1 DISEASES of the LIVER, GALLBLADDER AND PANCREAS V.Voloshyn (Frank Netter’s illustrations)
50
1 DISEASES of the LIVER, GALLBLADDER AND PANCREAS V.Voloshyn (Frank Netter’s illustrations)
-
Upload
alaina-wells -
Category
Documents
-
view
225 -
download
2
Transcript of 1 DISEASES of the LIVER, GALLBLADDER AND PANCREAS V.Voloshyn (Frank Netter’s illustrations)
1
DISEASES of the LIVER, GALLBLADDER AND
PANCREAS
V.Voloshyn
(Frank Netter’s illustrations)

2
Pankreatitis
Clinical motion of Pankreatitis can be acute (sharp) and chronic.
However necessary it is to know that patients with chronic one can have acute condition.
3
Acute Pancreatitis
Etiology.
Acute Pancreatitis can develop at: obstructions of pancreas duct; reflux of bile; alcoholism; violation of blood circulation (for example, at
shock); defeat by parotitis virus; hyperparathyroidism; hypothermia; trauma.
4
In many cases Pancreatitis is poorly expressed, but is a heavy disease which is characterized by high lethality. Pancreatitis of adults is observed more frequent than children’s one. A defeat develops difficultly & characterized by massive activation of pancreatic enzymes, which, in acute cases, may cause life-threatening autodigestion and shock.
In addition, these enzymes damage surrounding tissues & finishes by their dissolution.
5
Clinical displays :
Patients have sharp sudden painsharp sudden pain in an epigastria area, which is accompanied nausea and vomitnausea and vomit.
ShockShock can very quickly develop.A diagnosis is confirmed the increase increase
of amylaseof amylase levellevel in blood.
6
Pathogeny:
the initial stage depends on reasons: at the obstruction of pancreas channel
by a stone or at bile reflux there is a damage of epithelium pancreatic duct canaliculuses, especially if a bile is infected or contains activated.
A damage spreads after it on glands, that results in liberation and activating of proteolytic and other enzymes.
7
At a violation of blood circulation peripheries pancreas acinuses suffer primary (they are disconnected from blood supplying first).
After it rapid and widespread destruction of gland develops by proteolytic enzymes.
Pathogeny 2:
8
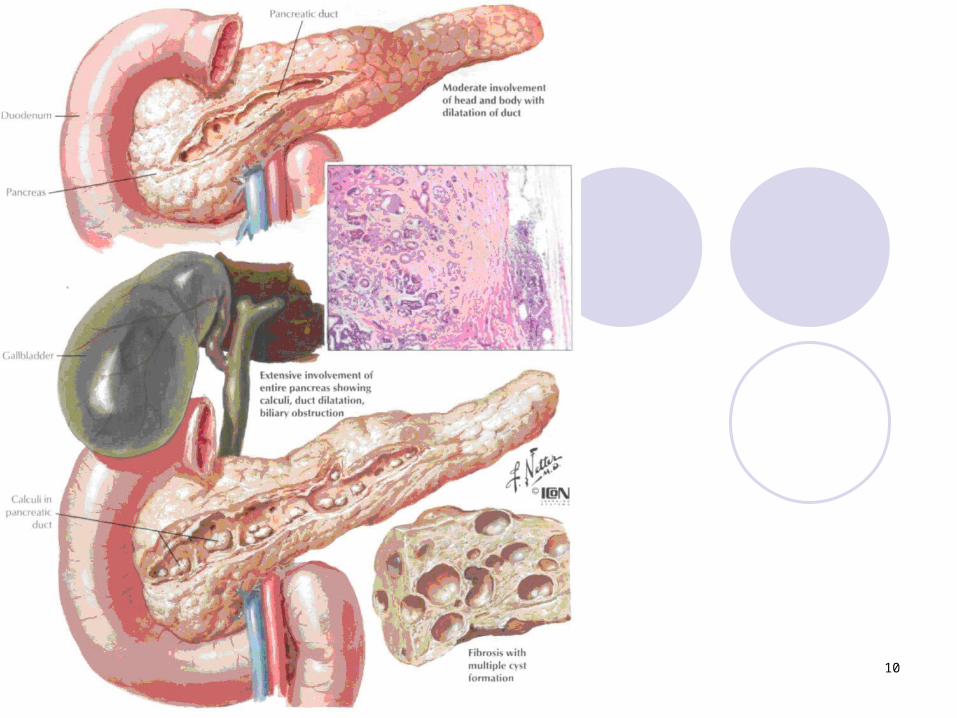
Morphology:
a gland swelling seat of hemorrhages as a result of destruction of
blood vessels fatty necrosis in grate omentum and hypodermic
cellulose (very often with skin colour change in epigastrium area (Grey-Terner's symptom)
fat acids link the ions of calcium→ calcium concentration decreas→ tetanus
insular apparatus destruct→hyperglycemia abscesses and cysts in pancreas & neighbors
tissues
9
10
11
PANCREATITIS KINDS
At hemorrhage prevailing they call – hemorrhage pancreatitis;
festering inflammation – acute festering pancreatitis;
necrotic changes – pancreonecrosis.
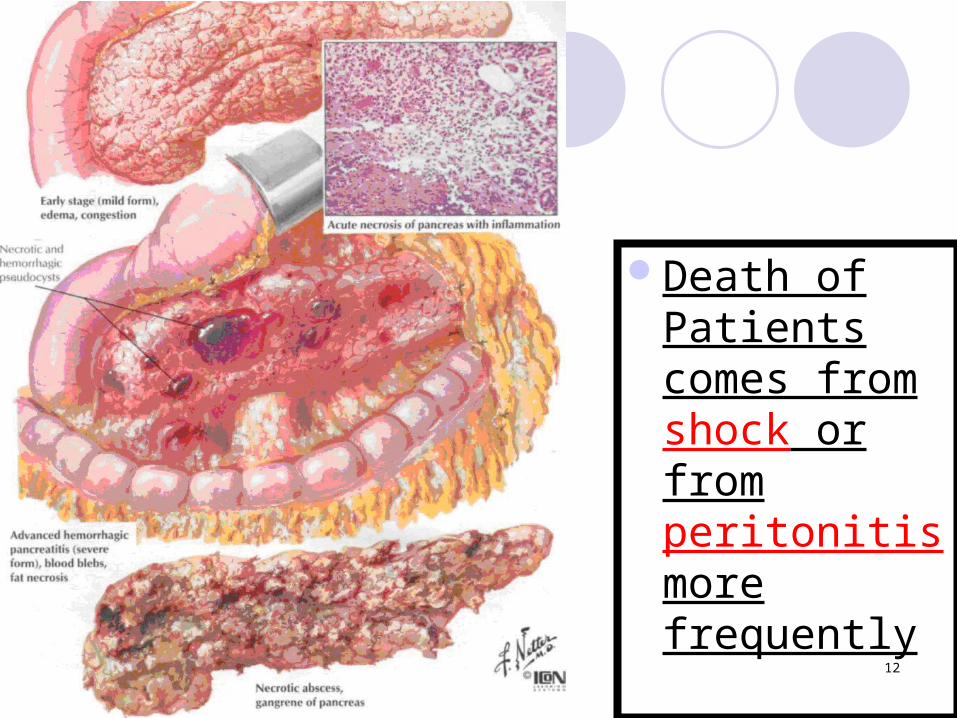
12
Death of Patients comes from shock or from peritonitis more frequently
13
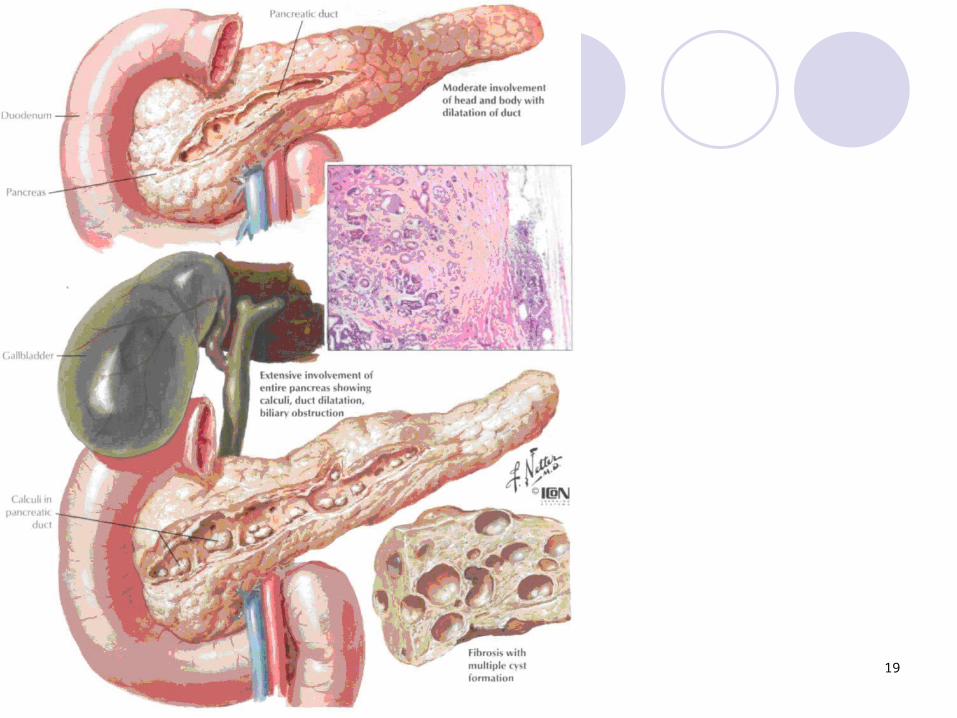
Chronic pancreatitis
cause extensive destruction of pancreatic parenchyma with fibrosis and loss of enzymatic activities
which can develop after the clinical acute one and independently without any displays
14
Etiology:
chronic P. can develop after the clinical acute one and independently without any displays which are preceded.
alcoholism is the most frequent reasonchronic P. is the display of
mucoviscidosis also.rarely there is inherited chronic P.
15
16
17
18
Pathoanatomical description.
Chronic P. is more frequent observed for adults, than for children
At X-ray examination – calcification areas as a result of preceding fatty necrosis.
Exocrine parts of gland transformed in to fibrosis tissue
Endocrine part mainly is not damaged.
19
20
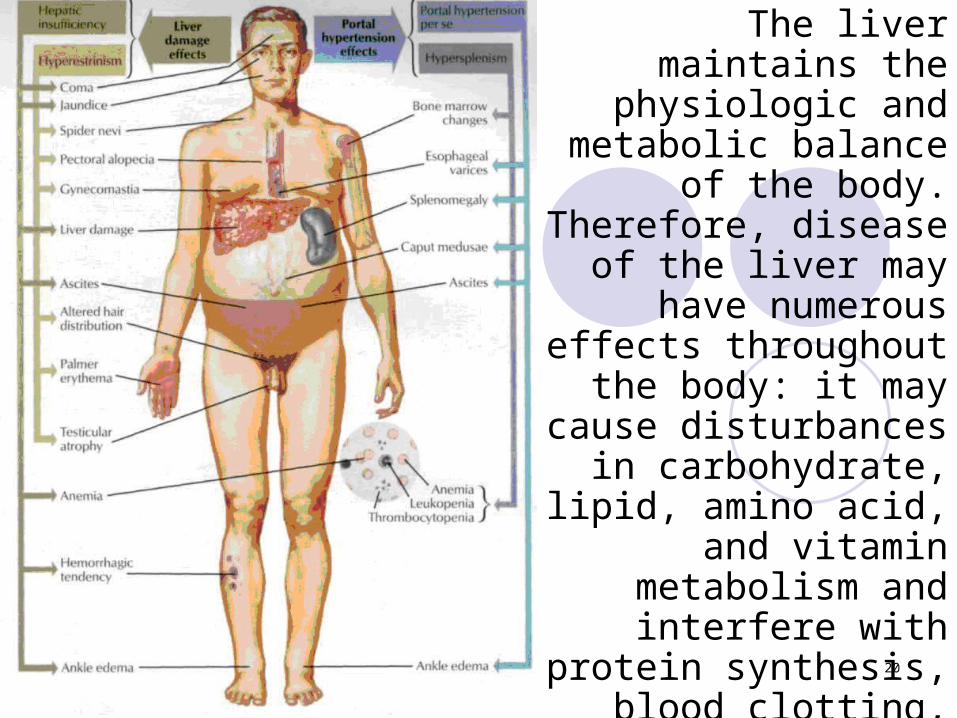
The liver maintains the physiologic and
metabolic balance of the body. Therefore, disease
of the liver may have numerous effects
throughout the body: it may cause disturbances
in carbohydrate, lipid, amino acid, and vitamin
metabolism and interfere with protein synthesis,
blood clotting, and detoxification of
endogenous and exogenous substances
21
LIVER ILLNESSES
Illnesses of liver are various and can be primary and secondary (at other diseases).
Chronic hepatitis is an inflammatory disease of liver, which lasts more than 6 months without the signs of recovery.
22
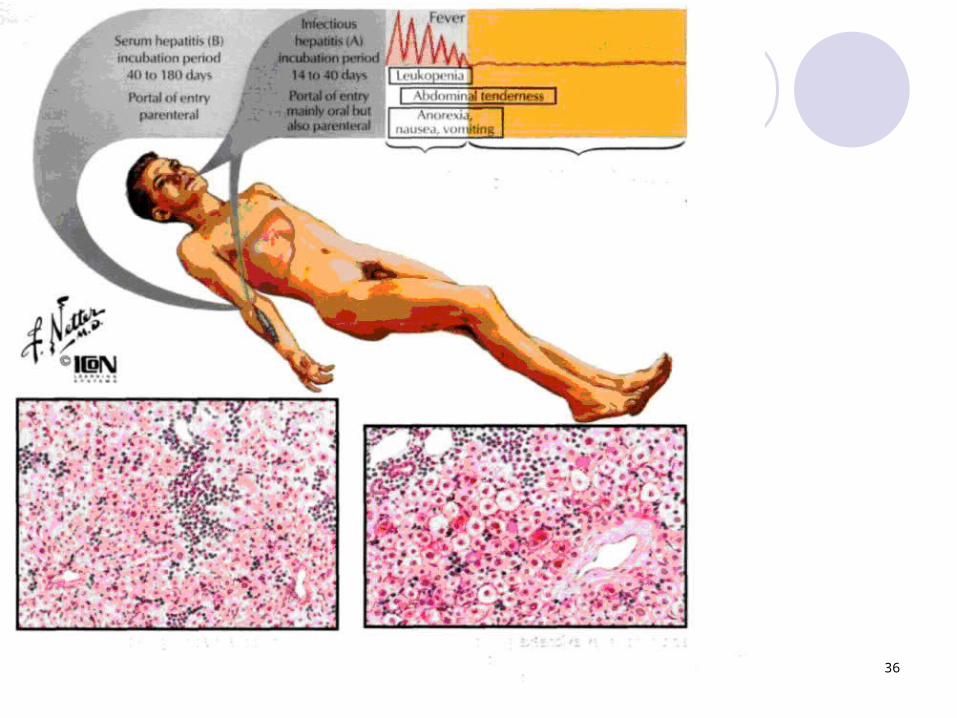
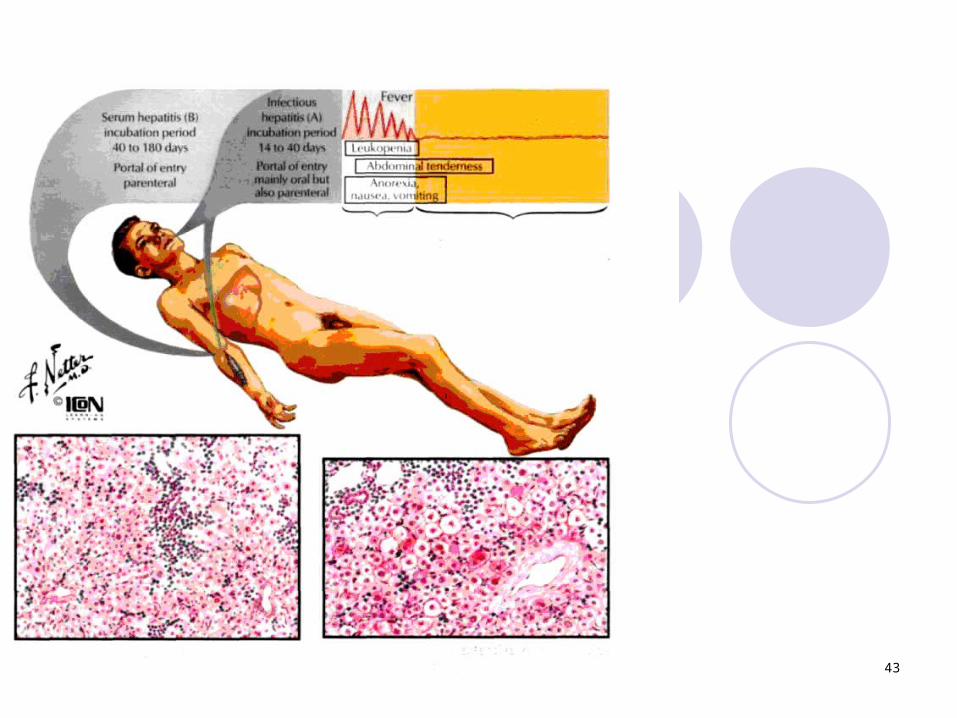
Acute Viral Hepatitis
an inflammatory disease of the hepatic parenchyma, is caused most frequently by the hepatitis viruses (HVs) and less frequently by other viruses. In the Western world, HBV and HBC are most prevalent.
23
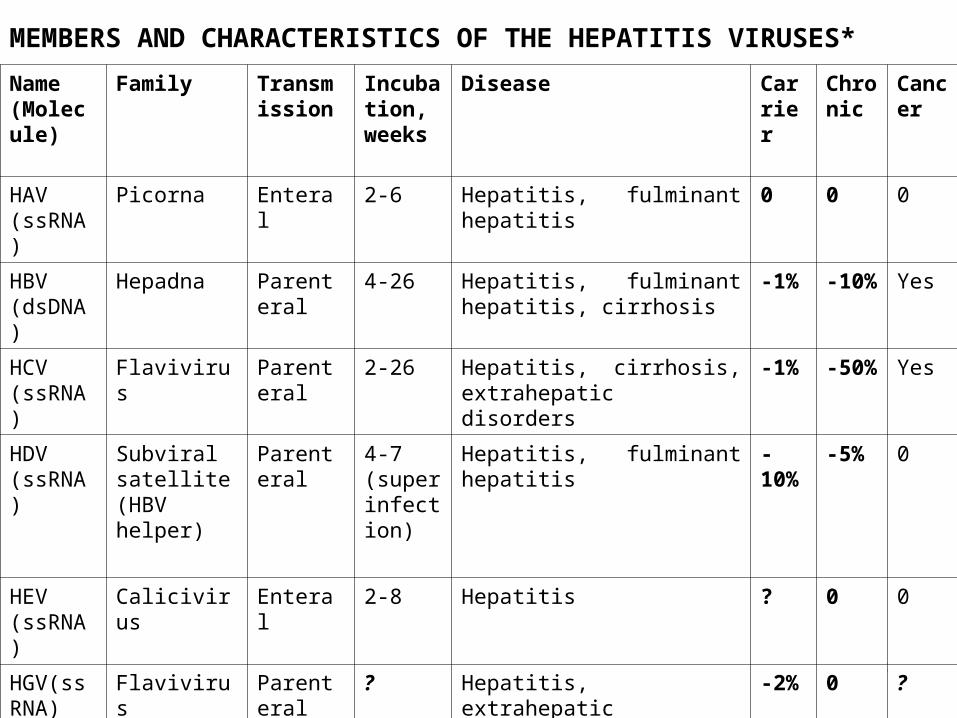
MEMBERS AND CHARACTERISTICS OF THE HEPATITIS VIRUSES*
Name (Molecule)
Family Transmission
Incubation, weeks
Disease Carrier
Chronic
Cancer
HAV (ssRNA)
Picorna Enteral 2-6 Hepatitis, fulminant hepatitis 0 0 0
HBV (dsDNA)
Hepadna Parenteral 4-26 Hepatitis, fulminant hepatitis, cirrhosis
-1% -10% Yes
HCV (ssRNA)
Flavivirus Parenteral 2-26 Hepatitis, cirrhosis, extrahepatic disorders
-1% -50% Yes
HDV (ssRNA)
Subviral satellite (HBV helper)
Parenteral 4-7 (superinfection)
Hepatitis, fulminant hepatitis -10%
-5% 0
HEV (ssRNA)
Calicivirus Enteral 2-8 Hepatitis ? 0 0
HGV(ssRNA)
Flavivirus Parenteral ? Hepatitis, extrahepatic disorders in drug addicts
-2% 0 ?
24
25
26
27
28
29
30

31
32
33
34
35
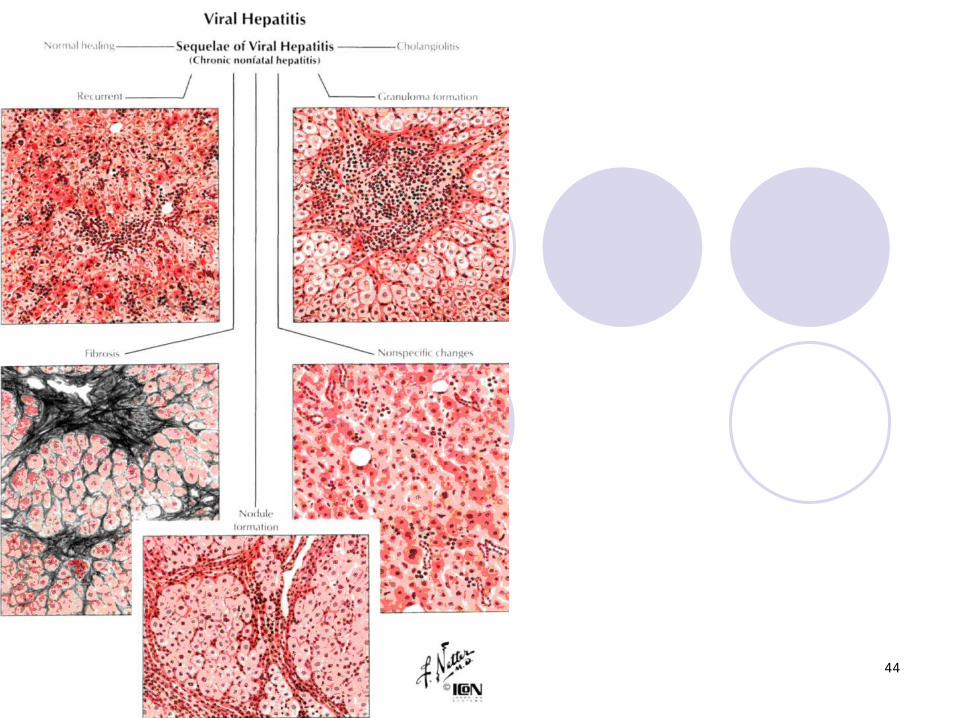
Disease symptoms develop between 2 and 26 weeks after the onset of immune reactions against virus/virus-infected cells. The pathogenesis of liver injury in viral hepatitis is not completely clear, although a cytotoxic T-lymphocyte reaction against hepatocytes presenting viral antigens seems to be the key reaction. Histology shows many lymphocytes invading the liver parenchyma from portal triads, which causes adjacent hepatocellular necroses (piecemeal necroses). Infected hepatocytes change to a ground-glass appearance. In more severe disease, infected hepatocytes show ballooning degeneration. In addition, there are single or multiple hepatocellular coagulation necroses of virus-infected hepatocytes (Councilman bodies) or lytic necroses (dropout necroses).
36
37
Etiology.Reason of chronic hepatitis can be different factors. Most frequent is:
• viruses of hepatitis, especially B and C;• alcohol;• medicinal preparations;• autoimmune processes;• illness of Vil'sona;• α1-antytrepsin insufficiency.
38
Classification.
On histological principle chronic hepatitis is divided on:
• chronic recurrent hepatitis (CHRG);• chronic active hepatitis (CHAG).
39
Chronic hepatitis is the unspecific display of many chronic diseases of liver
40
Chronic recurrent hepatitis
Chronic recurrent hepatitis is characterized:by limphocells infiltration only of portal tracts;saving of normal architectonics of liver;by absence or rare necrosis of liver cells;by a favourable prognosis.
Mostly at chronic recurrent hepatitis there is convalescence even without specific treatment.
41
Chronic active hepatitis
by boundary (for peripheries of particle on a border with portal highways) (necrosis of two particles is with involvement of portal highway which lies between them) necrosises;
by infiltration of portal highways and parenchyma of liver;
by the high risk of development of liver cirrhosis
is characterized:
42
Histologically
boundary necrosisesdecrease of hepatocells quantityviolation of normal architectonicssometimes specific signs which specify
on reason of hepatitis:(for example: Mellori's gialin at alcoholism)
43
44
45
Alcoholic hepatitis
An alcohol (ethyl spirit) is the most frequent reason of acute and chronic damage of liver.
46
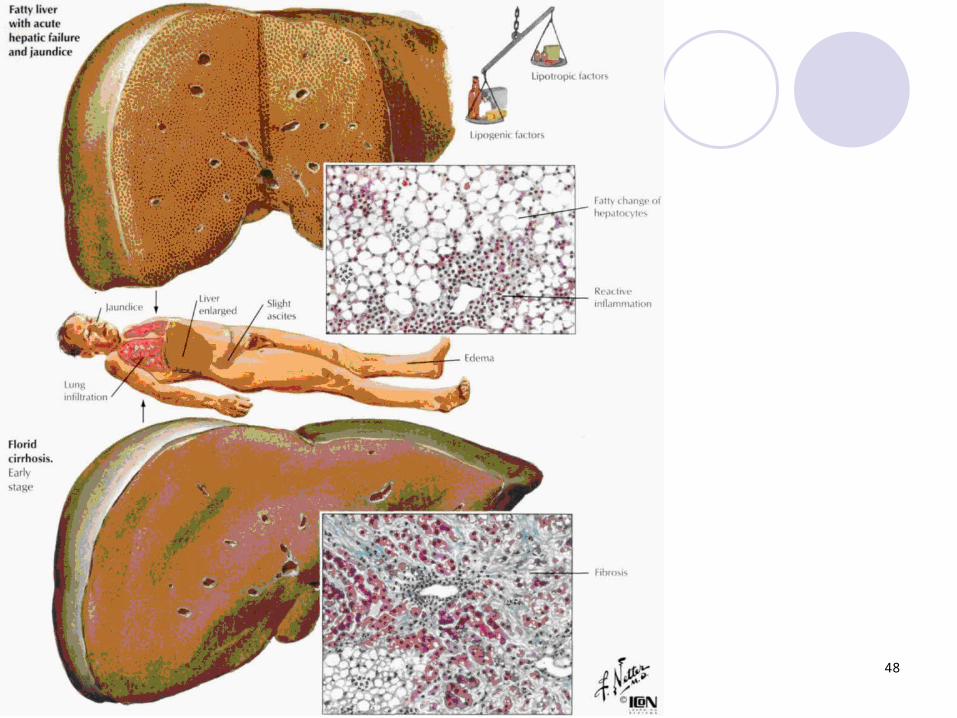
The defeat of liver takes a place as a result of the followings mechanisms:
the cells of liver begin to take away energy from more accessible source – alcohol (the oxidization processes of fat acids which are the source of energy in a norm are stopped, as a result of their accumulation in a cells, that fatty dystrophy develops;
an alcohol is poison & accumulat in a cells, results in its damage, an inflammatory reaction develops round their;
an alcohol stimulates the synthesis of collagen →fibrosis in portal highways primary.
47
Markers of biopsy changes
fatty dystrophy of hepatocells;
acute hepatitis with Mellori hyaline accummulated;
violation of architectonics of liver: portal primary, and than general cirrhosis of liver.
48
49
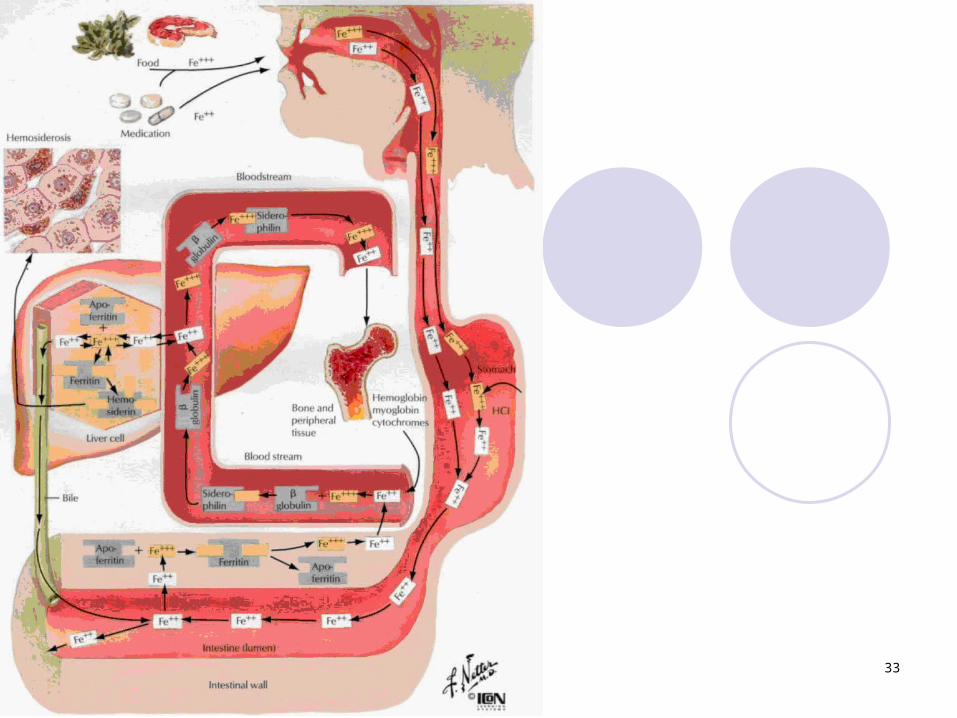
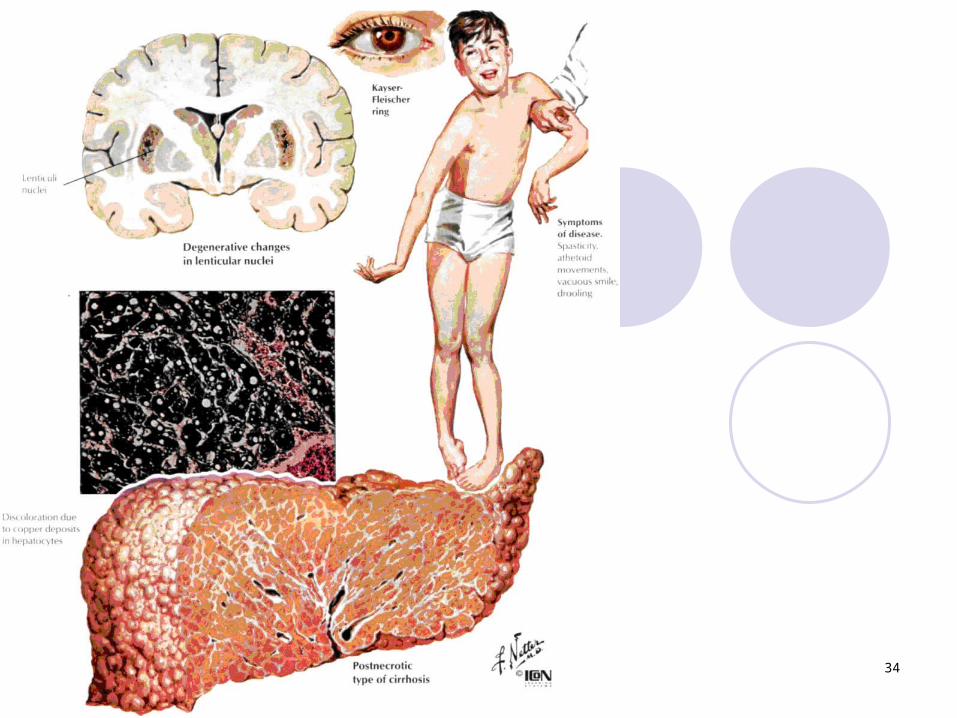
Chronic diseases of liverTo them belong:
overload of liver by iron (haemokhromatozis);illness of Vil'sona (hepatic lentikular
degeneration);insufficiency of α1-antitripsinum;autoimmune diseaseautoimmune ("lyupoid") hepatitis;primary bile cirrhosis.
50
THE END