1315 Lyme and Filariais A Wolbachia Connection: A Case · Lyme and Filariais A Wolbachia...
1
Introduction *As travel and immigration increases, health care providers must consider neglected tropical and endemic diseases. *Lymphatic filariasis is a mosquito-borne tropical disease and 120 million people in Africa are infected. *Lymphatic filariasis, endemic to Africa, is a neglected disease caused by Wuchereria bancrofti and can result in chronic disease that can be easily overlooked in immigrants coming to North America. *The symbiotic bacteria, Wolbachia, has been recently identified as a chemotherapeutic target for anti-filarial therapy. *Lyme disease, a common tick-borne illness due to Borrelia burgdorferi is endemic to North America. *We have taken advantage of the symbiotic relationship between filaria and Wolbachia to treat a recent immigrant with both Lyme disease and filariasis. A 1) Albany Medical College, Division of Internal Medicine-Pediatrics, Albany, NY. 2) Albany Medical College, Division of Internal Medicine, Albany, NY. 3) Albany Medical Center, Division of Infectious Disease, Albany, NY. Lyme and Filariais A Wolbachia Connection: A Case Jessica A. Kumar, MD, MPH, Graham Atkins, MD, Richard Blinkhorn, MD 1 1315 2 2, 3 Abstract: Health care providers must consider neglected tropical and regional endemic diseases. Lyme disease, commonly found in North Americarequires a diagnosis of erythema migrans with confirmatory serology. Lymphatic filariasis, endemic to Africa, is a neglected chronic disease thatcan be easily overlooked in immigrants coming to North America. Wepresent a case of a 21 year old Liberian male complaining of one weekof right knee pain and swelling during the summer. He had a historyof malaria and filariasis. He immigrated to Albany, New York eighteenmonths ago as a refugee from civil war and was taking isoniazid andpyridoxine for a positive tuberculin test. He had no known tick exposure or trauma. He was afebrile and hemodynamically stable complaining of rightknee discomfort, warmth, swelling and decreased range of motion. Hiswhite blood cell count was 4.7 with 52% neutrophils, 26% lymphocytes,9% eosinophils and 12% monocytes. C-reactive protein (101 mg/L) erythrocyte sedimentation rate (73 mm/hr) and IgE level (4123 U/ml) were elevated. Knee radiograph showed joint effusion. Synovial fluid aspirationcontained 116.5 tho/cmm white cells (95% neutrophils) but gram stain and culture were negative. Lyme PCR from synovial fluid was notsubmitted for analysis. Lyme C6 peptide was positive as was confirmatoryWestern blot which demonstrated IgG bands 18, 23, 30, 31, 39, 41, 58 and 93. Antifilarial IgG4 was positive indicative of past or chronic infection with filariasis. A course of Doxycycline was initiated for the managementof both acute Lyme arthritis and chronic filariasis. Antifilarial therapywith Doxcycline was directed toward the symbiotic bacteria, Wolbachia associated with microfilaria. While it is possible our patient’s positive Lymeserology reflected cross reacting antigens to filaria; his clinical presentationwas consistent with Lyme associated arthritis. This case is unique in that antimicrobial management of one endemic infection was useful in the management of a geographically separate pathogen. Case Presentation *A 21 year old Liberian male complained of one week of right knee pain and swelling during the summer. *He had a history of malaria and filariasis. *He immigrated to Albany, New York eighteen months earlier as a refugee from civil war and was taking isoniazid and pyridoxine for a positive tuberculin test. *He did not recall a tick bite or trauma. *Vital signs were normal. *Physical exam was notable for right knee warmth, swelling and decreased range of motion. *He had no rash, lymphedema or hydrocoele. *His white blood count was 4.7 with 52% neutrophils, 26% lymphocytes, 12% monocytes and 9% eosinophils, *Serum IgE level (4123 U/ml) was elevated. *Knee radiograph showed joint effusion. *Synovial fluid aspiration contained 116.5 tho/cmm white cells (95% neutrophils) and no crystals were identified. *Gram stain revealed no organisms, and bacterial culture was negative. *Lyme PCR from synovial fluid was not submitted for analysis. *Serum Lyme C6 peptide was positive as was confirmatory Western blot which demonstrated IgG bands 18, 23, 30, 31, 39, 41, 58 and 93. *Serum antifilarial antibody IgG4 EIA was positive. *A diagnosis of Lyme arthritis as well as filariasis were established. Microfilaria of Wuchereria bancrofti and spirochetes of Lyme disease (CDC Photo; Centers for Disease Control and Prevention's Public Health Image Library ) Management *He received a 28 day course of doxycycline 100mg twice daily for both Borrelia burgdorferi and filariasis. *We chose not to administer ivermectin, albendazole or diethylcarbamazine. *At follow-up visits, he was in good health and his knee effusion resolved. Discussion *This case illustrates the unusual crossroads of two geographically separate infectious diseases that may occur with increasing frequency due to the ease of foreign travel. *Whereas Lyme disease is highly prevalent in the Northeastern United States, filariasis is highly prevalent in Africa. *Our patients infectious diseases happened to have been acquired by two different arthropod vectors. *We recognized a unique commonality that permitted the use of one anti-microbial agent to treat two diverse infections. *Wolbachia are endosymbionts of filarial parasites -Essential for larval molting -Female worm fertility -Adult worm survival *Doxycycline possess anti-Wolbachia activity. -Animal and human trials demonstrate macrofilaricidal activity -Reduction in lymph vessel dilation -Absence of inflammatory reaction to filarial death *Doxycycline is the treatment of choice for Lyme disease. Conclusion *This case is unique in that antimicrobial management of one endemic infection was useful in the management of a geographically separate pathogen. *The unique relationship between Wolbachia and filarial has significantly changed the approach to anti-filarial therapy. References 1) Addiss, D.G. and Dreyer, G. Treatment of Lymphatic Filariasis. https://apps.who.int/ctd/filariasis/docs/chap7.pdf. 2) Deborah, A.Y., Mand, S., Marfo-Debrekyei, Y., Batsa, L., Albers, A., Specht, S., Klarmann, U., Pfarr, K., Adjei, O. and Hoerfauf, A. Macrofilaricidal Activity in Wucheria bancrofti after 2 Weeks of Treatment with a Combination of Rifampicin plus Doxycycline. 3) Hoerauf, A. Filariasis: new drugs and new opportunities for lymphatic filariasis and onchocerciasis. Current Opinions in Infectious Disease. 2008. 21: 673-681. 4) Hoerauf, A., Mand, S., Fischer, K., Kruppa, T., Marfo-Debrekyei, Y., Debrah, A.Y., Pfarr, K.M., Adjiei, O. and Buttner, D.W. Doxycycline as a novel strategy against bancroftian filariasis-depletion of Wolbachia endosymbionts from Wuchereria bancrofti and stop of microfilaria production. Med Microbiology Immunology. 2003 Nov. 192(4): 211-6. 5) Hoerauf, A., Pfar,K., Mand,S., Deobrah, A.Y. and Specht, S. Filariasis in Africa-treatment challeneges and prospects. Clincal Microbiology and Infection. 2011. 17:977-985. 6) Taylor, M.J., Bandi, C., Hoerauf, A.M. and Lazdins, J. Wolbachia bacteria of filarial nematodes: a target for control? Parasitology today Personal ed. 2000. 16(5,): 179-180. 7) Taylor, M.J., Makunde, W.H., McGarry, H.F., Turner, J.D., Mand, S. and Hoerauf, A. Macrofilaricidal activity after doxycycline treatment of Wuchereria bancrofti: a double-blind, randomised placebo-controlled trial. Lancet. 2005 Jun 18-24;365(9477):2116-21. Transmission electron micrograph of ''Wolbachia'' within an insect cell from ''Genome Sequence of the Intracellular Bacterium Wolbachia.'' Designed by Michelle Brozowski Snavely
Transcript of 1315 Lyme and Filariais A Wolbachia Connection: A Case · Lyme and Filariais A Wolbachia...

Introduction*As travel and immigration increases, health care providers must consider neglected tropical and endemic diseases.
*Lymphatic filariasis is a mosquito-borne tropical disease and 120 million people in Africa are infected.
*Lymphatic filariasis, endemic to Africa, is a neglected disease caused by Wuchereria bancrofti and can result in chronic disease that can be easily overlooked in immigrants coming to North America.
*The symbiotic bacteria, Wolbachia, has been recently identified as a chemotherapeutic target for anti-filarial therapy.
*Lyme disease, a common tick-borne illness due to Borrelia burgdorferi is endemic to North America.
*We have taken advantage of the symbiotic relationship between filaria and Wolbachia to treat a recent immigrant with both Lyme disease and filariasis.
A
1) Albany Medical College, Division of Internal Medicine-Pediatrics, Albany, NY. 2) Albany Medical College, Division of Internal Medicine, Albany, NY.3) Albany Medical Center, Division of Infectious Disease, Albany, NY.
Lyme and Filariais A Wolbachia Connection: A Case Jessica A. Kumar, MD, MPH, Graham Atkins, MD, Richard Blinkhorn, MD1
1315
2 2, 3
Abstract:Health care providers must consider neglected tropical and regional endemic diseases. Lyme disease, commonly found in North Americarequires a diagnosis of erythema migrans with confirmatory serology. Lymphatic filariasis, endemic to Africa, is a neglected chronic disease thatcan be easily overlooked in immigrants coming to North America. Wepresent a case of a 21 year old Liberian male complaining of one weekof right knee pain and swelling during the summer. He had a historyof malaria and filariasis. He immigrated to Albany, New York eighteenmonths ago as a refugee from civil war and was taking isoniazid andpyridoxine for a positive tuberculin test. He had no known tick exposure or trauma. He was afebrile and hemodynamically stable complaining of rightknee discomfort, warmth, swelling and decreased range of motion. Hiswhite blood cell count was 4.7 with 52% neutrophils, 26% lymphocytes,9% eosinophils and 12% monocytes. C-reactive protein (101 mg/L) erythrocyte sedimentation rate (73 mm/hr) and IgE level (4123 U/ml) were elevated. Knee radiograph showed joint effusion. Synovial fluid aspirationcontained 116.5 tho/cmm white cells (95% neutrophils) but gram stain and culture were negative. Lyme PCR from synovial fluid was notsubmitted for analysis. Lyme C6 peptide was positive as was confirmatoryWestern blot which demonstrated IgG bands 18, 23, 30, 31, 39, 41, 58 and 93. Antifilarial IgG4 was positive indicative of past or chronic infection with filariasis. A course of Doxycycline was initiated for the managementof both acute Lyme arthritis and chronic filariasis. Antifilarial therapywith Doxcycline was directed toward the symbiotic bacteria, Wolbachia associated with microfilaria. While it is possible our patient’s positive Lymeserology reflected cross reacting antigens to filaria; his clinical presentationwas consistent with Lyme associated arthritis. This case is unique in that antimicrobial management of one endemic infection was useful in the management of a geographically separate pathogen.
Case Presentation*A 21 year old Liberian male complained of one week of right knee pain and swelling during the summer.*He had a history of malaria and filariasis. *He immigrated to Albany, New York eighteen months earlier as a refugee from civil war and was taking isoniazid and pyridoxine for a positive tuberculin test. *He did not recall a tick bite or trauma.
*Vital signs were normal. *Physical exam was notable for right knee warmth, swelling and decreased range of motion.*He had no rash, lymphedema or hydrocoele.
*His white blood count was 4.7 with 52% neutrophils, 26% lymphocytes, 12% monocytes and 9% eosinophils,*Serum IgE level (4123 U/ml) was elevated.*Knee radiograph showed joint effusion.*Synovial fluid aspiration contained 116.5 tho/cmm white cells (95% neutrophils) and no crystals were identified.*Gram stain revealed no organisms, and bacterial culture was negative.*Lyme PCR from synovial fluid was not submitted for analysis.*Serum Lyme C6 peptide was positive as was confirmatory Western blot which demonstrated IgG bands 18, 23, 30, 31, 39, 41, 58 and 93.*Serum antifilarial antibody IgG4 EIA was positive.
*A diagnosis of Lyme arthritis as well as filariasis were established.
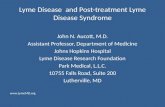
Microfilaria of Wuchereria bancrofti and spirochetes of Lyme disease (CDC Photo; Centers for Disease Control and Prevention's Public Health Image Library )
Management*He received a 28 day course of doxycycline 100mg twice daily for both Borrelia burgdorferi and filariasis.
*We chose not to administer ivermectin, albendazole or diethylcarbamazine.
*At follow-up visits, he was in good health and his knee effusion resolved.
Discussion*This case illustrates the unusual crossroads of two geographically separate infectious diseases that may occur with increasing frequency due to the ease of foreign travel.*Whereas Lyme disease is highly prevalent in the Northeastern United States, filariasis is highly prevalent in Africa.*Our patients infectious diseases happened to have been acquired by two different arthropod vectors.*We recognized a unique commonality that permitted the use of one anti-microbial agent to treat two diverse infections.*Wolbachia are endosymbionts of filarial parasites -Essential for larval molting -Female worm fertility -Adult worm survival*Doxycycline possess anti-Wolbachia activity. -Animal and human trials demonstrate macrofilaricidal activity -Reduction in lymph vessel dilation -Absence of inflammatory reaction to filarial death*Doxycycline is the treatment of choice for Lyme disease.
Conclusion*This case is unique in that antimicrobial management of one endemic infection was useful in the management of a geographically separate pathogen.
*The unique relationship between Wolbachia and filarial has significantly changed the approach to anti-filarial therapy.
References1) Addiss, D.G. and Dreyer, G. Treatment of Lymphatic Filariasis. https://apps.who.int/ctd/filariasis/docs/chap7.pdf.
2) Deborah, A.Y., Mand, S., Marfo-Debrekyei, Y., Batsa, L., Albers, A., Specht, S., Klarmann, U., Pfarr, K., Adjei, O. and Hoerfauf, A. Macrofilaricidal Activity in Wucheria bancrofti after 2 Weeks of Treatment with a Combination of Rifampicin plus Doxycycline.
3) Hoerauf, A. Filariasis: new drugs and new opportunities for lymphatic filariasis and onchocerciasis. Current Opinions in Infectious Disease. 2008. 21: 673-681.
4) Hoerauf, A., Mand, S., Fischer, K., Kruppa, T., Marfo-Debrekyei, Y., Debrah, A.Y., Pfarr, K.M., Adjiei, O. and Buttner, D.W. Doxycycline as a novel strategy against bancroftian filariasis-depletion of Wolbachia endosymbionts from Wuchereria bancrofti and stop of microfilaria production. Med Microbiology Immunology. 2003 Nov. 192(4): 211-6.
5) Hoerauf, A., Pfar,K., Mand,S., Deobrah, A.Y. and Specht, S. Filariasis in Africa-treatment challeneges and prospects. Clincal Microbiology and Infection. 2011. 17:977-985.
6) Taylor, M.J., Bandi, C., Hoerauf, A.M. and Lazdins, J. Wolbachia bacteria of filarial nematodes: a target for control? Parasitology today Personal ed. 2000. 16(5,): 179-180.
7) Taylor, M.J., Makunde, W.H., McGarry, H.F., Turner, J.D., Mand, S. and Hoerauf, A. Macrofilaricidal activity after doxycycline treatment of Wuchereria bancrofti: a double-blind, randomised placebo-controlled trial. Lancet. 2005 Jun 18-24;365(9477):2116-21.
Transmission electron micrograph of ''Wolbachia'' within an insect cell from ''Genome Sequence of the Intracellular Bacterium Wolbachia.''
Designed by Michelle Brozowski Snavely


![Wolbachia Seminar Master [Compatibility Mode]](https://static.fdocuments.net/doc/165x107/54679b73b4af9f623f8b588c/wolbachia-seminar-master-compatibility-mode.jpg)