Specific topics of interest are: ◦ Infant and child mortality ◦ Adult mortality ◦ Infectious...
49
-
Upload
regina-lester -
Category
Documents
-
view
217 -
download
2
Transcript of Specific topics of interest are: ◦ Infant and child mortality ◦ Adult mortality ◦ Infectious...


Specific topics of interest are: ◦ Infant and child mortality ◦ Adult mortality ◦ Infectious diseases
– new interest in Neglected Tropical Diseases ◦ Inherited diseases ◦ Serious injuries ◦ Health and Pregnancy/Childbirth ◦ Nutritional Status of both children and adults ◦ Mental Health
New interest in research related to child mental health from children left behind by parents who migrate to work (China)

1. Almost ½ of low life expectancy is due to high infant and child mortality.
2. Vaccinations to children and infants can reduce infant mortality• UNICEF and WHO had a huge campaign in
1980's and 1990's that did this, resulting in much lower infant and child mortality rates. (vaccines were measles, diphtheria, pertussis, tetanus, polio)
• 45% of deaths are due to infectious diseases or parasites in developing countries (5% in developed countries)
3. Oral rehydration therapy (ORT) dramatically reduces deaths due to infant diarrhea.
Source: 1993 World Development Report

Difference by income:
Source: 2011 World Health Report
Distribution of causes of death
Low Income High Income
HIV/AIDs 3% 0%
Diarrhea 18% 1%
Measles 1% 0%
Malaria 13% 0%
Pneumonia 18% 3%
Prematurity 9% 22%
Birth asphyxia 8% 7%
Neonatal sepsis 6% 2%
Congenital anomalies 2% 23%
Other 18% 32%
Injury 3% 9%

Differences by income
Source: 1993 World Development Report
Distribution of causes of death
Low Income High Income
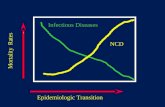
Communicable 72% 7%
Non-communicable 18% 77%
Injuries 10% 15%

Observation: Technological developments in health care are increasing. However - the cost of providing some kinds of "high-tech" health care can be very expensive.
Observation: Continuing problem that diseases evolve to become resistant to treatments (e.g. tuberculosis), and new diseases emerge (e.g. AIDS)
Reasons for Government Intervention (in terms of economic theory)1. Distributive: i.e. basic health care is a right 2. Externalities from communicable diseases3. Other market imperfections, e.g. lack of markets for
health insurance4. Lack of information on the part of many households

1. Provision of public health services ◦ immunization campaigns, visits by health workers to
homes and schools, construction of sewage treatment plants, reduce pollution, public education campaigns
2. Pricing policies ◦ subsidization of “essential” drugs and health
services, price controls on private providers, prices of all services offered by government health facilities, reducing distance to health facilities, prices of goods that effect health - alcohol and tobacco
3. Research on new methods to treat health problems (research is a public good).
◦ Most research is done in developed countries.4. Policies that promote equitable economic
growth5. Increase education, especially education of
women

Percentage reduction in child mortality, relative to mother having no schooling: Mother Mother has 4-6 years has 7+ years schooling schooling
Indonesia -35% -65% Kenya -31% -53% Morocco -45% -64% Peru -39% -72%
Source: 1993 World Development Report

Goal 4: Reduce child mortality ◦ Target 4.A. Reduce by two-thirds, between 1990 and
2015, the under-five mortality rate 4.1 Under-five mortality rate 4.2 Infant mortality rate 4.3 Proportion of 1 year-old children immunized against
measles
http://www.mdgmonitor.org/index.cfm

Goal 4: Reduce child mortality ◦ Target 4.A. Reduce by
two-thirds, between 1990 and 2015, the under-five mortality rate 4.1 Under-five
mortality rate 4.2 Infant mortality rate 4.3 Proportion of 1 year-
old children immunized against measles

Goal 4: Reduce child mortality ◦ Target 4.A. Reduce by
two-thirds, between 1990 and 2015, the under-five mortality rate 4.1 Under-five
mortality rate 4.2 Infant mortality rate 4.3 Proportion of 1 year-
old children immunized against measles

Goal 4: Reduce child mortality ◦ Target 4.A. Reduce by
two-thirds, between 1990 and 2015, the under-five mortality rate 4.1 Under-five mortality
rate 4.2 Infant mortality
rate 4.3 Proportion of 1 year-
old children immunized against measles


Goal 4: Reduce child mortality ◦ Target 4.A. Reduce by two-
thirds, between 1990 and 2015, the under-five mortality rate 4.1 Under-five mortality rate 4.2 Infant mortality rate 4.3 Proportion of 1 year-old
children immunized against measles

Goal 4: Reduce child mortality ◦ Target 4.A. Reduce by two-thirds, between 1990 and 2015, the
under-five mortality rate 4.1 Under-five mortality rate 4.2 Infant mortality rate 4.3 Proportion of 1 year-old children immunized against measles

Goal 5: Improve maternal health ◦ Target 5.A. Reduce by three-quarters, between 1990
and 2015, the maternal mortality ratio ◦ 5.1 Maternal mortality ratio◦ 5.2 Proportion of births attended by skilled health personnel
◦ Target 5.B: Achieve, by 2015, universal access to reproductive health 5.3 Contraceptive prevalence rate 5.4 Adolescent birth rate 5.5 Antenatal care coverage (at least one visit and at least
four visits) 5.6 Unmet need for family planning
http://www.mdgmonitor.org/index.cfm

Goal 5: Improve maternal health ◦ Target 5.A. Reduce by
three-quarters, between 1990 and 2015, the maternal mortality ratio ◦ 5.1 Maternal mortality
ratio◦ 5.2 Proportion of births
attended by skilled health personnel

Goal 5: Improve maternal health ◦ Target 5.A. Reduce by three-quarters, between 1990
and 2015, the maternal mortality ratio ◦ 5.1 Maternal mortality ratio◦ 5.2 Proportion of births attended by skilled health
personnel

Goal 5: Improve maternal health ◦ Target 5.B: Achieve, by
2015, universal access to reproductive health 5.3 Contraceptive prevalence
rate 5.4 Adolescent birth rate 5.5 Antenatal care
coverage (at least one visit and at least four visits)
5.6 Unmet need for family planning

Goal 5: Improve maternal health ◦ Target 5.B: Achieve, by 2015,
universal access to reproductive health 5.3 Contraceptive prevalence
rate 5.4 Adolescent birth rate 5.5 Antenatal care coverage (at
least one visit and at least four visits)
5.6 Unmet need for family planning

Goal 6: Combat HIV/AIDS, malaria, and other diseases ◦ Target 6.A. Have halted by 2015 and begun to reverse the spread
of HIV/AIDS ◦ 6.1 HIV prevalence among population aged 15-24 years ◦ 6.2 Condom use at last high-risk sex◦ 6.3 Proportion of population aged 15-24 years with comprehensive correct
knowledge of HIV/AIDS◦ 6.4 Ratio of school attendance of orphans to school attendance of non-
orphans aged 10-14 years
◦ Target 6.B Achieve, by 2010, universal access to treatment for HIV/AIDS for all those who need it◦ 6.5 Proportion of population with advanced HIV infection with access to
antiretroviral drugs
◦ Target 6.C. Have halted by 2015 and begun to reverse the incidence of malaria and other major diseases ◦ 6.6 Incidence and death rates associated with malaria ◦ 6.7 Proportion of children under 5 sleeping under insecticide-treated
bednets◦ 6.8 Proportion of children under 5 with fever who are treated with
appropriate anti-malarial drugs◦ 6.9 Incidence, prevalence and death rates associated with tuberculosis◦ 6.10 Proportion of tuberculosis cases detected and cured under directly
observed treatment short course
http://www.mdgmonitor.org/index.cfm

http://ddp-ext.worldbank.org/ext/GMIS/home.do?siteId=2
Goal 6: Combat HIV/AIDS, malaria, and other diseases ◦ Target 6.1. Have halted
by 2015 and begun to reverse the spread of HIV/AIDS ◦ 6.1 HIV prevalence
among population aged 15-24 years
◦ 6.2 Condom use at last high-risk sex
◦ 6.3 Proportion of population aged 15-24 years with comprehensive correct knowledge of HIV/AIDS
◦ 6.4 Ratio of school attendance of orphans to school attendance of non-orphans aged 10-14 years

Goal 6: Combat HIV/AIDS, malaria, and other diseases ◦ Target 6.1. Have halted by 2015 and begun to reverse
the spread of HIV/AIDS ◦ 6.1 HIV prevalence among population aged 15-24 years

http://ddp-ext.worldbank.org/ext/GMIS/home.do?siteId=2
Goal 6: Combat HIV/AIDS, malaria, and other diseases ◦ Target 6.1. Have halted
by 2015 and begun to reverse the spread of HIV/AIDS ◦ 6.1 HIV prevalence among
population aged 15-24 years
◦ 6.2 Condom use at last high-risk sex
◦ 6.3 Proportion of population aged 15-24 years with comprehensive correct knowledge of HIV/AIDS
◦ 6.4 Ratio of school attendance of orphans to school attendance of non-orphans aged 10-14 years

http://ddp-ext.worldbank.org/ext/GMIS/home.do?siteId=2
Goal 6: Combat HIV/AIDS, malaria, and other diseases ◦ Target 6.B Achieve, by
2010, universal access to treatment for HIV/AIDS for all those who need it◦ 6.5 Proportion of
population with advanced HIV infection with access to antiretroviral drugs

http://ddp-ext.worldbank.org/ext/GMIS/home.do?siteId=2
Goal 6: Combat HIV/AIDS, malaria, and other diseases ◦ Target 6.B Achieve, by
2010, universal access to treatment for HIV/AIDS for all those who need it◦ 6.5 Proportion of
population with advanced HIV infection with access to antiretroviral drugs

http://ddp-ext.worldbank.org/ext/GMIS/home.do?siteId=2
Goal 6: Combat HIV/AIDS, malaria, and other diseases ◦ Target 6.C. Have halted by 2015 and begun to reverse
the incidence of malaria and other major diseases ◦ 6.6 Incidence and death rates associated with malaria ◦ 6.7 Proportion of children under 5 sleeping under
insecticide-treated bednets◦ 6.8 Proportion of children under 5 with fever who are treated
with appropriate anti-malarial drugs◦ 6.9 Incidence, prevalence and death rates associated with
tuberculosis◦ 6.10 Proportion of tuberculosis cases detected and cured under
directly observed treatment short course

http://ddp-ext.worldbank.org/ext/GMIS/home.do?siteId=2

Goal 6: Combat HIV/AIDS, malaria, and other diseases ◦ Target 6.C. Have halted by
2015 and begun to reverse the incidence of malaria and other major diseases ◦ 6.9 Incidence, prevalence and
death rates associated with tuberculosis

Goal 7: Ensure environmental sustainability ◦ Target 7.C. Halve, by 2015, the proportion of people
without sustainable access to safe drinking water and basic sanitation 7.8 Proportion of population using an improved drinking water source 7.9 Proportion of population using an improved sanitation facility

Goal 7: Ensure environmental sustainability ◦ Target 7.C. Halve, by
2015, the proportion of people without sustainable access to safe drinking water and basic sanitation 7.8 Proportion of population
using an improved drinking water source
7.9 Proportion of population using an improved sanitation facility

Goal 7: Ensure environmental sustainability ◦ Target 7.C. Halve, by 2015, the proportion of people without
sustainable access to safe drinking water and basic sanitation 7.8 Proportion of population using an improved drinking water source 7.9 Proportion of population using an improved sanitation facility

Goal 7: Ensure environmental sustainability ◦ Target 7.C. Halve, by 2015, the proportion of people without
sustainable access to safe drinking water and basic sanitation 7.8 Proportion of population using an improved drinking water source 7.9 Proportion of population using an improved sanitation facility

Child health-education linkages (2 studies)1. Martorell, Habricht and Rivera (1995) INCAP
nutritional project in Guatemala. ◦ Basics: randomly chosen 4 villages were randomly
assigned into 2 groups Group 1 (2 villages): children and expecting moms got a high
energy/high-protein drink called "Atole“ children received a low energy/low protein drink called "Fresco".
◦ Results: After a decade of following the children children in Atole villages showed height/weight gains, greater
work capacity (especially among boys) and gains in some cognitive measures that are likely to be linked to school performance
this was one of the most convincing studies to date that childhood nutrition and health affect subsequent life outcomes.

Child health-education linkages (2 studies)2. Miguel and Kremer (2004) “Worms and Schooling in Rural Kenya◦Evaluated the Primary School Deworming Project (PSDP) in Busia, Kenya on education◦Basics: 75 schools with 32,565 primary students (7-17 years old)
90% of students were infected with helminths Schools were randomly divided into 3 groups of 25 school
Group 1 Group 2 Group 3
1998 treatment
1999 treatment treatment
2000 treatment treatment
2001 treatment treatment treatment

Child health-education linkages (2 studies)2. Miguel and Kremer (2004) “Worms and Schooling in Rural Kenya◦Results:◦treatment schools received ⇓in helminth infections, ⇓ in kids reporting being sick, ⇑ in HAZ scores, ⇓ in anemia. ◦⇓ in absenteeism and increase in school participation among youngest primary school children (grade 4 and below). ◦deworming ⇓ worm burden and ⇑ school participation among untreated children in the treatment schools and among children in neighboring primary schools

Child health-education linkages (2 studies)2. Miguel and Kremer (2004) “Worms and Schooling in Rural Kenya◦Points
failure to take into account these externalities into account would lead one to substantially underestimate the cost effectiveness of deworming
As a result of this study: most LDCs can receive donations of deworming medications for all (cost os $.02/pill 1-2x per year).
◦However: limited results on deworming effects on academic/cognitive test scores

Parent health-education linkages (4 studies)1. Case, Paxson and Ableidinger (2002): 10 SSA
countries between 1992-2000 to estimate the impact of parent death on school enrollment.
Find that orphans are less likely to be enrolled in school than non-orphans.
Orphans are more likely to stay with distant relatives who may have less genetic incentives to care for these children
2. Gertler, Levine and Ames (2004): use panel data in Indonesia in the 1990s.
Find that parent death during past 12 months leads to a doubling of probability that child drops out of school that year.

Parent health-education linkages (4 studies)3. Ainsworth, Beegle and Koda (2002): Study
children in northwestern Tanzania Find that school enrollment is unaffected by parent
death for non-poor households, whereas for poor households they find that enrollment is delayed for younger children and unaffected by older children.
Why mixed results?? 2 theories when the local orphan rates surpass a critical level, the
insurance networks breakdown. it is possible that HIV/AIDs victims were somewhat better off
(income wise) because they worked as: truckers, soldiers, teachers and prostitutes - relatively affluent jobs. Thus negative effects of death may be obscured...

Parent health-education linkages (4 studies)4. Evans and Miguel (2003): Kenya deworming dataset, look only
at kids whose parents were alive in 1998 and compare those children whose parents died during 1998-2002 with those that did not die.
Findings: ◦ parent death has a large effect on school participation rate, it does not
matter which parent dies◦ Participation rates drop sharply the year of the death and continue to
fall for up to 3 years.◦ the magnitude of the effect is smaller than the magnitude of eliminating
one worm infection a year◦ the effect of parent death is similar to the estimated impact of several
measures of poverty (households without latrines/toilets have similar participation rates)
◦ children from poorest households have greatest reduction in participation rates

Why is there little demand for health care among the poor? Visit: Udaipur District in western India◦ Rural, very poor village: 40% below the official poverty line
46% males illiterate & 11% females illiterate 21% have electricity
◦ Health status: most had very low BMI 80% were anemic work functioning was poor (>30% could not walk 5k, draw water or
work in the fields.)
◦ People seemed worried about their health See doctor about 0.5 visits per month per adult 7% of personal consumption expenditures is on heath 60% of visits
are to private doctor 20% to public (government) doctor 20% to bhopas (traditional healer) Poorest 1/3 most likely to see bhopa and richest 1/3 most likely to
see private doctor.

Why don’t they see public doctors? ◦ Public (gov) doctors are closest to village, more qualified
to treat and cheaper. Why little demand?◦ Supply side problems
the public facility is closed more than 1/2 of the time during regular hours and nurses don't show up to work
◦ Demand side problems: private doctors pander to what people want (medicine, shot
or a drip). Public doctors are said to provide less treatment and less
injectables

Why don’t the poor see public doctors? ◦ When do the poor see doctors?
fever, diarrhea, vomiting, upper abdominal pain (acute conditions that are likely to be self-limiting)
◦ When do they not seek treatment? * weakness, backache, pain during urination, hearing loss, chest pain,
memory loss, weight loss (these are chronic conditions that are often life-threatening)
◦ When do they see a bhopa? chronic, potentially life-threatening conditions. Why? Perhaps because the Bhopa provides some emotional support
and comfort whenthey don't expect to get well.
◦ Point: The poor may spend money on the wrong conditions. The poor get treatment, but incorrectly (lots of injections, antibiotics and
steroids). Since health care providers really might not have resources help the
chronic conditions, the poor seek providers to get comfort about doing some thing about acute conditions.

Policy Research Question: What do we gain from supply side intervention (will demand follow?) Or what do we gain from demand side intervention?
Two studies:1. Problem of non- attendance of government nurses. There
was no incentive to come to work because no one monitors them. Organization (Seva Mandir) proposed to monitor.◦ Intervention: a program to required monitoring of nurse attendance
at public health facilities (treatment facilities). ◦ Result: In the first 6 months, the results showed that the program
was initially quite effective; the rate of presence increased from 25% to 40%. Result: Monitoring had no effect on demand for services
Perhaps change is slow◦ Result: program failed after 6 months (system did not work well
because nurses protested... other internal problems).

Policy Research Question: What do we gain from supply side intervention (will demand follow?) Or what do we gain from demand side intervention?
Two studies:2. Problem of lack of child immunizations. A baseline study
revealed only 2.63% of children between ages 1-5 were fully immunized. Also 57.7% never received any vaccines.◦ Intervention: To increase parent demand for vaccines, a
program gave 1 kg of dal (dried lentils, peas or beans) for each immunization and set of plates for completing immunization.
◦ Result: It worked, affecting demand was easier in this case and might provide a basis for affecting supply.

We question again: Why is there a low demand for health? In particular, a low demand for preventative health care?
There exist technologies that are known to be effective and cheap ways to promote good health◦ Bed nets for malaria, immunization, breast feeding, ORS (oral
rehydration salts), bleach for water◦ Further studies have shown that a child not exposed to malaria in
Childhood would have an income 50% higher for all their life-time than a child exposed to malaria
Investments in malaria control measures seem highly cost effective◦ Why are the poor not spending on preventative health care?

Why are the poor not spending on preventative health care? ◦ Is it that people really don't care about their health care?
They do care, recall in the Udaipur survey they spent 7% per month on health care.
Most of this was spent to cure (not to prevent)◦ Is it that governments are to blame?
To some degree yes. Nurses are often absent Governments doctors and nurses do not treat patient very
well: 3 minutes, 3 questions, 3 medicines! When services are good, people do not always get them:
for example in the immunization camps, only 12% of people got all the shots: there is something about demand, not only about supply!

2 Problems with demand for preventative care1. It is difficult for the poor to know what works
For example: many diseases are ‘self-limiting’. They get better on their own after being worst.
Thus if you believe you need a shot (and can get a doctor to give you one) and you eventually get better. Tendency to attribute the health to a shot, when really it would have gotten better on its own.
Tendency to overmedicate! But that is not what really works!
2. Benefits are in the future and the cost is now. With Preventative care, you are taking action (vaccines) to prevent
something from happening….a long time after the fact. For many drawing the link is difficult.
Human tend to put too much weight on the present, relative to the entire future. Parents may intend every month that they will get the immunization next month…. But something else comes up, and they don't end up doing it.

Policy: Large benefits from making things easy/automatic for people:
1. Free Chlorine dispenser right where you collect your water2. Small incentives for immunization/compulsory
immunization if you can pull it off3. In many cases, the superficial cost benefit analysis gives
you the wrong answer.◦ Charging a small amount may be counter-productive◦ Giving people small incentives may save you money
4. The role of learning and trust is key◦ Because preventive care is hard to teach, need to maintain
trust: important for governments to chose their battles.