
Substance DITRIBUTION/TRANSPORTATION REGULATION of substances Body PROTECTION.
35
BLOOD
-
Upload
berenice-harper -
Category
Documents
-
view
220 -
download
0
Transcript of Substance DITRIBUTION/TRANSPORTATION REGULATION of substances Body PROTECTION.

BLOOD

FUNCTIONS OF BLOOD (12.1) Substance
DITRIBUTION/TRANSPORTATION REGULATION of substances Body PROTECTION

BLOOD FUNCTIONS: DISTRIBUTION (12.1) Blood transports:
Oxygen from the lungs and nutrients from the digestive tract
Metabolic wastes from cells to the lungs and kidneys for elimination
Hormones from endocrine glands to target organs

BLOOD FUNCTIONS: REGULATION (12.1)
Blood maintains:Appropriate body temperature by absorbing
and distributing heat to other parts of the bodyNormal pH in body tissues using buffer
systemsAdequate fluid volume in the circulatory
system

BLOOD FUNCTIONS: PROTECTION (12.1) Blood prevents blood loss by:
Initiating clot formation when a vessel is broken
Blood prevents infection by: Synthesizing and utilizing antibodiesActivating WBCs to defend the body
against foreign invaders

PHYSICAL CHARACTERISTICS OF BLOOD (12.1)
Average volume of blood:5–6 L for males; 4–5 L for females
Viscosity (thickness) - 4 - 5 (where water = 1)
Average pH of blood is 7.4 Salinity = 0.85%
Reflects the concentration of NaCl in the blood Temperature is 100F
slightly higher than “normal” body temperature
Blood accounts for approximately 8% of body weight

COMPOSITION OF BLOOD (12.2) Blood is the body’s only fluid connective
tissue Liquid = plasma (55%) Formed elements (45%)
Erythrocytes, or red blood cells (RBCs) Leukocytes, or white blood cells (WBCs) Platelets - fragments of cells
BLOOD PLASMA (12.6) Blood plasma components:
Water = 90-92%Inorganic/Organic substances = 6-8%Important for
maintain osmotic pressure of the blood, transport of lipids works as a clotting protein. transportation of nutrients such as glucose
and urea Regulation of blood pH (electrolytes)

COMPONENTS OF WHOLE BLOOD (12.2/12.3)
Withdraw blood and place in tube
1 2 Centrifuge
Plasma(55% of whole blood)
Formed elements
Buffy coat:leukocyctes and platelets(<1% of whole blood)
Erythrocytes(45% of whole blood)
• Hematocrit – the volume percentage of RBC in a
sample of whole blood. • Males: 47% ± 5%• Females: 42% ± 5%

ERYTHROCYTES (RBCS) 12.3
Biconcave disc No nucleus, no centrioles,
no organelles Filled with hemoglobin
(Hb) - 97% of cell contents Essential for carrying oxygen
Most numerous of the formed elements
Dedicated to respiratory transport.
BLOOD CELL PRODUCTION (12.4) Hemopoiesis – blood cell production
Occurs in the red bone marrowAxial skeleton and girdlesEpiphyses (end) of the humerus and femurMarrow contains immature erythrocytes
Erythropoiesis – production of RBC’s.
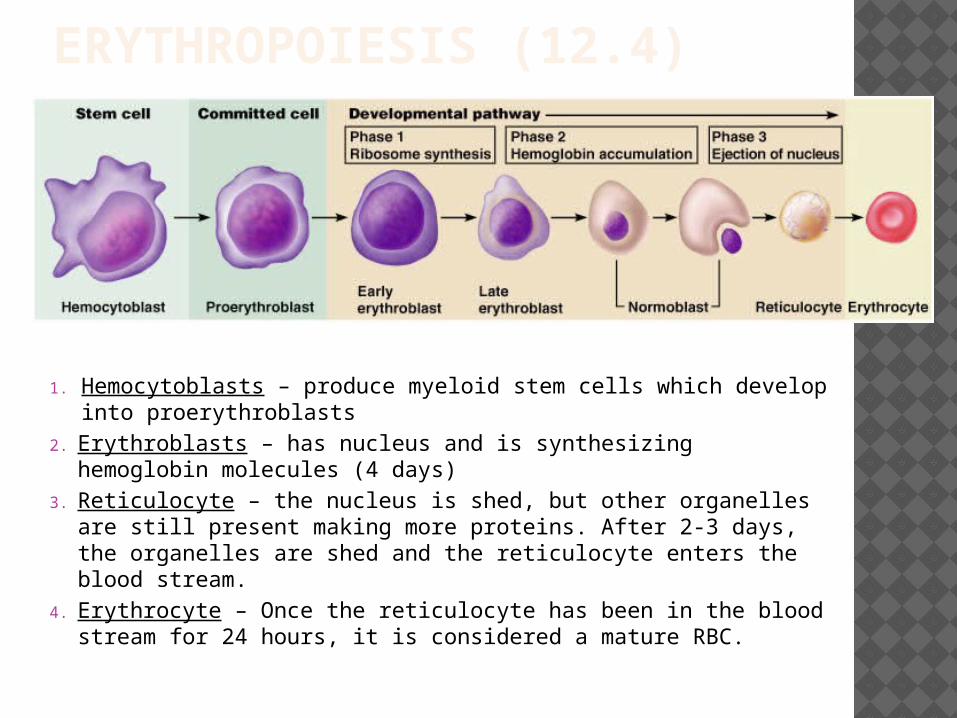
ERYTHROPOIESIS (12.4)
1. Hemocytoblasts – produce myeloid stem cells which develop into proerythroblasts
2. Erythroblasts – has nucleus and is synthesizing hemoglobin molecules (4 days)
3. Reticulocyte – the nucleus is shed, but other organelles are still present making more proteins. After 2-3 days, the organelles are shed and the reticulocyte enters the blood stream.
4. Erythrocyte – Once the reticulocyte has been in the blood stream for 24 hours, it is considered a mature RBC.

FATE AND DESTRUCTION OF ERYTHROCYTES (12.4)
The life span of an erythrocyte is 100–120 daysTravels about 750 miles in that time (Chicago to NYC)
Old erythrocytes become rigid and fragile, and their hemoglobin begins to degenerate
Dying erythrocytes are engulfed by macrophages
Heme and globin are separated Iron is removed from the heme and salvaged for reuse

HORMONAL CONTROL OF ERYTHROPOIESIS Erythropoietin (EPO) release by the
kidneys is triggered by:Hypoxia due to decreased RBCsDecreased oxygen availability Increased tissue demand for oxygen
Enhanced erythropoiesis increases the: RBC count in circulating bloodOxygen carrying ability of the blood
RBC/Oxygen levels EPO release RBC production
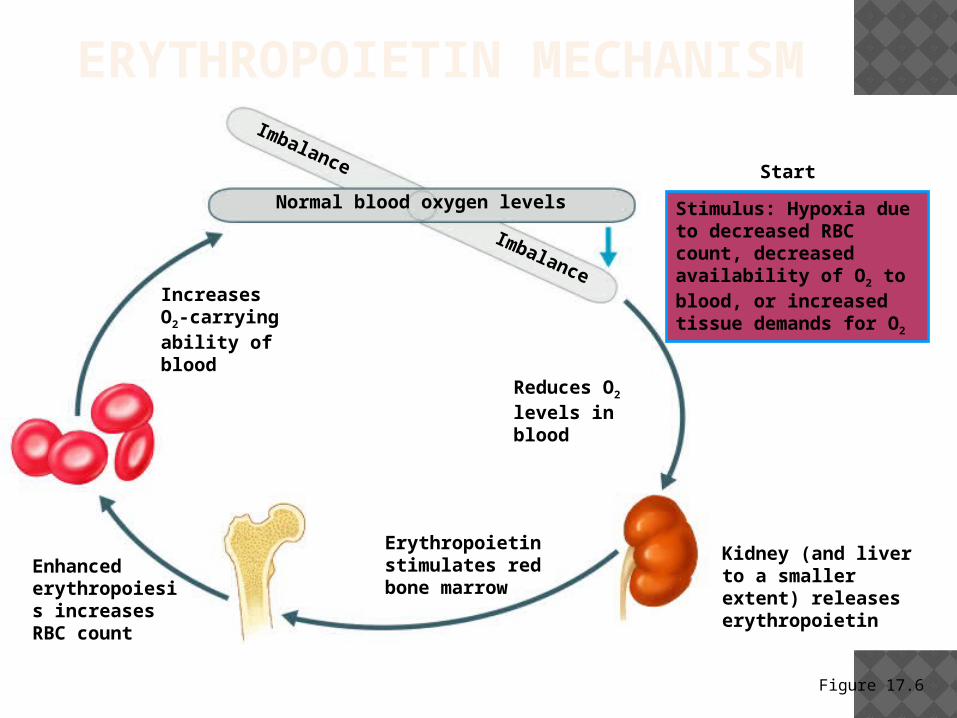
ERYTHROPOIETIN MECHANISM
Figure 17.6
Imbalance
Reduces O2 levels in blood
Erythropoietin stimulates red bone marrow
Enhanced erythropoiesis increases RBC count
Normal blood oxygen levels Stimulus: Hypoxia due to decreased RBC count, decreased availability of O2 to blood, or increased tissue demands for O2
Imbalance
Start
Kidney (and liver to a smaller extent) releases erythropoietin
Increases O2-carrying ability of blood

ERYTHROCYTE DISORDERS Polycythemia
Abnormal excess of erythrocytes Increases viscosity, decreases flow rate of blood
Anemia – blood has abnormally low oxygen-carrying capacityBlood oxygen levels cannot support normal
metabolismSigns/symptoms include fatigue, paleness,
shortness of breath, and chills

ERYTHROCYTE DISORDERS Sickle-cell anemia –
results from a defective geneCodes for an abnormal
hemoglobin called hemoglobin S (HbS)
This defect causes RBCs to become sickle-shaped in low oxygen situations
LEUKOCYTES (WBCS) 12.5 Leukocytes – complete cells with
nucleus and organelles4-8,000/mm3
Number increases in response to bacterial/viral invasion (over 11,000/mm3)
Protect the body from infectious microorganisms

TWO MAJOR TYPES OF WBCS 12.5 Granulocytes include Neutrophils,
Eosinophils, Basophils (ben)Are 2x larger than RBC and
only live for 12 hoursHave lobed nucleiAre all phagocytic cells
Agranulocytes include Monocytes, LymphyocytesLive for months to yearsNormal shaped nucleiLack granules

GRANULOCYTES (12.5) Neutrophils account for 65-75% of WBC
Our body’s bacteria slayers Eosinophils account for 1–4% of WBC
Lead the body’s attack against parasitic infections
Lessen the severity of allergies by phagocytizing immune complexes (ending allergic reactions)
Basophils account for 0.5-1% of all WBC Releases histamine – inflammatory
chemical that acts as a vasodilator and attracts other WBCs

AGRANULOCYTES (12.5) Lymphocytes Account for 20-25% of
WBCThe most important cells of the immune
system T cells - attack foreign cells directly B cells - give rise to cells that produce
antibodies Monocytes account for 3–7% of WBC
They are the largest leukocytesThey leave the circulation, enter tissue, and
differentiate into macrophages

LEUKOCYTE DISORDERS Leukocytosis
WBC count is abnormally high at 11,000 cells per millimeter cubed. This is common during sickness
Leukopenia decrease in WBC count - below 4,800 mm3
Leukemiacancer of WBCBone marrow begins to make abnormal
WBC’s that grow faster, and larger than normal cells.
PLATELETS “THROMBOCYTE” Platelets are small cell fragments
Platelets function in the clotting mechanism by forming a temporary plug that helps seal breaks in blood vessels
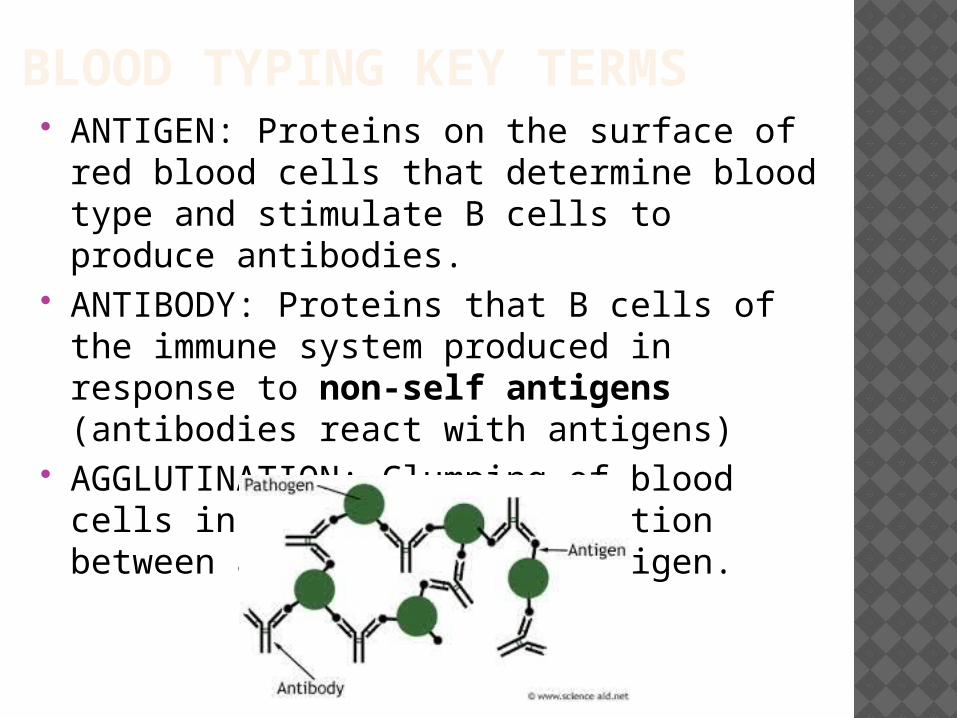
BLOOD TYPING KEY TERMS
ANTIGEN: Proteins on the surface of red blood cells that determine blood type and stimulate B cells to produce antibodies.
ANTIBODY: Proteins that B cells of the immune system produced in response to non-self antigens (antibodies react with antigens)
AGGLUTINATION: Clumping of blood cells in response to a reaction between an antibody and antigen.

HUMAN BLOOD GROUPS (12.9) RBC membranes have antigens on their external surfaces
These antigens are:Unique to the individual Recognized as foreign if
transfused into another individual
Promoters of agglutination Presence or absence of
these antigens is used to classify blood groups

BLOOD GROUPS (12.9)
Humans have 30 varieties of naturally occurring RBC antigens
The antigens of the ABO and Rh blood groups cause vigorous transfusion reactions when they are improperly transfused

ABO BLOOD GROUPS (12.9)
The ABO blood groups consists of:Two antigens (A and B) on the surface of the
RBCs Two antibodies in the plasma (anti-A and
anti-B)

ABO BLOOD GROUPS

RH BLOOD GROUPS (12.9)
85% of the population have the presence of the Rh antigen on RBCs = Rh+
15% - Lack of antigen indicated as Rh–
Anti-Rh are not spontaneously formed only in Rh– individualsOnly after the Rh– individual receives Rh+
blood will the anti-Rh antibodies form.A second exposure to Rh+ blood will result in
a negative transfusion reaction with agglutination.

TRANSFUSION REACTIONS (12.9) Transfusion reactions occur when
mismatched blood is infused Donor’s cells are attacked by the
recipient’s plasma antibodies causing:Diminished oxygen-carrying capacityClumped cells (agglutination) that impede
blood flowRuptured RBCs that release free
hemoglobin into the bloodstream Circulating hemoglobin precipitates in
the kidneys and causes renal failure

FETAL AND MATERNAL BLOOD TYPES (12.10)

FETAL AND MATERNAL BLOOD TYPES (12.10) Rh- mom pregnant with an Rh+ fetus Rh– mother becomes sensitized when Rh+ blood
(from Rh+ baby or a Rh+ transfusion) causes her body to synthesis Rh+ antibodies
In a second pregnancy, Rh+ antibodies of a sensitized Rh– mother cross the placenta and attack and destroy the RBCs of an Rh+ baby
DETERMINE THE BLOOD TYPE.. Has A antigens Universal donor A antibodies Universal recipient AB antigens Both Antibodies Rh factor is present NO antibodies
Type A
Type O
Type B
Type AB
Type AB
Type O
+
Type AB

BLOOD TYPE TESTING (12.9) When serum containing anti-A or anti-B
antibodies is added to blood, agglutination (clumping) will occur.
Positive reactions indicate (clumping)Signifying the correct blood type
*antibodies serum
BLOOD TYPE:
AB-
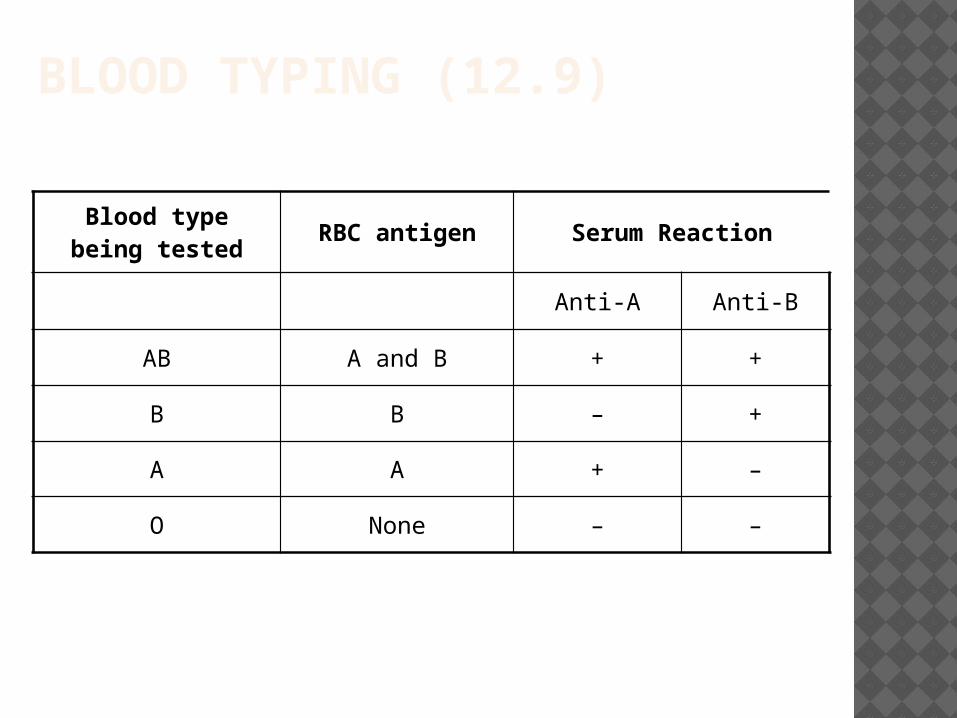
BLOOD TYPING (12.9)
Blood type being tested
RBC antigen Serum Reaction
Anti-A Anti-B
AB A and B + +
B B – +
A A + –
O None – –


















