephalopathy
HE ± is a reversible neuropsychiatric
syndrome - depressed LOC, seizures &/or
multifocal muscle twitching prior to coma
Absence of other factors that suppress brain
80% patients have cerebral (cytotoxic)
edema30-50% of patients have raised ICP

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 19/60

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 20/60
8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 21/60

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 22/60

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 23/60

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 24/60

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 25/60
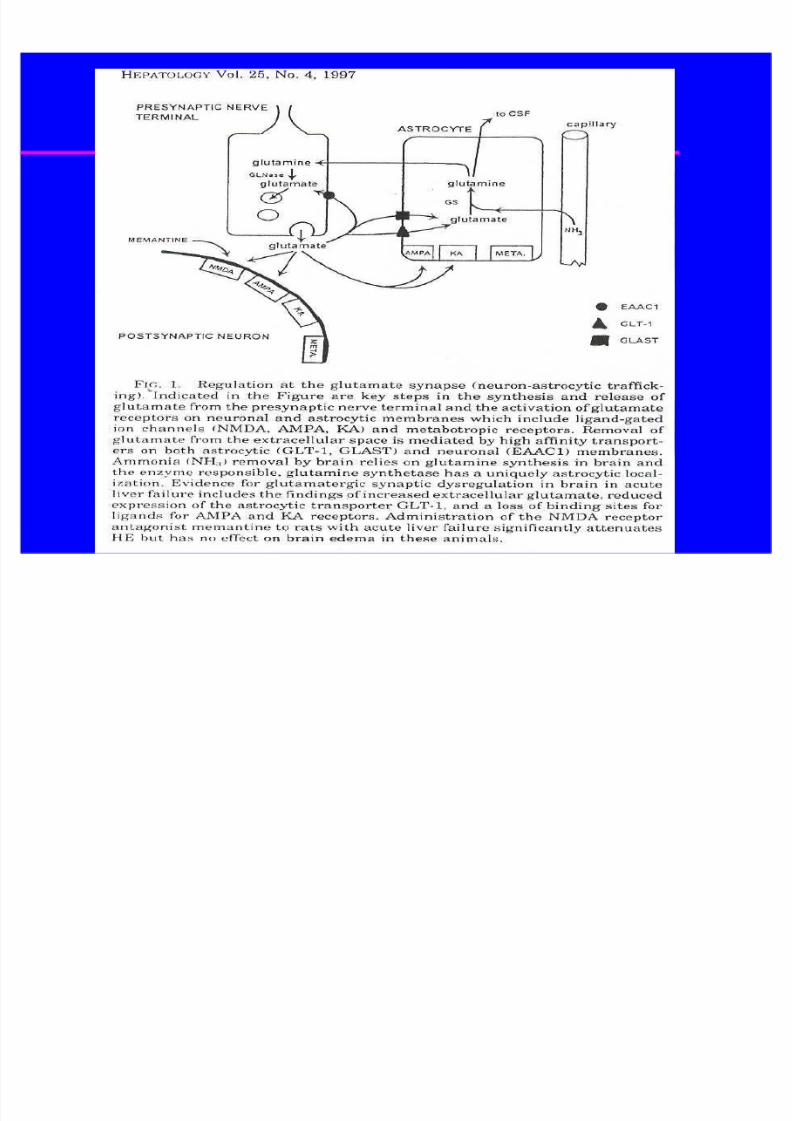
Pathophysiology of Cerebral EdemaPathophysiology of Cerebral Edema
Glutamine hypothesis
Ammonia detoxified in the cerebral astrocytes to
Glutamine which in turn is synthesized to glutamate
Osmotic effect of Glutamine
HE a result of Glutamine/ Glutamate cycling
dysregulation
? Use of Glutamine/ Glutamate inhibitors
Short chain fatty acids & mercaptan
Cerebral vasodilatation hypothesis, increased CBF
Blei: J. Hepatology 1999; 31:771

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 26/60
FHF: Goals of CareFHF: Goals of Care
Perform a comprehensive evaluation -
diagnosis & specific treatment (if available)
To prolong life, allow time for either nativeliver recovery (regeneration) or for donor
organ procurement & liver transplantation
Intervene with supportive care measures toprevent & ameliorate the complications of
FHF, and treat catastrophic events

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 27/60
FHF: History and ManagementFHF: History and Management
History - risk factors for hepatitis, HIV, H/O anesthesia or
ingestion, depression/suicidal behavior, initiation of
galactose or fructose, neuropsychiatric symptoms
PMH - chronic liver disease Family history - liver disease, neurologic disease,
emphysema, hepatitis, deaths in infancy
Physical exam - chronic liver disease, complications
Evaluation multidisciplinary team, early referral to transplant
center
a broad diagnostic evaluation unless clear etiology

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 28/60
FHF: Etiology and treatmentFHF: Etiology and treatment
Specific treatment - directed at the cause
Herpes and CMV - acyclovir /ganciclovir
Tyrosinemia - NTBC (nitrotrifluoromethylbenzoyl
cyclohexanedione)
N-acetylcysteine - acetaminophen
Neonatal iron storage disease - antioxidant and
iron-chelating cocktail (Se, Vit. E, n-acetylcysteine,
PGE1 and deferoxamine) Prevent further toxic injury: Acetominophen,
fructosemia, galactosemia
Early decision for transplant: Wilson¶s disease

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 29/60
FHF:Management and TreatmentFHF:Management and Treatment
Laboratory evaluation: Tests for
cause of FHF
functional status of the liver and other organs
Liver Biopsy - percutaneous needle, open surgical,
percutaneous jugular transvenous hepatic biopsy
CNS - EEG, VEP, SEP, CT scan of brain, MRI &
MRS
Monitoring: for complications
Radiology: CXR, Doppler abdominal sonography,
ECHO (if appropriate), CT scan of brain
8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 30/60
FHF: Supportive treatmentFHF: Supportive treatment
Maintain glucose (avoid hypoglycemia - D10W/D30W IV)
Maintain electrolytes (Na restricted, Hypophosphatemia -
KPhos infusions, Treat low K+, Ca++)
Maintain euvolemia with CVP monitoring - Diuresis withalbumin/blood products, fluid restriction
Maintain acid-base balance
Coagulation homeostasis
Hemodynamic & respiratory support to allow time for liver
regeneration or to bridge to liver transplantation
Prevent complications i.e. hemorrhage, cerebral edema, high
ICP

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 31/60
FHF:Management and TreatmentFHF:Management and Treatment
Nutrition:
NPO (initial stage)
Low Na+, low protein diet (stable - stage 1 or 2 HE)
TPN - use highest concentration of glucose tolerated
Amino acid (trophamine) 0.5 to 1.0 g/kg/day
Lipids (20% solution) 0.5 - 3 g/kg/day, ( triglycerides
< 250 mg/dl ) GI prophylaxis - H2 receptor antagonist - maintain
gastric pH > 4.0

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 32/60
FHF:Management of CoagulopathyFHF:Management of Coagulopathy
Vitamin K - 0.2 mg/kg/day (max. 10 mg) iv X 3
days, then every other day
Maintain PT at 20 - 25 sec (if no active bleeding)Maintain PT at < 20 sec ( if active bleeding )
Maintain Platelet count > 50,000 / ul
Maintain Hematocrit > 30%
FFP infusions for active bleeding
Plasmapheresis should be considered when
there is severe coagulopathy and/or bleeding

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 33/60
FHF:Management of EncephalopathyFHF:Management of Encephalopathy
Lactulose 0.5 ml/kg/dose (max. 30 ml/dose) PO/NG q.i.d.
for 3-4 loose stools (contraindicated in intestinal ileus )
Neomycin (vancomycin or metronidazole) not indicated -
not efficacious, significant GI absorption with toxicity
Sedation and Analgesia:
Avoid agents which may exacerbate HE
Agents initiated at low doses and intermittently
benzodiazepines - midazolam
opiates - fentanyl, remifentanyl
Continuous infusions are contraindicated

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 34/60
FHF: Intracranial HypertensionFHF: Intracranial Hypertension
ICP monitoring: controversial
signs and symptoms of raised ICP
stage 4 HE, rapidly progressing stage 3 HE
cerebral edema on CT scan (plasmapheresis prior to
catheter placement)
ICP therapy - ICP < 20 mmHg & CPP > 50 mmHg
Caution when using osmolar therapy
Barbiturate coma may be used if necessary
EEG monitoring
CVVH, plasmapheresis

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 35/60
FHF:FHF: PlasmapheresisPlasmapheresis
Double blood volumeDouble blood volume
exchangeexchange (1 -2 /day)
stage 3 or stage 4 HE active hemorrhage
severe coagulopathy
raised ICP
prior to procedures prior to OLTx with
ABO incompatible
graft
EffectEffect
reduces NH3
corrects PT controls
intravascular
volume
cerebral edemaor HE?
(inconsistent )

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 36/60
FHF: Bridge to transplantFHF: Bridge to transplant
Continuous veno-venous
hemofiltration
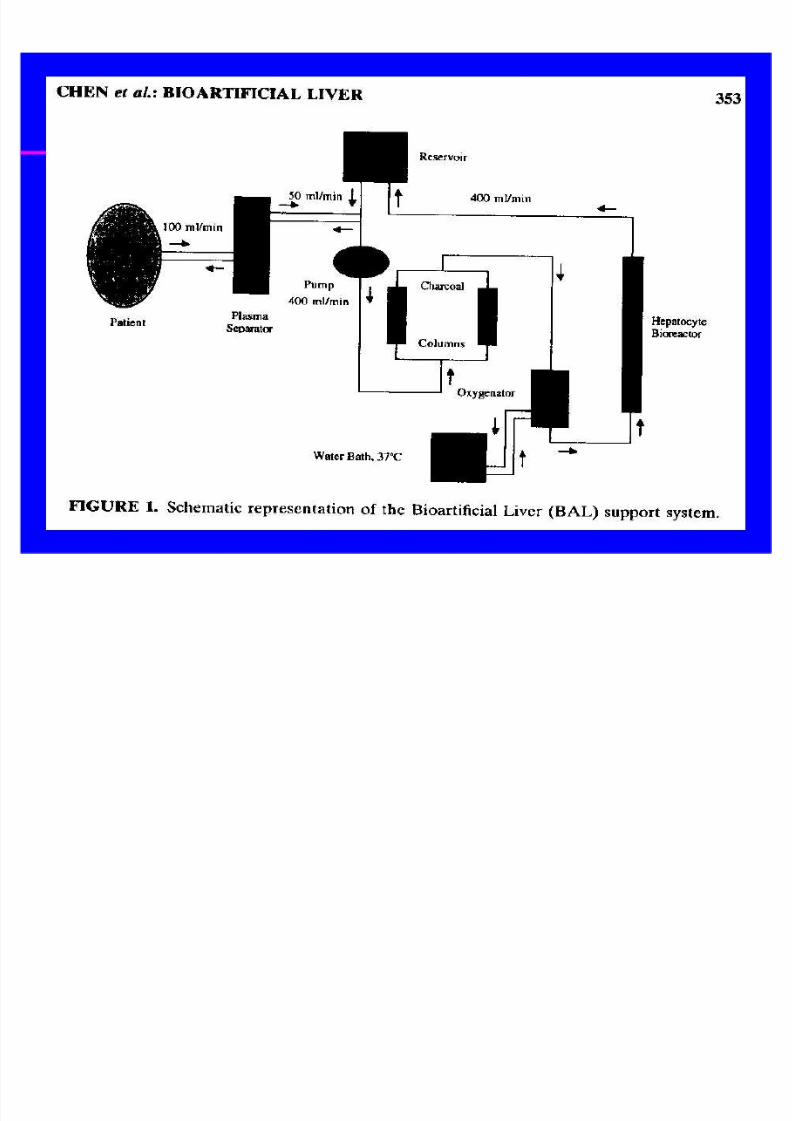
Bio-artificial liver support system
Liver cell transplantation
These techniques remain experimental

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 37/60
FHF: Extracorporeal liver support systemsFHF: Extracorporeal liver support systems
Non biologic systems:Non biologic systems:
- CVVH, charcoal hemoperfusion, plasmapheresis
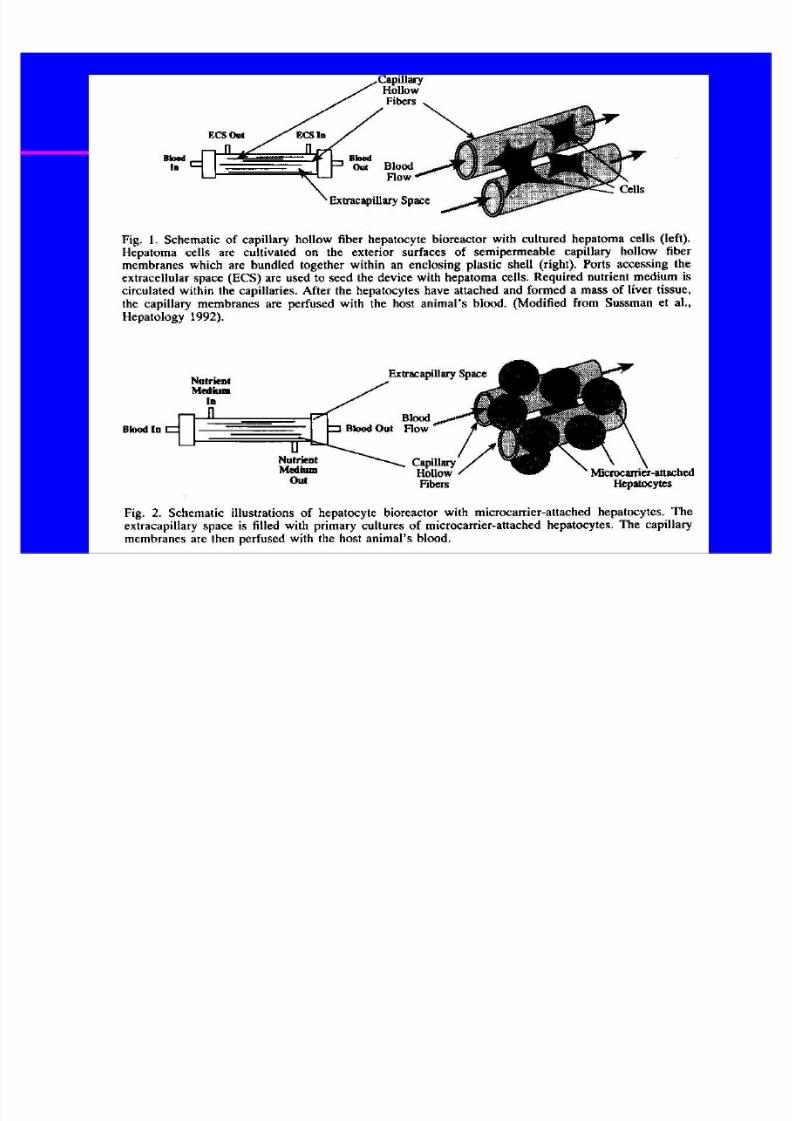
Biologic systems:Biologic systems:
- Extracorporeal circuits utilizing a hollow fiber
cartridge loaded with biologically active hepatocytes:
- human hepatoma cell (ELAD)
- porcine hepatocytes (BAL)
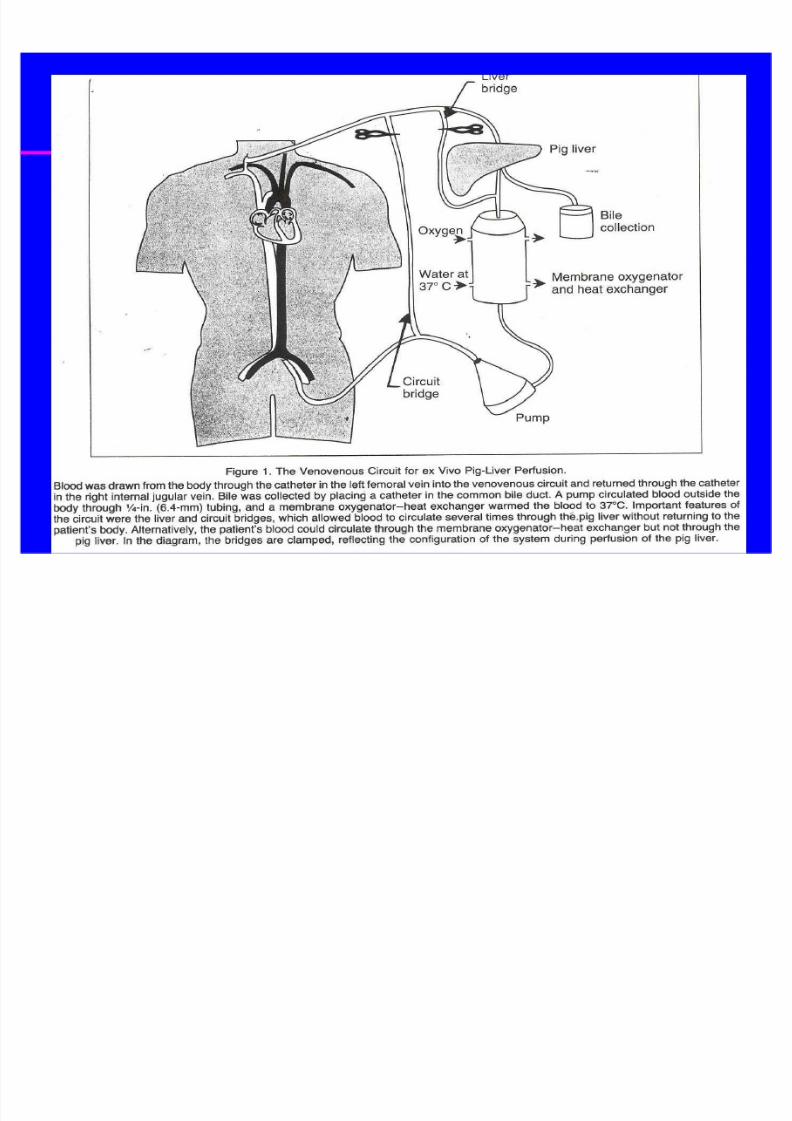
- Whole liver perfusion systems:
- human livers
- porcine livers - unaltered or transgenic
8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 38/60
8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 39/60

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 40/60
8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 41/60

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 42/60
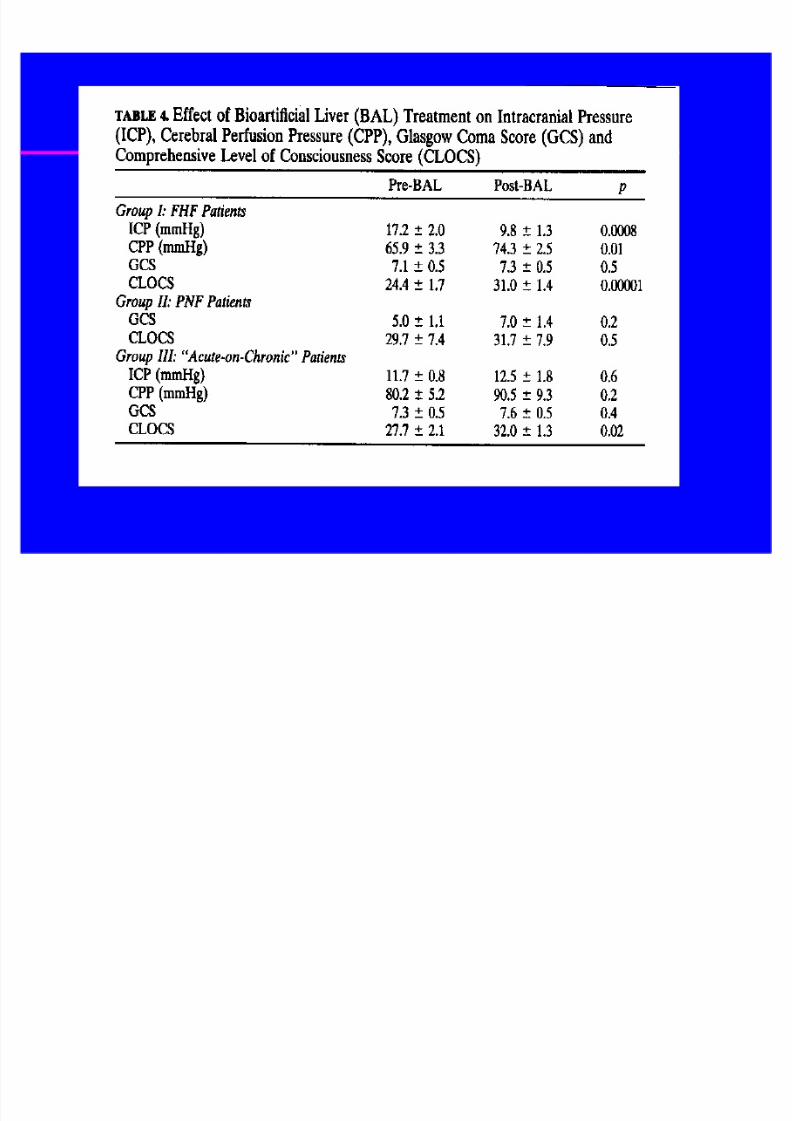
BioBio--artificial liver support systemartificial liver support system
Extracorporeal liver perfusion via an
oxygenated heparinized circuit
Neurologic state & liver functionimprove within hours on the circuit
Decreased ICP, decreased pressor
support requirement, improved urine
output
Goss, Arch Surg 1998; 133:839
8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 43/60
8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 44/60

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 45/60
Liver cell transplantation: ExperimentalLiver cell transplantation: Experimental
Provides temporarymetabolic support
Transplanted intonative liver orspleen, acts as anectopic liver
Sustains life untildonor becomesavailable
Harvested liver cellsfrozen at -90o c,stored in liquidnitrogen
Percutaneoustranshepatic or
femoral arterialapproach to accessthe splenic artery

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 46/60
Hepatocyte transplantation: PrinciplesHepatocyte transplantation: Principles
Hepatocytes are isolated from cadaveric liver grafts
Hepatocytes are infused into the portal vein - seed
the native liver
Standard immunosuppression is required
Hepatocytes proliferate and express differentiated
function
Provide temporary liver function in models of liverfailure
Correct metabolic defects

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 47/60
Hepatocyte transplantation: AdvantagesHepatocyte transplantation: Advantages
Act as a bridge to native
liver recovery
If recovery occurs, the
immunosuppression maybe discontinued & graft
allowed to atrophy to
avoid long term
immunosuppression Reduced cost
Increase the donor pool
for other recipients
In metabolic diseases -
can provide the
necessary enzymes to
correct the deficiencyand yet allows the
patient to continue to
utilize their native liver
Hepatocytes could begenetically manipulated
Multiple infusions
possible if needed

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 48/60
FHF: Auxiliary liver transplantation (AOLT)FHF: Auxiliary liver transplantation (AOLT)
Potential Advantages:
AOLT acts as a bridge to native liver recovery
if recovery occurs, immunosuppression may bediscontinued and the graft removed or allowed to
atrophy to avoid long term immunosuppression
in metabolic diseases AOLT can provide the
necessary enzymes to correct the deficiency andyet allows the patient to continue to utilize their
native liver

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 49/60
Hepatic Transplantation: AuxiliaryHepatic Transplantation: Auxiliary

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 50/60
Fulminant Hepatic Failure in Children:Fulminant Hepatic Failure in Children:
Predictive Factors and OutcomesPredictive Factors and OutcomesOverall survival for patients with FHF and
stage 3 or 4 HE has increased from 20% to
50% over past 2 decades. (Without transplant)
The best independent predictor of outcome isthe etiology of the FHF.
Survival
acetaminophen 40 - 64%
Non-ABC hepatitis < 20%Wilson¶s disease < 5%
Without OLTx - survival ~30%

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 51/60

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 52/60
FHF: Predictive Factors & OutcomesFHF: Predictive Factors & Outcomes
Predictive factors of poor outcome:
Several studies combined
etiology stage 3 or 4 coma (HE)
marked coagulopathy (PT > 100 sec, INR > 4)
factor V or factor VII levels < 15%
cerebral edema and raised ICP GI hemorrhage
MOF
8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 53/60
FHF: Indications for TransplantFHF: Indications for Transplant
3rd to 4th degree encephalopathy
Rising bilirubin (> 20mg/100ml)
Falling transaminases
Coagulopathy with prolonged PT >
100 seconds and Factor II, V, VII
decreased to < 20% of normal values
Acute renal decompensation

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 54/60
Status 1 - acute or chronic liver failure
(CLD), life expectancy < 7days without LTx
and 1 of the following:
FHF On ventilator
Upper GI bleed
Stage 3 or 4 HE
Refractory ascites Biliary sepsis
Hepatic artery thrombosis or Primary non-function
Hepatorenal syndrome
FHF:Hepatic TransplantationFHF:Hepatic Transplantation ± ± UNOSUNOS
Status designation in pediatricsStatus designation in pediatrics

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 55/60
Whole Organ Liver TransplantationWhole Organ Liver Transplantation

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 56/60
Reduced Sized Liver Transplantation: AnatomyReduced Sized Liver Transplantation: Anatomy

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 57/60
Indications for TransplantationIndications for Transplantation-- all patientsall patients
Biliary
hypoplasia
5%
Hepatitis
5%
Other
16%
Idiopathic
cirrhosis
6%Acute liver
necrosis
11%Metabolic
13%
Biliaryatresia
44%

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 58/60
Common causes leading to liver transplantCommon causes leading to liver transplant
Neonatal hepatitis in <4 month
Biliary atresia in < 3 years
Acetaminophen toxicity in teenagers
Metabolic disorders, acute liver necrosis,
idiopathic cirrhosis, biliary hypoplasia,
autoimmune hepatitis, tumors, CF

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 59/60
Status 1Status 1 -- FHF vs. Chronic liver disease patients: DiagnosisFHF vs. Chronic liver disease patients: Diagnosis
HF= 1
-CLD=
iral Hep. iliar tresia 1
o in C H
eta olic Dis. eonatal Hep.
cute e ection 1 C stic Fi rosis 1
n no n ther

8/6/2019 15 Hepatic Failure
http://slidepdf.com/reader/full/15-hepatic-failure 60/60
Status 1Status 1 -- FHF vs. Chronic liver disease patients: Post LTxFHF vs. Chronic liver disease patients: Post LTx