11.10.2009tracen.ppt1 Trace elements Lecture from pathological physiology Oliver Rácz 2009/2013.
41
11.10.2009 tracen.ppt 1 Trace elements Lecture from pathological physiology Oliver Rácz 2009/2013
-
Upload
timothy-chambers -
Category
Documents
-
view
218 -
download
1
Transcript of 11.10.2009tracen.ppt1 Trace elements Lecture from pathological physiology Oliver Rácz 2009/2013.
11.10.2009 tracen.ppt 1
Trace elements
Lecture from pathological physiology
Oliver Rácz2009/2013

11.10.2009 tracen.ppt 2
Trace elements - overview
• The elements of life• Current knowledge and unanswered
questions• Iron metabolism• Zinc and copper• Vanadium, nickel, molybdenium, cobalt• Selenium• Iodine and fluorine

11.10.2009 tracen.ppt 3
Elements of life
• Main biogenic elements - 6– C, H, N, O, & P, S
• Electrolytes– Na+, K+, Mg++, Ca++ against Cl- (?)
• Trace, < 1 g with two exceptions (Fe, Zn)– metals: Fe, Zn, Cu, Mn, Mo, Cr, Co, V, Sn– most of them transition metals (complexes)– nonmetals: F, I, Se, Si, B

11.10.2009 tracen.ppt 4
Elements of life - be careful!
• Not the same as the elements found in human body:– As, Au, Pb, Hg….(contaminations)
• Strong selection:– Earth crust - O, Si, Al, Fe, Ca– Sea water ? Sea when life was arising ?– Element composition of plants resembles that of
soil
• Life is „easy“ - first half of Mendelejev table, only 4 with atomic No > 30: 34Se (79) ,42Mo (96), 50Sn (119), 53I (127)

11.10.2009 tracen.ppt 5
Trace elements - current knowledge - 1• Composition of body, tissues, cells,
O.K.• Form - metals only as complexes!
– Stable complexes are well known (heme, molybdopterin, etc.)
– Less stable complexes are difficult to study
– Added to biochemical structures after their synthesis - with exception of Se

11.10.2009 tracen.ppt 6
Trace elements - current knowledge - 2• Cycles in biosphere - natural &
influenced by human activity (ecology) influence on health
• Cycles in human body - many unanswered questions
• Clinical chemistry– Only iron status is routinely assessed– Plasmatic levels do not reflect metabolism– Indirect markers - e.g. GPX for Se
11.10.2009 tracen.ppt 7
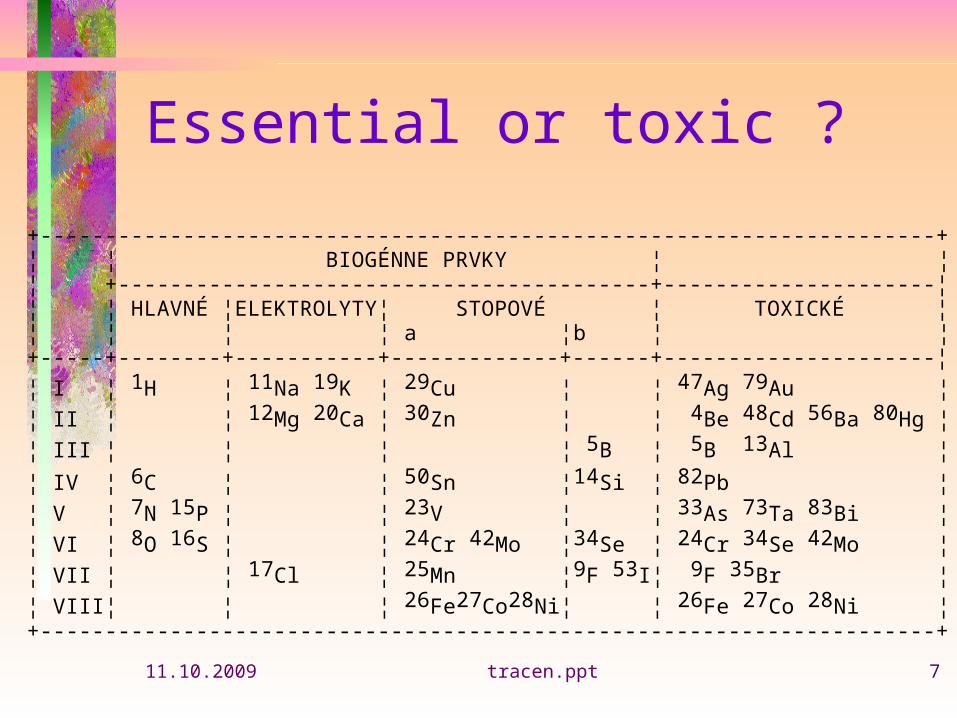
Essential or toxic ?
+---------------------------------------------------------------------+¦ ¦ BIOGÉNNE PRVKY ¦ ¦¦ +-----------------------------------------+---------------------¦¦ ¦ HLAVNÉ ¦ELEKTROLYTY¦ STOPOVÉ ¦ TOXICKÉ ¦¦ ¦ ¦ ¦ a ¦b ¦ ¦+-----+--------+-----------+-------------+------+---------------------¦
¦ I ¦ 1H ¦ 11Na 19K ¦ 29Cu ¦ ¦ 47Ag 79Au ¦
¦ II ¦ ¦ 12Mg 20Ca ¦ 30Zn ¦ ¦ 4Be 48Cd 56Ba 80Hg ¦
¦ III ¦ ¦ ¦ ¦ 5B ¦ 5B 13Al ¦
¦ IV ¦ 6C ¦ ¦ 50Sn ¦14Si ¦ 82Pb ¦
¦ V ¦ 7N 15P ¦ ¦ 23V ¦ ¦ 33As 73Ta 83Bi ¦
¦ VI ¦ 8O 16S ¦ ¦ 24Cr 42Mo ¦34Se ¦ 24Cr 34Se 42Mo ¦
¦ VII ¦ ¦ 17Cl ¦ 25Mn ¦9F 53I¦ 9F 35Br ¦
¦ VIII¦ ¦ ¦ 26Fe27Co28Ni¦ ¦ 26Fe 27Co 28Ni ¦+---------------------------------------------------------------------+

11.10.2009 tracen.ppt 8
Supplementaion ?• RDA = recommended daily allowance • Enough for deficiency prevention• New system - DRI = daily recommended
intake– Estimated average requirement– RDA– Adequate intake– Upper limit
• YES - Fe, Zn, Cr, Se, I, F (if indicated)• NO - Cu, V, Mn, Ni, Co, Sn, Si
11.10.2009 tracen.ppt 9
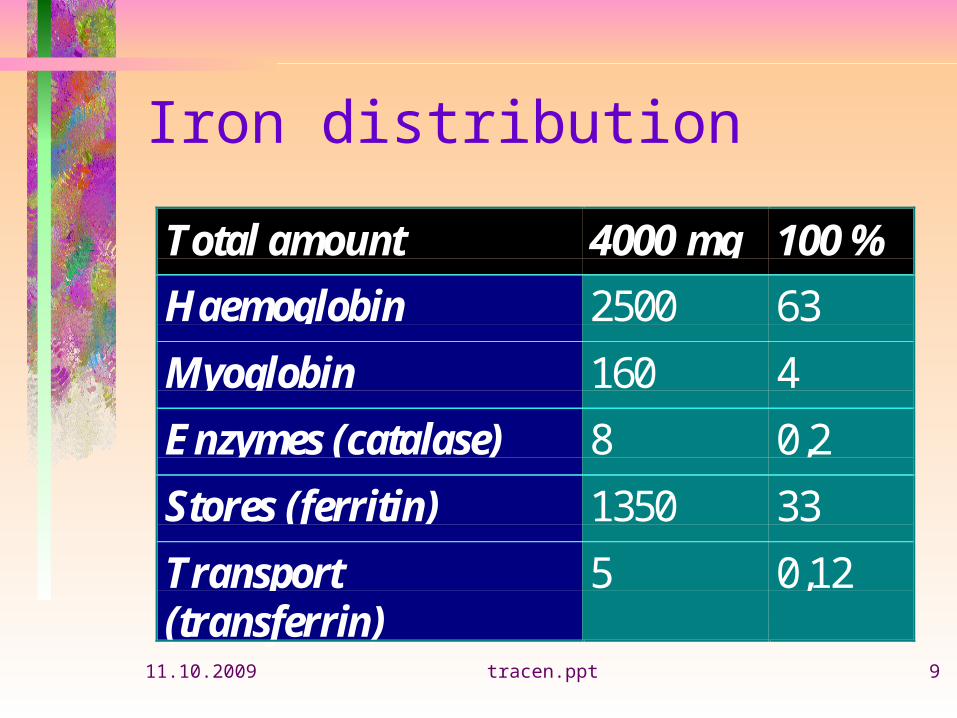
Iron distribution
Total amount 4000 mg 100 %
Haemoglobin 2500 63
Myoglobin 160 4
Enzymes (catalase) 8 0,2
Stores (ferritin) 1350 33
Transport(transferrin)
5 0,12

11.10.2009 tracen.ppt 10
Iron balance
• Destruction of red cells
(0,8 % /day 20 ml)20 - 25 mg Fe/ day• 90 - 95 % recycled!• Losses only 1 - 2 mg/d
• Average diet
10 - 15 mg/ daycontrolled resorbtion
1 - 2 mg/d
Physiologic increased losses: Menstruation: 30 mg, gravidity 300 mg, lactation 180 mg

11.10.2009 tracen.ppt 11
Diagnosis ?
• Anemia - suspected sideropenia• Serum iron (m: 14 - 29, w: 12 - 23 mol/l)
is not sufficient for dg. !!!• TIBS, total iron binding capacity is a
simple and not expensive assay• Ferritin assay ? if you are rich, it is an
excellent marker of total stores (plasma: 40 - 50 ng/l)
• Transferrin assay ? (2 - 3 mg/l), fluctuating• Soluble transferrin receptor assay

11.10.2009 tracen.ppt 12
Iron binding capacity (TIBC)• 1. Iron assay from serum (16)• Excess iron added to the sample -
saturation of transferrin to 100 %• Removal on non bound iron• 2. Iron assay (64)• Saturation index = 16/64 = 0,25 (25 %)• < 0,2 = sideropenia; > 0,55 = iron
excess

11.10.2009 tracen.ppt 13
Iron deficiency and excess
• Sideropenia is common in women living in poor countries – repeated gravidities, infections, poor nutrition
• In rich countries - achlorhydria & diseases associated with chronic blood loss - kidney, gynecologic diseases, peptic ulcer
• Strict vegetarians - children• 3 stages, microcytic hypochromic
anemia is the last

11.10.2009 tracen.ppt 14

11.10.2009 tracen.ppt 15
Iron deficiency and excess
• Popeye, the brave seaman and the spinach• Mistake - spinach is not a good source of iron
(meat)• Bigger mistake - iron excess is a risk factor
of coronary heart disease• Hereditary haemochromatosis - our
european heritage (10 - 15 thousand years ago)
• Secondary haemochromatosis (Sickle cell disease and transfusions)

11.10.2009 tracen.ppt 16
Clinical manifestation of haemochromatosis
• Bronze-colored skin• Hepatomegalia, later liver cirrhosis• Painful damage of joints• Disorders of endocrine glands (e.g. diabetes bronze).• Cardiomyopathy• Chronic fatigue syndrome• Loss of libido, impotency• Oxidative stress and accelerated
atherosclerosis already in latent stage
Factors of manifestation: sex (m>w), nutrition (meat), excess alcohol consumption

11.10.2009 tracen.ppt 17
Hemochromatosisand the regulation of iron resorbtion
OMIM *235200; carrier frequency 0,045 - 0,071 (!)
Homozygotes 2 - 5/1000 HFE gene in HLA region, 1 common mutation 1999 HFE2 - long arm, ch. 1 2000 HFE3 - 7q22, transferrin receptor 2 2001 HFE4 - ch 2; SCL40A1 gene for ferroportin 2003 HAMP gene; ch 1 for hepcidin 2004 HJV gene for hemojuvelin
11.10.2009 tracen.ppt 18
Hemochromatosisand the regulation of iron resorbtion For general practice these extremely rare
conditions are not important but they are important to understand the
physiological regulation of iron resorbtion The main regulator is the hepcidin from liver
increased expression in experiment - Fe deficiency
mutation or decreased expression – Fe excess and also hemojuvelin
And iron accumulation in substantia nigra - Parkinsonism
11.10.2009 tracen.ppt 19
11.10.2009 tracen.ppt 20

11.10.2009 tracen.ppt 21
Zinc, Zn2 - 3 g; RDA 12 - 15 mg• Constituent of enzymes (cca 300)
and other proteins ( insulin crystalls)• Smell and taste receptors, ion
channels• Not a catalyst• Stabilisation of proper spatial
structure of domains - zinc fingers, regulating gene expression

11.10.2009 tracen.ppt 22
Zn - history• Nihil album (ZnO) used already in Middle
Ages ro treat eye and skin diseases• 1746 A.S. Margaff, Germany• 1869 - 1957 essential micronutrient for
plants and domestic animals, deficiency described
• 1940 - 1961 essential for man, Zn-proteins described
• 1974 RDA• Now intensive research about marginal
deficiency not only in human but also in veterinary medicine

11.10.2009 tracen.ppt 23
Zn-metalloenzymes and proteins
• DNA polymerase• Zn-Cu SOD• Retinol
dehydrogenase • Collagenase
• Metallothionein• Zn fingers• Thymulin• Steroid receptors
• NA synthesis, cell division• Antioxidant defense• Regeneration of visual
pigment• Connective tissue, vessel
wall• Transport• Gene expression• T lymfocyte
differentiation !• Endocrine functions

11.10.2009 tracen.ppt 24
Zinc, Zn - deficiency2 - 3 g; RDA 12 - 15 mg• Sources, liver, kidney, mushrooms, red beet• Small stores, phytates from cereals block
resorbtion• Marginal deficiency is probably common -
repeated infections, growth retardation• Severe deficiency
– Middle East - cereals– Alcoholism, cirrhosis, nefrotic & malabosrbtion sy.
• Hereditary disturbance of absorbtion - acrodermatitis enteropathica

11.10.2009 tracen.ppt 25
Copper, Cu 100 - 150 mg; RDA 2 - 5 mg
• Muscles, bones, liver• Active centre of many enzymes,
mainly oxidoreductases• Cu++ + e- Cu+
• Superoxddismutase, lysyloxidase, cytochromoxidase and others
• Ceruloplasmin is the main transporter of copper

11.10.2009 tracen.ppt 26
Cu metabolism, deficiency and excess
• Sources: nuts, oysters, sea fish• Binding to albumin, transcuprein and in the
liver to ceruloplasmin• Excretion through bile• Deficiency - experimental and severe
malnutrition - anemia, leukopenia, brittle bones
• Accumulation in obstructive icterus, • Intoxication - diarrhoe, liver damage

11.10.2009 tracen.ppt 27
Hereditary pathological conditions
• m. Wilson is a hereditary deficiency of coeruloplasmin - hepatolenticular degeneration – Autosomal recessive, 1/30 000 newborns– Free copper induces oxidative damage– ATP7B 13q14; 200 different mutation, 1 common– Different clinical manifestation, from mild (only
higher transaminases and Kayser-Fleischer ring to serious liver damage, hemolysis and neurological/psychiatric spts.
• KF ring = green/brown ring in cornea = deposit of Cu

11.10.2009 tracen.ppt 28
Hereditary pathological conditions
• Menkes’ kinky hair syndrome– X chromosome related, ATP7A (1/250
000)– disorder of intracellular transport of Cu– Low activity of key copper enzymes
(SOD, Cytochromoxidase, etc.)– Severe fatal disease with progressive
neurological spts., connective tissue, skin, digestion

11.10.2009 tracen.ppt 29
m. Wilson
Index Norm m. Wilson
Ceruloplazmin 1,8 – 2,5 mol/l < 1,8 mol/l
Cu – plasma 16 – 31 mol/l < 16 mol/l
Cu – liver 30 – 50 g/g 100 – 150 g/g
Cu – urine traces 100 g/d

11.10.2009 tracen.ppt 30
m. Wilson – case report
• 22 yearold man, elevated transaminases during investigation for blood donation
• All possible causes of liver disease excluded• Targeted laboratory assays - m. Wilson• Two sisters - asymptomatic form, one healthy• No Kayser – Fleischer ring• Think of it! – molecular genetic dg. is possible

11.10.2009 tracen.ppt 31
Morbus Wilson
Age S-Cu mol/l
Du-Cu mol/d
CPL g/l
Father 59 16,1 0,35 0,37
Mother 56 12,0 0,42 0,24
Son 22 2,7 1,50 0,00
Daughter1 31 2,6 0,88 0,03
Daughter2 29 15,7 0,54 0,39
Daughter3 25 3,8 1,9 0,00

11.10.2009 tracen.ppt 32
m. Wilson – case report
• Manifestation mostly in age 8 - 20 y.• Mostly liver damage, if liver failure
and mental deterioration is present, too late for therapy!– Dysartria, dysphagia, rigidity, tremor,
psychiatric symptoms• Th: penicillamin, Zn, trietyltetramin,
also liver transplantation

11.10.2009 tracen.ppt 33
Chromium, Cr 1 mg, decrease with age
• Very toxic• In complex form (picolinate) increases
insulin sensitivity• Prevention of impaired glucose
tolerance • Adjuvant therapy in Type 2 diabetes• Cr activates a step in insulin induced
signal pathway (2003)

11.10.2009 tracen.ppt 34
Vanadium, manganese, nickel cobalt, a molybdenium
• Vanadium– No deficiency in humans, intoxication is possible– Insulin like effect in vitro ?
• Manganese, nickel– No deficiency syndromes
• Cobalt– very toxic - additive to beer - cardiomypathy
– only as the constituent of vitamin B12
• Molybdenium (molybdopterin)– No deficiency in humans, intoxication is possible
11.10.2009 tracen.ppt 35
Selenium, Se
• Toxic compound (semi-condcuctors)• m. Keshan (China), cardiomyopathy• No selenium in soil, plants, food• Active center of glutathione peroxidase
(GPX), key enzyme of antioxidant defense• Involved also in iodine metabolism• Selenocysteine is incorporated to peptide
chain during synthesis

11.10.2009 tracen.ppt 36
Selenium, Se• Sources: garlic, yeast, sea fish• Marginal deficiency in many countries of
Europe (SK, H, PL, CZ)• RDA m: 70 g; w: 50 g, • Recently up to 200 g • Supplementation is recommended in
atherosclerosis and cancer prevention• In 2001 after 10 years of supplementation
significantly less prostata and colon cancer
• Not a panacea
11.10.2009 tracen.ppt 37
Iodine, I Metabolism, differentiation, CNS development• Thyroid gland and hormones (TG, T3, T4)• RDA: 100 - 200 g/d• Deficiency threatens cca 1 billion people
living in mountains but also in lowlands (far from sea),
• This country: In the past high incidence of endemic goiter
• Sources: seafood, egg yolk / salt iodidation• Strumigens (cabbage) block thyroid
metabolism• Normal urine excretion > 100 g/d• USG volume measurement of thyroid

11.10.2009 tracen.ppt 38
Requirements
Group RDA, g/d Ioduria g/l
adults and adolescents
150 100 – 200
gravidity 200 200 – 300
newborns 90 > 150
children, 6mo – 6y 90 180 – 220
children, 6 – 12y 120 100 – 200

11.10.2009 tracen.ppt 39
Consequences of iodine deficiency
Embryo abortion, malformations
Newborn increased mortality goiter, hypothyreosis psychosomatic retardation cretenism
Child goiter, hypothyreosis psychosomatic retardation cretenism
Adult goiter, hypothyreosis low IQ cretenism

11.10.2009 tracen.ppt 40
Markers of iodine metabolismIoduria, g/l Deficiency
< 20 severe
20 – 50 significant
50 – 100 mild
100 – 200 no
Volume of thyroid
ml (USG)
men < 22 ml
women < 18 ml
children according to body surface
11.10.2009 tracen.ppt 41
Fluorine, F - metabolic toxin/caries prevention• Already 0,1 mmol/l fluoride blocks bacterial
enolase• Fluoroapatite, forming 10 % tooth enamel
is more resistant as hydroxyapatite• Fluorine helps convert amorph
calciumphosphate into crystallic apatite
Tooth pasta, mouthwash, KF pills, 1 - 2 mg/d
Fluoridation of tap water