03:15 pm – 03:30 pm Lecture: Bioresorbable vascular scaffolding (BVS) in clinical practice: what...
16
03:15 pm – 03:30 pm Lecture: Bioresorbable vascular scaffolding (BVS) in clinical practice: what can we expect after CE Mark? Raul Moreno University Hospital La Paz Madrid, Spain
-
Upload
conrad-stephens -
Category
Documents
-
view
214 -
download
0
Transcript of 03:15 pm – 03:30 pm Lecture: Bioresorbable vascular scaffolding (BVS) in clinical practice: what...

03:15 pm – 03:30 pmLecture: Bioresorbable vascular scaffolding (BVS) in clinical practice: what can we expect after CE Mark?
Raul MorenoUniversity Hospital La Paz
Madrid, Spain

JACC 1999;34;1498-1506.
START randomized study (n=452)Long-term follow-up
8-June-2011
The benefit of BMS is within the first months.
Is there any advantage of a permanent scaffolding?And any disadvantage?
Mechanical support is needed to avoid negative
remodeling and vessel shrinkage, that occur during the first 6 mo.
Bioresorbable vascular scaffolding (BVS)

Two Patients with Extremely Late (8 and 12 Years) Bare-Metal Stent Thrombosis: The Risk Never Completely Disappears!
8-June-2011
J Invasive Cardiol 2008;20:E329-330.
Long-term safety problems of coronary stents
Bioresorbable vascular scaffolding (BVS)
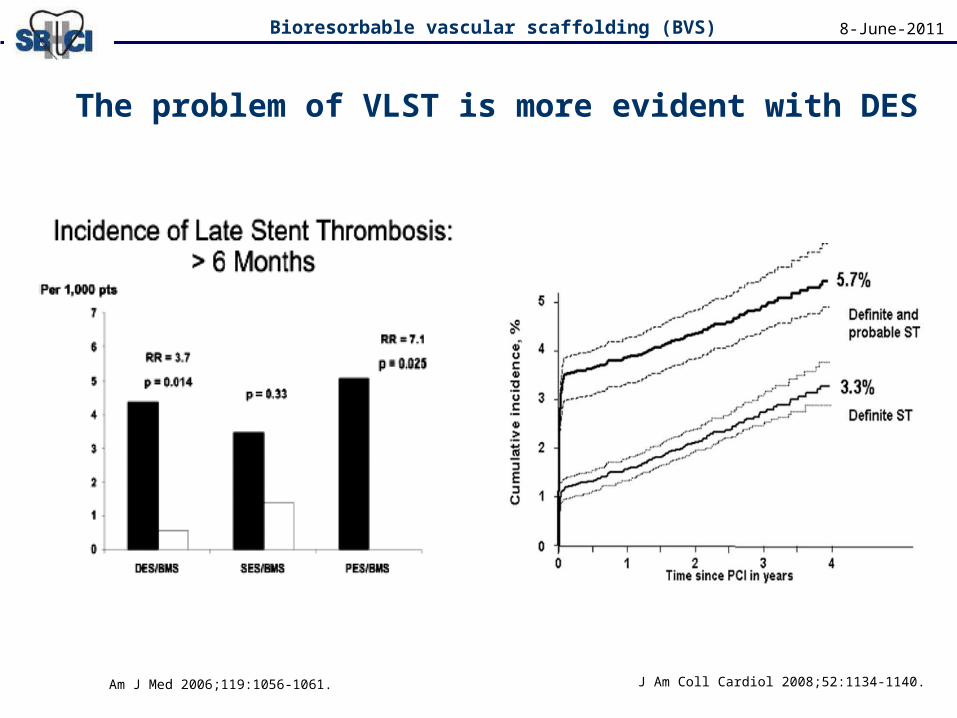
Am J Med 2006;119:1056-1061.
The problem of VLST is more evident with DES
8-June-2011
J Am Coll Cardiol 2008;52:1134-1140.
Bioresorbable vascular scaffolding (BVS)

Is there a need for bioabsorbable stents?
Potential advantages of bioasborbable stents• Risk of stent thrombosis never completely dissapears.
• Need for indefinite anti-platelet therapy.• Potential limitation for future CABG.• Stent fracture.• Prevent late stent malapposition & allow positive remodeling.
Stent in thrombus containing lesions.• Side branch compromise in bifurcations.• Bifurcations: Long-term safety issues of 2-stent techniques.• Aorto-ostial lesions.• Concerns about endothelial function.• PCI in children.• IRM & MSC imaging.
8-June-2011Bioresorbable vascular scaffolding (BVS)

0
0,2
0,4
0,6
0,8
1
1,2
1 1,1 1,2 1,3 1,4 1,5 1,6 1,7 1,8 1,9 2
BA
BMS
SESEES
PES
MgAG 1.42; LL 1.08 mm PROGRESS-AMSLate loss (4 months):• 42% vessel shrinkage• 45% hyperplasiaToo quick absortion
Lancet 2007;369:1869 PCR 2011
8-June-2011
Previous bioabsorbable stents
DREAMS
AG 1.44; LL 0.68 mm BIOSOLVE-1
Acute gain(mm)
Late loss(mm)
REVAAG 1.81; LL .1.89 mm
LL: NIH & loss of stent area
TCT 2009 & TCT 2010
Bioresorbable vascular scaffolding (BVS)
Net gain = 1

Lactic Acid(C3H6O3)
L-LA
D-LA
Meso L,D-LA
Racemic D,L-LA
CO2
&H2O
Krebs
Cycle
Poly-lactic acid- Poly-L-LA (PLLA).- Poly-D,L-LA (PDLLA).- etc.
~LA~LA~LA~LA~LA~LA~
J Exp Biol 2005;208:4561
8-June-2011
Polylactic acid
Bioresorbable vascular scaffolding (BVS)
*Polymer: a large molecule (macromolecule) composed of
repeating structural units.

0
0,2
0,4
0,6
0,8
1
1,2
1 1,1 1,2 1,3 1,4 1,5 1,6 1,7 1,8 1,9 2
BA
BMS
SESEES
PES
Mg
Tamai(PLLA)
AG 1.57; LL .75 mmLL: neo-intimal hyperplasia
Circulation 2000;102:399 TCT 2009 & TCT 2010
8-June-2011
REVA
DREAMS
Acute gain(mm)
Late loss(mm)
Bioresorbable vascular scaffolding (BVS)
Net gain = 1

• Acute gain should be optimal (radial strength).• Absorption should not be too quick.• Neo-intimal hyperplasia occurs: release anti-proliferative drugs.
Lessons:
BVS (Abbott vascular)
• Polymer backbone (PLLA) Semicrystalline• Polymer (PDLLA) and everolimus matrix. Amorphous
8-June-2011Bioresorbable vascular scaffolding (BVS)

ABSORB (Cohort A)
Eurointervention 2005;1:58-65 Lancet 2008;371:899-907
0.300.501.98NIH area (mm2)
-16.6-7.2-29.4Ʌ Lumen area (%)
-11.2-0.3-2.0Ʌ Stent area (%)
0.440.100.87Late loss (mm)
BVSEESBMS
*EES and BMS provided by SPIRIT-I
6 mo. IVUS: reasons for late loss
8-June-2011
Shrinkage (“late recoil”)… that does not continue
from 6 mo. to 2 yr (!!)
NCT00300131
Bioresorbable vascular scaffolding (BVS)
(30 patients treated with 3x12 or 3x18 mm BVS)
• Clinical FU (4 yr): 1 NQMI, 2 non-cardiac deaths, no ST.• OCT: resorption begins at 6 mo, almost complete at 2 yr.

• Same composition, dose of everolimus & resorption time.• Same strut thickness (150 µm).• Modified platform designed with a reduced maximal circular unsupported scaffold area (MCUSA) and a different manufacturing process of the polymer.• More uniform strut distribution.• Similar profile to a 1st-generation DES:
8-June-2011
Second generation BVS
BVS 1.1 Cypher Select
Profile 1.40 1.23
Strut thickness (µm) 158 (150 + 6-8 polymer) 164 (140 + 24 polymer)
Bioresorbable vascular scaffolding (BVS)

0.300.501.98NIH area (mm2)
-16.6-7.2-29.4Ʌ Lumen area (%)
-11.2-0.3-2.0Ʌ Stent area (%)
0.440.100.87Late loss (mm)
BVSEESBMS
*EES and BMS provided by SPIRIT-I0.08
-5.4
-2.0
0.19
BVS 1.1
8-June-2011Bioresorbable vascular scaffolding (BVS)
ABSORB (Cohort B)n = 101 (3x18 mm stents)
Current data: up to 1 year no deaths, no QMI, no stent thrombosis
TCT 2010 NCT00856856 PCR 2011

0
0,2
0,4
0,6
0,8
1
1,2
1 1,1 1,2 1,3 1,4 1,5 1,6 1,7 1,8 1,9 2
BA
BMS
SESEES
PES
Mg
Tamai(PLLA)
BVS-1AG 1.24; LL .44 mm
Lancet 2008;371:899
BVS-2AG 1.26; LL .19 mm
TCT 2010
8-June-2011
REVA
DREAMS
Acute gain(mm)
Late loss(mm)
Bioresorbable vascular scaffolding (BVS)
Net gain = 1
Raul Moreno
Reflection:In-stent late loss is a valid measurement to evaluate the efficacy of DES vs BMS and in head-to-head trials, but…May be that late loss is not valid to compare BVS and DES, because of different mehanical properties…May be that NET GAIN is the best parameter.
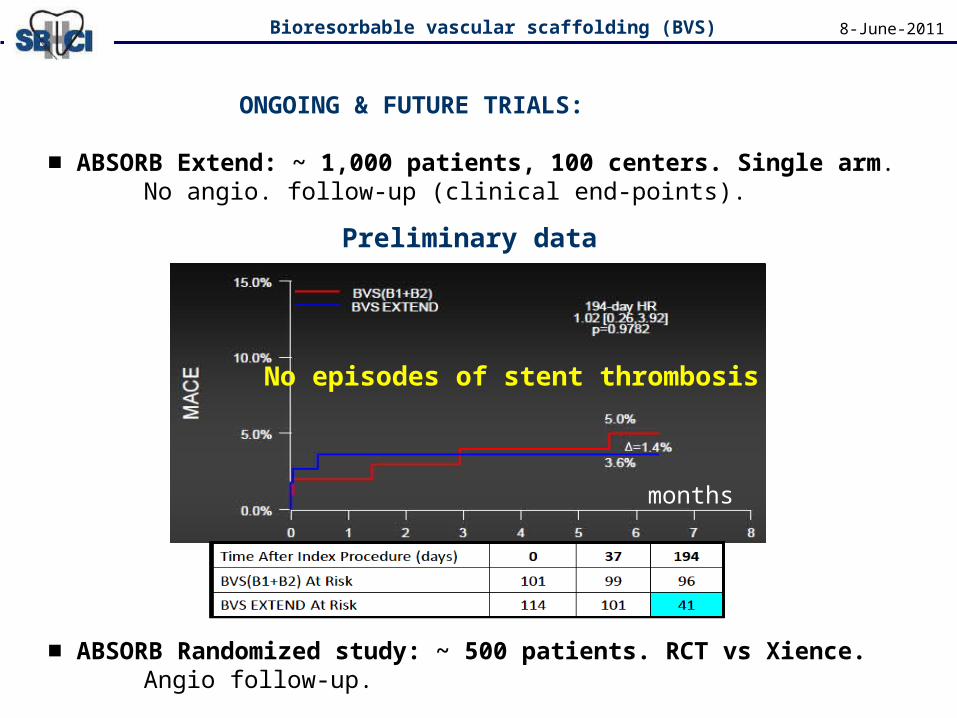
ONGOING & FUTURE TRIALS:
■ ABSORB Extend: ~ 1,000 patients, 100 centers. Single arm.No angio. follow-up (clinical end-points).
■ ABSORB Randomized study: ~ 500 patients. RCT vs Xience.Angio follow-up.
8-June-2011Bioresorbable vascular scaffolding (BVS)
months
Preliminary data
No episodes of stent thrombosis

What when I
had BVS in my cath.
Lab?
8-June-2011
• STRENGTH: No permanent device.
• WEAKNESS: Mechanical concerns.
• Consider in patients with soft plaques in whom VLST may be more frequent...• What about complex lesions? I need studies.
Abbott Receives CE Mark Approval for World's First Drug Eluting Bioresorbable Vascular Scaffold for
Treatment of Coronary Artery Disease
Bioresorbable vascular scaffolding (BVS)

• Fully bioabsorbable stents (BVS) are already here !
• Absorption and vessel wall integration are real phenomena.
• We do not have to worry about acute recoil.
• Neo-intimal hyperplasia inhibited by everolimus.
• Vessel shrinkage (late recoil) solutioned with BVS 1.1.
• No early, late or very late ST observed in ABSORB A&B (n=131) or the interim data of ABSORB-EXTEND.
• Concerns about acute gain (immediate result) in some subsets. Thus, lesions not included in ABSORB may be considered “off-label” (studies with complex lesions needed).
8-June-2011
CONCLUSIONS
Bioresorbable vascular scaffolding (BVS)