4. chronic inflammation granulomatous inflammation -dr. sinhasan- mdzah

Chapter V
Jamia Hamdard Page 280
1.0. Introduction to inflammation
Based on visual observation, the ancients have characterised inflammation by
five cardinal signs, namely redness (rubor), swelling (tumour), heat (calor; only
applicable to the body's extremities), pain (dolor) and loss of function (functio laesa).
The first four of these signs were named by Celsus in ancient Rome (30-38 B.C.) and
the last by Galen (A.D 130-200) [1]. However, beginning with the work of
Metchnikoff and others in the 19th
century, the contribution of inflammation to the
body's defensive and healing process was recognised [1]. More recently,
inflammation was described as "the succession of changes which occurs in a living
tissue when it is injured provided that the injury is not of such a degree as to at once
destroy its structure and vitality" [2], or "the reaction to injury of the living
microcirculation and related tissues [3]. Although, in ancient times inflammation was
recognised as being part of the healing process, up to the end of the 19th century,
inflammation was viewed as being an undesirable response that was harmful to the
host.
Inflammation is a part of the complex biological response of vascular tissues
to harmful stimuli, such as pathogen, damaged cells, or irritants [4]. Inflammation is a
process by which the body deals with insult and injury. Insult may be caused
mechanically (by pressure or foreign bodies), chemically (by toxins, acidity,
alkalinity), physically (by temperature), by internal processes (uremia) and by
mircoorganisms (bacteria, virus and parasites) etc. Inflammation rids the body of
foreign matter and disposes of damaged cells and initiates wound healing.
Furthermore, inflammation is considered as the corner stone of pathology in that the
changes observed are indicative of injury and disease.
During inflammation the sensation of heat is caused by the increased
movement of blood through dilated vessels into the environmentally cooled
extremities resulting in the increased redness. The swelling is the result of increased
passage of fluid from dilated and permeable blood vessels into the surrounding
tissues, infiltration of cells into the damaged area and in prolonged inflammatory
responses deposition of connective tissue. Pain is due to the direct effects of
mediators, either from initial damage or that resulting from the inflammatory response
itself and the stretching of sensory nerves due to oedema. The loss of function refers

Chapter V
Jamia Hamdard Page 281
to either simple loss of mobility in a joint, due to the oedema and pain, or to the
replacement of functional cells with scar tissue [5].
Inflammation is a diverse phenomenon (Figure1), ranging from the acute
inflammation associated with S. aureus infection of the skin (the humble boil),
through to chronic inflammatory processes resulting in remodelling of the artery wall
in atherosclerosis, the bronchial wall in asthma and chronic bronchitis and the
debilitating destruction of the joints associated with rheumatoid arthritis.
Figure 1. Inflammation - The basic cause of many diseases.
Inflammation is controlled by mast cells that are in close proximity to
autonomic nerves. Mast cells are the constituents of connective tissues containing
large granules that contain heparin, serotonin, bradykinin and histamine. These
substances are released from the mast cell (Figure 2) in response to injury and
infection and by their degranulation, they control most of the processes of
inflammation. Mast cells are responsive to other controls, for example, under the
influence of progesterone they release serotonin and under the influence of estrogen
they release histamine.

Chapter V
Jamia Hamdard Page 282
Figure 2. Role of the mast cells in inflammation.
Another important pathway is known as the arachidonic acid cascade which is
largely controlled by eicosanoids. Eicosanoids are local “hormones” made from 20-
carbon essential fatty acids; they are short-lived and can affect many aspects of
physiological function at the cellular level. Eicosanoids include all the prostaglandins,
thromboxanes and leukotrienes. Depending on genetic as well as other factors
eicosanoids transform or control prostaglandins, thromboxanes, and leukotrienes all
of which are inflammatory mediators. Eicosanoids can initiate, regulate and terminate
all local inflammatory responses. When inflammation affects a joint (such as in
rheumatoid arthritis), the cartilage can be damaged by neutrophils and lysosomal
enzymes that enter the area. This leads to a vicious cycle of repeated injury and
persistent inflammation. Inflammation may also lead to mental depression which is
commonly seen in chronic pain patients. Indolamine dioxygenase (IDO) is a rate-
limiting enzyme in the degradation of tryptophan and is induced during inflammation
by the cytokines interferon-gamma (IFN-gamma), interferon-alpha (ITN-alpha) and
tumor necrosis factor-alpha (TNF-alpha) in a broad variety of cells. Elevated levels of
IDO can enhance tryptophan degradation and subsequent serotonin depletion which
may cause depression [6].
Chapter V
Jamia Hamdard Page 283
1.1. Global status of inflammatory diseases
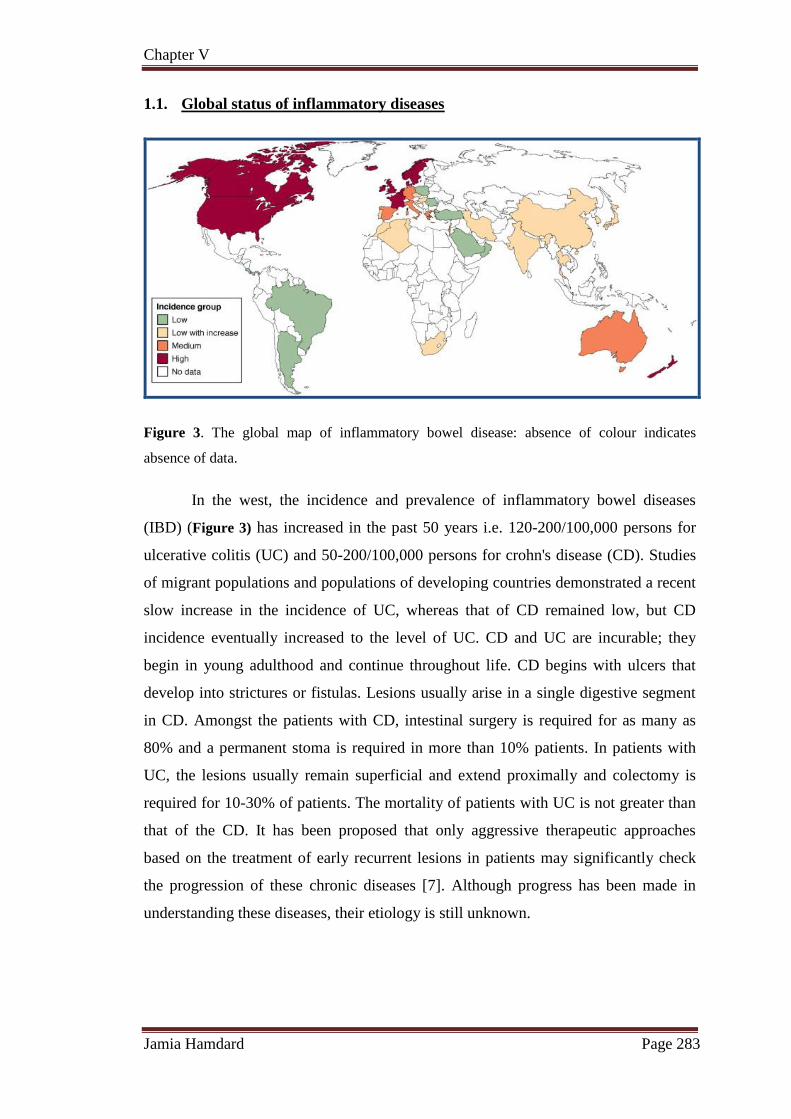
Figure 3. The global map of inflammatory bowel disease: absence of colour indicates
absence of data.
In the west, the incidence and prevalence of inflammatory bowel diseases
(IBD) (Figure 3) has increased in the past 50 years i.e. 120-200/100,000 persons for
ulcerative colitis (UC) and 50-200/100,000 persons for crohn's disease (CD). Studies
of migrant populations and populations of developing countries demonstrated a recent
slow increase in the incidence of UC, whereas that of CD remained low, but CD
incidence eventually increased to the level of UC. CD and UC are incurable; they
begin in young adulthood and continue throughout life. CD begins with ulcers that
develop into strictures or fistulas. Lesions usually arise in a single digestive segment
in CD. Amongst the patients with CD, intestinal surgery is required for as many as
80% and a permanent stoma is required in more than 10% patients. In patients with
UC, the lesions usually remain superficial and extend proximally and colectomy is
required for 10-30% of patients. The mortality of patients with UC is not greater than
that of the CD. It has been proposed that only aggressive therapeutic approaches
based on the treatment of early recurrent lesions in patients may significantly check
the progression of these chronic diseases [7]. Although progress has been made in
understanding these diseases, their etiology is still unknown.

Chapter V
Jamia Hamdard Page 284
1.2. Role of Natural products in the treatment of inflammatory diseases
Humans have been the most privileged form of life who has dominated the
rest of creatures. This most privileged class suffered from different ailments and
health disorders at different stages of life. For the treatment of illness, humans started
searching for the remedies in its surroundings i.e. the mother nature. The world health
organization (WHO) estimates that 80% of the population living in the developing
countries rely exclusively on traditional medicine for their primary health care needs.
In almost all the traditional medicines, the traditional plants play a major role and
constitute the backbone of the traditional medicine. Indian Materia Medica includes
about 2000 drugs of natural origin almost all of which are derived from different
traditional systems and folklore practices. Out of these drugs, 400 are of mineral and
animal origin while the rest are of vegetable origin. Since less than 10% of the
world’s biodiversity has been evaluated for potential biological activity, many more
useful natural lead compounds await discovery with the challenge being how to
access this natural chemical diversity [8]. The earliest records of natural products
were depicted on clay tablets in cuneiform from Mesopotamia (2600 B.C.) which
documented oils from Cupressus sempervirens (Cypress) and Commiphora species
(myrrh) which are still used today to treat coughs, colds and inflammation [8]. The
Ebers Papyrus (2900 B.C.) is an Egyptian pharmaceutical record, which documents
over 700 plant-based drugs ranging from gargles, pills, infusions, to ointments. The
Chinese Materia Medica (1100 B.C.) (Wu Shi Er Bing Fang, contains 52
prescriptions), Shennong Herbal (~100 B.C., 365 drugs) and the Tang Herbal (659
A.D., 850 drugs) are documented records of the uses of natural products [8].
1.3. Therapeutic potential of natural products
The Greek physician, Dioscorides (100 A.D.) recorded the collection, storage
and the uses of medicinal herbs, whilst the Greek philosopher and natural scientist,
Theophrastus (~300 B.C.) dealt with medicinal herbs. During the dark and middle
ages the monasteries in England, Ireland, France and Germany preserved this western
knowledge whilst the Arabs preserved the Greco-Roman knowledge and expanded the
uses of their own resources, together with Chinese and Indian herbs unfamiliar to the
Greco-Roman world [8]. It was the Arabs who were the first to privately own
pharmacies (8th century) with Avicenna, a Persian pharmacist, physician, philosopher

Chapter V
Jamia Hamdard Page 285
and poet, contributing much to the sciences of pharmacy and medicine through works
such as the Canon Medicinae [8].
In India Ayurveda originated long back in the pre‐vedic period. The Rigveda
and Atharvaveda (5000 BC), the earliest Indian documents have references on health
and diseases. During the Vedic period the Susruta samhita and the Charaka samhita
were influential works on traditional medicine. The fundamental and applied
principles of “Ayurveda” science of life; got organized and enunciated around 1500
B.C. Ayurveda traces its origins to the Vedas, Atharvaveda in particular, and is
connected to Hindu religion. Atharvaveda (one of the four most ancient books of
Indian knowledge, wisdom and culture) contains 114 hymns or formulations for the
treatment of diseases. Ayurvedic system of medicine was based on nature and its
products. Hundreds of medicinal plants were identified and have been traditionally
used since then. Over the following centuries, Ayurvedic practitioners developed a
number of medicinal preparations and surgical procedures for the treatment of various
ailments and diseases. Ayurvedic medicinal preparations consist mainly of plant
materials in the form of powders, semi‐solid preparations, decoctions, elixirs and
distillates. Many of them also contain inorganic chemical substances, minerals and
animal products. Alcoholic extracts and alcoholic solutions of the ingredients,
tinctures and elixirs are also frequently used in Ayurvedic medicine.
The role of natural products for the treatment of diseases has been recognized
since ancient times. There has been considerable public and scientific interest in the
use of natural products to combat human diseases such as inflammatory disease,
cardiovascular disease, and cancer etc. In spite of major scientific and technological
progress in combinatorial chemistry, drugs derived from natural products still make
an enormous contribution to drug discovery today [9]. Natural products with anti-
inflammatory activity have long been used as a folk remedy for inflammatory
conditions such as fever, pain, migraine and arthritis.
Boswellia serrata is native to India and has been used in traditional Ayurvedic
medicine for the treatment of inflammatory diseases in India [10]. The gum resin of
Boswellia serrata called ‘salai guggul’ or ‘Indian olibanum’ and is obtained from the
bark of Boswellia serrata after injury. Many commercial formulations of salai guggul
in the form of ointments, creams and capsules are available in the market [11]. As a
Chapter V
Jamia Hamdard Page 286
result of its alleged safety, boswellia was considered superior over mesalazine in
terms of a benefit-risk evaluation [12]. Research has shown that it is perhaps the
triterpenoid boswellic acids in the Boswellia serrata gum resin which exert the anti-
inflammatory action [13]. Boswellic acids inhibit the 5-LOX (Lipoxygenase) enzyme,
thereby reducing the production of the potent inflammatory mediators, the
leukotrienes [14].
Bromelain is a crude aqueous extract which is obtained from both the stem
and fruit of the pineapple plant and contains a number of proteolytic enzymes [15]. A
large body of scientific research shows that bromelain is a potential product for
treatment of osteoarthritis [16]. Bromelain was first reported to be used as an anti-
inflammatory for use in both rheumatoid arthritis and osteoarthritic patients in 1964
[16]. The mechanism of anti-inflammatory action of bromelain is known [16]. They
suggest that bromelain’s anti-inflammatory action is mediated by increasing serum
fibrinolytic activity, reducing plasma fibrinogen levels and decreasing bradykinin
levels (which results in reduced vascular permeability) and hence reducing oedema
and pain; by decreasing levels of PGE2 and thromboxane A2 (TXA2); and by
modulation of certain immune cell surface adhesion molecules.
Lyprinol is a stabilized lipid extract obtained from the New Zealand
green-lipped mussel (NZGLM) and is used to relieve the symptoms of arthritis. The
oil of the NZGLM contains a complex mixture of triglycerides, sterol esters, polar
lipids and free fatty acids [17].
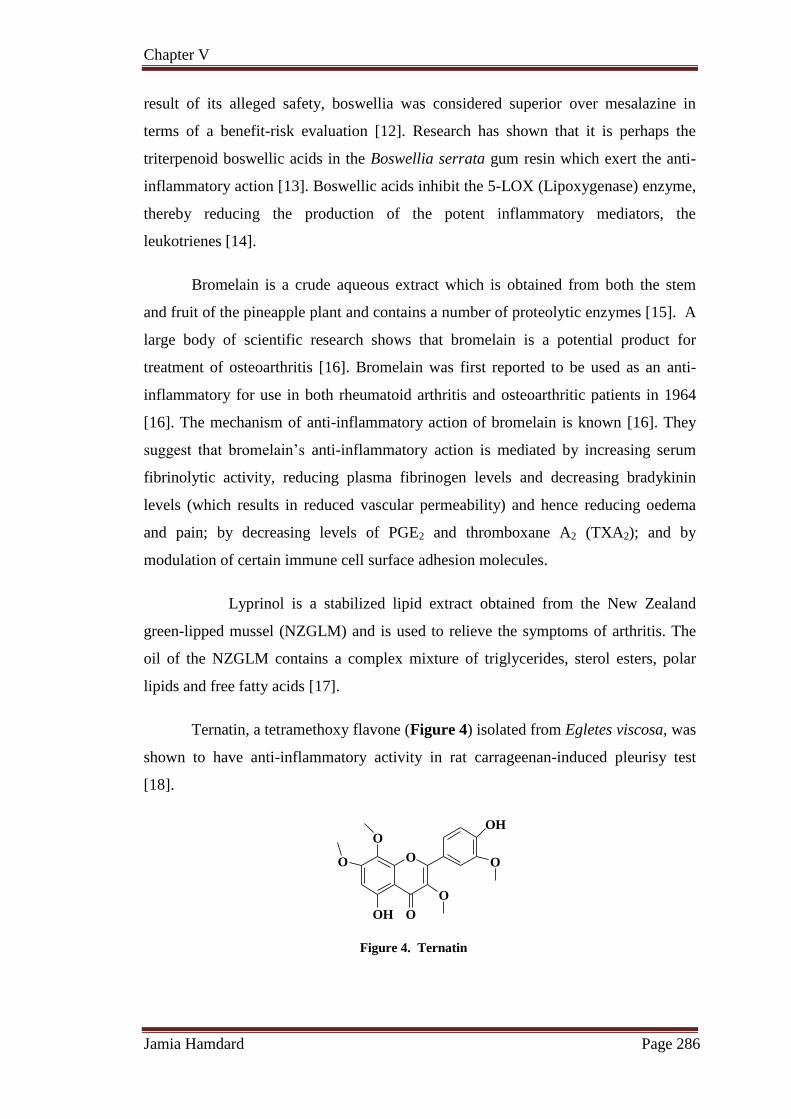
Ternatin, a tetramethoxy flavone (Figure 4) isolated from Egletes viscosa, was
shown to have anti-inflammatory activity in rat carrageenan-induced pleurisy test
[18].
O
O
O
OH O
O
O
OH
Figure 4. Ternatin

Chapter V
Jamia Hamdard Page 287
Quercitrin and rutin display beneficial effects in experimental inflammation
which is induced by trinitrobenzene sulfonic acid in the rat model [19]. The
mechanism by which flavonoids exert their anti-inflammatory effects involves the
inhibition of COX and LOX activities, eicosanoid biosynthesis and neutrophil
degranulation. Selective flavonoids such as quercetin inhibit both COX and LOX
activities [20]. Pelzer et al., (1998) investigated the anti-inflammatory activity of 30
flavonoids isolated from several plants of the compositae family and found that all the
flavonoids tested have anti-inflammatory activity depending on both their structure
and the method used for the assay [21].
Just et al., (1998) isolated three saponins (Fruticesaponin A, Fruticesaponin B,
ruticesaponin C) from Bupleurum fruticescens and investigated their anti-
inflammatory effects. All of them exerted anti-inflammatory activity in the mouse
oedema assay; however Fruticesaponin B has the highest anti-inflammatory activity
[22]. Silva et al., (2002) isolated a new steroidal saponin from the leaves of Agave
attenuata and investigated its anti-inflammatory activity using the capillary
permeability assay. It inhibits the increase in vascular permeability caused by acetic
acid [23]. Aescin, the main active constituent of Aesculus hippocastanum, is a
complex mixture of triterpenoid saponin glycosides. It has been shown to have anti-
oedematous, anti-inflammatory and venotonic properties in different animal models
[24]. Two triterpenoid saponins (Figure 5), kalopanaxsaponin A and pictoside A,
have been isolated from the stem bark of Kalopanax pictus and were found to exhibit
significant anti-inflammatory activity at the oral dose of 50 mg/ml [25].
O
COOH
HOH2C R2
R3O
OH
HO
R1O
R1 R2 R3
Kalopanaxsaponin A a-L-rhamnopyranosyl -H -H
a-L-rhamnopyranosyl -H -OHPictoside A
Figure 5. Kalopanaxsaponin A and Pictoside A

Chapter V
Jamia Hamdard Page 288
Probably the most famous and well known example to date would be the
synthesis of the anti-inflammatory agent, acetylsalicyclic acid (1) (aspirin) [26]
derived from the natural product, salicin (2) isolated from the bark of the willow tree
Salix alba L. Investigation of Papaver somniferum L. (opium poppy) resulted in the
isolation of several alkaloids including morphine (3) a commercially important drug,
first reported in 1803.
O
HO
O
O CH3
O
OH
HO
HO OH
O
HO
HO
O
HO
H
N CH3
1 2 3
It was in the 1870s that crude morphine derived from the P. somniferum was
boiled in acetic anhydride to yield diacetylmorphine (4) (heroin) which was readily
converted to codeine (5), a painkiller.
O
O
O
H
N CH3
5
O
O
O
O
HO
H
N CH3
H3C
4
Pilocarpine (6) found in Pilocarpus jaborandi (Rutaceae) is a L-histidine-
derived alkaloid, which has been used as a clinical drug for the treatment of chronic
open-angle glaucoma and acute angle-closure glaucoma for over 100 years. In 1998,
its oral preparation was approved for the treatment of Sjogren's syndrome, an
autoimmune disease that damages the salivary and lacrimal glands [27].
OO
N
N
CH3
6
Tripterygium wilfordii (Lei Gong Teng) is a Chinese herb that has been shown
to be quite effective in treating inflammation. It is a toxic herb that should be used

Chapter V
Jamia Hamdard Page 289
with caution as it can cause internal bleeding, kidney damage, decrease in blood cell
counts, decreased bone mineral density in females, hair loss, immune system dys-
function and even death. PG490-88, a diterpene-diepoxide (7), is a semisynthetic
analogue of triptolide which is isolated from Tripterygium wilfordii. It is used for the
treatment of autoimmune and inflammatory diseases in the People’s Republic of
China [28, 29].
O
OH
O
OO
O
O
O Na
O
7
Grandisines A (8) and B (9) are two indole alkaloids which were isolated from
the leaves of the Australian rainforest tree, Elaeocarpus grandis. Grandisine A (8)
contains a unique tetracyclic skeleton, while Grandisine B (9) possesses an unusual
combination of isoquinuclidinone and indolizidine ring systems. Both 8 and 9 exhibit
binding affinity for the human δ-opioid receptor and are potential leads for analgesic
agents [30].
O
O
N
H
H
HO
NO
N
H
8 9
The first notable discovery of biologically active compounds from marine
sources can be traced back to the reports of Bergmann on the isolation and
identification of C-nucleosides, spongouridine (10) and spongothymidine (11) from
the Caribbean sponge, Cryptotheca crypta in the early 1950s [31]. These compounds
were found to possess antiviral activity and the synthesis of its structural analogues
led to the development of cytosine arabinoside (Ara-C) as a clinical anticancer agent,
together with (Ara-A) as an antiviral agent 15 years later [31].

Chapter V
Jamia Hamdard Page 290
O
HO OH
N
OH
NH
O
O
O
HO OH
N
OH
NH
O
O
10 11
There are many anti-inflammatory natural products derived from marine
sponges. Eighty four anti-inflammatory compounds dominated by isoprenoid derived
metabolites, especially sesterterpenes (means 2.5 terpenes) have been isolated from
marine sponges [32]. Manoalide (12) is probably the most well-known of all the anti-
inflammatory products from sponge and was originally isolated by de Silva and
Scheuer in 1980 from the sponge Luffariella variabilis [33].
OHO
O
O
OH
12
The global marine pharmaceutical pipeline consists of three Food and Drug
Administration (FDA) approved drugs, one EU registered drug, 13 natural products
(or there derivatives) in different phases of the clinical trial and a large number of
marine chemicals in the pre-clinical pipeline [34]. Some examples include, Ziconotide
(Prialt®, Elan Corporation) a peptide first discovered in a tropical cone snail, which
was approved in December 2004 for the treatment of pain. Plitidepsin (13) (Aplidin®,
PharmaMa), a depsipeptide was isolated from the Mediterranean tunicate Aplidium
albicans [35,36]. Plitidepsin (13) is effective in treating various cancers, including
melanoma, small cell and non-small cell lung, bladder as well as non-hodgkin
lymphoma and acute lymphoblastic leukemia and is currently in Phase II clinical trials
[34,37].

Chapter V
Jamia Hamdard Page 291
N
O
O
O
N
O
NH
NHO
OH O
O
O
O
NHO
NO
N
O
O
13
Sativex, a mixture of dronabinol 14 and cannabidol 15 obtained from the
cannabis plant, is the world's first pharmaceutical prescription medicine that was
launched in Canada (April 2005) and was later approved by Health Canada (August
2007) as adjunctive analgesic for severe pain in advanced cancer patients [38].
Sativex has been recommended by FDA to enter directly in Phase III trials and as of
November 2009, GW Pharmaceuticals have completed the recruitment for Phase II/III
trial against cancer pain.
O
CH3
H3C
H3C
OH
CH3
14
CH3
OH
OHH2C
CH3
CH3
15

Chapter V
Jamia Hamdard Page 292
Natural product-derived drugs launched during 2005-2010; lead
compounds, and therapeutic area.
Year Trade name Lead Compound Disease area
2005 Dronabinol / Cannabidol
(Sativex®)
Dronabinol /
cannabidol Pain
2005 Fumagillin (Flisint®) Fumagillin Antiparasitic
2005 Doripenem
(Finibax® / DoribaxTM) Thienamycin Antibacterial
2005 Tigecycline (Tygacil®) Tetracycline Antibacterial
2005 Ziconotide (Prialt®) Ziconotide Pain
2005
Zotarolimus
(EndeavorTM stent)
Sirolimus Cardiovascular
surgery
2006
Anidulafungin
(EraxisTM / EcaltaTM)
Echinocandin B Antifungal
2006 Exenatide (Byetta®) Exenatide-4 Diabetes
2007 Lisdexamfetamine
(VyvanseTM) Amphetamine
Attention deficit-
hyperactivity
disorder (ADHD)
2007
Retapamulin
(AltabaxTM/AltargoTM)
Pleuromutilin Antibacterial
2007 Temsirolimus (ToriselTM) Sirolimus Oncology
2007 Trabectedin (YondelisTM) Trabectedin Oncology
2007 Ixabepilone (IxempraTM) Epothilone B Oncology
2008 Methylnaltrexone (Relistor®) Naltrexone Pain
2009 Everolimus (Afinitor®) Sirolimus Oncology
2009 Telavancin (VibativTM) Vancomycin Antibacterial
2009 Romidepsin (Istodax®) Romidepsin Oncology
2009 Capsaicin (Qutenza®) Capsaicin Pain
2010
Monobactam aztreonam
(CaystonTM)
Aztreonam Antibacterial

Chapter V
Jamia Hamdard Page 293
Natural products as anti-inflammatory agents
Compound Source Structure Reference
Curcumin
Curcuma longa
OHO
O O
OOH
CH3CH3
[39]
Parthenolide Tanacetum
parthenium
CH3
H3C OO
O
CH2
[40]
Cucurbitacins Wilbrandia
ebracteata
HH
HH
H
Basic structure
[41]
1,8-Cineole Eucalyptus
obliqua O [42]
Pseudopterosins Pseudopterogorgia
elisabethae H
O OHO OH
OH
OH
[43]
Amrubicin
hydrochloride
Streptomyces
peucetius
O
O
OH
OH O
OH
OHOH
O
NH2
[44]

Chapter V
Jamia Hamdard Page 294
The natural products discovered so far have played a vital role in improving
the human health and have been the drugs of choice despite facing a tough
competition from their synthetic counterparts, due to their safe and long lasting
effects. Current interest leads to the search for new natural products with anti-
inflammatory activity. Extensive scientific research deals with the finding, extracting,
pharmacological effects and mechanism by which natural products exert their activity.
In summary, we propose that a combination of metabolomics technologies with
natural product discovery processes will be highly beneficial. By increasing the
number of identifications in our metabolomics data we may provide novel structures
to be tested for bioactivity for a disease under investigation.
In view of the importance of natural products in the human health system, the
main objectives of this work are as follows:
1. Ethanolic extraction of the dried plant material followed by the fractionation
with different solvents of increasing polarity.
2. Isolation of the active principles from the biologically active fraction(s) of the
plant.
3. Structure elucidation of isolated compounds and biological evaluation of the
ethanolic extract and its fractions along with the isolated natural compounds
for their anti-inflammatory and analgesic activities with gastric ulceration
studies.

Chapter V
Jamia Hamdard Page 295
References
[1] J.V. Hurley: Acute inflammation. Edinburgh, London: Churchill Livingstone,
1972.
[2] J.B. Sanderson: A system of Surgery. 2nd
edition. London Longmans: Green
and Company, 1871.
[3] W.G. Spector, D.A. Willoughby, Bacter. Rev. 27, 117-149, 1963.
[4] M.L. Ferrero, O.H. Nielsen, P.S. Andersen, S.E. Girardin. Clin. Exp.
Immunol. 147, 227-235, 2007.
[5] A.P. Neville, J.W. Cliff, A. Ian, J. Inflamm. 1, 1-4, 2004.
[6] M.C. Wichers, M. Maes, J. Psych. Neurosci. 29, 11-7, 2004.
[7] C. Jacques, G.R. Corinne, S. Philippe, C. Antoine, Gastroenterology. 140,
1785-1794, 2011.
[8] G.M. Cragg, D.J. Newman, Pure Appl. Chem. 77, 7-24, 2005.
[9] V. Puni, D. Saint-Dic, S. Daghfal, J.R. Kanwar, Cancer Biol. Ther. 3, 708-
714, 2004.
[10] R. Lucas, A. Casapullo, L. Ciasullo, L. Gomez-Paloma, M. Payá, Life Sci. 72,
2543-2552, 2003.
[11] A.A. Kasali, A.M. Adio, A.O. Oyedeji, A.O. Eshilokun, M. Adefenwa, Flav.
Fragr. J. 17, 462-464, 2002.
[12] V.G. Sunnichan, R.H.Y. Mohan, K.R. Shivanna, Bot. J. Linn. Soc. 147, 73-82,
2005.
[13] I. Gupta, A. Parihar, P. Malhotra, S. Gupta, R. Ludtke, H. Safayhi, H.P.
Ammon, Planta Med. 67, 391-395, 2001.
[14] G.B. Singh, C.K. Atal, Agents actions. 18, 647-652, 1986.
[15] H.R. Maurer, Cell Mol. Life Sci. 58, 1234-1245, 2001.

Chapter V
Jamia Hamdard Page 296
[16] S. Brien, G. Lewith, A. Walker, S.M. Hicks, D. Middleton, Evid. Based
Compl. Altern. Med. 1, 251-257, 2004.
[17] AJ. Sinclair, K.J. Murphy, D. Li, Allerg. Immunol. 32, 261-271, 2000.
[18] M.F. Souza, V.S. Rao, E.R. Silveira, Braz. J. Med. Biol. Res. 25, 1029-1032,
1992.
[19] M.F. Sanchez de, J. Galvez, J.A. Romero, A. Zarzuelo, Life Sci. 70, 3097-
3108, 2002.
[20] H.P. Kim, I. Mani, L. Iversen, V.A. Ziboh, Prostagl. Leukot. Essent. Fatty
Acids. 58, 17-24, 1998.
[21] L.E. Pelzer, T. Guardia, J.A. Osvaldo, E. Guerreiro, Farmaco. 53, 421-424,
1998.
[22] M.J. Just, M.C. Recio, R.M. Giner, M.J. Cuellar, S. Manez, A.R. Bilia, J.L.
Rios, Planta Med. 64, 404-407, 1998.
[23] F. Wei, L.Y. W.T. Ma Jin, S.C. Ma, G.Z. Han, I.A. Khan, R.C .Lin, Chem.
Pharm. Bull. 52, 1246-1248, 2004.
[24] P. Sur, T. Chaudhuri, J.R. Vedasiromoni, A. Gomes, D.K. Ganguly, Phytother.
Res. 15, 4-176, 2001.
[25] D.W. Li, E.B. Lee, S.S. Kang, J.E. Hyun, W.K. Whang, Chem. Pharm. Bull.
50, 900-903, 2002.
[26] M.A. Der, J.A. Beutler, The Review of Natural Products, Facts and
Comparisons; Seattle, WA, USA, 2nd
edition, pp. 13-43, 2002.
[27] T. Aniszewski, Alkaloids-Secrets of Life. In Alkaloid Chemistry, Biological
Significance Applications and Ecological Role; Elsevier Science: Amsterdam,
The Netherlands, p. 334, 2007.
[28] T.M. Kiviharju, P.S. Lecane, R.G. Sellers, D.M. Peehl, Clin. Cancer. Res. 8,
2666-2674, 2002.

Chapter V
Jamia Hamdard Page 297
[29] J.M. Fidler, K. Li, C. Chung, Mol. Cancer. Ther. 2, 855-862, 2003.
[30] A.R. Carroll, G. Arumugan, R.J. Quinn, J. Redburn, G. Guymer, P. Grimshaw,
J. Org. Chem. 70, 1889-1892, 2005.
[31] O. McConnell, R.E. Longley, F.E. Koehn, The Discovery of Natural Products
with Therapeutic Potential; Gullo, V.P. Ed.; Butterworth-Heinemann: Boston,
MA, USA, pp. 109-174, 1994.
[32] H.J. Jung, S.G. Kim, J.H. Nam, K.K. Park, W.Y. Chung, W.B. Kim, K.T. Lee,
J.H. Won, J.W. Choi, H.J. Park, Biol. Pharm. Bull. 28, 1668-1671, 2005.
[33] R.A. Keyzers, M.T. Davies-Coleman, Chem. Soc. Rev. 34, 355-365, 2005.
[34] M. Alejandro, K.B. Glaser, C. Cuevas, R.S. Jacobs, W. Kem, R.D. Little, J.M.
McIntosh, D.J. Newman, B.C. Potts, D.E. Shuster, Trends Pharm. Sci. 31,
255-265, 2010.
[35] K.L. Rinehart, A.M. Lithgow-Bertelloni, PCT Int. Pat. April 18; WO
91.04985, 1991.
[36] J.L. Urdiales, P. Morata, I.N. De Castro, F. Sanchez-Jimenez, Cancer Lett.102,
31-37, 1996.
[37] R. Henríquez, G. Faircloth, C. Cuevas. In Ecteinascidin 743 (ET-743,
Yondelis), aplidin and kahalalide F. In Anticancer Agents from Natural
Products; Cragg, G.M., Kingston, D.G.I., Newman, D.J., Eds.; Taylor and
Francis: Boca Raton, FL, USA, p. 215, 2005.
[38] M.S. Butler, Nat. Prod. Rep. 25, 475-516, 2008.
[39] R. Srivastava, R.C. Srimal, Indian J. Med. Res. 81, 215-223, 1985.
[40] M. Heinrich, A. Ankli, B. Frei, C. Weimann, O. Sticher, Soc. Sci. Med. 47
1859-1871, 1998.
[41] M.C. Recio, M. Prieto, M. Bonucelli, C. Orsi, S. Manez, R.M. Giner, M.
Cerda-Nicolas, J.L. Rios, Planta Med. 70, 414-420, 2004.

Chapter V
Jamia Hamdard Page 298
[42] F.A. Santos, V.S. Rao, Phytother Res. 14, 240-244, 2000.
[43] S.A. Look, W. Fenical, R.S. Jacobs, J. Clardy, Proc. Natl. Acad. Sci. USA 83
6238-6240, 1986.
[44] P.M. Derwick, Medicinal Natural Products: A Biosynthetic Approach, 2nd
Edition, John Wiley & Sons, New York, 2002.