02. Common Opportunistic Infections

of 53
-
Upload
veerapong-vattanavanit -
Category
Documents
-
view
220 -
download
0
Transcript of 02. Common Opportunistic Infections
-
8/2/2019 02. Common Opportunistic Infections
1/53
Wanla Kulwichit, MDInfectious Diseases
Chulalongkorn University
SEARCH Regional HIV/AIDS TrainingSEARCH Regional HIV/AIDS Training
88thth January to 9January to 9thth February, 2007February, 2007
Supported by
A Training GrantFrom
Opportunistic Infections in HIV-infectedPatientsAn Overview
-
8/2/2019 02. Common Opportunistic Infections
2/53
TB & HIV
-
8/2/2019 02. Common Opportunistic Infections
3/53
-
8/2/2019 02. Common Opportunistic Infections
4/53
-
8/2/2019 02. Common Opportunistic Infections
5/53
MDRMDR--TB more than nonTB more than non--HIV?HIV?Same Rx or longer?Same Rx or longer?
RifampinRifampin V.S.V.S. antiretroviralsantiretrovirals
When to startWhen to start antiretroviralsantiretrovirals??
Beware of immune recovery!Beware of immune recovery!
-
8/2/2019 02. Common Opportunistic Infections
6/53
Primary MDR-TB: HIV - nonHIV
-
8/2/2019 02. Common Opportunistic Infections
7/53
Primary MDR-TB: HIV - nonHIV
Int J Tuberc Lung Dis2000; 4: 537-43
-
8/2/2019 02. Common Opportunistic Infections
8/53
-
8/2/2019 02. Common Opportunistic Infections
9/53
Primary MDR higher among
HIV (8.5%) than nonHIV(4.4%) P= 0.022
Int J Tuberc Lung Dis2001; 5: 32-9
-
8/2/2019 02. Common Opportunistic Infections
10/53
Same or longer?
N Engl J Med1995; 332: 779-84
-
8/2/2019 02. Common Opportunistic Infections
11/53
Optimal duration of
treatment is uncertain
CDC NIH IDSA Statement
MMWRDecember 17, 2004
-
8/2/2019 02. Common Opportunistic Infections
12/53
Optimal duration of
therapy for HIV-1-related TB disease
remains controversial
CDC NIH IDSA Statement
MMWRDecember 17, 2004
-
8/2/2019 02. Common Opportunistic Infections
13/53
Prolonged therapyrecommended for
patients with delayedCLINICAL or
BACTERIOLOGIC
responseCDC NIH IDSA Statement
MMWRDecember 17, 2004
-
8/2/2019 02. Common Opportunistic Infections
14/53
SYMPTOMATIC or
POSITIVE CULTUREat or after 2 months of
therapy
CDC NIH IDSA Statement
MMWRDecember 17, 2004
-
8/2/2019 02. Common Opportunistic Infections
15/53
Rifampicin and HAART:
problems with PI and NNRTI
-
8/2/2019 02. Common Opportunistic Infections
16/53
Rifam-nevirapine:CONTRAINDICATED!
MMWR1998; 47 (RR-20)
-
8/2/2019 02. Common Opportunistic Infections
17/53
Nevirapine andrifampin
MMWR2000; 49: 185-9
Data are insufficient to assess
whether dose adjustments arenecessary
-
8/2/2019 02. Common Opportunistic Infections
18/53
Nevirapine and rifampin(contd)
MMWR2000; 49: 185-9
Rifampin and nevirapine should
be used only if clearly indicatedand with careful monitoring
-
8/2/2019 02. Common Opportunistic Infections
19/53
Co-administration of rifampin
and nevirapine in HIV-infectedpatients with tuberculosis
AIDS2003,
17:637642
-
8/2/2019 02. Common Opportunistic Infections
20/53
-36 pts, 4 lost to follow-up-all pts cured of TB-74% undetectable viral loads-median CD4 increase116/cu.mm.
AIDS2003,
17:637642
-
8/2/2019 02. Common Opportunistic Infections
21/53
Nevirapine high therapeuticindex
With dose of 400 mg/day, steady state Cmin
4.5 + 1.9 microgram/ml IC50 for the drug = 0.00250.025microgram/ml
J Infect Dis 1995, 171:537545
-
8/2/2019 02. Common Opportunistic Infections
22/53
What do experts say?
Annu Rev Med2004; 55: 283-301
-
8/2/2019 02. Common Opportunistic Infections
23/53
Updated Guidelines for the Use of
Rifamycins for the Treatment ofTuberculosis Among HIV-Infected PatientsTaking Protease Inhibitors or Nonnucleoside
Reverse Transcriptase Inhibitors
http://www.cdc.gov/nchstp/tb/tb_hiv_drugs/toc.htm
-
8/2/2019 02. Common Opportunistic Infections
24/53
Updated Guidelines for the Use of
Rifamycins for the Treatment ofTuberculosis Among HIV-Infected PatientsTaking Protease Inhibitors or Nonnucleoside
Reverse Transcriptase Inhibitors
http://www.cdc.gov/nchstp/tb/tb_hiv_drugs/toc.htm
-
8/2/2019 02. Common Opportunistic Infections
25/53
Updated Guidelines for the Use of
Rifamycins for the Treatment ofTuberculosis Among HIV-Infected PatientsTaking Protease Inhibitors or Nonnucleoside
Reverse Transcriptase Inhibitors
http://www.cdc.gov/nchstp/tb/tb_hiv_drugs/toc.htm
-
8/2/2019 02. Common Opportunistic Infections
26/53
What do experts say?
(contd)
THE LANCET Vol 363 April 17,2004
-
8/2/2019 02. Common Opportunistic Infections
27/53
What does a pseudo-
expert need to say?
THE LANCET Vol 364 July 24, 2004
Wh t d d
-
8/2/2019 02. Common Opportunistic Infections
28/53
What does a pseudo-
expert need to say?(contd)
THE LANCET Vol 364 July 24, 2004
-
8/2/2019 02. Common Opportunistic Infections
29/53
What does the expert
counter-say? (contd)
THE LANCET Vol 364 July 24, 2004
-
8/2/2019 02. Common Opportunistic Infections
30/53
Immune ReconstitutionInflammatory Syndrome (IRIS)
Immune reconstitutionsyndrome
Immune restitution syndromeImmune recovery syndrome
Paradoxical response
C 1 t t t
-
8/2/2019 02. Common Opportunistic Infections
31/53
Case 1: pretreatment
Am J Roentgenol2000; 174: 43-9
-
8/2/2019 02. Common Opportunistic Infections
32/53
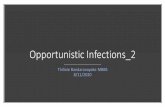
Case 1: worsening
-
8/2/2019 02. Common Opportunistic Infections
33/53
Case 1: worsening,
postHAART
Am J Roentgenol2000; 174: 43-9
Case 2: pretreatment
-
8/2/2019 02. Common Opportunistic Infections
34/53
Case 2: pretreatment
Am J Roentgenol2000; 174: 43-9
C 2 i tHAART
-
8/2/2019 02. Common Opportunistic Infections
35/53
Case 2: worsening postHAART
Am J Roentgenol2000; 174: 43-9
C fi ll i d
-
8/2/2019 02. Common Opportunistic Infections
36/53
Case 2: finally improved
Am J Roentgenol2000; 174: 43-9
-
8/2/2019 02. Common Opportunistic Infections
37/53
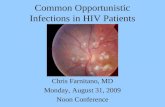
Case 3: pretreatment
Am J Roentgenol2000; 174: 43-9
Case 3: worsening postHAART
-
8/2/2019 02. Common Opportunistic Infections
38/53
Case 3: worsening postHAART
Am J Roentgenol2000; 174: 43-9
P d i l i f TB
-
8/2/2019 02. Common Opportunistic Infections
39/53
Paradoxical worsening of TB
postHAART: PPD conversion
Am J Resp Crit Care Med1998;158: 157-61
Incidence of IRIS HIV
-
8/2/2019 02. Common Opportunistic Infections
40/53
Incidence of IRIS: HIV-
nonHIV; HAART-nonHAART
Am J Resp Crit Care Med1998; 158: 157-61
-
8/2/2019 02. Common Opportunistic Infections
41/53
IRIS: any pretreatment clinical clue?
Am J Resp Crit Care Med1998; 158: 157-61
More extrapulm diseases and
-
8/2/2019 02. Common Opportunistic Infections
42/53
More extrapulm diseases and
lower CD4 in IRIS
Chest2001; 120: 193-7
-
8/2/2019 02. Common Opportunistic Infections
43/53
Delayed HAART until
after 2 months of TBtreatment, regardless of
CD4 count
Am J Respir Crit Care Med2001; 164: 7-12BMJ2002; 324: 802-3
-
8/2/2019 02. Common Opportunistic Infections
44/53
Starting HAART early: CD4
100
AIDS2002; 16: 75-83
-
8/2/2019 02. Common Opportunistic Infections
45/53
Waiting for controlled studies(until then) decision should be
individualized
CDC NIH IDSA StatementMMWRDecember 17, 2004
When to start ART?
-
8/2/2019 02. Common Opportunistic Infections
46/53
Avoid simultaneous prescription
CDC NIH IDSA Statement
MMWRDecember 17, 2004
When to start ART?(contd)mostmost HCPsHCPs wait at least 4wait at least 4--8 weeks8 weeks
Algorithm: focal brain lesions
-
8/2/2019 02. Common Opportunistic Infections
47/53
go t oca b a es o s
Amer i canAmer i canAcademyAcademy
o fo f
Neu ro logyNeu ro logy
1 9 9 71 9 9 7
Algorithm: focal brain lesions
-
8/2/2019 02. Common Opportunistic Infections
48/53
g
Amer i canAmer i canAcademyAcademy
o fo f
Neu ro logyNeu ro logy
1 9 9 71 9 9 7
-
8/2/2019 02. Common Opportunistic Infections
49/53
Algorithm:Toxoplasmic
encephalitis
Montoya&Remington
2000
M b t i i l
-
8/2/2019 02. Common Opportunistic Infections
50/53
Mycobacterium aviumcomplex
Infections at low CD4 count
(likely < 50 ; very likely < 75) No need for clarithromycin susceptibility
testing for primary treatment
(Official Statement of American ThoracicSociety - Am J Respir Crit Care Med
Vol. 156. pp. S1S25, 1997)
M b t i i l
-
8/2/2019 02. Common Opportunistic Infections
51/53
Mycobacterium aviumcomplex:disseminated disease
ART initiated simultaneously or within 1-2
weeks of MAC Rx
US CDC MMW R Dec 17 , 20 04
-
8/2/2019 02. Common Opportunistic Infections
52/53
Cryptococcal meningitis
Cryptococcal Ag titers partially correlatedwith treatment response in HIV-infected
patients
Clin I nfect Dis1994 May;18(5):789-792.
Cryptococcal meningitis (specific)
-
8/2/2019 02. Common Opportunistic Infections
53/53
Cryptococcal meningitis (specific)
treatment problem for Thailand 5-flucytosine not available
Monotherapy with high-dose AmphotericinB - ?adequate
AmB + 400 mg/d fluconazole not sig.different from AmB alone
AmB + 800-1,200 mg/d fluconazole V.S.
AmB alone still ongoing (multicenter trials)