
1 Physician Orders for Scope of Treatment: POST Physician Training Revised 06/29/2012.
29
1 Physician Orders for Scope of Treatment: POST Physician Training Revised 06/29/2012
-
Upload
claude-norris -
Category
Documents
-
view
215 -
download
1
Transcript of 1 Physician Orders for Scope of Treatment: POST Physician Training Revised 06/29/2012.

1
Physician Orders for Scope of Treatment: POST
Physician Training
Revised 06/29/2012

2
An Index Case
Mr. Jan, a 71-year-old male with severe COPD and mild dementia, was convalescing at a skilled-nursing facility after a hospital stay for pneumonia. Mr. Jan developed increasing SOB and decreasing LOC over 24 hours. The nursing facility staff called EMS who found the patient unresponsive, with a RR of 8 and an O2 sat at 85% on room air. Although Mr. Jan had discussed his desire to forgo aggressive, life-sustaining measures with his family and nursing personnel, the nursing facility staff did not document his preferences, inform the emergency team about them, or mention his do-not-resuscitate order.
3
After EMS was unable to intubate him at the scene, they inserted an oral airway, bagged, and transported the patient to the emergency department (2nd hospital). Mr. Jan remained unresponsive. He was afebrile, with a systolic BP of 190 mm Hg, P of 105 , RR of 8, and an O2 sat of 88% despite supplemental oxygen. He had diminished breath sounds without wheezes, and a chest X-ray showed large lung volumes without consolidation. Arterial blood gases showed marked respiratory acidosis. The emergency department physician wrote, “full code for now, status unclear.” The staff intubated and sedated Mr. Jan and transferred him to the intensive care unit.
Lynn, et al. Ann Intern Med 2003;138:812-818.

What went wrong?(Could this happen in Virginia?)
Advance Directives not documented DNR order not communicated in
transfer Fragmentation in care (2 hospitals) Overtreatment against patient’s wishes Unnecessary pain and suffering System-wide failure to respect pt’s
wishes Failure to plan ahead for contingencies No system for transfer of plan
4

What is POST? A physician order Can be completed by any provider but must
be signed by qualified MD or DO Compliments, but does not replace, Advance
Directives Voluntary use Recognized by VDH/EMS as a valid DDNR
5

POST is for…
Seriously ill patients* Terminally ill patients Frail and elderly.
6
* chronic, progressive disease’s

Purpose of POST To provide a mechanism to
communicate patients’ preferences for medical treatment across treatment settings
To improve implementation of Advance Care Planning
7
Expected Outcomes of Using POST Process
Improved continuity of care-form transferable across treatment settings
Clearer communication of wishes Reduced hospitalization and inappropriate life-
sustaining treatments Fewer EMS transports!
More accurate representation of preferences Higher adherence to wishes by medical
professionals.

Advance Directive* v. POST
Advance Directive For every adult Requires decisions about
myriad of future treatments Clear statement of
preferences Needs to be retrieved Requires interpretation
POST For the seriously ill Decisions among
presented options Checking of preferred
boxes Stays with the patient A physician’s order to be
followed
9
*Fagerlin & Schneider. Enough: The Failure of the Living Will.Hastings Center Report 2004;34:30-42.
Why POST Works…
MUST accompany patient Contains specifics Physician’s order- no interpretation is needed
POST orders are to be followed
10

POLST – POST – MOST – MOLST
POST Pilot Project
POST was first piloted in Virginia in Roanoke beginning in 2007.
Second POST pilot was in Norfolk/Virginia Beach which began in 2011.
Since then POST Form pilots have expanded around the state.
POST now has the endorsement from the Medical Society of Virginia.
Representative from POST pilots and other stakeholders from around Virginia are represented on the Virginia POST Collaborative.
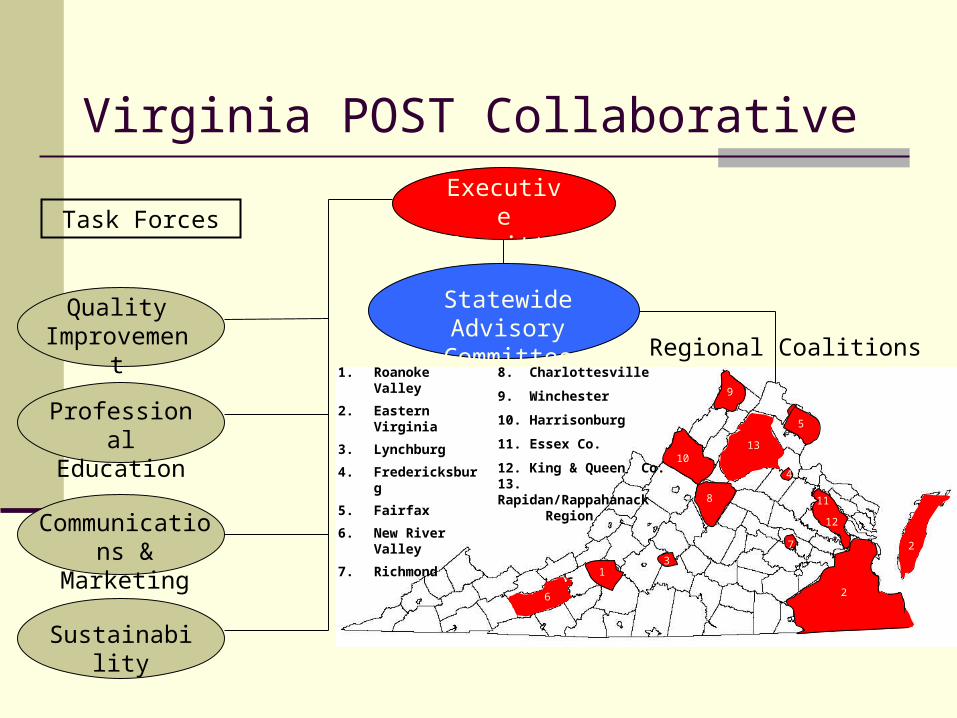
Virginia POST CollaborativeExecutive Committee
Statewide Advisory Committee
Regional Coalitions
Task Forces
Quality Improvement
Professional Education
Communications & Marketing
Sustainability
1. Roanoke Valley
2. Eastern Virginia
3. Lynchburg
4. Fredericksburg
5. Fairfax
6. New River Valley
7. Richmond
8. Charlottesville
9. Winchester
10. Harrisonburg
11. Essex Co.
12. King & Queen Co.13. Rapidan/Rappahanack
Region
13
2
12
2
8
10
9
5
6
13
7
4
11
POST FORM

Checklist…
Verify ID
Verify Code Status with Patient/Agent
Sign & date by physician, physician’s assistant § 54.1-2952.2 or nurse practitioner. § 54.1-
2957.02 per facility/practice protocal.
Indicate Medical Interventions, Antibiotics, Artificial Hydration/Nutrition, who discussed with and setting.

Verify signature of patient OR agent on behalf of patient.
Sections B - D
Sections B – D are currently not covered by any Virginia Statute.
Physicians are encouraged to honor Sections B – D, provided they have examined the POST Form and find all signatures valid including the signature of a license practitioner.
Physician compliance is currently voluntary. If you have concerns, discuss with the patient or
contact the patient’s Healthcare Agent for clarification.
17

Section A: Resuscitation
• DNR orders only apply if a person has no pulse and is not breathing
• Note: This section has 2 choices: Attempt Resuscitation and Do Not Attempt Resuscitation: Check to see which box is checked!
• POST Section A recognized as a valid Virginia Other DNR.
• When Do Not Attempt Resuscitation is checked, qualified healthcare personnel are authorized to honor this order as if it were a Durable DNR order• OEMS approval (Michael Berg)
18
A one only
CARDIOPULMONARY RESUSCITATION (CPR): Person has no pulse and is not breathing.
☐ Attempt Resuscitation ☐ Do Not Attempt Resuscitation (DDNR/DNR/No CPR)
A DNR order in this section qualifies as a Durable DNR order. In no case shall any person other than the patient have authority to revoke a Durable Do Not Resuscitate Order executed upon the request of and with the consent of the patient himself. § 54.1-2987.1.B

Section B
Person has pulse and/or is breathing Comfort Measures Only Limited Interventions Full Interventions – All care above plus intubation and
cardioversion.
19

Section C: Antibiotics
20

21
Section D: Artificial Nutrition and Hydration
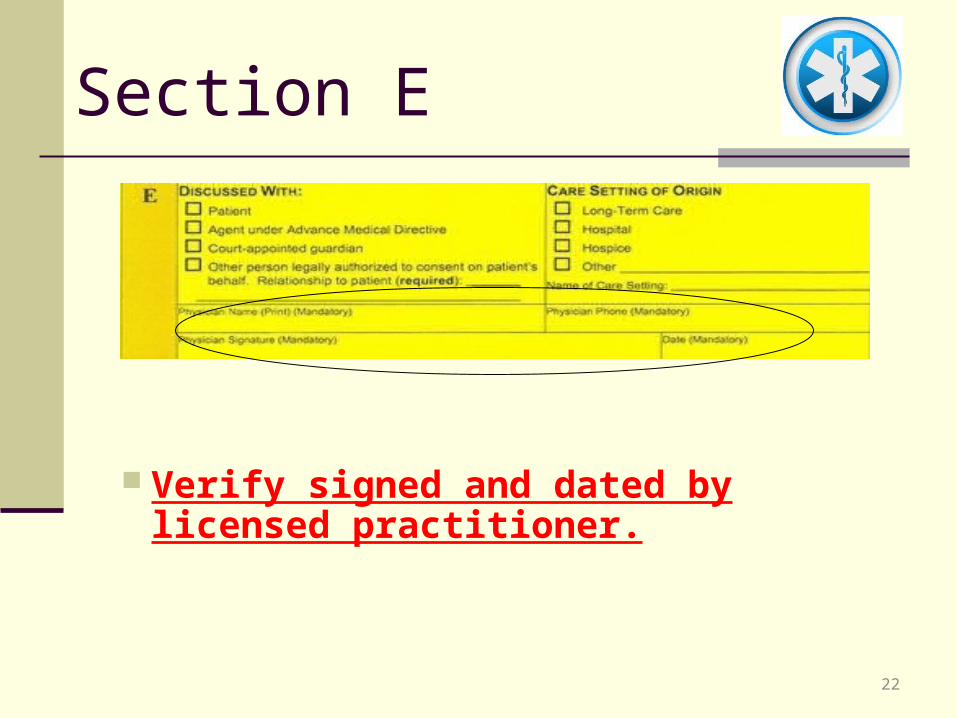
Section E
Verify signed and dated by licensed practitioner.
22

Back of Form
Signature of Patient/POA, and health care professionals completing the form.
Contact information Directions for Health Care Professionals
Verify Patient/Agent has signed.
23

Revocation
Patient can revoke POST Form at anytime. Agent/Family can only revoke Section A -
DDNR if they signed originally on behalf of patient.
If PATIENT signed - Agent/Family CAN NOT revoke Section A DDNR.
§ 54.1-2987.1.B ………In no case shall any person other than the patient have authority to revoke a Durable Do Not Resuscitate Order executed upon the request of and with the consent of the patient himself.
24

“Always ask if your patient might be appropriate for a POST form?”
If so……… you can enter an order in eCare for a Certified POST Facilitator to assist in facilitating the completion of the form……..
25

Form Shall Always Accompany Patient/Resident When Transferred or Discharged!
26
Place on the top of the transfer packet!
Know what the POST form looks like. Know location of POST form in transfer records. Scan POST form into emr. Honor Code Status (SECTION A) During transfer, communicate in your handoff that
patient has a POST form and the contents of all sections.
At receiving facility/unit, communicate that patient has a POST form and its location.
Document turnover of POST Form in your notes.
To Recap…………….

POST completion will improve medical treatment throughout our community.
Use of POST will require communication to make it work in our community
POST follows same guidelines of revocation as DDNR!
28
Take-Home Messages
Questions?
The Eastern Virginia POST Coordinator – David Cochran – 757-388-5977


















