
05abmdr Xdr Tuberculosis Seminar
71
MODERATOR : DR PANKAJ ABROL PRESENTED BY: DR VIRENDER VERMA MDR & XDR TUBERCULOS IS
-
Upload
milap-shah -
Category
Documents
-
view
219 -
download
0
Transcript of 05abmdr Xdr Tuberculosis Seminar

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 1/71
MODERATOR : DR PANKAJ ABROL
PRESENTED BY: DR VIRENDER
VERMA
MDR & XDR TUBERCULOSIS

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 2/71
MDR & XDR TUBERCULOSIS
Definition
Epidemiology
Etiology
Diagnosis
Treatment
Special situation

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 3/71
Introduction
Mycobacterium tuberculosis has been present in the human
population since antiquity
1882 - Robert Koch discovered Mycobacterium
tuberculosis

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 4/71
Introduction (Contd..)
Sanatorium - The first step against TB.
Measures available to doctors were still modest
Improve social and sanitary conditions
Reduction of the lung volume( Thoracoplasty ) Radiation
1943 - Streptomycin
1963 - Rifampicin

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 5/71
Introduction (Contd..)
Resistance to Streptomycin emerged in 85% cases
Mid-1990 - Most countries registered MDR-TB
2006 – XDR – TB term was coined
BMJ 1948;2:1009 – 1015
N Engl J Med 1993;328:521-6
Morb Mortal Wkly Rep 2006; 55: 301 – 05

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 6/71
Definition
Mono Resistance: Resistant to one drug
Poly-Resistance: Resistant to more than 1 drug
MDR-TB: Resistant to at least isoniazid and rifampicin
with or without resistance to other drugs XDR-TB: MDR-TB + any one of the fluoroquinolones +
one of three injectable second-line drugs (Amikacin,
Capreomycin or Kanamycin)
MMWR 2006;55:1176WHO

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 7/71
Epidemiology
An estimated 9.2 million new cases of TB in 2006 (139
per 100 000 population)
4.1 million new smear-positive cases (44% of the total)
0.7 million HIV-positive cases (8% of the total)
An estimated 14.4 million prevalent cases
Estimated 1.5 million deaths from TB in HIV-negative
people
Estimated 0.2 million death among people infected withHIV.
Semin Respir Crit Care Med 2008;29:481 –
491

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 8/71
EpidemiologyEstimated number of new TB cases
Asia accounts for 55% of global cases, and Africa
accounts for 31%
India ranks 1st
Incidence-168/1lkh pop/yr
Prevalance-299/1lkh pop/yr
WHO REPORT 2008 | GLOBAL TUBERCULOSIS CONTROL
Highest no of
cases

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 9/71
Epidemiology(Contd…)
An estimated 489,139 cases of MDR-TB in 2006
Accounts for 4.8% of all TB cases
Increase of 12% since 2004 and 56% since 2000
China and India carry approximately 50% of the global
burden of MDR-TB
.
Semin Respir Crit Care Med 2008;29:481 –
491

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 10/71
MDR PREVALENCE HIGHER THAN 5.0%AMONG NEW CASES 2002-2007
22.3%
WHO/IUATLD Drug Resistance Surveillance. 2008

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 11/71
MDR PREVALANCE HIGHER THAN 30% AMONGPREVIOUSLY TREATED CASES, 2002-2007
60.0%
WHO/IUATLD Drug Resistance Surveillance. 2008

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 12/71
MDR prevalence in south east Asian region
WHO/IUATLD Drug Resistance Surveillance. 2008

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 13/71
Epidemiology(Contd..)
The overall prevalence of XDR-TB is 2%
7% of total MDR – TB cases are XDR-TB
Countries conducting routine surveillance- XDR represent between 7% &34% of MDR isolates
The Global MDR-TB & XDR-TB Res onse Plan 2007 – 2008
The WHO/IUATLD Global Project on Anti-tuberculosis DrugResistance Surveillance 2002-2007

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 14/71
Till June 2008, 49 country have reported confirmed XDR-TB cases to WHO

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 15/71
Prevalence of drug resistancein new cases
Adapted from, Sharma et al TUBERCULOSIS

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 16/71
Prevalence of drug resistance inpreviously treated patient
Adapted from, Sharma et al TUBERCULOSIS

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 17/71
Drug resistant data fromsurvelance sites
Adapted from, Sharma et al. TUBERCULOSIS

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 18/71
Epidemiology(Contd…)
In India an estimated 110 132 cases of MDR-TB in 2006
Accounts for 4.8% of all TB cases
Prevalence among new cases - 2.8%
Prevalence among treated cases -17.2%.
For XDR - 7.4% & 9.3% among MDR-TB
WHO REPORT 2008 | GLOBAL TUBERCULOSIS CONTROL

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 19/71
Aiims Data
Primary MDR- 6%
Acquired MDR- 24%
XDR- 4%
Aiims microbiology department

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 20/71
Molecular basis
Drug resistance can be achieved by.
Barrier methods
Degrading or inactivating
enzyme Drug target modifications
MDR-TB reflects step wise accumulation of individual
mutation
Spontaneous mutations leading to resistance occur atrandom
Natural resistance
Resistance to ATT
Tubercle 1987; 68:5 –
18Lancet 1994; 344:293 – 8

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 21/71
Mechanism of drug action
National Institute of Allergy And Infectious Disease

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 22/71
Mechanisms of drug resistance
Thorax 1998;53:793 –
797

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 23/71
WEIGHTED MEAN OF RESISTANCETO SPECIFIC DRUGS
The WHO/IUATLD Global Project on Anti-tuberculosisDrug Resistance Surveillance 2002-2007
In new cases In previously treated cases

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 24/71
Amplifier effect of short coursechemotherapy
Semin Respir Crit Care Med 2008;29:499 – 524

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 25/71
Host factor
The frequencies of DRB1∗01and of DQB1∗0502
significantly decreased in the MDR-TB
DRB1∗14 occurred in 30.9% of MDR cases 6.8% in the
drug sensitive cases Patients with HLA-DRB1∗14 have a eight-fold risk of
developing MDR-TB
Odd ratio = 8.2
Sharma S K et al. I nfection, Genetics and Evolution 3 (2003) 183-188

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 26/71
Agent factor
The most wide spread Mycobacterium tuberculosis strains
are of Beijing family
W-Beijing genotype strong association with multidrug
resistance Method - Restriction fragment length polymorphism
(RFLP) analysis of IS6110 insertion
World wide prevalent
Int J Tuberc Lung Dis 2005; 9:646 –
653

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 27/71
Factors related to previoustreatment
MDR-TB is a man-made phenomenon
poor treatment, poor drugs and poor adherence lead to the
development of MDR-TB.
Most powerful predictor of presence of MDR-TB is ahistory of previous treatment
In management most common error is adding single drug to
failing regimen
Indian J Med Res 2004; 120:354 – 376

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 28/71
Causes of inadequate treatment
Lambregts et al. Tubercle and Lung Disease 1995: 76; 455-458

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 29/71
l f

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 30/71
Supranational reference LaboratoryNetwork
TRC
WHO/IUATLD Drug Resistance Surveillance. 2008

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 31/71
Who should go for drug sensitivity test?
A TB patient who fails an RNTCP Category I or III
treatment regimen
Any RNTCP Category II patient who is sputum smear
positive at the end of the fourth month of treatment or later. Concurrent illness such as epilepsy, alcoholism, renal and
hepatic problems, psychiatric illness
Excluded
Under 15 years of age; Having had >1 mth t/t with second-line anti-TB drug.
MDR Suspect
RNTCP DOTS-Plus Guidelines,2008

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 32/71
Laboratory aspect
Sputum should be good and satisfactory
Specimen should be transported as soon as possible
If delay
Refrigeration
Preservation -1% Cetyl Pyridinium Chloride (CPC) + 2%
NaCl
Sputum container labelled as BIO- HAZARD
Homogenisation and decontamination
Inoculation and incubation
RNTCP DOTS-Plus Guidelines,2008

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 33/71
Methods of Drug susceptibility
Conventional method
Culture uses Lowenstein-Jensen (LJ) or 7H11 solid media
Takes long time - 6-8 week
Sensitivity limited by availability of bacilli in sample
Methods
Absolute Concentration Method
The Resistance Ratio Method
Proportion Method

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 34/71
Proportion method
Method of choice: Recommended by DOTS-Plus
10-fold dilutions of inoculum are planted on both control
and drug – containing media
Resistant portion as a percentage of the total populationtested
CRITERIA OF RESISTANCE
Any strain with 1% (the critical proportion) of bacilli
resistant to any of the four drugs

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 35/71

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 36/71
Phage-based tests
Luciferase reporter phages
Infected bacteria emit light
Results in 2 days post culture
Limited reports of clinical application
FAST Plaque TB-RMP test
Plaques of lysed cells counted
Results in 2-3 days
Cannot be used for children or HIV-positive patients
S Afr Med J . 2007;97:858-863
J Infect. 2005;51:175-187.

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 37/71
Others
Microscopic-Observation Drug-Susceptibility assay
(MODS)
DST for first line drugs
Report within 7 days
Simple, rapid & low cost
Nitrate reductase assay
Sensitivity and specificity ≥ 90%.
Colorimetric method
For isoniazid and rifampicin
N Engl J Med. 2006;355:1539-1550Antimicrob Agents Chemother. 2003;47:3616-3619.
7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 38/71
Molecular method
DNA sequencing
Most accurate and reliable method for mutation detection
Detect both previously recognized and unrecognized mutations
For rifampicin only
The Line Probe assay (LiPA)
Detect rpoB mutations of rifampicin
Result in less than 48 hours
J Clin Microbiol. 2007;45:2635-2640

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 39/71
GenoType® MTBDR test
•Test available
within one day
•Sensitivity- 98.8%
•specificity - 100%
J Clin Microbiol 2005; 43: 3699-3703

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 40/71
Diagnosis(Contd..)
DNA microarrays
Based on the principle of hybridization
Detect Rifampicin resistance only
Analysis large amounts of DNA sequences
Molecular beacons
Sensitive enough to detect 2 bacilli,
Results in 3 hours
Single-strand conformation polymorphism (SSCP)
Fluorescence resonance energy transfer (FRET) probes
Genome Res 1998;8:435-48.Methods Mol Biol 2003;212:111-28

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 41/71
Difficulty in testing susceptibility of2nd line drugs
In vitro drug instability
Drug loss due to protein binding
Heat inactivation
Incomplete dissolution Filter sterilization
Varying drug potency
Critical concentration very close to the minimal inhibitory
concentration (MIC)
Guidelines for mangt of DR-TB Update 2008 WHO

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 42/71
Prevention
Self administered therapy is inferior to DOTS
Fixed dose combination (FDC) can be a cost effective
strategy, only somewhat inferior to DOTS
DOTS the most cost effective intervention in the control of
TB
DOTS the most cost effective prevention for MDR &
XDR- TB
Int. J . Tuberc. Lung Dis. 2000; 4: 201 –
7

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 43/71
DOTS in MDR – TB:
cure rate: ≤ 60%
recurrence rate: ≥ 28%
J AMA 2000; 283: 2537 – 45.
Int. J . Tuberc. Lung Dis. 2002; 6: 858 –
64.WHO/HTM/TB/2006.361

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 44/71
Programme strategies
Standardized treatment
On the basis of DRS data
All patients receive the same regimen
Empirical treatment Individually designed
Based on history of antituberculosis treatment &DRS data
Individualized treatment
Based on history of antituberculosis treatment & DST

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 45/71
Basic principles
Patient suspected of drug resistance, must under go culture
& DST
Patient should immediately started with treatment
A single drug should never be added to failing regimen
Drugs with potential cross resistance should never be used
At least 3 previously unused drugs to which there is in vitro
susceptibility , must be employed
Based on the history of drugs taken
Minimum duration is 18 months post culture conversion
7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 46/71
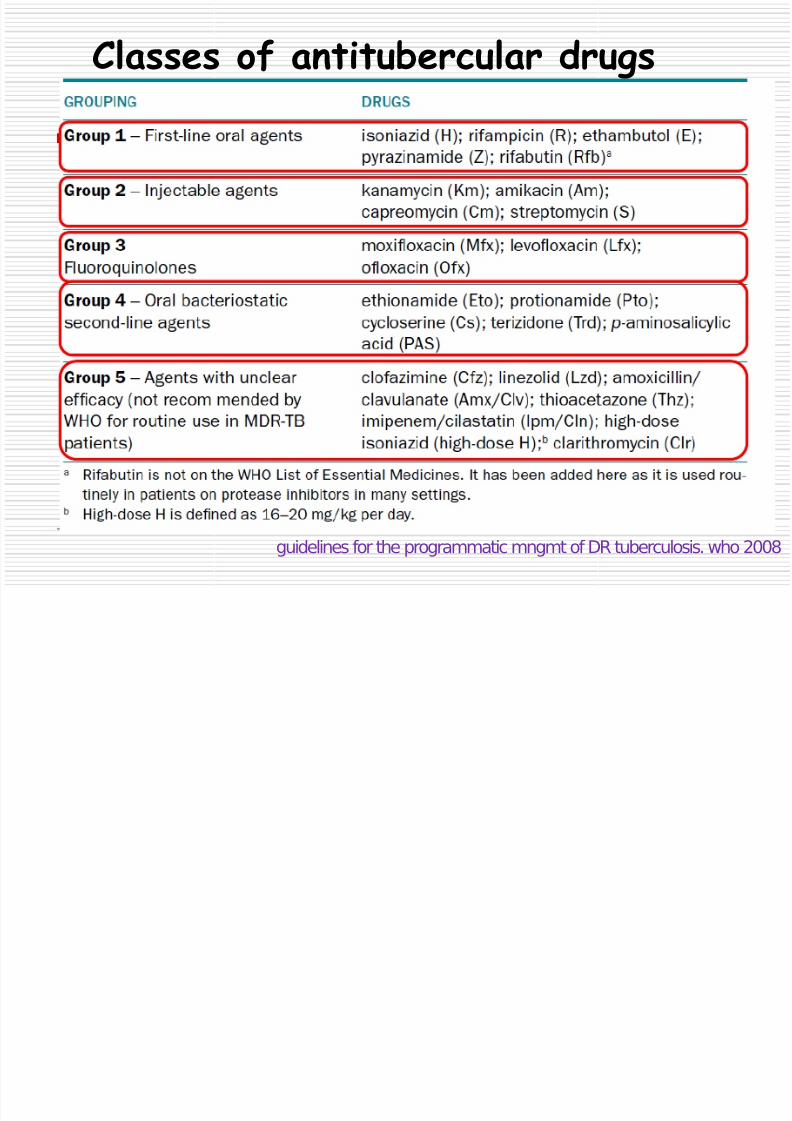
Classes of antitubercular drugs
guidelines for the programmatic mngmt of DR tuberculosis. who 2008
Use any available

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 47/71
Use any available
Group 1: First-line oral agents
Plus one of theseGroup 2: Injectable agents
Plus one of these
Group3: Fluoroquinolones
Pick one or more of
Group 4: Second-line oral
bacteriostatic agents
Consider use of these
Group 5: Drugs of unclear role in
DR-TB treatment
MDR TB suspect referred from MO-PHI to DTO

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 48/71
MDR TB suspect referred from MO PHI to DTO
with
• Copy of the Cat II (and Cat I/III) Rx card
• Request for culture and DST form
• Drug-o-gram
DTO confirms suspect and sends sputum
samples to IRL with• Request for culture and DST form
• Drug-o-gram
Enter in Culture and DST register at DTC
Culture and DST results
communicated to
the DTO electronically
continuesCat II
treatment
Non MDR
TB MDR TB
• Patient traced by DTO with the help of MO-TC
and STS.
• Patient counselled and referred to DOTS Plus
site
Continue
Cat II
RNTCP DOTS-Plus Guidelines,2008

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 49/71
RNTCP CATEGORY IV REGIMEN
6 (9) Km Ofx Eto Cs Z E / 18 Ofx Eto Cs E
RNTCP DOTS-Plus Guidelines,2008

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 50/71
Surgery
Indications
Localized disease
High probability of failure or relapse with medical therapy
3 months chemotherapy prior to surgery
Bilateral disease does not preclude surgical intervention,
unless extensive
Excellent cure rates ≥90% with post-surgery chemotherapy
Clin. Chest Med. 1997; 18: 123 – 30
Ann. Thorac. Surg. 2005; 79:959 –
63

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 51/71
Surgery(Contd..)
Poor prognosis
Low BMI (<18.5 kg/m2)
Bacillary resistance to ofloxacin
Cavitation beyond the range of surgical resection
Complications: Respiratory failure, Bronchopleural fistula,
Infections, Empyema, wound
Adjunctive surgical procedures : Myoplasty, Omentoplasty,
Thoracoplasty
Eur Respir. J . 2006; 28: 576 –
80

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 52/71
Immunotherapy
Mycobacterium vaccae
Mycobacterium w
Cytokine therapy
interferon-g
Interferon-α
Interleukin-2 (IL-2)
Others
Thalidomide Transfer factor
Pentoxifylline Inhibitors of transforming Imiquimod growth factor-
Levamisole Interleukin-12
Clin. Exp. Immunol. 2005; 141:541 – 8.
Respir. Med. 2001; 95: 444 –
7.

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 53/71
Exploratory approach
Local instillation of antimycobacterial agent
Plant products: cerulenin, transcinnamic acid, Flourensia
etc
Imipenem in murine model New delivery system: liposomes, solid lipid nano particles
Int. J . Antimicrob. Agents 2007; 29: 338 –
40

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 54/71
Newer therapy
The American J ournal of Medicine (2008) 121, 835-844

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 55/71
Infection control measures
Administrative controls
Reduced hospitalisation
Rapid drug-susceptibility assays
Detention for confirmed XDR tuberculosis patients
Environmental controls
Airborne Infection Isolation (AII) room
High-Efficiency Particulate Air (HEPA) Filter
Ultraviolet germicidal irradiation (UVGI)
Personal respiratory protection
Respirator
Surgical masks for patient
MMWR December 30, 2005 / 54 (RR17); 1-141

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 56/71
Treatment outcomes
Short course chemotherapy is ineffective for controlling
established MDR-TB
Cure rate ≤ 60%
Recurrence rate ≥ 28%
Cure rates up to 75% can be achieved with individualized
regimen
XDR-TB co infected with HIV, mortality is very high
Kwazulu Natal study 52 out of 53 XDR cases died
Sharma S K et al.Indian J Chest Dis Allied Sci. 1996 38(2):73-9N Engl J Med 1993; 328: 527
– 32

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 57/71
Outcome(contd..)
Total 801 patients referred among this 651 tested
651 patients tested XDR-TB - 48 (7.4%)
MDR-TB- 603 (92.6%)
Use of Comprehensive treatment with5 drugs (incl
fluoroquinolone and injectables) at highest tolerated dose,
T/t >2 years, drug susceptibility done to design and adjust
regimens. Cured or completed the treatment
XDR-TB- 29 (60.4%)
MDR-TB – 400 (66.3%)
N Engl J Med 2008;359:563-74

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 58/71
Outcomes(contd..)
N Engl J Med 2008;359:563-74
St d f bli ti T f DR TB T t t O t
Cure rates

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 59/71
Study, year of publication Type of DR-TB Treatment Outcome
Goble et al, 1993
Sharma et al, 1996
Park et al , 1998
Yew et al, 2000
Tahaoglu et al, 2001
Mitnick et al, 2003
Nathanson et al, 2006
Gandhi et al, 2006
Sharma, 2007
Mitnick et al, 2008
MDR-TB [ n = 171]
MDR-TB [ n = 19]
MDR-TB [ n = 107]
MDR-TB [ n = 63]
MDR-TB [ n = 158]
MDR-TB [ n = 75]
MDR-TB [ n = 1047]
XDR-TB [ n = 53]
MDR-TB [ n = 172]
XDR-TB [ n = 1]
XDR-TB [ n =48]
MDR-TB [ n = 603]
65% cured, treatment failure
35%
Sputum conversion in 18 cases
out of 19 82.5% cured, treatment failure
17.5%
81% cured, treatment failure
14.3%, death 4.7%
Cured or completed treatment
77%, default 11%, treatmentfailure 8%, death 4%
83% cured, death 8%
Cured or completed treatment
69.7%, treatment failure 6.7%
52 of the 53 patients died
41.6% cured, treatment failure
38.7%
60.4% with XDR-TB completed
treatment or cured; 66.3% with
MDR-TB completed treatment
or cured Adapted from, Sharma et al TUBERCULOSIS

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 60/71
Poor prognosis
HIV
Extrapulmonary involvement
Low haematocrit
Low BMI
Older age
Alcoholism
Bacillary and treatment characteristics
Extensive drug resistance
Resistance to ofloxacin in vitro
previous treatment
failure to apply appropriate therapy
Poor adherence during treatment

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 61/71
Management of contacts
Identify through contact tracing
If contacts have active disease the culture & DST required
Clinical follow up for a period of at least 2 year
If active disease then prompt MDR-TB regimen WHO not recommended 2nd line drugs as
Suggested regimens
Pyrazinamide plus Ethambutol
Pyrazinamide plus Quinolone
Am J Respir Crit Care Med 2000; 161(4 Pt 2) : 221-47
Guidelines for mangt of DR-TB Update 2008 WHO

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 62/71
MDR & XDR-TB and HIV
African region has high burden for both HIV and TB
TB -Most common opportunistic infection in HIV
Risk of reactivation : 5 to 8 per cent per annum
Cumulative lifetime risk : ≥ 30 % No predisposes for MDR-TB
High risk of mortality, especially when diagnosed late
AIDS 1998; 12 : 191-5
Thorax 2002; 57: 810 –
16

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 63/71
Contd...
Antiretroviral therapy must
Efavirenz is the preferred drug to be used in patients on
ATT
Drug interaction uncommon with 2nd
line drugs ex Fluoroquinolone – Didanosine
Higher rate of adverse drug reaction
Extrapulmonary localization, independent poor prognostic
factor .
Am. J . Respir. Crit. Care Med. 2001; 164

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 64/71
Children
Transmission of MDR-TB from adult patients to children
could occur
Adverse drug reactions are common.
Reasonably good cure rate
Fluoroquinolones- Conflicting evidence
Weight loss / absence of satisfactory weight gain is
suggestive of treatment failure
WHO/HTM/TB/2006.361Hampel B et al. Pediatr. Infect. Dis. J . 1997; 16: 127 – 9

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 65/71
Pregnancy
Not a contraindication for treatment of MDR-TB
Therapy may be delayed until the second trimester
Avoid aminoglycoside
Ethionamide can aggravate nausea and vomiting in pregnant women
Infant formula is good alternatively to breast feeding
Outcome is good
Chest 2003; 123: 953 – 6.

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 66/71
Summary
MDR & XDR tuberculosis pose greater challenge for
effective TB management
Poor treatment, poor drugs and poor adherence lead to the
development of drug resistance
MDR-TB and XDR-TB are pure laboratory diagnosis
Need for new methods for early diagnosis

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 67/71
Summary(Contd..)
DOTS treatment for TB patients is the most cost effective
method of preventing MDR TB
Prompt diagnosis early treatment is prerequisite for all
programmes
Adjuvant therapy should be use whenever possible
Comprehensive and individualized treatment have good
prognosis compared to standardized treatment

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 68/71
Thank you

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 69/71
21-female
•H/O Cough, Shortness of breath for 2
years
• Associated with blackish sputum – only
during menstruation
•Weight loss and reduction in appetite
• ATT – 1 year for this illness
Examination:
•No LAP•Chest: Bilateral crepitations
•CVS and Abdomen: Normal

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 70/71
DIFFERENTIALS:
•Interstitial lung disease –Lymphangiomyomatosis
•Catamenial Lung
• Atypical infections

7/29/2019 05abmdr Xdr Tuberculosis Seminar
http://slidepdf.com/reader/full/05abmdr-xdr-tuberculosis-seminar 71/71
Fibre-optic bronchoscopy:
Bronchial washing : AFB positive
Culture: Mycobacteria tuberculosisResistance: HRE
Sensitive: Fluoroquinolone, cycloserine,
Streptomycin


















