
1 Characterization of Streptococcus milleri Group Isolates from
7
JOURNAL OF CLINICAL MICROBIOLOGY, Feb. 2010, p. 395–401 Vol. 48, No. 2 0095-1137/10/$12.00 doi:10.1128/JCM.01807-09 Copyright © 2010, American Society for Microbiology. All Rights Reserved. Characterization of Streptococcus milleri Group Isolates from Expectorated Sputum of Adult Patients with Cystic Fibrosis Margot E. Grinwis, 1 Christopher D. Sibley, 1 Michael D. Parkins, 2,4 Christina S. Eshaghurshan, 1 Harvey R. Rabin, 2,4 and Michael G. Surette 1,3 * Department of Microbiology and Infectious Diseases, 1 Department of Medicine, 2 Department of Biochemistry and Molecular Biology, 3 and Adult Cystic Fibrosis Clinic, 4 University of Calgary, Calgary, Alberta, Canada T2N 4N1 Received 14 September 2009/Returned for modification 6 November 2009/Accepted 3 December 2009 With the recent insights into the Streptococcus milleri group (SMG) as pulmonary pathogens in patients with cystic fibrosis (CF), we sought to characterize 128 isolates from the sputum of adults with CF, along with 45 isolates from patients with invasive diseases for comparison. The tests performed included Lancefield group- ing; tests for hemolysis; tests for the production of hyaluronidase, chondroitin sulfatase, DNase, proteases, and hydrogen peroxide; and PCR for the detection of the intermedilysin gene (ily). We also generated biochemical profiles with the Rapid ID Strep 32 API system and tested cell-free supernatants for the presence of the signal molecule autoinducer-2 (AI-2) using a Vibrio harveyi bioassay with a subset of CF strains. The S. intermedius isolates from both strain collections were similar, while the S. constellatus and S. anginosus isolates yielded several biotypes that differed in prevalence between the two strain collections. Beta-hemolytic, Lancefield group C S. constellatus comprised 74.4% of the S. constellatus isolates from patients with CF but only 13.3% of the corresponding isolates from patients with invasive infections. This was the only S. constellatus biotype associ- ated with pulmonary exacerbations. Hyaluronidase-positive S. anginosus was detected only among the isolates from patients with CF. Strain-to-strain variability in AI-2 expression was evident, with the mean values being the highest for S. anginosus, followed by S. constellatus and then S. intermedius. Cluster analysis and 16S rRNA sequencing revealed that the species of SMG could be accurately determined with a minimum of three phenotypic tests: tests for the Lancefield group, hyaluronidase production, and chondroitin sulfatase produc- tion. Furthermore, isolates from patients with invasive infections clustered with isolates from the sputum of patients with CF, suggesting that the respiratory tract isolates were equally pathogenic. Streptococcus intermedius, Streptococcus anginosus, and Streptococcus constellatus are a group of organisms collectively referred to as the Streptococcus milleri group (SMG) or the S. anginosus group (8). Members of the SMG are generally con- sidered to be commensals of the oral cavity, gastrointestinal tract, and female urogenital tract in 15 to 30% of healthy individuals (22) but are clinically known for their association with purulent infections throughout the body (3). Recently, members of the SMG were found to be responsible for up to half of invasive pyogenic streptococcal infections in a large Canadian health region (13) and, after Staphylococcus aureus, were the most common isolates in a microbiological analysis of skin and soft tissue infections (36). Members of the SMG are not widely recognized as pulmonary pathogens, but they have recently gained attention as such, particularly in those with cystic fibrosis (CF) (20, 32; C. D. Sibley, M. E. Grinwis, T. R. Field, M. D. Parkins, J. C. Norgaard, D. B. Gregson, H. R. Rabin, and M. G. Surette, submitted for publication). We have previously shown that the members of the SMG are linked with clinical deterioration in roughly 40% of hospital admissions in our population of adult patients with CF (32; Sibley et al., submitted). We have also shown that the members of the SMG can easily be overlooked by standard clinical microbiology analysis with samples from patients with CF, even when it is the numerically dominant pathogen. Characterization of members of the SMG has shown that these microorganisms are phenotypically diverse (1) and that several strains produce candidate virulence factors, such as hydrolytic enzymes and hemolysins (4, 11, 28, 42, 44). While less than half of the members of the SMG appear to be he- molytic on standard media (10, 22), Nagamune et al. found that virtually all S. intermedius strains produce a potent human- specific cytoxin, intermedilysin, which shows little to no activity against the erythrocytes of other animals (18). Although the members of the SMG have been extensively characterized, there is little information on strains originating from patients with respiratory tract infections. Routine regimens for the cul- ture of specimens from patients with CF do not readily permit the growth of members of the SMG from sputum (9, 25, 32) and differentiation between members of the SMG and other streptococci from nonsterile sites is difficult (27), but the recent development of the semiselective medium McKay agar has led to the improved recovery of members of the SMG from spu- tum (32; Sibley et al., submitted). In the study described here, we characterized 128 SMG isolates from the sputum of pa- tients with CF along with 45 SMG isolates from patients with invasive infections and 3 reference strains. MATERIALS AND METHODS Bacterial strains and growth conditions. All respiratory isolates from patients with CF were obtained from sputum samples collected in sterile containers * Corresponding author. Mailing address: Department of Micro- biology and Infectious Diseases, University of Calgary, Faculty of Medicine, 3330 Hospital Drive NW, Calgary, Alberta, Canada T2N 4N1. Phone: (403) 220-2744 Fax: (403) 270-2772. E-mail: surette @ucalgary.ca. Published ahead of print on 9 December 2009. 395 Downloaded from https://journals.asm.org/journal/jcm on 06 February 2022 by 220.89.52.216.
Transcript of 1 Characterization of Streptococcus milleri Group Isolates from

JOURNAL OF CLINICAL MICROBIOLOGY, Feb. 2010, p. 395–401 Vol. 48, No. 20095-1137/10/$12.00 doi:10.1128/JCM.01807-09Copyright © 2010, American Society for Microbiology. All Rights Reserved.
Characterization of Streptococcus milleri Group Isolates fromExpectorated Sputum of Adult Patients with Cystic Fibrosis�
Margot E. Grinwis,1 Christopher D. Sibley,1 Michael D. Parkins,2,4 Christina S. Eshaghurshan,1
Harvey R. Rabin,2,4 and Michael G. Surette1,3*Department of Microbiology and Infectious Diseases,1 Department of Medicine,2 Department of Biochemistry and Molecular Biology,3 and
Adult Cystic Fibrosis Clinic,4 University of Calgary, Calgary, Alberta, Canada T2N 4N1
Received 14 September 2009/Returned for modification 6 November 2009/Accepted 3 December 2009
With the recent insights into the Streptococcus milleri group (SMG) as pulmonary pathogens in patients withcystic fibrosis (CF), we sought to characterize 128 isolates from the sputum of adults with CF, along with 45isolates from patients with invasive diseases for comparison. The tests performed included Lancefield group-ing; tests for hemolysis; tests for the production of hyaluronidase, chondroitin sulfatase, DNase, proteases, andhydrogen peroxide; and PCR for the detection of the intermedilysin gene (ily). We also generated biochemicalprofiles with the Rapid ID Strep 32 API system and tested cell-free supernatants for the presence of the signalmolecule autoinducer-2 (AI-2) using a Vibrio harveyi bioassay with a subset of CF strains. The S. intermediusisolates from both strain collections were similar, while the S. constellatus and S. anginosus isolates yieldedseveral biotypes that differed in prevalence between the two strain collections. Beta-hemolytic, Lancefield groupC S. constellatus comprised 74.4% of the S. constellatus isolates from patients with CF but only 13.3% of thecorresponding isolates from patients with invasive infections. This was the only S. constellatus biotype associ-ated with pulmonary exacerbations. Hyaluronidase-positive S. anginosus was detected only among the isolatesfrom patients with CF. Strain-to-strain variability in AI-2 expression was evident, with the mean values beingthe highest for S. anginosus, followed by S. constellatus and then S. intermedius. Cluster analysis and 16S rRNAsequencing revealed that the species of SMG could be accurately determined with a minimum of threephenotypic tests: tests for the Lancefield group, hyaluronidase production, and chondroitin sulfatase produc-tion. Furthermore, isolates from patients with invasive infections clustered with isolates from the sputum ofpatients with CF, suggesting that the respiratory tract isolates were equally pathogenic.
Streptococcus intermedius, Streptococcus anginosus, andStreptococcus constellatus are a group of organisms collectivelyreferred to as the Streptococcus milleri group (SMG) or the S.anginosus group (8). Members of the SMG are generally con-sidered to be commensals of the oral cavity, gastrointestinaltract, and female urogenital tract in 15 to 30% of healthyindividuals (22) but are clinically known for their associationwith purulent infections throughout the body (3). Recently,members of the SMG were found to be responsible for up tohalf of invasive pyogenic streptococcal infections in a largeCanadian health region (13) and, after Staphylococcus aureus,were the most common isolates in a microbiological analysis ofskin and soft tissue infections (36). Members of the SMG arenot widely recognized as pulmonary pathogens, but they haverecently gained attention as such, particularly in those withcystic fibrosis (CF) (20, 32; C. D. Sibley, M. E. Grinwis, T. R.Field, M. D. Parkins, J. C. Norgaard, D. B. Gregson, H. R.Rabin, and M. G. Surette, submitted for publication). We havepreviously shown that the members of the SMG are linked withclinical deterioration in roughly 40% of hospital admissions inour population of adult patients with CF (32; Sibley et al.,submitted). We have also shown that the members of the SMG
can easily be overlooked by standard clinical microbiologyanalysis with samples from patients with CF, even when it is thenumerically dominant pathogen.
Characterization of members of the SMG has shown thatthese microorganisms are phenotypically diverse (1) and thatseveral strains produce candidate virulence factors, such ashydrolytic enzymes and hemolysins (4, 11, 28, 42, 44). Whileless than half of the members of the SMG appear to be he-molytic on standard media (10, 22), Nagamune et al. foundthat virtually all S. intermedius strains produce a potent human-specific cytoxin, intermedilysin, which shows little to no activityagainst the erythrocytes of other animals (18). Although themembers of the SMG have been extensively characterized,there is little information on strains originating from patientswith respiratory tract infections. Routine regimens for the cul-ture of specimens from patients with CF do not readily permitthe growth of members of the SMG from sputum (9, 25, 32)and differentiation between members of the SMG and otherstreptococci from nonsterile sites is difficult (27), but the recentdevelopment of the semiselective medium McKay agar has ledto the improved recovery of members of the SMG from spu-tum (32; Sibley et al., submitted). In the study described here,we characterized 128 SMG isolates from the sputum of pa-tients with CF along with 45 SMG isolates from patients withinvasive infections and 3 reference strains.
MATERIALS AND METHODS
Bacterial strains and growth conditions. All respiratory isolates from patientswith CF were obtained from sputum samples collected in sterile containers
* Corresponding author. Mailing address: Department of Micro-biology and Infectious Diseases, University of Calgary, Faculty ofMedicine, 3330 Hospital Drive NW, Calgary, Alberta, Canada T2N4N1. Phone: (403) 220-2744 Fax: (403) 270-2772. E-mail: [email protected].
� Published ahead of print on 9 December 2009.
395
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 22
0.89
.52.
216.

according to ethical guidelines for adult patients with CF attending the SouthernAlberta Cystic Fibrosis Clinic. Ninety-nine strains were isolated on McKay agaras part of a 6-month surveillance study from September 2007 to March 2008(Sibley et al., submitted). The remaining 29 isolates were collected between 2006and 2008 and placed on McKay agar (32), brain heart infusion (BHI) agar(Difco), Trypticase soy agar (Difco) with 0.3% yeast extract (Bacto), Columbiablood agar (CBA; Difco) with 5% sheep blood (Med-Ox), Columbia-colistin-nalidixic acid (CNA) agar (BBL) with 5% sheep blood, BHI agar with 0.01 mg/mlcolistin sulfate salt and 0.005 mg/ml oxilinic acid (Sigma-Aldrich, St. Louis, MO)(BHI-CO), chocolate agar, fastidious anaerobe agar (Becton Dickinson), andphenylethyl alcohol agar (BBL) at 37°C under CO2-enriched (5%) and anaerobicconditions. Forty-five isolates from patients with invasive infections (blood, em-pyema, unknown sources, brain abscess, liver abscess, and hip abscess) wereobtained from Calgary Laboratory Services; 42 of these isolates were recoveredon CBA. Strains from patients with invasive infections had been identified asmembers of the SMG according to standard phenotypic procedures, and thespecies had been determined by partial 16S rRNA gene PCR and sequencing.Reference strains S. intermedius ATCC 27335, S. constellatus ATCC 27823, andS. anginosus ATCC 33397 were included in this study. All strains from patientswith CF were identified by partial 16S rRNA gene PCR and sequencing, asdescribed by Sibley et al. (32). The isolates were stored at �80°C with 15%glycerol or 10% skim milk as cryopreservatives.
Hemolysis and Lancefield grouping. Isolates were screened for hemolysis onCBA at 37°C with 5% CO2 after 48 h of incubation. Lancefield grouping wasperformed with all isolates by use of a commercial kit (Oxoid, Nepean, Ontario,Canada).
Intermedilysin PCR. PCR for the intermedilysin gene (ily) was performed asdescribed previously (19) by using Chelex-extracted DNA (Bio-Rad, Hercules,CA), as described previously (40).
Biochemical profiling. Biochemical profiles were determined with Rapid IDStrep 32 API strips (bioMerieux, Marcy l’Etoile, France), according to themanufacturer’s instructions, with the following adjustments: each inoculum wasprepared from isolated colonies that had been subcultured onto BHI-CO agarand incubated for 72 h at 37°C with 5% CO2.
Arginine hydrolysis and VP tests. Arginine hydrolysis and Vogues-Proskauer(VP) tests were performed as described by Ruoff and Ferraro (26). Moellerdecarboxylase broth base supplemented with arginine, MR-VP broth, alpha-naphthol, and 40% potassium hydroxide were purchased from Oxoid; creatinepowder was purchased from Sigma-Aldrich.
Hydrogen peroxide assay. All strains were tested for hydrogen peroxide pro-duction by the Prussian blue plate assay described by Saito et al. (29). Briefly,isolates were patched onto Prussian blue agar, and the plates were incubated at37°C with 5% CO2. The plates were checked for the development of the Prussianblue precipitate after 2 to 7 days. Dilutions of hydrogen peroxide were used aspositive controls.
Determination of enzymatic activities. Hyaluronidase and chondroitin sulfa-tase activities were determined by the plate assays described by Smith and Willet(33), except that hyaluronic acid sodium salt from a Streptococcus equi species(Fluka) was used instead of human umbilical potassium hyaluronidate and chon-droitin sulfate from whale and shark cartilage (sodium salt) (Sigma-Aldrich) wasused instead of bovine nasal chondroitin sulfate. DNase activity was determinedby the plate assay described by Porschen and Sonntag (23) with BHI agar as thebasal medium, except that the yeast extract and dyes were omitted. DNase plateswere flooded with 1 M HCl after 2 to 3 days of incubation and were observed fora zone of clearing around the growth. Protease activity was determined by theplate assay described by Lutticken et al. (15), except that 2% skim milk powder(Difco) was used in place of purified casein. The hyaluronic acid plates wereincubated for 24 h, and the DNA and skim milk plates were incubated for 48 to72 h at 37°C with 5% CO2. The chondroitin sulfate plates were incubatedanaerobically for 7 days. An S. intermedius isolate from this study was used as apositive control since that isolate yielded zones of clearing for all of the assaysdescribed above.
Cluster analysis. The results for all tests were recorded as either 0 (negative)or 1 (positive). Average-linkage hierarchal clustering was performed by using theCluster program (version 3.0) and was viewed by use of the Java Treeviewprogram (version 1.1.3) (7).
AI-2 expression assays. At 72 h, colonies of 27 strains from patients with CF(9 S. intermedius, 9 S. constellatus, and 9 S. anginosus strains) and 3 referencestrains were used to inoculate 2 ml of BHI broth, and the broths were incubatedfor 48 h at 37°C with 5% CO2. Fifty microliters was transferred to 5 ml ofTodd-Hewitt-yeast broth with 0.5% yeast extract (Bacto), and the broths wereincubated for 24 h at 37°C with 5% CO2. The tubes were checked for turbidityas a confirmation of growth, 1 ml was transferred to a sterile 1.5-ml tube, and the
tube was centrifuged at maximum speed for 5 min. Four hundred microliters ofthe supernatant was transferred to a clean tube and was stored at �20°C untiluse. The detection of AI-2 in the supernatants was performed in triplicate asdescribed by Surette and Bassler (37). Vibrio harveyi AI-2 reporter strain MM32(luxS and luxN negative) was maintained on Luria-marine agar (2) at 30°C.Sterile Todd-Hewitt-yeast broth was used as a negative control. Luciferase pro-duction (counts per second) was measured for 24 h by using a Wallac Victor2.For statistical analysis, Tukey’s multiple-comparison test was performed by theuse of Prism software (version 5.0; GraphPad Software, Inc.).
RESULTS
We characterized 128 isolates from the sputum of 47 pa-tients with CF recovered at times of both clinical stability andpulmonary exacerbation. We also examined 45 isolates frompatients with invasive infections and 3 reference strains forcomparison. Of the isolates from patients with CF, 22 fromeight patients were cultured from hospital admission samplesat levels of �107 CFU/ml, which was greater than or equivalentto the levels of the conventional CF pathogen present (Pseudo-monas aeruginosa in seven patients, Staphylococcus aureus inone patient). This is a unique strain collection from a singlepatient population with no evidence of transmission betweenpatients (unpublished data).
Table 1 shows the phenotypic characteristics of all isolateswith respect to hemolysis, Lancefield grouping, the productionof hydrolytic enzymes and hydrogen peroxide, and detection ofthe intermedilysin gene (ily). The S. intermedius isolates fromthe collections of isolates from patients with CF and patientswith invasive infections were highly similar. All strains wereLancefield nongroupable, and all except two strains producedall of the hydrolytic enzymes for which tests were conducted;the exceptions were two strains from patients with invasiveinfections, which lacked proteases. The S. intermedius isolateswere virtually devoid of �-hemolysis on CBA (60/61, 98.4%),although ily was found exclusively in all of the S. intermediusisolates. Two of the S. intermedius isolates from patients withCF produced a rosy pigment on BHI-CO agar.
The majority of S. constellatus isolates from patients with CF(32/43, 74.4%) were beta-hemolytic and Lancefield group Cand produced all of the hydrolytic enzymes for which tests wereconducted (Table 1). This was the only S. constellatus profilethat was linked to multiple pulmonary exacerbations in ourcollection. These strains resemble S. constellatus subsp. phar-yngis, a variant of S. constellatus of oral origin associated withpharyngitis (43). Only 2 of 15 (13.3%) invasive S. constellatusisolates shared this profile. All Lancefield group F S. constel-latus isolates were beta-hemolytic and lacked chondroitin sul-fatase and proteases. Likewise, all nongroupable S. constellatusisolates lacked chondroitin sulfatase, but 6/10 (60%) isolatesfrom patients with CF and 4/7 (57.1%) isolates from patientswith invasive infections were positive for proteases. The pro-tease-positive nongroupable S. constellatus isolates both frompatients with CF and from patients with invasive infectionstended to be nonhemolytic; only a single invasive isolate wasboth beta-hemolytic and protease positive. All S. constellatusisolates were positive for hyaluronidase and DNase.
The S. anginosus isolates from both strain collections exhib-ited diverse phenotypes (Table 1). Only beta-hemolytic Lance-field group C S. anginosus isolates were positive for hyaluron-idase (n � 5), and all of these strains were from patients with
396 GRINWIS ET AL. J. CLIN. MICROBIOL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 22
0.89
.52.
216.

CF. Two of these strains were linked to separate exacerbationsin a single patient. None of the S. anginosus isolates producedchondroitin sulfatase, and only a single isolate from a patientwith CF failed to produce DNase. Ninety-four percent of the S.anginosus (45/48) isolates from patients with CF were proteasepositive, while 66.7% of the S. anginosus (6/9) isolates frompatients with invasive infections were protease positive. Over-all, 10.2% (13/128) of the isolates from patients with CF werepositive for hydrogen peroxide production, and most of thesewere S. anginosus (10/13, 76.9%); the remaining 3 isolates wereS. constellatus. Similarly, 6.3% of the isolates from patientswith invasive infections (two S. constellatus isolates, one S.anginosus isolate) were hydrogen peroxide positive.
A subset of strains (nine S. anginosus, nine S. constellatus,and nine S. intermedius strains) of various phenotypes andfrom various patients with CF plus three reference strains wereused in a Vibrio harveyi bioassay for detection of the quorum-sensing signal molecule autoinducer-2 (AI-2) in cell-free su-pernatants (37). The levels of detection were from 5- to 552-fold greater than the background levels, and variability wasevident within each species (Fig. 1). The mean levels were thehighest for S. anginosus (330-fold), followed by S. constellatus
(199-fold) and S. intermedius (134-fold). Only the values for S.anginosus and S. intermedius were significantly different (P �0.05).
In addition to the phenotypes described in Table 1, testing
TABLE 1. Phenotypic differentiation of the S. milleri isolates used in this study
Isolate source No. ofisolates
No. ofpatients
No. of isolates positive for:
Hemolysis Lancefieldgroup
Hyaluronidaseproduction
Chondroitinsulfatase
production
DNaseproduction
Proteaseproduction
H2O2production ilya
S. intermediusCF stable sputumb 31 21 1 � 1 NGc 1 1 1 1 0 1
30 � or � 30 NG 30 30 30 30 0 30Exacerbation associated 6 3 6 � or � 6 NG 6 6 6 6 0 6Invasived 24 24 � or � 24 NG 24 24 24 22 0 24
S. constellatusCF stable sputum 30 11 22 � 19 C 19 19 19 19 0 0
1 F 1 0 1 0 1 02 NG 2 0 2 0 0 0
8 � or � 8 NG 8 0 8 6 2 0Exacerbation associated 13 3 13 � 13 C 13 13 13 13 0 0Invasive 15 11 � 2 C 2 2 2 2 0 0
6 F 6 0 6 0 0 03 NG 3 0 3 1 1 0
4 � or � 4 NG 4 0 4 3 1 0
S. anginosusCF stable sputum 45 24 15 � 3 C 3 0 3 3 0 0
4 F 0 0 4 3 1 03 G 0 0 3 2 1 05 NG 0 0 5 4 1 0
30 � or � 6 C 0 0 6 6 1 017 F 0 0 17 17 3 07 NG 0 0 6 7 2 0
Exacerbation associated 3 2 2 � 2 C 2 0 2 2 0 01 � or � 1 F 0 0 1 1 1 0
Invasive 9 6 � 1 A 0 0 1 1 0 02 C 0 0 2 1 1 02 G 0 0 2 2 0 01 NG 0 0 1 0 0 0
3 � or � 2 F 0 0 2 2 0 01 NG 0 0 1 0 0 0
a ily, intermedilysin gene, as determined by PCR.b Sputum samples were collected during periods of clinical stability.c NG, Lancefield nongroupable.d Samples from patients with invasive infections.
FIG. 1. Detection of AI-2 in SMG isolates. As a measure of AI-2expression, the maximum counts per second (CPSmax) were deter-mined for three replicates of each supernatant and the negative control(sterile Todd-Hewitt-yeast broth) during a 24-h assay period. Blackcircles, ratio of the average maximum counts per second for eachsupernatant to the average maximum counts per second for the neg-ative control; bars, mean for each species.
VOL. 48, 2010 STREPTOCOCCUS MILLERI FROM PATIENTS WITH CF 397
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 22
0.89
.52.
216.
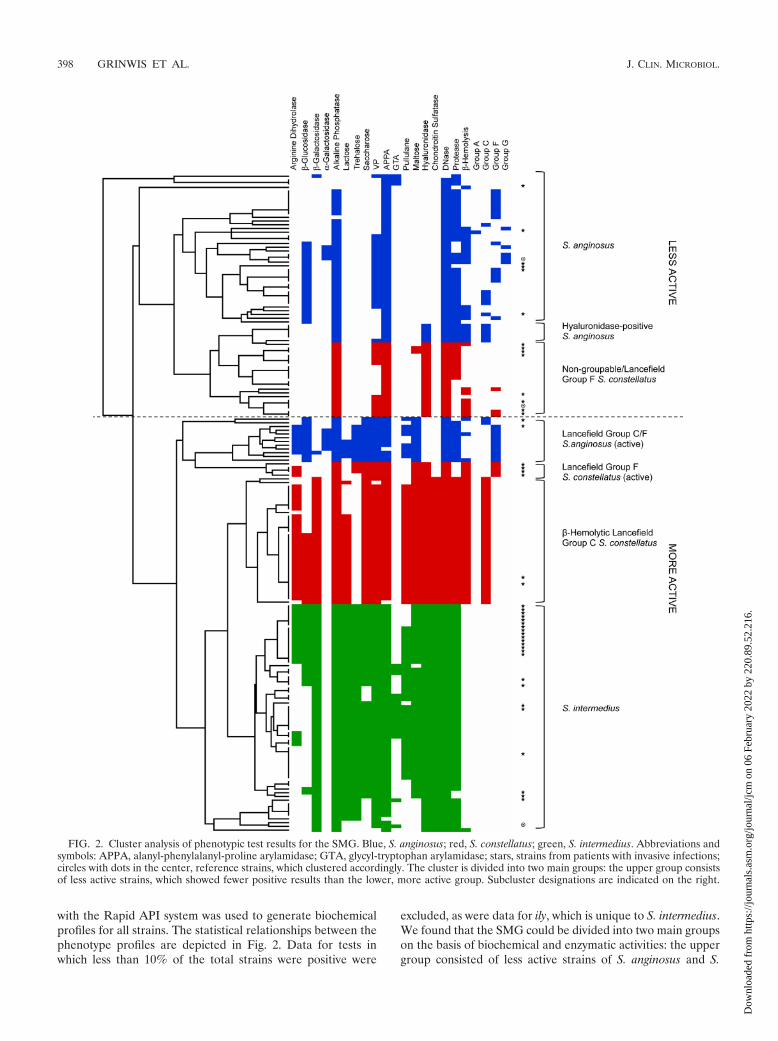
with the Rapid API system was used to generate biochemicalprofiles for all strains. The statistical relationships between thephenotype profiles are depicted in Fig. 2. Data for tests inwhich less than 10% of the total strains were positive were
excluded, as were data for ily, which is unique to S. intermedius.We found that the SMG could be divided into two main groupson the basis of biochemical and enzymatic activities: the uppergroup consisted of less active strains of S. anginosus and S.
FIG. 2. Cluster analysis of phenotypic test results for the SMG. Blue, S. anginosus; red, S. constellatus; green, S. intermedius. Abbreviations andsymbols: APPA, alanyl-phenylalanyl-proline arylamidase; GTA, glycyl-tryptophan arylamidase; stars, strains from patients with invasive infections;circles with dots in the center, reference strains, which clustered accordingly. The cluster is divided into two main groups: the upper group consistsof less active strains, which showed fewer positive results than the lower, more active group. Subcluster designations are indicated on the right.
398 GRINWIS ET AL. J. CLIN. MICROBIOL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 22
0.89
.52.
216.

constellatus (fewer numbers of positive results), while the lowergroup consisted of more active strains of all three species(greater numbers of positive results). Seven unique clusterswere identified (Fig. 2). From these clusters, it is clear that S.anginosus and S. constellatus each comprised at least threedistinct biotypes, while S. intermedius is more homogeneous. Intwo cases, clades that primarily consisted of invasive strainswere formed. One was the active Lancefield group F S. con-stellatus cluster, and the other was within the S. intermediuscluster, distinguished from the other clades by arginine hydro-lysis and �-glucosidase production. The beta-hemolytic, Lance-field group C, hyaluronidase-positive S. anginosus cluster con-sisted solely of isolates from patients with CF. Each of thereference strains clustered accordingly.
Only 35% of the strains hydrolyzed arginine and 81% of thestrains were VP test positive by use of the Rapid API strips(Fig. 2). Several reports have indicated that more than 90% ofSMG isolates are positive both for arginine hydrolysis and bythe VP test (1, 36, 44), which are considered to be of primaryvalue in distinguishing the SMG from other streptococci (26).To confirm whether this was due to a deficiency in the RapidAPI strips, we tested a subset of strains (111 strains frompatients with CF, 37 strains from patients with invasive infec-tions) for arginine hydrolysis and positivity by the VP test bythe method described by Ruoff and Ferraro (26). By thismethod, we found that 88% and 98% of the isolates frompatients with CF were positive for arginine hydrolysis and bythe VP test, respectively. The isolates from patients with inva-sive infections yielded similar results: 86% and 95% were pos-itive for arginine hydrolysis and by the VP test, respectively. Ofthe isolates in both groups that were arginine hydrolysis neg-ative (n � 19), 89.5% (17/19) were S. intermedius. Of the S.intermedius isolates from patients with CF (n � 11), 81.8%(9/11) were from patients who have had S. intermedius-associ-ated exacerbations. Two of the arginine hydrolysis-negative S.intermedius invasive isolates were also from a patient with CF.
Furthermore, we found that the cluster diagram was surpris-ingly accurate for determination of the species of the SMG.Before the identification of 35 isolates from patients with in-vasive infections by the 16S rRNA PCR, we used the sevencluster designations to determine the species of the strains anddid a blind comparison to the identifications obtained by the16S rRNA PCR. We observed a complete correlation betweenthe two identification methods and were able to compose a
minimal scheme that could accurately determine the species ofall of the strains in our study (Fig. 3). This scheme depends onhyaluronidase production, chondroitin sulfatase production,and the Lancefield grouping.
DISCUSSION
Our knowledge of pathogenic microorganisms and theirphenotypic traits predominantly stems from the analysis ofstrains from patients with acute infections, in which the patho-gen and the disease are short-lived. The airway of a patientwith CF, however, presents a unique scenario because patho-gens that typically form acute infections have the opportunityto adapt to their host and establish chronic infections, whichare also subject to the influence of antibiotic selective pres-sures. Thus, it is possible that the airways of patients with CFharbor unique biotypes of microorganisms that are differentfrom their invasive counterparts causing acute disease. Wesought to investigate this for the SMG by comparing strainsfrom the airways of patients with CF to strains from patientswith invasive infections. Additionally, our isolation and iden-tification techniques, which included a variety of types of me-dia, incubation conditions, and molecular methods, may haverecovered biotypes either that fail to grow on the typicallyemployed blood agar or that would be misidentified by stan-dard biochemical tests. Our novel collection of SMG strainsfrom a total of 47 patients with CF contained 22 isolates fromsputum linked to pulmonary exacerbation and 106 isolatesfrom sputum during periods of clinical stability.
Because of their ability to break down components of hosttissue, hydrolytic enzymes are presumed virulence determi-nants in the SMG. All of the S. intermedius and S. constellatusstrains studied produced hyaluronidase, while only 10% of S.anginosus strains produced hyaluronidase, consistent with thefindings of previous studies (11, 44). None of the hyaluroni-dase-positive S. anginosus isolates were from the group ofpatients with invasive infections, although they were similar tothe DNA group 2 strains described by Whiley et al. (43). S.anginosus was rarely associated with pulmonary exacerbationin this study, but hyaluronidase-positive S. anginosus waslinked to two separate exacerbations in a single patient.
The proportion of DNase-positive isolates was much higherin this study than in previous ones, in which no more than 75%of isolates produced detectable DNases (11, 24). Since the
FIG. 3. Proposed scheme for determination of the SMG species. The assignment of subtypes, namely, S. constellatus subsp. constellatus, S.constellatus subsp. pharyngis, and DNA group 2 strains, was based on the strain descriptions provided by Whiley et al. (43).
VOL. 48, 2010 STREPTOCOCCUS MILLERI FROM PATIENTS WITH CF 399
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 22
0.89
.52.
216.

strains from patients with invasive infections and patients withCF did not differ in this respect, it is possible that DNase ismore widespread in the SMG than was previously thought,which would be consistent with the invasive nature of thesepathogens (35, 41). It is interesting that the majority of strainsalso produced proteases, while none of the 72 SMG isolatestested by Ruoff and Ferraro (28) or the 86 isolates tested byLutticken et al. (15) showed protease activity. This observationmay be due to differences in the methodology used or theinterpretation of the results, as the zones of clearing in thisassay were not as vivid as those in the other plate assays used.In this study, many protease-negative strains belonged to thebeta-hemolytic nongroupable and Lancefield group F S. con-stellatus biotypes, which were more common in the group ofstrains from patients with invasive infections. Chondroitin sul-fatase activity was also more prevalent in the SMG than haspreviously been reported (11, 28) and was uniformly detectedin S. intermedius and beta-hemolytic Lancefield group C S.constellatus isolates. These findings corroborate those found byTakao and colleagues (38, 39), in that two types of hylauroni-dases exist within the SMG: those with chondroitin sulfataseactivity, found only in S. intermedius and S. constellatus subsp.pharyngis, and those without chondroitin sulfatase activity,found in S. constellatus subsp. constellatus and reference strainMAS624, a beta-hemolytic Lancefield group C S. anginosusstrain (43). Thus, the hyaluronidase and chondroitin sulfataseactivities observed are likely due to a single enzyme with abroad substrate range.
Hydrogen peroxide production in the SMG was consistentwith the findings described in previous reports (42, 44) and wasmost commonly associated with S. anginosus. In agreementwith the findings of Nagamune et al. (19), the intermedilysingene (ily) was found exclusively in all S. intermedius isolates.The heightened recovery of beta-hemolytic Lancefield group CS. constellatus strains, otherwise known as S. constellatus subsp.pharyngis, from the sputum of patients with CF (43) is likelyattributable to the use of McKay agar in our studies. Thisbiotype tended to grow poorly on CBA, the standard nonse-lective medium used for the primary isolation of streptococcifrom CF sputum and other specimens from non-CF patients,which might explain its low incidence in the collection of iso-lates from patients with invasive infections.
The quorum-sensing signal molecule AI-2 has been shown toinfluence virulence traits in several streptococcal species, in-cluding the SMG (16, 17, 21, 34). Unlike experiments involvingStreptococcus mutans or Streptococcus pneumoniae, in whichAI-2 was difficult to detect in culture supernatants (12, 17),AI-2 was readily detected in the supernatants of the SMGisolates. The range of levels observed highlights the strain-to-strain variability characteristic of AI-2 expression profiles.Since the SMG are commonly isolated from individuals withpolymicrobial infections (3) and have been shown to act syn-ergistically with other organisms (30, 31), it is possible thatAI-2 mediates synergistic virulence between species (5, 6).
Use of the combination of 16S rRNA PCR identificationmethods and phenotypic profiling affirms that the SMG isindeed composed of three distinct species, and these may befurther divided into multiple subtypes, as suggested previously(43, 45). The phenotypic diversity and the overlapping traits ofthe SMG isolates have generally made determination of the
species of the strains a difficult task (27). Through substantialcharacterization of the SMG, an effective and reliable schemewhich differentiates the three species on the basis of eightenzymatic tests has been developed (14, 44). We have foundhere that by the use of 16S rRNA PCR identification as the“gold standard” for comparison, tests for hyaluronidase pro-duction, chondroitin sulfatase production, and Lancefieldgroup are sufficient for determination of the species of themembers of the SMG and the subtype. Similarly, Takao et al.(39) found that the genes responsible for hyaluronidase andchondroitin sulfatase activity were useful for determination ofthe species of the members of the SMG by PCR, since theirrespective amplicons differed in size. We have yet to determinewhether the scheme presented here can be used to distinguishthe SMG from other streptococci or to what extent it holdstrue for the SMG.
This is the first study to provide a comprehensive character-ization of SMG isolates from patients with CF. Strains frompatients with invasive infections and patients with CF alike areequipped with potential virulence factors, which may even beuseful for species and subtype determination. We have shownhere that most SMG biotypes are shared by strains from pa-tients with invasive infections and patients with CF, but certainbiotypes may be more prevalent and clinically relevant in pa-tients with CF, such as beta-hemolytic Lancefield group C S.constellatus or arginine hydrolysis-negative S. intermedius. Inour previous studies, the only time that the members of theSMG were detected at elevated levels (�107 CFU/ml) was athospital admission, and treatment directed toward the SMGresulted in clinical resolution (20, 32). Our strain collection isrelatively small and is limited to one patient population, yet itprovides the groundwork for resolving the complexity of SMGbiotypes in chronic airway infections in patients with CF.
ACKNOWLEDGMENTS
We thank the Southern Alberta Cystic Fibrosis Clinic and CF pa-tients for their vital contributions to this study. We also thank CalgaryLaboratory Services for the generous provision of strains.
This work was supported by a grant from the Canadian CysticFibrosis Foundation to M.G.S. M.G.S. is supported as an AlbertaHeritage Foundation for Medical Research Scientist and Canada Re-search Chair in Microbial Gene Expression. M.E.G. is supported bystudentships from the Canadian Institutes of Health Research, Cana-dian Cystic Fibrosis Foundation, and the Alberta Heritage Foundationfor Medical Research.
REFERENCES
1. Ball, L. C., and M. T. Parker. 1979. The cultural and biochemical charactersof Streptococcus milleri strains isolated from human sources. J. Hyg. (Lond.)82:63–78.
2. Bassler, B. L., M. Wright, and M. R. Silverman. 1994. Multiple signallingsystems controlling expression of luminescence in Vibrio harveyi: sequenceand function of genes encoding a second sensory pathway. Mol. Microbiol.13:273–286.
3. Belko, J., D. A. Goldmann, A. Macone, and A. K. M. Zaidi. 2002. Clinicallysignificant infections with organisms of the Streptococcus milleri group. Pe-diatr. Infect. Dis. J. 21:715–723.
4. Bridge, P. D., and P. H. Sneath. 1983. Numerical taxonomy of Streptococcus.J. Gen. Microbiol. 129:565–597.
5. Duan, K., C. Dammel, J. Stein, H. Rabin, and M. G. Surette. 2003. Modu-lation of Pseudomonas aeruginosa gene expression by host microflorathrough interspecies communication. Mol. Microbiol. 50:1477–1491.
6. Duan, K., C. D. Sibley, C. J. Davidson, and M. G. Surette. 2009. Chemicalinteractions between organisms in microbial communities. Contrib. Micro-biol. 16:1–17.
7. Eisen, M. B., P. T. Spellman, P. O. Brown, and D. Botstein. 1998. Clusteranalysis and display of genome-wide expression patterns. Proc. Natl. Acad.Sci. U. S. A. 95:14863–14868.
400 GRINWIS ET AL. J. CLIN. MICROBIOL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 22
0.89
.52.
216.

8. Facklam, R. R. 1984. The major differences in the American and BritishStreptococcus taxonomy schemes with special reference to Streptococcus mil-leri. Eur. J. Clin. Microbiol. 3:91–93.
9. Harris, J. K., M. A. De Groote, S. D. Sagel, E. T. Zemanick, R. Kapsner, C.Penvari, H. Kaess, R. R. Deterding, F. J. Accurso, and N. R. Pace. 2007.Molecular identification of bacteria in bronchoalveolar lavage fluid fromchildren with cystic fibrosis. Proc. Natl. Acad. Sci. U. S. A. 104:20529–20533.
10. Jacobs, J. A., C. S. Schot, and L. M. Schouls. 2000. Haemolytic activity of the‘Streptococcus milleri group’ and relationship between haemolysis restrictedto human red blood cells and pathogenicity in S. intermedius. J. Med. Mi-crobiol. 49:55–62.
11. Jacobs, J. A., and E. E. Stobberingh. 1995. Hydrolytic enzymes of Strepto-coccus anginosus, Streptococcus constellatus and Streptococcus intermedius inrelation to infection. Eur. J. Clin. Microbiol. Infect. Dis. 14:818–820.
12. Joyce, E. A., A. Kawale, S. Censini, C. C. Kim, A. Covacci, and S. Falkow.2004. LuxS is required for persistent pneumococcal carriage and expressionof virulence and biosynthesis genes. Infect. Immun. 72:2964–2975.
13. Laupland, K. B., T. Ross, D. L. Church, and D. B. Gregson. 2006. Popula-tion-based surveillance of invasive pyogenic streptococcal infection in a largeCanadian region. Clin. Microbiol. Infect. 12:224–230.
14. Limia, A., T. Alarcon, M. L. Jimenez, and M. Lopez-Brea. 2000. Comparisonof three methods for identification of Streptococcus milleri group isolates tospecies level. Eur. J. Clin. Microbiol. Infect. Dis. 19:128–131.
15. Lutticken, R., U. Wendorff, D. Lutticken, E. A. Johnson, and L. W. Wanna-maker. 1978. Studies on streptococci resembling Streptococcus milleri and onan associated surface-protein antigen. J. Med. Microbiol. 11:419–431.
16. Lyon, W. R., J. C. Madden, J. C. Levin, J. L. Stein, and M. G. Caparon. 2001.Mutation of luxS affects growth and virulence factor expression in Strepto-coccus pyogenes. Mol. Microbiol. 42:145–157.
17. Merritt, J., F. Qi, S. Goodman, and M. Anderson. 2003. Mutation of luxSaffects biofilm formation in Streptococcus mutans. Infect. Immun. 71:1972–1979.
18. Nagamune, H., C. Ohnishi, A. Katsuura, K. Fushitani, R. A. Whiley, A.Tsuji, and Y. Matsuda. 1996. Intermedilysin, a novel cytotoxin specific forhuman cells secreted by Streptococcus intermedius UNS46 isolated from ahuman liver abscess. Infect. Immun. 64:3093–3100.
19. Nagamune, H., R. A. Whiley, T. Goto, Y. Inai, T. Maeda, J. M. Hardie, andH. Kourai. 2000. Distribution of the intermedilysin gene among the angino-sus group streptococci and correlation between intermedilysin productionand deep-seated infection with Streptococcus intermedius. J. Clin. Microbiol.38:220–226.
20. Parkins, M. D., C. D. Sibley, M. G. Surette, and H. R. Rabin. 2008. TheStreptococcus milleri group—an unrecognized cause of disease in cystic fi-brosis: a case series and literature review. Pediatr. Pulmonol. 43:490–497.
21. Pecharki, D., F. C. Petersen, and A. A. Scheie. 2008. LuxS and expression ofvirulence factors in Streptococcus intermedius. Oral Microbiol. Immunol.23:79–83.
22. Poole, P. M., and G. Wilson. 1979. Occurrence and cultural features ofStreptococcus milleri in various body sites. J. Clin. Pathol. 32:764–768.
23. Porschen, R. K., and S. Sonntag. 1974. Extracellular deoxyribonucleaseproduction by anaerobic bacteria. Appl. Microbiol. 27:1031–1033.
24. Pulliam, L., R. K. Porschen, and W. K. Hadley. 1980. Biochemical propertiesof CO2-dependent streptococci. J. Clin. Microbiol. 12:27–31.
25. Rogers, G. B., T. W. Daniels, A. Tuck, M. P. Carroll, G. J. Connett, G. J.David, and K. D. Bruce. 2009. Studying bacteria in respiratory specimens byusing conventional and molecular microbiological approaches. BMC Pulm.Med. 9:14.
26. Ruoff, K. L., and M. J. Ferraro. 1986. Presumptive identification of Strepto-coccus milleri in 5 h. J. Clin. Microbiol. 24:495–497.
27. Ruoff, K. L. 1988. Streptococcus anginosus (“Streptococcus milleri”): the un-recognized pathogen. Clin. Microbiol. Rev. 1:102–108.
28. Ruoff, K. L., and M. J. Ferraro. 1987. Hydrolytic enzymes of “Streptococcusmilleri.” J. Clin. Microbiol. 25:1645–1647.
29. Saito, M., M. Seki, K. Iida, H. Nakayama, and S. Yoshida. 2007. A novelagar medium to detect hydrogen peroxide-producing bacteria based on thePrussian blue-forming reaction. Microbiol. Immunol. 51:889–892.
30. Shinzato, T., and A. Saito. 1994. A mechanism of pathogenicity of “Strepto-coccus milleri group” in pulmonary infection: synergy with an anaerobe.J. Med. Microbiol. 40:118–123.
31. Shinzato, T., and A. Saito. 1995. The Streptococcus milleri group as a causeof pulmonary infections. Clin. Infect. Dis. 21(Suppl. 3):S238–S243.
32. Sibley, C. D., M. D. Parkins, K. Duan, J. C. Norgaard, H. R. Rabin, andM. G. Surette. 2008. A polymicrobial perspective of pulmonary exacerba-tions exposes an enigmatic pathogen in cystic fibrosis patients. Proc. Natl.Acad. Sci. U. S. A. 105:15070–15075.
33. Smith, R. F., and N. P. Willett. 1968. Rapid plate method for screeninghyaluronidase and chondroitin sulfatase-producing microorganisms. Appl.Microbiol. 16:1434–1436.
34. Stroeher, U. H., A. W. Paton, A. D. Ogunniyi, and J. C. Paton. 2003. Muta-tion of luxS of Streptococcus pneumoniae affects virulence in a mouse model.Infect. Immun. 71:3206–3212.
35. Sumby, P., K. D. Barbian, D. J. Gardner, A. R. Whitney, D. M. Welty, R. D.Long, J. R. Bailey, M. J. Parnell, N. P. Hoe, G. G. Adams, F. R. Deleo, andJ. M. Musser. 2005. Extracellular deoxyribonuclease made by group A Strep-tococcus assists pathogenesis by enhancing evasion of the innate immuneresponse. Proc. Natl. Acad. Sci. U. S. A. 102:1679–1684.
36. Summanen, P. H., M.-C. Rowlinson, J. Wooton, and S. M. Finegold. 2009.Evaluation of genotypic and phenotypic methods for differentiation of themembers of the anginosus group streptococci. Eur. J. Clin. Microbiol. Infect.Dis. 28:1123–1128.
37. Surette, M. G., and B. L. Bassler. 1998. Quorum sensing in Escherichia coliand Salmonella typhimurium. Proc. Natl. Acad. Sci. U. S. A. 95:7046–7050.
38. Takao, A. 2003. Cloning and expression of hyaluronate lyase genes of Strep-tococcus intermedius and Streptococcus constellatus subsp. constellatus. FEMSMicrobiol. Lett. 219:143–150.
39. Takao, A., H. Nagamune, and N. Maeda. 2004. Identification of the angino-sus group within the genus Streptococcus using polymerase chain reaction.FEMS Microbiol. Lett. 233:83–89.
40. Walsh, P. S., D. A. Metzger, and R. Higuchi. 1991. Chelex 100 as a mediumfor simple extraction of DNA for PCR-based typing from forensic material.Biotechniques 10:506–513.
41. Wartha, F., K. Beiter, S. Normark, and B. Henriques-Normark. 2007. Neu-trophil extracellular traps: casting the NET over pathogenesis. Curr. Opin.Microbiol. 10:52–56.
42. Whiley, R. A., and D. Beighton. 1991. Emended descriptions and recognitionof Streptococcus constellatus, Streptococcus intermedius, and Streptococcusanginosus as distinct species. Int. J. Syst. Bacteriol. 41:1–5.
43. Whiley, R. A., L. M. Hall, J. M. Hardie, and D. Beighton. 1999. A study ofsmall-colony, beta-haemolytic, Lancefield group C streptococci within theanginosus group: description of Streptococcus constellatus subsp. pharyngissubsp. nov., associated with the human throat and pharyngitis. Int. J. Syst.Bacteriol. 49(Pt 4):1443–1449.
44. Whiley, R. A., H. Fraser, J. M. Hardie, and D. Beighton. 1990. Phenotypicdifferentiation of Streptococcus intermedius, Streptococcus constellatus, andStreptococcus anginosus strains within the “Streptococcus milleri group.”J. Clin. Microbiol. 28:1497–1501.
45. Winstanley, T. G., J. T. Magee, D. I. Limb, J. M. Hindmarch, R. C. Spencer,R. A. Whiley, D. Beighton, and J. M. Hardie. 1992. A numerical taxonomicstudy of the Streptococcus milleri group based upon conventional phenotypictests and pyrolysis mass spectrometry. J. Med. Microbiol. 36:149–155.
VOL. 48, 2010 STREPTOCOCCUS MILLERI FROM PATIENTS WITH CF 401
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 22
0.89
.52.
216.















![Ludwig's angina and mediastinitis due to Streptococcus milleri ... · Ludwig's angina (LA) is a rapidly spreading cellulitis involving sublingual and submaxillary spaces [1]. Two](https://static.fdocuments.net/doc/165x107/5c83bc6209d3f2bc2b8b4c89/ludwigs-angina-and-mediastinitis-due-to-streptococcus-milleri-ludwigs.jpg)


