1 Bone and Soft-tissue Sarcomas: Epidemiology, Radiology ...
34
1 Bone and Soft-tissue Sarcomas: Epidemiology, Radiology, Pathology and Fundamentals of Surgical Treatment Barry Shmookler, Jacob Bickels, James Jelinek, Paul Sugarbaker and Martin M. Malawer OVERVIEW An understanding of the basic biology and pathology of bone and soft-tissue tumors is essential for appropriate planning of their treatment. This chapter reviews the unique biological behavior of soft-tissue and bone sarcomas, which underlies the basis for their staging, resection, and the use of appropriate adjuvant treatment modalities. A detailed description of the clinical, radiographic, and pathological characteristics for the most common sarcomas is presented. Malawer Chapter 01 21/02/2001 14:56 Page 3
Transcript of 1 Bone and Soft-tissue Sarcomas: Epidemiology, Radiology ...

1
Bone and Soft-tissue Sarcomas:Epidemiology, Radiology,Pathology and Fundamentals ofSurgical Treatment
Barry Shmookler, Jacob Bickels, James Jelinek, PaulSugarbaker and Martin M. Malawer
OVERVIEW
An understanding of the basic biology and pathology of bone and soft-tissue tumors is essential for appropriateplanning of their treatment. This chapter reviews the unique biological behavior of soft-tissue and bone sarcomas,which underlies the basis for their staging, resection, and the use of appropriate adjuvant treatment modalities.A detailed description of the clinical, radiographic, and pathological characteristics for the most commonsarcomas is presented.
Malawer Chapter 01 21/02/2001 14:56 Page 3

BIOLOGY AND NATURAL HISTORY OF BONEAND SOFT-TISSUE TUMORS
Soft-tissue and bone sarcomas are a rare and hetero-geneous group of tumors. Although soft tissues andbone comprise 75% of the average body weight, theseneoplasms represent less than 1% of all adult and 15%of pediatric malignancies. The annual incidence in theUnited States, which remains relatively constant, isapproximately 6000–7000 soft-tissue and 2500 bonesarcomas. Because these lesions are so rare, few pathol-ogists have sufficient experience to deal comfortablywith their diagnosis. This is further compounded bythe steady evolution in the classification of soft-tissueand bone tumors, which is based on their biologicalbehavior, ultrastructure, and results of immunohisto-chemical and cytogenetic studies.
Risk factors for soft-tissue and bone sarcomas includeprevious radiation therapy, exposure to chemicals (e.g.,vinyl chloride, arsenic), immunodeficiency, prior injury(scars, burns), chronic tissue irritation (foreign-bodyimplants, lymphedema), neurofibromatosis, Paget’sdisease, bone infarcts, and genetic cancer syndromes(hereditary retinoblastoma, Li–Fraumeni syndrome,Gardner’s syndrome). In most patients, however, nospecific etiology can be identified.
Sarcomas originate primarily from elements of themesodermal embryonic layer. Soft-tissue sarcomas areclassified according to the adult tissue that they resem-ble. Similarly, bone sarcomas are usually classifiedaccording to the type of matrix production: osteoid-producing sarcomas are classified as osteosarcomas,and chondroid-producing sarcomas are classified aschondrosarcomas. The three most common soft-tissuesarcomas are malignant fibrous histiocytoma (MFH),liposarcoma, and leiomyosarcoma. These tumors areanatomic site-dependent; in the extremities thecommon subtypes are MFH and liposarcoma, whereasliposarcomas and leiomyosarcoma are the commonsubtypes in the retroperitoneum and the abdominalcavity. The most common bone sarcomas are osteo-sarcoma, chondrosarcoma, and Ewing’s sarcoma.
Although soft-tissue sarcomas can arise anywhere inthe body, the lower extremities are the most commonsite. Incidence is as follows: lower extremities – 46%;trunk – 19%; upper extremities – 13%; retroperitoneum– 12%; head and neck – 9%; other locations – 1%. Thepresenting symptoms and signs of soft-tissue sarcomasare nonspecific; they commonly present as a painless,slow-growing mass. Diagnosis of sarcomas involvingthe abdominal and pelvic cavity is subtle; these tumorsmay progress for long periods without causing overtsymptoms. Their location deep within the bodyprecludes palpation of the tumor mass early in thecourse of the disease; consequently, these tumors oftenreach tremendous size prior to diagnosis.
In the past two decades, survival and the quality oflife of patients with soft-tissue and bone sarcomas havedramatically improved as a result of the multimodalitytreatment approach. Surgery, used in combination withchemotherapy and radiation therapy, can achieve curein the majority of patients with soft-tissue and bonesarcomas and resection is performed in lieu ofamputation in more than 90% of all patients. Principlesof chemotherapy and radiation therapy in thetreatment of soft-tissue and bone sarcomas arediscussed in Chapters 3, 4, and 5.
Biological Behavior
Tumors arising in bone and soft tissues have charac-teristic patterns of biological behavior because of theircommon mesenchymal origin and anatomical environ-ment. Those unique patterns form the basis of the stagingsystem and current treatment strategies. Histologically,sarcomas are graded as low, intermediate, or highgrade. The grade is based on tumor morphology, extentof pleomorphism, atypia, mitosis, and necrosis. Itrepresents its biological aggressiveness and correlateswith the likelihood of metastases.
Sarcomas form a solid mass that grows centrifugallywith the periphery of the lesion being the least mature.In contradistinction to the true capsule that surroundsbenign lesions, which is composed of compressednormal cells, sarcomas are generally enclosed by areactive zone, or pseudocapsule. This consists ofcompressed tumor cells and a fibrovascular zone ofreactive tissue with a variable inflammatorycomponent that interacts with the surrounding normaltissues. The thickness of the reactive zone varies withthe histogenic type and grade of malignancy. High-grade sarcomas have a poorly defined reactive zonethat may be locally invaded by the tumor (Figure 1.1).
Musculoskeletal Cancer Surgery4
Figure 1.1 A pseudocapsule of a high-grade soft-tissue sar-coma (arrows). It is composed of compressed tumor cellsand a fibrovascular zone of reactive inflammatory response.
Malawer Chapter 01 21/02/2001 14:56 Page 4

In addition, they may break through the pseudo-capsule to form metastases, termed “skip metastases”,within the same anatomic compartment in which thelesion is located. By definition, these are locoregionalmicrometastases that have not passed through thecirculation (Figure 1.2). This phenomenon may beresponsible for local recurrences that develop in spite ofapparently negative margins after a resection.Although low-grade sarcomas regularly interdigitateinto the reactive zone, they rarely form tumor skipnodules beyond that area.
Sarcomas respect anatomical borders. Local anatomyinfluences tumor growth by setting natural barriers toextension. In general, sarcomas take the path of leastresistance and initially grow within the anatomicalcompartment in which they arose. In a later stage thewalls of that compartment are violated (either thecortex of a bone or aponeurosis of a muscle), and thetumor breaks into a surrounding compartment (Figure1.3). Most bone sarcomas are bicompartmental at the
time of presentation; they destroy the overlying cortexand extend directly into the adjacent soft tissues(Figures 1.4, 1.5). Soft-tissue sarcomas may arisebetween compartments (extracompartmental) or in ananatomical site that is not walled off by anatomicalbarriers such as the intermuscular or subcutaneousplanes. In the latter case they remain extracompart-mental and only in a later stage break into the adjacentcompartment. Carcinomas, on the other hand, directlyinvade the surrounding tissues, irrespective ofcompartmental borders (Figure 1.6).
Bone and Soft-tissue Sarcomas 5
Figure 1.2 High-grade sarcomas may break through the pseudocapsule to form “skip” metastases within the same anatomicalcompartment. They are occasionally found with low-grade sarcomas. Skip nodules are tumor foci not in continuity with themain tumor mass that form outside the pseudocapsule. “Satellite"” nodules, by contrast, form within the pseudocapsule. (A)Multiple satellite nodules (arrows) associated with a high-grade MFH. Note the normal intervening tissue. (B) “Skip” metastases(arrows) from an osteosarcoma of the distal femur. This finding is preoperatively documented in less than 5% of patients.
A
B
Malawer Chapter 01 21/02/2001 14:56 Page 5

Musculoskeletal Cancer Surgery6
A B
Figure 1.3 (A) Sagittal section of a high-grade osteosar-coma of the distal femur. The growth plate, although notinvaded by the tumor in this case, is not considered ananatomical barrier to tumor extension. This is probablybecause of the numerous vascular channels that passthrough the growth plate to the epiphysis. However, thearticular cartilage is an anatomical barrier to tumorextension and very rarely is directly violated by a tumor. (B)Coronal section of a high-grade osteosarcoma of the distalfemur. Although gross involvement of the epiphysis andmedial cortical breakthrough and soft-tissue extension areevident, the articular cartilage is intact. This phenomenonallows intra-articular resection of high-grade sarcomas of thedistal femur in most cases. Thick fascial planes are barriers totumor extension. (C) axial MRI, showing a high-gradeleiomyosarcoma of the vastus lateralis and vastus inter-medius muscles. The tumor does not penetrate (clockwise)the lateral intermuscular septum, adductor compartment,and the aponeuroses of the sartorius and rectus femorismuscles.
C
Malawer Chapter 01 21/02/2001 14:56 Page 6

Joint Involvement
Direct tumor extension through the articular cartilage israre and usually occurs as the result of a pathologicalfracture with seeding of the joint cavity or by peri-capsular extension (Figure 1.7). Occasionally, structuresthat pass through the joint (e.g., the cruciate ligaments)act as a conduit for tumor growth (Figures 1.8, 1.9).Transcapsular skip nodules are demonstrated in 1% ofall osteosarcomas.
Metastatic Pattern
Unlike carcinomas, bone and soft-tissue sarcomasdisseminate almost exclusively through the blood.Hematogenous spread of extremity sarcomas is mani-fested by pulmonary involvement in the early stages
and by bony involvement in later stages (Figure 1.10).Abdominal and pelvic soft-tissue sarcomas, on theother hand, typically metastasize to the liver and lungs.Low-grade soft-tissue sarcomas have a low (< 15%)rate of subsequent metastasis while high-grade lesionshave a significantly higher (> 15%) rate of metastasis.Metastases from sarcomas to regional lymph nodes areinfrequent; the condition is observed in only 13% ofpatients with soft-tissue sarcomas and 7% of bonesarcomas at initial presentation. The prognosisassociated with such an event is similar to that ofdistant metastasis.
Most patients with high-grade primary bonesarcomas, unlike soft-tissue sarcomas, have distantmicrometastases at presentation; an estimated 80% ofpatients with osteosarcomas have micrometastatic lungdisease at the time of diagnosis. For that reason, in most
Bone and Soft-tissue Sarcomas 7
A B
Figure 1.4 (A) Ewing’s sarcoma of the distal two-thirds of the femur, and (B) osteosarcoma of the proximal tibia. Note theextraosseous component of the tumor. Most high-grade bone sarcomas are bicompartmental at the time of presentation (i.e., theyinvolve the bone of origin as well as the adjacent soft tissues). Tumors at that extent are staged as IIB tumors (see staging ofmalignant bone tumors: Enneking’s classification).
Malawer Chapter 01 21/02/2001 14:56 Page 7

cases, cure of a high-grade primary bone sarcoma canbe achieved only with systemic chemotherapy andsurgery. As mentioned, high-grade soft-tissue sarcomashave a smaller metastatic potential. Because of thatdifference in metastatic capability the role of chemo-therapy in the treatment of soft-tissue sarcomas and itsimpact on survival are still a matter of controversy.
STAGING OF MUSCULOSKELETAL TUMORS
Staging is the process of classifying a tumor, especiallya malignant tumor, with respect to its degree ofdifferentiation, as well its local and distant extent, inorder to plan the treatment and estimate the prognosis.Staging allows the surgeon to determine the type andthe extent of the operation that is necessary for aspecific type of tumor in a particular anatomic location,as well as the indication for neoadjuvant treatmentmodalities. Staging of a musculoskeletal tumor is basedon the findings of the physical examination and theresults of imaging studies. Biopsy and histopathologicalevaluation is an essential component of staging, butshould always be the final step. The concept andpractice of biopsy of musculoskeletal tumors isdiscussed in Chapter 2.
Plain radiographs remain the key imaging modalityin the evaluation of bone tumors. Based on medicalhistory, physical examination, and plain radiographs,accurate diagnosis of bone tumors can be made in morethan 80% of cases. Because of the fine trabecular detailrevealed by plain radiographs, bone lesions of theextremities can be detected at a very early stage; lesionsof the spine and pelvis, by contrast, are not diagnoseduntil a large volume of bone has been destroyed. Oncea bone lesion is found, computerized tomography (CT)is the imaging modality of choice to evaluate the extentof bone destruction. Magnetic resonance imaging(MRI) has been proven to be superior to CT in theevaluation of the intramedullary and extraosseous,soft-tissue extent of bone tumors (Figure 1.11).
In their early stages, soft-tissue tumors are hard todetect due to the lack of bone involvement.Occasionally, distortion of fat planes in plain radio-graphs implies the presence of a soft-tissue mass.
CT should be performed on a helical scanner thatenables improved two-dimensional images and three-dimensional reconstruction capability. The field of viewshould be small enough to allow adequate resolution,particularly of the lesion and the adjacent neuro-vascular bundle and muscle groups. The slice thicknessshould be designed in order to allow at least 10–15slices through the tumor. Intravenous contrast dyeshould be employed in the evaluation of soft-tissuetumors unless a clear contraindication for its use exists.On the other hand, contrast dye is of little value in theevaluation of bone tumors.
MRI is a valuable tool in the evaluation of soft-tissuetumors and of the medullary and soft-tissue com-ponents of bone tumors. The signal intensity of a tumoris assessed by comparing it with that of the adjacentsoft tissues, specifically skeletal muscle and subcu-taneous fat. MRI also enables one to view a lesion in allthree planes (axial, sagittal, and coronal). Contrast-
Musculoskeletal Cancer Surgery8
Figure 1.5 Biologic behavior of bone and soft-tissuesarcomas. Unique features are formation of reactive zone,intracompartmental growth, and, rarely, the presence ofskip metastases.
Malawer Chapter 01 21/02/2001 14:56 Page 8

enhanced MRI is useful in evaluating the relationshipof a tumor to the adjacent blood vessels and in charac-terizing cystic lesions. The presence of orthopedichardware or surgical clips is not a contraindication tothe performance of MRI; however, if a lesion isimmediately adjacent to the location of the hardware,the local field may be distorted.
Although the purpose of MRI is to evaluate theanatomical extent of a lesion, it also can accurately diag-nose a variety of soft-tissue tumors, including lipomas,liposarcomas, synovial cysts, pigmented villonodularsynovitis, hemangiomas, and fibromatoses.Hematomas frequently have a characteristic appear-ance in MRI; however, high-grade sarcomas that haveundergone significant intratumoral hemorrhage mayresemble hematomas. For this reason the diagnosis of asimple hematoma should be made cautiously and, onceit is made, close clinical monitoring must be made untilthe condition has been resolved. The general guidelines
regarding narrowing of the field and recommendednumber of slices per tumor are similar to those of CT.
Bone scintigraphy was traditionally used to assessthe medullary extension of a primary bone sarcoma. Asa rule the bone was cut approximately 6 cm proximal tothe margin of the increased uptake. MRI allows moreaccurate determination of the medullary tumor extent;as a result, safer resections in narrower margins can beperformed. Bone scan is currently used to determinethe presence of metastatic and polystotic bone diseaseand the involvement of a bone by an adjacent soft-tissue sarcoma. In addition, the appearance of a bonelesion in the flow and pool phases of a three-phasebone scan reflects its biological activity and may behelpful in its diagnosis. It is also used as an indirectmeans of evaluating tumor response to chemotherapy.
Angiography is essential prior to surgery becausevascular displacement is common in tumors that have alarge extraosseous component. Blood vessels are likely
Bone and Soft-tissue Sarcomas 9
Figure 1.6 (A) Axial MRI, showing metastatic bladder carcinoma to the posterior thigh. (B) Plain radiograph of the proximalfemur revealed direct invasion through the cortical bone with a pathological fracture of the lesser trochanter (arrows). (C) Insurgery, exploration of the sciatic nerve revealed direct tumor involvement with extension under the epineural sheath.
A B
C
Malawer Chapter 01 21/02/2001 14:56 Page 9

to be distorted or, less commonly, directly incorporatedto the tumor mass. Angiography provides informationthat helps the surgeon plan the anatomical approachand gauge the likelihood that a major blood vessel hasto be resected en-bloc with the tumor. It can also detectvascular anomalies (Figure 1.12) and establish patencyof collateral vessels. Proximal femur resection, forexample, frequently necessitates ligation of the profun-dus femoral artery (PFA). A patent superficial femoralartery (SFA) must be documented by angiography priorto surgery, otherwise the extremity will suffer severeischemia following ligation of the PFA. Preoperativeembolization may be useful in preparation for resectionof metastatic vascular carcinomas if an intralesionalprocedure is anticipated. Metastatic hypernephroma isan extreme example of a vascular lesion that may bleedextensively and cause exsanguination upon the execu-tion of an intralesional procedure without priorembolization.
Intra-arterial administration of chemotherapy allowsthe use of another type of information that canobtained from angiographs; reduction in tumorvascularity. As revealed by serial angiographs, suchreduction was shown to be indicative of good responseto preoperative chemotherapy. Figure 1.13 summarizesthe use of the various imaging modalities in the stagingprocess of a primary bone sarcoma.
There is no single universally accepted staging systemfor soft-tissue and bone sarcomas. Some systems arevaluable in the determination of the operative strategy,whereas others may be more useful in the estimation ofthe prognosis. An important variable in any stagingsystem for musculoskeletal tumors, unlike a staging
Musculoskeletal Cancer Surgery10
Figure 1.7 Pericapsular extension of an osteosarcoma of theproximal humerus (arrows).
Figure 1.8 Extension of an osteosarcoma of the distalfemur to the knee joint along the cruciate ligaments (arrowpoints to tumor); the articular cartilage is intact. Knee jointextension of a high-grade sarcoma of the distal femur is arare event, necessitating extra-articular resection (i.e., en-bloc resection of the distal femur, knee joint, and acomponent of the proximal tibia), as shown in this figure.
Figure 1.9 The five major mechanisms of joint involve-ment by a bone sarcoma. The most common mechanismsare pathologic fracture and pericapsular extension.
Malawer Chapter 01 21/02/2001 14:56 Page 10

system for carcinomas, is the grade of the tumor. Thesystem that is most commonly used for the staging ofsoft-tissue sarcomas is that of the American JointCommittee on Cancer (Table 1.1).1 It is based primarilyon the Memorial–Sloan Kettering staging system anddoes not apply to rhabdomyosarcoma. Critics of thissystem point out that it is based largely on single-institution studies that were not subjected to multi-institutional tests of validity. The MusculoskeletalTumor Society adopted staging systems that were
originally described by Enneking et al.,2,3 for malignantsoft-tissue and bone tumors (Table 1.2), and theAmerican Joint Committee on Cancer developed, withfew changes, a staging system for malignant bonetumors (Table 1.3).4
Enneking’s classical staging system is based on threefactors: histological grade (G), site (T), and the presenceor absence of metastases (M). The anatomical site (T)may be either intracompartmental (A) or extracompart-mental (B). This information is obtained preoperativelyon the basis of the data gained from the variousimaging modalities. A tumor is classified asintracompartmental if it is bounded by natural barriersto extension, such as bone, fascia, synovial tissue,periosteum, or cartilage. An extracompartmental tumormay be either a tumor that violated the borders of thecompartment from which it originated, or a tumor thatoriginated and remained in the extracompartmentalspace. A tumor is assigned to stage III (M1) if ametastasis is present at a distant site or in a regionallymph node. It should be emphasized that Enneking’sclassification system is based on clinical data from anera in which chemotherapy was not givenpreoperatively and compartmental resections weremuch more common. Therefore, there was a clearcorrelation between the extent of the tumor atpresentation, its relation to the boundaries of thecompartment in which it is located, and the extent ofsurgery. A close correlation was also found betweensurgical stage of bone sarcoma and patient survival(Figure 1.14). Since that time the use of neoadjuvantchemotherapy was shown to decrease tumor size andfacilitate limb-sparing surgery, as well as reduce thelocal recurrence rate. As a result, compartmentalresections became rare. Nonetheless, Enneking’sclassification is based on the biological behavior of soft-tissue and bone sarcomas, and its underlying concept isas relevant as it was in the early 1980s.
Enneking also described a staging system of benignbone tumors, which remains the one that is mostcommonly used (Table 1.4).2 That system is based on thebiological behavior of these tumors as suggested bytheir clinical manifestation and radiological findings.Benign bone tumors grow in a centrifugal fashion, asdo their malignant counterparts, and a rim of reactivebone is typically formed as a response of the host boneto the tumor. The extent of that reactive rim reflects therate at which the tumor is growing; it is usually thickand well-defined around slowly growing tumors, andbarely detectable around fast-growing, aggressivetumors.
Latent benign bone tumors are classified as stage 1.Such tumors are usually asymptomatic and arecommonly discovered as an incidental radiographicfinding. Their natural history is to grow slowly during
Bone and Soft-tissue Sarcomas 11
Figure 1.10 Lateral plain radiograph of the lumbar spine,showing metastatic high-grade osteosarcoma to the body ofL3 vertebra (arrow).
Malawer Chapter 01 21/02/2001 14:56 Page 11

Musculoskeletal Cancer Surgery12
A B
C
Figure 1.11 Primary lymphoma of the distal femur. Plainradiographs, (A) anteroposterior and (B) lateral views,suggest cortical integrity. This is confirmed by (C) axial CTand (D) MRI, T2-weighted image, which demonstrates theintraosseous extent of the tumor.
D
Malawer Chapter 01 21/02/2001 14:56 Page 12

normal growth of the individual and then to stop and,in most cases, heal spontaneously. These lesions neverbecome malignant and usually heal following simplecurettage. Examples include fibrous cortical defects andnonossifying fibromas (Figure 1.15). Active benignbone tumors are classified as stage 2 lesions. Thesetumors grow progressively but do not violate naturalbarriers. Associated symptoms may occur. Curettageand burr drilling are curative in most cases (Figure1.16). Aggressive benign bone tumors (stage 3) maycause destruction of surrounding bone and usuallybreak through the cortex into the surrounding softtissues. Local control can be achieved only by curettageand meticulous burr drilling with a local adjuvant suchas liquid nitrogen, or by resection of the lesion with a margin of normal tissue (i.e., wide resection) (Figure 1.17).
CLASSIFICATION OF SURGICAL PROCEDURES
There are four basic types of excisions; each is based onthe relationship of the dissection plane to the tumorand its pseudocapsule. An intralesional excision isperformed within the tumor mass and results inremoval of only a portion of it; the pseudocapsule andmacroscopic tumor are left behind. In a marginalexcision, the dissection plane passes through thepseudocapsule of the tumor. Such a resection may leavemicroscopic disease. Wide (en-bloc) excision entailsremoval of the tumor, its pseudocapsule, and a cuff ofnormal tissue peripheral to the tumor in all directions.This is the desired margin for sarcoma resection;however, the adequate thickness of the normal tissuecuff is a matter of controversy. For both soft-tissue and
Bone and Soft-tissue Sarcomas 13
Figure 1.12 Extensive giant-cell tumor of the proximaltibia. Angiography was performed prior to a proximal tibiaresection. It documented an absent peroneal artery. Asuccessful effort was made to preserve the anterior tibialartery during the resection; otherwise, the leg would havebeen dependent on a single vessel.
Table 1.1 System of the American Joint Committee on Cancer for the staging of soft-tissue sarcomas1
Stagea Gradeb Primary tumorc Metastasis in regional lymph nodesd Distant metastasise
IA G1 or G2 T1a or T1b N0 M0IB G1 or G2 T2a N0 M0IIA G1 or G2 T2b N0 M0IIB G3 or G4 T1a or T1b N0 M0IIC G3 or G4 T2a N0 M0III G3 or G4 T2b N0 M0IV Any G Any T N0 or N1 M1
aIA = Low-grade, small, and superficial or deep; IB = low-grade, large, and superficial; IIA = low-grade, largeand deep; IIB = high-grade, small, and superficial or deep; IIC = high grade, large, and superficial; III = high-grade, large, and deep; IV = any with metastasis.bG1 = Well differentiated; G2 = moderately well differentiated; G3 = poorly differentiated; G4 = undifferentiated.cT1 = Tumor is ≤ 5 cm in greatest dimension; T1a = T1 tumor is superficial (lesion does not involve the superficialfascia); T1b = T1 tumor is deep (lesion is deep to or invades the superficial fascia; that is, all intraperitoneal viscerallesions or lesions that invade major vessels or that are located in the thorax, head, or neck); T2 = tumor that is>5 cm in greatest dimension; T2a = T2 tumor is superficial; T2b = T2 tumor is deep.dN0 = No metastasis in regional lymph nodes; N1 = metastasis in regional lymph nodes.eM0 = No distant metastasis; M1 = distant metastasis.
Malawer Chapter 01 21/02/2001 14:56 Page 13

Musculoskeletal Cancer Surgery14
Figure 1.13 Relationship of the various imaging modalities to the different components of a bone sarcoma. Plain radiographs assessbony involvement and cortical breakdown. CT determines the exact extent of bone destruction and MRI determines the medullaryand extraosseous components of the tumor. Bone scan evaluates the cortical and intraosseous extents of the tumor, as well as thepresence of metastatic bone disease. Angiography reveals the anatomic relation of the tumor to the major blood vessels.
% S
UR
VIV
AL
X 1
02
100
80
60
40
20
1 2 3 4 5YEARS
I AI B
II A
II B
III
A
Bone SarcomaN = 219
Figure 1.14 Survival by Enneking’s surgical stage of 219patients with primary bone sarcoma.
Table 1.2 System of Enneking et al.2,3 for staging of soft-tissue and bone sarcomas
Stage Gradea Siteb Metastasisc
IA G1 T1 M0IB G1 T2 M0IIA G2 T1 M0IIB G2 T2 M0III G1 or G2 T1 or T2 M1
aG1 = Low grade; G2 = high grade.bT1 = Intracompartmental; T2 = extracompartmental.cM0 = No regional or distant metastasis; M1 = regional or distalmetastasis.
Malawer Chapter 01 21/02/2001 14:56 Page 14

Bone and Soft-tissue Sarcomas 15
Figure 1.15 Nonossifying fibroma (NOF) of the distalfemur (arrow). As in most cases of NOF, the lesion wasasymptomatic and the plain radiographs were orderedbecause of a trauma to the knee.
Figure 1.16 (see above right and bottom right) Aneurysmalbone cyst of the distal tibia as seen by plain radiographs, (A)anteroposterior and (B) lateral views.
A
B
Malawer Chapter 01 21/02/2001 14:56 Page 15
Musculoskeletal Cancer Surgery16
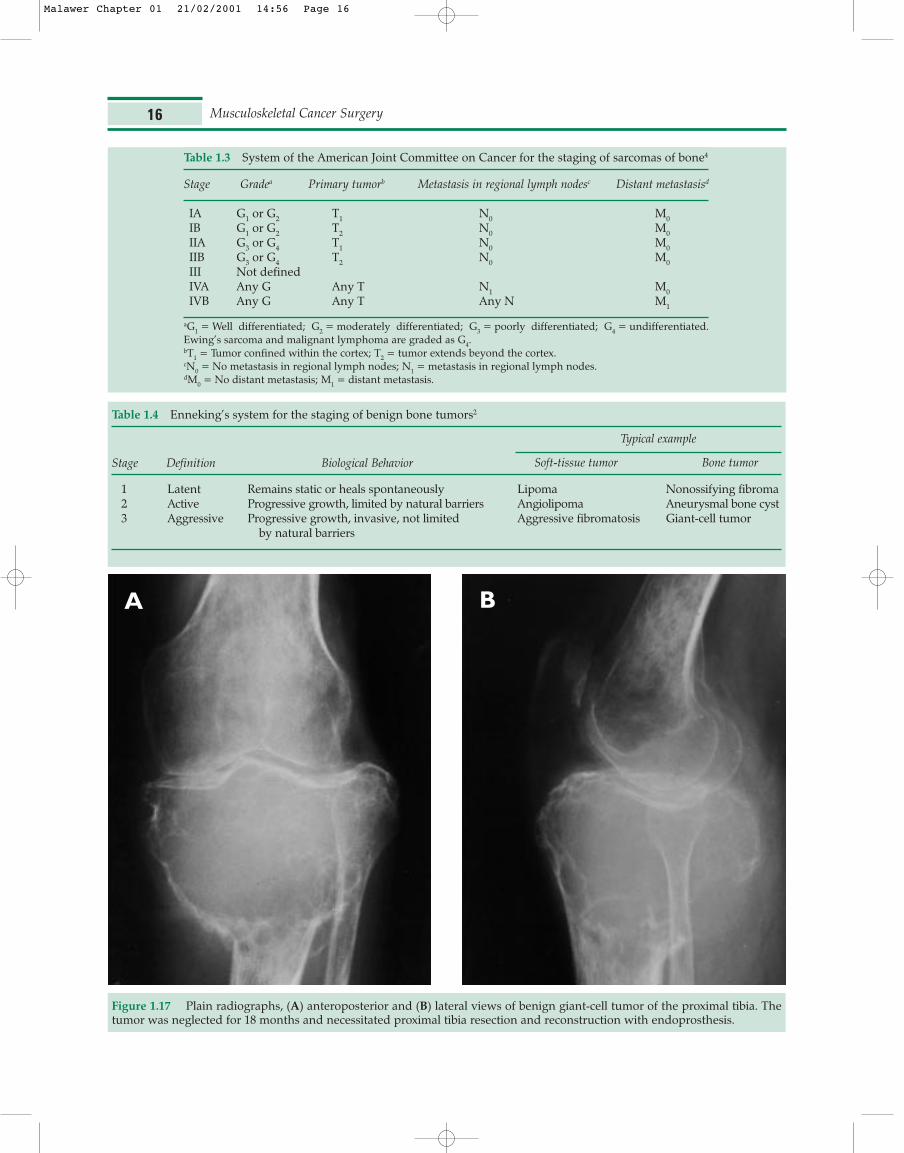
Table 1.3 System of the American Joint Committee on Cancer for the staging of sarcomas of bone4
Stage Gradea Primary tumorb Metastasis in regional lymph nodesc Distant metastasisd
IA G1 or G2 T1 N0 M0IB G1 or G2 T2 N0 M0IIA G3 or G4 T1 N0 M0IIB G3 or G4 T2 N0 M0III Not definedIVA Any G Any T N1 M0IVB Any G Any T Any N M1
aG1 = Well differentiated; G2 = moderately differentiated; G3 = poorly differentiated; G4 = undifferentiated.Ewing’s sarcoma and malignant lymphoma are graded as G4.bT1 = Tumor confined within the cortex; T2 = tumor extends beyond the cortex.cN0 = No metastasis in regional lymph nodes; N1 = metastasis in regional lymph nodes.dM0 = No distant metastasis; M1 = distant metastasis.
Table 1.4 Enneking’s system for the staging of benign bone tumors2
Stage Definition Biological Behavior
Typical example
Soft-tissue tumor Bone tumor
1 Latent Remains static or heals spontaneously Lipoma Nonossifying fibroma2 Active Progressive growth, limited by natural barriers Angiolipoma Aneurysmal bone cyst3 Aggressive Progressive growth, invasive, not limited Aggressive fibromatosis Giant-cell tumor
by natural barriers
Figure 1.17 Plain radiographs, (A) anteroposterior and (B) lateral views of benign giant-cell tumor of the proximal tibia. Thetumor was neglected for 18 months and necessitated proximal tibia resection and reconstruction with endoprosthesis.
A B
Malawer Chapter 01 21/02/2001 14:56 Page 16

bone sarcomas, it is generally believed to be a fewcentimeters.
Radical excision involves removal of the tumor andthe entire anatomical compartment within which it islocated (Figures 1.18, 1.19). Although traditionallymentioned as the fourth excision type, it does not definethe component of the tumor that is left behind. In otherwords, a radical excision can achieve a marginal or awide margin, depending on how close the tumor is tothe border of the compartment. However, radicalexcision excludes the possibility of skip metastases.
In general, benign bone tumors are adequatelytreated by either an intralesional procedure (curettageand burr drilling, cryosurgery) or by marginal excision.Primary bone sarcomas are treated with wide excision.Metastatic tumors are treated according to the generalintent of the surgery. When a palliative surgery isperformed, metastatic lesions are treated by an
intralesional procedure. If a curative procedure isperformed, as in the case of solitary breast metastasis,for example, the lesion is treated as if it was a primarybone sarcoma (i.e., wide excision). It is important toemphasize that any of these excision types may beaccomplished by a limb-sparing procedure or by ampu-tation. An amputation is not necessarily an adequatecancer operation, but it is a method of achieving aspecific margin. It may entail a marginal, wide, or radi-cal excision, depending upon the plane in which it passes.Staging studies are used to assess local tumor extentand relevant local anatomy, and thereby determinehow a desired surgical margin may be achieved.
SOFT-TISSUE SARCOMAS
Soft-tissue sarcomas are a heterogeneous group of raretumors that arise from the supporting extraskeletal
Bone and Soft-tissue Sarcomas 17
Figure 1.18 Various excision types for soft-tissue sarcoma. Figure 1.19 Various excision types for bone sarcoma.
Malawer Chapter 01 21/02/2001 14:57 Page 17
tissues (i.e., muscle, fascia, nerve, connective, fibrous,and fatty tissues). Although they share biologicalcharacteristics, and are treated in a similar fashion, eachof the various soft-tissue sarcomas has a unique mor-phology, biological behavior, and prognosis. Pathologicgrading is at times difficult. In general, the extent ofpleomorphism, atypia, mitosis, and necrosis correlateswith the grade of malignancy. Notable exceptions aresynovial sarcomas, which tend to behave like high-grade lesions even in the absence of histopathologicalhigh-grade characteristics. The exact histogenesis oftencannot be accurately defined, although the grade canbe determined.
Pathologic Characteristics of Specific Soft-tissueSarcomas
Malignant Fibrous Histiocytoma
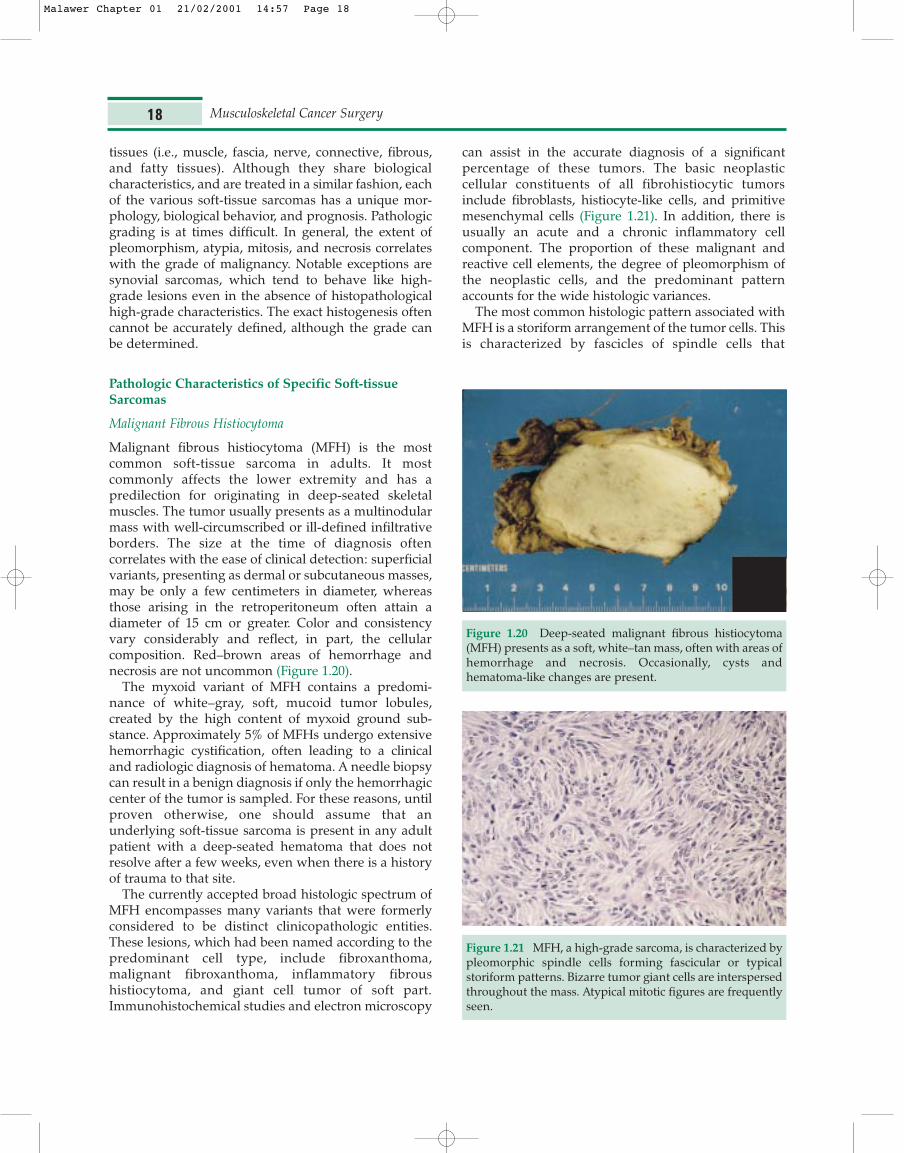
Malignant fibrous histiocytoma (MFH) is the mostcommon soft-tissue sarcoma in adults. It mostcommonly affects the lower extremity and has apredilection for originating in deep-seated skeletalmuscles. The tumor usually presents as a multinodularmass with well-circumscribed or ill-defined infiltrativeborders. The size at the time of diagnosis oftencorrelates with the ease of clinical detection: superficialvariants, presenting as dermal or subcutaneous masses,may be only a few centimeters in diameter, whereasthose arising in the retroperitoneum often attain adiameter of 15 cm or greater. Color and consistencyvary considerably and reflect, in part, the cellularcomposition. Red–brown areas of hemorrhage andnecrosis are not uncommon (Figure 1.20).
The myxoid variant of MFH contains a predomi-nance of white–gray, soft, mucoid tumor lobules,created by the high content of myxoid ground sub-stance. Approximately 5% of MFHs undergo extensivehemorrhagic cystification, often leading to a clinicaland radiologic diagnosis of hematoma. A needle biopsycan result in a benign diagnosis if only the hemorrhagiccenter of the tumor is sampled. For these reasons, untilproven otherwise, one should assume that anunderlying soft-tissue sarcoma is present in any adultpatient with a deep-seated hematoma that does notresolve after a few weeks, even when there is a historyof trauma to that site.
The currently accepted broad histologic spectrum ofMFH encompasses many variants that were formerlyconsidered to be distinct clinicopathologic entities.These lesions, which had been named according to thepredominant cell type, include fibroxanthoma,malignant fibroxanthoma, inflammatory fibroushistiocytoma, and giant cell tumor of soft part.Immunohistochemical studies and electron microscopy
can assist in the accurate diagnosis of a significantpercentage of these tumors. The basic neoplasticcellular constituents of all fibrohistiocytic tumorsinclude fibroblasts, histiocyte-like cells, and primitivemesenchymal cells (Figure 1.21). In addition, there isusually an acute and a chronic inflammatory cellcomponent. The proportion of these malignant andreactive cell elements, the degree of pleomorphism ofthe neoplastic cells, and the predominant patternaccounts for the wide histologic variances.
The most common histologic pattern associated withMFH is a storiform arrangement of the tumor cells. Thisis characterized by fascicles of spindle cells that
Musculoskeletal Cancer Surgery18
Figure 1.20 Deep-seated malignant fibrous histiocytoma(MFH) presents as a soft, white–tan mass, often with areas ofhemorrhage and necrosis. Occasionally, cysts andhematoma-like changes are present.
Figure 1.21 MFH, a high-grade sarcoma, is characterized bypleomorphic spindle cells forming fascicular or typicalstoriform patterns. Bizarre tumor giant cells are interspersedthroughout the mass. Atypical mitotic figures are frequentlyseen.
Malawer Chapter 01 21/02/2001 14:57 Page 18
intersect to form a pinwheel or cartwheel pattern(Figure 1.21). Atypical and bizarre giant cells, oftencontaining abnormal mitotic figures, may occur. Thehistologic grade (almost always intermediate to high) isa good prognosticator of metastatic disease. In themyxoid variant, the second most common histologictype, the tumor cells are dispersed in a richly myxoidmatrix (Figure 1.22). The less common giant cell type(malignant giant cell of soft parts) is characterized byabundant osteoclast-like giant cells that are diffuselydistributed among the malignant fibrohistiocyticelements. Myxoid MFH has a more favorable prognosisthan other subtypes.
Liposarcoma
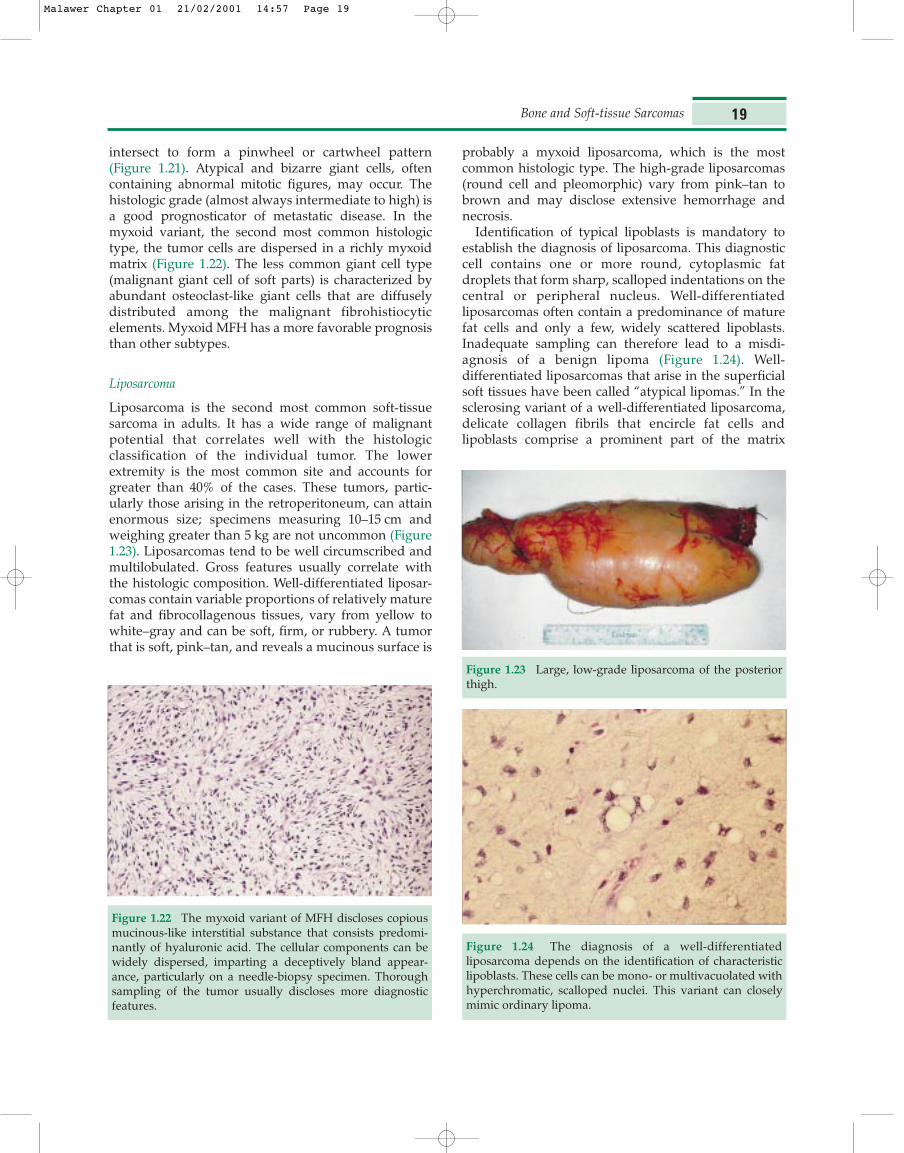
Liposarcoma is the second most common soft-tissuesarcoma in adults. It has a wide range of malignantpotential that correlates well with the histologicclassification of the individual tumor. The lowerextremity is the most common site and accounts forgreater than 40% of the cases. These tumors, partic-ularly those arising in the retroperitoneum, can attainenormous size; specimens measuring 10–15 cm andweighing greater than 5 kg are not uncommon (Figure1.23). Liposarcomas tend to be well circumscribed andmultilobulated. Gross features usually correlate withthe histologic composition. Well-differentiated liposar-comas contain variable proportions of relatively maturefat and fibrocollagenous tissues, vary from yellow towhite–gray and can be soft, firm, or rubbery. A tumorthat is soft, pink–tan, and reveals a mucinous surface is
probably a myxoid liposarcoma, which is the mostcommon histologic type. The high-grade liposarcomas(round cell and pleomorphic) vary from pink–tan tobrown and may disclose extensive hemorrhage andnecrosis.
Identification of typical lipoblasts is mandatory toestablish the diagnosis of liposarcoma. This diagnosticcell contains one or more round, cytoplasmic fatdroplets that form sharp, scalloped indentations on thecentral or peripheral nucleus. Well-differentiatedliposarcomas often contain a predominance of maturefat cells and only a few, widely scattered lipoblasts.Inadequate sampling can therefore lead to a misdi-agnosis of a benign lipoma (Figure 1.24). Well-differentiated liposarcomas that arise in the superficialsoft tissues have been called “atypical lipomas.” In thesclerosing variant of a well-differentiated liposarcoma,delicate collagen fibrils that encircle fat cells andlipoblasts comprise a prominent part of the matrix
Bone and Soft-tissue Sarcomas 19
Figure 1.22 The myxoid variant of MFH discloses copiousmucinous-like interstitial substance that consists predomi-nantly of hyaluronic acid. The cellular components can bewidely dispersed, imparting a deceptively bland appear-ance, particularly on a needle-biopsy specimen. Thoroughsampling of the tumor usually discloses more diagnosticfeatures.
Figure 1.23 Large, low-grade liposarcoma of the posteriorthigh.
Figure 1.24 The diagnosis of a well-differentiatedliposarcoma depends on the identification of characteristiclipoblasts. These cells can be mono- or multivacuolated withhyperchromatic, scalloped nuclei. This variant can closelymimic ordinary lipoma.
Malawer Chapter 01 21/02/2001 14:57 Page 19

(Figure 1.25). In rare cases, well-differentiated liposar-comas, usually after multiple local recurrences,transform into a high-grade spindle-cell sarcoma, oftenwith MFH-like features (“dedifferentiated liposar-coma”). This change imparts a high risk of metastases.
A diagnosis of myxoid liposarcoma requires theobservation of a delicate plexiform capillary networkassociated with both primitive mesenchyme-like cellsand a variable number of lipoblasts (Figure 1.26). Thestroma contains a high proportion of myxoid groundsubstance that may form numerous microcysts. Inround-cell liposarcomas, the lipoblasts are interspersedwithin sheets of poorly differentiated round cells(Figure 1.27). There is convincing evidence that myxoidand round-cell liposarcomas are the divergent ends ofa continuous spectrum of the same neoplasm. This issupported by the fact that both tumors have the same
chromosomal translocation. Finally, pleomorphicliposarcoma discloses a mixture of bizarre, oftenmultivacuolated, lipoblasts and atypical stromal cells,many of which contain abnormal mitotic figures(Figure 1.28). Areas of necrosis and hemorrhage arecommon. The presence of lipoblasts distinguishes thishigh-grade sarcoma from MFH and other pleomorphicsarcomas.
Unlike other soft-tissue sarcomas, liposarcomas maybe multiple and occur in unusual sites in the sameindividual. Therefore, careful evaluation of othermasses in a patient with a liposarcoma is mandatory.Accurate determination of the morphologic subtypeand its grade is essential. Low-grade liposarcomas are
Musculoskeletal Cancer Surgery20
Figure 1.25 The sclerosing variant of well-differentiatedliposarcoma contains a background of coarse wavy collagenfibers. The lipoblasts are dispersed among these fibers.
Figure 1.26 Lipoblasts associated with a plexiform capillarynetwork in a diffusely myxoid stroma define the myxoidliposarcoma. Cyst-like areas are occasionally present.
Figure 1.27 Sheets of round blue cells with clear toeosinophilic cytoplasm are typical of round-cell liposarcoma,a high-grade neoplasm. It has the identical chromosomalabnormality found in myxoid liposarcoma, evidence thatthese are morphologic variants of the same tumor.
Figure 1.28 The pleomorphic liposarcoma is another high-grade form of lipomatous malignancy. It is characterized bynumerous large, bizarre lipoblasts, abnormal mitotic figures,and necrosis. Many of its features overlap with malignantfibrous histiocytoma.
Malawer Chapter 01 21/02/2001 14:57 Page 20

treated with wide excision and adjuvant radiation ther-apy is recommended only if marginal margins wereachieved. The authors treat high-grade liposarcomas asany other high-grade soft tissue sarcoma; neoadjuvantchemotherapy, wide excision, and adjuvant chemo-therapy. Radiation therapy is indicated if wide marginswere not achieved. The role of chemotherapy andradiation therapy in the treatment of soft tissue isdiscussed in Chapters 3 and 5, respectively.
Fibrosarcoma
Fibrosarcoma used to be considered the most commonsoft-tissue sarcoma. Following the histopathologic defi-nition of MFH as a distinct entity and the subsequentassignment of “pleomorphic fibrosarcoma” to thatcategory, fibrosarcoma has become uncommon. Fibro-sarcomas usually arise from the fascial and aponeuroticstructures of the deep soft tissues. Superficial variantsare rare. Relatively small tumors present as firm,gray–white, partially to completely circumscribedmasses (Figure 1.29). As these lesions enlarge, a morediffusely infiltrative pattern predominates.
The fundamental cell of this neoplasm is thefibroblast, which is a spindle cell capable of producingcollagen fibers. The collagen matrix, appearing asbirefringent wavy fibers, can be easily recognized in themore differentiated fibrosarcomas (Figure 1.30). Itspresence can be confirmed with the application ofMasson trichrome stain. Well-differentiated fibrosar-coma is characterized by intersecting fascicles ofrelatively uniform spindle cells showing minimalatypical features and sparse mitotic figures. Thefascicles often intersect at acute angles to form thetypical herringbone pattern. Differentiating low-grade
fibrosarcomas from fibromatosis and its variants maybe difficult. In contrast, poorly differentiatedfibrosarcoma reveals a barely discernible fasciculararrangement. The smaller cells show significantpleomorphism, nuclear atypia, and often have a highmitotic rate. Necrosis and hemorrhage commonlyoccur in high-grade fibrosarcomas. In this situation,particularly in the presence of pleomorphic tumor cells,distinguishing fibrosarcoma from MFH is exceedinglydifficult.
Synovial Sarcoma
Synovial sarcoma ranks as the fourth most commonsoft-tissue sarcoma. In spite of its name, this tumorrarely arises directly from a joint but rather arises inproximity to it with a propensity for the distal portionof the extremities. Synovial sarcomas occur in ayounger age group than do most other sarcomas: mostpatients are below the age of 40. The tumor typicallypresents as a deep-seated, well-circumscribed, multi-nodular, firm mass. Contiguity with a synovium-linedspace is rare and, occasionally, lymphatic spread occurs.Unlike most soft-tissue sarcomas, synovial sarcomasmay be present as a painless mass for a few years. Plainradiographs often show small calcifications within themass. That finding should alert the physician to thediagnosis.
Virtually all synovial sarcomas are high-grade. Thepoorly differentiated neoplasms usually present as ill-defined, infiltrative lesions with a soft, somewhatgelatinous consistency. The classic histologic presenta-tion of this tumor is a biphasic pattern. This implies thepresence of coexisting but distinct cell populations,namely, spindle cells and epithelioid cells (Figure 1.31).
Bone and Soft-tissue Sarcomas 21
Figure 1.29 The gross appearance of a well-differentiatedfibrosarcoma is that of a white–gray whorled nodules. It hasa firm rubbery consistency.
Figure 1.30 Low-grade fibrosarcoma is composed ofslender, relatively uniform spindle cells forming elongatedfascicles. These nodules often intersect at acute anglesforming the typical herringbone pattern.
Malawer Chapter 01 21/02/2001 14:57 Page 21

The plump spindle cells, usually the predominantcomponent, form an interlacing fascicular pattern thatis reminiscent of fibrosarcoma. Within the spindle-cellportion of the tumor, areas resembling the acutelybranching vascular pattern of hemangiopericytoma arecommon. The arrangement of epithelioid cells variesfrom merely solid nests to distinct, gland-like structures(Figure 1.32). When comprising glandular spaces theconstituent cells range from cuboidal to tall columnar;rarely do they undergo squamous metaplasia. Theapplication of histochemical stains demonstrates thatthe glandular lamina contain epithelial-type acidmucins. The neoplasm may contain extensive areas ofdense stromal hyalinization, and focal calcification iscommon. The presence of extensive areas of calci-fication, sometimes with modulation to benign osteoid,deserves recognition because this rare variant imparts asignificantly more favorable prognosis than otherforms of synovial sarcoma. The existence of a mono-phasic spindle cell synovial sarcoma has been recognized,although distinguishing it from fibrosarcoma can bedifficult. In contrast to fibrosarcoma, the spindle cellvariant of synovial sarcoma may contain cytokeratins,as demonstrated with immunohistochemical studies.
PATHOLOGIC CHARACTERISTICS OF SPECIFICPRIMARY BONE SARCOMAS
Osteosarcoma
Osteosarcoma is the most common primary bonesarcoma. Its distinguishing characteristic is the produc-tion of “tumor” osteoid or immature bone matrix.Osteosarcoma typically occurs during childhood and
adolescence. In patients over the age of 40 it is usuallyassociated with a pre-existent condition such as Paget’sdisease or irradiated bone. Between 80% and 90% ofthe tumors occur in the metaphysis of long bone withthe most common sites being the distal femur, proximaltibia, and proximal humerus. Pain, accompanied by atender, soft tissue swelling, is the most commoncomplaint.
The classical radiologic appearance is a destructivetumor with increased intramedullary radiodensity, anarea of radiolucency, and a pattern of permeativeinvasion of the surrounding bone with poorly definedborders, cortical destruction, periosteal elevation, extra-osseous extension, and soft-tissue calcification. On thebasis of radiological presentation, osteosarcomas areclassified into three broad categories: sclerotic osteo-sarcomas (30%), osteolytic osteosarcomas (25%), andmixed pattern (45%) (Figure 1.33). The differentialdiagnosis of this tumor includes giant-cell tumor,aneurysmal bone cyst, fibrosarcoma, and MFH of bone.Errors in diagnosis most often occur with pureosteolytic osteosarcoma.
As the neoplasm permeates the cortex, theperiosteum may be elevated. This stimulates reactivebone formation and accounts for a distinctive radio-logic feature called “Codman’s triangle”. Longitudinalsectioning of the involved bone often reveals wideextension within the marrow cavity. Rarely, skip areaswithin the medullary canal can be demonstrated. Theremay be necrotic and hemorrhagic foci. At the time ofdiagnosis, most tumors have already caused substantialcortical destruction. Continued tumor growth results ininvolvement of the adjacent soft tissues (Figure 1.34).
The definitive diagnosis of osteosarcoma rests on theidentification of a malignant stroma that produces anosteoid matrix. The stroma consists of a haphazard
Musculoskeletal Cancer Surgery22
Figure 1.31 Synovial sarcoma is characterized by adistinctive biphasic pattern. This implies an admixture ofspindle-cell areas along with epithelioid cells forming gland-like structures. The proportion of these two components isvariable.
Figure 1.32 When only one of the elements of synovialsarcoma is present, almost invariably the spindle-cellcomponent, it is termed monophasic synovial sarcoma.
Malawer Chapter 01 21/02/2001 14:57 Page 22

arrangement of pleomorphic cells that contain hyper-chromatic and irregular nuclei. Mitotic figures, oftenatypical, are usually numerous. Deposited betweenthese cells is a lace-like eosinophilic matrix that isassumed to be malignant osteoid (Figure 1.35). Bothmalignant and benign osteoblast-like giant cells can befound in the stroma. An abundance of the latter typecan create confusion with giant-cell tumor of bone. Thepredominance of one tissue type in many osteosar-comas has led to a histologic subclassification of thisneoplasm. Thus, “osteoblastic osteosarcoma” refers tothose tumors in which the production of malignantosteoid prevails. The pattern is usually that of a delicatemeshwork of osteoid, as noted above, although broaderconfluent areas may be present. Calcification of thematrix is variable. Alternatively, some tumors reveal a
Bone and Soft-tissue Sarcomas 23
Figure 1.33 The three radiographic matrix types of osteosar-coma: (A) osteolytic (arrows indicate tumor), (B) mixed, and(C) sclerosing. There is no prognostic difference in survivalbased on the radiographic type of matrix formation.
A B
C
Malawer Chapter 01 21/02/2001 14:57 Page 23

predominance of malignant cartilage production;hence, the term “chondroblastic osteosarcoma”. Eventhough the malignant cartilaginous elements may beoverwhelming, the presence of a malignant osteoidmatrix warrants the diagnosis of osteosarcoma. Anothervariant, fibroblastic osteosarcoma, is characterized bylarge areas of proliferating fibroblasts arranged inintersecting fascicles. Such areas are indistinguishablefrom fibrosarcomas, and thorough sampling may benecessary to identify the malignant osteoid component.The so-called telangiectatic osteosarcoma containsmultiple blood-filled cystic and sinusoidal spaces ofvariable size. Identification of marked cytologic atypiain the septae and more solid areas rule out thediagnosis of aneurysmal bone cyst.
Variants of Osteosarcoma
There are 11 recognizable variants of osteosarcoma,with parosteal and periosteal osteosarcomas being themost common. In contrast to the classical osteosarcoma,which arises within bone, parosteal and periostealosteosarcomas arise in the surface of the bone.
Parosteal Osteosarcoma
Parosteal osteosarcoma is a distinct variant of osteo-sarcoma. Its prevalence is estimated to be 4%. It arisesfrom the cortical bone and generally occurs in an olderage group and has a better overall prognosis thanosteosarcoma. As in osteosarcoma, the distal femur isthe most common location; characteristically, the tumorattached to its posterior aspect. The proximal humerusand the proximal tibia are the next most frequent sites.Parosteal osteosarcomas usually present as a mass,occasionally associated with pain. The natural history isslow growth and late metastasis. The long-termsurvival rate is 75% to 85%. The tumor arises from thecortical surface and presents as a protuberantmultinodular mass. The surface of the lesion may becovered in part by a cartilaginous cap resembling anosteochondroma; other areas may infiltrate into theadjacent soft tissues. The tumor usually encircles,partially or completely, the shaft of the underlyingbone. In contrast to osteochondromas, the medullarycanal of the bone is not contiguous with that of theneoplasm. Radiologically, parosteal osteosarcomapresents as a large, dense, tabulated mass that isbroadly attached to the underlying bone without
Musculoskeletal Cancer Surgery24
Figure 1.34 High-grade osteosarcoma of the proximalhumerus with cortical breakthrough and tumor extensioninto the soft tissues.
Figure 1.35 Classical high-grade osteosarcoma reveals apopulation of pleomorphic spindle cells intimately asso-ciated with a mesh of immature lacy osteoid. Occasionallythe amount of osteoid can be minimal, or it may be apredominant element forming wide intersecting trabeculaelined by the malignant osteoblasts. Giant cells can also bepresent.
Malawer Chapter 01 21/02/2001 14:57 Page 24

involvement of the medullary canal (Figure 1.36). Ifpresent long enough, the tumor may encircle the entirebone. The periphery of the lesion is typically lessmature than the base. Despite careful evaluation,intramedullary extension is difficult to determine fromthe plain radiographs. It is more accurately detectedwith CT scan (Figure 1.37).
Diagnosis of parosteal osteosarcoma, more than thatof other bone tumors, must be based on the clinical,radiological, and pathological findings. Most parostealosteosarcomas are low-grade; they do not requireneoadjuvant and adjuvant chemotherapy, and are besttreated with wide excision. This tumor is commonlymistaken by inexperienced clinicians and pathologistsas osteochondroma, myositis ossificans, or conven-tional osteosarcoma. In the classical low-grade lesion,irregularly formed osteoid trabeculae, usually of wovenbone, are surrounded by a spindle-cell stromacontaining widely spaced, bland-appearing fibroblasticspindle cells (Figure 1.38). There may be foci of atypical
chondroid differentiation. With the higher grades thelikelihood of intramedullary involvement is increased.This, in turn, correlates well with the presence ofdistant metastases.
Periosteal Osteosarcoma
Periosteal osteosarcoma is a rare cortical variant ofosteosarcoma that arises superficially on the cortex,most often on the tibial shaft. It projects into theadjacent soft tissues as a well-circumscribed tabulatedmass. Radiologically, it is a small, radiolucent lesionwith some evidence of bone spiculation. The cortex ischaracteristically intact with scooped-out appearanceand a Codman’s triangle (Figure 1.39). On section, thetumor reveals a dominant chondroid consistency. Thehistologic features are essentially those of intermediate-grade chondroblastic osteosarcoma. The cartilaginouslobules may contain markedly atypical chondrocytes.At the periphery of the lobule is situated a cellular
Bone and Soft-tissue Sarcomas 25
Figure 1.36 Parosteal osteosarcoma. Plain radiographs of the distal femur, (A) anteroposterior and (B) lateral views, show adense, irregular, sclerotic lesion, attached to the posterior femoral cortex. The posterior aspect of the distal femur is a classicallocation for parosteal osteosarcomas and that diagnosis should be considered for any sclerotic lesion in that location.
A B
Malawer Chapter 01 21/02/2001 14:57 Page 25

Musculoskeletal Cancer Surgery26
Figure 1.37 (A) The relation of parosteal osteosarcoma tothe medullary canal is better viewed on CT that shows notumor extension to the canal. In contrast to osteochondro-mas, the medullary canal of the bone is not contiguous withthat of the tumor. (B) Surgical specimen, (C) illuminatedwith tetracycline fluorescence, demonstrates minimalmedullary tumor extension through the posterior cortex.Medullary extension of parosteal osteosarcomas has noimpact on survival; however, the extent of surgical resectionmust be changed to achieve wide margins.
A
B
C
Malawer Chapter 01 21/02/2001 14:57 Page 26

spindle-cell component wherein a fine intercellularosteoid matrix is produced. Areas of malignant osteoidand chondroid can be seen to infiltrate into the corticalbone at the base of the neoplasm.
Small-cell Osteosarcoma
In small-cell osteosarcoma the neoplastic cells areround rather than spindle-shaped. The tumor consistsof nests and sheets of small round cells separated byfibrous septae, a pattern reminiscent of Ewing’ssarcoma. Occasionally, transition to spindle cells isnoted. The cells have well-defined borders and adistinct rim of cytoplasm. The round nuclei disclose adelicate chromatin pattern. The presence of a charac-teristic lace-like osteoid matrix, often surroundingindividual or small nests of cells, confirms the diagnosis(Figure 1.40). The recommendations for treatment vary.Radiation and chemotherapy are used at some insti-tutions while others choose primary surgical ablationwith neoadjuvant and/or adjuvant chemotherapy. Toofew cases have been reported to make definitiverecommendations.
Chondrosarcoma
Chondrosarcoma is the second most common primarybone sarcoma. It is a heterogeneous group of tumorswhose basic neoplastic tissue is cartilaginous andshows no evidence of primary osteoid formation. It issubdivided in a variety of ways, including byhistological grade and by whether it is primary or
secondary or peripheral or central. The single mostuseful classification, both in terms of planning thesurgical procedure and determining the prognosis, ishistological grade. There are a few distinct, relativelyrare, histological variants of chondrosarcoma. Theseinclude clear-cell, mesenchymal, and dedifferentiatedchondrosarcoma.
Primary chondrosarcomas are not associated with apre-existing lesion. Secondary chondrosarcomas areassociated with a pre-existing chondroid lesion such as
Bone and Soft-tissue Sarcomas 27
Figure 1.38 Parosteal osteosarcoma belongs to a group ofbone surface sarcomas. It is usually a low-grade neoplasm.There are parallel or intersecting osseous trabeculae thatmay be either lamellar or woven-bone-type matrix. Theintervening fibrocollagenous tissue is composed of bland,widely spaced fibroblastic cells.
Figure 1.39 Periosteal osteosarcoma of the proximalhumerus. Plain radiograph shows a typical “scooped-out”appearance of a cortical lesion (arrows). The center of thelesion has a lytic appearance because of its chondroblasticfeatures.
Figure 1.40 A rare variant of high-grade osteosarcoma is theso-called small-cell type. It is composed of small round bluecells, often with only sparse osteoid matrix to reveal the truediagnosis. Consequently extensive tumor sampling isnecessary to differentiate it from Ewing’s sarcoma,rhabdomyosarcoma, and lymphoma.
Malawer Chapter 01 21/02/2001 14:57 Page 27

enchondroma, osteochondroma, chondroblastoma,chondromyxofibroma, periosteal chondroma, andsynovial chondromatosis (Figures 1.41, 1.42). Centralchondrosarcomas arise from within the medullarycanal, and peripheral chondrosarcomas arise from thesurface of the bone. Primary chondrosarcomas arevirtually always central; secondary chondrosarcomascan be central or peripheral. The treatment andprognosis of primary and central secondarychondrosarcomas are identical, and that distinction ismade only to clarify the underlying pathogenesis.
The majority of the “conventional” chondrosarcomasoccur between the ages of 40 and 60. The most commonsites are the pelvis, femur, and shoulder girdle. Pelvicchondrosarcomas are often large and present withreferred pain to the lower back, sciatic pain, urinarysymptoms from pressure on the bladder neck, unilat-eral swelling of the lower extremity due to iliac veinobstruction, or a painless pelvic mass. Central chondro-sarcomas usually present with pain. Correlation of theclinical, radiographic, and histological data is essentialfor accurate diagnosis and evaluation of the aggres-siveness and metastatic potential of a cartilage tumor.In general, proximal or axial location, skeletal maturity,and pain point toward malignancy. Radiologically,central chondrosarcoma presents as a well-defined lyticlesion with a narrow zone of transition andsurrounding sclerosis with faint calcification or with nosclerotic rim at all (Figure 1.43). Endosteal scalloping isthe key sign of malignancy (Figure 1.44).
Central chondrosarcoma is an expansive lesion thatcommonly causes cortical destruction and subsequentextension to the soft tissues. Typically, the tumor
consists of fused, variably sized nodules that, on cutsection, are composed of white–gray hyaline tissue,areas of calcification and even ossification. There maybe focal myxoid areas (Figure 1.45).
The histological spectrum and the ease of diagnosisvary tremendously. High-grade tumors can be easilyidentified; in contrast, it may be exceedingly difficult todistinguish low-grade tumors from other benigncartilage tumors. When this diagnostic dilemma arises,correlation of the histological features with both the
Musculoskeletal Cancer Surgery28
Figure 1.41 Secondary, low-grade chondrosarcomas,arising from osteochondromas of the (A) proximal humerus,(B) proximal femur, and (C) proximal tibia (arrows point tothe region of the cartilage cap that has undergone malignanttransformation).
A
B
C
Malawer Chapter 01 21/02/2001 14:57 Page 28

clinical setting and the radiographic changes becomesextremely important. Chondrosarcomas are histolog-ically graded as I (low), II (intermediate), or III (high);the majority are grade I or II. Grade I tumors arecharacterized by a slightly increased number ofchondrocytes, set in lobular chondroid matrix. The cellscontain hyperchromatic nuclei, occasionally binucleateforms that show minimal variation in size (Figure 1.46).Areas of markedly increased cellularity with moreprominent pleomorphism and significant nuclearatypia define a grade II tumor. Myxoid matrix changesare indicative of a grade II tumor, or even higher. GradeIII chondrosarcoma, which accounts for approximately10% of all chondrosarcomas, discloses greater cellu-larity, often with spindle-cell areas, and prominentmitotic activity. Areas of myxoid changes are common,and the malignant chondrocytes may contain large,bizarre nuclei (Figure 1.47). Calcification and enchon-dral ossification can be observed in tumors of all grades;however, the presence of unequivocal malignantosteoid production, even in the face of chondrosar-comatous areas, dictates that the tumor be classified asosteosarcoma.
Resection is the treatment of choice for allchondrosarcomas. Low-grade chondrosarcomas orenchondrosarcomas may be treated by intralesionalresection. Curettage, burr drilling, and, in most cases,the use of adjuvant liquid nitrogen should beconsidered. Intermediate- and high-grade chondro-sarcomas, on the other hand, are treated surgically bywide resection. The use of neoadjuvant and adjuvantchemotherapy for chondrosarcomas is controversial.Low- and intermediate-grade chondrosarcomas
respond poorly to chemotherapy. Although there arefew data on the efficacy of chemotherapy in thetreatment of high-grade chondrosarcomas, it should beconsidered in any young patient with a high-gradetumor. Radiation is recommended when anythingother than wide excision is performed for achondrosarcoma of any grade.
Ewing’s Sarcoma
Ewing’s sarcoma is a distinct round-cell sarcoma thatoccurs predominantly in the long bones of skeletallyimmature patients. The tumor is composed of undif-ferentiated, round, mesenchymal cells that are rich inglycogen and typically manifest a unique reciprocalchromosomal translocation, t(11;22)(q24;q12) thatresults in a chimeric protein, EWS/FLI-1. Thistranslocation occurs in approximately 90% of thesetumors. Very few other human tumors exhibit suchconsistent karyotypic alterations, which might play asignificant role in their pathogenesis.
Ewing’s sarcoma is the third most common primarybone sarcoma. It has a significant predilection for theWhite population; it is rare to diagnose Ewing’ssarcoma in a Black patient. The peak incidence is thesecond decade of life. In very young patients, and inpatients over the age of 30, a diagnosis of Ewing’ssarcoma should be questioned, because it occurs sorarely in these age groups. Common differentialdiagnoses include metastatic neuroblastoma and acuteleukemia (in the young age group) and small-cellcarcinoma and large-cell lymphoma (in patients olderthan 30). With the advent of molecular probes and
Bone and Soft-tissue Sarcomas 29
Figure 1.42 Secondary chondrosarcoma arising from the left proximal femur in a patient with multiple hereditaryenchondromatosis. (A) Plain radiograph shows a large, benign-appearing enchondroma arising from the right proximal femurand a large, poorly demarcated cartilage tumor, arising from the left. (B) CT shows a marked difference between the two lesions.The destructive neoplastic tissue has completely replaced the enchondroma on the left, and it is almost fungating through theskin. The patient underwent modified hemipelvectomy and remains disease-free after more than 10 years of follow-up.
A B
Malawer Chapter 01 21/02/2001 14:57 Page 29

Musculoskeletal Cancer Surgery30
Figure 1.43 Plain radiographs of the proximal tibia, (A)anteroposterior and (B) lateral views, show a centralchondrosarcoma (arrows). Macrosections of central chondro-sarcomas of the (C) proximal tibia and (D) proximal femur.
C
D
A B
Malawer Chapter 01 21/02/2001 14:57 Page 30

immunohistochemical stains, differentiation amongthese tumors has become simpler.
Radiologically, Ewing’s sarcoma presents as an ill-defined, permeative or focally moth-eaten, destructiveintramedullary lesion that affects the diaphysis.Ewing’s sarcomas are frequently lytic or have a mixedpattern; however, in approximately 40% of the cases asclerotic appearance is dominant. Ewing’s sarcomas areassociated with a diffuse, irregular, and wavy periostealreaction consisting of multiple parallel layers. That
reaction has been the named “onion-skin appearance”.The large majority of these tumors break through thecortex and have an extensive soft-tissue component(Figure 1.48). Histologically, the small round cells growin solid, densely packed sheets and nests that fill theintertrabecular spaces. They have round, centrallylocated nuclei with indistinct cytoplasmic features. Thenuclear chromatin is granular, and there are usuallyone to three clearly identifiable small- to intermediate-sized nucleoli (Figure 1.49). Often a biphasic pattern issimulated by the presence of “light” and “dark” cells(i.e., cells with an open chromatin structure and cellswith dark condensed nuclei, respectively). The latterrepresent apoptotic tumor cells. The ratio between light
Bone and Soft-tissue Sarcomas 31
Figure 1.44 Plain radiograph of the femoral shaft, showinga central chondrosarcoma, presenting as a well-defined lyticlesion with a sharp transition zone, calcifications, andendosteal scalloping.
Figure 1.45 Cross-section of an intramedullary chondro-sarcoma discloses its lobular architecture and translucent,hyaline-like matrix. Note the characteristic endostealerosions (arrows).
Malawer Chapter 01 21/02/2001 14:57 Page 31

and dark cells varies from tumor to tumor and even indifferent areas of the same lesion.
Ewing’s sarcoma is an extremely malignant tumorwith high rates of metastatic disease and localrecurrence following surgery alone. The 5-year survivalrate has risen dramatically, from 5% to more than 60%,because of the use of multimodality treatment thatincludes chemotherapy, surgery, and radiation therapyin selected cases in which wide margins were not orcould not be achieved at surgery. As with any high-grade primary bone sarcoma, the surgical aim is wideresection.
Giant-cell Tumor of Bone
Giant-cell tumor (GCT) is a locally aggressive tumorwith a low metastatic potential. It occurs slightly moreoften in females than in males. The primary areas ofinvolvement are the femoral condyles, tibial plateau,proximal humerus, and distal radius. The tumor isthought to arise in the metaphyseal–epiphysealjunction. Large tumors may extend into the metaphysisand, more rarely, into the diaphysis. GCT occasionallyoccurs in the vertebrae and sacrum. The descriptor“benign” was first applied to GCT to differentiate itfrom other bony malignancies that required ampu-tation. The quotation marks were gradually removedand GCT is now considered a benign aggressive lesion.This descriptor is misleading, because 3% of GCTs areprimarily malignant or will undergo malignant trans-formation either after radiation therapy or after severallocal recurrences. GCT is, therefore, considered by theauthors to be a low-grade primary bone sarcoma and istreated as such.
Radiologically, GCTs are eccentric lytic lesionswithout matrix formation. They have well-definedborders and a very sharp transition between the tumorand the host bone. Periosteal elevation is rare unless apathological fracture is present (Figure 1.50). Expandedand thinned cortex and, occasionally, corticalbreakthrough and soft-tissue extension are common(Figure 1.51). Histologically, two basic cell typescomprise the typical GCT. The stroma consists ofpolygonal to somewhat spindle cells containing centralround nuclei. Typical mitotic figures, sometimesnumerous, are often noted. Scattered diffuselythroughout the stroma are benign osteoclast-like giantcells (Figure 1.52). Small foci of osteoid matrix,produced by the stromal cells, can be observed.Chondroid matrix never occurs. Extensive hemorrhage,pathologic fracture, or previous surgery can altersignificantly the usual histologic picture of GCT andmake it resemble a primary bone sarcoma. These eventsmust be recognized at the time of histologic interpre-tation in order to prevent diagnostic errors. Cystic areaswith surrounding hemosiderin pigment and xanthomacells correspond to the grossly observed cyst. A malig-nant GCT contains areas of unequivocal sarcomatoustransformation, usually typical of fibrosarcoma orosteosarcoma. The sarcomatous component is devoidof ordinary GCT features; thus, it is only by the recog-nition of foci of residual GCT, or by the confirmation ofpre-existing GCT, that an accurate diagnosis ofmalignant GCT can be established.
Treatment of GCT is surgical removal. During thepast several decades, surgeons have used thefollowing: (1) curettage; (2) curettage and cytotoxicagents such as phenol, zinc chloride, alcohol, H2O2, or
Musculoskeletal Cancer Surgery32
Figure 1.46 Low-grade chondrosarcoma maintains alobular architecture. There is slightly increased cellularity,occasional binucleate cells and nuclear atypia. These cells aretypically found in lacunae. The tumor tends to permeatebetween the normal osseous trabeculae.
Figure 1.47 The juxtaposition of high-grade spindlesarcoma with lobules of low-grade chondrosarcoma is thehallmark of dedifferentiated chondrosarcoma. The spindle-cell component usually reveals features of malignant fibroushistiocytoma, osteosarcoma, or it may be unclassifiable. Thisneoplasm pursues an aggressive clinical course with verylow long-term survival.
Malawer Chapter 01 21/02/2001 14:57 Page 32

carbolic acid; (3) curettage and a physical adjuvant(polymethylmethacrylate and cryosurgery); (4)primary resection; (5) radiation therapy; and (6)embolization, which is practiced in unresectabletumors. Simple curettage, with or without cytotoxicagents, has a significantly high rate of local recurrenceof up to 57%. Treatment of GCT with curettage, burrdrilling, and cryosurgery using application of liquidnitrogen to the tumor cavity has achieved a recurrencerate of less than 3% among patients who wereprimarily treated with that modality. This is among thelowest reported recurrence rate after any surgicalintervention for GCT of bone. Cryosurgery is,therefore, recommended as a physical adjuvant tocurettage in the treatment of GCTs of bone.
Bone and Soft-tissue Sarcomas 33
Figure 1.48 (above and above right) (A) Plain radiograph ofthe proximal femur, showing Ewing’s sarcoma presenting asan ill-defined, permeative, destructive intramedullarydiaphyseal lesion. Extensive periosteal reaction, corticalbreakthrough, and soft-tissue extension are noted. (B)Macrosection of a proximal femur, showing Ewing's sarcomawith medial cortical breakthrough and soft-tissue extension.
A B
Figure 1.49 Ewing’s sarcoma belongs to the ever-expandingcategory of small, round, blue-cell tumors. It is composed of round cells with scanty cytoplasm and round to ovalnuclei. The nuclear chromatin tends to be fine homoge-neous. Differentiation from the other members of theround-cell family may require the use of immuno-histochemistry, electron microscopy, and cytogenetic andoncogene markers.
Malawer Chapter 01 21/02/2001 14:58 Page 33

SUMMARY
The unique biological behavior of soft-tissue and bonesarcomas is reviewed. In addition to serving as the basisfor the various staging systems, biological behaviordictates the surgical planning and the choice ofadjuvant treatment modalities such as chemotherapyand radiation therapy. Although each soft-tissue andbone sarcoma is a distinct clinical and pathologicalentity, the principles of evaluation and managementpresented in this chapter apply to all.
Musculoskeletal Cancer Surgery34
A
BFigure 1.50 GCT of the distal femur. (A) Plain radiographdemonstrating a typical eccentric, osteolytic lesion with athinned cortex without periosteal elevation. There is noevidence of matrix formation. (B) Corresponding T2-weighted image MRI and (C) gross specimen show hemor-rhage with an expanded but intact cortex. The majorradiological differential diagnosis is telangiectatic osteosarc-oma, MFH, or fibrosarcoma of bone.
C
Malawer Chapter 01 21/02/2001 14:58 Page 34

Bone and Soft-tissue Sarcomas 35
Figure 1.51 Macrosection of the proximal femur, showinggiant-cell tumor of bone with medial cortical breakthroughand extension to the surrounding soft-tissues.
Figure 1.52 Giant cell tumor of bone reveals a ratheruniform distribution of osteoclastic giant cells. Thebackground contains round to polygonal histiocytic cells.Normal mitotic figures can be seen. Hemorrhage withaneurysmal bone cyst changes is not unusual.
1. American Joint Committee on Cancer: Soft tissues. In:Fleming ID, Cooper JS, Henson DE, et al., editors. AJCCCancer Staging Manual, Edition 5. Philadelphia:Lippincott-Raven; 1997:149–56.
2. Enneking WF. Staging of muskuloskeletal tumors. In:Enneking WF, editor. Musculoskeletal Tumor Surgery, vol.1. New York: Churchill Livingstone; 1983:87–8.
3. Enneking WF, Spanier SS, Goodman MA. A system for thesurgical staging of musculoskeletal sarcoma. Clin Orthop.1980;153:106–20.
4. American Joint Committee on Cancer: Bone. In: FlemingID, Cooper JS, Henson DE, et al.., editors. AJCC CancerStaging Manual, Edition 5. Philadelphia: Lippincott-Raven, 1997:143–7.
References
Malawer Chapter 01 21/02/2001 14:58 Page 35

Malawer Chapter 01 21/02/2001 14:58 Page 36






![SARCOMAS Corregido[1]](https://static.fdocuments.net/doc/165x107/55721128497959fc0b8e7930/sarcomas-corregido1.jpg)