
Maggie Schroeder, MA, CADC Branch Manager Dept. Behavioral Health, Development and Intellectual...
78
WOMEN AND SUBSTANCE ABUSE
-
Upload
garry-hopkins -
Category
Documents
-
view
212 -
download
1
Transcript of Maggie Schroeder, MA, CADC Branch Manager Dept. Behavioral Health, Development and Intellectual...

WOMEN AND SUBSTANCE ABUSE

Presenters
Maggie Schroeder, MA, CADC
Branch Manager
Dept. Behavioral Health, Development and Intellectual Disabilities; Adult Substance Use Treatment and Recovery Services Branch
502-782-6188 [email protected]
ov
Katie Stratton, MS, LPCA
Training and Development Specialist
Dept. Behavioral Health, Development and Intellectual Disabilities; Adult Substance Use Treatment and Recovery Services Branch
502-782-6192 [email protected]
Biopsychosocial Differences
Biological
PsychologicalSociological

Biological Differences
BiologicalIntoxication Rate
Telescoping Effect
Medical Complications
Reproductive and Hormonal
Genetic Risk

Intoxication RateWomen’s bodies respond to alcohol differently
Lower proportion of water, women have less than men pound for pound (NIH, 2013)
Lower activity of alcohol dehydrogenase in gastric mucosa (Back, Contini, and Brady, 2006)
At similar levels of alcohol consumption, women: Have higher blood alcohol concentrations Have a higher risk of psychosocial problems
(stressful life experiences, interpersonal stressors) resulting in dependence on alcohol (Back, Contini, and Brady, 2006)

Biological Differences
BiologicalIntoxication Rate
Telescoping Effect
Medical Complications
Reproductive and Hormonal
Genetic Risk

Telescoping Effect
When dependence progresses more quickly in women than in men
Women develop more physical problems within fewer years of usage onset

Telescoping Across Substances
At similar levels of alcohol consumption, women:
Develop abuse or dependence in fewer years (telescoping)
Women often become impaired more easily and impairment could last longer
Have more medical problems and higher mortality rates
Bradley, KA, et al. (1998).

Telescoping Effect: Women and Opiates
Faster progression of dependence (telescoping) Faster addiction within 1st year of use Fewer years of use prior to treatment entry
with comparable or more severe addiction severity as men at treatment entry
May be more likely to inject and inject more frequently
By 2011–2013, opioid pain reliever abuse or dependence was more common among heroin users than alcohol, marijuana, or cocaine abuse or dependence.
Zilberman, et al. (2002), Harvard Health Publication (2010), CDC: Morbidity and Mortality Weekly Report (2013)
Stratton, Katie C (BHDID/Frankfort)
Use info from the CDC email copy graph

Telescoping Effects: Women and Opiates Cont…
Women are more likely to visit the emergency rooms because they abuse opioids, suggesting that they suffer more medical consequences.
Women are more likely than men to be prescribed opioids, to use them chronically, and to receive prescriptions for higher doses of opioids
Women also might be more likely than men to engage in "doctor shopping"
CDC: Morbidity and Mortality Weekly Report (2013)

Telescoping Effects:Women and Cocaine
Hormonal fluctuation during the menstrual cycle can increase responsiveness to cocaine cues or more severe use. Back, Contini, & Brady (2006)
Women more often report unsafe sexual and unsafe drug injection practices, increasing risk of sexually transmitted diseases, including HIV (Note: screen women for HIV, Hep B and C, and liver functioning) Zilberman, et al. (2002)
Women report using cocaine at much younger ages than men and quickly develop dependence. Harvard Health Publications (2010)
During 2002–2013, past-year heroin use increased among persons reporting past-year use of other substances. The highest rate was consistently found among users of cocaine; during 2011–2013, this rate was 91.5 per 1,000. During the study period, the largest percentage increase, 138.2%, occurred among nonmedical users of opioid pain relievers.
Biological Differences
BiologicalIntoxication Rate
Telescoping Effect
Medical Complication
s
Reproductive and Hormonal
Genetic Risk

Medical Complications:Mortality Rates
Women have higher mortality rates than men at lower levels of drinking
Higher relative risk of death from cirrhosis, cancer, and injury
Risk increases for women who drink more than 2 to 3 drinks a day Risk for men increases at four or more drinks
per day
Bradley, KA, et al. (1998).
Medical Complications: Liver Disease
Women who drink are more likely to develop alcoholic hepatitis then men who drink the same amount (NIH, 2013)
Women more likely to develop and die from liver disease than men drinking at comparable levels
Risk of liver disease and cirrhosis increases when women drink 7 drinks per week and men drink 14 drinks per weekBradley, KA, et al. (1998).

Medical Complications: Neurologic
More sedation with equivalent BAL Quicker brain shrinkage, peripheral
neuropathy
Bradley, KA, et al. (1998).

Medical Complications: Heart Disease
Chronic heavy drinking is the leading cause of heart disease. Among heavy drinkers, women are more susceptible to alcohol related heart disease than men (NIH, 2013)
Female smokers are 2x more likely to have a heart attack

Medical Complications: Breast Cancer
Women who consume about one drink per day have a 10% higher chance of developing breast cancer than women who do not drink at all.
For every extra drink they have per day, increases that risk by 10% more

Medical Complications:Women and Opioids
More severe psychiatric, medical, and employment complications (Hernandez-Avila, et al., 2004)
Increased frequency of medical problems, especially genitourinary and respiratory (Zilberman, et al., 2002)
More likely to accept needles from HIV+ associates and have multiple sex partners/get paid for sex than male users (Eaves, 2004)

Medical Complications:Neonatal Abstinence Syndrome (NAS)
Abuse or Opioids during pregnancy is a problem for women of child-bearing age
Health-care providers should include discussions of pregnancy plans within the context of treatment and monitoring of patients taking Opioids for medical or nonmedical reasons.
Women treated for Opioid abuse should be counseled regarding
risks to the fetus during pregnancy. The risks and benefits of treatment of chronic conditions with Opioids during pregnancy should be weighed carefully.
Use of benzodiazepines and antidepressants during pregnancy, or at any time in combination with Opioids, also should be considered carefully by women and their health-care providers. Psychological conditions, which might co-occurr with pain or substance abuse, need to be assessed and addressed within a treatment regime.
CDC: Morbidity and Mortality Weekly Report (2013)

Medical Complications:Women and Cocaine
Greater risk for cardiovascular complications and other cocaine-related emergencies (Hernandez-Avila, et al., 2004)

Medical Complications:Women and Injection Drug Use
Medical Complications:Women and Cannabis
Gender-specific impairment on visuospatial recall memory
Overall neuropsychologic impairment more prominent in males
Zilberman, M., Tavares, H., Blume, S., and el-Guebaly, N. (2002).

Biological Differences
BiologicalIntoxication Rate
Telescoping Effect
Medical Complications
Reproductive and
HormonalGenetic Risk

Reproductive and Hormonal Consequences
Infertility (6 or more drinks > 5 times/week; opiates)…but low use of contraception
Spontaneous abortion (> 2 drinks/day) Menstrual symptoms (irregular, painful,
heavy) Disrupted sex hormones Breast cancer (2-5 drinks/day) Uterine and ovarian cancers Early menopause
Bradley, et al. (1998), Harding and Ritchie (2003) and Zilberman, et al. (2002).

Reproductive Consequences: Prenatal Exposure
First trimester use of alcohol– low birth weight, decreased birth length and head circumference, minor physical anomalies, and fetal alcohol effects
Second and third trimester use of alcohol– developmental delay, adverse psychosocial/behavioral/physical/intellectual consequences
Prenatal use of drugs can cause low birth weight, preterm labor, hard-to-sooth infants, neonatal abstinence syndrome, possibly some emotional/learning problems
Bradley, KA, et al. (1998).

Reproductive Hormones
Women appear to have a greater subjective response to cocaine and amphetamine, especially during follicular phase of menstrual cycle Back, Contini, Brady (2006)
Preliminary research suggests that women who time their quit date to occur during the follicular phase (which begins after menstruation and ends at ovulation) are more likely to abstain from cigarettes for a longer period than women who quit during the luteal phase.
One theory is that the increase of estrogen levels during the follicular phase decreases anxiety and improves mood, helping a woman cope better with the challenges of smoking cessation.

Biological Differences
BiologicalIntoxication Rate
Telescoping Effect
Medical complications
Reproductive and Hormonal
Genetic Risk

Genetic Risk
50-60% of risk in males attributed to heritability
Research less clear for females Fewer female subjects in studies
Twin studies show similar genetic risk for females
Prescott, 2002

Sociological Differences
Sociological
Rate Differenc
esStigma
Financial and Employment
Discrepancies
Childcare Responsibilities
Other Barriers to Services
Assortative Mating

Rate Differences:Usage Rates
Men are more likely to drink and more likely to be heavy drinkers
Men drink larger quantities, drink more frequently, and report more problems
Male: Female ratios range from 4:1 to 8:1Wilsnack, S. and Wilsnack, R. (1994).
Rate Differences:Opioid Overdose Deaths
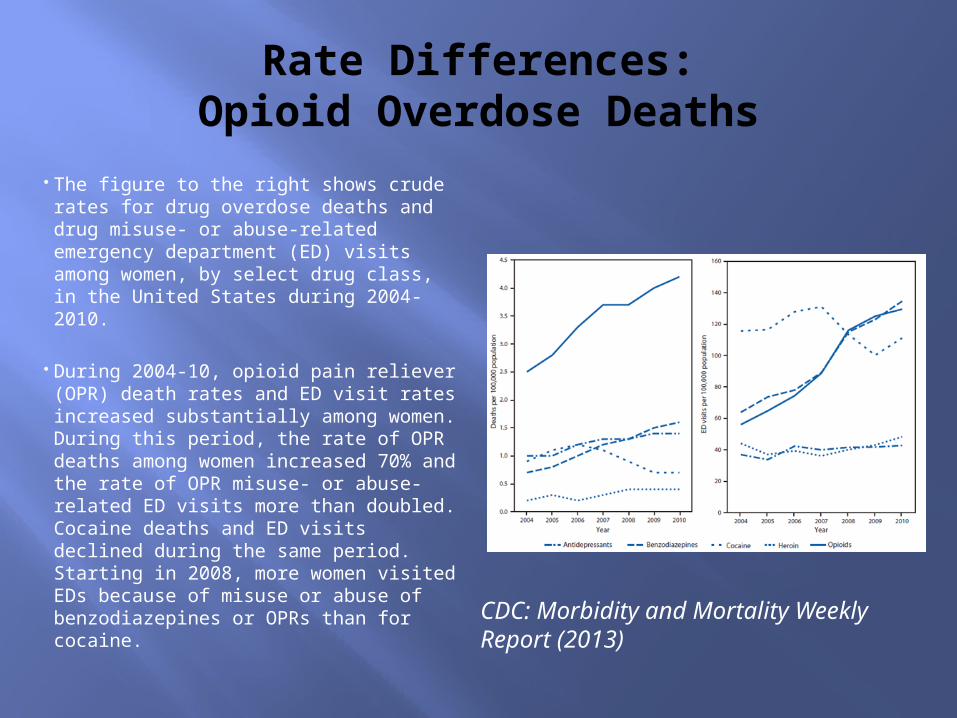
The figure to the right shows crude rates for drug overdose deaths and drug misuse- or abuse-related emergency department (ED) visits among women, by select drug class, in the United States during 2004-2010.
During 2004-10, opioid pain reliever (OPR) death rates and ED visit rates increased substantially among women. During this period, the rate of OPR deaths among women increased 70% and the rate of OPR misuse- or abuse-related ED visits more than doubled. Cocaine deaths and ED visits declined during the same period. Starting in 2008, more women visited EDs because of misuse or abuse of benzodiazepines or OPRs than for cocaine.
CDC: Morbidity and Mortality Weekly Report (2013)

Rate Differences:Opioid Overdose Deaths
Death rates varied by age and race. The rate for all drug overdose deaths among women was highest among those aged 45–54 years (21.8 per 100,000 population). American Indian/Alaska Native (14.5) and non-
Hispanic white (12.7) women had the highest drug overdose death rates.
The rate of suicide drug overdose deaths was similar for women (1.8) and men (1.7), although drug overdose–related suicide deaths accounted for 34% of all suicide deaths among women compared with 8% among men. OPRs were involved in one in 10 suicides among women.CDC: Morbidity and Mortality
Weekly Report (2013)

Rate Differences:Heroin

However…
High school girls are catching up
0 10 20 30 40 50 60
Tobacco
Alcohol
Painkillers
Stimulants
Tranquilizers
Cocaine
Inhalents
Marijuana
Boys
Girls
CASA (2003).
…they’re starting younger…
~30% of girls have smoked < age 13 ~35% of girls have tried alcohol < age 13 ~9% of girls have tried THC< age 13
Early puberty is a risk factor for girls
CASA (2003).

…and using more substances…

International Studies
Males use at higher rates in all countries studied Large variation in differences between men
and women May be a biological basis, but may also be
social forces Women are known to use substances at
rates similar to males when the substances are available to them
Wilsnack and Wilsnack, 2002

Sociological Differences
SociologicalRate Differences
StigmaFinancial and Employment
Discrepancies
Childcare Responsibilities
Other Barriers to Services
Assortative Mating

Stigma
Shame Social marginalization Degradation ATOD use = slut or prostitute Parenting ability disputed (Kandall, 1998,
and Ehrmin, 2001) In younger cohorts, attitudes more
permissive (Hernandez-Avila, et al., 2004)

Sociological Differences
SociologicalRate Differences
Stigma
Financial and
Employment
Discrepancies
Childcare Responsibilities
Other Barriers to Services
Assortative Mating

Financial and Employment Discrepancies
Women make less money than men Women in treatment
More educational deficits Lower employment rates Lack employment skills Fewer economic resources More likely to be single or divorced Have financial burden of children
Wechsberg (1998), Moran (1998), Oggins, Guydish, & Delucchi (2001), Gregoire and Snively (2001)

Sociological Differences
SociologicalRate Differences
Stigma
Financial and Employment
Discrepancies
Childcare Responsibilitie
sOther Barriers to
Services
Assortative Mating

Childcare Responsibilities
Women entering treatment are 2X more likely to have children at home and custody
Childcare issues Fear of losing custody Not want to leave children to go to
treatment
Wechsberg, Craddock, & Hubbard (1998), Moras (1998)

Sociological Differences
SociologicalRate Differences
Stigma
Financial and Employment
Discrepancies
Childcare Responsibilities
Other barriers to servicesAssortative
Mating

Other Barriers to Services
Lack of adequate services Lack of appropriate services Lack of outreach to women Transportation Partner limiting Social support
Marsh (2002)

Sociological Differences
SociologicalRate Differences
Stigma
Financial and Employment
Discrepancies
Childcare Responsibilities
Other Barriers to Services
Assortative
Mating

Assortative Mating
Possibility for an increase in the risk and severity of the disorder in consecutive generations.
Daughters of alcohol-abusing mothers, the rate of alcohol abuse was significantly higher.
Association between personality features and the liability to substance abuse.
Vanyuko, et al. (1996)

Assortative Mating cont…
May lead to further strengthening of the association between the liabilities to substance abuse and other behavioral deviations due to increase in both genetic and environmental mental correlations between the traits.
Females often marry men that present with a similar substance use disorder, men do not. 80% of husbands were alcoholics if at least 1
of her parents were alcoholics compared to 33% of the husbands. Vanyuko, et al. (1996)

Psychological Differences
Psychological
Reasons for using
Co-occurring disorders
Victimization
Relational Strengths and Risks

Males and Females Use for Different Reasons
Girls who use are more likely to be depressed, suicidal, or feel sad and hopeless
Women attribute initial heroin use to social reasons (Eaves, 2004)
Girls tend to use to improve mood, increase confidence, reduce tension, cope with problems, lose inhibitions, enhance sex, or lose weight. Boys use to seek sensation or enhance social status. (CASA, 2003).

Psychological Differences
Psychological
Reasons for using
Co-occurring Disorders
Victimization
Relational Strengths and Risks

Co-Occurring Disorders
(COD)
More common in women than in men Mental Health problems more common in
women than men (general population)

Increased Psychiatric Co-morbidity
0%
10%
20%
30%
40%
50%
60%
70%
SubstanceDependentMen
SubstanceDependentWomen
Bradley(1998), Zilberman et al. (2002)
COD and women Most frequent CODs in women are depression,
anxiety, eating disorders and borderline personality disorders (Most frequent COD in men is Antisocial Personality Disorder) (Back, Continii, & Brady 2006)
Phobic disorders, major depression, panic disorder, somatization, OCD, co-occurring drug abuse (especially Rx), PTSD, bipolar disorder
Suicide attempts more frequent in female alcoholics
Adolescent females with ADHD greater risk for substance abuse
For women the onset of the psychiatric disorder is more likely to antedate the onset of the substance use disorder. (Back, Continii, & Brady 2006)
Zilberman, et al. (2002)

Women and Depression
Depression and anxiety primary dx for women – predates alcohol abuse
Major depression predates alcohol dependence in 2/3 of women; vice versa for men
Among depressed alcoholics: depression is more severe in females, alcoholism more severe in males
Zilberman, et al. (2002)

Implications
The induction of negative mood increases alcohol cue-reactivity and craving in women but not in men
Craving, withdrawal, and premenstrual symptoms often overlap in female smokers
Women with COD more likely to show up in medical or mental health settings, be diagnosed with mental health disorders
Zilberman, et al. (2002)

Weight concerns increase vulnerability to substance use
Substances may be used for weight control, especially nicotine, cocaine, and other stimulants
If try one, likely to try another or two More girls 12-17 use cocaine than boys Disturbed eating usually predates
ATOD Sexual abuse linked with earlier onset
of co-occurring Substance Use and Emotional DisturbancesCASA (2003), Cochrane, Malcolm, & Brewerton (1998), Krahn
(1998), Deep, et al. (1999)

Co-occurring Eating Disorders
30% of SA women have some occurrence of bulimia, only 1-3% of general population
Bulimia most common in SA Electrolyte disturbance can worsen
withdrawal seizures Food deprivation is a stimulant for drug
use in animal and human studies
CASA (2003), Cochrane, Malcolm, & Brewerton (1998), Krahn (1998), Deep, et al. (1999)

Psychological Differences
Psychological
Reasons for using
Co-occurring disorder
Victimization
Relational Strengths and
Risks

Trauma Histories
Compared to women without substance abuse problems, twice as many women with substance abuse problems have a history of sexual abuse
Wilsnack and Wilsnack (1994)

Rates of abuse among women in treatment
Sexual assault: 40-65% Physical assault: 32-58% Both physical and sexual assault in
childhood increases chance of using illicit drugs
One form of violence often co-occurs with other forms
Najavits, Weiss, & Shaw (1997)

Intimate Partner Violence (IPV)
90% of women in treatment have a history of domestic violence (DV)
75% of DV incidents involve alcohol use by the victim, the perpetrator, or both
Crack cocaine use by women on methadone associated with IPV
Vicious cycle of increasing domestic violence and substance abuse
Wilsnack and Wilsnack (1994), Price and Simmel (2002), El-Bassel, et al.(2004)
Stratton, Katie C (BHDID/Frankfort)
instead of on Methadone- as this could be read as they are abusing methadone and Crack cocaine, may stay... Crack Cocaineuse by women in Methadone Treatment associated with IPV

Increased Risk, continued
Quicker onset of substance abuse
Higher rate of substance abuse even when controlling for family background
Severe trauma can damage brain anatomy, increasing vulnerability to mental health and substance abuse problems
CASA (2003)
Stratton, Katie C (BHDID/Frankfort)
Is this slide out of order? the slide before it is not Increased Risk. Should it say IPV Continued?

PTSD and Substance Abuse
Women in substance abuse treatment have 2 to 4 times the rates of PTSD than men
Women in the general population = 11%; women in treatment = 30 to 59% PTSD
Rates of victimization (with or without PTSD) = 55 to 99% of women in treatment
Najavits, Weiss, & Shaw (1997), Sullivan & Holt (2008)

PTSD and Substance Abuse
Women’s trauma is from physical and/or sexual assault (sexual assault more prevalent); men’s is from combat, crime victimization, or general disaster
Women are twice as likely as men to develop PTSD after trauma
Women have high rates of repeated trauma, averaging five traumas each
Najavits, Weiss, & Shaw (1997), Sullivan & Holt (2008)

PTSD and Substance Abuse
Women frequently have family perpetrators
Women have more self-blame, suicide attempts, re-victimization, and sexual dysfunction
Rape most likely to lead to PTSD for women and men (Lifetime rates: 9.2% of women vs. .7% of men are raped)
Najavits, Weiss, & Shaw (1997), Sullivan & Holt (2008)

Clinical Implications: Trauma & PTSD
PTSD symptoms can worsen with initial abstinence and with use
PTSD symptoms can trigger substance use
Traditional models for treating PTSD may not be indicated for substance abuse disorders and vice versa
Trauma counseling helps women avoid drug use and relapse
Najavits, Weiss, & Shaw (1997), Pride & Simmel (2002)
Clinical Implications: Trauma & PTSD cont…
AA may not work for female trauma survivors: men in meetings, not allow discussion of the past, surrendering to a higher power, sharing one’s story publicly
Confrontational approaches can re-evoke traumatic experiences
Uneasy alliances – trust issues Multiple crises Strong negative counter-transference by therapists Frequent labeling as “poor prognosis” and
“treatment failures” Non-compliance with aftercare Less motivation for treatment
Najavits, Weiss, & Shaw (1997), Price & Simmel (2002)

Psychological Differences
Psychological
Reasons for using
Co-occurring Disorders
Victimization
Relational Strengths and Risks

Relational Strengths and Risks
Women are less likely to enter treatment than men possibly due to sociocultural factors
Women tend to have better outcomes than men Higher rates of abstinence at 6-month and 5-
years follow-up Greater improvements in their domains Shorter relapse episodes Most likely to seek help following a relapse
Back, Contini, Brady (2006)

Child Influence on Female Alcoholics
If children are doing well, mother tends to drink less
Importance of assessing children’s well-being
Importance of child care support for women in treatment
Zilberman, et al. (2002),
Parenting
Drug-Dependent Mothers More frequently lose children to foster care Perform worse on parenting indices:
Sensitivity and responsiveness to children’s emotional cues
Understanding of basic child development Reflection on children’s emotion and cognitive
experience Ambivalence about having and keeping children Harsh, threatening, overly-involved, authoritarian or
permissive, neglectful, poor involvement, low tolerance of children, parent-child role-reversals
Suchman, et al., 2004

Partner Influence
Women tend to be introduced to drugs by a male partner
Heroin: adolescent girls introduced by boyfriend or male friend
Women tend to be influenced by the partner’s level of use; men are not
Perceived discrepancies = increased use Previous treatment of partner
Wilsnack and Wilsnack (1994), Eaves (2004), Logan, et al. (2002), Riehman, et al. (2000), Sack (2012)

Partner Influence, Heroin
Women report first narcotic drug was a gift Use because spouse was using Having a spouse who is an addict Being introduced to heroin by an addicted sex
partner Unlikely to inject on own, but will with a sex
partner Use to self medicate for other mental health
problems
Sack, 2012

Partner Influence, continued
Direct or indirect opposition to recovery efforts (intimidation or threats)
Partner resistance Male partners’ attitudes toward
treatment Marital instability Economic dependence Bonding mechanism
Logan, et al. (2002), Riehman, et al. (2000)
Relational Model
Women do less well in mixed-gender groups Don’t talk as much Attend to needs of males in group Less likely to share their needs or feelings
Women-focused outpatient or residential treatments often produce higher rates of treatment completion than traditional programs.
Back, Contini, Brady (2006)

Effective treatment for women
Gender specific: women-only groups Safe: protects women from re-
victimization and re-traumatization Gender responsive: addresses women’s
issues Holistic: understands the whole woman


















