1 Ecodevelopmental and Systemic Modeling and Implementing High Fidelity Interventions in Real World...
57
1 Ecodevelopmental and Systemic Modeling and Implementing High Fidelity Interventions in Real World Settings Guillermo Prado Guillermo Prado 1,2 1,2 , Hilda , Hilda Pantin Pantin 1 , Seth Scwartz , Seth Scwartz 1 , Jose , Jose Szapocznik Szapocznik 1 & Daniel J. Feaster & Daniel J. Feaster 1,2 1,2 1 1 Center for Family Studies, Center for Family Studies, University of Miami University of Miami 2 Stempel School of Public Stempel School of Public
-
Upload
emery-garrison -
Category
Documents
-
view
217 -
download
0
Transcript of 1 Ecodevelopmental and Systemic Modeling and Implementing High Fidelity Interventions in Real World...

1
Ecodevelopmental and Systemic Modeling and
Implementing High Fidelity Interventions in Real World
SettingsGuillermo PradoGuillermo Prado1,21,2, Hilda Pantin, Hilda Pantin11, ,
Seth ScwartzSeth Scwartz11, Jose Szapocznik, Jose Szapocznik11 & & Daniel J. Feaster Daniel J. Feaster 1,21,2
11 Center for Family Studies, Center for Family Studies,
University of MiamiUniversity of Miami22 Stempel School of Public Health, Stempel School of Public Health,
Florida International UniversityFlorida International University

2
The Ecodevelopmental Model and The Ecodevelopmental Model and Methodological QuestionsMethodological Questions

3
The Center for Family Studies is The Center for Family Studies is interested in the role of interested in the role of
ecodevelopmental context in the ecodevelopmental context in the prevention and treatment of prevention and treatment of
adolescent behavior problems, adolescent behavior problems, drug abuse, and HIV/AIDS.drug abuse, and HIV/AIDS.
4
Incorporates three primary, Incorporates three primary, integrated components: integrated components:
(a)(a) Social Ecological TheorySocial Ecological Theory
(b) Developmental Theory(b) Developmental Theory
(c) Emphasis on Social Interactions(c) Emphasis on Social Interactions
Ecodevelopmental Ecodevelopmental TheoryTheory

5
Highlights the Multiple Influences on Highlights the Multiple Influences on Adolescent Development, including:Adolescent Development, including:
(a)(a) MacrosystemsMacrosystems (e.g., cultural & societal (e.g., cultural & societal values)values)
(b) Exosystems(b) Exosystems (e.g., parents’ exosystemic (e.g., parents’ exosystemic stressors and social support for parents)stressors and social support for parents)
(c) Mesosystems(c) Mesosystems (e.g., parental monitoring (e.g., parental monitoring of peers and collaboration with youth’s of peers and collaboration with youth’s
school)school)
(d) Microsystems(d) Microsystems (e.g. family functioning)(e.g. family functioning)
Social Ecological Social Ecological TheoryTheory
Bronfenbrenner (1979, 1986)Bronfenbrenner (1979, 1986)

6
Emphasizes the changing nature of Emphasizes the changing nature of youth, contexts, & their youth, contexts, & their interdependenceinterdependence over time over time
e.g., family functioning is influenced not only by e.g., family functioning is influenced not only by parents’ current social support & work stress, but also parents’ current social support & work stress, but also by previous levels of social support & work stressby previous levels of social support & work stress
e.g., current family functioning in turn influences both e.g., current family functioning in turn influences both present and future levels of adolescent behavior present and future levels of adolescent behavior problemsproblems
Developmental Developmental ComponentComponent

7
Risk and protection are expressed in the Risk and protection are expressed in the patterns of direct transactions between patterns of direct transactions between individuals within and across the different individuals within and across the different contextual levels contextual levels
e.g., when parents engage in supportive interactions e.g., when parents engage in supportive interactions
with individuals outside the family, they are more with individuals outside the family, they are more likely to parent their children in supportive rather likely to parent their children in supportive rather than harsh ways.than harsh ways.
Social-Interactional Social-Interactional ComponentComponent

8
An Ecodevelopmental An Ecodevelopmental Perspective on Perspective on
PreventionPrevention

9
Context of Adolescent Behavior Context of Adolescent Behavior Problems, Drug Use, and Risky Sexual Problems, Drug Use, and Risky Sexual
BehaviorBehaviorSocial-Cultural ContextSocial-Cultural Context
Family MicrosystemFamily MicrosystemParent-adolescent communication about sex Positive ParentingParent-adolescent communication about sex Positive ParentingParent-Adolescent Communication Marital Conflict Parent-Adolescent Communication Marital Conflict Parental Involvement Family supportParental Involvement Family support
PeersPeersSubstance use w/ friendsSubstance use w/ friendsSexually active friendsSexually active friends
School School School BondingSchool BondingAcademic AchievementAcademic Achievement
Family-School Family-School RelationsRelations Parental involvement inParental involvement in schoolschool Monitoring homeworkMonitoring homework
Family-Peer RelationsFamily-Peer RelationsParental monitoring of peersParental monitoring of peersSupervision of situations ofSupervision of situations of sexual possibilitysexual possibility
Parental Resources/StressorsParental Resources/StressorsParents’ Social SupportParents’ Social SupportParents’ Work StressParents’ Work Stress
Cultural Cultural MismatchMismatch
ImmigrationImmigration PolicyPolicy PovertyPoverty
LanguageLanguageProblemsProblems

10
Ecodevelopmental Model of Problem Ecodevelopmental Model of Problem BehaviorsBehaviors
Family RelationsFamily RelationsParental-Adolescent Parental-Adolescent Communication about SexCommunication about Sex
Social Cognitive Mediators re. Sex
Social Cognitive Social Cognitive Mediators re.Drug UseMediators re.Drug Use
Early AdolescentEarly AdolescentSubstance UseSubstance Use
Early Adolescent Early Adolescent Sexual InitiationSexual Initiation
Parental Monitoring Parental Monitoring of Peersof Peers
Peer SexualPeer SexualBehaviorBehavior
Peer Substance Peer Substance UseUse
Early AdolescentEarly AdolescentProblem BehaviorsProblem Behaviors
AdolescentAdolescentAcculturationAcculturation
Social Support Social Support for Parentsfor Parents
Family Exosystemic Stressors
Parent Parent AcculturationAcculturation

11
Implications of Ecodevelopmental Theory for Methodological DevelopmentEcodevelopmental research involves Ecodevelopmental research involves
multiple levels of nestingmultiple levels of nesting Repeated Observations Repeated Observations Individuals Individuals
Families Families Ecosystemic levels across Ecosystemic levels across developmental stagesdevelopmental stages
Statistically, data are non-independent—Statistically, data are non-independent—Substantively people and their social Substantively people and their social contexts are interdependentcontexts are interdependent

12
Implications of Ecodevelopmental Theory for Methodological DevelopmentEcodevelopmental research involves Ecodevelopmental research involves
longitudinal processeslongitudinal processes Ecodevelopmental processes are Ecodevelopmental processes are
interrelated and influence each other interrelated and influence each other over over timetime
How do we model these interrelationships over How do we model these interrelationships over time?time?
Ecodevelopmental processes develop over Ecodevelopmental processes develop over time, and a snapshot of such a process time, and a snapshot of such a process (e.g., family functioning at baseline) is not (e.g., family functioning at baseline) is not accurateaccurate
How do we account for this in our model?How do we account for this in our model?

13
Implications of Ecodevelopmental Theory for Methodological DevelopmentEcodevelopmental research involves Ecodevelopmental research involves
influences from multiple systemsinfluences from multiple systems Ecodevelopmental models involve Ecodevelopmental models involve
two and three level interactionstwo and three level interactions How do we model these moderation How do we model these moderation
effects when the variables are observed?effects when the variables are observed? How do we model these moderation How do we model these moderation
effects when the variables are latent?effects when the variables are latent?

14
Multiple levels of nesting in effectiveness trials
Time is nested Time is nested within adolescents within adolescents
who are nested within families who are nested within families who are nested with therapistwho are nested with therapist who are nested both within treatment who are nested both within treatment
& site& site
Treatment crosses siteTreatment crosses site

15
Implementing a High Fidelity Implementing a High Fidelity Systemic Treatment in Drug Systemic Treatment in Drug Abuse Treatment CentersAbuse Treatment Centers

16
Plan of SectionPlan of Section
Clinical Trials Network (CTN)Clinical Trials Network (CTN) BSFTBSFT BSFT Design Issues—Level of BSFT Design Issues—Level of
ControlControl BSFT Experience in High BSFT Experience in High
Fidelity ImplementationFidelity Implementation

17
Clinical Trials NetworkClinical Trials Network NIDA funded network to test the effectiveness NIDA funded network to test the effectiveness
of efficacious treatments in real world settingsof efficacious treatments in real world settings As of 9/05:As of 9/05:
Nodes = 17Nodes = 17 States = 34+Puerto RicoStates = 34+Puerto Rico CTPs = 152CTPs = 152 Protocols = 27 (11 closed to enrollment, 5 in Protocols = 27 (11 closed to enrollment, 5 in
development)development) Currently 88 CTPs involved in 11 open studiesCurrently 88 CTPs involved in 11 open studies
Mission: To implement science-based Mission: To implement science-based efficacious treatments in community settings efficacious treatments in community settings AND to show that these implementations are AND to show that these implementations are an improvement over current practicean improvement over current practice

18
Brief Strategic Family Brief Strategic Family Therapy—BSFT, CTN0014Therapy—BSFT, CTN0014 Brief Strategic Family Therapy is a Brief Strategic Family Therapy is a
systemic, process-focused family therapysystemic, process-focused family therapy 4 months with weekly sessions4 months with weekly sessions Up to 8 booster sessions over 8 monthsUp to 8 booster sessions over 8 months Focus on changing repetitive (maladaptive) Focus on changing repetitive (maladaptive)
interactions within the familyinteractions within the family Note that the focus is on underlying processes, not Note that the focus is on underlying processes, not
crisescrises May use a crisis as a content focus, but therapy May use a crisis as a content focus, but therapy
addresses underlying “everyday” processesaddresses underlying “everyday” processes
BSFT has been the focus of over 30 years BSFT has been the focus of over 30 years of research at the Center for Family Studiesof research at the Center for Family Studies

19
BSFT-Therapy BSFT-Therapy ComponentsComponentsThree major techniquesThree major techniques
Joining (Engaging Participants into Joining (Engaging Participants into Treatment)Treatment)
• Balanced across all family membersBalanced across all family members• Must join with most powerfulMust join with most powerful
Diagnosis (Family Relationships and Roles)Diagnosis (Family Relationships and Roles) Restructuring (Implementing the Restructuring (Implementing the
Treatment Plan)Treatment Plan)• Work in Present—EnactmentsWork in Present—Enactments• ReframingReframing• Shifting boundariesShifting boundaries

20
BSFT CTN0014BSFT CTN0014
8 Sites8 Sites 60 participants per site on average60 participants per site on average 480 adolescent participants480 adolescent participants Drug Use assessed monthly for 12 Drug Use assessed monthly for 12
monthsmonths Full assessments at Baseline, 4 months, Full assessments at Baseline, 4 months,
8 months and 12 months8 months and 12 months Delinquent Behaviors, Conduct Problems, Delinquent Behaviors, Conduct Problems,
Sexual risk behaviors, Adolescent Pro-social Sexual risk behaviors, Adolescent Pro-social Activities, & Family FunctioningActivities, & Family Functioning

21
BSFT—RandomizationBSFT—Randomization
Participants will be randomized to Participants will be randomized to BSFT or the clinic’s standard BSFT or the clinic’s standard outpatient treatmentoutpatient treatment
Note, randomization is at the Note, randomization is at the individual level, not at the clinic individual level, not at the clinic levellevel

22
Design Considerations for Design Considerations for Effectiveness TrialsEffectiveness Trials Level of ControlLevel of Control
Homogeneity of Study Population Homogeneity of Study Population (Szapocznik)(Szapocznik)
Standardization & Monitoring of Standardization & Monitoring of Treatment (Szapocznik)Treatment (Szapocznik)
Standardization & Monitoring of Control (Feaster)Standardization & Monitoring of Control (Feaster)
Handling of Site Variance (Feaster)Handling of Site Variance (Feaster) Efficacy study—Fixed EffectEfficacy study—Fixed Effect Effectiveness—Random EffectEffectiveness—Random Effect

23
BSFT: BSFT: Heterogeneous Treatment Heterogeneous Treatment PopulationPopulation
Inclusion Criteria:Inclusion Criteria: 12-17 years of age12-17 years of age Any illicit drug use in last 30 days Any illicit drug use in last 30 days Lives or is expected to with “family”Lives or is expected to with “family” Reside in the same geographic area as CTPReside in the same geographic area as CTP Signed consent & assentSigned consent & assent
Exclusion Criteria:Exclusion Criteria: Not living with family (halfway house, institution, Not living with family (halfway house, institution,
etc.)etc.) Suicidal or homicidal risk must be stabilized, firstSuicidal or homicidal risk must be stabilized, first Current or pending severe Current or pending severe criminalcriminal charges if likely charges if likely
to lead to incarcerationto lead to incarceration If already receiving drug treatment servicesIf already receiving drug treatment services

24
Choice for BSFT:Choice for BSFT:Full Control of Full Control of Experimental ConditionExperimental Condition
Extensive Training and SupervisionExtensive Training and Supervision 5 months of training5 months of training Weekly supervisionWeekly supervision
Training and Supervision are Training and Supervision are considered integral to the BSFT considered integral to the BSFT modelmodel
25
Multiple Levels of Clinical Supervision & Adherence Monitoring Clinical SupervisionClinical Supervision Weekly conference calls with Weekly conference calls with
a BSFT supervisor. Supervision includes:a BSFT supervisor. Supervision includes: videotape reviewvideotape review case discussion and planning.case discussion and planning.
National Clinical SupervisorNational Clinical Supervisor weekly face-to-face sessions with each clinical weekly face-to-face sessions with each clinical
supervisorsupervisor Regularly sits in on selected supervision calls with sitesRegularly sits in on selected supervision calls with sites
Adherence Ratings of VideotapesAdherence Ratings of Videotapes Randomly selected sessionsRandomly selected sessions trained independent raters in Miami trained independent raters in Miami
Failure to adhere to the BSFT modelFailure to adhere to the BSFT model DefinitionDefinition-<70% adherence for 3 consecutive sessions-<70% adherence for 3 consecutive sessions Consequences & Corrective ActionConsequences & Corrective Action
no new cases until no new cases until 80% in two consecutive sessions80% in two consecutive sessions Increased supervision & retraining until meets criteria Increased supervision & retraining until meets criteria If criteria not met before conclusion of current cases If criteria not met before conclusion of current cases
withdrawn from study (at discretion of clinical supervisor)withdrawn from study (at discretion of clinical supervisor)

26
Therapist Consent and Selection Process Identification of volunteersIdentification of volunteers
ConsentConsent DemographicsDemographics Views of Adolescent Drug Abuse – Q-sortViews of Adolescent Drug Abuse – Q-sort
SelectionSelection Interviews (Site PI, National Study Interviews (Site PI, National Study
Director/ Coordinator, and BSFT Head Director/ Coordinator, and BSFT Head Training Supervisor)Training Supervisor)
Family SessionFamily Session RandomizationRandomization
Academic trainingAcademic training Years of clinical experienceYears of clinical experience

27
Training Phase for BSFT Therapists Five-month clinical training programFive-month clinical training program WorkshopsWorkshops
Four 3-day workshopsFour 3-day workshops Week 1 (Workshop 1) *MiamiWeek 1 (Workshop 1) *Miami Week 3 (Workshop 2)Week 3 (Workshop 2) Week 5 or 6 (Workshop 3)Week 5 or 6 (Workshop 3) Week 13 (Workshop 4)Week 13 (Workshop 4)
SupervisionSupervision Weekly group supervisionWeekly group supervision
Each therapist will have ½ hour for videotape Each therapist will have ½ hour for videotape review and ½ for case discussionreview and ½ for case discussion
Pilot Cases: 2-4 cases for each Pilot Cases: 2-4 cases for each therapisttherapist
CertificationCertification

28
Implementation Phase
Active Cases Active Cases Caseload builds over timeCaseload builds over time Study caseload will range from 2-8 cases Study caseload will range from 2-8 cases
(minimum = 0; maximum = 10)(minimum = 0; maximum = 10) SupervisionSupervision
Weekly group supervisionWeekly group supervision Review of videotapesReview of videotapes Review of clinical formsReview of clinical forms Treatment planningTreatment planning Each therapist (2 active) will have 30-45 Each therapist (2 active) will have 30-45
minutes for videotape review and 30-45 minutes for videotape review and 30-45 minutes for case discussion minutes for case discussion

29
Adherence Ratings By Site
Node/Site All Sites 15/301 7/802 7/302 7/604 13/701 9/200
Domain Average for Blind Ratings
Median (25th, 75th) 3.5 (3.2, 3.9) 3.5 (3.2, 3.7) - 3.4 (3.0, 3.7) 3.5 (3.3, 4.1) 3.8 (3.7, 4.0) 3.6 (3.1, 4.0)
% Good Adherence2 108/130 (83.1%) 38/46 (82.6%) - 21/26 (80.8%) 30/34 (88.2%) 4/4 (100.0%) 15/20 (75.0%)
Domain Average for Clinical Ratings
Median (25th, 75th) 3.9 (3.6, 4.0) 3.8 (3.5, 4.0) 4.1 (4.0, 4.2) 4.0 (3.8, 4.0) 4.0 (3.5, 4.3) 3.8 (3.8, 3.8) 3.7 (3.6, 4.0) % Good Adherence 102/112 (91.1%) 41/46 (89.1) 6/6 (100.0%) 16/16 (100.%) 28/31 (90.3%) 1/1 (100.0%) 10/12 (83.3%)
Overall Supervisor’s Ratings
Median (25th, 75th) 4.0 (3.0, 4.0) 4.0 (3.0, 4.0) 4.0 (4.0, 4.0) 4.0 (4.0, 4.0) 4.0 (3.0, 4.0) 4.0 (4.0, 4.0) 4.0 (3.5, 4.0)
% Good Adherence 108/112 (96.4%) 44/46 (95.7%) 6/6 (100.0%) 16/16 (100.0%) 29/31 (93.6%) 1/1 (100.0%) 12/12 (100.0%)
Good Adherence is 3

30
Adherence Ratings
Show adequate adherenceShow adequate adherence
Some variability across sitesSome variability across sites
Supervisors’ ratings uniformly Supervisors’ ratings uniformly higher than than independent higher than than independent raters’raters’

31
32
Some Statistical Approaches and
Areas for Further Research in Systemic Modeling
and Design of Effectiveness Trials

33
Plan of Section:
Specification of Site Effects & Specification of Site Effects & Bounds of InferenceBounds of Inference
Power analysis and Trial PlanningPower analysis and Trial Planning Time Structure of Models & Time Structure of Models &
Reciprocal EffectsReciprocal Effects Need for Simulation ResearchNeed for Simulation Research Questions about Mplus & SimulationQuestions about Mplus & Simulation

34
Design Considerations for Design Considerations for Effectiveness TrialsEffectiveness Trials Level of ControlLevel of Control
Homogeneity of Study Population (Szapocznik)Homogeneity of Study Population (Szapocznik) Standardization & Monitoring of Treatment (Szapocznik)Standardization & Monitoring of Treatment (Szapocznik)
Standardization & Monitoring of Control Standardization & Monitoring of Control (Feaster)(Feaster)
Handling of Site Variance (Feaster)Handling of Site Variance (Feaster) Efficacy study—Fixed EffectEfficacy study—Fixed Effect Effectiveness—Random EffectEffectiveness—Random Effect

35
Considerations for Choice Considerations for Choice of Comparison Conditionof Comparison Condition Standardized Control GroupStandardized Control Group
Smaller sample size (sites & participants)Smaller sample size (sites & participants) High internal validity High internal validity Lacks ecological validity for CTPsLacks ecological validity for CTPs
Treatment As UsualTreatment As Usual Larger sample size (sites & participants)Larger sample size (sites & participants) High external validityHigh external validity Highly variable across sitesHighly variable across sites Minimum site size— within site comparisonsMinimum site size— within site comparisons

36
Choice for BSFT:Choice for BSFT:Treatment As UsualTreatment As Usual
Compare BSFT to the population of Compare BSFT to the population of treatments in the communitytreatments in the community
Currently drug abuse treatment has Currently drug abuse treatment has considerable variability in considerable variability in treatment approach and treatment approach and implementationimplementation
37
Handling of Site Handling of Site VarianceVariance Fixed Effect (control for site & Fixed Effect (control for site &
remove variance from error): remove variance from error): Cannot generalize statisticallyCannot generalize statistically
Random Effect: Can generalize Random Effect: Can generalize effect beyond the clinics included effect beyond the clinics included Both site & site X treatment are Both site & site X treatment are
randomrandom Implications on power of studyImplications on power of study

38
Choice for BSFT: TAUChoice for BSFT: TAU
Differences in TAU at each site Differences in TAU at each site implies larger variance of the implies larger variance of the random Site X Treatment effectrandom Site X Treatment effect
Sites need not be randomly Sites need not be randomly assigned, but need to describe the assigned, but need to describe the generality of clinics (if not generality of clinics (if not randomly selected)randomly selected)
39
Fidelity of Implementation
Variability in fidelity across sites will Variability in fidelity across sites will increase the site and site by increase the site and site by treatment effectstreatment effects

40
Specifics of BSFT Specifics of BSFT Statistical PlanStatistical Plan
Hypothesis 1: BSFT will be Hypothesis 1: BSFT will be significantly more effective than significantly more effective than TAU in reducing adolescent drug TAU in reducing adolescent drug abuse, abuse, defined as the percentage defined as the percentage of days with positive drugs useof days with positive drugs use..

41
Example of Expected Example of Expected TrajectoriesTrajectories
Drug Use Over Follow-up
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
T4 T8 T12
BSFT-Outpatient
TAU-Outpatient

42
Secondary HypothesesSecondary HypothesesBSFT will be significantly more BSFT will be significantly more
effective than TAU in :effective than TAU in :– Reducing:Reducing:
Delinquent behaviors & conduct Delinquent behaviors & conduct problemsproblems
Sexually risky behaviorsSexually risky behaviors
– Increasing:Increasing: Prosocial activities (school, Prosocial activities (school,
employment)employment) Family functioning (parenting, Family functioning (parenting,
parent-adolescentparent-adolescent communication) communication)
43
Analysis StrategyAnalysis Strategy Randomization at the Individual Client Randomization at the Individual Client
LevelLevel Multi-level Growth Curve with 3 levelsMulti-level Growth Curve with 3 levels
Level 1 is within person—TimeLevel 1 is within person—Time Level 2 is between persons (and incorporates Level 2 is between persons (and incorporates
treatment assignment)treatment assignment) Level 3 is between site Level 3 is between site
Controlling for baseline drug use (ANCOVA-Controlling for baseline drug use (ANCOVA-type specification)type specification)
Note: not accounting for all levels of Note: not accounting for all levels of nesting in primary hypotheses (therapist nesting in primary hypotheses (therapist effects examined in post-hoc analyses)effects examined in post-hoc analyses)

44
Proposed Model
0 1ijt ij ij ijt ijty a
0 0 0 1 0 0ij j j ijBSFT r
1 0 1 1 1 1ij j j ijBSFT r
0 0 000 0 0j ju
1 0 100 1 0j ju
0 1 001 0 1j ju
1 1 101 1 1j ju
Level 1—Time:
Level 2—Between Adolescents:
Level 3—Between Sites:
Time, a, is centered at Month 4
000
100
001
101
Grand Mean Month 4 Drug Use in TAU
Increment to Month 4 Drug Use for BSFT
Grand Mean Slope in Drug Use in TAU
Increment to Slope in Drug Use for BSFT

45
Multisite Power AnalysesMultisite Power Analyses (Raudenbush & Liu,
2001)
Effect Size
Power
0.20 0.40 0.60 0.80 1.00
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0 = 0.050
J= 8,n= 56,2= 0.05
J= 8,n= 56,2= 0.10
J= 8,n= 56,2= 0.15
Procedure assumes single post test (not growth curve)We have 12 monthly drug use assessmentsHowever, drug use is not normally distributed
46
Methodological Issues
Most research on design implications Most research on design implications of site effects has been done by of site effects has been done by statisticians with drug trial experiencestatisticians with drug trial experience
Aim is to prevent site effects or Aim is to prevent site effects or justifying ignoring them if they existjustifying ignoring them if they exist
Therefore, little prior evidence Therefore, little prior evidence published on site variability & published on site variability & particularly on the site by treatment particularly on the site by treatment interaction interaction

47
Methodological Issues Power AnalysisPower Analysis
Lack of prior info makes difficultLack of prior info makes difficult Lack of software (Raudenbush & Liu, 2001)Lack of software (Raudenbush & Liu, 2001) Simulation in M-PlusSimulation in M-Plus
Have been doing simulationsHave been doing simulations In SAS, have difficulty with 8 sites identifying In SAS, have difficulty with 8 sites identifying
the site & site X treatment variance in growth the site & site X treatment variance in growth curve frameworkcurve framework
Specifically, it may not be possible to identify Specifically, it may not be possible to identify the covariance between the site and site X the covariance between the site and site X treatment random componentstreatment random components
Simulations do not exactly match Raudenbush Simulations do not exactly match Raudenbush & Liu& Liu

48
Resource Allocation Resource Allocation IssueIssue Random site X treatment effect Random site X treatment effect
with variability in Treatment as with variability in Treatment as Usual requires a large sampleUsual requires a large sample
Necessity of effectiveness Necessity of effectiveness research if to generalize to new research if to generalize to new clinicsclinics
Some disagree Some disagree (due in part to costs)(due in part to costs) Simulation to show Type 1 errorSimulation to show Type 1 error Look at potential mistakes of policy based Look at potential mistakes of policy based
on inappropriate overly precise estimateson inappropriate overly precise estimates
49
Reciprocal Effects
Person-specific cross-lagged panel Person-specific cross-lagged panel modelmodel
Could be formulated in a latent Could be formulated in a latent difference score frameworkdifference score framework
Model is important for systemic Model is important for systemic phenomenon like family interactionsphenomenon like family interactions
Illustrated within a person using Illustrated within a person using coping and distress datacoping and distress data
50
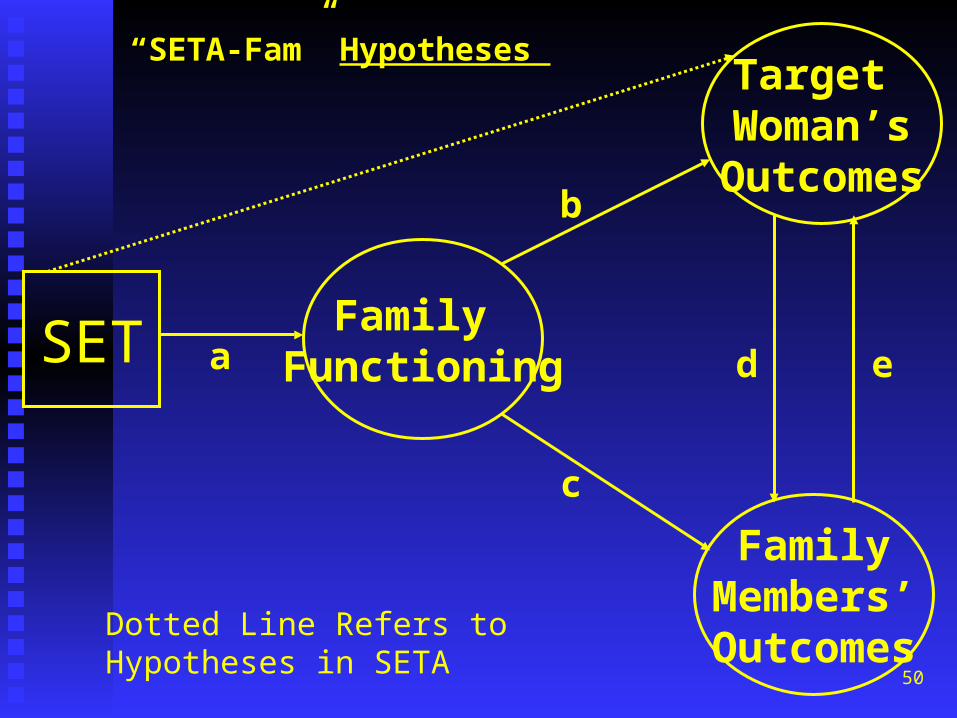
SET Family Functioning
Target Woman’sOutcomes
FamilyMembers’Outcomes
a
b
c
d e
““SETA-Fam” SETA-Fam” Hypotheses Hypotheses
Dotted Line Refers to Hypotheses in SETA

51
Within A Person
Distress 1 Distress 2 Distress 3 Distress 4a a a
Coping 1 Coping 2 Coping 3 Coping 4b b b
Test a through d as random effects
c c c
d d d
z e e ef f f

52
Within a Family
Distressj 1 Distressj 2 Distressj 3 Distressj 4a a a
Distressk1 Distressk 2 Distressk 3 Distressk 4b b b
Test a through d as random effects
c c c
d d d
z e e ef f f

53
Cross Lagged w/AR Random
DistressT1
CopingT1
DistressT2
DistressT3
DistressT4
CopingT2
CopingT3
CopingT4
CopingAR
DistressAR
Adj. BIC=2206.9
.03
.19*
.19*
.19*
.03 .03
M=.61*
V=.02*
M=.55*
V=.03

54
How does Model Fit Compare to Growth Curve Specification?
DistressBaseline
DistressLinear
DistressQuadratic
CopingQuadratic
CopingLinear
CopingBaseline
V=0
V=0
-.46*
.9999*
.77*
Adj. BIC=2219.5, *Difficulty with Psi

55
Selected Issues to Address Questions to be addressed:Questions to be addressed:
Parameter interpretationParameter interpretation Comparative Model Fit/DiscriminationComparative Model Fit/Discrimination Initial ConditionsInitial Conditions Different time frames both within and between Different time frames both within and between
individuals (data is collected on only one time individuals (data is collected on only one time frame, though with variability in exact times of frame, though with variability in exact times of collection)collection)
SimulationsSimulations Question, is it possible to vary parameters in a Question, is it possible to vary parameters in a
simulation within Mplus and save the parameter simulation within Mplus and save the parameter settings to the generated data file?settings to the generated data file?
[[email protected] to .8 by .1].[[email protected] to .8 by .1]. AR @ 0 to 5 by .5.AR @ 0 to 5 by .5.

56

57