1 Male Infertility

of 17
-
Upload
csingleton2364 -
Category
Documents
-
view
226 -
download
1
Transcript of 1 Male Infertility
-
8/12/2019 1 Male Infertility
1/17
MALE INFERTILITY
Yefim R. Sheynkin, M.D.
I. Brief anatomy and physiology of male reproductie system
In order to properly understand the causes and treatment of male
infertility it is essential to appreciate thenormal anatomy and physiology
of male reproduction. Human male reproductive systemincludes hypothalamic-pituitary-testis ais,
the epididymis, vas deferens, seminal
vesicles, prostate and urethra. !roduction ofspermato"oa re#uires approimately $
months from the initial mitotic division. %he
testis is composed primarily of seminiferoustu&ules packed closely together '()* of
testicular volume+, and interstitial cells.
ach tu&ule is $- cm long and /-$
microns in diameter. %here areapproimately ) tu&ules per testis %he
cells 0ithin the seminiferous tu&ules are
germ cells that mature into spermato"oa,and Sertoli cells that serve as supporting
cells for developing germ cells. Sertoli cells
create a &lood-testis &arrier, and separate thegerminal epithelium into &asal and
adluminal compartments. %he ma1or cell in
the interstitial space outside the
seminiferous tu&ule is the
2eydig cell, 0hich producestestosterone, a necessary
component for germ cellmaturation. Spermatogenic
development involves &oth
mitotic and meiotic divisions ofgerm cells. %he mature
spermato"oon is released into
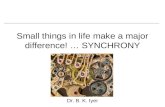
the tu&ule lumen.It is approimately 3 microns
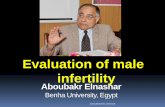
in length. %he head consists of
1
!ead
Midpiece
Tail
Mitochondria
A"oneme
#entral sheath
Microtu$ule
dou$lets % &'()
#entral pair of
microtu$ules
Acrosome*lasma mem$rane
Nucleus
-
8/12/2019 1 Male Infertility
2/17
the condensed nucleus, the acrosome, mem&rane-&ound organelle that contains the en"ymes
re#uired for penetration of the egg prior to fertili"ation.
%he tail consists of a middle piece containing mitochondria, the principal piece, and an endpiece. Sperm form the seminiferous tu&ule enter the efferent ducts connecting the testis to the
caput epididymis. %he epididymis is a single duct / meters in length, and is divided
anatomically into caput 'head+, corpus '&ody+, and cauda 'tail+. pididymis serves as spermconduit and sperm reservoir 0here sperm ac#uire motility and fertili"ing capacity. %he vas
deferens then transports sperm into the pelvis, 0here it 1oins the seminal vesicles to form thee1aculatory ducts, 0hich enter the prostatic urethra.
4ust prior to e1aculation, the testes are &rought close to the a&domen and fluid is rapidlytransported through the vas deferens to the e1aculatory duct and su&se#uently into the prostatic
urethra.
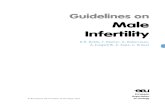
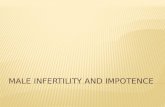
II.EN+,#RIN,L,-Y ,F MALE RE*R,+#TI,N.
!ulsatile hypothalamic release of 56RH stimulates the secretion of 7SH and 2H &y anterior
pituitary. %hese hormones then act at the level of the testis. 2H stimulating testosterone
production &y the 2eydig cells, and 7SH acting on the Sertoli cell to support spermatogenesis.
Serum testosterone and inhi&in ' Sertoli-cell product+ do0nregulate 2H and 7SH secretion vianegative feed&ack loop.
III. Male Factor Infertility
Infertility is defined as a couple8s ina&ility to achieve pregnancy follo0ing one year ofunprotected intercourse. It has &een estimated that 9)-/* of couples attempting to achieve
pregnancy are una&le to do so. : male factor is contri&utory in more than )* of couples
presenting for fertility evaluation. Sperm form the seminiferous tu&ule enter the efferent ductsconnecting the testis to the caput epididymis.
2
%herefore, a thorough evaluation of mal
partner should &e pursued as strongly as female evaluation at the same time. It ha
&een sho0n that the longer couple
remains infertile, the 0orse their chancefor an effective treatment. Initial
screening of the male partner should &e
considered 0henever patient presents 0itchief complaint of infertility regardless of
length of infertility valuation of the
infertile man should include completehistory/ detailed physical e"amination
-erm cells 0ertoli cells Leydig cells
F0!L!*rolactin
0permatogenesis
0e" accessory glandsInhi$in
T
E1
%2) %')
%')
%2)3
%2)
%2)
#orte"Neurotransmitters
-nR! !ypothalamus
*ituitary
-
8/12/2019 1 Male Infertility
3/17
and pertinent la$oratory tests. ;se of detailed 4uestionnairefacilitates the accumulation of
necessary information. %he male reproductive history often helps to eplain a&normal semen
analysis and direct further treatment.
!I0T,RY
(. Fertility history. !roper evaluation &egins 0ith a comprehensive
fertility #uestionnaire. %he age of the partners, detailed history of couple8s
length of infertility, prior pregnancies, miscarriages and a&ortions must &e
ascertained. :ny previous evaluation or treatment should &e noted.
1. 0e"ual history. %oo fre#uent intercourse or compulsive mastur&ation depletes
sperm reserve. Most effective fre#uency of intercourse is every ryptorchidism' (* of men attending an infertility clinic+?progressive and irreversi&le
loss of germ cells. )* of men 0ith a history of unilateral and (* of men 0ith &ilateralcryptorchidism are su&fertile. Ho0ever, paternity 0as documented in =* of men 0ith a
history of unilateral and $)* 0ith a history of &ilateral cryptorchidism. %he effect ofearly' &efore 9 year of life+ corrective surgery is not clear and may not preserve spermatogenicepithelium.
!repu&ertal mumps does not affect testes 0hile postpu&ertal mumps orchitis may cause
severe spermatogenic disorders and testicular atrophy.
Hernia@hydrocele repair? ./* of men 0ith o&structive a"oospermia attending aninfertility clinic 0as found to have iatrogenic in1uries to the vas deferens.
:dolescence
3
89:59:
19:
INFERTILITY
(9: of other;ise healthy men are infertile
,ne in eery < couples in the .nited 0tates is infertile
-
8/12/2019 1 Male Infertility
4/17
%esticular torsion@trauma? !atients 0ith unilateral torsion may &e at risk for contralateral
testicular damage. %he etiology of the contralateral damage is thought to &e immunologically
mediated.
:dult
Many systemic diseases directly or indirectly affect fertility. 1aculatory disorders are
common in patients 0ith dia&etes mellitus, multiple sclerosis, transverse myelitis and spinalcord in1uries. !atients 0ith testicular cancer have impaired pretreatment testicular function and
also are at risk of infertility secondary to various surgical, chemotherapeutic and AR%treatment strategies due to destruction of spermatogonia. Men 0ho under0ent retroperitoneal
lymph nodes dissection are at risk of e1aculatory failure due to damage of sympathetic chain
overlying aortic &ifurcation. :ny recent fe&rile illness may cause significant, &ut usually transient, damage to
spermato"oa. %herefore semen analysis should &e repeated in at least $ months.
%he history should include detailed revie0 of medications and eposure to environmentalgonadotoins. Medications that affect spermatogenesis include cimetidine, ketocona"ole,
spironolactone,dilantin, caffeine, sulfasala"ine, colchicine, allopurinol, calcium channel
&lockers. Mari1uana, heroin, cocaine, alcohol, nicotine sho0ed Spermatotoic effect.%he use of ana&olic steroids &y athletes suppresses gonadal function &y depressing pituitaryoutput of 2H and 7SH through feed&ack inhi&ition. %he usual results are severe oligospermia
or a"oospermia, 0hich is usually, &ut not al0ays, reversi&le after discontinuation of steroids.
*!Y0I#AL E=AM
!hysical eamination is performed in a ;arm room $y an e"aminer ;ith ;arm2
gloed handssince contraction of dartos muscle induced &y lo0 temperature makes
eamination of scrotal contents difficult. !hysical eamination &egins 0ith thorough
o&servation of the general status and &ody ha&itus of the patient as 0ell as secondary secharacteristics. Incomplete masculini"ation 0ith disproportional long etremities due to
deficient androgen stimulation re#uired for epiphyseal closure at time of pu&erty often
indicates Bleinfelter8s syndrome.%he thyroid is palpated and heart and lungs auscultated. %he &reasts are o&served and
palpated for gynecomastia ' may &e associated 0ith estrogen secreting testicular tumors,
adrenal tumor and liver disease+. 5alactorrhea may &e associated 0ith prolactin-secretingpituitary adenoma. !alpation and percussion of a&domen then performed.
!enis and urethral meatus are eamined for condylomata, discharge, position of the
meatus' hypospadia+ Scrotal eamination is first performed 0ith patient supine. %his allo0s varicocele, if
present to collapse. : large varicocele that does not collapse 0arrants a search fora&dominal mass.
Normal testesare firm, a&out ongenital &ilateral a&sence of the vas deferens 0as o&served in 9.$*
4
-
8/12/2019 1 Male Infertility
5/17
of men presenting for infertility evaluation. %his condition is associated 0ith renal agenesis
and a&normalities in /* of patients, therefore renal sonogram should &e o&tained. Men
0ith this condition may test positive for cystic fi&rosis gene mutation.
>aricocelemay &e graded in severity as follo0s?
5rade I? present only 0ith Calsalva 5rade II? present 0ithout Calsalva
5rade III? visi&le through the skin ' &ag of 0orms +
Digital rectal eamination is al0ays performed for evaluation of the prostate for masses,cysts, irregularities. Stool should &e tested for occult &lood.
N+ER0TAN+IN- 0EMEN ANALY0I0
0ource >olume #haracteristics
rethral and$ul$ourethral glands
9.(29.1cc >iscous/ clear
Testes/ epididymides/asa
deferentia
9.(29.1cc 0perm present
*rostate 9.82(.9cc Acidic/;atery
0eminal esicles (.925.9cc Al?aline/gelatinous/
fructose positie
#omplete e6aculate 1.928.9cc Li4uefies in 19218min
0emen analysis is not a test for fertility. 7ertility determination is a couple-related
phenomenon that re#uires the initiation of a pregnancy. !atient cannot &e declare fertile&ased only on normal semen analysis. It 0as sho0n that $* of all patients 0ith normal
semen analysis have a&normal sperm function .Semen specimen are o&tained &y mastur&ation into a sterile 0ide-mouth container after
/-) days of a&stinence and analy"ed 0ithin 9 hour of collection. %ypically t0oe semen
analyses are o&tained over 9 months period prior to making any final conclusion regarding
&aseline sperm #uality or #uantity.
0emen analysis@ #ommonly used normal parameters
>,LME 1.9 MLp! .12.C
#,N#ENTRATI,N 19"(9IABILITY 89:
M,R*!,L,-Y 59: IT! N,RMAL M,R*!,L,-Y
B# ("(9
-
8/12/2019 1 Male Infertility
6/17
+efinitions?
Azoospermia: no sperm
Oligospermia: low sperm concentration Aspermia no ejaculate
Asthenospermia: low motility
Teratospermia: poor morphology
Normal e6aculate olumeis &et0een / and 3 ml. 3)*of the volume is from seminalvesicles, $-$)* is from the prostate and only )* from the vasa. 6ormal semen pH is ./-=..
!rostatic secretion is acidic 0hile seminal vesicle fluid is alkaline' seminal fructose derivedfrom seminal vesicles+. :"oospermia 0ith lo0 e1aculate volume , fructose negative and acidic
may imply o&struction of the e1aculatory ducts. pH over =. may indicate infection
#oncentration? a"oospermic specimen contains no sperm, oligoseprmic specimen reveals
concentration of less than /93@ml and normospermic specimen contains more than
/93@ml.
Motility and for;ard progression? normally E)* of sperm in the specimen are motile.
7or0ard progression descri&es ho0 fast the motile sperm are moving' normal /F in the scalefrom to ompared to somatic cells, sperm
contain an unusually high percentage of polyunsaturated fatty acids in their mem&ranes. %his,
ho0ever, is an essential prere#uisite for normal sperm mem&rane function, &ut makes sperm inparticular suscepti&le for oidation &y reactive oygen species 'RS+, 0hich cause lipid
peroidation. In etreme cases this might result in a dramatic loss of normal sperm function orimpaired mem&rane integrity , thus indicating decreased fertili"ing capa&ility of spermato"oa.
idative damage to spermato"oa is closely correlated 0ith inflammatory processes in thegenital tract and occurrence of leukocytes that generate at least 9 times more RS than
spermato"oa themselves. Several authors revealed that $-
-
8/12/2019 1 Male Infertility
7/17
antioidants may &e a&le to tolerate greater concentrations of seminal leukocytes. Despite an
apparently a&normal threshold level for leukocytes 0ithin the semen, a 0ide range of
conflicting evidence still eists as to the significance of seminal leukocytes, normal num&er ofJ> and infertility
+NA integrity
D6: fragmentation is closely related to fertili"ation D6: fragmentation can &e measured&y different methods including %;62 assay, S>SI ' Sperm >hromatin Structure :ssay+ or
7ISH assays. D6: fragmentation inde ' D7I+ assessed as * sperm 0ith fragmentedD6:' &y S>SI+ indicates ?
KcellentL fertility potential if 9)* K5oodL fertility potential if 9)-/(.(*
K!oorL fertility potential if E$*
It seems that patients that have a treatment 0ith assisted reproductive technologies, especially
0ith I>SI, have a significantly higher risk that sperm 0ith fragmented D6: fertili"e an oocyte
that may lead to em&ryo death and higher rate of miscarriage.Ho0ever, high D7I inde does not preclude a normal full-time pregnancy. %here is still noa&solute cut-off point for S>S: that 0ill preclude success for natural pregnancy or for
IC7@I>SI
Fructose? 7ructose is androgen-dependent and is produced in the seminal vesicles. 7ructose
levels should &e determined in any patient 0ith a"oospermia and especially in those 0hose
e1aculate volume is less than 9 ml, suggesting seminal vesicle o&struction or atresia. :&senceof fructose, lo0 semen volume, and failure of the semen to coagulate indicate either congenital
a&sence of the vas deferens and seminal vesicles or o&struction of the e1aculatory duct.
Additional ealuation includes :ntisperm :nti&odies testing and advanced sperm functiontests ' Sperm !enetration :ssay, Hemi"ona :ssay, test for acrosome reaction e.t.c+
Endocrine ealuation.
ndocrine evaluation includes measurement of serum testosterone, follicle-stimulatinghormone'7SH+, luteini"ing hormone'2H+ and prolactin.
Testosteroneis good measure of 2eydig cells function.F0! &inds to Sertoli cells and stimulates #uantitatively normal spermatogenesis . 7SH
crudely reflects the status of seminiferous epithelium .:mong men presenting 0itha"oospermia, serum 7SH level that is greater than t0ice the upper limit of normal is
suggestive of intrinsic testicular failure..
L!is stimulatory to the 2eydig cells and testosterone production.
*rolactinlevel should &e o&tained in patients 0ith a history of galactorrhea, visual changes
and @or lo0 levels of testosterone, 7SH,2H levels. !rolactin is produced &y the cells of the
anterior pituitary. levated serum prolactin represents a pathological state that may indicate asignificant underlying pituitary a&normality contri&uting to male reproductive failure. %he
ma1ority of men 0ith elevated serum prolactin levels 0ill also manifest decreased serum
7
-
8/12/2019 1 Male Infertility
8/17
testosterone. Significant elevation of prolactin may result from prolactin secreting pituitary
macroadenoma and 0hich re#uires head >% or MRI for the diagnosis.
Estradiol levels should &e o&tained in patients 0ith gynecomastia or in patients 0ith signs offemini"ation.
Thyroid diseasemay rarely result in infertility ',.)* of infertile men+, &ut this is usually
associated 0ith uncontrolled hypo-or hyperthyroidism
F0! L! T +iagnosis E"ample
!igh !igh Lo; !ypergonadotropic
!ypogonadism
GlinefelterHs
syndrome
Lo; Lo; Lo; !ypogonadotropic
hypogonadism
GallmannHs
syndrome
I>. +iagnostic procedures
Diagnostic testis $iopsy is indicated in patient 0ith a"oospermia or severe oligospermia,
normal testicular volume and consistency, palpa&le vas deferens and normal serum 7SHin
order to differentiate o&structive from non-o&structive a"oospermia. pen &ilateral &iopsy is
the safe techni#ue and performed through &ilateral 9-cm transverse scrotal incision, a0ay fromthe epididymis.%esticular &lood supply consists of internal spermatic artery'from a&dominalaorta+, deferential artery'from internal iliac or superior vesical artery+ and cremasteric artery
'from inferior epigastric artery+. Jiopsy incision is recommended in the upper medial and
lateral surfaces of the testis 0ith fe0er arteries in these areas. Incision is carried do0n totunica al&uginea. :fter opening of the tunica al&uginea the etruded tu&ules are cut 0ith sharp
iris scissors and immediately deposited into B,INs solution. NE>ER 0E F,RMALIN.If testis &iopsy revealed normal spermatogenesis in patient 0ith a"oospermia, o&struction of
the epididymis, vas deferens or e1aculatory duct should &e suspected. %estis &iopsy in patients
0ith nono&structive a"oospermia may reveal different histological patterns including Sertoli-
cell only, maturation arrest, hypospermatogenesis.
Recently diagnostic testicular &iopsy is mostly performed together 0ith therapeutic testis &iopsy
' sperm retrieval and cryopreservation + and not necessarily as a separate procedure
>asographyis radiological procedure, 0hich is used to evaluate patency of the vas deferens. Itshould &e performed ,NLYat the time of planned reconstruction. %he vas deferens is
approached via scrotal incision, hemitransected and cannulated 0ith /) gauge angiocath sheath
. Diluted 0ater-solu&le contrast media instilled for formal vasography and A-ray performed.
Casography site has to &e closed microsurgically.
Transrectal ltrasound %TR0)@ %he principal application of %R;S in infertile men is to
evaluate the patency of distal ecurrent duct system of the male genitalia. %he prostate, seminalvesicles, ampulla of the vas deferens may &e easily visuali"ed &y transrectal ultarsonography.
%R;S is indicated in patients 0ith a"oospermia, normal testicular si"e, normal 7SH and lo0
8
-
8/12/2019 1 Male Infertility
9/17
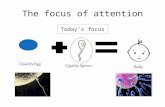
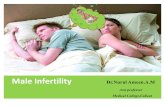
#entromere
AJFa
AJF$
AJFc
0RY
AJF region containing +AJ
The Y2#hromosome and Male Infertility
AJF region containing +AJ
e1aculate volume in 0hom o&structive etiology of a"oospermia is suspected. Dilated seminal
vesicles' E9.) cm 0ide+ may &e aspirated and fluid eamined microscopically. !resence of
sperm confirms o&struction of the e1aculatory ducts and the a&sence of epididymalo&struction.
>.-ENETI# ,F MALE INFERTILITY
Specific genetic a&normalities are associated 0ith a"oospermia@severe oligospermia in men
A. #ystic fi$rosis gene mutations. >ongenital &ilateral a&sence of the vas deferens '>J:CD+ isfound in 9-/* of the infertile male population, and J:CD 0ill have one ormore cystic fi&rosis gene mutations detecta&le. >onversely, ()* of men 0ith cystic fi&rosis
manifest infertility due to &ilaterally a&sent vasa. In addition, up to
-
8/12/2019 1 Male Infertility
10/17
spermatogenesis. 6on-o&structive a"oospermia or poor sperm production may occur 0hen this
gene is deleted.verall prevalence of Y chromosome microdeletions - =* '9*-$)*+. D:Ogene 'Deleted in :"oospermia+ 0as found to &e a&sent in 9$* of a"oospermic men. D:O gene0as proposed as a candidate gene for :O7. %hree relatively discreet regions of Y# 'AJFa/ AJF$/
and AJFc+ 0ere found to &e deleted in non-o&structive a"oospermia and severe oligospermia.:particular type of Y-chromosome microdeletion in patients 0ith non-o&structive a"oospermiamay predict the a&sence of sperm 0ith testicular sperm etraction.AJFa and AJF$
microdeletions have &een associated 0ith more severe testicular changes inclduing Sertoli cell-only and spermatogenic arrest and less chances in finding sperm. AJFcmicrodeletions have
&een associated 0ith less testicular changes and higher success in sperm retrieval. Since Y-chromosome a&normalities are passed on to any offspring produced &y assisted
reproduction, these offspring are at risk of infertility. Since the fathers are usually other0ise
healthy, the presence of ma1or medical illness transmitted 0ith Y-chromosome microdeletionsappears unlikely. Ho0ever, the ans0er to this #uestion may &e delayed for years 0hen children
&orn from assisted reproduction gro0 up.
All men ;ith aKoospermia or seere oligospermia should $e tested ;ith ?aryotype
analysis / #ystic Fi$rosis % $oth partners) and Y2chromosome microdeletions ealuation
prior to the application of I>FDI#0I. *atients ;ith diagnosed genetic a$normalities must
hae detailed genetic counseling.
TREATMENT ,F MALE INFERTILITY
I. 0pecific treatment @ Identifia$le causes
% e.g. ,$struction/ >aricocele/E6aculatory dysfunction
Endocrinopathy/ Infection)
II. Empirical Medical treatment @ Idiopathic Infertility
III. Assisted reproduction technologies@ 0perm retrieal
>aricocele
Caricocele is the most common identifia&le and treata&le cause for male factor infertility.It is an a&normal dilatation of veins that drain the testis. Caricocele is found in 9)* of men
in general population &ut in a&out $)* of men &eing evaluated for infertility.
Caricocele has &een sho0n to affect all seminal parameters ' sperm concentration, motilityand morphology+ , sperm function, testicular si"e and histology. : varicocele may also cause
progressive testicular dysfunction over time, 0hich is more dramatic than the small changes
10
-
8/12/2019 1 Male Infertility
11/17
epected &y aging alone. Some studies indicate adverse effect of varicocele in
hormonal' mainly testosterone+ production.
%he pathophysiology of varicocele remains unclear, although the most likely mechanism ispro&a&ly elevation of scrotal temperature.
!atients 0ith larger varicocele eperience significantly greater seminal improvement
postoperatively. Recent studies also confirmed the effect of su&linical varicocele repair onpregnancy rates .
2imited controlled randomi"ed studies sho0ed improvement in seminal parameters and
pregnancy rates after surgical repair of the varicocele compare to control group.
Author *atients *regnancy rate
-oldstein/ (&&1/(&& 0urgery
#ontrol
75:
(:
Marmar/ (&&7 0urgery
#ontrol
5ARI#,#ELE RE*AIR
I. !ersistent a&normalities in count, motility or morphology
II. Decreased testicular si"e ' /* and more+III. Scrotal discomfort@pain
%he &est method for diagnosing a varicocele is a good physical eamination in standing
position.. :dditional tests are helpful in certain e#uivocal clinical situations and include
Doppler sonography, venography, thermopgraphy and radionuclide scrotal scan.
:ll these methods are not a gold standard and have a high range of false-positive and false
negative results.%he goal of treatment is to o&struct the refluing venous drainage to the testis 0hile
maintaining arterial inflo0 and lymphatic drainage.
Techni4ues of >aricocelectomy
Techni4ue Artery
presered
!ydrocele Failure *otential for
serious
mor$idity
Retroperitoneal No : (8218: NoInguinal No 5259: 82(8: No
Laparoscopic Yes (1: 382(8: Yes
Radiographic
em$oliKation
Yes 9: (8218: Yes
Microscopic
su$inguinal
Yes 9: (: No
7or each couple, the relative risks and &enefits of varicocelectomy must &e 0eighed against
alternative treatment 0ith assisted reproductive techni#ues' I;I, I7C, IC7@I>SI+
11
-
8/12/2019 1 Male Infertility
12/17
AKoospermia
&structive 6ono&structive
Epididymis
>as deferens
E6aculatory ducts
0permatogenic failure
Retrograde E6aculation
'I>SI+, treatment of most men 0ith a"oospermia can no0 &e considered, even if the a"oospermia
is caused &y testicular failure. !rior to initiating treatment for a couple in 0hom the man hasa"oospermia, it is important to distinguish 0hether the lack of sperm in the e1aculate is from an
o&structive or non-o&structive process.
,$structie aKoospermiamay &e congenital '>J:CD- >ongenital :&sence of the CasDeferens,+ or ac#uired' infection, stricture, vasectomy+ , repara&le or nonrepara&le.
&struction of the ecurrent duct system may occur at any level from efferent ductules to
e1aculatory duct. :&sence of sperm should &e confirmed &y centrifugation of semen specimen.&structive a"oospermia is suggested in patients 0ith normal testicular volume, full
epididymis and normal hormonal studies. 6et step is testicular &iopsy, 0hich should confirm
the presence of normal spermatogenesis.>ongenital a&sence of the vas deferens in most of thecases may &e diagnosed &y physical eam and testicular &iopsy is not indicated. 1aculatory
duct o&struction is suspicious in men 0ith lo0 volume ' less than 9 cc+ or a&sent e1aculate,
negative fructose test, acidic semen pH, normal 7SH and normal testicular volume .%ransrectal ultrasound may confirm dilatation of seminal vesicles ' .9.) cm+ or midline
prostatic cyst.
hen a diagnosis of o&structive a"oospermia is esta&lished, a 0ide variety of treatment
options may &e considered &efore an optimal treatment option is determined for an individualcouple8s situation. %reatment options include microsurgical reconstruction 'vasovasostomy
and vasoepididymostomy+, transurethral resection of the e1aculatory ducts '%;RD+ and
assisted reproductive technologies ':R%+. Sperm retrieval 0ith :R% 'IC7-I>SI+ is thetreatment of choice for men 0ith reproductive tract o&struction 0hen restoration of genital tract
continuity is not possi&le or associated 0ith etremely lo0 success rates 'congenital anomalies,
severe loss of vasal length, failed multiple reconstructive procedures, female factors re#uiring
assisted reproduction+. :lthough sperm retrieval techni#ues may &e universally applied to anypatient 0ith o&structive a"oospermia, :R% may not &e advisa&le 0hen specific, more cost-
effective treatment is availa&le.
%he principles of microsurgical reconstruction are to approimate healthy tissue,maintain a good &lood supply 0ithout tension on the anastomosis, using accurate mucosa to
mucosa approimation.Microsurgical asoasostomy %>>) is performed to correct
repara&le o&struction of the vas deferens.
12
2ittle more than a decade ago,patients 0ith a"oospermia 0ere
often una&le to &e successfully
treated. Since the introduction ofintracytoplasmic sperm in1ection
-
8/12/2019 1 Male Infertility
13/17
>asoepididymostomy%>E)is indicated for cases of
epididymal o&struction. !resently most common thechni#ue is
microsurgical end-to side invagination' triangulation or < pointinvagination 0ith longitudinal or transverse incision of the
epididymal tu&ule+. : microsurgical approach is necessary to
allo0 accurate approimation of the vasal mucosa to that of a
single epididymal tu&ule. Casoepididymostomy is a complemicrosurgical procedure re#uiring significant eperience to
achieve optimal results. It should only &e undertaken &y
surgeons 0ith epertise in this techni#ue.
!atency rates follo0ing CC and C are (* and 3-*
respectively 0hen motile sperm are found. Ho0ever, pu&lishedpregnancy rates range from )-* after vasovasostomy and only /-SI. :ll of these procedures may &e performed undergeneral or local anesthesia.
TFNA. Testicular Fine Needle Aspiration involves placing a //-gauge needle into the testis.
Significant negative pressure is applied 0ith a 7ran"en needle holder and the needle is passed
in and out the testicle in order to disrupt the seminiferous tu&ules. %his procedure should &eperformed using a single puncture of the tunica al&uginea to minimi"e the risk of in1ury to
testicular vessels under the tunica al&uginea. Several ad1acent regions of the testis may &e
sampled through a single needle hole.*TNB% *ercutaneous testis needle $iopsy). %his is
a minimally invasive small &iopsy that is rapid,
simple and easy to learn. e use a 9
-
8/12/2019 1 Male Infertility
14/17
syringe is inserted into the caput epididymis and 0ithdra0n gently until fluid is seen entering
the tu&ing of the aspiration set. %he procedure is repeated until ade#uate amounts of
epididymal fluid 0ith motile sperm are retrieved.
ME0A% Microsurgical epididymal sperm aspiration). Microsurgical epididymal sperm
aspiration involves a linear incision in the epididymal tunic and se#uentially puncturing
individual epididymal tu&ules under an operating microscope at 9-/) po0er. : siliconi"edglass micropipet attached to an aspiration device consisting of a 9 cc glass syringe and a 9 cc
plastic tu&erculin syringe may &e used. Microliter #uantities of epididymal fluid pass into themicropipet, through the silastic tu&ing and the plastic syringe. Se#uentially more proimal
punctures 0ere performed until optimal sperm #uality 'motility+ 0as o&served. MS: is anopen surgical procedure that re#uires microsurgical eperience &ut it allo0s sperm retrieval
from over ((* of men 0ith o&structive a"oospermia, even if etensive scarring is present from
multiple prior scrotal procedures. MS: also allo0s retrieval of an ade#uate num&er andmotility of sperm to relia&ly cryopreserve sperm for su&se#uent fertility attempts.
!ercutaneous procedures are less invasive and do not re#uire microsurgical skill.
Ho0ever, sperm are not relia&ly retrieved from the epididymis using percutaneous approaches,and sufficient sperm num&er and #uality are also not typically o&tained from the testis for
cryopreservation. %he pregnancy rates achieved after retrieval of testicular spermato"oa 0ith
I>SI have ranged from /* to )*. !regnancy rates 0ith percutaneous epididymal spermretrieval or MS:-I>SI have ranged from /
-
8/12/2019 1 Male Infertility
15/17
preserved. It commonly seen in patients 0ith dia&etes. Diagnosis re#uires poste1aculate urine
analysis 0hich reveals high sperm concentration
+rug +ose
*seudoephedrine hydrochloride hang %SB? %he testis, epididymis,and ductus deferens, in !hysiology of
Male reproduction, >hapter alsh et al.,eds. >amp&ell8s;rology, Seventh
dition, .J.Saunders >o., !hiladelphia, !:, 9((5. Sigman M? 2a&oratory testing in the evaluation of male infertility. orld 4 ;rol
9(($P99?(3
7. orld Health organi"ation 'H+ Manual for amination of Human Semen and Semen-
>ervical Mucus Interaction.9((/, >am&ridge, ngland?>am&ridge ;niversity !ress
8. !olansky, 7.7., 2am&, .4.? Do the Results of Semen analysis !redict 7uture 7ertilityQ :
Survival analysis. 7ertil Steril 9(==Plin 6orth :m 9(=P9
-
8/12/2019 1 Male Infertility
16/17
4. ;rol 9(=(P9
-
8/12/2019 1 Male Infertility
17/17
/
5. Hopps >C, 5oldstein M, Schlegel !6.%he diagnosis and treatment of the a"oospermic
patient in the age of intracytoplasmic sperm in1ection. ;rol >lin 6orth :m. //6ovP/('lin 6orth
:m. /$ 7e&P$'9+?9ell ndocrinol. // 4an /)P9=3'/+?93$-.
79. ood S, 2e0is-4ones I, %roup S, Desmond :, Bingsland >.Surgical sperm retrieval? arevie0 of current practice. Hum 7ertil '>am&+. // 7e&P)'9+?9-//
7(. Marmar 42 %he pathophysiology of varicoceles in the light of current molecular andgenetic information. Hum Reprod ;pdate. /9 Sep-ctP')+?lin ndocrinolMeta&. / 4unP9