14/09/2015 and Neck Tumours - CPD University of Toronto · Head and Neck Tumours ... • Irregular...
9
14/09/2015 1 Head and Neck Tumours What the clinician wants to know? M.Machnowska, MD FRCPC Sunnybrook Health Sciences Centre • Perineural spread – Pterygopalatine fossa and skull base • Lymph node involvement – Nodal spread in thyroid and nasopharyngeal ca. – Determining radiologic evidence of extracapsular disease • Invasion into adjacent structures – Laryngeal and thyroid cancers Perineural Spread • Which of these nerves does not course into the pterygopalatine fossa? – A) V2 – B) Greater palatine nerve – C) V1 – D) Vidian nerve Lymph nodes • What is the typical route of nodal spread of NPC? – A) Retropharyngeal, level II, level V, level III – B) Level I, level II, level III, level IV – C) Level II, Level III, retropharyngeal, level V – D) Retropharyngeal, level II, level III, level IV, supraclavicular, level V Lymph nodes • Which of these radiologic features suggest extracapsular disease spread? – A) Increased nodal enhancement – B) Ill defined nodal margins following biopsy – C) Internal cystic change in nodes from HPV positive cancers – D) Invasion of adjacent structures Invasion of adjacent structures • Invasion into which structure constitutes a T4 glottic cancer – A) Invasion of the arytenoid cartilage – B) Invasion of the inner cortex of the thyroid cartilage – C) Invasion through the thyroid cartilage – D) All of the above
Transcript of 14/09/2015 and Neck Tumours - CPD University of Toronto · Head and Neck Tumours ... • Irregular...

14/09/2015
1
Head and Neck Tumours
What the clinician wants to know?
M.Machnowska, MD FRCPC
Sunnybrook Health Sciences Centre
• Perineural spread– Pterygopalatine fossa and skull base
• Lymph node involvement– Nodal spread in thyroid and nasopharyngeal ca.– Determining radiologic evidence of extracapsulardisease
• Invasion into adjacent structures– Laryngeal and thyroid cancers
Perineural Spread
• Which of these nerves does not course into the pterygopalatine fossa?
– A) V2
– B) Greater palatine nerve
– C) V1
– D) Vidian nerve
Lymph nodes
• What is the typical route of nodal spread of NPC?
– A) Retropharyngeal, level II, level V, level III
– B) Level I, level II, level III, level IV
– C) Level II, Level III, retropharyngeal, level V
– D) Retropharyngeal, level II, level III, level IV, supraclavicular, level V
Lymph nodes
• Which of these radiologic features suggest extracapsular disease spread?
– A) Increased nodal enhancement
– B) Ill defined nodal margins following biopsy
– C) Internal cystic change in nodes from HPV positive cancers
– D) Invasion of adjacent structures
Invasion of adjacent structures
• Invasion into which structure constitutes a T4 glottic cancer
– A) Invasion of the arytenoid cartilage
– B) Invasion of the inner cortex of the thyroid cartilage
– C) Invasion through the thyroid cartilage
– D) All of the above

14/09/2015
2
Tumours at risk for perineural spread
• Cutaneous malignancies
• Nasopharynx
• Tumours of the palate
• Tumours of the parotid
• Small salivary gland tumours– Adenoid cystic carcinoma
– Mucoepidermoid carcinoma
Primary Site
Type
Why is it important?
• It often precludes the possibility of a surgical cure
• Full extent of spread needs to be mapped out for radiation planning
V1
V2
V3
VII
Pterygopalatine fossa
CASES

14/09/2015
3
Nasopharyngeal ca. Nasopharyngeal ca.
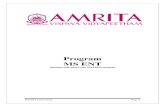
Nasopharyngeal ca. Adenoid cystic
14/09/2015
4
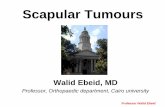
Adenoid cystic Adenoid cystic
Lymph nodes Nasopharyngeal cancer
• Nodal spread is first to retropharyngeal nodes
– N1 disease whether unilateral or bilateral
– Better characterized as discrete nodal disease on MRI
– May be mistaken for tumour on CT
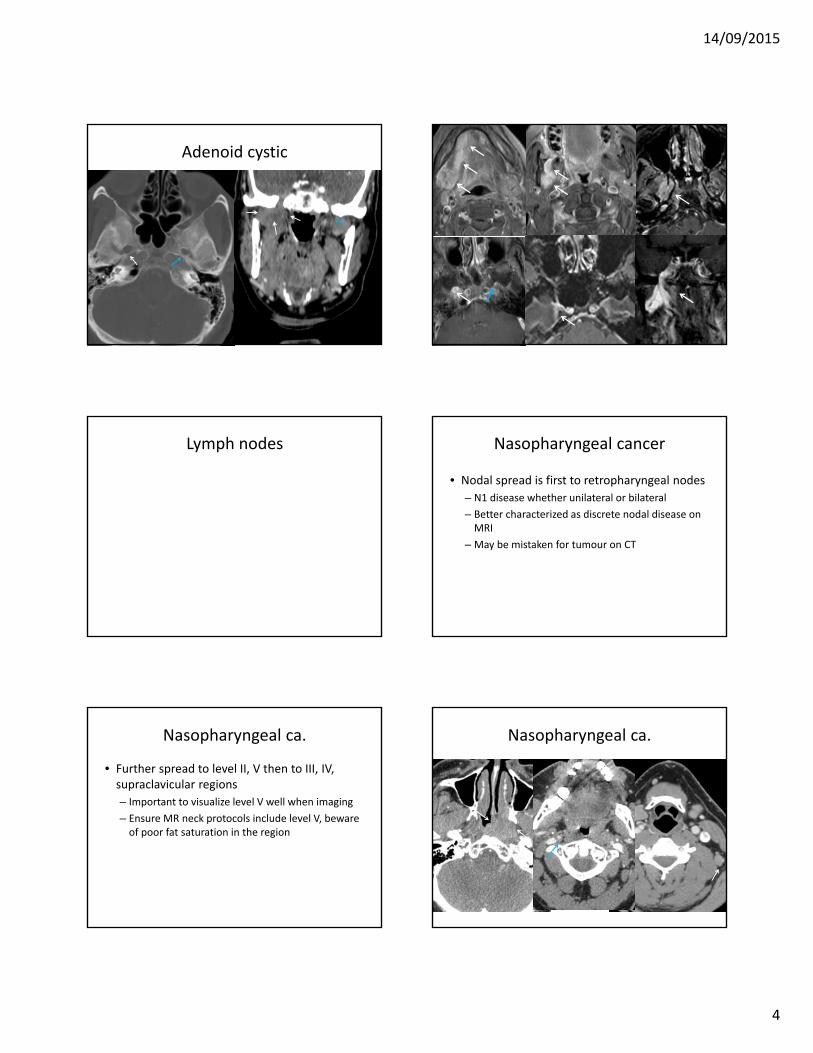
Nasopharyngeal ca.
• Further spread to level II, V then to III, IV, supraclavicular regions
– Important to visualize level V well when imaging
– Ensure MR neck protocols include level V, beware of poor fat saturation in the region
Nasopharyngeal ca.

14/09/2015
5
Nasopharyngeal ca. Nasopharyngeal ca.
Thyroid cancer
• Lymph node metastases frequently involve the pretracheal and paratracheal nodes within level VI
• Progression can be lateral to III and IV or inferior to level VII (mediastinum)
• 20% of patients have a lymphatic vessel connecting the upper pole of the thyroid to the retropharyngeal lymphatics
• Spread tends to occur if other levels are involved or the neck has been previously treated
Previously resected thyroid ca. Extracapsular spread
• Invasion of adjacent tissues
• Irregular nodal boundaries
• Streaky changes of adjacent fat planes
• >3 matted nodes with effacement of intervening fat
• Necrotic nodes (in HPV –ve tumours)
Chai et al. JAMA Otol Head Neck Surg 2013;139:1187–1194.Url et al. Eur J Rad 2013; 82: 1783– 1787Aiken et al. AJNR 2015; 36: 1776‐1781

14/09/2015
6
Radiologic Diagnosis of ExtracapsularSpread
• Sensitivity from 60% to 90%
• Specificity from 70% to 90%
• CT accuracy is generally lower for HPV positive tumours
Chai et al. JAMA Otol Head Neck Surg 2013;139:1187–1194.Url et al. Eur J Rad 2013; 82: 1783– 1787Aiken et al. AJNR 2015; 36: 1776‐1781
Invasion of adjacent structures
• Laryngeal ca.
• Thyroid
Hyoepiglotticligament
Pre‐epilotticspace
Pre‐epilotticspace
Paraglotticfat
Paraglottic spaceThyroarytenoidm
Laryngealventricle
True vc
False vc
Arytenoidcartilage
Thyroarytenoidtunnel
cricoid
thyroid
Tracheal ring
Laryngeal ca.
• Glottic ca.– T1, tumor limited to the vocal cord (may involve anterior or posterior commissure) with normal mobility
– T2, tumor extension to the supraglottis and/or subglottisand/or impaired vocal cord mobility
– T3, tumor limited to larynx with vocal cord fixation and/or paraglottic space, and/or inner cortex of thyroid cartilage
– T4, tumor invasion through the thyroid cartilage and/or other tissues beyond the larynx (eg, trachea or soft tissues of the neck, including the thyroid and pharynx)
Edge S, Byrd D, Compton C, et al. American Joint Committee on Cancer. AJCC cancer staging manual, 7th edition. New York: Springer‐Verlag;
2010

14/09/2015
7
Laryngeal ca.
• Glottic ca.– T1, tumor limited to the vocal cord (may involve anterior or posterior commissure) with normal mobility
– T2, tumor extension to the supraglottis and/or subglottisand/or impaired vocal cord mobility
– T3, tumor limited to larynx with vocal cord fixation and/or paraglottic space, and/or inner cortex of thyroid cartilage
– T4, tumor invasion through the thyroid cartilage and/or other tissues beyond the larynx (eg, trachea or soft tissues of the neck, including the thyroid and pharynx)
Edge S, Byrd D, Compton C, et al. American Joint Committee on Cancer. AJCC cancer staging manual, 7th edition. New York: Springer‐Verlag;
2010
Laryngeal ca.
• Glottic ca.– T1, tumor limited to the vocal cord (may involve anterior or posterior commissure) with normal mobility
– T2, tumor extension to the supraglottis and/or subglottisand/or impaired vocal cord mobility
– T3, tumor limited to larynx with vocal cord fixation and/or paraglottic space, and/or inner cortex of thyroid cartilage
– T4, tumor invasion through the thyroid cartilage and/or other tissues beyond the larynx (eg, trachea or soft tissues of the neck, including the thyroid and pharynx)
Edge S, Byrd D, Compton C, et al. American Joint Committee on Cancer. AJCC cancer staging manual, 7th edition. New York: Springer‐Verlag;
2010
Laryngeal ca.
• Supraglottic ca.– T1, tumor limited to 1 subsite of the supraglottis with normal vocal cord mobility
– T2, tumor invasion of the mucosa of more than 1 adjacent subsite of the supraglottis or glottis or of a region outside the supraglottis (eg, mucosa of base of tongue, vallecula, medial wall of pyriform sinus), without fixation of the larynx
– T3, tumor limited to the larynx with vocal cord fixation and/or invasion of any of the postcricoid area or pre‐epiglottic tissues
– T4, tumor invasion through the thyroid cartilage and/or extension into soft tissues of the neck, thyroid, and/or esophagus
Edge S, Byrd D, Compton C, et al. American Joint Committee on Cancer. AJCC cancer staging manual, 7th edition. New York: Springer‐Verlag;
2010
Laryngeal ca.
• Supraglottic ca.– T1, tumor limited to 1 subsite of the supraglottis with normal vocal cord mobility
– T2, tumor invasion of the mucosa of more than 1 adjacent subsite of the supraglottis or glottis or of a region outside the supraglottis (eg, mucosa of base of tongue, vallecula, medial wall of pyriform sinus), without fixation of the larynx
– T3, tumor limited to the larynx with vocal cord fixation and/or invasion of any of the postcricoid area or pre‐epiglottic tissues
– T4, tumor invasion through the thyroid cartilage and/or extension into soft tissues of the neck, thyroid, and/or esophagus
Edge S, Byrd D, Compton C, et al. American Joint Committee on Cancer. AJCC cancer staging manual, 7th edition. New York: Springer‐Verlag;
2010
Laryngeal ca.
• Supraglottic ca.– T1, tumor limited to 1 subsite of the supraglottis with normal vocal cord mobility
– T2, tumor invasion of the mucosa of more than 1 adjacent subsite of the supraglottis or glottis or of a region outside the supraglottis (eg, mucosa of base of tongue, vallecula, medial wall of pyriform sinus), without fixation of the larynx
– T3, tumor limited to the larynx with vocal cord fixation and/or invasion of any of the postcricoid area or pre‐epiglottic tissues
– T4, tumor invasion through the thyroid cartilage and/or extension into soft tissues of the neck, thyroid, and/or esophagus
Edge S, Byrd D, Compton C, et al. American Joint Committee on Cancer. AJCC cancer staging manual, 7th edition. New York: Springer‐Verlag;
2010
Laryngeal ca
• Subglottic ca.– T1, tumor limited to the subglottis
– T2, tumor extension to a vocal cord with normal or impaired mobility
– T3, tumor limited to the larynx with vocal cord fixation
– T4, tumor invasion through cricoid or thyroid cartilage and/or extension to other tissues beyond the larynx (eg, trachea or soft tissues of neck, including the thyroid and esophagus)
Edge S, Byrd D, Compton C, et al. American Joint Committee on Cancer. AJCC cancer staging manual, 7th edition. New York: Springer‐Verlag;
2010

14/09/2015
8
Laryngeal ca
• Subglottic ca.– T1, tumor limited to the subglottis
– T2, tumor extension to a vocal cord with normal or impaired mobility
– T3, tumor limited to the larynx with vocal cord fixation
– T4, tumor invasion through cricoid or thyroid cartilage and/or extension to other tissues beyond the larynx (eg, trachea or soft tissues of neck, including the thyroid and esophagus)
Edge S, Byrd D, Compton C, et al. American Joint Committee on Cancer. AJCC cancer staging manual, 7th edition. New York: Springer‐Verlag;
2010
Laryngeal ca
• Subglottic ca.– T1, tumor limited to the subglottis
– T2, tumor extension to a vocal cord with normal or impaired mobility
– T3, tumor limited to the larynx with vocal cord fixation
– T4, tumor invasion through cricoid or thyroid cartilage and/or extension to other tissues beyond the larynx (eg, trachea or soft tissues of neck, including the thyroid and esophagus)
Edge S, Byrd D, Compton C, et al. American Joint Committee on Cancer. AJCC cancer staging manual, 7th edition. New York: Springer‐Verlag;
2010
Thyroid cancer
• T1 Tumor 2 cm or less in greatest dimension limited to the thyroid
• T2 Tumor more than 2 cm but not more than 4 cm in greatest dimension, limited to the thyroid
• T3 Tumor more than 4 cm in greatest dimension limited to the thyroid, or any tumor with minimal extrathyroidextension (eg, extension to sternothyroid muscle or perithyroid soft tissues)
• T4a Tumor of any size extending beyond the thyroid capsule to invade subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve
• T4b Tumor invades prevertebral fascia or encases carotid artery or mediastinal vessels
Greene FL, Trotti A, Fritz AG, et al, editors. AJCC Cancer staging handbook. 7th edition. Chicago: American Joint Committee on Cancer;
2010. Chapter 7: Major Salivary Glands
Thyroid cancer
• T1 Tumor 2 cm or less in greatest dimension limited to the thyroid
• T2 Tumor more than 2 cm but not more than 4 cm in greatest dimension, limited to the thyroid
• T3 Tumor more than 4 cm in greatest dimension limited to the thyroid, or any tumor with minimal extrathyroidextension (eg, extension to sternothyroid muscle or perithyroid soft tissues)
• T4a Tumor of any size extending beyond the thyroid capsule to invade subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve
• T4b Tumor invades prevertebral fascia or encases carotid artery or mediastinal vessels
Greene FL, Trotti A, Fritz AG, et al, editors. AJCC Cancer staging handbook. 7th edition. Chicago: American Joint Committee on Cancer;
2010. Chapter 7: Major Salivary Glands
14/09/2015
9
Perineural Spread
• Which of these nerves does not course into the pterygopalatine fossa?
– A) V2
– B) Greater palatine nerve
– C) V1
– D) Vidian nerve
Lymph nodes
• What is the typical route of nodal spread of NPC?
– A) Retropharyngeal, level II, level V, level III
– B) Level I, level II, level III, level IV
– C) Level II, Level III, retropharyngeal, level V
– D) Retropharyngeal, level II, level III, level IV, supraclavicular, level V
Lymph nodes
• Which of these radiologic features suggest extracapsular disease spread?
– A) Increased nodal enhancement
– B) Ill defined nodal margins following biopsy
– C) Internal cystic change in nodes from HPV positive cancers
– D) Invasion of adjacent structures
Invasion of adjacent structures
• Invasion into which structure constitutes a T4 glottic cancer
– A) Invasion of the arytenoid cartilage
– B) Invasion of the inner cortex of the thyroid cartilage
– C) Invasion through the thyroid cartilage
– D) All of the above