1. Field Epidemiology Field Epidemiology NATIONAL INSTITUTE ...
11
1. Field Epidemiology 1.1. MAE-FETP Training programme The Master of Applied Epidemiology (MAE) is a Field Epidemiology Training Programme (FETP) designed to develop a cadre of professional epidemiologists capable of identifying and addressing the public health needs and priorities of a country efficiently and effectively. 1.1.1. Objectives The objectives of the MAE-FETP course at NIE are to: a. Strengthen the Human Resource Base in Epidemiology by fostering the development of field-trained epidemiologists in the country. b. Build the capacity of Public Health Programme managers for developing and establishing sensitive disease surveillance systems, early detection, preparedness and rapid response to outbreaks. c. Enhance the health status of people across their life spans. 1.1.2. Course Description The MAE-FETP course has been ongoing at NIE as an off campus degree programme of the Sree Chitra Tirunal Institute of Medical Sciences and Technology (SCTIMST), Thiruvananthapuram, since January 2001. Five batches, totalling 37 scholars, have been admitted, from different states in the country (Kerala, Orissa, Andhra Pradesh, Madhya Pradesh, West Bengal, Mizoram, Himachal Pradesh, Maharashtra, Bihar, Uttaranchal, Andaman & Nicobar Islands and Tamilnadu) since its inception. The MAE-FETP is a 2 year course consisting of upto 6 months contact sessions at NIE , and 18 months practical field experience in the scholars' district/state. The philosophy of training methodology adopted is "learning-by-doing" through "practical hands on field experience". Guidance and supervision to scholars are provided by NIE core faculty, local preceptors and technical advisors. Assessment of scholars is continuous, competency oriented and based on multiple methods e.g. class and home assignments, class participation, group discussions, problem solving, satisfactory Field Epidemiology 1 NATIONAL INSTITUTE OF EPIDEMIOLOGY
Transcript of 1. Field Epidemiology Field Epidemiology NATIONAL INSTITUTE ...

1. Field Epidemiology
1.1. MAE-FETP Training programme
The Master of Applied Epidemiology (MAE) is a Field Epidemiology Training Programme
(FETP) designed to develop a cadre of professional epidemiologists capable of identifying and
addressing the public health needs and priorities of a country efficiently and effectively.
1.1.1. Objectives
The objectives of the MAE-FETP course at NIE are to:
a. Strengthen the Human Resource Base in Epidemiology by fostering the development of
field-trained epidemiologists in the country.
b. Build the capacity of Public Health Programme managers for developing and establishing
sensitive disease surveillance systems, early detection, preparedness and rapid response
to outbreaks.
c. Enhance the health status of people across their life spans.
1.1.2. Course Description
The MAE-FETP course has been ongoing at NIE as an off campus degree programme of the Sree
Chitra Tirunal Institute of Medical Sciences and Technology (SCTIMST), Thiruvananthapuram,
since January 2001. Five batches, totalling 37 scholars, have been admitted, from different states
in the country (Kerala, Orissa, Andhra Pradesh, Madhya Pradesh, West Bengal, Mizoram,
Himachal Pradesh, Maharashtra, Bihar, Uttaranchal, Andaman & Nicobar Islands and Tamilnadu)
since its inception.
The MAE-FETP is a 2 year course consisting of upto 6 months contact sessions at NIE , and 18
months practical field experience in the scholars' district/state. The philosophy of training
methodology adopted is "learning-by-doing" through "practical hands on field experience".
Guidance and supervision to scholars are provided by NIE core faculty, local preceptors and
technical advisors.
Assessment of scholars is continuous, competency oriented and based on multiple methods e.g.
class and home assignments, class participation, group discussions, problem solving, satisfactory
Field Epidemiology 1
NATIONAL INSTITUTE OF EPIDEMIOLOGY

completion of assigned field projects and defence of dissertation through a viva voce
examination.
1.1.3. Visits of External Faculty:
a. Dr. Rubina Imtiaz - Participated in the teaching programme of IV cohort
b. Dr. Hoang Dong - Demonstrated Horizon live programme for III cohort
scholars and FETP Faculty
c. Ms. Nadine Sunderland - Developed a needs assessment tool for conduct of
needs assessment to plan for a mentoring workshop
d. Dr. Elliott Churchill - Conducted one week
training programme in
"Excellence in Scientific
Writing" for IV cohort
scholars and NIE Scientists
e. Dr. Shuba Kumar - Conducted two days training
programme in Qualitative Research methods
1.1.4. Participation of FETP Scholars in National and International Conferences
a. Assisted scholars in preparation and submission of abstracts for national and international
conferences
b. Assisted scholars in preparation of oral and poster presentations for national and interna-
tional conferences
1.1.5. Achievements
a. All six scholars from the II cohort successfully completed the MAE-FETP Course
b. Of the six scholars who graduated, 2 have been placed in Training Institutes, 2 as State
Epidemiologists, in-charge of IDSP activities, 1 as Deputy Director of Health Services,
in-charge of District level Health Programmes and 1 in-charge of Population Development
Project at district level
Field Epidemiology 2
NATIONAL INSTITUTE OF EPIDEMIOLOGY

c. The MAE-FETP at NIE was assessed by an assessing team from SCTIMST and granted
continuation of affiliation for another five years i.e. up to 2008.
d. Nine scholar/graduates attended III TEPHINET Global Scientific Conference at Beijing,
China in November 2004.
e. One Scholar from I Cohort, was selected and deputed with scholarship to participate in
a writers workshop at CDC Atlanta
f. Four scholars from III Cohort submitted proposals for CDC/TEPHINET Micronutrient
Malnutrition (MNM) Projects. All four proposals were accepted and funded by
CDC/TEPHINET. The successful scholars have completed their projects as dissertation
work for their MAE-FETP course
g. Research papers of three scholars from III cohort scholar were accepted for presentation
for the EIS Night at Atlanta
h. Two scholars received CDC/TEPHINET small grant for their research proposal under
Micronutrient Malnutrition (MNM) Projects
i. The visiting WHO Team from Geneva and NTI Team from USA were highly apprecia
tive of the work carried out by FETP Scholars at NIE
j. CDC facilitated appointment of a Resident WHO Advisor, Dr. Yvan Hutin for FETP
at NIE
1.1.6. Annual Epidemiology week
Since 2002 NIE has been organising "Epidemiology Week" as a conscious effort to network
and develop partnerships with like-minded institutions. So far 3 such Epidemiology weeks viz.
30th Dec.2002 to 3rd Jan '03; 12th to 17th Oct. 2003 and 25th to 29th July 2005, had been
conducted.
The epidemiology week provided a common platform for interactions with the national and
international expert epidemiologists with the public health programme managers of central and
Field Epidemiology 3
NATIONAL INSTITUTE OF EPIDEMIOLOGY

state governments as well as international organizations. State level academic and research
institutions also gained good exposure on epidemiological aspects.
The epidemiology week was composed of,
(a) Meeting of public health training institutions in India
(b) Annual MAE-FETP scientific conference
(c) Meeting of ICMR Forum for epidemiology.
a. Meeting of public health training institutions in India
Main recommendations/outcomes were: (1) standardization of training programmes in the
field of epidemiology for public health in India and ensuring appropriate career opportunities
for field trained epidemiologists. (2) National institutes agreed to assume lead role in developing
training programmes for different cadres of public health professionals. (3) Strengthen public
health school initiatives in India and establish a commission for accreditation of public health
schools in the country and monitoring their academic initiatives (4) Networking of WHO
collaborating institutes for epidemiology training in India so as to build capacity and provide
technical support for rapid response teams under the Integrated Disease Surveillance Project
(IDSP)
b. Annual MAE-FETP scientific conference
The MAE-FETP scholars shared field experience and interacted with experts. The Scholars
received specific inputs on their presentations and field projects.
c. ICMR forum for epidemiology
ICMR forum for epidemiology serves as a formal network of epidemiologists and public health
specialists within ICMR. The forum provided an opportunity to develop functional networking of
ICMR institutions for closer relationship and facility sharing. During the forum, all ICMR
Institutes presented and discussed their epidemiological contributions. The meeting identified
resources available within ICMR to address basic methodological issues in epidemiology and
biostatistics.
Field Epidemiology 4
NATIONAL INSTITUTE OF EPIDEMIOLOGY

1.1.7. ICMR School of Public Health
ICMR, through NIE, has initiated training programme in field epidemiology relevant to public
health, leading to MAE. With this experience and the required expertise available, it is a logical
development for ICMR to create a School of Public Health and enter into the area of public health
training. This will be synergistic and symbiotic development, mutually beneficial to public health
and ICMR scientists. The proposal was discussed in-depth in the Scientific Advisory Committee
meeting and the core committees were formed for this purpose.
The goals of the proposed ICMR School of Public Health were derived as follows:
� Create professional and efficient public health trained manpower for different regions of
the country
� Link public health laboratories with public health institutes
� Develop effective network of public health institutes for rapid action and support surveil
lance programme, epidemic alerts and response
� Evaluate public health activities for continuing quality improvement
The Council will hold discussions with the stakeholders to decide on curriculum for various
courses, actual needs for different courses, time lines, university accreditation, quality assurance
mechanisms, funding needs and the sustainability components.
Field Epidemiology 5
NATIONAL INSTITUTE OF EPIDEMIOLOGY

1.2. Out-break investigations
During 2004-05, the institute was involved in investigations of post-tsunami measles outbreak in
Tamil Nadu , hepatitis E in Andhra Pradesh, measles and hepatitis E in Uttaranchal and acute
gastro-enteritis, measles, malaria and cholera in West Bengal:
1.2.1. Post-tsunami measles outbreak in Cuddalore district, Tamil Nadu
Background: On 26th December 2004, tsunami struck coast of Tamilnadu, India, affecting
several thousand people. Supplemental measles immunization was initiated in tsunami-affected
districts in Tamilnadu on 29th December targeting children aged six to sixty months. On 30th
December, a cluster of measles was reported in Cuddalore district of Tamilnadu that was affected
by tsunami. We investigated the outbreak to assess its magnitude and estimate vaccine efficacy.
We also studied measles virus genotype to understand source of virus.
Methods: We used WHO case definition to define a measles case. We received notification
of measles cases through stimulated passive surveillance system. We collected information
regarding date of onset, age, sex, vaccination status and residence. Blood samples were collected
from suspected cases of measles and examined for IgM antibodies. To estimate vaccine efficacy,
we conducted age and area matched case-control study in one of the blocks of Cuddalore district.
Results: We identified 101 measles cases meeting WHO case definition. Eight of 11 samples had
IgM antibodies against measles. Mean age of affected individuals was 5.1 years (range: 4 months
- 21 years). Cases were reported from tsunami-affected (n=71) and unaffected villages (n=30) in
the district. The attack rate was significantly lower in tsunami-affected areas. Ninety-five children
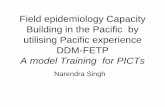
had no vaccination cards. Phylogenetic analysis revealed that the sequences of measles virus
belonged to genotype D8, (Diagram 1.) already in circulation in Tamil Nadu. The estimation of
vaccine efficacy was limited by the lack of information about the children immunization status.
Conclusions: Reported measles vaccine coverage in Tamilnadu is more than 95% since 1988.
Outbreak in area with high coverage with single dose indicated effectiveness of single dose
measles vaccination strategy was limited. Overall, few children had vaccination cards and hence
vaccine efficacy could not be estimated precisely. Information, education and communication
activities should emphasize importance of this document. Nearly 40% cases in this outbreak
were above five years. It will be beneficial to target supplemental immunization for older
children during such emergencies in future.
Field Epidemiology 6
NATIONAL INSTITUTE OF EPIDEMIOLOGY

Diagram 1.
Phylogenetic analysis of measles virus isolated during measles outbreak in Cuddalore
Field Epidemiology 7
NATIONAL INSTITUTE OF EPIDEMIOLOGY

1.2.2. Hepatitis E outbreak in Hyderabad, Andhra Pradesh
Background: Hepatitis E virus (HEV) is the leading cause of outbreak of acute jaundice in South
Asia. In the absence of guided prevention and control measures, these outbreaks may continue
until they die out spontaneously. An out break of jaundice occurred in the old city of Hyderabad,
Andhra Pradesh, India between March and August 2005. We investigated the outbreak to
identify the source of infection and facilitated control measures.
Methods: We defined a case of acute hepatitis as a resident of Hyderabad, suffering with jaun-
dice after 1st of March 2005 and serologically positive for anti IgM HEV. We identified cases
admitted for care at the Main fever hospital of the city. We calculated population-based incidences
and described the outbreak by time, place and person. We compared blocks where the attack rate
exceeded the median attack rate for a number of characteristics.
Results: A total of 1585 cases and 3 deaths were reported between 1st of March and 31st of
August2005 (Attack rate: 39 per 100,000, case fatality ratio: 0.2%). Among 565 serum samples
tested,446 (79%) were positive for IgM against HEV. The number of cases reported each
week reached 102 between 22nd and 29th of March and remained stable during April, May
and June, suggesting a persisting common source outbreak. The incidence was highest
among 20 to 44 years of age (53 per 100,000). The geographical distribution of cases was
highly heterogeneous and centered around open sewage drains that crossed the old city.
There was a trend for an increasing incidence of acute hepatitis in the block where the
pipelines of the water supply crossed the open sewage drains (Chi square for heterogeneity
of odds ratio: 1255.7, p value: 0.0). Blocks with water supply crossing the open sewage
drains accounted for 1210 of the 1585 cases reported (76%). Intermittent water supply in the
damaged, leaking pipelines and sucking sewage water into the water distribution system,
resulted in water contamination.
Outcome: This outbreak of hepatitis E was caused by water supplied in pipelines that crossed
open sewage drains. Direct collaboration between the health department and the water board dur-
ing this outbreak allowed using epidemiological data to direct the repairs in the water supply,
which ultimately controlled the outbreak in August 2005.
Field Epidemiology 8
NATIONAL INSTITUTE OF EPIDEMIOLOGY

Field Epidemiology 9
NATIONAL INSTITUTE OF EPIDEMIOLOGY

1.2.3. Acute gastro-enteritis outbreak at Malikpara village, Haora district,
West Bengal
Background: Riverine low lying areas of southern part of West Bengal, including Malikpara, are
prone to water logging and flood. These areas are hyper-endemic for acute gastro-enteritis (AGE).
Outbreaks are common. Poor agricultural labourers from backward community inhabit in con-
gested hutments of Malikpara (population: 229).They use one tube well for drinking water and
four ponds for other domestic purposes. A young woman had AGE on 12.09.2004 after taking
food from outside. A boy in her neighbourhood was affected on 19th and died on 20th. A feast
took place on 22nd and from 23rd to 28th 11 persons became ill. All total 11 patients were admit-
ted in hospital. All cases and the feast place were clustered around ponds.
Methods: Investigation was started from 29.09.2004. Outbreak and diagnosis were confirmed by
available records, interviews and sample testing. Definition of case was corroborated with WHO
definition.
Results: Vibrio cholerae non01 non0139 was found in pond water. Attack Rate was 4.8% and
Case Fatality Rate was7.8%. Incidence Rates were higher in females and in 15 - 45 years age
groups (both 54.54%). Relative Risk associated with pond water was (used by 17 houses): 4.63
(95% CI = 1.38 < 15.82, p = 0.0102).
Conclusion: Outbreak of cholera was clustered around ponds. This disease was transmitted
through contaminated pond water.
1.2.4. Measles outbreak in Hussendih village, Purulia district, West Bengal
Background: WHO estimates 30 million cases and one million deaths from measles annually.
Despite availability of safe and effective vaccine, failure to administer it to all infants is main
cause of measles outbreak. We investigated an outbreak of measles at Hussendih village, in the
neighbourhood of Majherpara village to estimate the magnitude, improve case management.
Methods: We conducted active case search using WHO case definition for measles. We
collected information on age, sex, residence, date of onset, symptoms, signs, vaccination
Field Epidemiology 10
NATIONAL INSTITUTE OF EPIDEMIOLOGY

status and outcome to analyze by time, place and person. We conducted a retrospective cohort
study among children between 7-120 months of age and calculated attack rates of measles by
vaccination status.
Results: Generation of cases occurred with peak around 3-4 March, one incubation period after a
religious festival. Case fatality ratio was 4%. Attack rate was 57% with highest among <9 months
children. Supplemental measles immunization was without vitamin A administration. In
Majherpara 43% were vaccinated. Vaccination coverage was below 80% since 1999 in the block.
Attack rates of measles among vaccinated and non-vaccinated children were 79% and 27%
respectively. Vaccine efficacy estimated was 64%.
Conclusion: The outbreak in a community, known for poor participation in measles immunization
activities. Routine immunization must be strengthened and awareness of vaccination must be
raised to prevent future outbreaks.
In addition to local ICMR labs, other district and state labs were utilised for the above outbreak
investigations
Field Epidemiology 11
NATIONAL INSTITUTE OF EPIDEMIOLOGY