0616 Immuniz
22
Abdul Ghaffar Microbiology and Immunology
-
Upload
guest08e813 -
Category
Documents
-
view
876 -
download
8
Transcript of 0616 Immuniz

Abdul GhaffarMicrobiology and Immunology

2
Milestones in immunizationMilestones in immunization
1500BC Turks introduce
variolation
3000BC Evidence of sniffing
powdered small pox crust in Egypt
2000BC Sniffing of small
pox crust in China
1700AD Introduction of
variolation in England and later in the US

3
The wife of the British Ambassador in Turkey, in March 1717 wrote, followingthe variolation of her son, to a friend inEngland: “The small pox, so fatal, so general amongst us, is entirely harmless here by the invention of ingrafting….I am patriot enough to bring this invention into fashion in England.
The wife of the British Ambassador in Turkey, in March 1717 wrote, followingthe variolation of her son, to a friend inEngland: “The small pox, so fatal, so general amongst us, is entirely harmless here by the invention of ingrafting….I am patriot enough to bring this invention into fashion in England.
Introduction of variolationIntroduction of variolation

4
Milestones in immunizationMilestones in immunization
1780AD Edward Jenner discovers
small pox vaccine

5
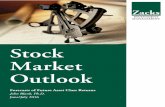
Edward Jenner
Discovery of small pox vaccine

6
Edward JennerAmong patients awaiting small pox vaccination

7
1920sDiphtheria and Tetanus
1934Pertussis
1955Salk polio
Modern era of the vaccineModern era of the vaccine
1885Rabies vaccine (Pasteur)

8
1960sMumps measles and rubella virus
Sabin polio
1990s
Hepatitis and varicella
1985
Haemophilus
Modern era of the vaccineModern era of the vaccine

9
Pre- & post-vaccine incidence of common preventable diseases
Pre- & post-vaccine incidence of common preventable diseases

10
Different modes of acquiring immunity
Different modes of acquiring immunity
Natural resistance
Artificial Natural
Passive
Artificial Natural
Active
Immunity
Acquired

11
Natural Artificial
Colostral transfer of IgA
Placental transfer of IgG
Antibodies or immunoglobulins
Immune cells
Passive ImmunityPassive Immunity

12
disease indicationantibody source
Passive ImmunizationPassive Immunization
human, horsediphtheria, tetanus prophylaxis, therapy
vericella zoster human immunodeficiencies
gas gangrene, botulism, snake bite, scorpion sting
horse post-exposure
rabies, human post-exposure
hypogamma-globulinemia
human prophylaxis

13
Advantages Disadvantages
serum sicknessimmediate protection
no long term protection
graft vs. host disease (cell graft only)
risk of hepatitis and Aids
Advantages and Disadvantages of Passive Immunization
Advantages and Disadvantages of Passive Immunization

14
Active ImmunizationActive Immunization
Natural Artificial
exposure to sub-clinical infections
Attenuated organisms
killed organisms
sub-cellular fragments
toxins
others

15
tuberculosisnot used in this country
polio*not used in std. schedule
measles, mumps & rubella
yellow feverMilitary and travelers
Varicella zosterchildren with no history of chicken pox
hepatitis Anot required in SC
Live Attenuated VaccinesLive Attenuated Vaccines

16
polio
influenzaelderly and at risk
typhoid, cholera, plagueepidemics and travelers
rabiespost exposure
pertussis replaced by the acellular vaccine
Killed Whole-Organism VaccinesKilled Whole-Organism Vaccines
Q feverpopulation at risk

17
Microbial Fragment VaccinesMicrobial Fragment Vaccines
Bordetella. Pertussisvirulence factor protein
Haemophilus influenzae Bprotein conjugated polysaccharide
Streptococcus pneumoniaePolysaccharide mixture
Neisseria meningitidispolysaccharide

18
Microbial Fragment VaccinesMicrobial Fragment Vaccines
Clostridium tetani (tetanus)inactivated toxin (toxoid)
Corynebacterium diphtheriaeinactivated toxin (toxoid)
Vibrio choleraetoxin subunits
Hepatitis B viruscloned in yeast

19
Modification of Toxin to ToxoidModification of Toxin to Toxoid
toxin moiety antigenic determinants
chemical
modification
Toxin Toxoid

20
anti-Idiotype Vaccine
Immuno-dominant peptide
Future VaccinesFuture Vaccines
DNA

21
Recommended Childhood Immunization Schedule

22
Adverse Events OccurringWithin 48 Hours DTP of Vaccination
Adverse Events OccurringWithin 48 Hours DTP of Vaccination
Event Frequencylocalredness, swelling, pain 1 in 2-3 doses
systemic: Mild/moderatefever, drowsiness, fretfulness vomiting anorexia
1 in 2-3 doses
1 in 5-15 doses
systemic: more serious persistent crying, fevercollapse, convulsionsacute encephalopathypermanent neurological deficit
1 in 100-300 doses1 in 1750 doses1 in 100,000 doses1 in 300,000 doses