
| AIDS Support and Technical Resources AIDSTAR-One A Systematic Analysis of Three Promising...
44
| AIDS Support and Technical Resources AIDSTAR-One A Systematic Analysis of Three Promising Approaches to Combination HIV Prevention Programming Sharon Stash, Heather Bergmann, Michele Clarke, Peter Okaalet, LaHoma Romocki, Bill Rau, Jim Stansbury Produced by the AIDS Support and Technical Assistance Resources Project, Sector 1, Task Order 1 (AIDSTAR-One), USAID Contract # GHH-I- 00-07-00059-00, funded January 31, 2008. The opinions expressed in this presentation do not necessarily reflect the views of USAID or the U.S. Government.
-
Upload
annabel-johns -
Category
Documents
-
view
213 -
download
0
Transcript of | AIDS Support and Technical Resources AIDSTAR-One A Systematic Analysis of Three Promising...

| AIDS Support andTechnical Resources
AIDSTAR-One
A Systematic Analysis of Three Promising Approaches to
Combination HIV Prevention Programming
Sharon Stash, Heather Bergmann, Michele Clarke, Peter Okaalet,
LaHoma Romocki, Bill Rau, Jim Stansbury
Produced by the AIDS Support and Technical Assistance Resources Project, Sector 1, Task Order 1 (AIDSTAR-One), USAID Contract # GHH-I-00-07-00059-00, funded January 31, 2008.
The opinions expressed in this presentation do not necessarily reflect the views of USAID or the U.S. Government.
| AIDS Support and Technical Resources
Definition
• Combination HIV prevention includes a mix of strategies and risk reduction approaches that use current epidemiological and programmatic evidence to target different audiences with simultaneous behavioral, biomedical, social normative and structural interventions, and that respond to local realities
• “A mix that produces the maximum effect in a given setting” (M. Merson)

| AIDS Support and Technical Resources
Definition
• Cross-cutting components– Community engagement– Policy support – Systems strengthening– Gender

| AIDS Support and Technical Resources
Combination Prevention Case Studies Purpose
• Target audience includes program administrators, managers and planners
• Case studies describe – in good programmatic detail – how combination programs are implemented
• Describing core technical components and operational characteristics of promising combination prevention programs
| AIDS Support and Technical Resources
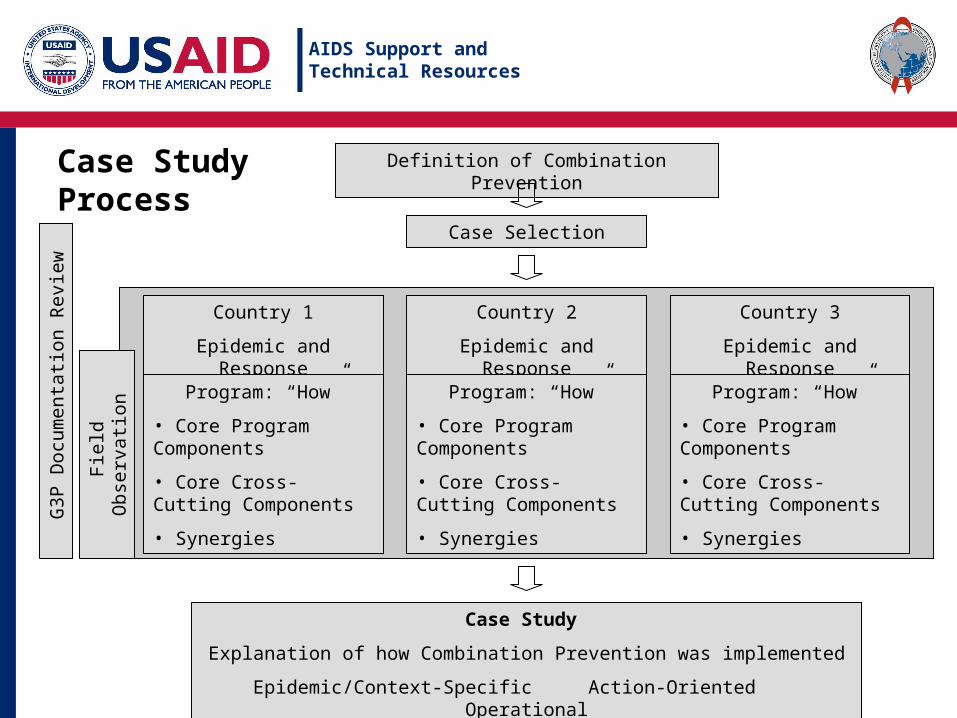
Case StudyProcess
|
Definition of Combination Prevention
Case Selection
Country 1
Epidemic and Response
Country 2
Epidemic and Response
Country 3
Epidemic and Response
Program: “How”
• Core Program Components
• Core Cross-Cutting Components
• Synergies
Program: “How”
• Core Program Components
• Core Cross-Cutting Components
• Synergies
Program: “How”
• Core Program Components
• Core Cross-Cutting Components
• Synergies
Case Study
Explanation of how Combination Prevention was implemented
Epidemic/Context-Specific Action-Oriented Operational
Fie
ld O
bser
vatio
n
G3P
Doc
umen
tatio
n R
evie
w

| AIDS Support and Technical Resources
Selection of Sites for Case Studies
• Recommended by experts• Documentation of the program was collected using
the guideline developed by AIDSTAR-One for Good and Promising Programmatic Practices
• Of about 25 potential cases identified, 3 were selected by a committee of 8 people from AIDSTAR-One partner organizations and USAID
• 2 additional programs remain to be selected
| AIDS Support and Technical Resources
Selected Case Study Sites
• Generalized epidemic settings– APHIA-II Project, Kenya, Family Health International
supported by PEPFAR/USAID– Another 2 sites pending selection in southern Africa
• Concentrated epidemic settings– Avahan-India AIDS Initiative, supported by the Bill & Melinda
Gates Foundation– Alliance-Ukraine, supported by USAID (SUNRISE Project)
and the Global Fund

| AIDS Support and Technical Resources
Core Components of HIV Services• Program uses evidence (epidemiologic and programmatic
data) to target prevention activities – How does the program employ primary and secondary sources of
data? – Does the program address prevention activities to all risk groups?
(directly/linkages)– Is there evidence that the program adapts its activities to new
information? • Program includes a combination of various risk reduction
approaches– Directly or through linkages– Targeted interventions– General population, male circumcision
• Program participants are linked to diagnostic and other treatment services– Facility-based services (e.g., ART, OI, and other treatment
services, care and support, PMTCT)

| AIDS Support and Technical Resources
Cross-Cutting Program Components
• Program engages appropriate leaders and opinion makers• Program involves local communities in different stages of
program development and implementation• Capacity building and management systems strengthening to
strengthen institutions to implement complex combination programs, with multiple linked activities, at scale and understand their effects
• Program understands and addresses gender dimensions that affect the transmission/prevention of HIV

| AIDS Support and Technical Resources
Synergistic Effects – “Program Footprint”
|
Combination Prevention Program
Core Components of HIV Services
Data-based targeting of prevention activities
Includes a combination of various risk reduction approaches (biomedical, behavioral, structural)
Linked to diagnostic, treatment, care and other services
Cross-Cutting
Engages appropriate leaders and opinion makers
- +++
Involves local communities at all levels of program development and implementation
+ ++ +
Capacity building to strengthen management systems to coordinate/implement multiple linked activities at scale, with intensity and quality
+
Addresses gender dimensions
+ -
| AIDS Support and Technical Resources
Case 1:
AIDS, Population and Health Integrated Assistance Program
(APHIA-II)
Kenya

| AIDS Support and Technical Resources
Context: HIV/AIDS in Kenya
• Prevalence (adults 15-49): 7.8%*
• Generalized epidemic– Some populations at higher risk: sex workers (prevalence 27%),
uniformed service members, truck, taxi and boat drivers
– New information on HIV among MSM and IDUs
– Young women are currently experiencing higher prevalence rates than men
• Prevalence has declined
* Source: 2007 Kenyan AIDS Indicator Survey

| AIDS Support and Technical Resources
Case: AIDS, Population and Health Integrated Assistance Program (APHIA-II)
• Use of epidemiologic and programmatic data• Various risk reduction approaches• Participants linked to treatment services• Engages leaders and opinion makers• Involves local communities in program development• Capacity building and strengthening systems
| AIDS Support and Technical Resources
Case: AIDS, Population and Health Integrated Assistance Program (APHIA-II)
• Evidence-based development of field activities using:– KAIS survey data (2007)– Behavioral Monitoring Survey (BHS)– IMPACT final report: lessons learned– Kenyan National Bureau of Statistics– Kenya Demographic Health Survey Reports
• Implementing partners use data:– Provide monitoring and evaluation on all program
components– Use data to adjust activities and workplans

| AIDS Support and Technical Resources
Case: AIDS, Population and Health Integrated Assistance Program (APHIA-II)
• Biomedical risk reduction approaches– VCT, home-based VCT and couples’ VCT– ARV treatment; ARV prophylaxis for MTCT– STI treatment– Family Planning– OVC– * Nyanza – Introduction of male circumcision

| AIDS Support and Technical Resources
Case: AIDS, Population and Health Integrated Assistance Program (APHIA-II)
• Behavioral activities– Abstinence education, be faithful to one partner or limited
partners, and condoms– Prevention for Positives (PCP)– BCC materials specific to target audience– Prevention activities for MSM

| AIDS Support and Technical Resources
Case: AIDS, Population and Health Integrated Assistance Program (APHIA-II)• Structural activities:
– Advocacy for change in social and cultural norms (i.e., female genital mutilation, early marriages, family planning)
– Empowerment: of women, PLWH and youth– Income generating activities– Workplace policies– Private sector involvement– Adult education (literacy)– Political advocacy– Collaborative arrangements with law enforcement– Stigma reduction activities

| AIDS Support and Technical Resources
Case: AIDS, Population and Health Integrated Assistance Program (APHIA-II)• Involving local communities in program development: implementing
partners– Define their scope of work– Representatives participate in provincial and district planning in addition
to their own individual programs
• Capacity-building and systems strengthening– Technical support and training to MOH and implementing partners– Support supervision of service providers– Widely publicized recognition of IP(s) accomplishments– Opportunities for advancements for PE(s)– APHIA-II PE(s) hired by other programs– Regular meetings of all stakeholders– Comprehensive recordkeeping

| AIDS Support and Technical Resources
Case: AIDS, Population and Health Integrated Assistance Program (APHIA-II)• By September 2008, the APHIA-II Rift Valley project alone had
reached– 1,008,967 people with education to increase their skills in remaining
abstinent or faithful
– 1,487,288 people with education and skills building regarding other prevention strategies
– 328,860 people with counseling and testing services
– 12,133 PLWH with ART
– 19,216 PLWH with home-based palliative care
– 29,239 OVC with life-saving services and support
– 166,158 pregnant women with counseling and testing for HIV at PMTCT sites

| AIDS Support and Technical Resources
Case 2:
International HIV/AIDS Alliance in Ukraine

| AIDS Support and Technical Resources
Context: HIV/AIDS in Ukraine
• Prevalence (adults 15-49): 1.6% (440,000)*
• Concentrated epidemic: most affected groups are IDUs, sex workers, MSM
• Some bridging to general population through heterosexual transmission
* Source: UNAIDS Epidemiological Fact Sheet on HIV and AIDS, 2008

| AIDS Support and Technical Resources
Case: Alliance-Ukraine
• Programs represent majority of HIV prevention activities in Ukraine– Programs operate in all 24 Oblasts and the Autonomous
Republic of Crimea to reach 300,000 - members of groups most vulnerable to HIV: IDUs, sex workers, MSM, and incarcerated individuals
– Programs work through 101 local NGOs

| AIDS Support and Technical Resources
Case: Alliance-Ukraine
• Program elements:– Behavioral risk reduction strategies for IDUs, sex workers,
MSM; peer support and drop-in centers– Opiate substitution therapy (to reduce illicit drug use and
needle sharing); VCT; STI diagnosis and treatment; links to ART adherence
– Structural interventions; legal and regulatory support for IDUs
• Data-driven process to select prevention activities• Effective linkages

| AIDS Support and Technical Resources
Case: Alliance-Ukraine
• Innovative approaches for MARPs• Medically Assisted Therapy• Peer-Driven Interventions
– Gaining access to most hard-to-reach populations– Targeting young, female and/or stimulant users– Educating peers in community and sharing information about
available services– Piloted for IDUs, now implemented in 17 sites; model being
applied to sex workers
| AIDS Support and Technical Resources
Case: Alliance-Ukraine
• High importance placed on use of data to inform activities and approaches – Surveillance of MARPs, including a size estimation (using
RDS and TLS), special studies of MARPs– Operations research: integrated into program activities to
learn more about risk groups that are hard to reach, to document risk behaviors in newly-defined MARPs (e.g., stimulant users), to understand the behaviors that place people at increased risk of HIV; to explore gender dimensions
– Ability to change the course of programming to match changes in the epidemic

| AIDS Support and Technical Resources
Case: Alliance-Ukraine
• Strong emphasis on community involvement– Recruitment of peer outreach workers from target
communities– Transition to NGO status allows “initiative groups” to involve
more community members and build capacity– Co-locating government and NGO services– Bringing government healthcare workers to community
centers fosters ties between two sectors– Mobile vans
| AIDS Support and Technical Resources
Case: Alliance-Ukraine
• Major role of advocacy for supportive policies– Funding for HIV/AIDS programs– Negotiation of medicines prices (ARVs)– Liberalization of drug policies– Use of rapid testing in VCT
• Significant role in advocacy to allow use of methadone in substitution therapy
• Trainings and “summer schools” on policy and advocacy
| AIDS Support and Technical Resources
Case: Alliance-Ukraine
• Achievements in 2008 include– Prevention services reached 195,379 IDUs, 33,449 female sex
workers, 19,749 MSM and 57,558 prisoners
– Substitution maintenance therapy provided to 2,202 individuals with opioid dependency
– ART provided to 6,070 PLWH and to 9,875 HIV-positive mothers for PMTCT
• Evidence is emerging that harm reduction programs for IDU is stabilizing the HIV epidemic in this risk group– IDU reporting less risky behavior
– Harm reduction program coverage has increased

| AIDS Support and Technical Resources
Case 3:
Avahan-India AIDS Initiative
| AIDS Support and Technical Resources
Context: HIV/AIDS in India
• Prevalence (adults 15-49): 0.36% (2,400,000)*– Concentrated in 4 southern and 2 northeastern states
• Concentrated epidemic: most affected groups are IDUs, sex workers, MSM, truck drivers
• Estimate 80% of HIV-infected people do not know their status
* Source: UNAIDS Epidemiological Fact Sheet on HIV and AIDS, 2008

| AIDS Support and Technical Resources
• Program elements:– Targeted prevention activities with at-risk groups (sex
workers and clients, MSM, transgenders, IDUs, truckers)– Increased access to STI management services, condoms
and target-appropriate behavioral change messages– Lowering stigma and discrimination, develop peer education
messages, capacity building for community ownership
• Data-driven process to select prevention activities• Contributions to national and state-level planning
Case: Avahan-India AIDS Initiative

| AIDS Support and Technical Resources
Case: Avahan-India AIDS Initiative
• Program operates in 605 towns in 83 districts in 6 states to reach– 200,000 sex workers– 60,000 high-risk MSM– 20,000 IDUs– 5 million at-risk men
• Program works through– 134 local NGOs– 7,500 peer educators
• Activities reach over 80% of high-risk people in the 6 states• Moved quickly to scale, applying appropriate financial,
training, and management resources to achieve results

| AIDS Support and Technical Resources
Case: Avahan-India AIDS Initiative
• Multi-layered HIV prevention program• Strong emphasis on building community ownership
and control for prevention and livelihoods improvements
• “Micro-planning” enables peer educators to monitor contacts and identify on a weekly and monthly basis most vulnerable individuals; data also used by state partners and Avahan managers
| AIDS Support and Technical Resources
Case: Avahan-India AIDS Initiative
• Peer educators– Drawn from female and male sex workers, transgender people,
IDUs, and long-distance truck drivers– Each peer educator is responsible for individually mapping then
maintaining contact with 40-50 peers– Promote behavior change, condom usage, seeking treatment for
STIs and other health conditions – Trained to maintain records, analyze results, conduct advocacy with
peers and power structures (such as police and government service providers)
– Responsibilities include basic TB screening with peers and appropriate referrals; referrals for opportunistic infections; emotional and prevention counseling

| AIDS Support and Technical Resources
Case: Avahan-India AIDS Initiative
• Peer micro-planning feeds into monitoring by implementing partners and local NGOs, state partners, and Avahan program managers
• From peer educators to program managers, there is flexibility to respond to changing epidemic conditions and behaviors evident at all levels
• Program has built confidence, skills, and commitment to community and pride in accomplishments among peers, staff and participants
• Program promotes a willingness to learn from mistakes and non-effective approaches and to change quickly, if necessary

| AIDS Support and Technical Resources
Case: Avahan-India AIDS Initiative
• Achievements to date include– 412 program-funded clinics set up that have provided free STI
diagnosis and treatment services
– Lowered STI rates (in some cases reduced by half in 3 years)
– 10 million free condoms distributed monthly
– Stimulated creation of target population support groups, committees and CBOs in most sites at which it works
– Built confidence and self-esteem of target populations to engage in safe sex behaviors and organize for improvements in their lives and communities
• Impact on HIV prevalence will emerge during next round of major data collection
| AIDS Support and Technical Resources
Case: Avahan-India AIDS Initiative
• Challenges– Transitioning program to national and state government
programs will require• Maintaining comprehensive data collection and analysis
• Providing strong technical support to implementing groups at all levels
• Incorporating CBOs created by peers into government structures
– Replicating approach and methods in other countries, including countries with more generalized epidemics

| AIDS Support and Technical Resources
Next Steps
• In sum– Process began with a “standard definition” of combination
prevention– A series of case studies was conducted with the aim of producing a
more actionable description of how to implement combination prevention programs
• Next steps– Initial observations– Conduct 2 more case studies in southern Africa– Produce a series of 5 case studies – Write a comparative analysis summary by December 2009

| AIDS Support and Technical Resources
Initial Findings: Core Components of “Combination Prevention”• “Know your epidemic”
– Track the epidemic, drivers and underlying risk factors; change the composition of the response – and the activities that compose it – with changes in the epidemic (or what can be learned about it)
– Conduct on-going operations (and other) research to understand programmatic “gaps,” e.g., to learn more about risk groups that are not being adequately reached by the programs and the behaviors that put them at risk
– Local actors, e.g. peer educators, must understand data, why they are collecting it and how to use it; workers must be vested in getting quality data
| AIDS Support and Technical Resources
Initial Findings: Core Components of “Combination Prevention”• “A mix of activities that produce a maximum effect in
a given setting”– Add new activities to the “mix” – for example, with the
emergence of strong evidence on the effectiveness of MC– Introducing innovative approaches to solve “old” problems –
for example, increasing reach to younger stimulant users and women through Peer-Driven Interventions
– Bring in new areas of programming to tackle underlying factors that increase vulnerability; NGOs can take on new activities to change social norms, reduce stigma, or address gender dimensions
– Plan locally using local data; then feed data up to affect planning at other levels
| AIDS Support and Technical Resources
Initial Findings: Core Components of “Combination Prevention”• A core commitment to strengthening civil society and the local
response– Strengthening the local response provides the basis for going to
scale
– Requires a sincere investment in the development of civil society and strengthening the response at the local level
– Strong implementing partners with their own mission and vision, who integrate HIV into their own structure
– Program engenders confidence, skills, and commitment to community and pride in accomplishments among peers, staff and participants
– Program promotes a willingness to learn from mistakes and non-effective approaches and to change quickly, if necessary
| AIDS Support and Technical Resources
Initial Findings: Core Components of “Combination Prevention”
• Policy engagement and advocacy at all levels– Serious commitment to creating and nurturing an enabling
environment– Advocating for supportive policies – Persisting, innovating; continuously changing what is done
to get decision makers on board – at national, regional, local and client levels
| AIDS Support and Technical Resources
Acknowledgements
• USAID/Washington & PEPFAR• Participating organizations, their staff, and clients – the case
study hosts!– Alliance-Ukraine and the International HIV/AIDS Alliance– APHIA-II Project, Family Health International– Avahan-India AIDS Initiative– Bill & Melinda Gates Foundation– The Global Fund– USAID Missions in India, Kenya, and Ukraine– PLWH networks– UNAIDS– WHO– NGO coalitions– JSI program offices, and others!

| AIDS Support and Technical Resources
Thank You
For more information,
visit: http://www.aidstar-one.com
|
Produced by the AIDS Support and Technical Assistance Resources Project, Sector 1, Task Order 1 (AIDSTAR-One), USAID Contract # GHH-I-00-07-00059-00, funded January 31, 2008.
The opinions expressed in this presentation do not necessarily reflect the views of USAID or the U.S. Government.


















