1 of 4: Reducing Neonatal Mortality - Prevention, Early Detection and Treatment of Infections -...
17
BETTER CORD CARE SAVES BABIES LIVES Leela Khanal, Project Director, JSI Chlorhexidine Navi (Cord) Care Program February 13, 2015
-
Upload
jsi -
Category
Health & Medicine
-
view
312 -
download
1
Transcript of 1 of 4: Reducing Neonatal Mortality - Prevention, Early Detection and Treatment of Infections -...
BETTER CORD CARE SAVES BABIES LIVES
Leela Khanal, Project Director, JSI Chlorhexidine Navi (Cord) Care Program February 13, 2015

Nepalese Context of Delivery and Cord Care
45% deliveries occurred at home (Source: MICS 2014)
Among the home deliveries, 82 % used a clean delivery kit or new/boiled blade (Source: NDHS 2011)
Child birth considered an impure and dirty process
Among the home deliveries, 41% of newborns had material on stump (Source: NDHS
2011)
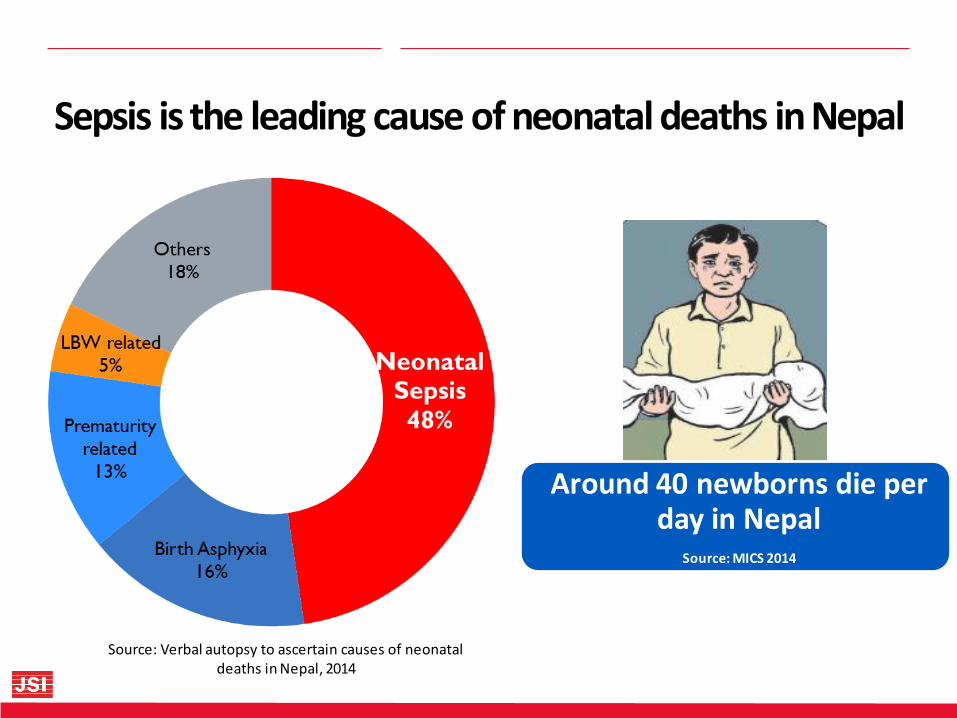
Around 40 newborns die per day in Nepal
Source: MICS 2014
Source: Verbal autopsy to ascertain causes of neonatal deaths in Nepal, 2014
Sepsis is the leading cause of neonatal deaths in Nepal
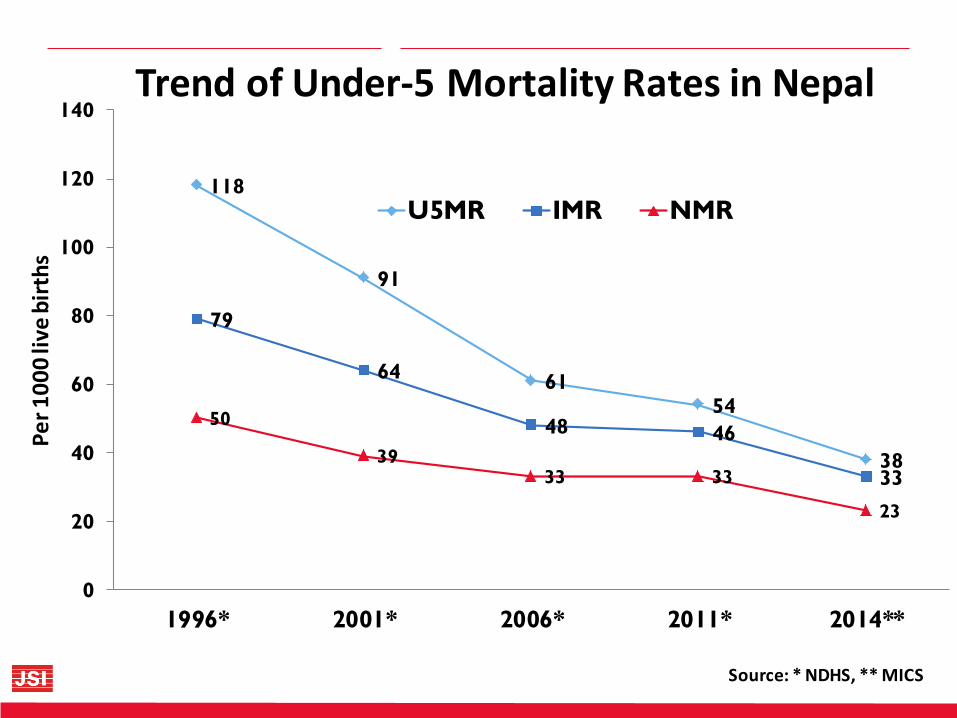
Source: * NDHS, ** MICS
118
91
61 54
38
79
64
48 46
33
50
39 33 33
23
0
20
40
60
80
100
120
140
1996* 2001* 2006* 2011* 2014**
Pe
r 1
00
0 li
ve b
irth
s
Trend of Under-5 Mortality Rates in Nepal
U5MR IMR NMR
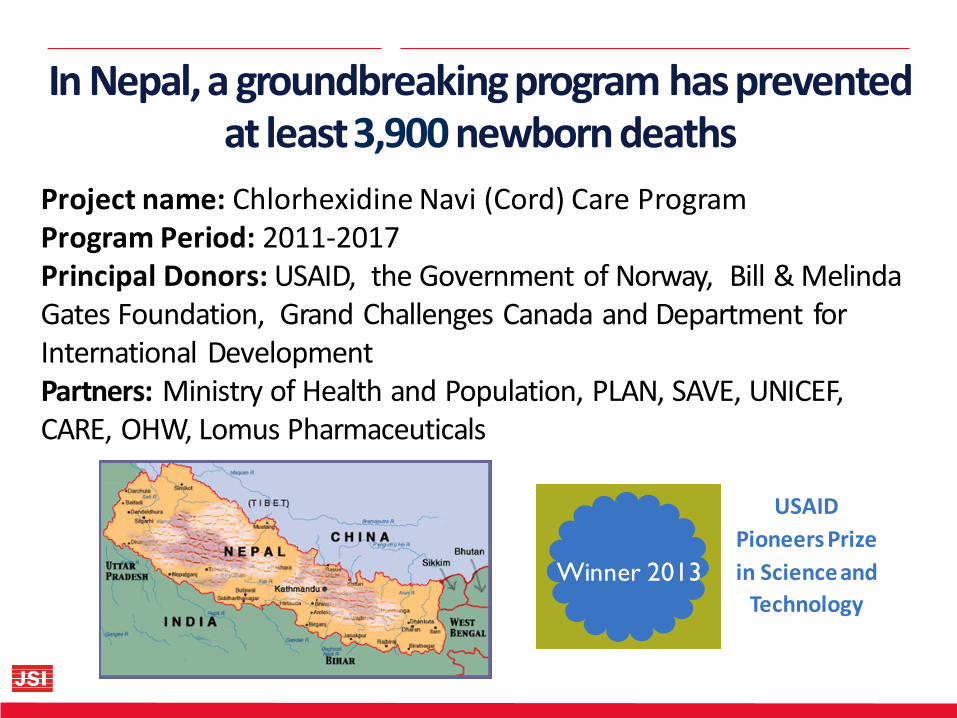
In Nepal, a groundbreaking program has prevented at least 3,900 newborn deaths
Winner 2013
USAID
Pioneers Prize
in Science and
Technology
Project name: Chlorhexidine Navi (Cord) Care Program Program Period: 2011-2017 Principal Donors: USAID, the Government of Norway, Bill & Melinda Gates Foundation, Grand Challenges Canada and Department for International Development Partners: Ministry of Health and Population, PLAN, SAVE, UNICEF, CARE, OHW, Lomus Pharmaceuticals

Addressing a problem with high
population health burden
Efficacy & low cost
Simplicity, acceptability & safety
Low regulatory requirements
Health system compatibility &
scalability
Why Nepal accepted Chlorhexidine (CHX) cord care
First evidence was from Nepal (Source: JHU/NNIPS RCT, 2006)
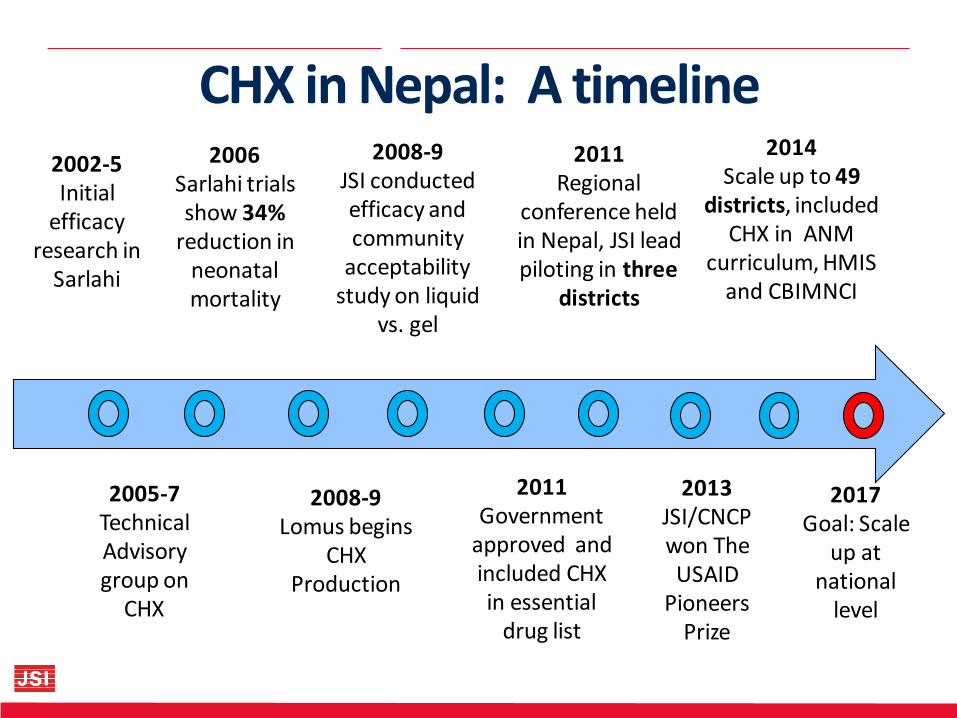
CHX in Nepal: A timeline 2002-5 Initial
efficacy research in
Sarlahi
2008-9 Lomus begins
CHX Production
2006 Sarlahi trials show 34%
reduction in neonatal mortality
2014 Scale up to 49
districts, included CHX in ANM
curriculum, HMIS and CBIMNCI
2017 Goal: Scale
up at national
level
2011 Government
approved and included CHX in essential
drug list
2005-7 Technical Advisory group on
CHX
2008-9 JSI conducted efficacy and community
acceptability study on liquid
vs. gel
2011 Regional
conference held in Nepal, JSI lead piloting in three
districts
2013 JSI/CNCP won The USAID
Pioneers Prize
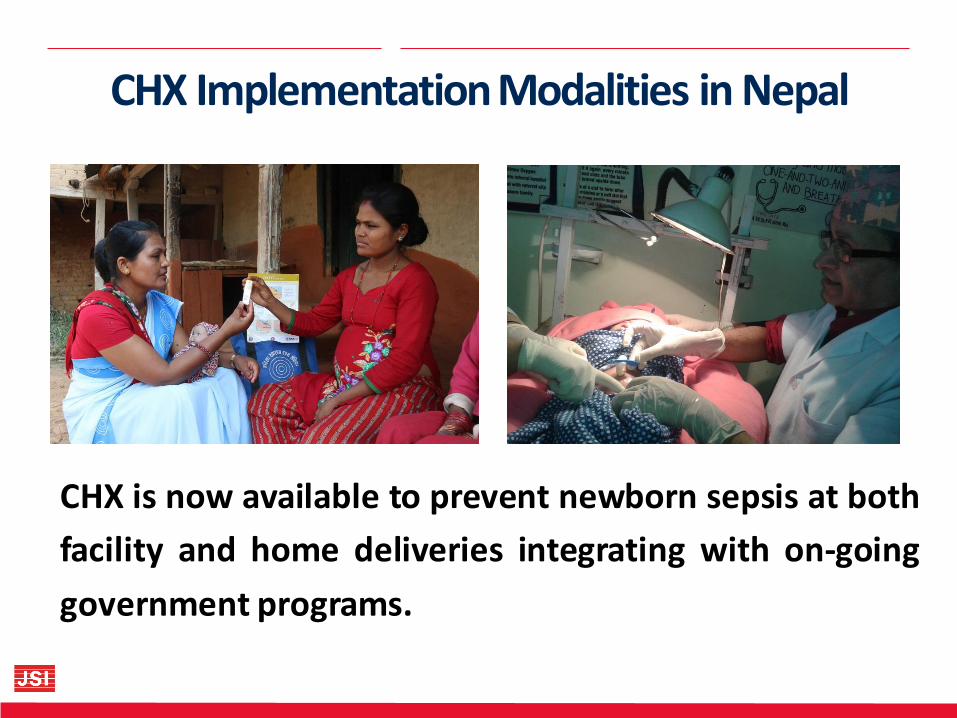
CHX Implementation Modalities in Nepal
CHX is now available to prevent newborn sepsis at both
facility and home deliveries integrating with on-going
government programs.

9
Central Region
Eastern Region
Mid-Western Region
Far-Western Region
Western Region
Humla
Darchula
Baitadi
Dadeldhura
Kanchanpur
Kailali
Doti
Bajhang
Achham
Mugu
Mustang
Manang
Rasuwa
Kalikot
Dailekh
Surkhet
Jumla
Jajarkot
Banke
Rukum
Salyan
Rolpa
Pyuthan
Myagdi
Baglung
Gulmi
Kapilvastu
Arghakhanc
hi
Kaski
Syangha
Rupandehi
Palpa
Lamjung
Tanahu
Gorkha
Chitwan
Dhading
Nuwakot
Makwanpur
Nawalparasi
Pars
a
Bara
Rau
tah
at*
Taplejung
Solukhumbu Sankhuwasava
Sindhupalchowk
Sarl
ah
i
Dh
an
ush
a
Siraha
Saptari
Sindhuli
Kavre
Dolakha
Ramechhap
Okhaldhunga
Udayapur
Morang Jhapa
Ilam
Khotang Bhojpur
Dhankuta
K
L
B
N
Mah
ott
ari
Dang
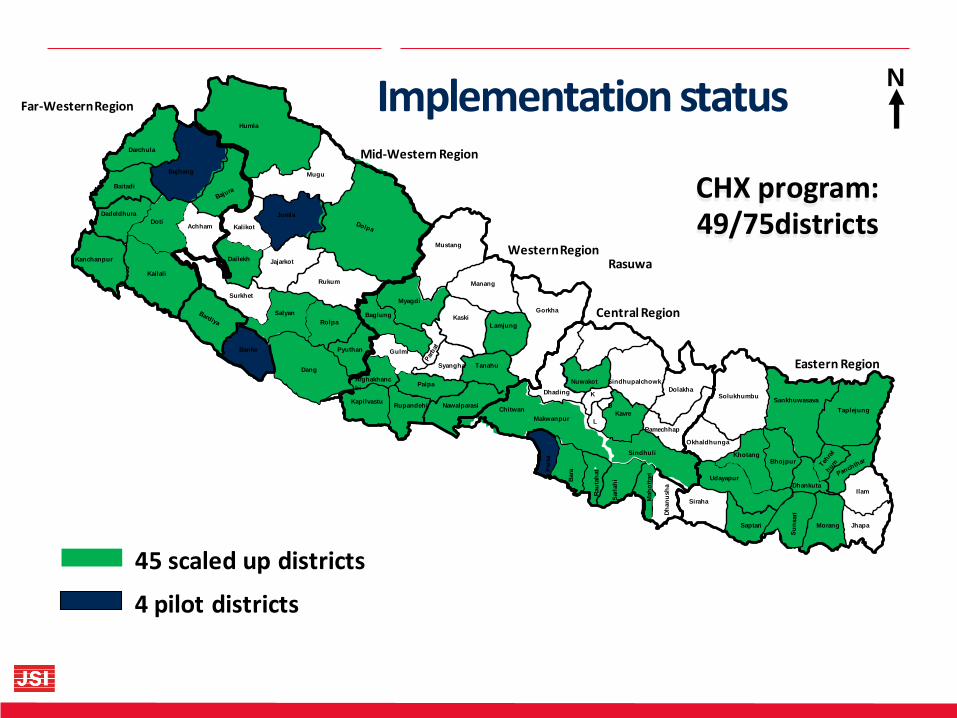
45 scaled up districts
4 pilot districts
Implementation status
CHX program: 49/75districts

11
12
Enabling Factors
1. The involvement of government and implementing partners from initial phase
2. The utilization of existing public health delivery systems to implement
3. The integration with on-going health programs at the health facility and community level
13
Enabling Factors continued
4. The integration of CHX in pre-service and in-service curricula
5. The logistics supply mechanism through the existing government system
6. Ensuring the sustainability through the government ownership of the program (included in the multi-year Procurement plan, HMIS, essential drug list, etc.)
14
Challenges • Maintaining high coverage at scale
• Assuring the quality of the CHX product by
different pharmaceutical companies
• Assuring the quality of routine information
systems
• Ensuring timely supply of CHX
• WHO cord care guidelines need updating
Next Steps 1. Expansion at the national level
2. Continue efforts to ensure the quality of the program
3. Integrate CHX in national health policy documents
4. Include CHX in logistics information system, free drug
list, in-service and pre-service curricula
5. Strengthen routine health information systems
6. Support for uninterrupted supply of CHX
Based on the experience of the Nepal CHX program, we recommend:
• Ensuring government leadership from the start
• Planning integration from the start
• Joining existing networks
• Adding CHX to the essential medicines list
• Leveraging resources from other countries and programs
• Ensuring funding commitments for sustainability

Conclusions • CHX application saves newborn lives
• CHX is safe, acceptable and low-cost
• Harmful cord care practices can be replaced
• Mother or family members can easily apply
• Easy to distribute to pregnant women through community-
based volunteers and antenatal clinics included in the public
health service delivery system
• Other countries with similar conditions should consider CHX to
save newborn lives